Case Report Pitfalls in Neuroimaging of Headache: A Case...
4
Hindawi Publishing Corporation Case Reports in Otolaryngology Volume 2013, Article ID 735147, 3 pages http://dx.doi.org/10.1155/2013/735147 Case Report Pitfalls in Neuroimaging of Headache: A Case Report and Review of the Literature V. Vallamkondu, 1 M. Shakeel, 1 A. Hussain, 1 and D. McAteer 2 1 Department of Otolaryngology-Head and Neck Surgery, Aberdeen Royal Infirmary, Aberdeen AB252ZN, UK 2 Department of Radiology, Aberdeen Royal Infirmary, Aberdeen, UK Correspondence should be addressed to V. Vallamkondu; [email protected] Received 17 December 2012; Accepted 5 February 2013 Academic Editors: D. K. Chhetri and L. J. DiNardo Copyright © 2013 V. Vallamkondu et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Headache is a common symptom, with a lifetime prevalence of over 90% of the general population in the United Kingdom (UK). It accounts for 4.4% of consultations in primary care and 30% of neurology outpatient consultations. Neuroimaging is indicated in patients with red flag features for secondary headaches. e guidelines recommend CT or MRI scan to identify any intracranial pathology. We present a unique case where the initial noncontrast CT scan failed to identify a potential treatable cause for headache. A middle aged man presented with headache and underwent a CT scan without contrast enhancement. e scan was reported as normal. e headache persisted for years and the patient underwent a staging CT scan to investigate an oropharyngeal cancer. is repeat CT scan utilized contrast enhancement and revealed a meningioma. Along with other symptoms, headache is an established presenting complaint in patients with meningioma. e contrast enhanced CT brain proved superior to a nonenhanced CT scan in identifying the meningioma. In a patient with persistent headache where other causes are excluded and a scan is to be requested, perhaps contrast enhanced CT is a better option than a plain CT scan of brain. 1. Introduction Headache is a common symptom, with a lifetime prevalence of over 90% of the general population in the clinical practice [1]. Overall 1-year prevalence of headache in European adults is 51% [2]. It accounts for 4.4% of consultations in primary care and 30% of neurology outpatient consultations. Neuroimaging is indicated in select patients with headache. e guidelines suggest that either a CT or MRI scan can be done to identify any intracranial pathology. We report a unique case where the initial CT scan failed to identify a potentially treatable cause for headache. 2. Case Report A 74-year-old Caucasian male originally presented to the headache clinic with 1-year history of right sided headache affecting the frontotemporooccipital region. It was daily per- sistent headache with a pain intensity of 4/10. e nature of pain varied between dull ache with short lived shooting in the right retroorbital area once or twice a week with occasional photophobia. ere was no nausea or visual dysfunction. Pos- tural changes or valsalva did not aggravate the headache. e headache failed to settle with analgesics. ere was a previous history of migraine in his teens which varied in frequency and severity. e last episode of migraine was experienced 10 years ago. ere was a positive family history of migraine with both mother and sister undergoing treatment presently. e patient had significant medical history of ischemic heart disease, diabetes mellitus, and COPD. ere was no clinical abnormality on routine head and neck examination. Detailed neurological examination failed to reveal any abnormality. e differential diagnosis included hemicrania continua or chronic migraine. A trial of indomethacin with a starting
-
Upload
duongkhanh -
Category
Documents
-
view
217 -
download
0
Transcript of Case Report Pitfalls in Neuroimaging of Headache: A Case...

