Case Presentation Kriska Shalin Lara Joaquin Abdominal pain.
55
Case Presentation Kriska Shalin Lara Joaquin Abdominal pain
-
Upload
thomasina-harrington -
Category
Documents
-
view
223 -
download
0
Transcript of Case Presentation Kriska Shalin Lara Joaquin Abdominal pain.

Case PresentationKriska Shalin Lara Joaquin
Abdominal pain

To present the history and physical examination of a pediatric patient presenting with abdominal pain
To discuss the approach and management to a pediatric patient presenting with abdominal pain
To highlight differences in approach and management in pediatric and adult patients
To review basic anatomy and pathophysiology relevant for this case
Objectives

Patient data• CV• 16/M• Single• Filipino• Roman Catholic• College student• 4/12/1995• Makati City

Chief complaint
Abdominal pain, 17 hours

History of Present Illness
(+) epigastric pain 6/10
Diffuse
(-) fever
17 hours PTC
(+) loss of appetite
Last meal: >20h PTC

7 hours PTC (+) migration of pain to
RLQ 10/10, sharp, localized
(-) fever
(+) vomiting
Consult at ER
History of Present Illness

Past Medical history
• No prior surgeries• Past hospitalization. 2010- Dengue fever
(-) Asthma, (-) congenital diseases• Born FT via NSD in a hospital, developmentally at par
with age• Patient claims to have complete immunizations from
health center • No known allergies to food and drug

Family history
• (+) asthma
• (+) HTN
• (+) DM
• (-) allergies

Personal & Social history
• Denies smoking and illicit drug use• Occasional alcohol use• Lives in a well-ventilated house in Makati City• Potable water source• Garbage collected regularly• 1st year college student

HEADSSS
• Comfortable at home• 1st year college• Involved in sports, watches TV, computer games• Denies use of any drugs• Denies involvement in sexual activities, heterosexual, does
not have a girlfriend• Safety – no high risk activities, does not drive• Attends mass every now and then

Review of Systems
• No weight loss• No rash• No cough/colds• No difficulty of breathing• No palpitations• No diarrhea, no constipation• No frequency, no dysuria, no penile discharge

Physical examination

Vital signs
• BP 120/70
• HR 92
• RR 16
• T 38 C
• VAS 9/10
• BMI 22.5

General
• Ambulatory, walking limited by pain• Refused to jump
• Awake, coherent, not in cardiorespiratory distress

Skin
• Not flushed
• Warm to touch
• No active lesions or discolorations

Head and neck
• Normocephalic head• Anicteric sclerae, pink palpebral conjunctiva• Ears symmetric, no discharge• No nasal discharge• No tonsillopharyngeal congestion• No nasal discharge• No CLAD

Chest and Lungs
• Equal chest expansion
• Resonant on all lung fields
• Clear breath sounds
• No rales/wheezes

Heart
• Adynamic precordium
• PMI at 5th ICS along MCL
• Good S1 and S2
• Normal rate, Regular rhythm
• No murmurs

Abdomen
• Flabby, no visible lesions• normoactive bowel sounds, tympanitic on all
quadrants• Soft, (+) direct and indirect tenderness with guarding
at RLQ(-) Obturator sign(-) Psoas sign(-) Rovsing's sign

Extremities
• MMT: 5/5 upper and lower left and right
• Sensory: 100% bilaterally
• Full ROM, active and passive

Acute appendicitisPrimary
Impression

RULE IN: RULE OUT:
Acute mesenteric adenitis
Common in pedia, abdominal pain
Usually preceded with feverm cough/colds, generalized
lymphadenopathy, pain not localized
No signs of perotinitis
Acute gastroenteritisVomiting, abdominal
pain, fever
Hyperactive bowel sounds, diarrhea
No signs of perotinitis
UTIMay present with abdominal pain,
fever
Frequency, dysuria, hematuria, usually no signs of
perotinitis

Ureteral stone
Costovertebral tenderness, urinary
symptoms, usully sharp colicky pain
Meckels diverticulitisMay present as
appendicitisIncidence is low
RULE IN:Present in patient
RULE OUT:Absent in this case

