Cardiopulmonary exercise testing and prognosis in severe heart failure: 14 mL/kg/min revisited
7
undergo transplantation, resulting in a net increase of 200 or more patients to the waiting list per month. 10 To direct the limited number of donor hearts to patients who need them the most, a great deal of effort has been directed toward stratifying risk among patients with severe chronic heart failure through the use of clinical, hemodynamic, and exercise test data. In recent years, exercise capacity has been demonstrated to be an important component of the risk profile among persons with chronic heart failure. In particular, directly mea- sured peak oxygen uptake in some studies has outper- formed clinical, hemodynamic, and other exercise test data in predicting 1 to 2 year mortality. 11-15 Several investigators have reported that patients who achieve a peak VO 2 of 14 mL/kg/min appear to have a prog- nosis similar to that among patients who receive trans- plants (approximately 90% at 1 year). 11-17 This finding implies that transplantation can be safely deferred among these patients. This cutpoint has emerged as a prominent prognostic marker in chronic heart failure and is listed as a relative indication for transplantation in Prognosis remains a major concern for patients with chronic heart failure. Despite advances in therapeutic options for this condition, the risk for death among patients with severe chronic heart failure remains 30% to 60% annually. 1-4 Transplantation has been demonstrated to improve prognosis considerably. The 1-year survival rate is 85% to 90% and the 5-year survival rate 70% to 75%. Successful transplantation combined with rehabili- tation is associated with improvements in exercise capacity. 5-9 However, there remains a paucity of available donor hearts relative to demand. United Network for Organ Sharing data suggest that among approximately 400 new patients placed on the heart transplant waiting list each month, only 150 to 200 patients are able to From the Palo Alto Veterans Affairs Health Care System, Falk Cardiovascular Research Center, Stanford University School of Medicine. Submitted January 20, 1999; accepted June 27, 1999. Reprint requests:Michael B. Fowler, MD, The Falk Cardiovascular Research Center, Stanford University School of Medicine, Stanford, CA 96305. Copyright © 2000 by Mosby, Inc. 0002-8703/2000/$12.00 + 0 4/1/101493 Congestive Heart Failure Cardiopulmonary exercise testing and prognosis in severe heart failure: 14 mL/kg/min revisited Jonathan Myers, PhD, Lars Gullestad, MD, Randall Vagelos, MD, Dat Do, BS, Daniel Bellin, BS, Heather Ross, MD, and Michael B. Fowler, MD Stanford, Calif Background Accurately establishing prognosis in severe heart failure has become increasingly important in assessing the efficacy of treatment modalities and in appropriately allocating scarce resources for transplantation. Peak exercise oxy- gen uptake appears to have an important role in risk stratification of patients with heart failure, but the optimal cutpoint value to separate survivors from nonsurvivors is not clear. Methods Six hundred forty-four patients referred for heart failure evaluation over a 10-year period participated in the study. After pharmacologic stabilization at entrance into the study, all participants underwent cardiopulmonary exercise test- ing. Survival analysis was performed with death as the end point. Transplantation was considered a censored event. Four- year survival was determined for patients who achieved peak oxygen uptake values greater than and less than 10, 11, 12, 13, 14, 15, 16, and 17 mL/kg/min. Results Follow-up information was complete for 98.3% of the cohort. During a mean follow-up period of 4 years, 187 patients (29%) died and 101 underwent transplantation. Actuarial 1- and 5-year survival rates were 90.5% and 73.4%, respectively. Peak ventilatory oxygen uptake (VO 2 ) was an independent predictor of survival and was a stronger predictor than work rate achieved and other exercise and clinical variables. A difference in survival of approximately 20% was achieved by dichotomizing patients above versus below each peak VO 2 value ranging between 10 and 17 mL/kg/min. Survival rate was significantly higher among patients achieving a peak VO 2 above than among those achieving a peak VO 2 below each of these values (P < .01), but each cutpoint was similar in its ability to separate survivors from nonsurvivors. Conclusion Peak VO 2 is an important measurement in predicting survival from heart failure, but whether an optimal cut- point exists is not clear. Peak VO 2 may be more appropriately used as a continuous variable in multivariate models to pre- dict prognosis in severe chronic heart failure. (Am Heart J 2000;139:78-84.)