Hindawi Publishing CorporationCase Reports in OtolaryngologyVolume 2013, Article ID 735147, 3 pageshttp://dx.doi.org/10.1155/2013/735147
Case ReportPitfalls in Neuroimaging of Headache: A Case Report andReview of the Literature
V. Vallamkondu,1 M. Shakeel,1 A. Hussain,1 and D. McAteer2
1 Department of Otolaryngology-Head and Neck Surgery, Aberdeen Royal Infirmary,Aberdeen AB252ZN, UK
2Department of Radiology, Aberdeen Royal Infirmary, Aberdeen, UK
Correspondence should be addressed to V. Vallamkondu; [email protected]
Received 17 December 2012; Accepted 5 February 2013
Academic Editors: D. K. Chhetri and L. J. DiNardo
Copyright © 2013 V. Vallamkondu et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Headache is a common symptom, with a lifetime prevalence of over 90% of the general population in the United Kingdom (UK).It accounts for 4.4% of consultations in primary care and 30% of neurology outpatient consultations. Neuroimaging is indicatedin patients with red flag features for secondary headaches. The guidelines recommend CT or MRI scan to identify any intracranialpathology.We present a unique case where the initial noncontrast CT scan failed to identify a potential treatable cause for headache.A middle aged man presented with headache and underwent a CT scan without contrast enhancement. The scan was reported asnormal.The headache persisted for years and the patient underwent a staging CT scan to investigate an oropharyngeal cancer.Thisrepeat CT scan utilized contrast enhancement and revealed a meningioma. Along with other symptoms, headache is an establishedpresenting complaint in patients with meningioma. The contrast enhanced CT brain proved superior to a nonenhanced CT scanin identifying the meningioma. In a patient with persistent headache where other causes are excluded and a scan is to be requested,perhaps contrast enhanced CT is a better option than a plain CT scan of brain.
1. Introduction
Headache is a common symptom, with a lifetime prevalenceof over 90% of the general population in the clinical practice[1]. Overall 1-year prevalence of headache in Europeanadults is 51% [2]. It accounts for 4.4% of consultations inprimary care and 30% of neurology outpatient consultations.Neuroimaging is indicated in select patients with headache.The guidelines suggest that either a CT or MRI scan canbe done to identify any intracranial pathology. We report aunique case where the initial CT scan failed to identify apotentially treatable cause for headache.
2. Case Report
A 74-year-old Caucasian male originally presented to theheadache clinic with 1-year history of right sided headache
affecting the frontotemporooccipital region. It was daily per-sistent headache with a pain intensity of 4/10. The nature ofpain varied between dull ache with short lived shooting in theright retroorbital area once or twice a week with occasionalphotophobia.Therewas no nausea or visual dysfunction. Pos-tural changes or valsalva did not aggravate the headache.Theheadache failed to settle with analgesics.There was a previoushistory of migraine in his teens which varied in frequencyand severity. The last episode of migraine was experienced10 years ago. There was a positive family history of migrainewith both mother and sister undergoing treatment presently.The patient had significant medical history of ischemic heartdisease, diabetes mellitus, and COPD.
There was no clinical abnormality on routine head andneck examination. Detailed neurological examination failedto reveal any abnormality.
The differential diagnosis included hemicrania continuaor chronic migraine. A trial of indomethacin with a starting

2 Case Reports in Otolaryngology
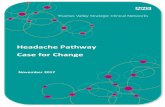
Figure 1: Noncontrast CT scan showing age related atrophychanges.
Figure 2: Contrast CT scan showing a 4 cm enhancing mass inthe right middle cranial fossa in keeping with a sphenoidal ridgemeningioma.
dose of 25mg was given and the dose was titrated slowlyupward weekly depending on his tolerability and his INR. Anon-contrast CT scan of the brain was carried out to rule outintracranial pathology.
During the follow-up visits the headache hadmigrated tothe rest of cranium.The CT scan showed age related cerebralatrophy with no intracranial abnormality (Figure 1). Patientwas reassured that no serious intracranial abnormality wasidentified and was treated with a diagnosis of migraine.The response to the standard prophylactic and therapeutictreatment for migraine was suboptimal and variable.
Six months later, the patient presented with new symp-toms of right sided odynophagia and dysphagia which wereconfirmed to be due to the advanced oropharyngeal carci-noma with cervical metastasis. A staging contrast enhancedCT scan of head, neck, and chest was performed whichalso identified a 4 cm enhancing mass in the right middlecranial fossa in keeping with a sphenoidal ridge menin-gioma (Figure 2). There was mild surrounding edema but
no midline shift was noted. The case was discussed in themultidisciplinary meeting and it was concluded that brainmetastasis from the oropharyngeal cancer was unlikely. Thepatient underwent surgery with postoperative radiotherapyfor his oropharyngeal cancer. Because of the serious comor-bidity, surgical resection of meningioma was considered toorisky and inadvisable. The patient will remain under serialradiological (MRI scan) surveillance for hismeningioma.Theheadache is thought to be secondary tomeningioma and painis managed with standard analgesics.
3. Discussion
Headache is one of the most common presenting featuresin general practice, neurology, or otolaryngology clinics.Headache constitutes a major public health problem andsocioeconomic burden.
