Cardiovascular Effects, Dr. C Sedacca, 4/5/14
97
Cardiovascular Effects of Systemic Diseases Cassidy Sedacca, MS, DVM, DACVIM (Cardiology) [email protected]
-
Upload
upstatevet -
Category
Health & Medicine
-
view
149 -
download
2
Transcript of Cardiovascular Effects, Dr. C Sedacca, 4/5/14

Cardiovascular Effects of Systemic
Diseases
Cassidy Sedacca, MS, DVM, DACVIM (Cardiology)

Lecture Outline
Short description of disease Cardiac pathophysiology Diagnostics
◦ Cardiopulmonary physical examination◦ ECG◦ Radiography◦ Echocardiography
Therapy Prognosis Key Point

Systemic Diseases
Endocrine◦ Hyperthyroidism◦ Hypothyroidism◦ Cushing’s disease◦ Addison’s disease◦ Pheochromocytoma◦ Acromegaly◦ Diabetes mellitus
Metabolic◦ Hyperkalemia◦ Hypokalemia◦ Hypercalcemia◦ Hypocalcemia◦ Anemia◦ Uremia
Infectious/Inflammatory◦ Viral
◦ Bacterial
◦ Protozoal
◦ Mycotic
Miscellaneous◦ GDV
◦ Traumatic myocarditis
Neoplasia◦ Hemoangiosarcoma
◦ Lymphoma
◦ Ectopic thyroid carcinoma

Hyperthyroidism
Most common systemic disturbance to affect cardiac function in cats
Disease of middle-aged to geriatric cats (unusual before age 6)
Generally caused by thyroid adenoma in cats
Rare in dogs◦ Thyroid tumors usually nonfunctional adenocarcinomas

Hyperthyroidism
Cardiac Pathophysiology◦ Positive inotropic effects
Increased sarcolemma Na,K-ATPase activity
Increased synthesis and enhanced contractile properties of myosin
Increased # of L-type calcium channels
◦ Positive chronotropic effects
Increased rate of SA node firing
Decreased threshold of atrial activation
Shortened refractory period of conduction tissue

Hyperthyroidism
Cardiac Pathophysiology◦ Increased responsiveness to catecholamines
Number of β-receptors increase
Changes in intracellular G-protein populations
◦ “High cardiac output state” CHF
Increased metabolic rate increased tissue oxygen demands requires greater CO
Increased intravascular volume (preload)
Peripheral vasodilation = decreased SVR (afterload)
Increased contractility and HR

Hyperthyroidism
Cardiac Pathophysiology◦ Systemic hypertension
73% of cats in one study
Occurs in spite of peripheral vasodilation
Consequence of increased SV and HR
◦ Myocardial hypertrophy
Increased myosin protein synthesis
Increased responsiveness to catecholamines
Chronic volume overload
Systemic hypertension
CO = SV x HRBP = CO x SVR

Hyperthyroidism
Cardiopulmonary Examination◦ Tachycardia, premature beats, gallop sound, systolic murmur, forceful precordial impulse, hyperdynamic femoral pulses, jugular venous distension, episodic dyspnea even without CHF
ECG◦ Sinus tachycardia (42%), tall R waves (22%), R-BBB (7%), left anterior fascicular block (4%), APCs (5%), atrial tachycardia or a-fib (2%), VPCs (1%)
◦ Ventricular tachycardia and AV block (rare)

Hyperthyroidism
Radiography◦ Mild to severe cardiomegaly (50%)
◦ CHF = pulmonary edema or pleural effusion (< 5%)
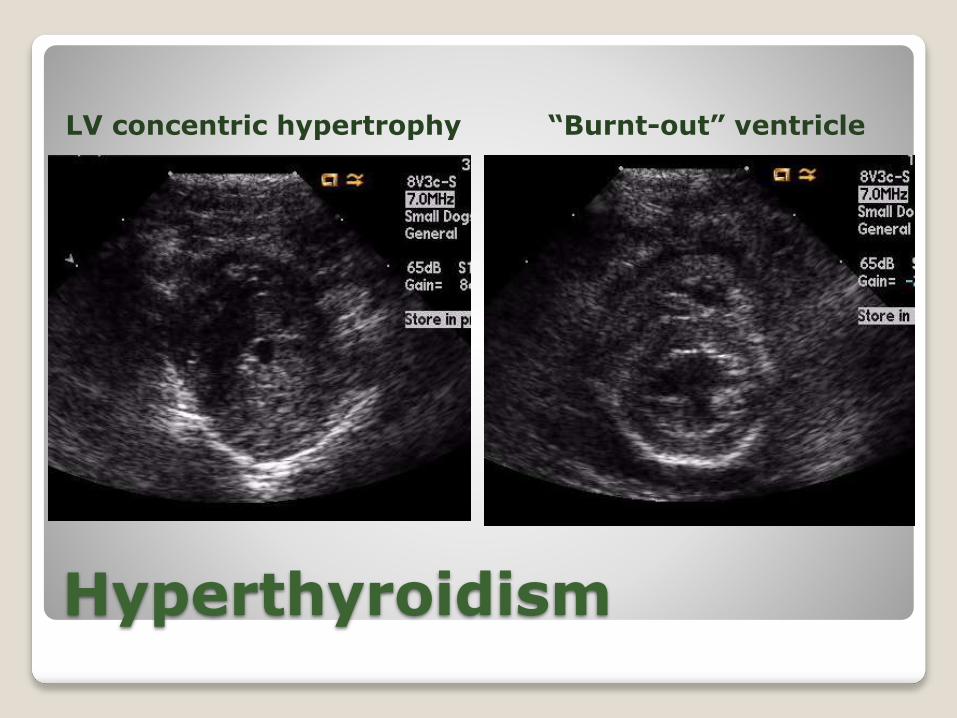
Echocardiography◦ Symmetrical LV concentric hypertrophy, hyperkinetic wall motion, increased aortic outflow velocity, normal LA size to mild dilation
◦ “Burnt-out” ventricle: wall thinning, fibrosis, LV dilation, poor contractility, severe LA dilation
Hyperthyroidism
LV concentric hypertrophy “Burnt-out” ventricle

