Lipoid pneumonia presenting as non resolving community acquired ...
Case ReportGastrointestinal Involvement in Lipoid Proteinosis:A Ten-Year Follow-Up of a Brazilian Female Patient
Juliana Custódio Lima,1 Cristiane Kibune Nagasako,2
Ciro Garcia Montes,1 Irene Harumi Kamata Barcelos,3
Rita Barbosa de Carvalho,2 and Maria Aparecida Mesquita1
1 Gastroenterology Unit, Faculty of Medical Sciences, State University of Campinas (UNICAMP),13083-887 Campinas, SP, Brazil
2 Gastrocenter, State University of Campinas (UNICAMP), 13083-878 Campinas, SP, Brazil3 Department of Radiology, Faculty of Medical Sciences, State University of Campinas (UNICAMP),13083-887 Campinas, SP, Brazil
Correspondence should be addressed to Maria Aparecida Mesquita; [email protected]
Received 5 May 2014; Accepted 9 June 2014; Published 19 June 2014
Academic Editor: Jahn M. Nesland
Copyright © 2014 Juliana Custodio Lima et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Lipoid proteinosis is a rare autosomal recessive disease characterized by the deposition of hyaline material in the skin and internalorgans. The main clinical features are hoarseness and typical skin lesions. In this report we describe the endoscopic and radiologicfindings in a Brazilian female patient presenting extensive gastrointestinal involvement and the evolution of the detected lesions inten years of follow-up. Initial upper endoscopy and colonoscopy showed a similar pattern of multiple yellowish nodules throughoutthe esophagus, stomach, duodenum, and colons. Histological analysis confirmed the diagnosis of lipoid proteinosis. In addition,small bowel follow through demonstrated numerous well defined, round, small filling defects throughout the jejunum. Ten yearslater, the esophageal lesions remained the same, but none of the previous alterations were detected in the stomach, duodenum, andcolons. In conclusion, lipoid proteinosismay affect all gastrointestinal organswith the same pattern ofmacroscopic andmicroscopiclesions. Some lesions may regress with increasing age.
1. Background
Lipoid proteinosis (LP), also known as Urbach-Wiethe dis-ease or hyalinosis cutis et mucosae, is a rare autosomal-recessive disease, with less than 400 cases reported to date[1–3]. The disorder is characterized by hyaline deposits inthe skin, mouth, upper respiratory tract, and other viscera.The most common clinical features of LP are hoarseness,whichmay present in the first months of life, and skin lesions,characterized by skin infiltration and thickening, papules,chicken pox-like scars, and the presence of beaded papulesalong the eyelid [4].
Reports on gastrointestinal (GI) involvement in thiscondition are scarce. It appears that macroscopic lesions areunusual, although the histological analysis of visceral biopsiesand autopsy specimens has shown the typical hyaline deposits
in the esophagus, stomach, small bowel, and rectum [5]. Ear-lier reports on radiological studies, gastroscopic examination,and sigmoidoscopy in patients suffering from LP revealedno abnormality in the gastrointestinal tract [5, 6]. Morerecently, the involvement of the esophagus was documentedin one patient from Saudi Arabia, but the authors provided nodescription of the endoscopic findings [7]. So far the only GIcomplication of the disease was described in one patient withacute gastrointestinal bleeding secondary to deposits typicalof LP in the small bowel [8]. In all other cases patients had nogastrointestinal complaints.
In this report we describe the typical macroscopic andhistological characteristics of the lesions affecting the wholegastrointestinal tract in a Brazilian female patient with LP andthe evolution of the detected lesions over a ten-year period.
