Headache Management - c.ymcdn.com · (Headache Classification Subcommittee of the International...
15
4/14/18 1 Headache Management Utilizing an Integrative Approach Karen Williams, DNPc, RN, FNP-BC TNP 2018 1 Patient with refractory headaches • 44yr old female with a history of refractory headaches for the last 2 years • Migraines since 1990’s- described as posterior pressure, treated with Advil. If untreated will cause photophobia/phonophobia & worse with exertion • 2 nd type started 2 years prior. Described as bi-frontal and right eye pressure increases to 4-6/10 and occasion to 8-9/10 w/photo/phonphobia • Would occur upon waking up in the morning, worsen with exertion and when dehydrated. Lasting up to 2 weeks and occurring monthly • Treated with zomig and advil- with about 1/3 resolved with this • Treated in past by a neurologist- MRI of Brain WNL 2 VITAL BEHAVIORS Diagnosis Correctly Treat Appropriately Communicate Effectively Headache Management 3 Objectives • Discuss the burdens and risk factors associated with headaches • Review tension type headache and migraine • Identify appropriate medication treatments and medication overuse headaches • Review alternative headache treatments • Case presentations 4 Disclosures • Off label use of medications • The views expressed in this presentation are those of the author and do not reflect the official policy of the Department of the Veterans Affairs, Department of Defense, or U.S. Government 5 Epidemiology of Headaches • Primary headache disorder is estimated to affect 45(+) million individuals in the US (Cleveland Clinic Health Information Center, 2008) • World-wide, the percentage of the adult population with an active headache disorder is 46% (Stover, 2007) – 42% suffer from tension-type – 11% from migraine – 3% from chronic daily headache 6
Transcript of Headache Management - c.ymcdn.com · (Headache Classification Subcommittee of the International...

4/14/18
1
Headache Management Utilizing an Integrative Approach
Karen Williams, DNPc, RN, FNP-BCTNP 2018
1
Patient with refractory headaches
• 44yr old female with a history of refractory headaches for the last 2 years
• Migraines since 1990’s- described as posterior pressure, treated with Advil. If untreated will cause photophobia/phonophobia & worse with exertion
• 2nd type started 2 years prior. Described as bi-frontal and right eye pressure increases to 4-6/10 and occasion to 8-9/10 w/photo/phonphobia
• Would occur upon waking up in the morning, worsen with exertion and when dehydrated. Lasting up to 2 weeks and occurring monthly
• Treated with zomig and advil- with about 1/3 resolved with this
• Treated in past by a neurologist- MRI of Brain WNL
2
VITAL BEHAVIORS
Diagnosis Correctly
Treat Appropriately
Communicate Effectively
Headache Management
3
Objectives
• Discuss the burdens and risk factors associated with headaches
• Review tension type headache and migraine
• Identify appropriate medication treatments and medication overuse headaches
• Review alternative headache treatments
• Case presentations
4
Disclosures
• Off label use of medications
• The views expressed in this presentation are those of the author and do not reflect the official policy of the Department of the Veterans Affairs, Department of Defense, or U.S. Government
5
Epidemiology of Headaches
• Primary headache disorder is estimated to affect 45(+) million individuals in the US (Cleveland Clinic Health Information Center, 2008)
• World-wide, the percentage of the adult population with an active headache disorder is 46% (Stover, 2007)
– 42% suffer from tension-type– 11% from migraine– 3% from chronic daily headache
6

4/14/18
2
Socioeconomic
• Headache is the most common pain-related complaint among workers(Stewart, 2003)
• One of the most common complaints in the ER, with over 3 million ER visits in 2000 (Stewart, 2003)
• Most common cause of absenteeism from work and school (Cleveland Clinic Health Information Center, 2008)
• Estimated $17 billion annually, for the cost of healthcare associated with migraines (Goldberg, 2005)
7
Types of Headache Disorders
• Primary- not associated with any cause or pathology– Migraine, Tension, cluster migraine
• Secondary- associated with some underlying pathology– Traumatic, Drug/substance related, infection, malignancy, vascular(Headache Classification Subcommittee of the International Headache Society, 2013)
8
VITAL BEHAVIORS
Diagnosis Correctly
Treat Appropriately
Communicate Effectively
Headache Management
9
Step 1- Diagnosis the headache
• Migraine verses Tension Type
• Chronic Daily Headache
• Medication overuse
• Trauma related
• Disease related
• Others?
10
11
Tension- Type Headache
• The most common primary headache
• Pain is bilateral, often described as pressing, band–like or vise-like. In the forehead, temples or back of head and neck
• Intensity - Mild to moderate
• Can last from 30 minutes to 7 days
• Can be associated with photophobia or phonophobia but not both
12