Hyperthyroidism
Management of hyperthyroidism◦ Radioactive iodine
◦ Surgical: thyroidectomy
◦ Medical: methimazole, carbimazole
Management of arrhythmias◦ Start medical treatment
◦ Beta-blockers (atenolol) for most
Careful of negative inotropic effects if CHF
◦ If CHF, diltiazem or digoxin for atrial ectopy

Hyperthyroidism
Management of hypertension◦ Control of hyperthyroid state
◦ Beta-blockers (atenolol) or vasodilators (amlodipine)
Management of CHF◦ Diuretics (furosemide) and ACE-inhibitors (enalapril, benazepril)
◦ Ancillary drugs (diltiazem, atenolol, pimobendan, digoxin, etc.)

Hyperthyroidism
Prognosis◦ Favorable – ECG, echocardiography, and blood pressure changes are reversible in most cases
◦ Poor – “burnt-out” ventricle and CHF
Key Point
The net effects of hyperthyroidism on CV system are enhanced contractility, tachycardia, cardiomegaly,
LV hypertrophy, high cardiac output, systemic hypertension, and occasionally high-output heart failure.

Hypothyroidism
Common endocrinopathy in dogs Most common causes: idiopathic atrophy
and immune-mediated thyroiditis Clinical signs usually develop middle age Rare as a naturally occurring condition in
cats Cardiac effects rarely have severe
consequences◦ Can aggravate CHF and complicate the management of cardiac patients

Hypothyroidism
Cardiac Pathophysiology◦ Opposite of hyperthyroidism
◦ Negative inotropic effects
Decreased Na, K-ATPase activity
Decreased synthesis and contractile properties of myosin
Decreased # of β-receptors
◦ Negative chronotropic effects
Decreased rate of SA node firing
Increased threshold of atrial activation
Prolonged refractory period of conduction tissue
Hypothyroidism
Cardiac Pathophysiology◦ Alters cholesterol and lipid metabolism Can result in atherosclerosis (rare)
Hypercoagulability leading to myocardial infarction or systemic/pulmonary thrombosis
◦ Decreases metabolic rate thus lessening the “required” cardiac output Correcting hypothyroidism increased workload on heart
◦ Hypothyroidism decreases digoxin clearance, predisposing to digoxin toxicity

Hypothyroidism
Cardiopulmonary Examination◦ Bradycardia, arrhythmias, weak precordial impulse, weak femoral pulses
ECG◦ Sinus bradycardia◦ Low voltage QRS complexes◦ Atrial and ventricular arrhythmias ◦ AV block◦ Prolonged QRS duration◦ Inverted T waves

Hypothyroidism
Echocardiography◦ Mild to marked decreases in indices of contractility
◦ Can cause a secondary form of DCM
Always check thyroid status when depressed contractility is noted in a breed not predisposed to heritable/primary DCM

Hypothyroidism
Treatment◦ Levothyroxine
◦ Cautious with treatment in patients with CHF
Supplementation increases metabolic rate and thus work required by heart
Start with ¼ standard dose and increase it by ¼ dose weekly
Prognosis◦ Favorable – most cardiac changes are reversible
Key Point
Hypothyroidism rarely causes congestive heart failure but can exacerbate cardiac function if underlying cardiac disease
is present.
Key Point
Evaluate thyroid status in any dog in congestive heart failurewith an inappropriately slow heart rate.