Discussion

Anatomy
• Landmarks• Size of Appendix:
>1 cm - 30 cm,Ave: 6-9 cm
• Appendiceal artery
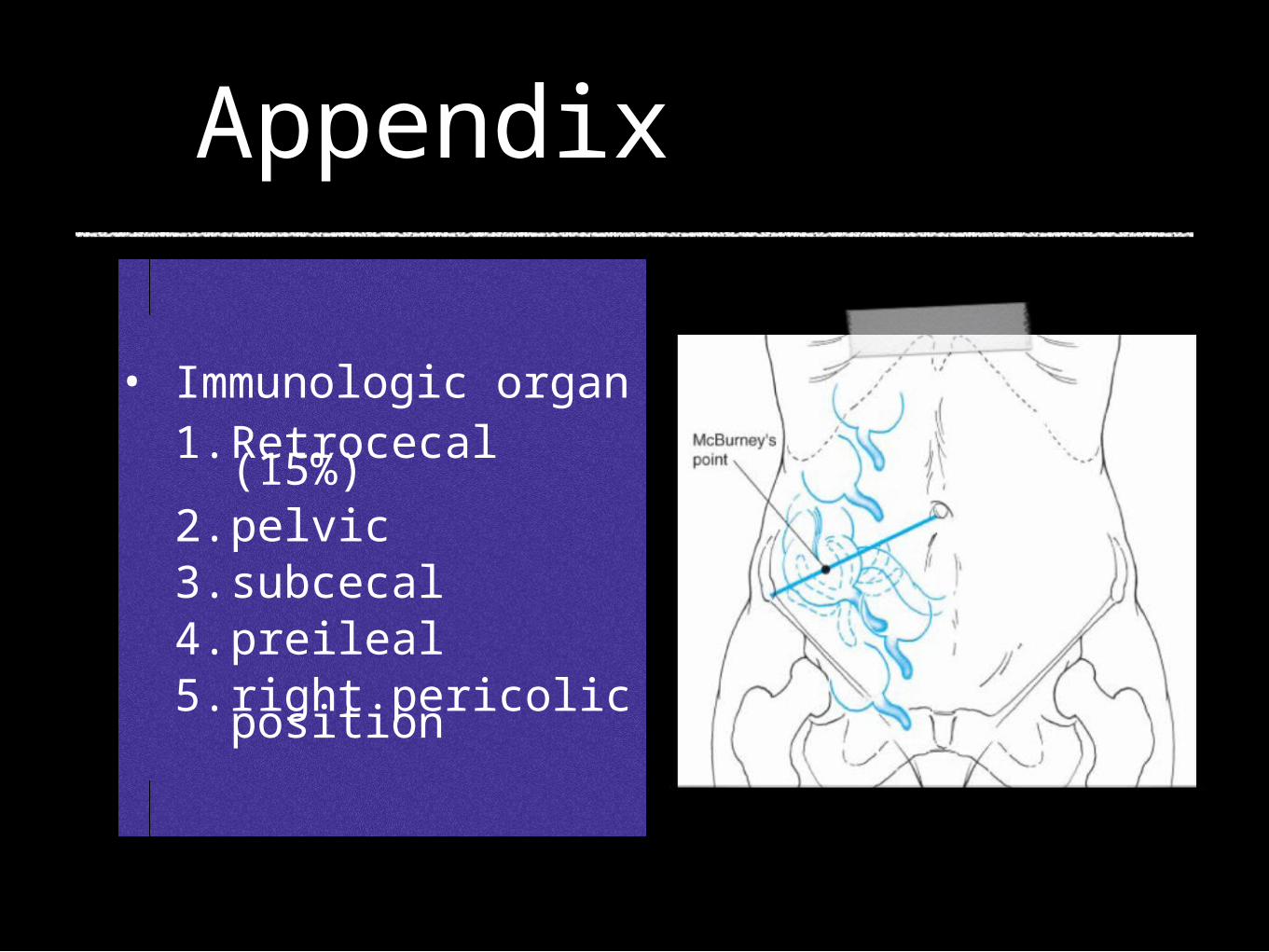
Appendix
• Immunologic organ1. Retrocecal (15%)2. pelvic3. subcecal4. preileal5. right pericolic position