-
Upload
jonathan-myers -
Category
Documents
-
view
215 -
download
0
Transcript of Cardiopulmonary exercise testing and prognosis in severe heart failure: 14 mL/kg/min revisited

undergo transplantation, resulting in a net increase of200 or more patients to the waiting list per month.10
To direct the limited number of donor hearts topatients who need them the most, a great deal of efforthas been directed toward stratifying risk among patientswith severe chronic heart failure through the use ofclinical, hemodynamic, and exercise test data. In recentyears, exercise capacity has been demonstrated to be animportant component of the risk profile among personswith chronic heart failure. In particular, directly mea-sured peak oxygen uptake in some studies has outper-formed clinical, hemodynamic, and other exercise testdata in predicting 1 to 2 year mortality.11-15 Severalinvestigators have reported that patients who achieve a peak VO2 of 14 mL/kg/min appear to have a prog-nosis similar to that among patients who receive trans-plants (approximately 90% at 1 year).11-17 This findingimplies that transplantation can be safely deferredamong these patients. This cutpoint has emerged as aprominent prognostic marker in chronic heart failureand is listed as a relative indication for transplantation in
Prognosis remains a major concern for patients withchronic heart failure. Despite advances in therapeuticoptions for this condition, the risk for death amongpatients with severe chronic heart failure remains 30% to60% annually.1-4 Transplantation has been demonstratedto improve prognosis considerably. The 1-year survivalrate is 85% to 90% and the 5-year survival rate 70% to75%. Successful transplantation combined with rehabili-tation is associated with improvements in exercisecapacity.5-9 However, there remains a paucity of availabledonor hearts relative to demand. United Network forOrgan Sharing data suggest that among approximately400 new patients placed on the heart transplant waitinglist each month, only 150 to 200 patients are able to
From the Palo Alto Veterans Affairs Health Care System, Falk CardiovascularResearch Center, Stanford University School of Medicine.Submitted January 20, 1999; accepted June 27, 1999.Reprint requests:Michael B. Fowler, MD, The Falk Cardiovascular Research Center,Stanford University School of Medicine, Stanford, CA 96305.Copyright © 2000 by Mosby, Inc.0002-8703/2000/$12.00 + 0 4/1/101493
Congestive Heart Failure
Cardiopulmonary exercise testing and prognosis insevere heart failure: 14 mL/kg/min revisitedJonathan Myers, PhD, Lars Gullestad, MD, Randall Vagelos, MD, Dat Do, BS, Daniel Bellin, BS, Heather Ross, MD,and Michael B. Fowler, MD Stanford, Calif
Background Accurately establishing prognosis in severe heart failure has become increasingly important in assessingthe efficacy of treatment modalities and in appropriately allocating scarce resources for transplantation. Peak exercise oxy-gen uptake appears to have an important role in risk stratification of patients with heart failure, but the optimal cutpoint valueto separate survivors from nonsurvivors is not clear.
Methods Six hundred forty-four patients referred for heart failure evaluation over a 10-year period participated in thestudy. After pharmacologic stabilization at entrance into the study, all participants underwent cardiopulmonary exercise test-ing. Survival analysis was performed with death as the end point. Transplantation was considered a censored event. Four-year survival was determined for patients who achieved peak oxygen uptake values greater than and less than 10, 11, 12,13, 14, 15, 16, and 17 mL/kg/min.
Results Follow-up information was complete for 98.3% of the cohort. During a mean follow-up period of 4 years, 187patients (29%) died and 101 underwent transplantation. Actuarial 1- and 5-year survival rates were 90.5% and 73.4%,respectively. Peak ventilatory oxygen uptake (VO2) was an independent predictor of survival and was a stronger predictorthan work rate achieved and other exercise and clinical variables. A difference in survival of approximately 20% wasachieved by dichotomizing patients above versus below each peak VO2 value ranging between 10 and 17 mL/kg/min.Survival rate was significantly higher among patients achieving a peak VO2 above than among those achieving a peakVO2 below each of these values (P < .01), but each cutpoint was similar in its ability to separate survivors from nonsurvivors.
Conclusion Peak VO2 is an important measurement in predicting survival from heart failure, but whether an optimal cut-point exists is not clear. Peak VO2 may be more appropriately used as a continuous variable in multivariate models to pre-dict prognosis in severe chronic heart failure. (Am Heart J 2000;139:78-84.)