Addison’s Disease
Potentially life-threatening endocrinopathy
Uncommon in dogs; rare in cats
More common in females
Usually young to middle age
Immune-mediated destruction within adrenal gland◦ Zona glomerulosa = aldosterone
◦ Zona fasciculata = cortisol

Addison’s Disease
Cardiac Pathophysiology◦ Cortisol needed to maintain vascular integrity and responsiveness to catecholamines
Cortisol deficiency predisposes to hypotension
◦ Cortisol has a mild positive inotropic effect

Addison’s Disease
Cardiac Pathophysiology◦ Aldosterone acts on distal renal tubule and collecting duct to enhance Na+ retention and K+ excretion
Deficiency = hyponatremia and hyperkalemia
Hyponatremia intravascular fluid shifts causing
hypovolemia and hypotension
Hyperkalemia alters cardiac conduction and
repolarization leading to bradycardia and various dysrhythmias

Addison’s Disease
Hyperkalemia◦ Early: increases in Ikr affects repolarization phase (phase 3) of action potential Peaked T waves, QT interval shortening
◦ Persistent: reduces RMP inactivates INa
decreases rate of phase 0 of action potential reduction in myocardial conduction Prolongation of P wave, PR interval, and QRS complex
Loss of P wave and progressive widening of QRS
Sinoventricular rhythm (“atrial standstill”)
◦ Eventually: Ventricular fibrillation and asystole
Na+inK+out
RMP _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _
Addison’s Disease
Cardiopulmonary Examination◦ Weakness, collapse, dehydration, hypothermia, slow CRT, bradycardia, weak femoral pulses
ECG◦ Previously discussed
Radiography◦ Signs of hypovolemia
◦ Small caudal vena cava
◦ Microcardia
◦ Decreased pulmonary vascular markings

Addison’s Disease

Addison’s Disease
Addisonian Crisis Therapy◦ Volume replacement (0.9% saline)
◦ Glucocorticoid replacement (methylprednisolone, dexamethasone)
◦ Mineralocorticoid replacement (DOCP, Florinef)
◦ Hyperkalemia Calcium gluconate – counteracts effects on conduction
tissue; no effect on serum K+ levels
Saline infusion – causes rapid dilution of serum K+
NaHCO3 (if pH ≤ 7.0) – moves K+ inside cell by correcting acidosis
50% dextrose – stimulates endogenous insulin secretion which moves K+ inside cell
Regular insulin – moves K+ inside cell

Addison’s Disease
Maintenance Therapy◦ DOCP + Prednisone
◦ Florinef + Prednisone
Prognosis◦ Excellent with therapy
Key Point
Net CV effects are hypovolemia, systemic hypotension, altered cardiac conduction, and depressed myocardial function.

Cushing’s Disease
Common endocrinopathy in older dogs; rare in cats
Excessive cortisol levels◦ Pituitary (80-85%) – excess ACTH release
No sex predilection
◦ Adrenal – functional adrenocortical tumors
Females affected more frequently
◦ Rarely produces significant cardiac disease
◦ Systemic effects can exacerbate underlying cardiac disease

Cushing’s Disease
Cardiac Pathophysiology◦ Systemic hypertension Present in 57-82% of cushingoid dogs
Cortisol increases SVR by increasing smooth muscle sensitivity to catecholamines and increasing production of angiotensinogen
Can cause secondary LV concentric hypertrophy
Increased afterload can exacerbate mitral regurgitation
Cortisol enhances renal reabsorption of Na+ and secondary fluid retention increases intravascular volume

Cushing’s Disease
Cardiac Pathophysiology◦ Concentric hypertrophy of left ventricle
Primary – exact cause unknown
Secondary to systemic hypertension
Can lead to diastolic myocardial dysfunction but rarely causes CHF if concomitant heart disease not present

Cushing’s Disease
Cardiac Pathophysiology◦ Thromboembolism
Both pulmonary and systemic
High incidence of PTE in cushingoid patients
Cause of distal aortic thrombus in dogs
Cushing’s disease clearly causes hypercoaguability◦ Higher levels of clotting factors II, V, VIII, IX, XI,
protein C, protein S decreases aPTT
◦ Impaired fibrinolytic capacity increases clot lysis
time
Cushing’s Disease
Cardiac Pathophysiology◦ Panting/tachypnea/mild dyspnea
Altered ventilation mechanics
Weakness in muscles of respiration
Increased thoracic fat deposition decreases
chest wall compliance
Increased diaphragmatic abdominal pressure from excessive adipose tissue and hepatomegaly
+/- concurrent lower airway disease or pulmonary parenchymal disease

Cushing’s Disease
Cardiopulmonary Examination◦ Abdominal distension, hepatomegaly, muscle
weakness, obesity
ECG – no characteristic changes Radiography
◦ Calcification of tracheal and bronchial rings
◦ Osteoporosis of thoracic vertebrae
◦ Rarely metastatic pulmonary lesions from adrenal tumors
◦ Changes associated with PTE
Echocardiography◦ Primary or secondary LV concentric hypertrophy
Cushing’s Disease
Therapy◦ Pituitary dependent
Mitotane Trilostane
◦ Adrenal dependent Surgical removal of affected adrenal gland(s) Medical therapy
Prognosis◦ Excellent for resectable, benign adrenal tumors ◦ Poor for non-resectable or metastatic adrenal tumors◦ Most dogs with PD respond well to therapy◦ Systemic hypertension usually resolves with control
of hypercortisolism
Key Point
Hypercortisolism exacerbates concomitant heart disease by activating the RAAS, increasing intravascular volume,
increasing SVR (afterload), and potentially causing systemic hypertension and left ventricular concentric hypertrophy.

