Cardiovascular Risk Management in HIV · HIV RNA level (
19
4/12/19 1 ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals Cardiovascular Risk Management in HIV Judith A. Aberg, MD George Baehr Professor Medicine Icahn School of Medicine at Mount Sinai Health System
Transcript of Cardiovascular Risk Management in HIV · HIV RNA level (

4/12/19
1
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health ProfessionalsACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
CardiovascularRiskManagementinHIV
JudithA.Aberg,MDGeorgeBaehr ProfessorMedicine
IcahnSchoolofMedicineatMountSinaiHealthSystem

4/12/19
2
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
LearningObjectivesUponcompletionofthispresentation,learnersshouldbebetterableto:
• AbilitytoeducateandcounselpersonswithHIVonrisk factormodificationtoreducetherisk ofcardiovascular disease.
• Abilitytodetectandmanagecardiovascularrisk factorsamongpersonswithHIVaccordingtoevidence-basedguidelines
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
FacultyandPlanningCommitteeDisclosuresPleaseconsultyourprogrambookortheConferenceApp.
Therewillbenooff-label/investigationalusesdiscussedinthispresentation.
Off-LabelDisclosure

4/12/19
3
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
MultifactorialetiologyofCVDinHIV
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
Tobacco
Mdodo R et al. Ann Intern Med. 2015;162(5):335-344. doi:10.7326/M14-0954

4/12/19
4
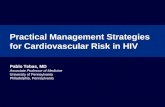
HIVandMultimorbidity 2000-2009
NAACORD Clin. Infect Dis 2017 Nov 15. doi: 10.1093/cid/cix998
28% 27% 30% 31% 32% 32% 33% 33% 32% 32%
7% 7% 9% 10% 11% 13% 14% 14% 15% 15%
2% 2% 2%
3% 3% 4%
4% 5% 6% 6%
0%
10%
20%
30%
40%
50%
60%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
6 conditions
5 conditions
4 conditions
3 conditions
2 conditions
1 condition
Perc
enta
ge o
f Ind
ivid
uals
in H
IV
Car
e w
ith A
ge-A
ssoc
iate
d C
ondi
tions
N= 4172 6325 8365 9121 9733 10861 11166 12277 9074 3705No of conditions
1 1162 1705 2512 2833 3137 3517 3687 4004 2892 11952 287 452 727 923 1108 1375 1601 1756 1363 5623 73 126 179 234 296 405 499 592 530 2144 2 8 16 30 39 69 96 111 120 525 0 1 1 1 1 1 8 10 8 36 0 0 0 0 0 0 0 0 1 0
HLDandHTNRemainMostCommon
NAACORD Clin. Infect Dis 2017 Nov 15. doi: 10.1093/cid/cix998
Hypercholesterolemia18.2%
Hypercholesterolemia19.8%3.6% 8.9% Hypertension 8.7%
0.8%0.8%1.0%
Diabetes 1.5% CKD1.3%
1.6%1.6%
1.3%
Hypertension 5.9%
2000N=4172
2009N=3705

4/12/19
5
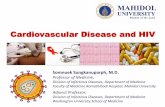
CardiovascularDiseaseMortalityAmongHIV-Infected
§ In HIV+ individuals, CVD deaths increased from 6% to 15% of all deaths (p<0.001)– Decreased in the general population: 47% →
39%
§ HIV associated with a 56% increased rate of CVD death
§ Both viremic and virologically suppressed HIV+ individuals had higher CVD mortality rates than uninfected individuals until age 65.
Hanna DB, et al. CID 2016;63:1122-9.
New York City HIV Surveillance Registry
Evaluation of age-adjusted mortality rates due to CVD inNew York City from 2001-2012; N=29,588 deaths
*Adjusted for sex, race/ethnicity, borough of residence, and calendar year
Adjusted relative rate* (95% CI) of CVD death for HIV-diagnosed New Yorkers, by age
0.27 (0.18-0.41)
0.65 (0.54-0.80)
1.10 (0.99-1.23)
1.31 (1.20-1.42)
1.75 (1.60-1.92)
2.66 (2.35-3.01)
3.02 (2.21-4.13)
2.81 (1.04-7.53)
85+
75-84
65-74
55-64
45-54
35-44
25-34
13-24
0.1 1 10
Age
CVD mortality was lower among HIV-diagnosed individuals with a suppressed HIV RNA level (<40 copies/mL) versus an unsuppressed level (age-standardized rate 3.9 vs. 7.7/1,000, p<0.001)
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
Treatment—PrimaryPrevention
• ThinkaboutASCVDriskandassessmentinHIVpatients*1st stepistoapplyGenpopguidelines
• Smokingcessationresources-Bupropion,varenicline andnon-pharmacologictherapies
• ARTforHIVVLSuppression• Manageco-morbidities:Glucose,HTN,Lipids,Obesity

