Case Report Étude de cascanjsurg.ca/wp-content/uploads/2014/03/39-4-333.pdf · 14457 August/96 CJS...
3
CJS, Vol. 39, No. 4, August 1996 333 P rimary nonHodgkin’s lym- phoma (NHL) is a rare form of malignant breast disease. It constitutes between 0.04% and 0.5% of primary malignant breast tumours in cumulative series. 1–8 A recent re- view 1 reported that approximately 350 cases of primary NHL had been described in the literature. The disease tends to follow a bimodal age distrib- ution, with a unilateral, localized type resembling typical breast carcinoma in older women and a bilateral, more dif- fuse type affecting younger often puerperal women. 2,9 In this paper we report on a young woman with bilat- eral primary breast lymphoma. CASE REPORT A previously healthy 27-year-old white woman, with no family history of breast disease, presented at 7 months’ gestation with profound en- gorgement, tenderness and lumpiness of the right breast but no constitu- tional symptoms. She had a normal vaginal delivery but was unable to breast feed because of breast discom- fort. There was no improvement after treatment with bromocriptine. Examination of the breast revealed a large, firm central mass, 15 cm in di- ameter, in the right breast, with no fixation or skin changes. There was a 5 cm diameter mass in the left breast at the six o’clock position. Fine-needle aspiration biopsy showed cellular atypia but was not diagnostic. Mam- mography of the breast demonstrated ill-defined abnormalities, with calcifi- cations suggestive of malignancy. An incisional biopsy of the right breast revealed diffuse infiltration by a large cell malignant neoplasm with a high mitotic rate. Necrosis was com- mon and in some areas there was a “starry sky” pattern. The cells were non-cohesive and had rounded nuclei with prominent, usually single, nucle- oli that were centrally located (Fig. 1). The cytoplasm was moderately abun- dant and basophilic. Immunoperoxi- dase analysis in formalin-fixed sections showed strong positive staining of the malignant cells for common leukocyte antigen and the B-cell marker L26 (CD20). Staining was negative for ker- atin, S100 protein and histiocytic markers. The tumour was diagnosed as a large cell immunoblastic lymphoma of B-cell type. Findings on bone mar- row and lumbar puncture were normal. Case Report Étude de cas BILATERAL PRIMARY BREAST LYMPHOMA IN PREGNANCY: A CASE REPORT AND LITERATURE REVIEW Andrew W. Kirkpatrick, MD;*Denis J. Bailey, MD, FRCPC;† Harold A.E. Weizel, MD, FRCSC* From the *Division of General Surgery and the †Department of Pathology, University of Toronto, The Toronto Hospital, General Division, Toronto, Ont. Accepted for publication Mar. 24, 1995 Correspondence and reprint requests to: Dr. Andrew W. Kirkpatrick, 590 Wellington St. W, Toronto ON M5V 2X5 © 1996 Canadian Medical Association (text and abstract/résumé) Primary lymphoma of the breast is an uncommon malignant breast tumour, which is seldom distinguished preoperatively from other more common forms of breast cancer. The management differs from the more typical adenocarcinoma of breast in that the emphasis is on systemic chemotherapy. A young white woman presented during the 3rd trimester with bilateral breast enlargement, which failed to involute post partum. Subsequent biopsy revealed primary breast lymphoma of the large cell immunoblastic type. She received systemic chemotherapy and was alive and well with no evidence of recurrence 28 months later. Le lymphome primaire du sein est une tumeur maligne du sein inhabituelle, qu’on peut rarement dis- tinguer avant l’intervention d’autres formes plus courantes de cancer du sein. Le traitement diffère de celui de l’adénome plus typique du sein du fait qu’il faut mettre l’accent sur la chimiothérapie systémique. Une jeune femme blanche s’est présentée pendant le 3 ième trimestre de grossesse avec une hypertrophie bi- latérale des seins, qui ne s’était pas résorbée après l’accouchement. Une biopsie ultérieure a révélé un lym- phome principal du sein du type grande cellule blastique. Elle a subi une chimiothérapie systémique et elle était vivante et en santé sans manifestation de récurrence 28 mois plus tard.
Transcript of Case Report Étude de cascanjsurg.ca/wp-content/uploads/2014/03/39-4-333.pdf · 14457 August/96 CJS...

14457 August/96 CJS /Page 333
CJS, Vol. 39, No. 4, August 1996 333
Primary nonHodgkin’s lym-phoma (NHL) is a rare form ofmalignant breast disease. It
constitutes between 0.04% and 0.5%of primary malignant breast tumoursin cumulative series.1–8 A recent re-view1 reported that approximately350 cases of primary NHL had beendescribed in the literature. The diseasetends to follow a bimodal age distrib-ution, with a unilateral, localized typeresembling typical breast carcinoma inolder women and a bilateral, more dif-fuse type affecting younger oftenpuerperal women.2,9 In this paper wereport on a young woman with bilat-eral primary breast lymphoma.