American Heart JournalVolume 139, Number 1, Part 1 Myers et al 79
both the recent Bethesda Task Force recommendationson recipient priority18 and the American Heart Associa-tion Scientific Statement on Cardiac Transplantation.19
Previous studies have generally made dichotomouscomparisons, such as above versus below 14 or 15mL/kg/min, above and below 10 mL/kg/min, and above14 versus below 10 mL/kg/min. To our knowledge,there have been no direct comparisons between differ-ent values for peak VO2 within the relevant range inthis population. To determine the optimal peak VO2criteria for stratifying risk among patients with severeheart failure, we performed this study.
MethodsPatients
The study group included 644 ambulatory patients withadvanced heart failure referred for evaluation at Stanford Uni-versity. The duration of heart failure was at least 1 month, andmost of the patients had one or more hospital admissions fordecompensated heart failure. Evaluation included a historyinterview, cardiovascular examination, and a maximal exer-cise test with ventilatory gas exchange analysis. Standard med-ical treatment, including digoxin, diuretics, and angiotensin-converting enzyme (ACE) inhibitors was administered. Manypatients were taking warfarin (46%), antiarrhythmic agents(23%), or a β-blocking agent, usually metoprolol. All patients’conditions were stabilized clinically before exercise testing,right heart catheterization, and echocardiography.
Exercise testingSymptom-limited maximal exercise tests were performed
upright on an wording ergometer at a constant cadence of 60rpm. A continuous ramp protocol was used in which workrate was increased by 10 W/min. VO2 was measured with a
Medical Graphics Corporation 2001 system (St Paul, Minn).Gas exchange data were obtained breath by breath andrecorded every 30 seconds. Oxygen uptake, carbon dioxideproduction, minute ventilation, and respiratory exchangeratio were calculated on line. Peak oxygen uptake wasdefined as the highest VO2 achieved during exercise. The ven-tilatory threshold was determined by two experiencedreviewers (J.M. and L.G.) using the V-slope method and con-firmed with ventilatory criteria. Heart rate was recorded con-tinuously from an electrocardiogram, and blood pressure wasrecorded at regular intervals throughout the test with a semi-automated recorder (Quinton STBP-680; Quinton Instruments,Seattle, Wash).
Follow-up data collectionFollow-up assessment was conducted at the Stanford Heart
Failure Clinic or by referring physicians. Patient status wasdetermined from medical records, by telephone interviewwith patient or family, or by an information resource researchservice (IRSC, Fullerton, Calif). Follow-up information couldnot be obtained for 12 patients (1.7%). The analysis was per-formed with death as the end point; transplantation was con-sidered a censored event.
Statistical analysisData were expressed as mean ± SD or as otherwise stated.
A Cox proportional hazards model was used to determine theeffect of a given independent variable on time to death. Thefollowing variables were included in the model: peak VO2,pulmonary capillary wedge pressure, left ventricular end-dias-tolic dimensions, ejection fraction, resting cardiac index, rest-ing heart rate and resting systolic blood pressure, peak heartrate and peak systolic blood pressure, VO2 at the ventilatorythreshold, heart rate at the ventilatory threshold, peak wattsachieved, VO2 as a percentage of age-predicted maximum,
Characteristic Finding
No. of patients 644Age (y) 48.5 ± 11.2Sex (M/F) 514 (80%)/130 (20%)Cause of heart failure
Coronary artery disease 221 (34%)Idiopathic dilated cardiomyopathy 383 (59%)Other 40 (6%)
MedicationDigoxin 360 (76%)Diuretics 388 (82%)ACE inhibitor 380 (80%)Warfarin 221 (46%)Antiarrhythmic 109 (23%)β-Blocker 58 (12%)
Follow-up (mo) 47.2 ± 28.3Death 187 (29%)Alive 457 (71%)No. who underwent transplantation 104 (16%)
Data are presented as mean and SD or number and percentage.ACE, Angiotensin-converting enzyme.
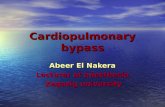
Table I. Baseline clinical characteristics of the study population Figure 1
ROC curves for 3-year survival. Area under curve was signifi-cantly greater for peak VO2 than for age and ejection fraction(P < .05).

American Heart JournalJanuary 2000Myers et al80
and VO2 greater than 14 mL/kg/min or 14 mL/kg/min orless. Time to event was coded in days. Differences in sur-vival rates between patients achieving greater than or lessthan a given peak VO2 value (above versus below 10, 11,12, 13, 14, 15, 16 and 17 mL/kg/min) were assessed with χ2
analysis. Receiver operating characteristic (ROC) curves(NCSS, Kaysville, Utah) were constructed by means of plot-ting true-positive rates (sensitivity) against false-positiverates (1-specificity) to compare survival among clinical,exercise, and hemodynamic variables.
