Cardiac valve disorders

of 46
-
Upload
svc-student -
Category
Documents
-
view
216 -
download
0
Transcript of Cardiac valve disorders
-
7/29/2019 Cardiac valve disorders
1/46
12/17/20
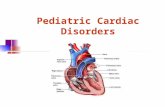
Septal Defects
Chapter 29 (Brunner)
Chapter 41 (Pillitteri: 1206-14)
Septal Defects
Congenital Heart Disorders
Management of Pts with Complications from Heart Disease
Chapter 30 (Brunner)
HF, Pulmonary Edema, Cardiogenic Shock, Pulmonary Emboli,
Pericardial Effusion, Cardiac Tamponade, & Sudden CardiacDeath/Cardiac Arrest
Outline1. d Pulmonary Blood Flow (Acyontic Defect)
1. Septal Defects
1. Ventricular Septal Defect (VSD)
2. Atrial Septal Defect (ASD)
2. Atrioventricular Canal Defect
3. Patent Ductus Arterious
2. d pulmonary blood flow (cyanotic defect)
1. Tetralogy of Fallot
3. Obstruction of Blood Flow
1. Aortic Stenosis
2. Pulmonary Stenosis
3. Coartation of Aorta
4. Cyanotic Defects (Mixed blood flow)
1. Transposition of Great Vessels
2. Tetralogy of Fallot (also falls under
category of d pulmonary blood flow)
-
7/29/2019 Cardiac valve disorders
2/46
12/17/20
Question
Meena was born with a ventricular septal
defect. A chief concern that parents of
children with heart disease often report is:
a) infant is gaining weight rapidly.
b) the baby always seems hungry.
c) she seems to have trouble sucking.
d) their babys face appears pale.
d Pulmonary Blood FlowAcyontic Defects
-
7/29/2019 Cardiac valve disorders
3/46
12/17/20
Septal Defects
Chapter 29 (Brunner)
Chapter 41 (Pillitteri)
Atrial or ventricular septum has abnormal opening b/t right & left side of heart
Most septal defects are
Congenital
Repaired during infancy or childhood
Adults may develop septal defects as a result of MI or trauma
Symptoms
May not experience symptoms
Or may gradually develop symptoms
Or may rapidly develop heart failure
Types
d pulmonary blood flow
Obstruction of blood flow
Mixed blood flow
d pulmonary blood flow
Septal DefectsBrunner Chapter 29
Atrial septal defect (ASD)
Right atrial pressures become >than left atrial pressures
Blood begins to flow from rightatrium into left atriuma right-to-left shunt
Symptoms gradually develop
d exercise tolerance
DOE Palpitations
Syncope
Symptoms of rightventricular or CHF
May cause cyanosis
May cause CVA
Ventricular septal defect (VSD)
Extra blood volume causes rightventricle to dilate
Also causes pulmonary vascularcongestion & HTN
Symptoms gradually develop
SOB
Syncope
Chest pain
Symptoms of left ventricularfailure
-
7/29/2019 Cardiac valve disorders
4/46
12/17/20
Septal Defects
Brunner Chapter 29 Septal DefectTreatment
Vasodilators
left-to-right shunting
s resistance to ventricular ejection
Septal Defect Repair
Percutaneous septal defect repair
Many septal defects can be repaired percutaneously in cardiac cath lab
Post-op care
Same care as post-procedure cardiac cath or PTCA
Pt remains in the hospital for 24 to 48 hours
Surgical septal defect repair
Post-op care
Same as other cardiac surgeries
d Pulmonary Blood FlowAcyontic Defects
Ventricular Septal Defect (acyanotic)
Opening is present in septum b/t two ventricles
Blood gets shunted from left ventricle, across septum,to right ventricle
2 pressure > left ventricle than right ventricle
Refer to next slide
Assessment
May not evident at birth
Usually evident at about 4 to 8 wks Baby becomes easily fatigued when shunting begins
Has abnormal murmur as opposed to functional innocent murmur
Abnormal murmur associated with VSD
Loud, harsh systolic murmur
Heard along left sternal border (at 3rd or 4th intercostal space)
Murmur may be palpable (has thrill vibration)
Functional innocent heart murmurs
Normal heart sounds heard in children
Made as blood flows through the heart
-
7/29/2019 Cardiac valve disorders
5/46
12/17/20
d Pulmonary Blood Flow
Acyontic Defects
Ventricular Septal Defect (cont)
Ineffective tissue perfusion r/t inefficiency of heart as a pump
Treatment
Must be closed (2 can cause HF)
Can cause right ventricular hypertrophy & d pulmonary artery pressure
2 blood is getting shunted back into pulmonary circulation instead ofgoing out of aorta & to body
85% of VSDs are so small they close spontaneously
Moderate sized VSD are closed by cardiac catheterization
Large sized VSD are closed by open-heart surgery
