Case Pres1
32
CASE PRESENTATION East Aven ue Med ical Center Female Surgical Ward Group D
-
Upload
kyle-tampoya -
Category
Documents
-
view
231 -
download
0
Transcript of Case Pres1

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 1/32
CASE PRESENTATION
East Avenue Medical Center
Female Surgical WardGroup D

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 2/32

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 3/32
Background of the case:Upper Gastrointestinal
bleeding refers to
hemorrhage in the upper
gastrointestinal tract. Theanatomic cut-off for
upper GI bleeding is the
ligament of Treitz, which
connects the fourthportion of the duodenum
to the diaphragm near the
splenic flexure of the
colon.

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 4/32

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 5/32
FAMILY HISTORY
Ô Father had a stroke.
Ô Patients paternal uncle was operated in the
esophagus of unknown reason and that currently
patient had no voice.
Ô No known heredo-familial diseases such as BA,
PTB, DM, or Cancer.

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 6/32
OB HISTORY
Ô G2P2 (2002)
Ô Menarche at 12 years old
Ô Consuming 2 pads a day
Ô Menstruation last from 5-6 days duration
Ô Regular monthly interval

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 7/32
DIETARY HISTORY
Ô Patient not taking any vitamins as Vit C
Ô fond of salted foods
Ô fond of smoked foods
Ô fond of canned foods
Ô (+) smoker
Ô (+) alcohol drinker

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 8/32
PAST MEDICAL HISTORY
Ô As above, not known to have DM, BA, PTB,
HPN, or Cancer.
Ô No previous hospitalization, surgeries, or
allergies to foods and medications.

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 9/32
HISTORY OF PRESENT ILLNESS
Ô 5 months PTA ² patient had epigastric pain radiating to
the back, relieved by food but eventually recurs 2-3 hours
after associated with early satiety, greenish LBM of 4
episodes a day approximately ½ cup per episode that
lasted for 3 days. Patient self-medicated with
Loperamide to relief self of LBM. Patient also noted
gradual weight loss approximately 40%. Consult done at
Health Center and was prescribed with antacid takenTID for 2 weeks with relief of symptoms.
8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 10/32
Ô 1 ½ month PTA ² Patient started to have 4-5 times
vomiting usually occuring in the late afternoon with
persistent epigastric pain and heartburn.
Ô 5 weeks PTA ² With persistence of symptoms, patient
consulted to a private MD and was told that she has
gastritis. Given Xeloid Gel, TID, Gasmed tab TID and
Omeprazole 20mg OD with relief. But 1 week later, the
symptoms recurred after the patient completed her
medications.

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 11/32
Ô 2 weeks PTA ² Patient consulted at TALA Hospital and
was prescribed with Omeprazole OD, Maalox 1tbsp QID
and Ofloxacin 200mg BID for 1 week for her UTI.
Ô 3 days PTA ² Patient had coffee ground post prandial
vomiting occuring 5 times a day with anorexia, epigastric
pain but no melena. Self treated with Maalox 1tbsp OD
and Omeprazole 20mg OD. Persistence prompted
consult hence admission.
8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 12/32

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 13/32
Ô Blood Pressure: 90/60 mmHg
Ô Cardiac Rate: 90 bpm
Ô Respiratory Rate: 22 cpm
Ô Temperature: 37.1°c
Ô Height: 1.55m
Ô Weight: 45 kg
Ô BMI: 18.75 kg/m2

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 14/32
HEENT:
Ô Pale palpebral conjunctiva
Ô Anicteric sclera
Ô No nasoaural discharge
Ô No tonsillopharyngeal congestion
Ô Noted eyes to be slightly protruded
Ô (+) Coffee Ground output per NGT

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 15/32
NECK:
Ô Supple
Ô No neck vein engorgement
Ô No palpable lymphadenopathies
Ô (-) supraclavicular
Ô Lymphadenopathy

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 16/32
HEART:
Ô Adynamicprecordium
Ô Apex beat at 5th ICS MCL
Ô Regular heart rate
Ô No murmur

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 17/32
ABDOMEN:
Ô Flat and soft
Ô (+) ovoid fixed non mobile smooth mass atepigastric area with tenderness
Ô Normoactive bowel sound

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 18/32
EXTREMITY:
ÔNo gross deformity
ÔFull and equal pulses
ÔNo edema
Ô Pale nail beds

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 19/32
DRE:
Ô (+) skin tag at anus
Ô Good sphincter tone
Ô Empty rectal vault
Ô Smooth wall with no mass
Ô Noted dark brown stool per examining finger
8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 20/32
ROS:
Ô (-) orthopnea
Ô (-) easy fatigability
Ô (-) palpitations
Ô (-) PNO
Ô (-) chest pain
Ô (-) chest discomforts
Ô (-) diarrhea
Ô (-) constipation

