
CARCINOMAS OF THE ORAL CAVITY STRUCTURED REPORTING ...
75
i CARCINOMAS OF THE ORAL CAVITY STRUCTURED REPORTING PROTOCOL (2nd Edition 2019) Incorporating the: International Collaboration on Cancer Reporting (ICCR) Carcinoma of the Oral Cavity Dataset www.ICCR-Cancer.org
Transcript of CARCINOMAS OF THE ORAL CAVITY STRUCTURED REPORTING ...

i
CARCINOMAS OF THE ORAL
CAVITY STRUCTURED
REPORTING PROTOCOL
(2nd Edition 2019)
Incorporating the:
International Collaboration on Cancer Reporting (ICCR)
Carcinoma of the Oral Cavity Dataset
www.ICCR-Cancer.org
ii
Core Document versions:
• ICCR dataset: Carcinoma of the Oral Cavity Dataset 1st edition
• AJCC Cancer Staging Manual 8th edition
• World Health Organization (WHO). Classification of Head and Neck Tumours. 4th edition.

iii
ISBN: 978-1-76081-118-1 Publications number (SHPN): (CI)190199
Online copyright
© RCPA 2019
This work (Protocol) is copyright. You may download, display, print and reproduce the Protocol for your personal, non-commercial use or use within your organisation subject to the following terms and conditions:
1. The Protocol may not be copied, reproduced, communicated or displayed, in whole or in part, for profit or commercial gain.
2. Any copy, reproduction or communication must include this RCPA copyright notice in full.
3. With the exception of Chapter 6 - the checklist, no changes may be made to the wording of the Protocol including any Standards, Guidelines, commentary, tables or diagrams. Excerpts from the Protocol may be used in support of the checklist. References and acknowledgments must be maintained in any reproduction or copy in full or part of the Protocol.
4. In regard to Chapter 6 of the Protocol - the checklist:
o The wording of the Standards may not be altered in any way and must be included as part of the checklist.
o Guidelines are optional and those which are deemed not applicable may be removed.
o Numbering of Standards and Guidelines must be retained in the checklist, but
can be reduced in size, moved to the end of the checklist item or greyed out or other means to minimise the visual impact.
o Additional items for local use may be added but must not be numbered as a Standard or Guideline, in order to avoid confusion with the RCPA checklist items.
o Formatting changes in regard to font, spacing, tabulation and sequencing may be made.
o Commentary from the Protocol may be added or hyperlinked to the relevant checklist item.
Apart from any use as permitted under the Copyright Act 1968 or as set out above, all other rights are reserved. Requests and inquiries concerning reproduction and rights should be addressed to RCPA, 207 Albion St, Surry Hills, NSW 2010, Australia.
First published: December 2019, 2nd Edition (Version 2.0)

iv
Disclaimer
The Royal College of Pathologists of Australasia ("College") has developed these protocols as an educational tool to assist pathologists in reporting of relevant information for specific cancers. Each protocol includes “standards” and “guidelines” which are indicators of ‘minimum requirements’ and ‘recommendations’, which reflect the opinion of the relevant expert authoring groups. The use of these standards and guidelines is subject to the clinician’s judgement in each individual case.
The College makes all reasonable efforts to ensure the quality and accuracy of the protocols and to update the protocols regularly. However subject to any warranties, terms or conditions which may be implied by law and which cannot be excluded, the protocols are provided on an "as is" basis. The College does not warrant or represent that the protocols are complete, accurate, error-free, or up to date. The protocols do not constitute medical or professional advice. Users should obtain appropriate medical or professional advice, or where appropriately qualified, exercise their own professional judgement relevant to their own particular circumstances. Users are responsible for evaluating the suitability, accuracy, currency, completeness and fitness for purpose of
the protocols.
Except as set out in this paragraph, the College excludes: (i) all warranties, terms and conditions relating in any way to; and (ii) all liability (including for negligence) in respect of any loss or damage (including direct, special, indirect or consequential loss or damage, loss of revenue, loss of expectation, unavailability of systems, loss of data, personal injury or property damage) arising in any way from or in connection with; the
protocols or any use thereof. Where any statute implies any term, condition or warranty in connection with the provision or use of the protocols, and that statute prohibits the exclusion of that term, condition or warranty, then such term, condition or warranty is not excluded. To the extent permitted by law, the College's liability under or for breach of any such term, condition or warranty is limited to the resupply or replacement of services or goods.

v
Contents
Scope ................................................................................................................ vi
Abbreviations ................................................................................................... vii
Definitions ....................................................................................................... viii
Introduction .......................................................................................................1
Authority and development ................................................................................5
1 Clinical information and surgical handling ...............................................8
2 Specimen handling and macroscopic findings ........................................ 10
3 Microscopic findings ............................................................................... 14
4 Ancillary studies findings ....................................................................... 22
5 Synthesis and overview.......................................................................... 23
6 Structured checklist ............................................................................... 25
7 Formatting of pathology reports ............................................................ 47
Appendix 1 Pathology request form for oral tumours .......................... 48
Appendix 2 Guidelines for formatting of a pathology report ................ 51
Appendix 3 Example of a pathology report .......................................... 53
Appendix 4 WHO classification of histology and grading of squamous cell carcinoma .................................................. 56
References ....................................................................................................... 57

vi
Scope
This protocol contains standards and guidelines for the reporting of resection and biopsy specimens of invasive carcinomas of the oral cavity, including lip and tongue. Mucosal melanoma, lymphomas and sarcomas are not included. In addition, neck dissections and nodal excisions are dealt with in a separate protocol, and this protocol should be used in conjunction, where applicable.
There are separate protocols for carcinomas of the oropharynx, hypopharynx, larynx, nasal cavity and paranasal sinuses as well as the salivary glands.
Structured reporting aims to improve the completeness and usability of pathology reports for clinicians, and improve decision support for cancer treatment. This protocol can be used to define and report the minimum data set but the structure is scalable and can equally accommodate a maximum data set or fully
comprehensive report.

vii
Abbreviations
AJCC American Joint Committee on Cancer
DOI Depth of invasion
ENE Extranodal extension
HPV Human papilloma virus
ICCR International Collaboration on Cancer Reporting
IHC Immunohistochemistry
IHI
Individual health identifier
LIS
lic
liC
Laboratory Information System
NOS Not otherwise specified
RCPA Royal College of Pathologists of Australasia
TNM Tumour-node-metastasis
UICC International Union Against Cancer
WHO World Health Organization

viii
Definitions
The table below provides definitions for general or technical terms used in this protocol. Readers should take particular note of the definitions for ‘standard’, ‘guideline’ and ‘commentary’, because these form the basis of the protocol.
Ancillary
study An ancillary study is any pathology investigation that may form part of a cancer pathology report but is not part of routine histological assessment.
Clinical information
Patient information required to inform pathological assessment, usually provided with the specimen request form, also referred to as “pre-test information”.
Commentary Commentary is text, diagrams or photographs that clarify the standards (see below) and guidelines (see below), provide examples and help with interpretation, where necessary (not every standard or guideline has commentary).
Commentary is used to:
• define the way an item should be reported, to foster reproducibility
• explain why an item is included (e.g., how does the item assist with clinical management or prognosis of the specific cancer).
• cite published evidence in support of the standard or guideline
• state any exceptions to a standard or guideline.
In this document, commentary is prefixed with ‘CS’ (for commentary on a standard) or ‘CG’ (for commentary on a guideline), numbered to be consistent with the relevant standard
or guideline, and with sequential alphabetic lettering within each set of commentaries (e.g., CS1.01a, CG2.05b).
General commentary
General commentary is text that is not associated with a specific standard or guideline. It is used:
• to provide a brief introduction to a chapter, if necessary
for items that are not standards or guidelines but are included in the protocol as items of potential importance, for which there is currently insufficient evidence to recommend their inclusion. (Note: in future reviews of protocols, such items may be reclassified as either standards or guidelines, in line with diagnostic and prognostic advances, following
evidentiary review).

