Case Bersama - TTH Edit
35
Presented by : NATASHA ASTAR Pembimbing: Prof. Dr. H. Basjiruddin A, Sp. S (K)
-
Upload
natasha-astar -
Category
Documents
-
view
218 -
download
0
Transcript of Case Bersama - TTH Edit

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 1/35
Presented by :
NATASHA ASTAR
Pembimbing:
Prof. Dr. H. Basjiruddin A, Sp. S (K)

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 2/35
A 56 years old male presented with right upperand lower limb weakness since 4 days beforeadmitted to hospital,
•Right upper and lower limb
weakness
Chief Complaint

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 3/35
•
Right upper and lower limb weakness since 4 daysbefore admitted to Dr M Djamil Hospital. Earlier
patient were brought to a general practitioner and
then were admitted to Sijunjung Hospital for 2
days and then were refered here from SijunjungHospital. Weakness are seen suddenly during
activity (lifting farming items), and fall. Conscious
after attack. The upper and lower limb weakness
are equal. Now patient are unable to lift anything
and have to be hold by family to walk. He also
have difficulty in eating and drinking.
Current Illness History

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 4/35
This complain are accompanied with wrymouth and patient cannot speak. Patientcannot understand conversation and cannotsay any words.
No complain of headache, vomiting,decreased consciousness, and seizures.
No complain in sensing, miction and
defecation

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 5/35
• Known hypertensive since 3 years ago. No regular
checkup to doctor.•No previous history of stroke.
•No history of diabetes.
Past Illness History
•No family history of hypertension, diabetes, heart
disease and stroke.
Family History of Illness
• Patient is a farmer, smoke 12 stick of cigarette a
day since 30 years ago.
Socioeconomic Background

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 6/35
•General Appearance: Moderately Ill
•Level of Consciousness: compos mentiscooperative
•Pulse : 72 x/menit
•Respiratory Rate : 20 x/menit
•Blood Pressure : 180/120 mmHg
•Temperature : 36,7oC
General

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 7/35
GCS 15 : E4 M6 Aphasia

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 8/35
•Neck stiffness: (-) Brudzinsky II : (-)
•Brudzinsky I : (-) Kernig Sign : (-)
Meningeal SIgn
•Vomiting (-)
•Progressive headache (-)
Intracranial Pressure Examination

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 9/35
N. I : Difficult to evaluate N. II : Difficult to evaluate
N. III, IV, VI : Light reflex +/+
Doll eye movement N. V : difficult to evaluate
N. VII : Right Nasolabial plica flatter
than the left side, EyelashesReflex +/+
N VIII : difficult to evaluate

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 10/35
N IX : Vomitting Reflex +, capableto swallow
N X : Pharinx arch symmetric, Uvulaon the midline
N XI : difficult to evaluate
N XII difficult to evaluate

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 11/35
Motor Function Test Upper Limb Right
Left Movement Limited
active Strength 0/0/0
5/5/5 Tonus eutonus
eutonus Trophy eutrophy
eutrophy Fall Test Right side
lateralisation

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 12/35
Lower Limb Right Left
Movement Limited active Strength 0/0/0 5/5/5
Tonus eutonus eutonus
Trophy eutrophy eutrophy Fall test Right side lateralisation

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 13/35
Sensibility Test Pain Sensibility +, Tactil Sensibility +.

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 14/35
•
Mixturition : neurogenic bladder (-)•Defecation : normal
• Sweat secretion : normal
Autonomous Nervous System

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 15/35
Reflex Right Left
Biceps +++ ++
Triceps +++ ++APR +++ ++
KPR +++ ++