Requires general anesthesia & cardiopulmonary bypass
Ventricular septal defect is occluded by using a Silastic or Dacron patch As time passes, babys septal tissue will grow across synthetic patch
Prophylactic antibiotics for 6 months to prevent bacterial endocarditis
May participate in normal activities after surgery as long as withoutcomplications
Acyanotic defectsd pulmonary blood flow
Atrial Septal Defect (ASD)
Abnormal opening b/t two atria
Blood ends up shifting from left (oxygenated)
atrium to right (deoxygenated) atrium
2 stronger contraction of left side of heart
Adverse Side Effects
d volume in right side of heart
Inventricular hypertrophy
d pulmonary artery blood flow (like VSD)
-
7/29/2019 Cardiac valve disorders
6/46
12/17/20
d pulmonary blood flow
Atrial Septal Defect (ASD) Atrial Septal Defect (ASD) cont
Assessment
Harsh systolic murmur over 2nd or 3rd intercostal space (around pulmonic area)
2 can hear extra blood being shunted across pulmonic valve
This causes pulmonic valve to close later than aortic valve [AKA a split S2]
Fixed splinting of 2nd heart sound is indicative of ASD
Treatment
Elective surgery
Needs to be done b/t 1 3 y/o
2 must be closed b/c baby isat risk for infectious endocarditis & HF
Women are at risk for emboli during pregnancy Closed by:
(1) Cardiac catheterization
or (2) Open-heart surgery(Silastic or Dacron patch to occlude space)
d Pulmonary Blood Flow
Acyontic Defects
1. Ventricular Septal Defect (VSD)
2. Atrial Septal Defect (ASD)
3. Atrioventricular Canal Defect
4. Patent Ductus Arterious
Atrioventricular canal defect
Example
-
7/29/2019 Cardiac valve disorders
7/46
12/17/20
d pulmonary Blood Flow
Acyontic Defects
Atrioventricular Canal Defect
AKA endocardial cushion defect
Incomplete fusion of endocardialcushion
This is where septum of heartjoins junction of atria & ventricles
AEB low ASD & high VSD; &distorted mitral & tricuspid valves
Blood flow is left-to-right, but mayflow b/t all 4 heart chambers
Approximately 50% of children withtrisomy 21 (Down syndrome) whohave heart disease have this type ofcongenital cardiac defect
d pulmonary Blood FlowAcyontic Defects
Atrioventricular Canal Defect cont
Assessment
ECG often shows 1st -degree heart block
2 impulse is halted before AV node
Symptoms
Same as ASD:
(1) right ventricular hypertrophy
(2) d pulmonary blood flow
(3) fixed S2 splitting
Treatment:
Surgery is always necessary
2 defects are too large to close spontaneously
Requires septal repair & possibly valve repair
Hence, may need prophylactic anticoagulation & antibiotics
-
7/29/2019 Cardiac valve disorders
8/46
12/17/20
d pulmonary Blood Flow
Acyontic Defects
Ductus arterious
An accessory fetal structure that connects pulmonary artery to aorta
Allows babys lungs to be bypassed
Begins to close at birth with 1st breath
Completely closes b/t 7-14 days old
Prostaglandins
when baby begins to breath on own
2 oxygen levels make ductus arteriosus close
d incidence in babies born at higher altitudes
Patent Ductus Arteriosus
Ductus arteriosus fails to close 2 babys prostaglandin levels fail to
d pulmonary Blood FlowAcyontic Defects
Patent Ductus Arteriousus cont
Pathophyiology
Blood gets shunted from aorta(oxygenated blood) topulmonary artery (deoxygenatedblood)
2 to d pressure in aorta
From pulmonary artery
Blood then goes to lungs, topulmonary vein, & thenback to left atrium, to leftventricle, & back to aorta
Hence, blood never makesit out to body
It just continues to getshunted throughpulmonary artery, & thecycle continues
-
7/29/2019 Cardiac valve disorders
9/46
12/17/20
d pulmonary Blood Flow
Acyontic Defects Patent Ductus Arteriousus cont
Adverse Effects
d pressure in pulmonary circulation r/textra shunted blood
Results in right ventricle hypertrophy
Assessment
(1) Widened pulse pressure
(2) Continuous (systolic & diastolic)machinery murmur
Heard at upper left sternal border
Or under left clavicle in older children
Treatment
Prostaglandin Inhibitors
IV indomethacin or ibuprofen
Ibuprofen is becoming drug of choice2 has fewer SEs
Question
Which happening makes an infant high risk for
patent ductus arteriosus?
a) Infant had difficulty beginning respirations.
b) Infants mother had an epidural block for labor.
c) Infants father worked at a sedentary desk job.d) Infants mother had an infection during
pregnancy.