ix
Guideline Guidelines are recommendations; they are not mandatory, as indicated by the use of the word ‘should’. Guidelines cover items that are unanimously agreed should be included in the dataset but are not supported by National Health and Medical Research Council (NHMRC) level III-2 evidence.1 These elements may be clinically important and recommended as good practice but are not yet validated or regularly used in patient management.
Guidelines include key information other than that which is essential for clinical management, staging or prognosis of the
cancer such as macroscopic observations and interpretation, which are fundamental to the histological diagnosis and conclusion e.g., macroscopic tumour details, block identification key, may be included as either required or recommended elements by consensus of the expert committee. Such findings are essential from a clinical governance perspective, because they provide a clear, evidentiary decision-making trail.
Guidelines are not used for research items.
In this document, guidelines are prefixed with ‘G’ and numbered consecutively within each chapter (e.g., G1.10).
Macroscopic
findings Measurements, or assessment of a biopsy specimen, made by
the unaided eye.
Microscopic findings
In this document, the term ‘microscopic findings’ refers to histo-morphological assessment.
Predictive factor
A predictive factor is a measurement that is associated with response or lack of response to a particular therapy.
Prognostic factor
A prognostic factor is a measurement that is associated with clinical outcome in the absence of therapy or with the application of a standard therapy. It can be thought of as a measure of the natural history of the disease.

x
Standard Standards are mandatory, as indicated by the use of the term ‘must’. Standards are essential for the clinical management, staging or prognosis of the cancer. These elements will either have evidentiary support at Level III-2 or above (based on prognostic factors in the NHMRC levels of evidence1 document). In rare circumstances, where level III-2 evidence is not available an element may be made a Standard where there is unanimous agreement in the expert committee. An appropriate staging system e.g., Pathological TNM staging would normally be included as a required element. These elements must be
recorded and at the discretion of the pathologist included in the pathology report according to the needs of the recipient of the report.
The summation of all standards represents the minimum dataset for the cancer.
In this document, standards are prefixed with ‘S’ and numbered consecutively within each chapter (e.g., S1.02).
Structured report
A report format which utilises standard headings, definitions and nomenclature with required information.
Synoptic
report A structured report in condensed form (as a synopsis or precis).
Synthesis Synthesis is the process in which two or more pre-existing elements are combined, resulting in the formation of something new.
The Oxford dictionary defines synthesis as “the combination of
components or elements to form a connected whole”.
In the context of structured pathology reporting, synthesis represents the integration and interpretation of information from two or more modalities to derive new information.

1
Introduction
Oral cancer
Head and neck cancers are not as common as other cancers such as those of the prostate, colon, breast and lung, and often don’t receive the same attention. In addition, many can be attributed to lifestyle factors such as smoking, excess alcohol consumption, poor diet and excess sun exposure. Oral cancer particularly
affects the socially disadvantaged.2 Smoking is a well-known risk factor for oral cancer however, there is a lag in time between smoking and the onset of cancer and this must be considered when interpreting data. More recently, Human Papilloma Viruses (HPV) have also been recognised as contributing to cancers affecting oral cavity and oropharynx particularly the high-risk HPVs (type 16).
In 2009, 3896 new head and neck cancers were diagnosed in Australia accounting for 3.4% of all cancers and of these, 2037 arose in the oral cavity.3 Males accounted for at least 60% of these new oral cancers. Although there has been an increasing trend in the incidence of new oral cancers from 1982 when 1263 new cases were diagnosed, this increase in numbers of new cases is despite the accompanying reduction in smoking rates from 40.3% in 1983 to 16.4% in 2010.3 The age standardised incidence rates however have decreased from 12.1 per
100,000 persons in 1992 to 8.8 in 2009.3
In 2011 the number of deaths related to cancer of the oral cavity were 294, accounting for 31.1% of all deaths from head and neck cancer - an increase from the 237 deaths in 1982. Mortality rates are relatively stable for cancer of the oral cavity at around 1.5 deaths per 100,000 persons. During the period 2006–2010, the 5-year relative survival rate for oral cavity cancer was 75.0%, the highest when compared to other head and neck cancers (75.6% males and 73.8% females).3
Benefits of structured reporting
The pathology report lays the foundation for a patient’s cancer journey and conveys information which:
• Provides the definitive diagnosis • Includes critical information for Tumour-Node-Metastasis (TNM) staging • Evaluates the adequacy of the surgical excision • Provides morphological and biological prognostic markers which determine
personalised cancer therapy
However, the rapid growth in ancillary testing such as immunohistochemistry, flow cytometry, cytogenetics, and molecular studies, have made the task of keeping abreast of advances on specific cancer investigations extremely difficult for pathologists. The use of structured reporting checklists by pathologists ensures that all key elements are included in the report specifically those which have clinical management, staging or prognostic implications. Consequently minimum or comprehensive datasets for the reporting of cancer have been developed4,5 around the world. Both the United Kingdom,6 and United States7 have produced standardised cancer reporting protocols or “datasets” for national use for many years.

2
The use of cancer reporting checklists improves completeness and quality of cancer reporting and thereby ensures an improved outcome for cancer patients. This has long term cost implications for public health by ensuring the most
effective and timely treatment based on accurate and complete information.
The use of a structured reporting format also facilitates easy extraction of the necessary information by secondary users of the information i.e., cancer registries.
Importance of histopathological reporting
The information contained within a pathology report includes prognostic information for the patient and treating clinical team. The content will assist in subsequent management, whether this may be surveillance, further surgery, radiotherapy or chemotherapy, or a combination of these modalities.
International Collaboration on Cancer Reporting
The International Collaboration on Cancer Reporting (ICCR), founded in 2011 by the Australasian (RCPA), United States College of American Pathologists (US CAP) and Royal College of Pathologists United Kingdom (RCPath UK) Colleges of Pathology and the Canadian Association of Pathology - Association Canadienne des Pathologistes (CAP-ACP) in association with the Canadian Partnership Against
Cancer (CPAC), was established to explore the possibilities of a collaborative approach to the development of common, internationally standardised and evidence-based cancer reporting protocols for surgical pathology specimens.
The ICCR, recognising that standardised cancer datasets have been shown to provide significant benefits for patients and efficiencies for organisations through
the ease and completeness of data capture8-11 undertook to use the best
international approaches and the knowledge and experience of expert pathologists, and produce cancer datasets which would ensure that cancer reports across the world will be of the same high quality – ensuring completeness, consistency, clarity, conciseness and above all, clinical utility.
Representatives from the four countries participating in the initial collaboration undertook a pilot project in 2011 to develop four cancer datasets - Lung, Melanoma, Prostate (Radical Prostatectomy), and Endometrium. Following on from the success of this pilot project, the ICCR was joined by the European Society of Pathology (ESP) in 2013 and in 2014 incorporated a not-for-profit organisation focussed on the development of internationally agreed evidence-based datasets developed by world leading experts. The ICCR Datasets are made freely available from its website www.ICCR-Cancer.org
Design of this protocol
This structured reporting protocol has been developed using the ICCR dataset on carcinoma of the oral cavity as the foundation.
This protocol includes all of the ICCR cancer dataset elements as well as additional information, elements and commentary as agreed by the RCPA expert committee. It provides a comprehensive framework for the assessment and documentation of pathological features of carcinomas in the oral cavity.