ResultsBaseline characteristics
Descriptive characteristics of the study population arepresented in Table I. Eighty percent of the patients weremen, and idiopathic dilated cardiomyopathy was thepredominant underlying etiologic factor (59%). Despiteoptimal medical treatment, all patients had symptomaticheart failure with a marked decrease in ventricular func-tion as evidenced by a mean ejection fraction of 19.6% ±9.6%, a peak oxygen uptake of 16.1 ± 5.7 mL/kg/min, andechocardiographic data demonstrating ventricularenlargement with decreased fractional shortening.Eighty percent of the patients were treated with an ACEinhibitor, 76% with digoxin, and 82% with diuretics. Afterinitial examination, 225 (34.9%) patients were acceptedfor transplantation and put on the waiting list, whereas331 (51.4%) were rejected because they were too well,too sick, or too old (>60 years) or had pulmonary hyper-tension (systolic pulmonary arterial pressure >50 mm Hg)or other contraindications to transplantation.
Survival and transplantationDuring the follow-up period of 48.2 ± 28.3 months,
187 patients (29%) died. Actuarial 1- and 5- year sur-
vival rates were 90.5% and 73.4%, respectively. Ofthe patients listed for heart transplantation (n = 225),104 (16.1% of the total cohort) underwent transplan-tation (of these 34 died later), and 48 (7.5% of totalcohort) died while on the list. Of the patientsrejected from transplantation, 81 (12.6% of cohort)died later.
As a continuous variable, peak VO2 was a significantpredictor of death in multivariate analysis, yielding ahigher χ2 than all other clinical, hemodynamic, andexercise data. Figure 1 presents ROC curves withpeak VO2, age, and ejection fraction. The ROC areawas higher for peak VO2 (0.64) than for the othervariables (0.56 for age and 0.55 for ejection fraction; P< .05). Table II presents 3-year risk for death stratifiedaccording to peak VO2 value less than or equal to orgreater than 10, 11, 12, 13, 14, 15, 16, or 17mL/kg/min. A significant difference in survival ratewas observed among patients who achieved greaterthan versus less than each cutpoint (P < .001). Thedifferences ranged from 14% to 25% (for example, the3-year risk for death among patients achieving lessthan or equal to 14 mL/kg/min was 48%, whereas forthose achieving greater than 14 mL/kg/min the riskfor death was 23%).
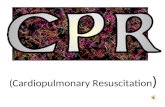
Figure 2 illustrates 3-year survival curves for patientsachieving peak VO2 values above versus below 10, 12,14, and 16 mL/kg/min. Whereas the survival rate washigher for patients achieving above versus below eachcutpoint at 1, 2, and 3 years, there was no advantageto using one cutpoint over another in terms of separat-ing survivors from nonsurvivors. Because of the waythe figure dichotomizes the groups, it may be mislead-ing to mix the cutpoints (eg, <16 vs 10 or moremL/kg/min).
Peak VO2 Percentage risk for(mL · kg · min) No. of patients No. of deaths dying in 3 years 95% CI
≤10 69 37 54 42-66>10 573 177 31 27-35≤11 102 50 49 39-59>11 540 164 30 26-34≤12 146 72 49 41-57>12 496 142 29 25-33≤13 198 99 50 43-57>13 444 115 26 22-30≤14 268 128 48 42-54>14 374 86 23 19-27≤15 318 45 46 40-52>15 324 69 21 16-26≤16 367 159 43 38-48>16 275 55 20 15-25≤17 425 172 40 35-45>17 217 42 19 14-24
All differences (above vs below each VO2 level) were significant (P < .001).