-
7/29/2019 Cardiac valve disorders
10/46
12/17/20
Obstruction of Blood Flow Defects
1. Aortic Stenosis
2. Pulmonary Stenosis
3. Coartation of Aorta
4. Cyanotic Defects (Mixed blood flow)
1. Transposition of Great Vessels
2. Tetralogy of Fallot
1. Also falls under category of
d pulmonary blood flow
Obstruction of Blood Flow Coarctation of the Aorta
Narrowing of aortas lumen
2 constricting band
Blood has difficulty passing through
narrowed aorta lumen
Results in BP changes
d BP proximal (close) to coarctation
AEB d BP in heart & upper portions of childs body
& d BP distal to coarctation
Assessment d upper-body BP causes HA & vertigo
But, baby cant tell you
Hence, S&S: irritability, epistaxis, & possible CVA (for dangerouslyd BP)
BP in arms
At least 20 mm Hg > legs (reversal of normal pattern)
For slight coarctation
Absent palpable femoral pulses may be the only symptom
Hence, newborn femoral pulses are always assessed
-
7/29/2019 Cardiac valve disorders
11/46
12/17/20
Obstruction of Blood Flow
Coarctation of the Aorta
Treatment
Digoxin & diuretics
2 CHF from HTN
Angiography (a balloon catheter)
Surgery
Narrowed portion of aorta is removed & new ends of aorta areanastomosed
Usually occurs before 2 y/o
But, ideal situation would be to operate on adult height
2 prevents strain on incision line as they grow
Girls need to have surgery before childbearing age 2 extra blood volume during pregnancy can cause HF
If surgery is successful, child can expect to live a normal life
Questions
1. If an infant were born with coarctation of the aorta, thisproduces few symptoms at first. An important finding to assess tobest suggest this exists isa) excessive sleeping and crying.
b) presence of a cardiac murmur.
c) elevated body temperature.
d) lack of both femoral pulses.
2. Which of the following is a symptom of coarctation of aorta thata school nurse might notice when the child reaches school age?a) Pain in the legs on physical exercise
b) An especially short attention span
c) Eating little lunch from lack of appetite
d) Abdominal bloating and chronic pain
-
7/29/2019 Cardiac valve disorders
12/46
12/17/20
Obstruction of Blood Flow
To be covered in Brunner Chapter 29
Cyanotic Defects
Mixed blood flow
1. Transposition ofGreat Vessels
2. Tetralogy ofFallot
-
7/29/2019 Cardiac valve disorders
13/46
12/17/20
Cyanotic Defect
Mixed blood flow
Transposition of Great Vessels Severe defect that is incompatible with life
Baby is usually cyanotic at birth
Aorta arises from right ventricle instead of left
Pulmonary artery arises from left ventricle instead of
right
Blood flow
Comes into heart from vena cava to right atrium
To right ventricle
Then to aorta (instead of pulmonary artery)
Hence, blood goes out to body completely deoxygenated
There is an existence of a second closed circulatory system
Sp, blood enters heart from pulmonary veins to left atrium
To left ventricle, to pulmonary artery, to lungs to be oxygenated & returns to
left atrium
So, b/c of this closed circulatory system, none of this oxygenated blood ever
makes it out to body
Cyanotic DefectMixed blood flow
Transposition of the Great Vessels
Treatment
Need to get blood to lungs Prostaglandins
2 to keep ductus arteriosus patent Creation of artifical atrial septal defect
2 allows deoxygenated blood to getto lungs for oxygenation
In most cases, baby has an atrial& ventriclular septal defect, aswell as the transposed vessels
Hence, some of deoxygenatedblood is getting oxygenated
Surgical correction of transposed greatvessels
Surgery is done to separate the greatvessels
Performed when baby is about 1 to 3months of age
-
7/29/2019 Cardiac valve disorders
14/46
12/17/20
Question
Suppose an infant had been born with
transposition of the great vessels so the baby
was prescribed ibuprofen. The purpose of this
medication is to
a) increase blood pressure to reverse blood flow.
b) increase the strength of atrial contractions.
c) decrease and strengthen the heart rate.
d) keep the ductus arteriosus from closing.
