Care Group Trios: An Innovative Household Behavioral Change Model_Carolyn Kruger, Ph.D._4.23.13
14
April 23, 2013 Carolyn Kruger, Ph.D. Senior Advisor MNCH, PCI CARE GROUP TRIOS: AN INNOVATIVE HOUSEHOLD BEHAVIOR CHANGE MODEL CORE Group Spring Meeting 2013
-
Upload
core-group -
Category
Documents
-
view
147 -
download
0
description
Transcript of Care Group Trios: An Innovative Household Behavioral Change Model_Carolyn Kruger, Ph.D._4.23.13

April 23, 2013Carolyn Kruger, Ph.D.
Senior Advisor MNCH, PCI
CARE GROUP TRIOS: AN INNOVATIVE HOUSEHOLD
BEHAVIOR CHANGE MODEL
CORE Group Spring
Meeting 2013

USAID/FFP: PROSHAR – “Program for Strengthening Household Access to Resources”, June 2010 to May 2015
½ million beneficiaries (direct and indirect) in 23 unions of three Upazilas
Implementing partners include : ACDI/ VOCA; PCI; GOB; and three partner NGOs
PROSHAR OVERVIEW

SO1: Income and access to food of poor
and ultra poor households increased
SO2: “Health of pregnant & lactating women and children under 5 (with particular attention to children under 2) improved”
SO3: Institutions and households prepared to
respond effectively to shocks
IR. 2.1. Malnutrition prevented and treatedIR. 2.1. Malnutrition prevented and treated
IR. 2.2. Improved effectiveness of health
clinic services
IR. 2.2. Improved effectiveness of health
clinic services
Goal of PROSHAR: Reduced Food
Insecurity Among Vulnerable Rural
Populations in Selected Upazilas in Khulna
Division
Goal of PROSHAR: Reduced Food
Insecurity Among Vulnerable Rural
Populations in Selected Upazilas in Khulna
Division
IR. 1.2. Market linkages developed and strengthened
IR. 1.2. Market linkages developed and strengthened
IR. 1.1. Agricultural productivity
increased and diversified
IR. 1.1. Agricultural productivity
increased and diversified
IR. 1.3. Non-agriculture opportunities expanded
and diversified
IR. 1.3. Non-agriculture opportunities expanded
and diversified
IR. 3.1. Disaster Risk Reduction Plans (DRRPs)
functional
IR. 3.1. Disaster Risk Reduction Plans (DRRPs)
functional
IR. 3.2. Early warning system
functional
IR. 3.2. Early warning system
functional
IR. 3.3 Increase knowledge and
skills
IR. 3.3 Increase knowledge and
skills
INTEGRATED PROGRAM DESIGN

PCI’s research showed mothers are often the least influential in decisions about nutrition & health care
Fathers & mothers-in-law have strongest influence on behavior change; fathers dictate care seeking behaviors & mothers-in-law set child rearing practices
PCI thus developed “CG trios” that involve fathers & mothers-in-law in order to sustainably change behaviors
DEVELOPMENT OF TRIO CONCEPT

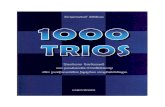
WHO INFLUENCES BEHAVIORS?
Husband Mother-in-law* Sister-in-law Neighbors No one0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
8%6%
2%
24%
41%
10%
22%
12%
28%
40%
Disapproval of pregnant women consuming extra food during pregnancy
NonDoersDoers
Targeting influential people

Sufficient breastmilk
Family Support*
Don't need extra food
Less work load
No expense* Baby doesn't cry
0%
10%
20%
30%
40%
50%
60%
70%
55%
20%
33%
12%
0%
12%
61%57%
31%
14%10%
4%
Perceived self-efficacy: What made it easier for you to exclusively breastfeed?
NonDoersDoers
Improving the knowledge and responsibility of family members on
the importance of EBF and their support of the mother
WHAT INFLUENCES NUTRITION PRACTICES
(E.G. EBF)?

TRADITIONAL CARE GROUP MODEL

Each Care Group Trio consists of 12 leaders each. Mother CGs meet monthly. Grandmothers & Father CGs will meet every three
months with the mother CGs.
(162 Care Group Trios total)
Each paid promoter oversees
approximately 10 Care Group Trios
(12 promoters
total)
Each supervisor oversees
approximately three paid promoters
(4 supervisors total)
Supervisor
PromoterGrandmothers
Mothers Fathers
Promoter
Promoter
PROSHAR TRIO CARE GROUP APPROACH
Each leader will meet with approximately 14 peers regularly (monthly/mothers & quarterly/fathers &
grandmothers) reaching 81,648 HH decision-makers

CG TRIOS MEETING
Care
Group
(Mother Leaders)
• Mother leaders (ML) meet 2x/month• Health promoter (HP) meets with MLs 2x/month; MLs organize
meeting with their groups the following week• Flipchart with specific health & nutrition messages used
Care Group
(Grand
Mother Leaders
)
• Grandmother leaders (GmLs) meet 1x/month• HP meets with GmLs in the first month of the quarter; GmLs meet with their
groups in the following two months• Flash card set is used with specific health & nutrition messages
Care Grou
p (Fath
er Leaders)
• Father leaders (FLs) meet 1x every two months• HP meets with the FL 1x/month; FLs meets with their groups in the following
two months• Flash card set is used with specific messages
Care
Group (Trios meeting)
• Every quarter HP meets with the three leader groups together• Objectives are to discuss: CG activity status; challenges; success stories;
lessons learned and plans for addressing challenges

Flipcharts Flash Cards
BCC MATERIALS DEVELOPED
Puzzles Posters
Stickers

Exclus
ive
Brea
st F
eedi
ng
Early
Initi
atio
n of
BF
3+ A
NC Visits
Post
Par
tum
Vit-
A
3 C
orre
ct IY
CF Be
havior
s0
20
40
60
80
100
31.4 38.2 32.3 34.6 29.2
56
88.7
53
73
40.9
Baseline Sept 2012 Results
BEHAVIOR CHANGE TRENDS

Building capacity of MLs to counsel CG participants using ASPIRE (ask, show, probe, inform, request, examine) – need practice!
ML uses specific CG monitoring tools – picture checklist, registration
Weak MLs are targeted for intensive one-on-one counseling by HPs
High performing CGs & families are recognized to encourage optimal behaviors at household level
Fathers need flexible meeting times that don’t interfere with work schedule
TRIO IMPLEMENTATION

1. The Trio Care Group approach is a “promising practice” that makes a diff erence in changing behaviors among pregnant women.
2. CG Trios overall have had a high level of participation (even for fathers and grandmothers who have greater participation challenges).
3. Focus on household and community behavior change, not just communication messages.
4. The three groups have diff erent roles in the family and community – discuss and demonstrate how their roles can infl uence change.
5. Promote the Trio groups as change agents, not just messengers.
6. Provide pictures of desired mother, father, grandmother desired behaviors and focus on “why the behavior is healthy”.
7. Promote home visits to promote healthy behavior change and focus on “why the behavior is healthy”.
8. Groups should meet together to identify barriers to change, to problem solve for solutions and to be accountable for change in their families and communities.
LESSONS LEARNED TO DATE

Thank You!