Acromegaly
Hypersomatotropism = abnormally high levels of growth hormone
Rare endocrinopathy in cats◦ Much more common in males
◦ Functional pituitary adenoma
Associated with generalized organomegaly◦ Increased protein synthesis and reduction in protein catabolism
◦ Modulation in glucose utilization and storage (often associated with diabetes)

Acromegaly

Acromegaly
Cardiac Pathophysiology◦ Myocardial hypertrophy, interstitial fibrosis,
myocytolysis, intramural arteriosclerosis
◦ Systemic hypertension
Cardiopulmonary Examination◦ Systolic murmur, gallop sound, signs of CHF
ECG – no characteristic changes Radiography
◦ Cardiomegaly
◦ Pulmonary edema and/or pleural effusion (CHF)
Echocardiography◦ LV concentric hypertrophy

Acromegaly

Acromegaly
Treatment◦ Surgery – hypophysectomy◦ Medical – somatostatin analogue (hypothalamic hormone that inhibits GH release from pituitary)
◦ Radiation – seems to be the best treatment option thus far
Prognosis◦ Survival ranges from 4 to 60 months◦ Most die or euthanized from CHF, renal failure, or expanding pituitary tumor

Pheochromocytoma
Catecholamine-secreting tumors derived from chromaffin cells of adrenal medulla
Excessive epinephrine and norepinephrine
Uncommon in dogs, extremely rare in cats
Usually older dogs
Locally invasive

Pheochromocytoma
Cardiac Pathophysiology◦ Alpha-1, beta-1, and beta-2 adrenergic agonistic effects of epinephrine and norepinephrine
Beta-1 (cardiac): positive inotropic, chronotropic, and dromotropic effects
Beta-2 (vessel): venous and arteriole vasodilation
Alpha-1 (vessel): venous and arteriole vasoconstriction◦ Dominant effect varies with receptor density

Pheochromocytoma
Cardiac Pathophysiology◦ Systemic hypertension
Alpha predominates in vascular smooth muscle so systemic hypertension is common (~50% of dogs)
◦ Arrhythmias from excessive catecholamines
Promote all 3 “mechanisms” of arrhythmias
Myocardial injury
Coronary vasoconstriction ischemia
◦ Local invasion into caudal vena cava
Thrombosis

Pheochromocytoma
Cardiopulmonary Examination◦ Clinical signs often episodic
◦ Collapse, syncope, weakness
◦ Pale MM, tachycardia, arrhythmias, pulse deficits
ECG◦ Nonspecific ST segment changes – myocardial
ischemia/hypoxia
◦ Sinus tachycardia very common
◦ Arrhythmias – APCs, VPCs, SVT, VT, etc.
Radiography and Echocardiography◦ Nonspecific

Pheochromocytoma
Therapy◦ Systemic hypertension
Alpha-blocking agents
Phenoxybenzamine (oral), Phentolamine (IV) –non-selective
Prazosin (oral) – alpha-1 only
◦ Tachyarrhythmias
Beta-blocking agents
Propranolol (oral, IV) – non-selective
Atenolol (oral), esmolol (IV) – beta-1 only
◦ Surgical removal definitive treatment
Key Point
Use of a beta-blocker without an alpha-blocker can cause severe hypertension.

Diabetes Mellitus
Insulin deficiency or resistance
CV system of dogs and cats is relative immune to the effects of hyperglycemia compared to humans
Humans ◦ Systemic hypertension
◦ Arrhythmias
◦ Coronary atherosclerosis
◦ Myocardial infarction
◦ “Diabetic cardiomyopathy”
Diabetes Mellitus
Cardiac Pathophysiology◦ Systemic hypertension
46% of dogs in one study
Severity associated with duration of disease in dogs
Less common in cats
Cause: not known◦ Changes in vascular compliance
◦ Changes in lipid profile
◦ Microangiopathy affecting the basement membrane