d pulmonary Blood Flow
Tetralogy of Fallot
-
7/29/2019 Cardiac valve disorders
15/46
12/17/20
d pulmonary blood flow
Tetralogy of Fallot
Tetralogy of Fallot
Consists of 4 anomalies
1. Pulmonary stenosis
Causes d pressure in right side of heart
Causes blood to be shunted from right side of heart to left ventricle (via
VSD)
Systolic murmur (heard at left 2nd, 3rd, or 4th intercostal space)
& then out through overriding aorta
2. Hypertrophy of right ventricle
Caused by d force to push blood through stenosed pulmonary artery3. VSD (usually large)
Systolic murmur (heard at left 2nd, 3rd, or 4th intercostal space)
4. Dextroposition (overriding) of aorta
Many children with Tetralogy of Fallot have deletion abnormality of chromosome 22
Tetralogy of FallotAssessment
Squatting in knee-chest position
2 overstressed heart is relieved
Squatting
Traps blood in lower extremities
Helps trapped blood supply oxygen to major body organs
Cyanosis
May not be evident immediately after birth
But, as become more active, skin has bluish tint
Clubbing
Child develops severe dyspnea, growth restriction, & clubbing of the fingers Syncope (fainting) & hypercyanotic episodes
AKA tet spells
2 d blood flow & oxygen to brain (risk for cognitive defects)
Polycythemia (d RBCs)
2 helps supply body with extra oxygen
This is dangerous 2 causes thickening of blood (d viscosity)
Risk for clot; thrombophlebitis, embolism, & CVA
Systolic murmur
Heard at left 2nd, 3rd, or 4th intercostal space
Polycythemia
Systolic
murmur
-
7/29/2019 Cardiac valve disorders
16/46
12/17/20
Tetralogy of Fallot
Blalock-Taussig Procedure
Temporary surgery
2 Tetralogy of Fallot is not fully
corrected until child is 1-2 y/o
Need to correct, or will cause severe
dyspnea, growth restriction, &
clubbing of the fingers
Prior to surgery
hypercyanotic episodes
Give O2 for hypoxic episode
Place in kneechest position
To trap blood into LEs
Keeps heart from being
overwhelmed
Morphine sulfate
To symptoms
Tetralogy of Fallot
Blalock-Taussig Procedure
A shunt is created b/t aorta & pulmonary artery (it creates
a ductus arteriosus)
Allows blood to leave aorta & enter pulmonary artery to
oxygenate lungs
Blood then returns to left side of heart, to aorta, & out
to body
Uses subclavian artery Hence, at post-op, baby will have no palpable pulse in
right arm
Need to avoid all BPs & venipunctures to affected arm
Brock Procedure
Corrects pulmonary stensosis, VSD, & overiding aorta
Performed when child is old enough to have full surgery to
correct pulmonary stensosis, VSD, & overriding aorta
-
7/29/2019 Cardiac valve disorders
17/46
12/17/20
Question
1. Tetralogy of Fallot is the most frequently occurring type of cyanotic heart
disease. What are the four anomalies associated with this defect are:
a) atrial septal defect, pulmonary stenosis, left ventricular hypertrophy, and
overriding aorta.
b) ventricular septal defect, aortic stenosis, mitral stenosis, and right-sided
aorta.
c) mitral stenosis, right ventricular hypertrophy, pulmonary stenosis, and atrial
septal defect.
d) ventricular septal defect, pulmonary stenosis, right ventricular hypertrophy,
and overriding aorta.
2. Suppose an infant with Tetralogy of Fallot turns cyanotic and short of breath.
Your best action would be to:
a) put her head between her legs.
b) place her in a knee-chest position.
c) tell her to breathe into a paper bag.
d) sit her upright to lower blood pressure.
Questions
1. What is a common laboratory finding with children withcyanotic heart disease?a) Decreased platelet count
b) Elevated sedimentation rate
c) Elevated total red cell count
d) Elevate white blood count
2. The best place to assess if cyanosis is present in childrenis in thea) conjunctiva of the lower eyelid.
b) fingertips or toes for color.
c) circumoral area by the mouth.
d) tongue or buccal membrane.
-
7/29/2019 Cardiac valve disorders
18/46
12/17/20
Questions
1. A baby had a cardiac catheterization to diagnose congenitalheart disease. Following cardiac catheterization, which of thefollowing is the most important measure?a) Assessing the pressure dressing is intact
b) Assuring the baby the procedure is now over
c) Letting the baby adjust to room light gradually
d) Letting the baby kick and exercise her legs
2. Which nursing diagnosis would best apply to an infant withTetralogy of Fallot?a) Impaired gas exchange related to a left to right septal shunt
b) Impaired skin integrity related to consistent cyanosisc) Ineffective airway clearance related to a constricted aorta
d) Altered tissue perfusion related to pulmonary artery stenosis
Questions
1. An infant is prescribed digoxin. The action of digoxin is toa) increase the heart rate and dilate blood vessels.
b) slow heart rate and strengthen heart contractions.
c) decrease the amount of blood filling the ventricles.
d) stimulate angiotension to increase blood pressure.