Table II. Risk for death based on peak VO2 achieved

American Heart JournalVolume 139, Number 1, Part 1 Myers et al 81
DiscussionThe shortage of donor hearts for patients with severe
heart failure has resulted in prolonged waiting times formost patients on lists for heart transplantation. Theaddition of peak VO2 measurements to other clinicaldata has been suggested for more accurate stratificationof risk among patients with severe chronic heart failureand might help determine which patients should con-tinue medical therapy or undergo transplantation.Specifically, a peak exercise VO2 value of 14mL/kg/min has become a recognized cutpoint for con-sideration for transplantation.11,13,17-19 This number isbased on data that indicate that a value of ≤14mL/kg/min identifies patients with an extremely poorshort-term prognosis.11,13,16,17,20 An exercise limitationto this degree also has been associated with poor out-comes among patients with stable coronary artery dis-ease.21
In general, previous studies of survival in patientswith severe heart failure have been limited by short fol-low-up periods (usually ranging from less than 1 up to 2years), and the number of end points tends to be small(frequently ranging from less than 10 to approximately
30). After stratification according to VO2 level or otherclinical factors, there have frequently been fewer than10 deaths per subgroup over 1 to 2 years in previousstudies. To increase the number of end points, manystudies have included end points other than death,such as change in listing status for transplantation ortransplantation. Because a change in listing status issubjective, and transplantation and other events changethe natural history of the disease, they result in“chronology bias”22 and are generally not considered tobe appropriate end points in the context of epidemio-logic research. Relative to those from previous studies,our data provide a more robust model with which toassess the role of cardiopulmonary exercise testing insurvival among patients with heart failure. The inclu-sion of patients evaluated for heart failure over a 10-year period allowed a considerably larger number of“hard” end points (deaths), and a longer mean follow-up period (4 years).
Although the use of a cutpoint such as 14 mL/kg/minis inherently attractive to clinicians, it has several limita-tions. First, it is often difficult to separate a givenpatient’s true cardiopulmonary limits from motivation
Figure 2
Survival curves for patients achieving peak VO2 values above versus below 10, 12, 14, and 16 mL · kg · min.

American Heart JournalJanuary 2000Myers et al82
or deconditioning, particularly in a population ofpatients with severe heart failure. Second, althoughstratifying patients above and below 14 mL/kg/min hasdemonstrated marked differences in survival, so havevalues above versus below 10 mL/kg/min,1,11,16,23 11mL/kg/min,24 12 mL/kg/min,25 13 mL/kg/min,26 15mL/kg/min,21 and a variety of exercise tolerance valuespredicted from exercise workload or time.27-29 Third,dichotomizing data in this way tends to oversimplify aclinical issue by forcing patients into one of two cate-gories, minimizing the ability to carefully study those inthe most clinically relevant range of interest, in this case,10 to 15 mL/kg/min. Moreover, not all studies havefound 14 mL/kg/min to be particularly sensitive for sepa-rating survivors from nonsurvivors.14,30,31 Two recentstudies have suggested that peak VO2 has limited prog-nostic value within this range, that is, 10 to 18mL/kg/min31 and 12 to 17 mL/kg/min.32 Peak VO2 wasstrongly associated with mortality only among patientsachieving values below the lower limit and strongly pre-dicted survival among those achieving above the higherlimit. Finally, peak VO2 may not reliably identify severehemodynamic dysfunction during exercise.33
Our data suggest that the commonly used peak VO2cutpoint of 14 mL/kg/min is not superior to other cut-points ranging between 10 and 17 mL/kg/min.Although each of these values significantly separatedsurvivors from nonsurvivors (Table II, Figure 2), theredid not appear to be any benefit to using one cutpointover another in terms of stratifying risk for death over amean follow-up period of 4 years. Table II suggests thatan improvement in survival of approximately 20%occurs for a patient achieving a high compared with alow peak VO2 value irrespective of the cutpoint used.Although this gain in the estimation of survival is sub-stantial, and one that is achieved with a relatively inex-pensive, noninvasive test, it is not as great a differenceas that reported in other studies.11,13,16 Mancini et al11
reported 94% and 47% 1-year survival rates for patientsachieving above versus below 14 mL/kg/min, respec-tively (a 47% difference). Roul et al13 reported that all 9deaths that occurred over 1 year in a small cohort ofpatients with chronic heart failure occurred amongthose achieving 14 mL/kg/min or less (a survival rate of71%). No patient died who achieved more than 14mL/kg/min. Although population differences no doubtexplain much of the differences observed in these stud-ies, cumulatively they suggest that directly measuredpeak VO2 has an important place in stratifying riskamong patients with chronic heart failure.