Uncomplicated Appendicitis the acutely inflamed, phlegmonous, suppurative, or mildly inflamed appendix with or without peritonitis Complicated Appendicitis gangrenous appendicitis, perforated appendicitis, localized purulent collection at operation, generalized peritonitis and periappendiceal abscess
DefinitionsEVIDENCE-BASED CLINICAL PRACTICE GUIDELINES ON THE DIAGNOSIS AND TREATMENT OF ACUTE APPENDICITIS Philippine College of Surgeons 2002

Equivocal Appendicitis • a patient with right lower quadrant abdominal
pain who presents with an atypical history and physical examination and the surgeon cannot decide whether to discharge or to operate on the patient
DefinitionsEVIDENCE-BASED CLINICAL PRACTICE GUIDELINES ON THE DIAGNOSIS AND TREATMENT OF ACUTE APPENDICITIS Philippine College of Surgeons 2002

Incidence
• In pedia: more common 4-15 yo
• Lifetime risk 7% (Irvin, 1989)
• Lifetime rate of appendectomy:
• 12% men
• 25% women
• 20s-40s, mean 31, median 22 yo
• Misdiagnosis and negative appendectomy is higher in females

Organisms
• Escherichia coli
• Bacteroides fragilis

Schwartz 8th ed

Pathophysiology
Obstuction of lumen
Secretions
Dull diffuse pain
Distention
Bacteria
Marked distention
Reflex nausea/vomiting
Exceeds venous pressureOccluded
cap/veinsInflammation:Serosa and
parietalPeritoneum
RLQ pain
Manifestation

• In more than 95% of patients with acute appendicitis: anorexia, abdominal pain, vomiting
anorexia – almost always
abdominal pain – most common complaint
vomiting – 75%

McBurney's point
Rovsing's sign
Psoas sign
Obturator sign
REVIEW

TRUE or FALSE
• Most common site of rupture is at the tip

Rupture
• Distal to the point of luminal obstruction along the antimesenteric border of the appendix
• overall rate of perforated appendicitis is 25.8% (Schwartz)17-48% (JAMAevidence 2010)
• Happens 36-48 h after onset of symptoms• Children <5 and > 65 years have the highest rate of
perforation (45 and 51%, respectively) • in elderly as high as 60-70% (JAMAevidence)
Suspect in:
> 39 deg
> 18000 WBC

Misdiagnosis
• Higher in females (45%)
• accounting for more than 75% of misdiagnosis are:
1. acute mesenteric lymphadenitis
2. no organic pathologic conditions
3. acute pelvic inflammatory disease
4. twisted ovarian cyst or ruptured graafian follicle
5. acute gastroenteritis.

Alvarado scoring Pre-test probabilities Diagnostic modalities
Diagnostics

Alvarado scoring:MANTRELS
Symptoms M- Migration of pain 1
A- Anorexia 1
N- Nausea/vomiting 1
Signs T- Tenderness, RLQ 2
R- Rebound tenderness
1
E- Elevated temp 1
Labs L- Leukocytosis 2
S- Shift to the left 1

Pre-test probabilities
Clinical Likelihood ratio
RLQ pain 8.0
Rigidity 4.0
Migration of pain 3.2
Rebound tenderness 1.1 to 6.3
Evidence-based Rational Clinical Examination. JAMAEvidence 2010

Atypical features in children
Atypical features of pediatric appedicitis. Acad Emerg Med. 2007 Feb;14(2):124-9. Epub 2006 Dec 27.