3
ICCR dataset elements for carcinoma of the oral cavity are included verbatim. ICCR Core elements are mandatory and therefore represented as standards in this document. ICCR Non-core elements, that is, those which are not mandatory but are recommended, may be included as guidelines or upgraded to a standard based on the consensus opinion of the local expert committee.
The ICCR elements are identified in each chapter with the ICCR logo placed before the Standard or Guideline number or bullet and the ICCR element description and commentary is boarded by a grey box as shown below:
S3.01 The histological tumour type must be recorded.
Additional commentary by the RCPA expert committee may be added to an ICCR element but is not included in the grey bordered area nor indicated with an ICCR
logo e.g.,
G2.03 If present, the laterality of the lymph nodes submitted may be recorded as left, right or bilateral.
CS2.03a If present, record site and number. All lymph node tissue should be submitted for histological examination.
Further information on the ICCR is available at www.iccr-cancer.org
Checklist
Consistency and speed of reporting is improved by the use of discrete data elements recorded from the checklist. Items suited to tick boxes are distinguished from more complex elements requiring free text or narrative. A structured or discrete approach to responses is favoured, however the pathologist is encouraged to include free text or narrative where necessary to document any
other relevant issues, to give reasons for coming to a particular opinion and to explain any points of uncertainty.
Report format
The structure provided by the following chapters, headings and subheadings describes the elements of information and their groupings, but does not
necessarily represent the format of either a pathology report (Chapter 7) or checklist (Chapter 6). These, and the structured pathology request form (Appendix 1) are templates that represent information from this protocol, organised and formatted differently to suit different purposes.
Key documentation
• Guidelines for Authors of Structured Cancer Pathology Reporting Protocols, Royal College of Pathologists of Australasia, 200912
4
• World Health Organization (WHO). Classification of Head and Neck Tumours.,
4th Edition. El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ (editors). Lyon, France: IARC Press;201713
• AJCC Cancer Staging Manual, 8th edition, American Joint Committee on Cancer, 201614
Changes since the last edition
Inclusion of all ICCR agreed REQUIRED and RECOMMENDED elements.
Inclusion of all AJCC 8th Edition errata (Update 13/5/2021) identified to August 2021.

5
Authority and development
This section provides information about the process undertaken to develop this protocol.
This 2nd edition of the protocol is an amalgam of two separate processes:
1. This protocol is based on the ICCR dataset – carcinoma of the oral cavity
1st edition. All ICCR elements from this dataset, both required (mandatory) and recommended (optional), are included in this protocol, verbatim. (It should be noted that RCPA feedback from all Anatomical Pathology fellows and specifically the local expert committee was sought during the development process of the ICCR dataset.) Details of the ICCR development process and the international expert authoring committee responsible for the ICCR dataset are available on the ICCR website: iccr-
cancer.org.
2. Additional elements, values and commentary have been included as deemed necessary by the local expert committee. In addition, the standard inclusions of RCPA protocols e.g., example reports, request information etc, have also been added.
Authorship – 2nd edition 2019
A/Prof Hedley Coleman, (Lead author), Oral and Maxillofacial Pathologist
Prof Jane Dahlstrom, (Chair, Head & Neck Cancers), Pathologist
Dr Dylan Hyam, Surgeon
Dr Alexandra Allende, Pathologist
Dr Brandon Nguyen, Radiation Oncologist
Dr Spinder Samra, Pathologist
Dr Purnima Sundaresan, Radiation Oncologist
Dr Eva Wong, Surgeon
Authorship – 1st edition 2011
Prof Jane Dahlstrom (Chair), Pathologist
A/Prof Hedley Coleman (Lead author), Oral Pathologist
Prof Newell Johnson, Oral Pathologist
A/Prof Elizabeth Salisbury, Pathologist
A/ Prof Michael Veness, Radiation Oncologist
Clinical A/Prof Gary Morgan, Head and Neck Surgeon
Editorial managers
Meagan Judge, Royal College of Pathologists of Australasia
Christina Selinger, PhD, Royal College of Pathologists of Australasia
6
Acknowledgements
The head and neck cancers expert committee wish to thank all the pathologists
and clinicians who contributed to the discussion around this document.
Stakeholders
ACT Cancer Registry
ACT Health
Australian and New Zealand Association of Oral & Maxillofacial Surgeons
Australian and New Zealand Head and Neck Cancer Society
Australian Cancer Network
Australian Commission on Safety and Quality in Health Care
Australian Digital Health Agency
Australian Institute of Health and Welfare
Australian Society of Otolaryngology Head and Neck Surgery
Beyond Five
Cancer Australia
Cancer Council ACT
Cancer Council Queensland
Cancer Council Victoria
Cancer Council Western Australia
Cancer Institute NSW
Cancer Services Advisory Committee (CanSAC)
Cancer Voices NSW
Clinical Oncology Society of Australia (COSA)
Department of Health, Australia
Health Informatics Society of Australia (HISA)
Independent Review Group of Pathologists
International Academy of Pathology (IAP)
Medical Oncology Group of Australia
Medical Software Industry Association (MSIA)
Ministry of Health, New Zealand
National Pathology Accreditation Advisory Council (NPAAC)
New Zealand Cancer Registry
Northern Territory Cancer Registry
Pathology Australia
Public Pathology Australia
7
Queensland Cooperative Oncology Group (QCOG)
RCPA Anatomical Pathology Advisory Committee (APAC)
Representatives from laboratories specialising in anatomical pathology across Australia
Royal Australasian College of Physicians (RACP)
Royal Australasian College of Surgeons (RACS)
Royal Australian and New Zealand College of Radiologists (RANZCR)
Royal Australian College of General Practitioners (RACGP)
Royal College of Pathologists of Australasia (RCPA)
South Australia Cancer Registry
Standards Australia
Tasmanian Cancer Registry
Victorian Cancer Registry
Western Australia Clinical Oncology Group (WACOG)
Western Australian Cancer Registry
Development process
This protocol has been developed following the ten-step process set out in Guidelines for Authors of Structured Cancer Pathology Reporting Protocols.12
Where no reference is provided, the authority is the consensus of the local expert group for local inclusions and the ICCR Dataset Authoring Committee for ICCR components denoted with the ICCR logo.

8
1 Pre-analytical
This chapter relates to information that should be recorded on receipt of the specimen in the laboratory.
The pathologist is reliant on the quality of information received from the clinicians or requestor. Some of this information may be received in generic pathology request forms, however, the additional information required by the pathologist specifically for the reporting of carcinomas of the oral cavity, is outlined in Appendix 1. Appendix 1 also includes a standardised request information sheet that may be useful in obtaining all relevant information from the requestor.
Surgical handling procedures affect the quality of the specimen and recommendations for appropriate surgical handling are included in Appendix 1.
S1.01 All demographic information provided on the request form and with the specimen must be recorded.
CS1.01a The Royal College of Pathologists of Australasia (RCPA) The Pathology Request-Test-Report Cycle — Guidelines for Requesters and Pathology Providers must be adhered to.15 This document specifies the minimum information to be provided by
the requesting clinician for any pathology test.
CS1.01b Document whether or not the patient identifies as Aboriginal and/or Torres Strait Islander in Australia, or Māori in New Zealand. This is in support of government initiatives to monitor the health of those who identify as indigenous, particularly in relation to cancer.
CS1.01c The patient’s health identifiers may include the patient’s Medical Record Number as well as a national health number such as a patient’s Individual Healthcare Identifier (IHI) (Australia) or the National Healthcare Identifier (New Zealand).
S1.02 All clinical information as documented on the request form must
be recorded verbatim.
CS1.02a The request information may be recorded as a single text (narrative) field or it may be recorded in a structured format.
CS1.02b In most cases all clinical information should be transcribed:
however, in a small number of cases the pathologist may exercise discretion regarding the inclusion of provided clinical information, for instance, possibly erroneous information or information that may impact on patient privacy. In such case reference should be made as to the location of the complete clinical information e.g., “Further clinical information is available from the scanned request form.”
G1.01 The copy doctors requested on the request form should be recorded.
S1.03 The pathology accession number of the specimen must be recorded.