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 21/32
Assessment: Upper Gastrointestinal Bleeding
probably secondary to:
1. BPUD
2. Bleeding Gastric mass

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 22/32
8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 23/32
CYTOLOGY REPORT
DIAGNOSIS:
Gastric mucosa, biopsy:
Ô Gastric Adenocarcinoma
Ô Poorly differentiated with signet ring features
Ô Negative for Helicobacter pylori
8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 24/32
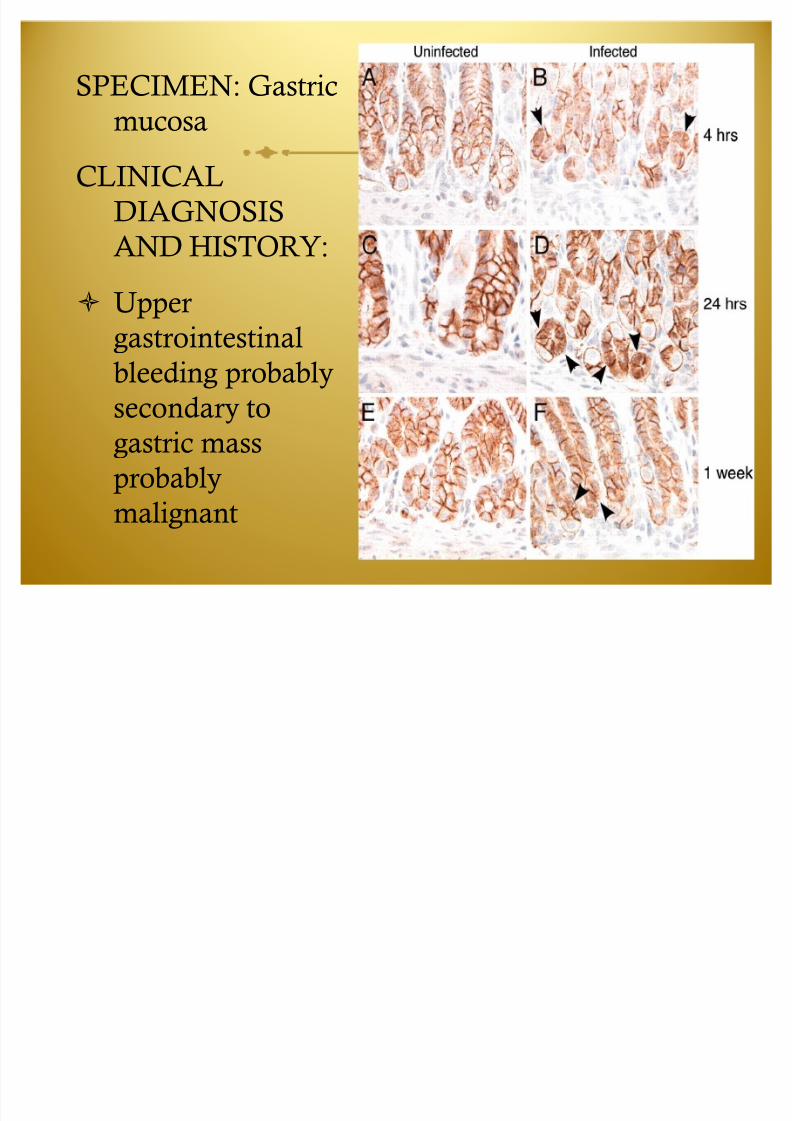
SPECIMEN: Gastric
mucosa
CLINICAL
DIAGNOSIS
AND HISTORY:
Ô Upper
gastrointestinal
bleeding probably
secondary togastric mass
probably
malignant

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 25/32
GROSS AND MICROSCOPIC
DESCRIPTION:
Ô Rectered specimen labeled ́ gastric
mucosaµ consist of 8 cream-white-
black, irregular, soft tissue
fragments.
Ô Sections show gastric tissues with
involvement of a neoplasm seen in
sheets.
Ô No Helicobacter pylori organisms
are evident on Giemsa stain.

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 26/32
GASTRIC ADENOCARCINOMA
Ô It is also called malignant tumor of the stomach.
Ô Risk factors include: chron

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 27/32
LABORATORY RESULTS
HEMATOLOGY
COMPONENTS R ESULT NOR MAL
VALUES
SI UNITS
Hemoglobin 70 120-140 for female
adults
gm/L
Hematocrit 0.210 0.38-0.48 for
female adults
gm/L

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 28/32
ANATOMY AND PHYSIOLOGY

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 29/32

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 30/32
PATHOPHYSIOLOGY

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 31/32
DRUG STUDY
ÔAminoleban 500cc
ÔOmeprazole 40mgÔFerrous Sulfate (TID) P.O

8/8/2019 Case Pres1
http://slidepdf.com/reader/full/case-pres1 32/32
Nursing Care Plan