4/12/19
6
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health ProfessionalsAberg J, et al. Clin Infect Dis. 2014 Jan;58(1): 1-10 and e1-34http://www.eacsociety.org/guidelines/eacs-guidelines/eacs-guidelines.html
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
Question1:WhoisRecommendedtobeprescribedastatin?
• 1.PWHwithLDL>130mg/dL• 2.PWHwithLDL>190mg/dL• 3.PWHaged40-75withLDL160-190mg/dL andCACscorezero• 4.PWHaged40-75withACC/AHAriskscore5%

4/12/19
7
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
TwoDifferentPreventionApproacheswithTwoDifferentPerspectives
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
SimilaritiesbetweentheACC/AHAandNLA• Lipidscreeningforprimarypreventionevery5years• Lifestyleadvocacyisrecommendedfirst• ASCVDriskreductionisprimarygoal• Moderate-HighStatinIntensityforprimarypharmacotherapy• Patient-providerdiscussionofrisk-to-benefitprecedesallprescribing• “Regular”lipidprofilestoassessadherence

4/12/19
8
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals

4/12/19
9
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
LipidManagement• 2013 AHA guidelines for general
population age >21 for ASCVD and aged 40-75 for other categories
– LDL-C >190, DM, ≥7.5%risk of atherosclerotic CV disease àstatins
– No lipid targets• Risk calculator controversy• How to apply to HIV+ pts
is uncertain
Stone NJ et al, Circulation, 2013
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
FourStatinBenefitGroups

4/12/19
10
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
DefiningCVDriskamongPWH
• Riskscoresfluctuateasweage,changebehaviorsandtreatconditions• Atwhattimeistheriskscoreaccurate?• WhendoesHVIVcontributetorisk?
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals

4/12/19
11
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
HIVasRiskEnhancingFactor
• Inadults40to75yearsofagewithoutdiabetesmellitusand10-yearriskof7.5%to19.9% (intermediaterisk),risk-enhancingfactorsfavorinitiationofstatintherapy
• Risk-enhancingfactorsmay favorstatintherapyinpatientsat10-yearriskof5-7.5%(borderlinerisk).

4/12/19
12
6. Inadults40to75yearsofageevaluatedforprimaryASCVDprevention,haveaclinician–patientriskdiscussionbeforestartingstatintherapy.
Riskdiscussionshouldincludeareviewofmajorriskfactors(e.g.,cigarettesmoking,elevatedbloodpressure,(LDL-C),hemoglobinA1C[ifindicated],andcalculated10-yearriskofASCVD);
•thepresenceofrisk-enhancingfactors(seeNo.8);•thepotentialbenefitsoflifestyleandstatintherapies;•thepotentialforadverseeffectsanddrug–druginteractions;•theconsiderationofcostsofstatintherapy;and•thepatientpreferences&valuesinshareddecision-making.
Top10TakeHomeMessages
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
Imaging• Inadults40to75yearsofagewithoutdiabetesmellitusandwithLDL-Clevels≥70mg/dl-89mg/dl(≥1.8-4.9mmol/L),ata10-yearASCVDriskof≥7.5%-19.9%,ifadecisionaboutstatintherapyisuncertain,considermeasuringCAC.– IftheCACscoreiszero,treatmentwithstatintherapymaybewithheldordelayed,exceptincigarettesmokers,thosewithdiabetesmellitus,andthosewithastrongfamilyhistoryofprematureASCVD.
– ACACscoreof1-99favorsstatintherapy,especiallyinthose>55yearsofage.

4/12/19
13
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
Aberg J, et al. CID 2014
Cardiovascular Disease Prevention:Lipid Management• Screening: fasting lipids
– At HIV diagnosis– Start of ART– Change of ART– Every 6-12 months
• Lipid management– Beware of drug interactions
between statins and ART
Safe (Prava caution with DRV/r)
Statin Levelwith PI/cobi
Use
Pitavastatin --Pravastatin --Atorvastatin ↑Rosuvastatin ↑Simvastatin ↑↑↑Lovastatin ↑↑↑
Contraindicated
Use with caution/low dose
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
INTREPID:StatinsWorkinPWHwithDyslipidemia
. Aberg J et al. Lancet HIV 2017

4/12/19
14
REPRIEVEStudy Design
REPRIEVEBaseline Demographics
39
Characteris'cs Total (n=7530)
Sexat Birth
Age (years)
Male 5135 (68%)
Female 2395 (32%)
Median(Q1, Q3) 50 (45--55)
EverBeenona StatinNo 6927 (94%)
Yes 467 (6%)
10--yearASCVDRisk (%) Median(Q1,Q3) 4.3 (2.1--6.9)
Race
White 2349 (32%)
Black or African 3309 (44%)American
Asian 1136 (15%)
Ethnicity Hispanicor Latino 1890 (25%)