4/14/18
3
Tension(Continued)
• Often accompanied by fatigue, inadequate sleep
• Triggered by stress, fatigue or emotional bursts
• Usually not aggravated by physical activity
• Usually relieved with OTC analgesics, relaxation, reduction of stress
• Frequently coexists with migraine(Headache Classification Subcommittee of the International Headache Society, 2013)
13
Case #1
14
18 year old Male High School Student
• History of occasional annoying headaches for the last year• The last month have increased to almost daily lasting about an hour at a
time• Described as a band around the head, sometimes accompanied with
phonophobia• Denies any nausea/vomiting and not worsened by routine physical
activities• Relieved by Tylenol or OTC NSAIDS• Triggers: Stress and inadequate sleep• Family history was noncontributory• Neurologic exam was normal
15
Migraine
• World wide prevalence of 11% and is the 2nd most common primary headache (Stovner, et al., 2007)
• Affecting women 3 times more than men, with a comparison of 17% female vs 6% male (Lipton & Bigal, 2007)
• Occurs from childhood to adulthood with the peak prevalence occurring in mid-adulthood (Lipton & Bigal, 2007)
16
17
Migraine
• Recurrent episodes of generally unilateral (may be bilateral), pulsating/throbbing pain
• Usually aggravated by physical activity and often relieved with sleep
• Pain is moderate to severe and debilitating
• Associated symptoms of nausea, vomiting, photophobia and phonophobia
• Time frame of 4 to 72 hours, if untreated(Headache Classification Subcommittee of the International Headache Society, 2013)
18

4/14/18
4
19
Case #2
20
38 year old Pediatrician
• 38 yr old female with reoccurring headaches since high school: left more often than right temporal or occasional bi temporal pressure
• Nausea occasional vomiting lasting 24 hours• Headaches could interfere with her activities including awakening her
from sleep• Frequency was 1-4 times per month, now weekly• OTC’s of little help• Triggers: Stress and heat, not triggered by menses, foods or alcohol• No recent contraceptive use• Family history was noncontributory• Neurologic exam was normal
21
Step 2 - Headache Evaluation and Diagnosis
• Accurate and detailed headache history
– Family Hx, Personal medical Hx, Hx of head trauma, Time frame of headache, age of onset, how frequent, duration, triggers, aggravating factors, co-morbid illnesses, impact on family and work/school
– Clinical description of the headache: Location, intensity, nature of the pain, preceding symptoms, aura or neurologic symptoms
– Do they have more than 1 type of headache?
22
Helpful questions
23
Diagnosis of Migraine or TTH
• Helpful questions:– How do headaches interfere with your life?
– How Frequently do you experience headaches of any type?
– Has there been a change in your headache pattern over the last 6 months?
– How often and how effectively do you use medications to treat headaches? (Martin, 2004)
24