Another noteworthy finding is that our data confirmthe improving survival rate among patients with severechronic heart failure in the 1990s.1 Even among patientsachieving less than 10 mL/kg/min, 46% were alive at 3years (Table II). The higher survival rates among patientswith chronic heart failure in recent years have been
attributed to therapeutic advances such as more vigor-ous reduction of filling pressures, broader use of ACEinhibitors, and avoidance of type I antiarrhythmicagents.34-37 Our survival rate is comparatively high evenrelative to those in follow-up studies performed in themodern treatment era. Stevenson et al1 reported a 2-yearsurvival rate of 48% for patients achieving a peak VO2less than or equal to 10 mL/kg/min, which contrasts the70% 2-year survival rate among the patients in our study.The higher survival rate among our patients might alsobe explained by the fact that not all were in New YorkHeart Association class IV and by the philosophy of ther-apeutic rigor at our institution beginning in the late1980s.38 These higher survival rates starkly contrastthose published in the 1980s even among patients withless severe heart failure. In a 1985 study, Szlachcic et al23
reported that only 23% of patients achieving a peak VO2<10 mL/kg/min survived 1 year. The overall 1-year mor-tality was 40%, similar to that in other studies from theearly 1980s involving patients with severe chronic heartfailure.39-42
LimitationsThis study was a retrospective assessment of patients
consecutively referred for evaluation of heart failure,and the philosophy of treatment of patients with thiscondition has evolved over the 10-year period of evalu-ation. Because there has been so much discussionabout peak VO2 measurements in this context in the1990s, we limited the focus of the analysis to this vari-able. Numerous other variables clearly influence prog-nosis in chronic heart failure.15,19,20,43 Multivariatemethods, including Cox hazard function techniquesthat address a wide variety of clinical, hemodynamic,and exercise data have been used in recent years byour group14,25,38,44 and others.1,11,12,20
The survival rate was comparatively high in our pop-ulation, which may reflect the fact that patients“referred for heart failure evaluation” were a low riskgroup. Thus the results may not necessarily be applica-ble to those seen at other centers. Our values for peakVO2 were obtained with a cycle ergometer. Becausepeak VO2 is generally higher with a treadmill, theseresults should be considered applicable only to patientswho undergo testing on a cycle ergometer. Finally,whereas most of the patients in our cohort wereobserved at Stanford (approximately 90%), some werereferred from the other parts of the western UnitedStates, and we did not have detailed information oncontinued use of ACE inhibitors, β-blockers, or othertreatments of these patients.
SummaryThe results of this study confirm our previous find-
ings14,25,44 and those of others1,11-13,15-20,24,26 regardingthe value of peak VO2 in stratifying risk among patients

American Heart JournalVolume 139, Number 1, Part 1 Myers et al 83
with severe heart failure. Measurement of VO2 shouldbe included in clinical evaluations of patients withchronic heart failure to optimize the therapeutic strat-egy. However, we did not find a specific peak VO2value that was superior to any other. Over a 4-year fol-low-up period, a difference in survival rate of approxi-mately 20% was achieved by dichotomizing patientsabove versus below peak VO2 values ranging from 10to 17 mL/kg/min. These data suggest that an optimalcutpoint for predicting survival may not exist and thatpeak VO2 should be considered a continuous variablein a multivariate model to predict prognosis in severe,chronic heart failure.
References1. Stevenson LW, Couper G, Natterson B, et al. Target heart failure popu-
lations for newer therapies. Circulation 1995;92 suppl II:II-174-II-181.2. Bourassa MG, Gurne O, Bangdiwala SI, et al. Natural history and
patterns of current practice in heart failure. J Am Coll Cardiol 1993;22 suppl A:9A-14A.
3. Garg R, Packer M, Pitt B, et al. Heart failure in the 1990’s: evolu-tion of a major public health problem in cardiovascular medicine. JAm Coll Cardiol 1993;22:3A-5A.
4. Hosenpud JD, Novick RJ, Breen TJ, et al. The Registry of the Interna-tional Society for Heart and Lung Transplantation: eleventh officialreport. J Heart Lung Transplant 1994;13:561-70.
5. Marzo KP, Wilson JR, Mancini DM. Effects of cardiac transplantationon ventilatory response to exercise. Am J Cardiol 1992;69:547-53.
6. Giverz MM, Hartley LH, Colucci WS. Long-term sequential changesin exercise capacity and chronotropic responsiveness after cardiactransplantation. Circulation 1997;96:232-7.
7. Osada N, Chaitman BR, Donohue TJ, Wolford TL, Stelken AM,Miller LW. Long-term cardiopulmonary exercise performance afterheart transplantation. Am J Cardiol 1997;79:451-6.