TRUE or FALSE
CT scan is preferred because it is more superior to Ultrasound
Ultrasound should be requested for all pediatric patients

Diagnostics
• CBC• Leukocytosis: 10,000 to 18,000/mm3
• Urinalysis• Graded compression sonography
• Non-compressible 6 mm and apendicolith• presence of thickening of the appendiceal wall and
periappendiceal fluid - highly suggestive

• CT scan
• 5 mm or greater, Thickened wall
• Fecaliths - not pathognomonic
• Target sign/ Arrowhead sign - thickening of the cecum, which funnels contrast toward the orifice of the inflamed appendix
Diagnostics

• Ultrasound preferred in pedia
• CT scan preferred over ultrasonography in clinically equivocal appendicitis in adults because of its superior accuracy (PCS 2002)
• Laparoscopy - both diagnostic and therapeutic, more beneficial in women

Therapeutics
• Appendectomy is the appropriate treatment for acute appendicitis.
• Open vs Lap: equally effective but...
• Incisions:
• Mc Burney
• Rocky davis

UNCOMPLICATED:
•Cefoxitin 2 grams IV single dose (Adults) 40 mg/kg IV single dose (Children)
Alternative agents:
• Ampicillin-sulbactam 1.5-3 grams IV single dose (Adults) 75 mg/kg IV single dose (Children)
• Amoxicillin-clavulanate 1.2 –2.4 grams IV single dose (Adults) 45 mg/kg IV single dose (Children)
EVIDENCE-BASED CLINICAL PRACTICE GUIDELINES ON THE DIAGNOSIS AND TREATMENT OF ACUTE APPENDICITIS Philippine College of Surgeons 2002

• Ticarcillin-clavulanic acid 75 mg/kg IV every 6 hours
• Alternative: Imipenem-Cilastatin 15-25 mg/kg IV every 6 hours
For children with beta-lactam allergy
Gentamicin 5 mg/kg IV every 24 hours plus Clindamycin 7.5 –10 mg/kg IV every 6 hours
COMPLICATED (PEDIA)

Principles of Pediatric Surgery. O’Neill JJr et. al 2003
COMPLICATED:
• Cefotetan
• Triple: Ampicillin, Gentamicin, Clindamycin or Metronidazole

• Ertapenem 1 gram IV every 24 hours
• Tazobactam-piperacillin 3.375 grams IV every 6 hours or 4.5 grams IV every 8 hours
For adults with beta-lactam allergy: Ciprofloxacin 400 mg IV every 12
COMPLICATED (ADULTS)

Duration of antibiotics
• non-perforated appendicitis: 24 to 48 hours
• perforated appendicitis: 7 to 10 days (Schwartz)
• 1 – 2 weeks
• clinician’s assessment after the operation: 5-7 days of antibiotics and Sequential therapy to oral antibiotics Discontinuation of antibiotics
• absence of fever for 24 hours (temperature < 38 C)
• the ability to tolerate oral intake
• normal WBC count with 3 per cent or less band forms

Antibiotics and appendicitis in the pediatric population: an American Pediatric Surgical Association Outcomes and Clinical Trials Committee Systematic Review
Journal of Pediatric Surgery (2010) 45, 2181–2185
1. broad-spectrum antibiotics for nonperforated2. Broad-spectrum, single, or double agent therapy is as
effective as and more cost-effective for perforated3. duration of administration of broad-spectrum IV
antibiotics based on clinical criteria: fever, pain, return of bowel function, and WBC count
4. perforated appendicitis: 5-day IV antibiotics but completing the antibiotic course with oral antibiotics (total 7 days IV + oral) had similar results

Ruptured
• Antibiotics
• Drainage of abscess, CT-guided
• Interval appendectomy performed 6-8 weeks following the acute event

ENDKriska Shalin L. Joaquin

Principles of Pediatric Surgery 2nd ed
Schwartz's Principles of Surgery 8th ed
EVIDENCE-BASED CLINICAL PRACTICE GUIDELINES ON THE DIAGNOSIS AND TREATMENT OF ACUTE APPENDICITIS Philippine College of Surgeons 2002
Evidence-based Rational Clinical Examination. JAMAEvidence 2010
Pediatric appendicitis: pathophysiology and appropriate use of diagnostic imaging. Brennan, C. CJEM 2006;8(6):425-432
Antibiotics and appendicitis in the pediatric population: an American Pediatric Surgical Association Outcomes and Clinical Trials Committee Systematic Review Journal of Pediatric Surgery (2010) 45, 2181–2185
Reference
s