4/12/19
15
BaselineCVDHistoryandRisk Factors
40
Characteris'cs Total (n=7530)
Totalcholesterol (mg/dL) Median(Q1, Q3) 184 (162--208)
LDL calculated (mg/dL) Median(Q1,Q3) 108 (87--127)
HDL--C (mg/dL) Median(Q1,Q3) 48 (39--59)
SystolicBP(mmHg) Median(Q1,Q3) 122 (113--132)
BMI(kg/m2) Median(Q1,Q3) 25.8 (22.8--29.4)
Smoking Status
Current 1746 (24%)
Former 1811 (25%)
Never 3821 (52%)
FamilyHistoryof CVDNo 5812 (79%)
Yes 1333 (18%)
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
PCSK-9inhibitors??• LeuckerTM.JAmHeartAssoc2018
48PWHonART,noknownCADvs.15age/LDLmatchedHIVnegativePCSK-9levels65%higherPWHv.controlPWHwithmorecoronaryendothelialdysfunction(%changeincoronaryacrosssectionalareaduringisometrichandgriponMRI)
• ZanniMV.OpenForumInfectDis.2017149PWHv.69matchedHIVnegativePWHhigherPCSK-9;PCKS-9assoc.withsCD14andsCD163(monocyteactivation)LDL-candFraminghamscorebutnotsubclinicalcoronaryatheroscleroticplaque
• BoccaraF.AIDS2017103PWHbeforeandafterstartingPIbasedARTv.90HIVnegativePWHhigherPCSK-9,nochangepre/postPIbasedARTPCSK-9assoc.withdetectableVLandCD4<200

4/12/19
16
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
Question2:WhoisRecommendedtobeprescribedaspirin?
• 1.PWHonstatins• 2.PWHwithknownASCVD• 3.PWHaged40-75asprimaryprevention• 4.PWHaged40-75withACC/AHAriskscore5%
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals

4/12/19
17
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
HypercoaguabilityinHIV
BibasMMediterrJHematolInfectDis2011
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
BackgroundASA• PWHonARThaveanincreasedriskofischemiccardiovascularevents• Activatedplateletshavebeenimplicatedinthromboticcardiovascularevents
becauseoftheirproinflammatoryandthrombogenic effects• PWHhaveincreasedcirculatingplatelet-monocytecomplexesandtheirplatelets
expresshighlevelsofP-selectin• Aspirinisalow-risk andlow-costplateletinhibitorthathasimmunomodulatory
properties• Aspirindecreasesriskofmortalityandcardiovasculareventsinindividualswith
knownCVDandmayplayanimportantroleincardiovascularandcancerpreventioninthoseatrisk
Refs:Triant etal.JID2012;205Suppl 3:5255-361.,Singhetal.2012;JVirol MethodsMay;181(2):170-6.,Mayneetal.JAIDS2012;59:340-346.,Berger,etal.AmJMed2012;12143-49.,Thunetal.NatRevClinOnc2012;9,259-267.,Hussainetal.Int Immunopharmacol 2012;12,10-20.

4/12/19
18
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
AspirinBenefits• Aspirinhasprovenbenefitsinsecondaryprevention• QuestionabletonobenefitsasprimarypreventionexceptinDM
– ARRIVE:over12,000ptsRCTasa 100mgvsplb over5years(Lancet2018;392:1036-1046)• Nosignificantdifferencesintheratesofdeaths,heartattacks,orstrokes• SignificantincreaseinGIB
– ASCEND:over15,000ptswithDMRCTover7.4years(NEnglJMed2018;379:1529-1539)
• Seriousvascularevents658participants[8.5%]vs.743[9.6%];rateratio,0.88;95%confidenceinterval[CI],0.79to0.97;P=0.01)
• Majorbleedingeventsoccurredin314participants(4.1%)intheaspiringroup,ascomparedwith245(3.2%)intheplacebogroup(rateratio,1.29;95%CI,1.09to1.52;P=0.003)
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals
TakeHomePoints• ExcessCVDriskinHIV+population(1.5x)• Individualsagingwith HIVvs.IndividualsnewlydiagnosedwithdifferentCVDrisk
• LargestmodifiableRFissmoking• Etiologymultifactorial:chronicinflammation,directviraleffect,ARVsetc.
• TreatHIVandmanageco-morbiditiesaggressively• NeedforimprovedCVDriskassessment• Anydiabeticw/LDL>70shouldbeonastatinandpossibleaspirin(oftenoverlookedpopulationinHIVclinicalpractice)

4/12/19
19
ACTHIV 2019: A State-of-the-Science Conference for Frontline Health ProfessionalsACTHIV 2019: A State-of-the-Science Conference for Frontline Health Professionals