CASE REPORT
A previously healthy 27-year-old
white woman, with no family historyof breast disease, presented at 7months’ gestation with profound en-gorgement, tenderness and lumpinessof the right breast but no constitu-tional symptoms. She had a normalvaginal delivery but was unable tobreast feed because of breast discom-fort. There was no improvement aftertreatment with bromocriptine.Examination of the breast revealed
a large, firm central mass, 15 cm in di-ameter, in the right breast, with nofixation or skin changes. There was a5 cm diameter mass in the left breastat the six o’clock position. Fine-needleaspiration biopsy showed cellularatypia but was not diagnostic. Mam-mography of the breast demonstratedill-defined abnormalities, with calcifi-cations suggestive of malignancy.
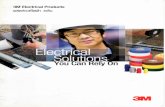
An incisional biopsy of the rightbreast revealed diffuse infiltration by alarge cell malignant neoplasm with ahigh mitotic rate. Necrosis was com-mon and in some areas there was a“starry sky” pattern. The cells werenon-cohesive and had rounded nucleiwith prominent, usually single, nucle-oli that were centrally located (Fig. 1).The cytoplasm was moderately abun-dant and basophilic. Immunoperoxi-dase analysis in formalin-fixed sectionsshowed strong positive staining of themalignant cells for common leukocyteantigen and the B-cell marker L26(CD20). Staining was negative for ker-atin, S100 protein and histiocyticmarkers. The tumour was diagnosed asa large cell immunoblastic lymphomaof B-cell type. Findings on bone mar-row and lumbar puncture were normal.
Case ReportÉtude de cas
BILATERAL PRIMARY BREAST LYMPHOMA IN PREGNANCY: A CASE REPORT AND LITERATURE REVIEW
Andrew W. Kirkpatrick, MD;*Denis J. Bailey, MD, FRCPC;† Harold A.E. Weizel, MD, FRCSC*
From the *Division of General Surgery and the †Department of Pathology, University of Toronto, The Toronto Hospital, General Division, Toronto, Ont.
Accepted for publication Mar. 24, 1995
Correspondence and reprint requests to: Dr. Andrew W. Kirkpatrick, 590 Wellington St. W, Toronto ON M5V 2X5
© 1996 Canadian Medical Association (text and abstract/résumé)
Primary lymphoma of the breast is an uncommon malignant breast tumour, which is seldom distinguishedpreoperatively from other more common forms of breast cancer. The management differs from the moretypical adenocarcinoma of breast in that the emphasis is on systemic chemotherapy. A young white womanpresented during the 3rd trimester with bilateral breast enlargement, which failed to involute post partum.Subsequent biopsy revealed primary breast lymphoma of the large cell immunoblastic type. She receivedsystemic chemotherapy and was alive and well with no evidence of recurrence 28 months later.
Le lymphome primaire du sein est une tumeur maligne du sein inhabituelle, qu’on peut rarement dis-tinguer avant l’intervention d’autres formes plus courantes de cancer du sein. Le traitement diffère de celuide l’adénome plus typique du sein du fait qu’il faut mettre l’accent sur la chimiothérapie systémique. Unejeune femme blanche s’est présentée pendant le 3ième trimestre de grossesse avec une hypertrophie bi-latérale des seins, qui ne s’était pas résorbée après l’accouchement. Une biopsie ultérieure a révélé un lym-phome principal du sein du type grande cellule blastique. Elle a subi une chimiothérapie systémique et elleétait vivante et en santé sans manifestation de récurrence 28 mois plus tard.

14457 August/96 CJS /Page 334
Seven courses of a chemotherapyregimen, consisting of cyclophos-phamide, doxorubicin, vincristine andprednisone were given. This resultedin almost complete clinical resolutionof disease in both breasts. Biopsy of aresidual lump in the scar of the rightbreast that remained after five coursesof chemotherapy revealed coagulativenecrosis with a foreign-body reaction.The appearance was consistent withtumour necrosis secondary to achemotherapy effect. The chemother-apy was followed with bilateral breastradiotherapy (35 Gy in 20 fractions).At follow-up 28 months later the pa-tient was well, with no evidence of re-current disease.