4/14/18
5
Headache Assessment Tools
• Headache Calendar- iHeadache/Migrainebuddy (free phone apps)
• Headache Impact test (6 questions)
– Helps patients communicate the severity of the headache pain to their provider
• The Migraine Disability Assessment Questionnaire (5 questions)
– Measures headache-related disability in: work/school, household and family/social
• Migraine Specific Quality of Life Questionnaire (MSQ) (14 questions)
– Role Function-Restrictive
– Role Function- Preventive
– Emotional Function
25
Step 3 - Physical Exam
• Neurological exam: Cranial nerves, Strength, Coordination, DTR’s (rule-out papilledema, diploplia, facial weakness, gait disturbances, nuchal rigidity)
• ROM of neck/Palpation of the TMJ and occipital nerves (looking for tenderness or edema, trigger points in paraspinal, shoulder areas)-
• Blood Pressure: diastolic over 120 mmHg are associated with an increase in headaches
• Consider CBC, CMP, Thyroid function testing, Vit D level (Looking for treatable cause) (Deluca & Bartleson, 2010)
•Rule out a systemic illness or other organic cause26
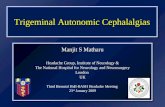
Trigger points
With permission from Sean Riehl Real Bodywork 27
Red Flags SNOOP4
• Systemic symptoms or disease (fever, weight loss, jaw claudication)
• Neurologic signs or symptoms (motor weakness, memory loss, papillary abnormality, sensory loss)
• Onset sudden (if < 60 sec, called thunderclap headache)
• Onset before age 5 or after age 50
• Pattern change from prior headaches
28
SNOOP4 (continued)
• Precipitated by Valsalva maneuver- worrisome for underlying vascular lesion
• Positional – headache precipitated by laying down or standing up
• Papilledema- elevated intracranial pressure (DeLuca & Bartleson, 2010);(Sheller, Vargas,& O’neil 2016)
29
Diagnostics for Red Flags
• Imaging studies: Ct of head, MRI– Looking for structural abnormalities
• Blood chemistries and Blood counts– Sed rate should be measured in adults that are 50 and older
• Lumbar puncture (after obtaining brain imaging): in suspected meningitis, subarachnoid hemorrhage, Pseudotumor cerebri, encephalitis or systemic illness (lupus, sarcoidosis, vasculitis) (Elkind, 2004)
30

4/14/18
6
Case # 3
31
39 year old Designer
• Female presents to the ER: complains of a severe occipital headache and vomiting
• Describes it as the “Worst headache of her life”, stated that is started suddenly after a stressful day at work
• She had a similar headache 2 days prior but it only lasted a few seconds, then resolved
• No prior history of a similar headache• No prior head trauma, fever, vision changes, photophobia• Medical history: 2 normal pregnancies, only taking oral contraceptive for
15 years, no use of illicit drugs, tobacco or alcohol• Family history was noncontributory
32
39 yr old DesignerPhysical Exam
Obese female, mild distress due to painPulse- 78, B/P 160/80, Resp-20, AfebrileHead is normal with no tenderness, ENT exam WNL, pupils are small at 2mm
but reactive to light with EOM intact, no photophobia or nystagmus. Fundi and optic discs WNL.
No neck mass but does have nuchal rigidityChest/heart exam WNL, lungs clear with normal respiratory effort. Abdomen
soft and nontenderNeuro exam reveal fully alert, orientated and mildly anxious. Cranial nerves
intact, with motor strength symmetrical, DTR’s symmetric and brisk without clonus. Cerebellar function and sensory systems are normal
CBC, CMP, U/A are WNLNoncontrast Cerebral CT : hyperdensity in the subarachnoid space
33
Step 4- Identify Common Triggers of Migraine
• Hormonal-– menstruation, ovulation, oral contraceptives with estrogen
• Dietary-– ETOH, nitrates, caffeine, aged cheese, MSG, aspartame, chocolate,
skipping meals• Psychological-
– stress, anxiety, depression• Environmental-
– glare, flashing lights, strong odors, barometric changes, high altitude• Sleep-
– lack of or too much sleep• Drug-related –
– Nitroglycerin, Histamine, Hydralazine, Ranitidine, Estrogen
34
Identify Exacerbating Factors
• Medication overuse• Caffeine overuse• Depression/anxiety/stress• Increased BMI• Suboptimal sleep- < 6 or > 8, Sleep apnea- untreated• Low economic status
• Frequency of baseline headache- greater frequency leads to progression
• Nutrition/diet- skipping meals
• Tobacco use
• Prior head or neck trauma*
• Any use of barbiturates or opioids can increase chance of CDH, to include Butalbital (Fioricet) (Sheeler et.al, 2016); Murinova & Karshin, 2015)
35
VITAL BEHAVIORS
Diagnosis Correctly
Treat Appropriately
Communicate Effectively
Headache Management
36