Hindawi Publishing CorporationCase Reports in MedicineVolume 2014, Article ID 952038, 4 pageshttp://dx.doi.org/10.1155/2014/952038
2 Case Reports in Medicine
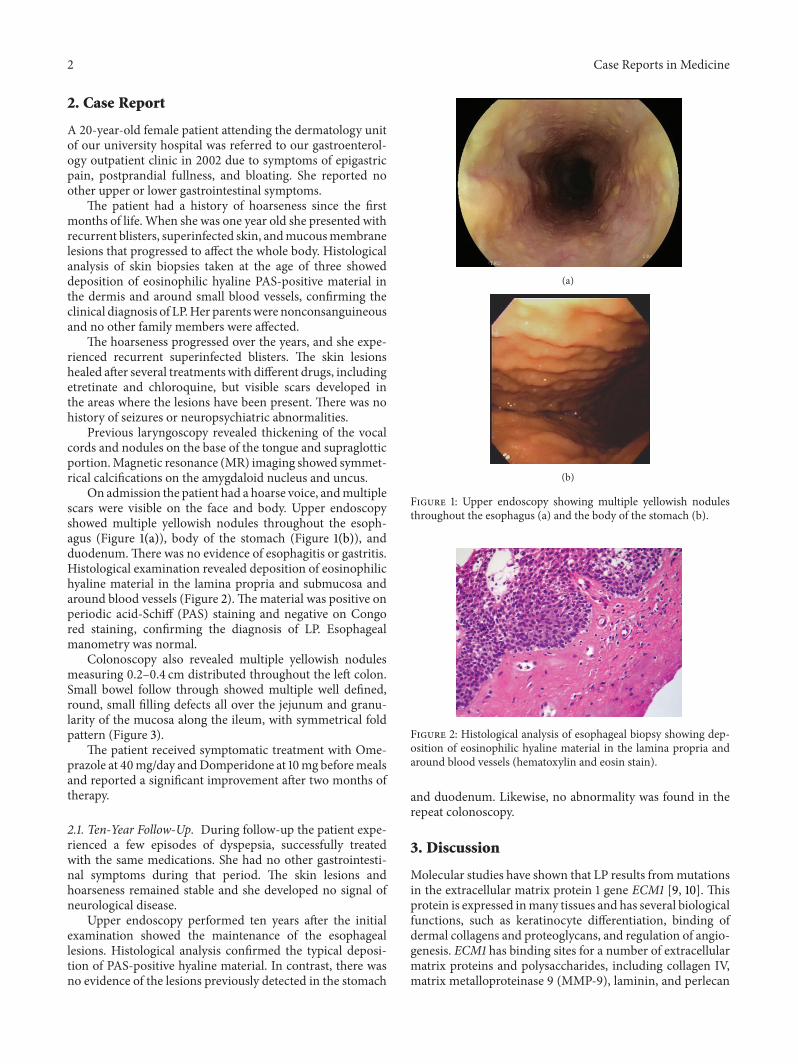
2. Case Report
A 20-year-old female patient attending the dermatology unitof our university hospital was referred to our gastroenterol-ogy outpatient clinic in 2002 due to symptoms of epigastricpain, postprandial fullness, and bloating. She reported noother upper or lower gastrointestinal symptoms.
The patient had a history of hoarseness since the firstmonths of life. When she was one year old she presented withrecurrent blisters, superinfected skin, andmucousmembranelesions that progressed to affect the whole body. Histologicalanalysis of skin biopsies taken at the age of three showeddeposition of eosinophilic hyaline PAS-positive material inthe dermis and around small blood vessels, confirming theclinical diagnosis of LP.Her parentswere nonconsanguineousand no other family members were affected.
The hoarseness progressed over the years, and she expe-rienced recurrent superinfected blisters. The skin lesionshealed after several treatments with different drugs, includingetretinate and chloroquine, but visible scars developed inthe areas where the lesions have been present. There was nohistory of seizures or neuropsychiatric abnormalities.
Previous laryngoscopy revealed thickening of the vocalcords and nodules on the base of the tongue and supraglotticportion.Magnetic resonance (MR) imaging showed symmet-rical calcifications on the amygdaloid nucleus and uncus.
On admission the patient had a hoarse voice, andmultiplescars were visible on the face and body. Upper endoscopyshowed multiple yellowish nodules throughout the esoph-agus (Figure 1(a)), body of the stomach (Figure 1(b)), andduodenum.There was no evidence of esophagitis or gastritis.Histological examination revealed deposition of eosinophilichyaline material in the lamina propria and submucosa andaround blood vessels (Figure 2).Thematerial was positive onperiodic acid-Schiff (PAS) staining and negative on Congored staining, confirming the diagnosis of LP. Esophagealmanometry was normal.