9
S1.04 The principal clinician involved in the patient’s care and responsible for investigating the patient must be recorded.
CS1.04a The principal clinician should provide key information regarding the clinical presentation of the patient. Follow up may be required with the principal clinician for a number of reasons:
• The clinical assessment and staging may be incomplete at the time of biopsy.
• The pathology request is often authored by the clinician performing the surgical excision/biopsy rather than the clinician who is investigating and managing the patient.
• The identity of this clinician is often not indicated on the pathology request form
In practice therefore, it is important in such cases that the reporting pathologist should be able to communicate with the managing clinician for clarification.
CS1.04b The Australian Healthcare identifiers i.e., Healthcare Provider Identifier - Individual (HPI-I) and Healthcare Provider
Identifier - Organisation (HPI-O) should be included, where possible, to identify the principal clinician involved in the patient's care.
G1.02 Any clinical information received in other communications from the requestor or other clinician should be recorded together with the source of that information.

10
2 Specimen handling and macroscopic findings
This chapter relates to the procedures required after the information has been handed over from the requesting clinician and the specimen has been received in the laboratory.
Specimen handling
➢ Detailed fixation and specimen handling instructions are available from the RCPA online Cut-up Manual:
https://www.rcpa.edu.au/Manuals/Macroscopic-Cut-Up-Manual
➢ The specimen must be handled in a systematic and thorough fashion to ensure completeness and accuracy of pathological data.
Macroscopic findings
S2.01 The labelling of the specimen(s) must be clearly recorded.
S2.02 The operative procedure must be recorded.
CS2.02a It is important to correlate the type of procedure (excisional biopsy or resection) with the material received for patient safety. Site-specific designations are required for accurate staging and for cancer registration. Modification of the resection, e.g., partial, total should be described. For example: hemi-glossectomy, partial glossectomy; hemi-mandibulectomy, segmental (partial) mandibulectomy; partial maxillectomy, total maxillectomy; selective neck dissection, modified neck dissection.16,17
S2.03 The specimen(s) submitted must be recorded.
CS2.03a The anatomy and surgical interventions of the oral cavity are complex and it is important to ensure accurate and precise communication between the pathologists and the treating and diagnostic team with
respect to exact anatomic site of involvement, tumour laterality and specific operative procedures.18-20
The protocol applies to all carcinomas arising at these sites (see Figure 1). For large cancers that involve more than one site, the primary site of involvement should be recorded.
Mucosal Lip. The lip begins at the junction of the vermilion border with the skin and includes only the vermilion surface or that portion of the lip that meets the opposing lip.
11
Buccal Mucosa (Inner Cheek). Refers to the mucous membrane lining of the inner surface of the cheeks and lips of contact of the opposing lips to the line of attachment of mucosa of the upper and lower alveolar ridge and pterygomandibular raphe.
Lower Alveolar Ridge. This refers to the mucosa overlying the alveolar process of the mandible, which extends from the line of attachment of mucosa in the buccal vestibule to the line of free mucosa of the floor of the mouth. Posteriorly, it extends to the ascending
ramus of the mandible.
Upper Alveolar Ridge. This refers to the mucosa overlying the alveolar process of the maxilla, which extends from the line of attachment of mucosa in the upper gingival buccal vestibule to the junction of the hard palate. The posterior margin is the upper end of
the pterygopalatine arch.
Floor of the Mouth. This is a semilunar space over the mylohyoid and hypoglossus muscles, extending from the inner surface of the lower alveolar ridge to the undersurface of the tongue. The posterior boundary is the base of the anterior pillar of the tonsil. It is divided
into two sides of the submaxillary and sublingual salivary glands.
Hard Palate. This is the semilunar area between the upper alveolar ridge and the mucous membrane covering the palatine process of the maxillary palatine bones. It extends from the inner surface of the superior alveolar ridge to the posterior edge of the palatine
bone.
Anterior Two-Thirds of the Tongue (Oral Tongue). This is the freely mobile portion of the tongue that extends anteriorly from the line of circumvallate papillae to the undersurface (ventral) of the tongue at the junction of the floor of the mouth. It includes the tip of tongue,
lateral borders, dorsal surface and ventral tongue.
Retromolar trigone. A triangular shaped region extending distal from the mandibular third molar as the base and attaches to the hamulus of the medial pterygoid process of the sphenoid bone as the apex.
‘Not specified’ should be used rarely and only after
good effort has been employed to obtain the requisite information.
S2.04 The macroscopic tumour site(s) must be recorded.
G2.01 Tumour focality should be recorded.
CG2.01a True multifocal or synchronous oral cavity carcinomas are rare. Patients with oral squamous cell carcinomas have a high incidence (2-3%) of developing a second primary lesion however these are usually metachronous lesions. The theory of field cancerization whereby

12
contiguous genetically altered areas of mucosa lead to the development of neoplasms have been supported by studies evaluating clonality and other molecular markers. Proliferative verrucous leukoplakia has the propensity of developing multifocal tumours. It is rare to have multiple tumours disconnected but not uncommon to have more than one squamous cell carcinoma connected via dysplasia. The location, proximity to dysplastic epithelium, depth and nodal status remain important. Tumour focality seems to be a
standard not just for staging and pathology but for clinical trials and treatment considerations.21-24
S2.05 The surface dimensions of largest tumour and the maximum tumour thickness must be measured.
CS2.05a Tumour dimension is an important component in
pathologic staging.14 The macroscopic diameter (in millimetres) should be used unless the histological extent is greater than macroscopically apparent, in which case the microscopic dimension is used. At times only microscopic evaluation actually differentiates what clinically (phenotypically) appears to be tumour from what is actual invasion (not dysplasia or inflammation). The maximum depth of invasion should be recorded as core and the discussion should include how/why depth of invasion is different than tumour thickness.25-33 As for other tissues, measurements are made pragmatically, acknowledging distortion of tissues by fixation and processing.11
S2.06 A differential ink application and block identification key listing the nature and origin of all tissue blocks must be recorded.
CS2.06a The colours of the ink used to designate the various surfaces (particularly superficial and deep) should be clearly stated in the macroscopic description to guide
margin assessment.
CS2.06b The origin/designation of all tissue blocks should be recorded. This information should be documented in the final pathology report and is particularly important should the need for internal or external review arise. The reviewer needs to be clear about the origin of each block in order to provide an informed specialist opinion. If this information is not included in the final pathology report, it should be available on the laboratory computer system and relayed to the reviewing pathologist. Utilising photography to record the specimen can be of benefit and should be considered.
Recording the origin/designation of tissue blocks also facilitates retrieval of blocks for further immunohistochemical or molecular analysis, research studies or clinical trials.

13
G2.02 A descriptive or narrative field should be provided to record any other macroscopic information that may not be recorded in the above standards and guidelines, and that would normally form part
of the macroscopic description.
CG2.02a A traditional macroscopic description may be required when the Laboratory Information System (LIS) does not allow a structured approach.
CG2.02b Where the LIS offers an electronic interface for
structured data entry the need for narrative can be significantly reduced to describe only information not otherwise captured.
Figure 1 Anatomy of the Oral Cavity. Copyright ICCR – reproduced with permission.
14
3 Microscopic findings
Microscopic findings relates to purely histological (morphological) assessment. Information derived from multiple investigational modalities, or from two or more chapters, are described in Chapter 5.
S3.01 The histological tumour type must be recorded.
CS3.01a Refer to Appendix 4.
CS3.01b The major histologic tumour types of squamous cell carcinoma as recognized by the World Health Organization (WHO) classification are squamous cell carcinoma, conventional type, basaloid, papillary, spindle, adenosquamous, acantholytic, lymphoepithelial, verrucous carcinoma and carcinoma cuniculatum. Hybrid lesions such as verrucous carcinoma and squamous cell carcinoma exist and should be recognized, as it may affect prognosis.34 Subtypes should be assigned for both prognosis and cancer registry.35-37
The major histologic salivary gland carcinomas of minor salivary glands as recognized by the WHO classification are acinic cell carcinoma, adenoid cystic carcinoma, adenocarcinoma not otherwise specified (NOS), (mammary analogue) secretory carcinoma, cystadenocarcinoma, epithelial-myoepithelial carcinoma, mucoepidermoid carcinoma (low,
intermediate and high grade), polymorphous adenocarcinoma (low, intermediate and high grade), (hyalinizing) clear cell carcinoma, intraductal carcinoma, carcinosarcoma, myoepithelial carcinoma, oncocytic carcinoma.
Carcinoma ex pleomorphic adenoma is subclassifed by type and extent of invasion, the latter including minimally invasive, invasive and intracapsular (non-invasive) cancers. The definition for minimally invasive carcinomas varies, ranging from 1.5 mm to 6 mm. Invasive carcinomas extend beyond 6 mm; non-invasive cancers are completely confined to within the capsule without evidence of penetration into
extracapsular tissue. Prior to diagnosing a non-invasive carcinoma ex pleomorphic adenoma, sectioning of the entire lesion for histologic evaluation is recommended to exclude the presence of invasive growth. Prognosis has been linked to degree of invasion with non-invasive and minimally invasive cancers apparently having a better prognosis than invasive cancers.38,39
S3.02 The Histological tumour grade40-46 must be recorded.
CS3.02a Based on the WHO classifications, three histologic grades of squamous cell carcinoma, conventional type