4/14/18
7
Step 5- Action Plan
• Preventative
• Acute treatments
• Lifestyle modifications
• Education- on going
• Realistic expectations
37
Migraine Treatments
38
Abortive Treatments for Migraine
• Abortives: – First line: NSAIDS/Aspirin or Acetaminophen, (Caffeine + analgesic )
– First line if moderate to severe: Triptans (7 types) (Triptan/NSAID)• Constrict dilated blood vessels, reduce neuropeptide release and
inhibit impulse transmission centrally within the trigeminovascularsystem
• Consider the associated symptoms for type of delivery– Oral, Subcutaneous injection, Intranasal
• May need to try several, Individual responses cannot be predicted
– Ergotamine/Dihydroergotamine (DHE)- Nasal spray, Injection
– Oxygen inhalation (100%) for cluster migraine
(Marmura, Silberstein, & Schwedt , 2015); (Murinova, & Krashin, D. 2015); (Pringsheim, Davenport, Marmura, Schwedt, & Silberstein, 2016); (Silberstein, 2000)
39
Preventative Treatments for Migraines• Consider if 4 or more headaches per month, consider co-morbid
conditions– Propranolol*– Topiramate* *FDA approved for migraine prevention – Divalproex*– Antidepressants – TCA’s– NSAIDS– Tizanidine – Calcium Channel Blockers- Cluster migraine
(Sheeler, et al., 2016); (Marmura, Silberstein & Schwedt, 2015); (Murinova & Krashin, 2015); (Pringsheim, Davenport, Marmura, Schwedt & Silberstein, 2016)
Avoid narcotics& benzodiazepines
40
Preventatives(continued)
• Riboflavin (Vit B2) - Dosed at 100mg, 2 tabs twice per day• Magnesium 400mg per day (dose in evening) (Murinova & Krashin, 2015)
• OnabotulinumtoxinA (Botox) * FDA (Sheeler, et al., 2016); (Murinova & Krashin, 2015)
• Cefaly *FDA
• Acupuncture - more research showing this to be promising (Coeytaux & Befus, 2016)
• Occipital Nerve Blocks (Sheeler, et al., 2016); (Murinova & Krashin, 2015)
• Biofeedback and Cognitive therapy (Sheeler, et al., 2016); (Murinova & Krashin, 2015)
41
Calcitonin Gene-Related Peptide
(CGRP)
• Strongly associated with migraine and cluster headache
– 37 Amino-acid sensory neuropeptide- powerful vasodilator– Detected in the trigeminovasclar system
– Higher concentrations in the blood during a migraine
• Blockage- ? Prevent and/or treat a migraine
! "#$ %&' ()*+(ℎ)*%- &)*./01 1213)4 &6 "#$ %&' )&3)*+7 &)*./01 1213)4 {9: 1213)4} ,
=/3ℎ +&&)*.%3+&> .%170-%30*)
(Deen et al., 2017; Hay & Walker, 2017; Krasenbaum, 2017)
42

4/14/18
8
CGRP Inhibitors• Monoclonal antibodies
– Block production of CGRP– Reduce level of CGRP released– Prevent CGRP from activating
• Evidence shows effectiveness- in episodic and chronic migraine
• Side effects- URI/UTI, fatigue, back pain, N/V arthralgia, injection site pain– Less side effects than Topiramate
(Deen et al., 2017; Hay & Walker, 2017; Krasenbaum, 2017)
43
Sleep Headache
Irritability/MoodCognitive
Symptom Interaction
44
Preventatives and Co-morbid ConditionsCondition Consider Avoid or CautionDepression TCA, SSRI, SNRI Beta Blocker
Bipolar Disorder Divalproex,* Topiramate*
TCA, SSRI, SNRI
Anxiety TCA, SSRI, SRNI, Beta Blocker*
Sleep Disturbances TCA, Prazosin, Magnesium
Stroke/CVD/HemiplegicMigraine
Aspirin, Magnesium Ergot, Triptan
Fibromyalgia TCA, SNRI, Pregablin Beta Blockers
Obesity Topiramate TCA, Divalproex, SSRI
Epilepsy Topiramate, Divalproex TCA, SSRI, SNRI
Raynaud’s Phenomenon Calcium Channel Blocker
Beta Blockers, Ergot
Muscle Spasms Tizanidine, Cyclobenzaprine,
Magnesium
* FDA approved for migraine
45
Medication Overuse
• Starting a preventative medication while stopping the offending agent is
helpful
• When weaning off the offending agent a transient increase in headache
can occur lasting 2-10 days
• Consider short course of corticosteroids, NSAIDS, or dihydroergotamine
(unless these were the offending agent)
• Occipital blocks
(Sheeler et.al, 2016); Murinova & Karshin, 2015)
46
VITAL BEHAVIORS
Diagnosis Correctly
Treat Appropriately
Communicate Effectively
Headache Management
47
Education
• Headache calendar• Sleep hygiene techniques• Abstinence/limited alcohol use• Proper nutrition/limited caffeine/proper water consumption• Coping strategies/Journaling/Stress management• Limited use of abortive medication/avoid overuse headaches
• Realistic expectations (Sheeler et.al, 2016); Murinova & Karshin, 2015)
48