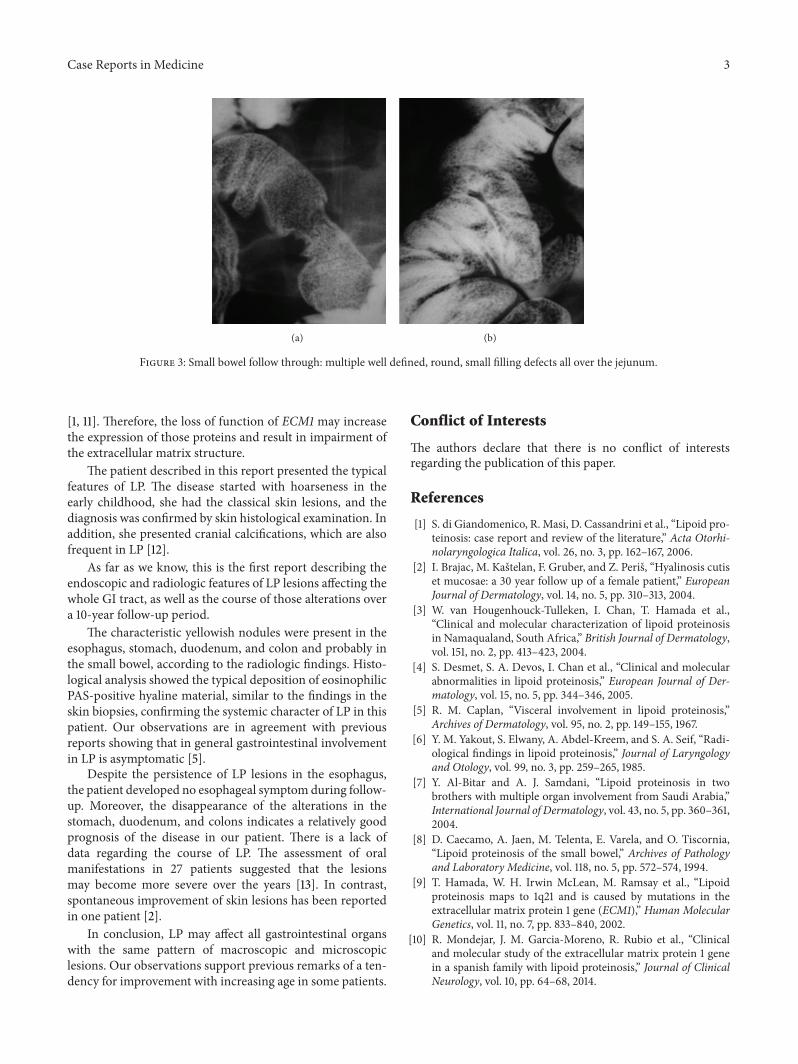
Colonoscopy also revealed multiple yellowish nodulesmeasuring 0.2–0.4 cm distributed throughout the left colon.Small bowel follow through showed multiple well defined,round, small filling defects all over the jejunum and granu-larity of the mucosa along the ileum, with symmetrical foldpattern (Figure 3).
The patient received symptomatic treatment with Ome-prazole at 40mg/day andDomperidone at 10mg beforemealsand reported a significant improvement after two months oftherapy.
2.1. Ten-Year Follow-Up. During follow-up the patient expe-rienced a few episodes of dyspepsia, successfully treatedwith the same medications. She had no other gastrointesti-nal symptoms during that period. The skin lesions andhoarseness remained stable and she developed no signal ofneurological disease.
Upper endoscopy performed ten years after the initialexamination showed the maintenance of the esophageallesions. Histological analysis confirmed the typical deposi-tion of PAS-positive hyaline material. In contrast, there wasno evidence of the lesions previously detected in the stomach
(a)
(b)
Figure 1: Upper endoscopy showing multiple yellowish nodulesthroughout the esophagus (a) and the body of the stomach (b).
Figure 2: Histological analysis of esophageal biopsy showing dep-osition of eosinophilic hyaline material in the lamina propria andaround blood vessels (hematoxylin and eosin stain).
and duodenum. Likewise, no abnormality was found in therepeat colonoscopy.
3. Discussion
Molecular studies have shown that LP results frommutationsin the extracellular matrix protein 1 gene ECM1 [9, 10]. Thisprotein is expressed inmany tissues and has several biologicalfunctions, such as keratinocyte differentiation, binding ofdermal collagens and proteoglycans, and regulation of angio-genesis. ECM1 has binding sites for a number of extracellularmatrix proteins and polysaccharides, including collagen IV,matrix metalloproteinase 9 (MMP-9), laminin, and perlecan
Case Reports in Medicine 3
(a) (b)
Figure 3: Small bowel follow through: multiple well defined, round, small filling defects all over the jejunum.
[1, 11]. Therefore, the loss of function of ECM1 may increasethe expression of those proteins and result in impairment ofthe extracellular matrix structure.
The patient described in this report presented the typicalfeatures of LP. The disease started with hoarseness in theearly childhood, she had the classical skin lesions, and thediagnosis was confirmed by skin histological examination. Inaddition, she presented cranial calcifications, which are alsofrequent in LP [12].
As far as we know, this is the first report describing theendoscopic and radiologic features of LP lesions affecting thewhole GI tract, as well as the course of those alterations overa 10-year follow-up period.