DISCUSSION
Many reported cases of breast lym-phoma may not have been truly pri-mary, because secondary involvementof the breast is often difficult to ruleout. Criteria for a diagnosis of primaryNHL of the breast require the follow-ing: adequate tissue for pathologicalexamination, close association of breast
tissue and the lymphoma infiltrate, noevidence of concurrent widespread dis-ease at presentation and no precedingextramammary lymphoma.2,3,10,11
The B-cell type is the commonlyseen breast lymphoma, with the T-celltype being very rare.1,7,12 An increasedincidence of right-breast versus left-breast involvement has been reportedin numerous series.1,5–7,11,13–15
Bilateral primary NHL of the breasthas been reported sporadically in theliterature.16 The Italian literature in theearly part of the century reported casesof primary bilateral breast lymphomawith an aggressive course in youngwomen.16–18 This has been reportedmore recently, emphasizing two dis-tinct clinicopathological types.2,9 Casereviews revealed a bimodal age distrib-ution with a unilateral type, which re-sembles the typical adenocarcinoma ofthe breast in age distribution, and a bi-lateral, diffuse type that affects younger,often puerperal woman.2,9,19,20
These tumours tend to disseminatewidely, and histologically they most of-ten correlate with a small noncleavedcell, or Burkitt-type, lymphoma.
Two series from Africa,21,22 have re-ported on Burkitt’s lymphoma of thebreast associated with pregnancy andlactation. The majority of the caseswere characterized by widespread ag-gressive disease. However, they werenot staged according to presently ac-cepted criteria and could not be classi-fied as primary lymphoma of thebreast.The small noncleaved cell that
constitutes Burkitt’s and Burkitt’s-type lymphoma is distinct from thecells that constitute diffuse large celllymphoma, which is the most com-monly reported primary lymphomaof breast,1,4,10–13,23,24 and the large cellimmunoblastic lymphoma that thispatient had. It has been suggestedthat Burkitt’s lymphoma25 and someother primary NHLs of the breast maybe derived from mucosa-associatedlymphoid tissue (MALT) and have adifferent behaviour from nodally de-rived lymphomas. There appears tobe a markedly increased potential forprolonged disease-free survival aftereven local therapy in distinction tothe non-MALT lymphomas. Thistheory, however, is not universallyaccepted.20
Lymphocytic mastopathy, or lym-phocytic lobulitis, is described as apossible autoimmune breast diseasethat is characterized by lymphocyticinfiltrates and sclerosis.10,20,26 It hasbeen suggested that this conditionmay be an antecedent of mammarylymphoma. This might explain howMALT lymphomas develop in breast,which normally does not have an ap-preciable lymphoid component.Preoperatively NHL of the breast
is usually not distinguished from themore common adenocarcinoma ofbreast.9 Clinical features that mightraise suspicion of lymphoma include:a rapidly enlarging mass, absence ofnipple discharge and retraction, mul-tiple or bilateral lesions, violaceous
KIRKPATRICK, BAILEY, WEIZEL
334 JCC, Vol. 39, no 4, août 1996
FIG. 1. Numerous cells having rounded nuclei with large, single, central nucleoli and moderately abun-dant, strongly basophilic cytoplasm. These features are most in keeping with B immunoblasts (hema-toxylin–eosin, original magnification × 450).

14457 August/96 CJS /Page 335
skin colour and a softer consistencythan expected in axillary nodes whenpresent.11
Frozen or quick sections may notbe reliable in distinguishing lym-phoma from adenocarcinoma histo-logically.1,23 Fine-needle aspiration cy-tology has been suggested as the bestmethod of preoperative assessment forprimary breast lymphoma.9,11,23 Im-munohistochemical study of frozen orparaffin-embedded tissue sections,with a panel of antibody reagents maybe required to establish a definite di-agnosis.In 1987 Brustein and associates14
reported on 57 cases of primary breastlymphoma and found clinical stageand histologic grade to be the mostimportant prognostic factors for out-come, a finding corroborated by oth-ers.12,23 Although treatment resultsvary greatly among reported series,avoidance of radical surgery in favourof systemic chemotherapy has gener-ally been recommended.5,7,11,13,22
CONCLUSIONS
Because of the rarity and variabilityof primary lymphoma of the breast,the question of the most appropriatetreatment is controversial. Cooperativemulticentre studies will be required toaccrue appropriate numbers of compa-rable patients to study and thus to de-rive appropriate therapeutic principles.Practising surgeons with an interest indiseases of the breast must be aware ofthe possibility of lymphoma in the dif-ferential diagnosis of breast masses soas to avoid unnecessary surgery. Ahematologist-oncologist should beconsulted to help in determining man-agement that will give the best results.