2. What is the usually designated level of pulse rate considered safe
for administration of digoxin for a 6-month-old infant?a) 40 beats per minuteb) 60 beats per minute
c) 100 beats per minute
d) 150 beats per minute
-
7/29/2019 Cardiac valve disorders
19/46
12/17/20
Chapter 30
Managing Pts with
Complications from
Heart Disease
HF, Pulmonary Edema,
Cardiogenic Shock, PulmonaryEmboli, Pericardial Effusion,
Cardiac Tamponade, & Sudden
Cardiac Death/Cardiac Arrest
Heart Failure
Inability of heart to pump sufficient blood to meet needs of tissues for oxygen &
nutrients
Incidence of HF s with age
Most common in pts > 75 y/o
Most HF is a progressive, lifelong disorder managed with lifestyle changes &
meds
Recognized as a Syndrome AEB
Fluid overload
or inadequate tissue perfusion
2 heart cant generate sufficient CO to meet bodys demands
Ejection fraction (EF)
Assists in determining HF type
WNL EF is 55% to 65% of ventricular volume
2 ventricle does not completely empty b/t contractions
-
7/29/2019 Cardiac valve disorders
20/46
12/17/20
Heart Failure
2 major types of HF
Systolic heart failure
More common type
Characterized by altered ventricular contraction
Low EF is a hallmark of systolic HF
EF is < 55% to 65% of ventricular volume
Diastolic heart failure
Less common type
Characterized by stiff & noncompliant heart muscle
Makes it difficult for ventricle to fill
EF is normal
Heart Failure
Primary Cause
Atherosclerosis of coronary
arteries
in CO activates multiple
neurohormonal mechanisms
Results in S&S of HF
Compensatory mechanisms of HF
AKA vicious cycle of HF
-
7/29/2019 Cardiac valve disorders
21/46
12/17/20
Heart Failure Symptoms Left-sided HF
Pulmonary congestion Occurs when left ventricle cant effectively pump blood out of ventricle
into aorta & to systemic circulation
d pulmonary venous blood volume & pressure
This forces fluid from pulmonary capillaries into
pulmonary tissues & alveoli
Results in pulmonary edema AEB
Dyspnea
Cough
May have frothy pink tinged
sputum pink 2severe pulmonary edema
Pulmonary crackles Low O2 sat
Heart Sounds
May have S3 heart sound ventricular gallop,
2 large volume of fluid entering ventricle at beginning of diastole
Heart FailureRight-sided HF As right ventricle fails, it will cause congestion in peripheral
tissues & viscera
2 right side of heart
Cant eject blood
Cant accommodate blood that normally returns
from venous circulation
d venous pressure leads to
JVD
& d capillary hydrostatic pressure
throughout venous system
Systemic S&S
Lower extremity edema (dependent edema)
Usually affects feet &ankles
Worsens when stands or sits for long period
Hepatomegaly (enlarged liver)
Ascites (fluid in peritoneal cavity)
Anorexia & nausea, & weakness
Weight gain 2 retention of fluid
-
7/29/2019 Cardiac valve disorders
22/46
12/17/20
Questions
Heart Failure
Overall goals
Relieve symptoms
Improve functional status & quality of life
Extend survival
Treatment options Vary according to severity of condition
Meds
Major lifestyle changes
Supplemental oxygen
Implantation of assistive devices
Cardiac transplantation
-
7/29/2019 Cardiac valve disorders
23/46
12/17/20
-
7/29/2019 Cardiac valve disorders
24/46
12/17/20
Questions1. Medications routinely prescribed for systolic HF
a. ACE inhibitors (eg, lisinopril [Prinivil, Zestril])
b. Beta-blockersc. Diuretics
d. Digitalis
2. Which of the following is a primary cause of chronic heart failure?
a. Atherosclerosis
b. Valvular dysfunction
c. Hypertension
d. Cardiomyopathy
Suppose an infant develops congestive heart failure. An important nursing
intervention would be to
a) restrict milk or dairy-product intake.
b) Maintain a semi-Fowlers position.
c) plan ways to reduce potassium intake.
d) Keep lower extremities elevated.
Heart Failure Systolic HF Meds
ACE Inhibitors
Prescribed for mild failure AEB
Fatigue or DOE
But, without signs of fluid overload &
pulmonary congestion
Start at low dose for 2 weeks
Then until optimal dose is achieved & is
hemodynamically stable
Angiotensin II receptor blockers
An alternative to ACE inhibiters
2 some pts cant tolerate ACE inhibitors
AEB develops cough, d creatinine level,
or hyperkalemia
Or combo of hydralazine (antihypertensive) &
isosorbide dinitrate (vasodilator)
Drug tx specifically indicated for African
Americans with HF
-
7/29/2019 Cardiac valve disorders
25/46
12/17/20
Systolic HF Meds
Beta-blockers
(carvedilol (Coreg)
& metoprolol (Lopressor, Toprol)
adverse effects from constant SNS stimulation
B/c of SEs, when pt is stable & euvolemic (WNL volume),
pt is started low dose
Dose is titrated slowly (every 2 weeks)
Educate after each titration:
Risk for potential worsening of symptoms
& improvement may take several week
2 beta-blockers can cause bronchioleconstriction
Ex. beta-1selective betablocker blocks
beta-adrenergic receptor sites in heart
Systolic HF Meds
Beta-blockers (cont)
Asthma
Well-controlled, mild to moderate asthma
Recommend metropolol
But, still need to monitor closely for d asthma symptoms
2 cardioselective beta-blockers retain some beta-2 effects
Severe or uncontrolled asthma
All types of beta-blocker are contraindicated
-
7/29/2019 Cardiac valve disorders
26/46
12/17/20
Systolic HF Meds
Systolic HF Meds
-
7/29/2019 Cardiac valve disorders
27/46
12/17/20
Systolic HF Medications
IV Systolic HF Meds
Nesiritide (Natrecor)
A BNP to tx acute decompensated HF
BNP is naturally produced by myocardium as compensatory mechanism
in response to HF, such as:
d ventricular end-diastolic pressure
& d release ofneurohormones (eg, norepinephrine, renin,
aldosterone)
Causes arterial & venous dilation
Suppresses neurohormones responsible for fluid retention
Promotes diuresis
Results in d preload & afterload
& d SV
Most common side effect
Dose-related hypotension
Systolic HF Medications
IV Systolic HF Meds (cont)
Milrinone (Pimacor)
Delays release of calcium from cell
Prevents uptake of extracellular calcium
Promotes vasodilation
Resulting in d preload & afterload
& d cardiac workload.