Diabetes Mellitus
Cardiac Pathophysiology◦ “Diabetic cardiomyopathy” Humans – myocardial hypertrophy, fibrosis, coronary microvascular endothelial proliferation, glycoprotein accumulation
Mild in humans without macrovascular coronary disease and systemic hypertension
Mild subclinical systolic myocardial dysfunction in dogs with experimental diabetes
Diastolic dysfunction mild and inconsistent in dogs
CHF not reported in dogs or cats
Increased risk for coronary artery disease notdemonstrated in dogs or cats
Key Point
Decreased cardiac performance in dogs and cats with diabetes is mild and unlikely to cause clinical problems unless accompanied by other forms of heart disease.
Hyperkalemia
95% of body K+ is intracellular ◦ 2-5% extracellular◦ Serum K+ values are not always reliable indicator of total body stores
Clinical causes◦ Decreased renal elimination (renal failure)◦ Ruptured urinary tract, urethral obstruction◦ Reperfusion injury (ie, aortic thromboembolism)
◦ Addison’s disease◦ Metabolic acidosis◦ Drugs (spironolactone, ACE-inhibitors)◦ Excessive supplementation
Hyperkalemia
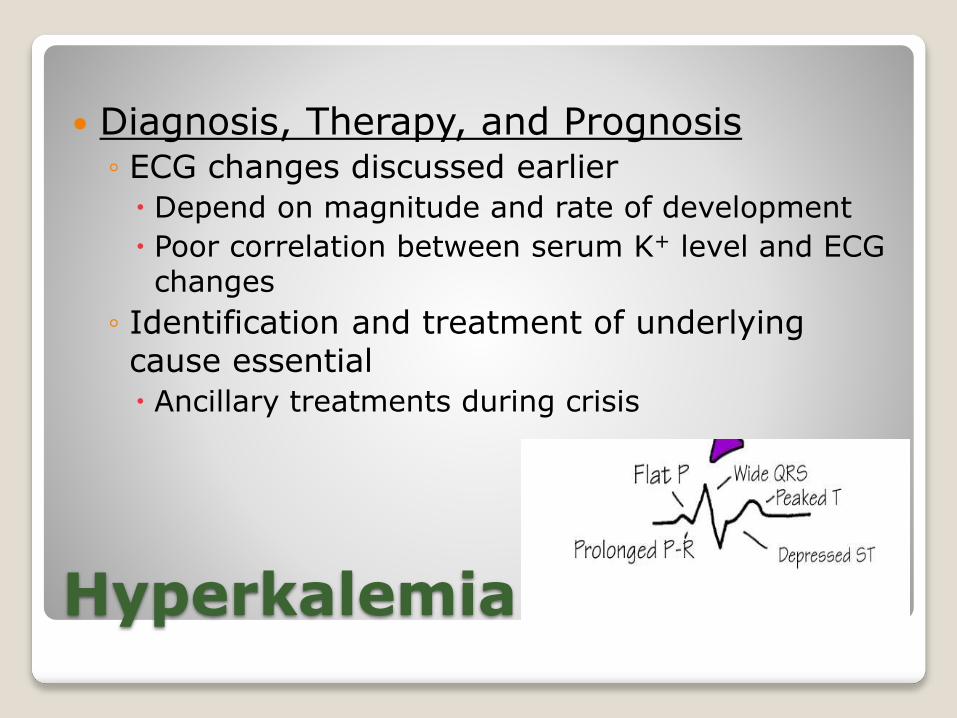
Diagnosis, Therapy, and Prognosis◦ ECG changes discussed earlier
Depend on magnitude and rate of development
Poor correlation between serum K+ level and ECG changes
◦ Identification and treatment of underlying cause essential
Ancillary treatments during crisis

Hyperkalemia

Hypokalemia
Severe K+ loss leads to muscle weakness or paralysis
Clinical causes◦ Decreased intake (anorexia, K+ deficient fluids)
◦ Excessive GI loss (chronic vomiting, diarrhea)
◦ Overuse of enemas
◦ Excessive urinary loss (renal disease, drugs)
◦ Hyperaldosteronism (primary: tumor vs. secondary: liver failure, nephrotic syndrome)
◦ Metabolic alkalosis

Hypokalemia
Cardiac Pathophysiology◦ Hyperpolarization of nerve and myocyte cell
membrane, thus increasing RMP
◦ Delayed/abnormal repolarization
◦ Increased action potential duration
◦ Increased automaticity
ECG◦ Prolonged QT interval
◦ ST segment depression
◦ U wave (repolarization of
papillary m. and Purkinje
fibers)
◦ Ventricular arrhythmias

Hypokalemia
Tilley LP: Essentials of canine and feline electrocardiography, 3rd ed., 1992

Hypokalemia
Cardiopulmonary Examination◦ Muscle weakness
◦ Depression
◦ Ventroflexion of neck in cats
◦ Arrhythmias
Therapy◦ Treat underlying disease process
◦ Parental replacement
Do not exceed 0.5 mEq/kg/hr
◦ Oral supplementation if needed

Hypokalemia
Key Points◦ Increased likelihood of digoxin toxicity
Digoxin competes with K+ for same binding site on the Na+/K+-ATPase
◦ Increased risk of ventricular arrhythmias
◦ Decreased effectiveness of Class I antiarrhythmic agents (lidocaine, mexiletine, procainamide)
Hypercalcemia
Clinical causes◦ Normal in young, growing puppies◦ Paraneoplastic (lymphoma, anal sac carcinoma)◦ Addison’s disease◦ Renal failure◦ Skeletal lesions (osteomyelitis, multiple myeloma)
◦ Nutritional (hypervitaminosis D)◦ Primary hyperparathyroidism ◦ Severe hypothermia◦ Lab error