15
are used: well, moderately or poorly differentiated.46 The most aggressive or highest grade should be recorded if the tumour has a varied histology. Grading requires the assessment of keratinization, mitotic activity, cellular and nuclear pleomorphism, pattern of invasion and host response.16,47-50 Squamous cell carcinoma subtypes such as verrucous carcinoma, basaloid squamous cell carcinoma, papillary squamous cell carcinoma are not graded.
Grading of minor salivary gland tumours follows the
criteria for major salivary gland tumours.38,51 Refer to protocol for major salivary gland tumours.
S3.03 Tumour dimensions must be recorded.
S3.04 For resection specimens and excisional biopsies, the
maximum depth of invasion must be recorded.
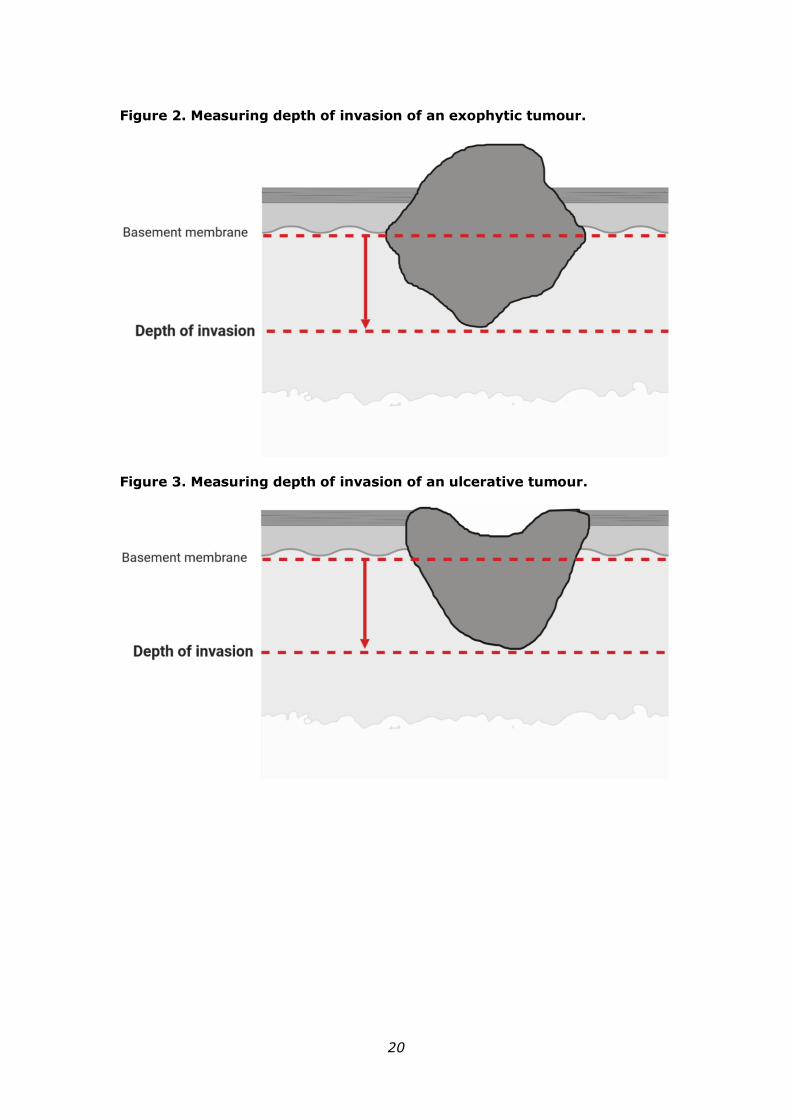
CS3.04a Depth of invasion (DOI) in oral cavity squamous cell carcinoma, particularly of the tongue, has been identified as an important prognostic indicator. DOI is not synonymous with tumour thickness. In the recent American Joint Committee on Cancer (AJCC) the
tumour stage (T) has been changed to reflect the importance of DOI.14 DOI increases T by 1 step for every 5 mm, whereby T1 is tumour ≤2 cm and DOI ≤5 mm, T2 is tumour ≤2 cm and DOI >5 mm and ≤10 mm or tumour >2 cm but ≤4 cm and ≤10 mm DOI and T3 is tumour >4 cm or any tumour >10 mm DOI. The Union for International Cancer Control (UICC) staging
system is similar to the AJCC with one exception: if the tumour is >4 cm AND > 10 mm DOI then the stage is T4a.52 DOI measures the invasiveness of the carcinoma. To measure DOI, the basement membrane is identified and an imaginary line is drawn across the tumour. A vertical or “plumb line” extends to the deepest part of the tumour which represents the DOI.
It is important to note that DOI is not synonymous with tumour thickness. An exophytic tumour (Figure 2) may be thicker than an ulcerative tumour (Figure 3), but the DOI of the ulcerative lesion may be greater.53-56
S3.05 The growth pattern of invasion at the invasive front must be recorded.
CS3.05a The pattern of invasion in oral squamous cell carcinoma has proven prognostic value and should be reported as cohesive or non-cohesive (Figure 4). It is important to evaluate the most complex area of tumour-stroma interface (“worst” area) and ideally assessment should only be made on resection specimens or excisional
biopsies. Acknowledgement is made that at times non-surgical treatment decisions are made on incisional biopsy only specimens and consequently the best assessment of pattern of invasion should be noted. Cohesive invasion is defined as broad sheets of cancer
16
cells and/or tumour nests >15 cells across. Non-cohesive invasion shows a spectrum of appearances that includes narrow strands, small groups of <15 tumour cells and single infiltrating tumour cells.53-56 For stage T1/T2 oral squamous cell carcinoma, particularly those arising in the tongue there is evidence that tumour satellites localized ≥ 1 mm away from the main tumour or nearest satellite (worst pattern of invasion WPOI-5) is a valid adverse prognostic factor.55,57
G3.01 Any response to neoadjuvant therapy should be recorded.
CG3.01a There is no agreed system for grading tumour regression in oral squamous cell carcinoma that has been treated with neoadjuvant therapy. Specific pathologic changes in response to neoadjuvant chemotherapy, although well described in other organ
systems is lacking in oral cavity cancer. These changes include necrosis, fibrosis, cytologic atypia and inflammation. As the field of neoadjuvant therapy for oral cavity cancer evolves histologic changes important for treating clinicians may be better elucidated.
S3.06 The presence or absence of lymphovascular invasion must be
recorded.
CS3.06a There is a need to distinguish between intravascular tumour embolization and retraction artefact. Positive vascular invasion should be reported only when tumour emboli are identified within endothelial lined spaces. No distinction between venous channels and small
lymphatics is required.50,58
S3.07 The presence or absence of perineural invasion at the advancing tumour front must be recorded.
CS3.07a Perineural invasion is associated with a worse prognosis, regardless of nerve size and should be recorded. The presence or absence of perineural and/or endoneural/intraneural invasion may impact subsequent therapy and prognosis.16,48,59-61
S3.08 The presence or absence of bone invasion must be recorded.
CS3.08a Infiltrative bone involvement by squamous cell
carcinoma correlates with a worse prognosis. Bone invasion may be a macroscopic feature, however sampling through the involved bone for histologic examination should be performed to obtain histologic evidence. The presence of bone invasion affects tumour staging and patients with bone invasion often have a worse prognosis. It is important to distinguish
superficial cortical bone erosion from infiltrative invasion to the medullary bone as this is critical in accurate tumour staging. If bone is resected, then bone margins should be recorded.27