4/14/18
9
49 50
Additional Modalities
When medication is not working or not tolerated
51
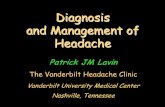
(Onabotulinumtoxin A “Botox”) Injection Paradigm
31 injections in to 7 muscle groups
Blumenfeld et. al, Headache 2010;50:1406-1418.
52
53
Occipital Nerve Anatomy
54

4/14/18
10
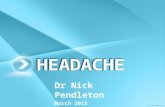
Occipital Block Injection Sites
GON aiming slightly up maintaining a subcutaneous courseLOC aiming lateral and up, maintaining a subcutaneous course
55
Transcutaneous Supraorbital Neurostimulation/ Cefaly
• FDA approved for prevention of migraine (March 2014)• Varying results- need to use it daily for 20 min• Currently not covered by Insurance
– Cost $349.00, pack of 3 electrodes $25.00 (good for 20 treatments each)
56
Cranial Electrotherapy StimulationAlpha-stim AID
• FDA approved for treatment of Anxiety, Depression, Insomnia
• No need to monitor labs/minimal side effects/no dependency
• Cost savings in reduction of other meds/treatments
57
Acupuncture
Qi, or energy, travels along 12 main pathways or meridians within the body
Health is influenced by the quality, quantity and balance of our Qi
Qi is profoundly disturbed by traumatic stress
• Cochrane systemic review 2016– Acupuncture should be
considered for migraine patients for prevention, particularly if having adverse effects from medications
– Acupuncture effect size was statically significantly larger in real acupuncture verses sham acupuncture for chronic headaches
– Acupuncture should be considered for treating episodic or chronic tension headaches (Coeytaux & Befus, 2016)
58
Auriculotherapy/Auricular Acupuncture
With permission from Terry Oleson, Ph.Dwww.auriculotherapy.org
59
Relaxation Techniques
60

4/14/18
11
Mobile Apps
• Breath2Relax
• Virtual Hope Box
• Mindfulness Coach
61
Mobile APPS
• http://t2health.dcoe.mil/products/mobile-apps
• http://t2health.dcoe.mil/sites/default/files/T2-TSWF-AIM-Client-Handout-Aug2016-web.pdf– Checklist for providers to recommend specific
apps or websites
62
Square Breathing
HOLD
HOLD
INHALE
EXHALE
1 2 3 4
1 2 3 4
1234
1234
KDW Health Management LLC 63
Peppermint oil
• Well tolerated- used for aromatherapy, topical use, enema• Helpful for:
– Tension headache– Irritable Bowel– Non-ulcer dyspepsia– Nausea– Relaxes smooth muscle/relieves colonic spasms with barium enemas
64
Peppermint oil
• When ingested side effects- allergic reactions, heartburn, perianal
burning, blurred vision, nausea/vomiting
• May inhibit cytochrome P450 1A2 system
• Contraindicated - Hiatal hernia, severe GERD, gallbladder d/o, caution with
pregnancy and breast feeding. (Has been used to trigger menstruation)
• Should not be used near the face of infants due to potential to cause
bronchspasms(Briggs, 2016); (Kliger & Chaudhary, 2007)
65
Lavender
• Thought to act on the limbic system, when inhaled, especially on the amygdala and hippocampus-
• Safety concerns- short term safe, need long term studies, some concern for gynecomastia when applied to skin. Some GI upset when ingested
• Do not ingest during pregnancy or breastfeeding
• Helpful for-– Anxiety – Depression– Insomnia
• No potential for drug abuse(Koulivand, Ghadiri & Gorji, 2013)
66