Administered if has not responded to other therapies
Major side effect is hypotension
Dobutamine (Dobutrex)
Given for significant left ventricular dysfunction & hypoperfusion
Stimulates the beta-1adrenergic receptors to cardiac contractility
-
7/29/2019 Cardiac valve disorders
28/46
12/17/20
Question
Tell whether the following statement is true or
false.
Digoxin immune FAB (Digibind) may be given to
treat severe digoxin toxicity.
Questions
-
7/29/2019 Cardiac valve disorders
29/46
12/17/20
Questions
Heart Failure
Nutritional Therapy
Low-sodium (2 to 3 g/day) diet
Dietary restriction of sodium
s fluid retention & symptoms of peripheral and pulmonary congestion
Purpose of sodium restriction
amount of circulating blood volume
smyocardial work Need to avoid drinking excessive amounts of fluid
Pt compliance is important
2 dietary indiscretions may result in severe exacerbations of HF
requiring hospitalization
Oxygen therapy
May become necessary as HF progresses
-
7/29/2019 Cardiac valve disorders
30/46
12/17/20
3
Heart FailureOther Interventions
PCI or CABG: for underlying CAD
Implantable cardioverter defibrillator (ICD)
For pts with severe left ventricular dysfunction & possibility of life-threatening
dysrhythmias
HF places pt at high risk for dysrhythmias
2 sudden cardiac death is common cause of death for pts advanced HF
Cardiac resynchronization therapy (CRT)
For pts with conduction defect
Example: left bundle branch block is frequently seen in HF
Results in dyssynchronous conduction & contraction of both
ventricles, which can further EF
CRT uses of biventricular pacemaker
Txs conduction defects
Improves CO
s mitral regurgitation
Slows ventricular remodeling process
Heart Failure
Other Interventions (cont)
Ultrafiltration
To tx severe fluid overload
Removes fluid via small bedside machine
Implanted ventricular assist device
A mechanical circulatory assistance device
Serves as bridge therapy to a cardiac transplant Cardiac transplantation
May be only option for long-term survival.
-
7/29/2019 Cardiac valve disorders
31/46
12/17/20
3
Care of the Patient with HF
Assessment Mental status
Assess for confusion
2 EF s O2 to brain
Lung sounds
Assess for crackles & wheezes
Heart sounds
Assess for S3 S3 means heart is failing & d blood is filling ventricle with each beat
Fluid status/signs of fluid overload
JVD: estimates central venous pressure
Abnormal: > 3 cm above the sternal angle
Hepatojugular reflux of Liver Apply pressure to right upper abdominal quadrant for 30 to 60 seconds
If neck vein distends > 1 cm, then positive for d venous pressure
Care of Patient with HFAssessment (cont)
Dependent edema
d SV can cause perfusion to periphery AEB
Cool, pale, cyanotic skin
Edema to sacrum, back, & hands, & fingers
Daily weight
Weigh at same time of day, with same type of clothing, & on same scale
Notify the MD if gained 2- to 3-lb in a day
Or 5-lb in a week (may need diuretics adjusted) I&O
Assess if ingested more fluid than excreted (positive fluid balance)
Compare positive fluid balance to any gain in weight
Monitor for oliguria
d urine output, < 500 mL/24 h
Monitor for anuria
Urine output < 50 mL/24 h
Monitor responses to meds
-
7/29/2019 Cardiac valve disorders
32/46
12/17/20
3
Questions
Questions
-
7/29/2019 Cardiac valve disorders
33/46
12/17/20
3
Care of Patient with HF
Nursing Diagnoses
Activity intolerance & fatigue r/t d CO
Excess fluid volume r/t HF syndrome
Anxiety r/t breathlessness from inadequate oxygenation
Powerlessness r/t chronic illness & hospitalizations
Ineffective therapeutic regimen management r/t lack of
knowledge
Heart Failure
Major Teaching Goals
Promote activity and fatigue
Relieving fluid overload symptoms
anxiety
ability to manage anxiety Verbalizes ability to make decisions & influence
outcomes
Verbalizes understanding about self-care program
-
7/29/2019 Cardiac valve disorders
34/46
12/17/20
3
Activity Intolerance
Bed rest for acute exacerbations
Encourage regular physical activity (AEB 30 minutes daily)
Exercise training
Pacing of activities
Wait 2 hours after eating before doing physical activity
Avoid activities in extremely hot, cold, or humid weather.