Hypercalcemia
Cardiac Pathophysiology◦ Little, if any, direct adverse effect on cardiac function
◦ Very high levels can cause arrhythmias
◦ Long-standing may predispose to calcification of myocardium, blood vessels, and other soft tissues (“metastatic calcification”)
Cardiopulmonary Examination◦ None specific

Hypercalcemia
ECG◦ ECG changes do not correlate closely with serum calcium concentration
◦ Short QT interval
◦ Sinus bradycardia
◦ Ventricular irritability and fibrillation at very high levels
Radiography/Echocardiography◦ None specific

Hypercalcemia
Therapy◦ IV fluids (0.9% saline) – promote renal excretion
◦ Calcitonin – parafollicular cells of thyroid (opposite of parathyroid hormone)
◦ Furosemide – promote renal excretion
◦ Corticosteroids – decrease intestinal absorption, limit bone resorption, increase renal excretion
◦ Bisphosphonates – limit osteoclastic resorption

Hypocalcemia
Clinical causes◦ Eclampsia
◦ Renal failure
◦ Acute pancreatitis
◦ Hypoparathyroidism
◦ Bilateral thyroid gland removal
◦ Post-op parathyroid tumor removal
◦ Ethylene glycol toxicity
◦ Hyperphosphatemia
◦ Relative (due to hypoalbuminemia)

Hypocalcemia
Cardiac Pathophysiology◦ Excitatory effect on nerve and muscle cells
Neuromuscular irritability, tetany, and seizures
◦ Decreased contractility
Only clinically important if concurrent heart disease
◦ Acute reductions can result in severe hypotension leading to cardiovascular shock
Cardiopulmonary Examination◦ None specific

Hypocalcemia
Synchronous diaphragmatic flutter◦ Synchronous contraction of the diaphragm with the heart beat
◦ Rhythmic abdominal contractions with heart beat
◦ Excitation of pericardial segment of phrenic nerve(s) by electrical activity of heart
◦ Most commonly seen in patients that are hypocalcemic from persistent vomiting
◦ Cause unknown – alkalosis or hypocalcemialeading to hyperirritability of phrenic nerve

Tiley LP, 1992.
Hypocalcemia
ECG◦ Classic: QT prolongation
Therapy◦ Calcium gluconate IV
while monitoring ECG
Slowly (15-30 min)
Temporarily stop if
bradycardia or ST segment elevation
Reinstate at slower rate
◦ Oral vitamin D
Increases intestinal Ca+2 absorption
Key Point
Calcium is cardiotoxic if replaced too quickly; even a normal serum concentration may be toxic if replaced too rapidly

Anemia
Sign of disease; not a disease entity
Symptoms of “reduced cardiac reserve”◦ Severity of anemia
◦ Rate of development
◦ Presence and extent of underlying cardiac disease

Anemia
Cardiac Pathophysiology◦ O2 delivery to tissues, blood viscosity SVR RAAS, ADH, SNS Na+ and H2O retention HR, SV, SVR CO and BP
◦ Depends on developmental rate of anemia
Acute – hypovolemic shock
Chronic – volume overload to all four cardiac chambers (eccentric hypertrophy), tachycardia,
SVR, increased myocardial oxygen demands
◦ Rarely causes CHF but certainly can exacerbate subclinical/pre-existing heart disease

Anemia
Cardiopulmonary Examination◦ Lethargy, exercise intolerance, weakness, collapse, syncope, stupor, exertional dyspnea
◦ Strong precordial impulse, hyperdynamicfemoral pulses (bounding), pale/icteric MM, prolonged CRT
◦ Soft (grade I-II/VI) systolic heart murmur due to blood viscosity and SV
Radiography◦ Cardiomegaly◦ Rarely, pulmonary venous distension, pulmonary edema, pleural effusion (CHF)

Anemia
ECG◦ Sinus tachycardia◦ Evidence of LV or LA enlargement (prolonged P wave or QRS duration, increased R wave amplitude)
◦ Ventricular arrhythmias from tissue (myocardial) hypoxia
Echocardiography◦ LV, LA, RV, and RA chamber dilation (volume overload)
◦ Hyperdynamic systolic myocardial function

Anemia
Therapy◦ Treatment depends on underlying cause
◦ Cautious with IV fluids when cardiomegaly present in the face of significant anemia
◦ If blood transfusion needed, packed RBCs are preferred b/c of smaller volume
◦ Furosemide if CHF present
Often can be discontinued once anemia corrected

Uremia
Clinical manifestation of azotemia
Can effect cardiac function
Reduce elimination of many cardiac drugs

Uremia
Cardiac Pathophysiology◦ Systemic hypertension common in CRF of both dogs (50-93%) and cats (65%)
◦ RF can cause elevations or reductions of K+ and Ca+2
Associated ECG changes
◦ Volume overload from chronic anemia
◦ Secondary pericarditis
Serositis of parietal pericardium
Small volume pericardial effusion

Uremia
Cardiac Pathophysiology◦ Pulmonary or systemic thromboembolism
Protein-losing nephropathy (antithrombin)
◦ Uremic pneumonitis
Rare cause of non-cardiogenic pulmonary edema

Uremia
Cardiopulmonary Examination◦ Uremic pneumonitis can cause dyspnea
◦ Metabolic acidosis can cause compensatory hyperventilation (tachypnea)
◦ Both can be confused with signs of CHF
ECG◦ Nonspecific
Electrolyte abnormalities
Pericardial effusion (decreased R wave amplitude)
◦ Conduction abnormalities (high grade 2nd or 3rd
degree AV block in cats???)