17
G3.02 Involvement of adjacent structures should be recorded.
CG3.02a Such as the:
• Cortical bone
• Floor of mouth
• Skin of face, i.e., chin or nose
• Deep muscle of tongue (genioglossus, hyoglossus, palatoglossus, and styloglossus)
• Maxillary sinus
• Pterygoid plates
• Encases internal carotid artery
• Internal jugular vein
• Sternocleidomastoid muscle
• Salivary gland
S3.09 The status of the surgical resection margins must be recorded with documentation of the distance of tumour from the margins.
CS3.09a All surgical margins should be measured in millimetres histologically for both mucosal and deep margins. In the comments section, acknowledgement should be made how the surgical margin was measured, for example if the margin was submitted from the tumour bed margin at the time of the operative procedure rather than from the surgical specimen.62-65 The presence of high grade dysplasia/carcinoma in situ at the margin is associated with an increased risk of local recurrence and this should be recorded. The definition of a “close” margin is not standardized but in the oral cavity from a surgical point of view >5 mm is clear and 1-5 mm is close while <1 mm is involved. Acknowledgement is made of fixation and processing
distortion on measurements which may cause tissue shrinkage including the surgical margin.66 Acknowledgement is also made of any laser or electrocautery associated tissue distortion such as cellular and nuclear polymorphism, nuclear hyperchromatism, epithelial cell separation, collagen
denaturation, etc. on measurements including the surgical margin.67-69 Any bone resection margins should be identified and comment on the presence or absence of carcinoma at these margins should be provided.27 Dysplastic changes include abnormal cellular organization, increased mitotic activity, and nuclear enlargement with pleomorphism.16,47,48,56,62-65,70 Although terminology varies, using the 2017 WHO criteria for oral dysplasia, dysplasia limited to the lower one-third of the epithelium is generally referred to as mild dysplasia.47 Moderate dysplasia is defined as cytological atypia extending to the middle third of the
18
epithelium and severe dysplasia extends to the upper third of the epithelium. Carcinoma in situ is considered synonymous with severe dysplasia. Currently the use of a binary grading system similar to laryngeal dysplasia has been proposed but to date lacks validation in the oral cavity. In a binary system low grade dysplasia includes mild dysplasia and mild-moderate dysplasia. The term high grade dysplasia includes moderate dysplasia, severe dysplasia and carcinoma in situ.47
Reporting of surgical margins for carcinomas of the
minor salivary glands should follow those used for squamous cell carcinoma of oral cavity.
G3.03 The presence of coexistent pathology should be recorded.
CG3.02a The most common sites of dysplasia with the highest risk of malignant transformation are lateral and ventral
tongue, floor of mouth, and lower lip. Dysplastic changes include abnormal cellular organization, increased mitotic activity including abnormal forms, and nuclear enlargement with pleomorphism. Although terminology varies, dysplasia limited to the lower one-third of the epithelium is generally referred to as mild
dysplasia (low grade dysplasia), dysplasia limited to the lower two-thirds as moderate dysplasia and dysplasia involving the full thickness as severe dysplasia/carcinoma in situ.70 However, when moderate dysplasia has marked cytologic atypia, then often the lesion will be upgraded to severe dysplasia. The term high grade dysplasia includes moderate and severe dysplasia and carcinoma in situ. A recently described subset of oral dysplasia is positive for high-risk HPV. The epithelium exhibits full-thickness dysplastic changes with karyorrhexis and apoptosis and the cells are strongly positive for p16 by immunohistochemistry.71
Proliferative verrucous leukoplakia (PVL) is a distinct
form of oral precancer of unknown etiology with a multifocal presentation and a progressive course with high recurrence rates and malignant transformation in as many as 70% of cases.72,73 This diagnosis requires adequate clinical information. Subepithelial fibrosis is a characteristic of oral submucous fibrosis and increased
fibrosis is associated with an increased risk of epithelial dysplasia.74 Some inherited genetic mutations are associated with a higher risk of oral cancer development including Fanconi anemia, Li-Fraumeni syndrome and dyskeratosis congenita.46 Care must be taken to rule out reactive atypia which can be seen in epithelium adjacent to ulcers and with fungal infections.
G3.04 Radiation induced tissue damage can be recorded.
CG3.04a An observation regarding radiation induced tissue damage can be provided if the request form includes

19
history regarding neoadjuvant radiotherapy or recurrence in a previous radiotherapy field. Currently, there are no internationally standardised guidelines for evaluation of radiotherapy induced damage or whether this should influence any decisions regarding further radiotherapy. However, description of the radiotherapy induced tissue damage will allow collection of this data to develop evidence base for the future. Features such as stromal atypia, hyalinization, interstitial fibrosis, small vessel endothelial proliferation, and other
features may be mentioned.
G3.05 Any additional relevant comments should be recorded.
20
Figure 2. Measuring depth of invasion of an exophytic tumour.
Figure 3. Measuring depth of invasion of an ulcerative tumour.

21
Figure 4. Pattern of Invasive front. Copyright ICCR. Reproduced with
permission.
22
4 Ancillary studies findings
Ancillary studies may be used to determine lineage, clonality or disease classification or subclassification; as prognostic biomarkers; or to indicate the likelihood of patient response to specific biologic therapies. Research continues into various prognostic biomarkers, however at the present time there is no specific single or group of molecular markers that are used routinely in surgical practice to assist clinicians in predicting tumour behaviour or response to therapy
for their patients who have oral cancer.
The few ancillary tests that may be required in certain situations will be listed by technique. No ancillary tests are currently used on a routine basis for the diagnosis of oral cancer.
G4.01 Whether or not ancillary tests are performed should be recorded
and the results incorporated into the pathology report.
CG4.01a In most cases, further studies are not required for the diagnosis. Epithelial immunohistochemical markers may be required for poorly differentiated or spindle cell carcinoma including AE1/AE3, CK5/6, p63 and p40.75 Lymphoepithelial squamous cell carcinoma in the oral
cavity is rare and although not all cases are EBV-positive, Epstein-Barr virus (EBV)-encoded small RNAs (EBERs) studies are indicated.76 There is currently no role for routine HPV high risk type testing in oral squamous cell carcinoma.75-79
p16 and HPV in situ hybridisation (ISH) may be utilised
to distinguish HPV associated oral intraepithelial neoplasia from other forms of oral epithelial dysplasia.