8. Kobashigawa JA, Leaf DA, Lee N, Gleeson MP, Liu H, HamiltonMA, et al. A controlled trial of exercise rehabilitation after hearttransplantation. N Engl J Med 1999;340:272-7.
9. Badenhop, DT. The therapeutic role of exercise in patients with ortho-topic heart transplant. Med Sci Sports Exerc 1995;27:975-85.
10. 1998 report of center-specific organ acceptance rates. [UnitedNetwork for Organ Sharing Transplantation information Web site].Available at: www.unos.org
11. Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH, Wilson JR.Value of peak exercise oxygen consumption for optimal timing ofcardiac transplantation in ambulatory patients with heart failure.Circulation 1991;83:778-86.
12. Stelken AM, Younis LT, Jennison SH, et al. Prognostic value of car-diopulmonary exercise testing using percent achieved of predictedpeak oxygen uptake for patients with ischemic and dilated cardiomy-opathy. J Am Coll Cardiol 1996;27:345-52.
13. Roul G, Moulichon ME, Bareiss P, et al. Exercise peak VO2 deter-mination in chronic heart failure: is it still of value? Eur Heart J1994;15:495-502.
14. Myers J, Gullestad L, Vagelos R, Do D, Bellin D, Ross H, et al. Clini-cal, hemodynamic, and cardiopulmonary exercise test determinantsof outcome in patients referred for evaluation of heart failure. AnnIntern Med 1998;129:28-93.
15. Myers J, Gullestad L. The role of exercise testing and gas exchange
measurement in the prognostic assessment of patients with heartfailure. Curr Opin Cardiol 1998;13:145-55.
16. Aaronson KD, Mancini DM. Is percentage of predicted maximalexercise oxygen consumption a better predictor of survival thanpeak exercise oxygen consumption for patients with severe heartfailure? J Heart Lung Transplant 1995;14:981-9.
17. Pina IL. Optimal candidates for heart transplantation: is 14 the magicnumber? J Am Coll Cardiol 1995;26:436-7.
18. Mudge GH, Goldstein S, Addonizio LJ, et al. Twenty-fourth Bethesdaconference: cardiac transplantation—Task Force 3, recipient guide-lines/prioritization. J Am Coll Cardiol 1993;22:21-31.
19. Costanzo MR, Augustine S, Bourge R, et al. Selection and treatment ofcandidates for heart transplantation. Circulation 1995;92:3593-612.
20. Cohn JN, Johnson GR, Shabetai R, et al. Ejection fraction, peakexercise oxygen consumption, cardiothoracic ratio, ventriculararrhythmias, and plasma norepinephrine as determinants of prog-nosis in heart failure. Circulation 1993;87 Suppl VI-5–VI-16.
21. Vanhees L, Fagard R, Thijs L, Staessen J, Amery A. Prognostic sig-nificance of peak exercise capacity in patients with coronary arterydisease. J Am Coll Cardiol 1994;23:358-63.
22. Feinstein AR. Clinical Biostatistics; XI: sources of “chronology bias”in cohort statistics. Clin Pharmacol Ther 1971;12:864.
23. Szlachcic J, Massie BM, Kramer BL, Topic N, Tubau J. Correlatesand prognostic implication of exercise capacity in chronic conges-tive heart failure. Am J Cardiol 1985;55:1037-42.
24. Saxon LA, Stevenson WG, Middlekauff HR, et al. Predicting deathfrom progressive heart failure secondary to ischemic or idiopathicdilated cardiomyopathy. Am J Cardiol 1993;72:62-5.
25. Haywood GA, Rickenbacher PR, Trindade PT, et al. Analysis ofdeaths in patients awaiting heart transplantation: impact on patientselection criteria. Heart 1996;75:455-62.
26. Likoff MJ, Chandler SL, Kay HR. Clinical determinants of mortal-ity in chronic congestive heart failure secondary to idiopathicdilated or to ischemic cardiomyopathy. Am J Cardiol 1987;59:634-8.
27. Gradman A, Deedwania P, Cody R, et al. Predictors of total mortalityand sudden death in mild to moderate heart failure. J Am CollCardiol 1989;14:564-70.
28. Morris CK, Ueshima K, Kawaguchi T, Hideg A, Froelicher VF. Theprognostic value of exercise capacity: a review of the literature.Am Heart J 1991;122:1423-31.