Uremia
Radiography◦ None specific
Echocardiography◦ LV concentric hypertrophy secondary to systemic hypertension
◦ Volume overload from chronic anemia
◦ Small volume pericardial effusion
Therapy◦ IV fluids, protein/P restriction, phosphate binders, calcitriol, erythropoietin

Uremia
Uremia
Challenge of managing azotemia with concurrent heart disease◦ “Cardiorenal Syndrome” in people
◦ Azotemia both pre-renal and renal
◦ Two subsets of patients
Subclinical heart disease
Congestive heart failure
◦ Uremic and currently in CHF?
No – reduce diuretic doses, improve cardiac output, or administer parental fluids
Yes – “rock and a hard place” unless Ultrafiltration

Uremia
Therapeutic considerations in azotemicpatients with heart disease◦ Use IV fluids cautiously
Slowly correct azotemia by reducing fluid rates
Consider low-Na+ fluids (half-strength saline)
Continually monitor for CHF (body weight, RR, thoracic auscultation, radiographs)
◦ No reason for simultaneous diuretic and parental (IV/SQ) fluid administration

Uremia
Therapeutic considerations in azotemicpatients with heart disease◦ Reduce doses of renally-excreted drugs Digoxin, sotalol, atenolol
◦ Careful with ACE-inhibitors Angiotensin II causes preferential vasocontrictionof efferent arteriole of glomerulus
Enalapril vs Benazepril
Safe to use other vasodilators (pimobendan, amlodipine, hyralazine, prazosin)
Spironolactone (aldosterone antagonist) as an alternative

Myocarditis
Inflammation involving cardiomyocytes, interstitium, or coronary vessels
Myocardial injury1. Direct invasion by an infectious agent
◦ Fungal, Toxoplasma, Neospora, Trypanosoma, Bartonella, viral (parvovirus, distemper virus, others)
2. Myocardial toxin produced by the agent◦ Trypanosoma, bacterial (endotoxin)
3. Secondary immune-mediated reaction◦ Vaccine, Lyme, rickettsial, bacterial (sepsis), neoplasia,
idiopathic/auto-immune

Myocarditis
Wide range of clinical disease◦ Subclinical myocarditis
◦ Array of arrhythmias and conduction abnormalities
◦ Secondary DCM-phenotype leading to CHF
Cardiac troponin-I◦ Released with cardiomyocyte damage, swelling, or necrosis
◦ Highly specific (compared to CPK) but notsensitive

Myocarditis
ECG◦ Supraventricular or ventricular ectopy◦ Bundle branch block◦ High-grade 2nd or 3rd degree AV block
Echocardiography◦ No changes at all◦ Acute – hypoechoic or mottled myocardium with concentric hypertrophy, small volume pericardial effusion
◦ Chronic – dilated chambers with decreased contractility and thin walls (2o DCM)

Myocarditis
ChronicAcute

Myocarditis
Therapy◦ Treat the primary agent IF KNOWN
◦ Treatment usually supportive and focused on the most prominent systemic manifestation
◦ Often permanent/irreversible damage even if treated appropriately
Prognosis◦ Highly variable
Key Point
If an underlying infectious agent cannot be determined, anti-inflammatory doses of corticosteroids are
often administered.
Gastric Dilation-Volvulus
Life-threatening emergency in dogs
Most common in large, deep-chested dogs
Exact etiology yet to be determined◦ Exercise following a large meal
Arrhythmias in up to 40% of cases◦ Most are ventricular
◦ Usually occur within 36 hours of admission
◦ Presence of arrhythmias does not worsen prognosis

Gastric Dilation-Volvulus
Cardiac Pathophysiology◦ Exact mechanism for arrhythmias not known
◦ Theories
Acid-base imbalances
Electrolytes imbalances
Autonomic nervous system imbalances
Myocardial hypoxia
Myocardial depressant factor

Gastric Dilation-Volvulus
Cardiopulmonary Examination◦ Pale MM, weak pulses, tachycardia, arrhythmias, signs of shock
ECG◦ All types of ventricular arrhythmias
Accelerated idioventricular rhythm most common
◦ Occasionally atrial arrhythmias
◦ ST segment changes myocardial
ischemia/hypoxia

Gastric Dilation-Volvulus
Accelerated idioventricular rhythm◦ Wide, bizarre rhythm
◦ Rate similar to sinus rate (< 160 bpm)
◦ As sinus rate slows, ventricular rate may “capture” the heart rhythm
◦ Fusion beats common

Gastric Dilation-Volvulus
Radiography◦ Microcardia and small caudal vena cava
◦ Decreased venous return
Therapy◦ Gastric decompression
◦ Shock therapy
◦ Treatment of arrhythmias
See above
Lidocaine for malignant ventricular ectopy
Traumatic Myocarditis
Arrhythmias that occur following blunt trauma
Trauma does not have to occur directly to chest
Exact mechanism for arrhythmias notknown◦ Direct damage to myocardium from trauma not necessary
◦ Autonomic nervous system imbalances?◦ Reperfusion of ischemic tissue?