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 16/35
8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 17/35
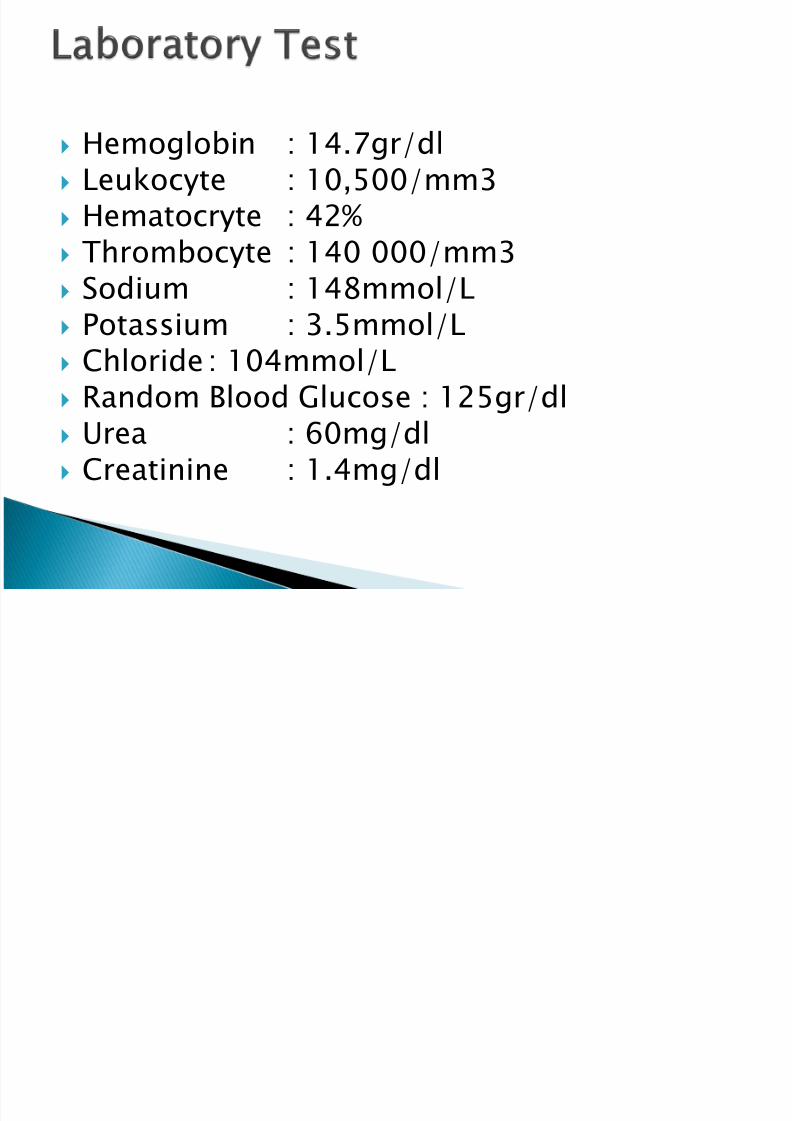
Hemoglobin : 14.7gr/dl Leukocyte : 10,500/mm3 Hematocryte : 42% Thrombocyte : 140 000/mm3 Sodium : 148mmol/L Potassium : 3.5mmol/L Chloride : 104mmol/L Random Blood Glucose : 125gr/dl Urea : 60mg/dl Creatinine : 1.4mg/dl

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 18/35

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 19/35
EKG : Atrial Fibrilation Normoventricular
response

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 20/35
Clinical Diagnosis Right Hemiparesis+RightNVII and NXII Paresiscentral type +Globalaphasia
Topic Diagnosis Right brain hemisphere,
Subcortical
Etiology Diagnosis Cerebral Thromboemboli
Secondary Diagnosis Emergency Hypertension,Atrial Fibrillation Normoventricular Response

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 21/35
•Right Hemiparesis+Right NVII and NXII Paresis
central type +Global aphasia
Clinical Diagnosis
•Right brain hemisphere, Subcortical
Topic Diagnosis
•Cardiooemboli
Etiology
•Emergency Hypertension, Atrial Fibrillation
•Normoventricular Response
Secondary Diagnosis

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 22/35
•Head elevation 30degree
•Oxygen 2L/minute
•IVFD RL 12hour/kolf
•
Catheter (fluid balance)•Diet Soft Food, Low Sodium II
Supportive

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 23/35
•Piracetam 4x3gr (IV)
•Bisoporolol 1x2.5mg (Oral)
•Aspilet 2x 80mg
•Herbesser Drip 50mg in 50cc Ringer
lactate via syringe pump 50cc/hour
Medicinal Therapy

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 24/35
Dietary control Physical Therapy
Family education and prevention onhypertension and stroke
Medicinal Therapy

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 25/35
A 26 years old male visited NeurologyAmbulatory Service with pain in the head anddiagnosed Frequent episodic tension typeheadache associated with pericarnial
tenderness.
Diagnosed made by anamnesis and physical
examination that associated with AmericanHeadache Society diagnostic criteria.

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 26/35

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 27/35

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 28/35

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 29/35

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 30/35
The exact cause or causes of tension
headache are unknown.
Experts used to think that the pain of tensionheadache stemmed from muscle contractionin the face, neck and scalp, perhaps as aresult of heightened emotions, tension orstress.
But research suggests that there doesn'tappear to be a significant increase in muscletension in people diagnosed with tensionheadache.

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 31/35
The most common theories support
interference or "mixed signals" involvingnerve pathways to the brain, which isdemonstrated by a heightened sensitivity topain in people who have tension headaches.
Increased muscle tenderness, a commonsymptom of tension headache, may be theresult of overactive pain receptors.

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 32/35
It's likely other factors also contribute to the
development of tension headaches. Potential
triggers may include
•stress, depression and anxiety, poor posture.
•working in awkward positions or holding one position
for a long time, and
• jaw clenching
Some people with tension headaches don't
seek medical attention and try to treat the
pain on their own. The problem with that isthat repeated use of over-the-counter (OTC)
pain relievers can actually cause overuse
headaches.
8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 33/35
A variety of medications, both OTC and
prescription, are available to stop orreduce the pain of an existing headache
attack, including pain reliever and
combination medications. Also there arepreventive medications include tricyclic
antidepressants, selective serotonin
reuptake inhibitors (SSRIs), andanticonvulsants and muscle relaxants.

8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 34/35
For this patient
•we choose combination aspirin and caffeine to relief
the pain, and also give muscle relaxants based on
the theory.
•manage his stress
•
According to his behavior and job, he has to perfecthis posture. Good posture can help keep your
muscles from tensing up.
•Massage can help reduce stress and relieve tension.
It's especially effective for relieving tight, tendermuscles in the back of your head, neck and
shoulders.
8/13/2019 Case Bersama - TTH Edit
http://slidepdf.com/reader/full/case-bersama-tth-edit 35/35