23
5 Synthesis and overview
Information that is synthesised from multiple modalities and therefore cannot reside solely in any one of the preceding chapters is described here.
For example. tumour stage is synthesised from multiple classes of information – clinical, macroscopic and microscopic.
By definition, synthetic elements are inferential rather than observational, often representing high-level information that is likely to form part of the report ‘Summary’ or ‘Diagnosis’ section in the final formatted report.
Overarching case comment is synthesis in narrative format. Although it may not necessarily be required in any given report, the provision of the facility for overarching commentary in a cancer report is essential.
S5.01 The pathological pT tumour category must be recorded according to the AJCC TNM system (8th edition).14 Used with the permission of the American College of Surgeons, Chicago, Illinois. The original source for this information is the AJCC Cancer Staging Manual, Eighth Edition (2016) published by Springer Science+Business Media., www.springerlink.com.
CS5.01a By AJCC/UICC convention, the designation “T” refers to a primary tumour that has not been previously treated. Both staging systems integrate DOI into the T categories. Similar to skin malignancies, DOI is significantly associated with disease-free survival.80 Per the AJCC 8th edition, specific instructions are given to measure DOI.14 To measure DOI, the basement membrane is identified and an imaginary line is drawn across the tumour. A vertical or “plumb line” extends to the deepest part of the tumour which represents the DOI. It is important to note that DOI is not synonymous with tumour thickness. An exophytic
tumour may be thicker than an ulcerative tumour, but the DOI of the ulcerative lesion may be greater. An important point to highlight is that the UICC 8th edition does not specify how DOI should be measured.52 In addition as outlined in Note 8, UICC staging system is similar to the AJCC with one exception: if the tumour is >4 cm AND >10 mm DOI then the stage is T4a.52
Superficial erosion alone of bone/tooth socket by primary gingival tumour is not sufficient to classify a tumour as T4a which requires invasion into medullary bone.
Extranodal extension (ENE) is associated with adverse outcomes. ENE is defined as microscopic or macroscopic. Microscopic ENE is defined as ≤0.2 cm
whereas macroscopic ENE is defined as ENE clinically apparent at time of dissection or microscopic tumour extension >0.2 cm beyond the lymph node capsule.
24
S5.02 The year of publication and edition of the cancer staging system must be included in the report.
G5.01 The ‘Diagnostic summary’ section of the final formatted report should include:
a) Type of specimen
b) Anatomical site
c) Tumour type
d) Histological grade
e) Tumour dimensions
f) Depth of invasion
g) Pattern of invasion
h) Lymphovascular invasion
i) Perineural invasion
j) Bone invasion
k) Involved or close margins with measurements
S5.03 The reporting system must provide a field for free text or narrative in which the reporting pathologist can give overarching case comment, if required.
CS5.03a This field may be used, for example, to:
• explain the decision-making pathway, or any
elements of clinicopathological ambiguity, or factors affecting diagnostic certainty, thereby allowing communication of diagnostic subtlety or nuance that is beyond synoptic capture
• give recommendations for further action or investigation
• document further consultation or results still pending.
CS5.03b Use of this field is at the discretion of the reporting pathologist.
G5.02 The edition/version number of the RCPA protocol on which the
report is based should be included on the final report.
CG5.02a For example, the pathology report may include the following wording at the end of the report: “the data fields within this formatted report are aligned with the criteria as set out in the RCPA document “ XXXXXXXXXX” XXXX Edition dated XXXXXXX”.
25
6 Structured checklist
The following checklist includes the standards and guidelines for this protocol which must be considered when reporting, in the simplest possible form. The summation of all “Standards” is equivalent to the “Minimum Data Set” for tumours of the central nervous system. For emphasis, standards (mandatory elements) are formatted in bold font.
S6.01 The structured checklist provided below may be modified as required but with the following restrictions:
a. All standards and their respective naming conventions, definitions and value lists must be adhered to.
b. Guidelines are not mandatory but are recommendations and
where used, must follow the naming conventions, definitions and value lists given in the protocol.
G6.01 The order of information and design of the checklist may be varied according to the laboratory information system (LIS) capabilities and as described in Functional Requirements for Structured Pathology Reporting of Cancer Protocols.81
CG6.01a Where the LIS allows dissociation between data entry and report format, the structured checklist is usually best formatted to follow pathologist workflow. In this situation, the elements of synthesis or conclusions are necessarily at the end. The report format is then optimised independently by the LIS.
CG6.01b Where the LIS does not allow dissociation between data entry and report format, (for example where only a single text field is provided for the report), pathologists may elect to create a checklist in the format of the final report. In this situation, communication with the clinician takes precedence and the checklist design is according to principles given in
Chapter 7.
G6.02 Where the checklist is used as a report template (see G6.01), the principles in Chapter 7 and Appendix 2 apply.
CG6.02a All extraneous information, tick boxes and unused values should be deleted.
G6.03 Additional comment may be added to an individual response where necessary to describe any uncertainty or nuance in the selection of a prescribed response in the checklist. Additional comment is not required where the prescribed response is adequate.

26
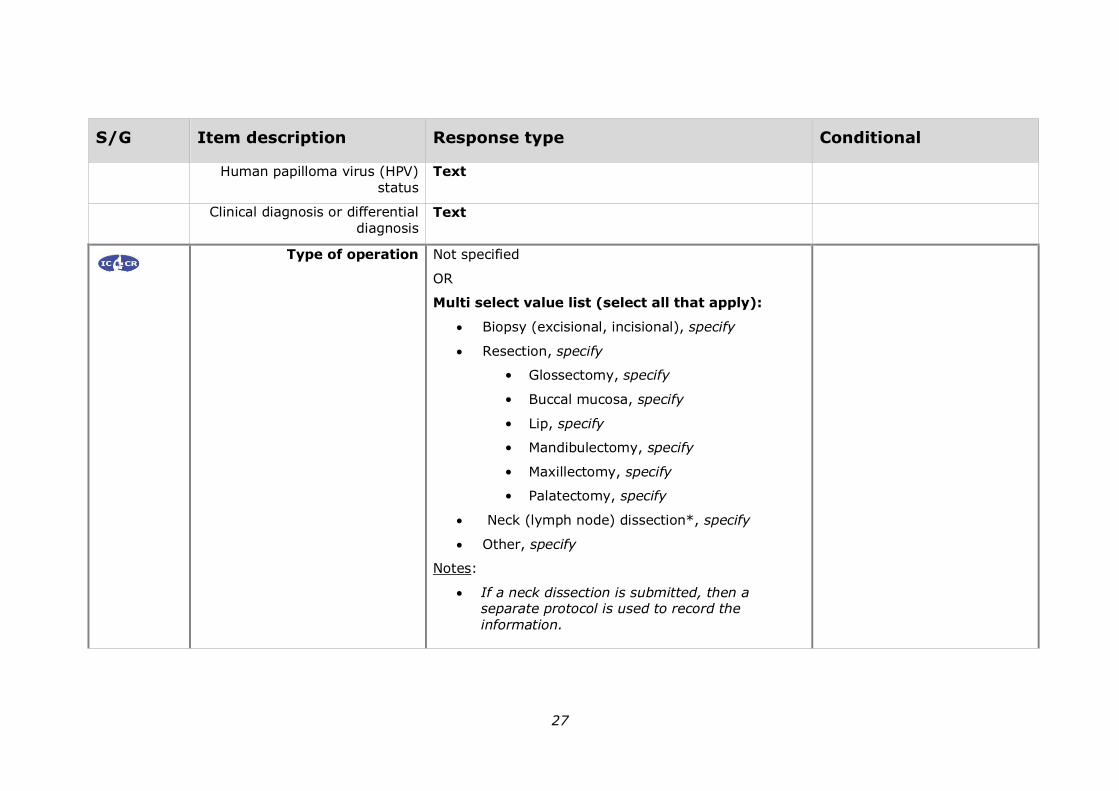
Values in italics are conditional on previous responses.
Values in all caps are headings with sub values.
S/G Item description Response type Conditional
Pre-analytical
S1.01 Demographic information provided
S1.02 Clinical information provided on request form
Not provided
OR
Text
OR
Structured entry as below:
CLINICAL INFORMATION
Anatomical site Text
Laterality of the lesion Single selection value list:
• Not stated
• Left
• Right
Clinical history Text
OR
Not stated
27
S/G Item description Response type Conditional
Human papilloma virus (HPV)
status
Text
Clinical diagnosis or differential diagnosis
Text
Type of operation Not specified
OR
Multi select value list (select all that apply):
• Biopsy (excisional, incisional), specify
• Resection, specify
• Glossectomy, specify
• Buccal mucosa, specify
• Lip, specify
• Mandibulectomy, specify
• Maxillectomy, specify
• Palatectomy, specify
• Neck (lymph node) dissection*, specify
• Other, specify
Notes:
• If a neck dissection is submitted, then a separate protocol is used to record the information.
28
S/G Item description Response type Conditional
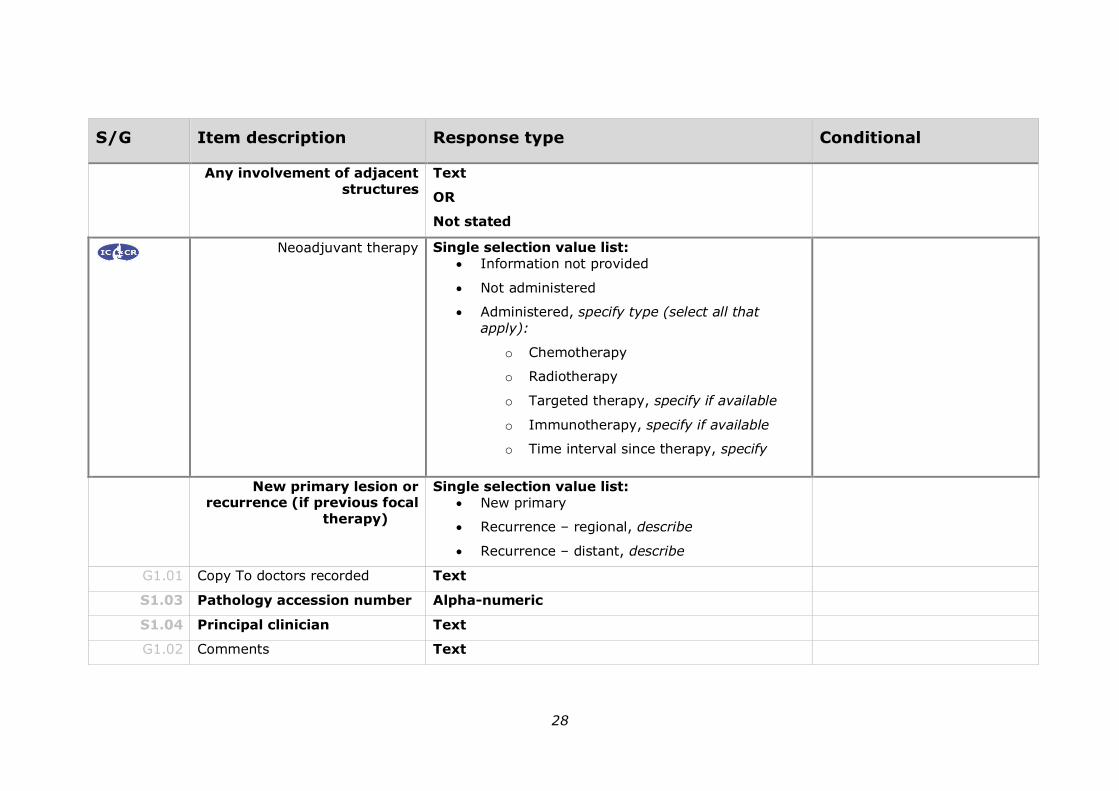
Any involvement of adjacent
structures
Text
OR
Not stated
Neoadjuvant therapy Single selection value list:
• Information not provided
• Not administered
• Administered, specify type (select all that apply):
o Chemotherapy
o Radiotherapy
o Targeted therapy, specify if available
o Immunotherapy, specify if available
o Time interval since therapy, specify
New primary lesion or recurrence (if previous focal
therapy)
Single selection value list:
• New primary
• Recurrence – regional, describe
• Recurrence – distant, describe
G1.01 Copy To doctors recorded Text
S1.03 Pathology accession number Alpha-numeric
S1.04 Principal clinician Text
G1.02 Comments Text