Modify activities to conserve energy.
Positioning
HOB (semi-Fowlers) to facilitate breathing & rest, andsupport of arms
Caring for HF
Fluid Volume Excess
Assess for symptoms of fluid overload
Daily weight
I&O
Diuretic therapy
Fluid intake
Fluid restriction
Maintenance of sodium restriction (refer to Chart 30-4)
Lifestyle changes & meds to education to:
(1) number of recurrences of acute HF
(2) life expectancy
(3) unnecessary hospitalizations
-
7/29/2019 Cardiac valve disorders
35/46
12/17/20
3
Patient Teaching for HFSelf-Care Program
Meds
Timing of med administration Oral diuretics should be taken early in morning
2 diuresis wont interfere with nighttime rest
Diet
Low-sodium diet & fluid restriction
Low sodium foods
Example: Potatoes & chicken
High sodium foods
Example: Ham, sardines, & bouillon
Monitor for signs of excess fluid:
Example daily weight
Exercise & activity program
Stress management
Prevention of infection
Know how & when to contact health care provider
Include family in teaching
-
7/29/2019 Cardiac valve disorders
36/46
12/17/20
3
Pulmonary Edema
Abnormal accumulation of fluid in
interstitial spaces of lungs that
diffuses into alveoli
Resistance to left ventricular
filling
Causes blood to back up into
pulmonary circulation
Can result in flash
pulmonary edema
Etiology
MI
Exacerbation of chronic HF
Renal failure
S&S
LOC
Hypoxemia
Restlessness
Anxiety
Dyspnea
Cool & clammy skin
Cyanosis
Weak & rapid pulse
Cough
sputum production (maybe mucoid, frothy & blood-
tinged)
Lung congestion
Moist, noisy respirations
Pulmonary EdemaPathophysiology
-
7/29/2019 Cardiac valve disorders
37/46
12/17/20
3
Management of Pulmonary Edema Prevention
Early recognition
Monitor lung sounds
Signs of d activity tolerance
Signs of d fluid retention
Place pt upright & dangle legs
Oxygen
exertion & stress
As ability to breathe s, pts fear
& anxiety s
Makes condition more severe.
Hence, pt is unstable, nurse must
remain with pt
Medications
Morphine
Assess for resp depression,
hypotension,vomiting
Keep morphine antagonist
(naloxone hydrochloride
(Narcan) available
Give if exhibits serious
respiratory depression
Diuretic (furosemide)
If on continuous IV of vasoactive
meds
Needs to be on ECG
monitoring & frequent VS
(BP, pulse, resp)
-
7/29/2019 Cardiac valve disorders
38/46
12/17/20
3
Pulmonary Edema
Case Study (cont)
Pulmonary EdemaCase Study (cont)
-
7/29/2019 Cardiac valve disorders
39/46
12/17/20
3
Potential Complications of HF
Cardiogenic shock
Dysrhythmias
Thromboembolism
Pericardial effusion
Cardiac tamponade
Complications of HFCardiogenic Shock
Life-threatening condition with a high mortality rate
CO leads to inadequate tissue perfusion & initiation of shock syndrome.
High risk pts
S/p MI
End-stage HF
Cardiac tamponade
Pulmonary embolism
Cardiomyopathy
Dysrhythmias.
S&S: symptoms of HF, shock state, & hypoxia
Pt is managed in ICU to assess:
Cardiac rhythm
Hemodynamic parameters
Fluid status
Action of meds
-
7/29/2019 Cardiac valve disorders
40/46
12/17/20
4
Complications of HF
Cardiogenic Shock
Management
Correct underlying problem
Meds
Diuretics
Positive inotropic agents
Vasopressors
Circulatory assist devices
Intra-aortic balloon pump
(IABP)
Cardiogenic Shock
Complications of HF
Cardiogenic Shock
Mechanical Circulatory Assistive Devices
Intra-Aortic Balloon Pump
Uses internal counterpulsation
through inflation & deflation of
balloon
Augments pumping action of heart
Balloon inflates during diastole
s perfusion of coronary &
peripheral arteries
Balloon deflates just before systole
s afterload
resistance to ejection
left ventricular workload
inflates
deflates
-
7/29/2019 Cardiac valve disorders
41/46
12/17/20
4
Complications of HF
Thromboembolism
Intracardiac thrombi
Especially common in pts with A-fib
Pulmonary embolism
Most common complication of HF
Hence, HF places pt at d risk for
pulmonary embolism
2 d mobility & d
circulation
2 blood clots may form in
deep veins of legs & embolize
to pulmonary vasculature
Results in life-threatening
embolic eventPulmonary emboli may be single or multiple
Questions
-
7/29/2019 Cardiac valve disorders
42/46
12/17/20
4
Complications of HF
Pericardial Effusion Accumulation of fluid in pericardial sac May accompany advanced HF
Normally, pericardial sac contains20 mL of fluid
2 s friction as heart beats
d fluid in pericardial sac causes:
pressure inside pericardialsac
& compresses heart
Slow in pericardial fluid
Results in no noticeablesymptoms.