Traumatic Myocarditis
ECG◦ All types of ventricular arrhythmias Accelerated idioventricular rhythm common
◦ Supraventricular arrhythmias
Therapy◦ Main goal is supportive care (pulmonary contusions, shock, hemorrhage, pain, etc.)
◦ Treatment of arrhythmias if hemodynamically significant Causing tachycardia, hypotension, malignant characteristics, etc.

Traumatic Myocarditis
PPVP Diniz, DS Schwartz, RC Collicchio-Zuanaze. Arq. Bras. Med. Vet. Zootec, 59: 2007

Traumatic Myocarditis
Treatment of ventricular arrhythmias◦ Lidocaine – class Ib (Na+ blocker)
◦ Procainamide – class Ia (Na+ blocker)
◦ Esmolol – class II (beta-blocker)
◦ Magnesium chloride
Treatment of supraventricular arrhythmias◦ Diltiazem – class IV (Ca+2 blocker)
◦ Esmolol
◦ Procainamide

Traumatic Myocarditis
Prognosis◦ Arrhythmias generally resolve after 2-5 days and do not require maintenance oral therapy
◦ Arrhythmias generally not lethal
◦ Progression of underlying disorders, not arrhythmias, usually lead to patient’s demise

Systemic Neoplasia
Systemic neoplasia with a cardiac manifestation◦ Hemangiosarcoma
◦ Lymphoma
◦ Ectopic thyroid carcinoma
Clinical signs◦ Pericardial effusion/cardiac tamponade
◦ CHF from myocardial dysfunction or ventricular inflow or outflow obstruction
◦ Arrhythmias
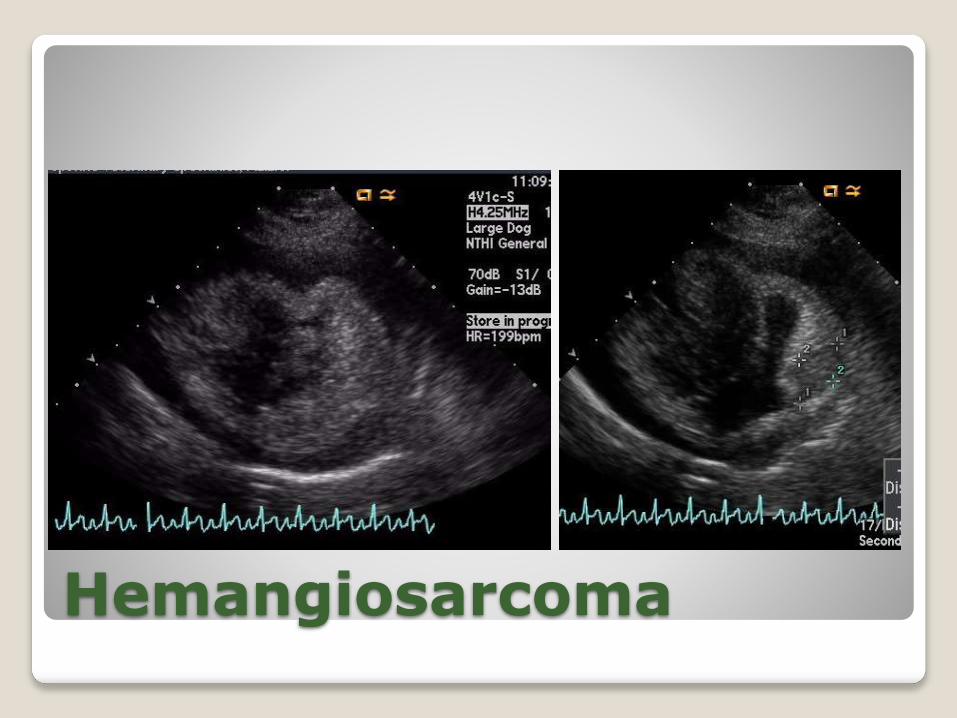
Hemangiosarcoma
Originates from endothelial cells
Systemic sites of origin◦ Spleen, liver, lungs, skin, etc.
Can be seen in any portion of heart◦ Right atrium and right auricle most common
Metastasis is common
Most common in large breed dogs
Rare in cats
Hemangiosarcoma
Lymphoma
Most common tumor that metastasizes to heart in cats
Infiltrative myocardial disease◦ Ventricular hypertrophy
◦ Severe changes to myocardial architecture and echogenicity
◦ Can produce a well-defined mass
◦ Pericardial effusion

Thank You!