4/14/18
12
Empathetic Listening
• No one cares how much you know, untilthey know how much you care” – Theodore Roosevelt
67 68
Case Presentation
69
Headache Syndrome
Migraines + new onset headaches for 2 years
70
Background
• 44yr old female with a history of refractory headaches for the last 2 years
• Migraines since 1990’s- described as posterior pressure, treated with Advil. If untreated will cause photophobia/phonophobia & worse with exertion
• 2nd type started 2 years prior. Described as bi-frontal and right eye pressure increases to 4-6/10 and occasion to 8-9/10 w/photo/phonphobia
• Would occur upon waking up in the morning, worsen with exertion and when dehydrated. Lasting up to 2 weeks and occurring monthly
• Treated with zomig and advil- with about 1/3 resolved with this
• Treated in past by a neurologist- MRI of Brain WNL
71
Social & Medical History
• 44 yr old female/Married/Home-maker/ Graduated High School- some college
• No Tobacco/ Occasional ETOH/Occasional caffeine/Diet balanced/Elliptical 3 x’s per week
• Enjoys travel, reading and volunteering
• Migraines, Right shoulder arthritis, Cervical DDD, low back pain
• Hx of fall while skiing 2006 with tailbone fx, right shoulder injury and concussion
• Allergic to Sulfa
• Surgical- none
• Family hx- Migraines- Mother & Father
72

4/14/18
13
Significant Exam Findings
• Normal Neurologic exam
• Bil occipital tenderness
• Pulling sensation to right of C4 to C7 with rotation of head to left
• MRI of c/spine- DDD with disc protrusion
73
Treatment
• Topiramate titration/maintain zolmitriptan• Botox• Headaches improved at f/u but still with multiple headaches • Consult to neurosurgeon- stable- consult to PT • Occipital blocks & auricular acupuncture at f/u with dramatic reduction in
headaches• B/P elevated and switched Topiramate to Propranolol 80 LA• 2nd & 3rd rounds of Botox• Maintained on Propranolol 80LA• Continued control of headaches to one per month and occasional occipital
headache• Overjoyed at having this treated!
74
Summary
• Step 1- Diagnosis the headache or headaches- Tension and Migraine are the most common primary headaches
• Step 2- Accurate and through headache history
• Step 3- Physical exam/ rule out systemic illness
• Step 4- Identifying triggers and exacerbating factors
• Step 5- Action Plan- Acute , preventative, lifestyle modifications, education is a key component (Realistic Expectations)
75
VITAL BEHAVIORS
Diagnosis Correctly
Treat Appropriately
Communicate Effectively
Headache Management
76
Headache table
Migraine Tension-Type SAHLocation Unilateral Bilateral OccipitalIntensity Moderate to Severe Mild to Moderate Severe/”Worst HA
of life”Duration 4 to 72 hours 30 mins to 7 days Sudden/rapid onset
Sentinel HA may be seconds to minutes
Quality Pulsating Pressure/Tightening “Thunderclap”Associated Symptoms
Nausea, vomiting, photophobia, phonophobia
Photophobia or phonophobia ( but not both)
N/V, Photophobia, Neck stiffness, seizures, LOC, COMA
Female: Male ratio 3 : 1 1.3 : 1 Higher in females, African and Asian heritages
77
Headache tableMigraine Tension-Type CDH
Location Unilateral Bilateral Varies
Intensity Moderate to Severe Mild to Moderate Mild to severe
Duration 4 to 72 hours 30 mins to 7 days Minutes to hours. 15 or more headache days per month for 3 months or more
Quality Pulsating Pressure/Tightening Varies depending the type of primary headache
Associated Symptoms
Nausea, vomiting, photophobia, phonophobia
Photophobia or phonophobia ( but not both)
Look for medication over use, exacerbating factors
Female: Male ratio 3 : 1 1.3 : 1 No preference
78