Rapid in pericardial fluid
Results in stretchingpericardium to maximum size
Results in CO
Results in cardiactamponade (compressionof heart)
S&S of Pericardial Effusion
Feeling of pressure in chest Engorged neck veins
SOB
Labile or low BP
Pulsus paradoxus
Systolic BP is markedly lower
during inhalation
AEB > 10 mm Hg in
systolic BP during
inhalation & exhalation
Refer to next slide
Pulsus Paradoxus Normal conditions of rest
Inspiration will cause a of arterial systolic pressure of < 10 mm Hg occurs
Inspiration will cause a fall in venous pressure
Paradoxical pulse
Pulsus paradoxus differs from a normal pulse in two respects
1) inspiration will cause a in arterial pressure is > 10 mm Hg
2) inspiraion will cause venous pressure to remain steady or increases.
The exaggerated waxing & waning in pulse volume can usually be
palpated & demonstrated with a sphygmomanometer or arterial catheter.
-
7/29/2019 Cardiac valve disorders
43/46
12/17/20
4
Complications of HFCardiac Tamponade
Restricts heart function
Results in:
d venous return
CO
S&S of cardiac tamponade 2 pericardial effusion
CO causes pt to feel anxiety, faintness, & SOB
Cough
2 swelling of pericardial sac causes pressureon trachea
Distended neck veins
2 venous pressure
Paradoxical pulse
Indicative sign of: cardiac tamponade,
pericarditis chronic sleep apnea, COPD,asthma
AEB > 10 mm Hg in systolic BP during
inhalation & exhalation
Muffled or distant heart sounds
Cardinal signsing systolic BP
Narrowing pulsepressureing venous pressureDistant heart sounds
Cardiac Arrest Heart ceases to produce effective pulse & circulate blood
Causes
Dysrhythmia (e.g. V-Fib)
Profound bradycardia
Asystole (absense of a cardiac rhythm)
Respiratory arrest
Pulseless electrical activity (PEA)
Electrical activity is present
But, has no effective cardiac contraction or circulating volume
Causes
Hypovolemia (eg, from excessive bleeding)
Hypoxia,
Hypothermia
Hyperkalemia
Massive pulmonary embolism
MI
Med overdose (eg, beta-blockers, calcium channel blockers).
-
7/29/2019 Cardiac valve disorders
44/46
12/17/20
4
Cardiac Arrest
Assessment
Pt will immediately lose consciousness, pulse, & BP
Pupils will begin dilating within 45 seconds.
Seizures may or may not occur
Risk of irreversible brain damage & death
s with every minute from time that circulation ceases
Need to take immediate measures to restore circulation
Cardiac ArrestInterventions
Provide CPR
2 s blood flow to vital organs until effective
circulation can be reestablished
Start CPR after recognition of unresponsiveness,
lack of pulse & respiration
First
Assess LOC (which is first step in basic life
support) Shake pts shoulders & shout, "Are you OK?"
Second
Open airway & check for respirations
If breathing is absent, give two mouth-to-
mouth breaths
Then check circulation by palpating carotid
artery
Once LOC is restored
Priority for adults
Activate code teamor EMS
911 home
77 SVC
Exceptions
Near drowning
Drug or medoverdose
Respiratory arrest
These need 2minutes of CPRperformed beforeactivating EMS
-
7/29/2019 Cardiac valve disorders
45/46
12/17/20
4
Sudden Cardiac Death/Cardiac Arrest
The ABCDs of Basic CPR A- airway
Maintain an open airway
B- breathing
Provide artificial ventilation by rescue breathing
C- circulation
Promote artificial circulation by external cardiac compression if has no
pulse
Give meds (example: epinephrine for asystole)
D- defibrillation for VT and VF; with standard defibrillator
Perform CPR initially only if defibrillator is not immediately available.
Survival rate s for every minute defibrillation is delayed
Pts who have not been defibrillated within 10 minutes, have little chance
of survival.
Question
1. All of the following are clinical manifestations ofright-sided heart failure except:a. Hepatomegaly
b. Jugular vein distention
c. Ascites
d. Orthopnea
2. Tell whether the following statement is true orfalse.The most reliable sign of cardiac arrest is absence of
breath sounds.
-
7/29/2019 Cardiac valve disorders
46/46
12/17/20
Questions