The characteristic yellowish nodules were present in theesophagus, stomach, duodenum, and colon and probably inthe small bowel, according to the radiologic findings. Histo-logical analysis showed the typical deposition of eosinophilicPAS-positive hyaline material, similar to the findings in theskin biopsies, confirming the systemic character of LP in thispatient. Our observations are in agreement with previousreports showing that in general gastrointestinal involvementin LP is asymptomatic [5].
Despite the persistence of LP lesions in the esophagus,the patient developed no esophageal symptom during follow-up. Moreover, the disappearance of the alterations in thestomach, duodenum, and colons indicates a relatively goodprognosis of the disease in our patient. There is a lack ofdata regarding the course of LP. The assessment of oralmanifestations in 27 patients suggested that the lesionsmay become more severe over the years [13]. In contrast,spontaneous improvement of skin lesions has been reportedin one patient [2].
In conclusion, LP may affect all gastrointestinal organswith the same pattern of macroscopic and microscopiclesions. Our observations support previous remarks of a ten-dency for improvement with increasing age in some patients.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] S. di Giandomenico, R. Masi, D. Cassandrini et al., “Lipoid pro-teinosis: case report and review of the literature,” Acta Otorhi-nolaryngologica Italica, vol. 26, no. 3, pp. 162–167, 2006.
[2] I. Brajac, M. Kastelan, F. Gruber, and Z. Peris, “Hyalinosis cutiset mucosae: a 30 year follow up of a female patient,” EuropeanJournal of Dermatology, vol. 14, no. 5, pp. 310–313, 2004.
[3] W. van Hougenhouck-Tulleken, I. Chan, T. Hamada et al.,“Clinical and molecular characterization of lipoid proteinosisin Namaqualand, South Africa,” British Journal of Dermatology,vol. 151, no. 2, pp. 413–423, 2004.
[4] S. Desmet, S. A. Devos, I. Chan et al., “Clinical and molecularabnormalities in lipoid proteinosis,” European Journal of Der-matology, vol. 15, no. 5, pp. 344–346, 2005.
[5] R. M. Caplan, “Visceral involvement in lipoid proteinosis,”Archives of Dermatology, vol. 95, no. 2, pp. 149–155, 1967.
[6] Y. M. Yakout, S. Elwany, A. Abdel-Kreem, and S. A. Seif, “Radi-ological findings in lipoid proteinosis,” Journal of Laryngologyand Otology, vol. 99, no. 3, pp. 259–265, 1985.
[7] Y. Al-Bitar and A. J. Samdani, “Lipoid proteinosis in twobrothers with multiple organ involvement from Saudi Arabia,”International Journal of Dermatology, vol. 43, no. 5, pp. 360–361,2004.
[8] D. Caecamo, A. Jaen, M. Telenta, E. Varela, and O. Tiscornia,“Lipoid proteinosis of the small bowel,” Archives of Pathologyand Laboratory Medicine, vol. 118, no. 5, pp. 572–574, 1994.
[9] T. Hamada, W. H. Irwin McLean, M. Ramsay et al., “Lipoidproteinosis maps to 1q21 and is caused by mutations in theextracellular matrix protein 1 gene (ECM1),” Human MolecularGenetics, vol. 11, no. 7, pp. 833–840, 2002.
[10] R. Mondejar, J. M. Garcia-Moreno, R. Rubio et al., “Clinicaland molecular study of the extracellular matrix protein 1 genein a spanish family with lipoid proteinosis,” Journal of ClinicalNeurology, vol. 10, pp. 64–68, 2014.

4 Case Reports in Medicine
[11] S. Sercu,M. Zhang,N.Oyama et al., “Interaction of extracellularmatrix protein 1 with extracellular matrix components: ECM1is a basement membrane protein of the skin,” Journal ofInvestigative Dermatology, vol. 128, no. 6, pp. 1397–1408, 2008.
[12] H. B. Thornton, D. Nel, D. Thornton, J. van Honk, G. A. Baker,and D. J. Stein, “The neuropsychiatry and neuropsychologyof lipoid proteinosis,” Journal of Neuropsychiatry and ClinicalNeurosciences, vol. 20, no. 1, pp. 86–92, 2008.
[13] P. A. Hofer and A. Bergenholtz, “Oral manifestations inUrbach—Wiethe disease (lipoglycoproteinosis; lipoid pro-teinosis; hyalinosis cutis et mucosae),” Odontologisk Revy, vol.26, no. 1, pp. 39–57, 1975.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com