4/14/18
14
Headache table
Migraine Tension-Type Occipital NeuralgiaLocation Unilateral Bilateral Occipital
Intensity Moderate to Severe Mild to Moderate Mild to severe
Duration 4 to 72 hours 30 mins to 7 days Minutes to hours
Pain transiently
relieved by occipital
block
Quality Pulsating Pressure/Tightening Sharp, throbbing,
pressure
Associated
Symptoms
Nausea, vomiting,
photophobia,
phonophobia
Photophobia or
phonophobia ( but
not both)
Pain behind the
eyes, nausea when
pain severe,
photophobia
Female: Male ratio 3 : 1 1.3 : 1 No preference, seen
often after
head/neck trauma
79 80
References
1. Becker, W. J. (2015). Acute migraine treatment in adults. Headache: The Journal of Head and Face Pain, 55(6), 778-793.
2. Briggs, P. (2016). Inhaled peppermint oil for postop nausea in patients undergoing cardiac surgery. Nursing, 46(7), 61-67.
3. Coeytaux, R. R., & Befus, D. (2016). Role of acupuncture in the treatment or prevention of migraine, tension-type headache, or chronic headache disorders. Headache: The Journal of Head and Face Pain, 56(7), 1238-1240.
4. Deen, M., Correnti, E., Kamm, K., Kelderman, T., Papetti, L., Rubio-Beltrán, E., … On behalf of the European Headache Federation School of Advanced Studies (EHF-SAS). (2017). Blocking CGRP in migraine patients – a review of pros and cons. The Journal of Headache and Pain, 18(1), 96.
81
5. De Luca GC, Bartleson JD. When and how to investigate the patient with headache. Semin Neurol. 2010; 30:131-144.
6. Goldberg LD. The cost of migraine and its treatment. AM J ManagCare 2005:11(2 suppl): 562-567.
7. Hay, D. L., & Walker, C. S. (2017). CGRP and its receptors. Headache: The Journal of Head and Face Pain, 57(4), 625-636.
8. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders:3rd
edition (beta version). Cephalagia 2013; 33(9): 629-808.9. Kligler, B., & Chaudhary, S. (2007). Peppermint oil. American Family
Physician, 75(7), 1027-1030.
References(continued)
82
References(continued)
10. Koulivand, P. H., Ghadiri, M. K., & Gorji, A. (2013). Lavender and the nervous system. Evidence-Based Complementary & Alternative Medicine (eCAM), 2013, 1-10.
11. Lipton RB, Bigal ME, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007; 68:343-349.
12. Marmura, M. J., Silberstein, S. D., & Schwedt, T. J. (2015). The acute treatment of migraine in adults: The american headache society evidence assessment of migraine pharmacotherapies. Headache: The Journal of Head and Face Pain, 55(1), 3-20.
13. Martin V, Elkind A. Diagnosis and classification of primary headache disorders. In: Standards of Care for Headache Diagnosis and Treatment. Chicago Ill: National headache Foundation 2004; 4-18.
83
References (continued)
14. Murinova, N., & Krashin, D. (2015). Chronic daily headache. Physical Medicine and Rehabilitation Clinics of North America, 26(2), 375-389.
15. Sheeler, R. D., Garza, I., Vargas, B. B., & O'Neil, A. E. (2016). Chronic daily headache: Ten steps for primary care providers to regain control.Headache: The Journal of Head and Face Pain, 56(10), 1675-1684.
16. Silberstein SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000; 55-754.
17. Stewart WF, et al. Lost Productive Time and Cost Due to Common Pain Conditions in the US Workforce. JAMA 2003; 290 2443-2454.
18. Stovner LJ, et al. The Global Burden of headache: A Documentation of Headache Prevalence and Disability Worldwide. Cephalgia 2007; 27:193-210.
84

4/14/18
15
References(continued)
19. Pringsheim, T., Davenport, W. J., Marmura, M. J., Schwedt, T. J., & Silberstein, S. (2016). How to apply the AHS evidence assessment of the acute treatment of migraine in adults to your patient with migraine. Headache: The Journal of Head and Face Pain, 56(7), 1194-1200.
20. The Cleveland Clinic Health Foundation. Overview of headache in adults. Cleveland Clinic Health Information Center website. Accessed Feb 12 2008.
85
Karen Williams, DNPc, RN, [email protected]
704-706-5519
86