We thank Dr. U. Ambus, Department ofSurgery, The Toronto Hospital, General Divi-sion, for reviewing the manuscript.
References
1. Giardini R, Piccolo C, Rilke F: Lym-phomas of the breast. Cancer 1992;69: 725–735
2. Hugh JC, Jackson FI, Hanson J et al:Primary breast lymphoma: an im-munohistological study of 20 newcases. Cancer 1990; 66: 2602–2611
3. Mambo NC, Burke JS, Butler JJ: Pri-mary malignant lymphomas of thebreast. Cancer 1977; 39: 2033–2040
4. Elavathil LJ, Kahn HJ, Hanna W:Primary multilobulated B-cell lym-phoma of the breast. Arch Pathol LabMed 1989; 113: 1081–1084
5. Shiiki S, Fuchimoto S, Inoue F et al:Primary malignant lymphoma of thebreast mimicking breast carcinoma: acase report. Jpn J Surg 1991; 21:244–248
6. Bucciarelli E, Cavaliere A, Sidoni Aet al: Bilateral primary malignant lym-phoma of the breast. A case report.Tumori 1988; 74: 581–591
7. Eskelinen M, Collan Y, Puittinen J etal: Lymphoma of the breast. AnnChir Gynaecol 1989; 78: 149–152
8. Mattia AR, Ferry JA, Harris NL:Breast lymphoma: a B-cell spectrumincluding the low grade B-cell lym-phoma of mucosa associated lym-phoid tissue. Am J Surg Pathol 1993;17: 574–587
9. Jeon HJ, Akagi T, Hoshida Y et al:Primary non-Hodgkin malignantlymphoma of the breast. An im-munohistochemical study of sevenpatients and literature review of 152patients with breast lymphoma inJapan. [review] Cancer 1992; 70:2451–2459
10. Aozasa K, Oshawa M, Saeki K et al:Malignant lymphoma of the breast:immunologic type and associationwith lymphocytic mastopathy. Am JClin Pathol 1992; 97: 699–704
11. Misra A, Kapur BM, Rath GK: Pri-mary breast lymphoma. J Surg Oncol1991; 47: 265–270
12. Cohen PL, Brooks JJ: Lymphomas ofthe breast: a clinicopathologic andimmunohistochemical study of pri-mary and secondary cases. Cancer1991; 67: 1359–1369
13. El-Gazawy IM, Singletary SE: Surgi-cal management of primary lym-phoma of the breast. Ann Surg 1991;214: 724–726
14. Brustein S, Kimmel M, Lieberman etal: Malignant lymphoma of thebreast. A study of 53 patients. AnnSurg 1987; 205: 144–150
15. Jackson FI, Lalani ZH: Breast lym-phoma: radiologic imaging and clini-cal appearances. Can Assoc Radiol J1991; 42: 48–54
16. Kay S: Lymphosarcoma of the femalemammary gland. AMA Arch Pathol1955; 60: 575–579
17. Tweeddale DN, Mahr MM: Sec-ondary lymphosarcoma of the breastin pregnancy: report of a case. ObstetGynecol 1964; 24: 584–586
18. Adair FE, Herrmann JB: Primarylymphosarcoma of the breast. Surgery1944; 16: 836–853
19. Rooney N, Snead D, Goodman S etal: Primary breast lymphoma withskin involvement arising in lympho-cytic lobulitis. Histopathology 1994;24: 81–84
20. Arber DA, Simpson JF, Weiss LM etal: Non-Hodgkin’s lymphoma in-volving the breast. Am J Surg Pathol1994; 18: 288–295
21. Shepherd JJ, Wright DH: Burkitt’stumour presenting as bilateralswelling of the breast in women ofchild-bearing age. Br J Surg 1967;54: 776–780
22. Durodola JI: Burkitt’s lymphomapresented during lactation. Int J Gy-naecol Obstet 1976; 14: 225–231
23. Dixon JM, Lumsden AB, KrajewskiA et al: Primary lymphoma of thebreast. Br J Surg 1987; 74: 214–217
24. Lamovic J, Jancar J: Primary malig-nant lymphoma of the breast: lym-phoma of the mucosa-associated lym-phoid tissue. Cancer 1987; 60:3033–3041
25. Wright DH: Histogenesis of Burkitt’slymphoma: a B-cell tumour of mu-cosa-associated lymphoid tissue.IARC Sci Publ 1985; 60: 37–45
26. Schwartz IS, Strauchen JA: Lympho-cytic mastopathy. An autoimmunedisease of the breast? Am J ClinPathol 1990; 93: 725–730
BREAST LYMPHOMA IN PREGNANCY
CJS, Vol. 39, No. 4, August 1996 335