There are many classification systems for headaches.World Health Organization (WHO) classification was pub-lished in Cephalalagia 2004 based on the InternationalHeadache Society’s revised International Classification ofHeadache Society’s Disorders (ICHD 2) [3]. The BritishAssociation for the Study of Headache simplified the ICHD 2into primary and secondary headaches. Primary headachesare not associated with underlying pathology. Migraine,cluster headache, and tension headaches are grouped asprimary headaches. Secondary headache is due to underlyingpathology such as infections, vascular causes, trauma, andneoplasms [4].
The aetiology of most headaches can be elucidated bycareful history and examination. The diagnosis is furthersupplemented by judicious use of radiological investigation.If neurological symptoms are present then a brain CT orMRI should be done as a primary investigation [5]. Perhapscontrast enhanced CT is a better option than a plain CT scanof brain.The disadvantages ofMRI as a first line investigationare cost, availability, and perhaps most importantly, a veryhigh sensitivity leading to a high detection of indeterminatefindings.
In our case, the non-contrast CT failed to diagnosemeningioma which is thought to be the underlying causefor his headache. Headache may be noticed in 60% ofpatients with intracranial tumour but headache may not bethe presenting feature. Schankin et al. [6] published dataon 58 cases of meningioma, 40% of meningioma patientshad associated headache features. Of these, the pain wasmigraine-like in 22% and tension-type-headache- (TTH-)like in 57%. There is a consensus that mass lesion producesheadache either by inducing pressure on pain sensitive duraor arachnoid membranes or by increase in ICP but robustevidence is lacking. Moreover the literature suggests thatpatients with meningioma present with isolated headachewithout clinical signs of raised intracranial pressure [7].
In our case there were no neurological symptoms to raisethe suspicion of intracranial neoplasm. Therefore he was notgiven any contrast during neuroimaging. The exact causeof his headache remained unknown. The meningioma was

Case Reports in Otolaryngology 3
diagnosed on a repeat CT scan with contrast enhancement.Meningioma is a potentially treatable cause of headache.
4. Conclusion
Theneuroimaging guidelines for investigation of headache donot recommend contrast enhancement as routine. However,this case highlights the inadequacy of the non-contrast CTscan to diagnose meningioma. In a patient with persistentheadache where other causes are excluded and a CT scanis to be requested, the clinician should be aware of thelimitations in the sensitivity of an un-enhanced head CT, andwhere concerning symptoms persist, an alternative imagingmodality such as MRI scan should be considered.
Authors’ Contributions
Mr. V. Vallamkondu contributed to literature search andpreparing and finalizing the paper. Mr. M. Shakeel con-tributed to data collection and preparing and finalizingthe paper. Mr. A. Hussain contributed to data collectionand preparing and finalizing the paper. Dr. D. McAteercontributed to radiology data collection and preparing andfinalizing the paper.
References
[1] B. K. Rasmussen, R. Jensen,M. Schroll, and J. Olesen, “Epidemi-ology of headache in a general population—a prevalence study,”Journal of Clinical Epidemiology, vol. 44, no. 11, pp. 1147–1157,1991.
[2] L. J. Stovner, J. A. Zwart, K. Hagen, G. M. Terwindt, andJ. Pascual, “Epidemiology of headache in Europe,” EuropeanJournal of Neurology, vol. 13, no. 4, pp. 333–345, 2006.
[3] Headache Classification Subcommittee of the InternationalHeadache Society, “The International Classification ofHeadache Disorders: 2nd edition,” Cephalalgia, vol. 24,supplement 1, pp. 9–160, 2004.
[4] British Association for the Study of Headache, Guidelines forAll Healthcare Professionals in the Diagnosis and Managementof Headache, 3rd edition, 2010, http://217.174.249.183/upload/NS BASH/2010 BASH Guidelines.pdf.
[5] Scottish Intercollegiate Guidelines Network, “Diagnosis andmanagement of headache in adults. Guideline no. 107,” Novem-ber 2008.
[6] C. J. Schankin, M. Krumbholz, P. Sostak, M. Reinisch, R.Goldbrunner, and A. Straube, “Headache in patients with ameningioma correlates with a bone-invasive growth pattern butnot with cytokine expression,” Cephalalgia, vol. 30, no. 4, pp.413–424, 2010.
[7] M. Levin, “Resident and fellow section,” Headache, vol. 49, no.4, pp. 627–630, 2009.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com