29. Madsen BK, Hansen JF, Stokholm KH, Brons J, Husum D, Mortensen.Chronic congestive heart failure: description and survival of 190consecutive patients with a diagnosis of chronic congestive heartfailure based on clinical signs and symptoms. Eur Heart J 1994;15:303-10.
30. Chomsky DB, Lang CC, Rayos GH, et al. Hemodynamic exercisetesting: a valuable tool in the selection of cardiac transplantationcandidates. Circulation 1996;94:3176-83.
31. Opasich C, Pinna GD, Bobbio M, Sisti M, DeMichelis B, Febo O,et al. Peak exercise oxygen consumption in chronic heart failure:toward efficient use in the individual patient. J Am Coll Cardiol1998;31:766-75.
32. Kao W, Winkel EM, Johnson MR, Piccione W, Lichtenberg R, Con-stanzo MR. Role of maximal oxygen consumption in establishmentof heart transplant candidacy for heart failure patients with interme-diate exercise tolerance. Am J Cardiol 1997;79:1124-7.
33. Wilson JR, Rayos G, Keoh TK, Gothard P. Dissociation betweenpeak exercise oxygen consumption and hemodynamic dysfunctionin potential heart transplantation candidates. J Am Coll Cardiol1995;26:429-35.

American Heart JournalJanuary 2000Myers et al84
34. Stevenson LW. Tailored therapy before transplantation for treatmentof advanced heart failure: effective use of vasodilators and diuret-ics. J Heart Lung Transplant 1991;10:468-76.
35. Fonarow GC. Chelimsky-Fallick C, Stevenson LW, et al. Effect ofdirect vasodilatation vs angiotensin-converting enzyme inhibition onmortality in advanced heart failure: the Hy-C Trial. J Am Coll Car-diol 1992;19:842-50.
36. The SOLVD Investigators. Effect of enalapril on survival in patientswith reduced left ventriclar ejection fractions and congestive heartfailure. N Engl J Med 1991;325:293-302.
37. Cardiac Arrhythmia Suppression Trial. Preliminary report: effect ofencainide and flecainide on mortality in a randomized trial ofarrhythmia suppression after myocardial infarction. N Engl J Med1989;321:406-12.
38. Rickenbacher PR, Trindade PT, Haywood GA, et al. Transplantcandidates with severe left ventricular dysfunction managed withmedical treatment: characteristics and survival. J Am Coll Cardiol1996;27:1192-7.
39. Wilson JR, Schwartz JS, Sutton M, et al. Prognosis in severe heartfailure: relation to hemodynamic measurements and ventricularectopic activity. J Am Coll Cardiol 1983;2:403-10.
40. Franciosa JA, Wilen M, Ziesche S, Cohn JN. Survival in men withsevere chronic left ventricular failure due to either coronary heartdisease or idiopathic dilated cardiomyopathy. Am J Cardiol 1983;51:831-6.
41. Stevenson LW, Fowler MB, Schroeder JS, Stevenson WG, DracupKA, Fond V. Poor survival of patients with idiopathic cardiomyopathyconsidered too well for transplantation. Am J Med 1987;83:871-6.
42. Unverforth DV, Magorien RD, Moeschberger ML, Baker PB, FettersJK, Leier CV. Factors influencing the one-year mortality of dilatedcardiomyopathy. Am J Cardiol 1984;54:147-52.
43. Francis GS. Determinants of prognosis in patients with heart failure.J Heart Lung Transplant 1994;12:S113-S116.
44. Gullestad L, Myers J, Ross H, et al. Serial exercise testing and prog-nosis in selected patients considered for cardiac transplantation.Am Heart J 1998;135:221-9.
AVAILABILITY OF JOURNAL BACK ISSUES
As a service to our subscribers, copies of back issues of the American Heart Journal for the preceding 5 years are maintainedand are available for purchase from Mosby until inventory is depleted. The following quantity discounts are available: 25% offon quantities of 12 to 23, and one third off on quantities of 24 or more. Please write to Mosby, Inc., Subscription Services,11830 Westline Industrial Drive, St. Louis, MO 63146-3318, or call (800)453-4351 or (314)453-4351 for information onavailability and prices of particular issues. If unavailable from the publisher, photocopies of complete issues may be purchasedfrom Bell & Howell Information and Learning, 300 N. Zeeb Rd., Ann Arbor, MI 48106, (734)761-4100 or (800) 521-0600.