29
S/G Item description Response type Conditional
Macroscopic findings
S2.01 Specimen labelled as Text
S2.02 Type of operation Not specified
OR
Multi select value list (select all that apply):
• Biopsy (excisional, incisional), specify
• Resection, specify
• Glossectomy, specify
• Buccal mucosa, specify
• Lip, specify
• Mandibulectomy, specify
• Maxillectomy, specify
• Palatectomy, specify
• Neck (lymph node) dissection*, specify
• Other, specify
Notes:
• If a neck dissection is submitted, then a separate protocol is used to record the information.
S2.03 Specimens submitted Not specified
OR
30
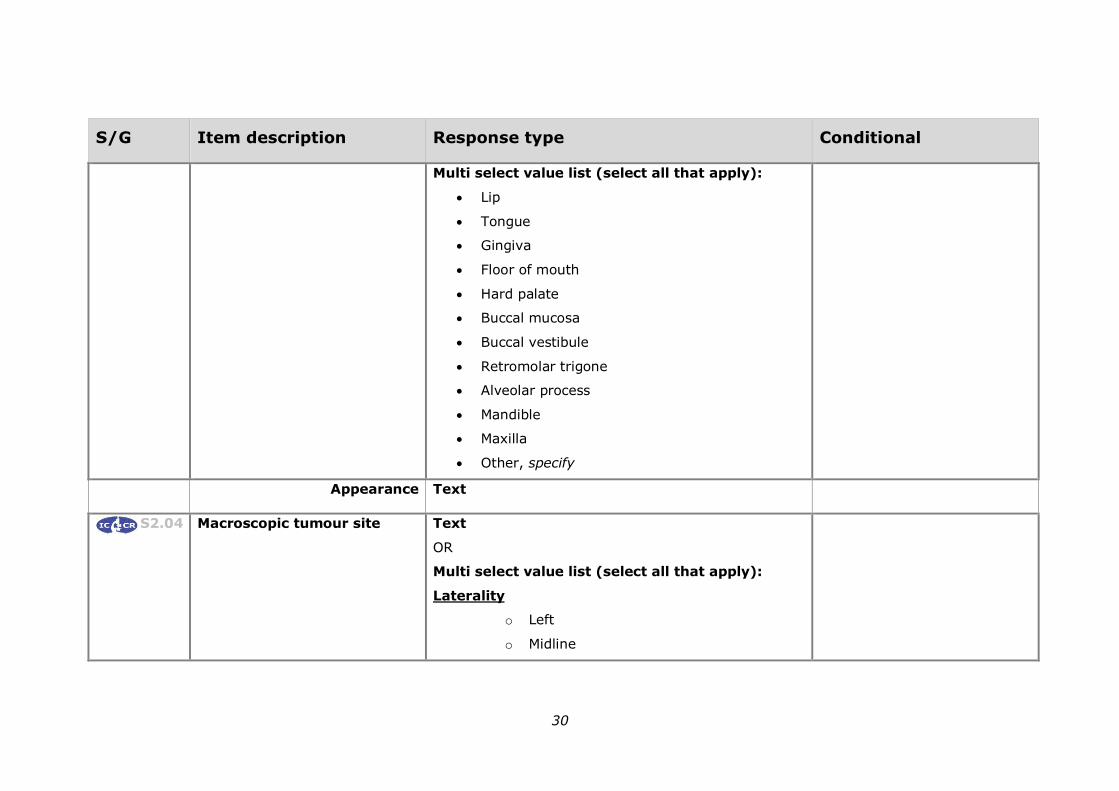
S/G Item description Response type Conditional
Multi select value list (select all that apply):
• Lip
• Tongue
• Gingiva
• Floor of mouth
• Hard palate
• Buccal mucosa
• Buccal vestibule
• Retromolar trigone
• Alveolar process
• Mandible
• Maxilla
• Other, specify
Appearance Text
S2.04 Macroscopic tumour site Text
OR
Multi select value list (select all that apply):
Laterality
o Left
o Midline

31
S/G Item description Response type Conditional
o Right
o Laterality not specified
• Lip
o Vermilion border upper lip
o Vermilion border lower lip
o Mucosa of upper lip
o Mucosa of lower lip
o Commissure of lip
• Oral cavity
o Lateral border of tongue
o Ventral surface of tongue
o Dorsal surface of tongue, NOS
o Anterior two-thirds of tongue, NOS
o Upper gingiva (gum)
o Anterior floor of mouth
o Floor of mouth, NOS
o Hard palate
o Buccal mucosa (inner cheek)
o Retromolar trigone
o Vestibule of mouth –
▪ Maxillary
32
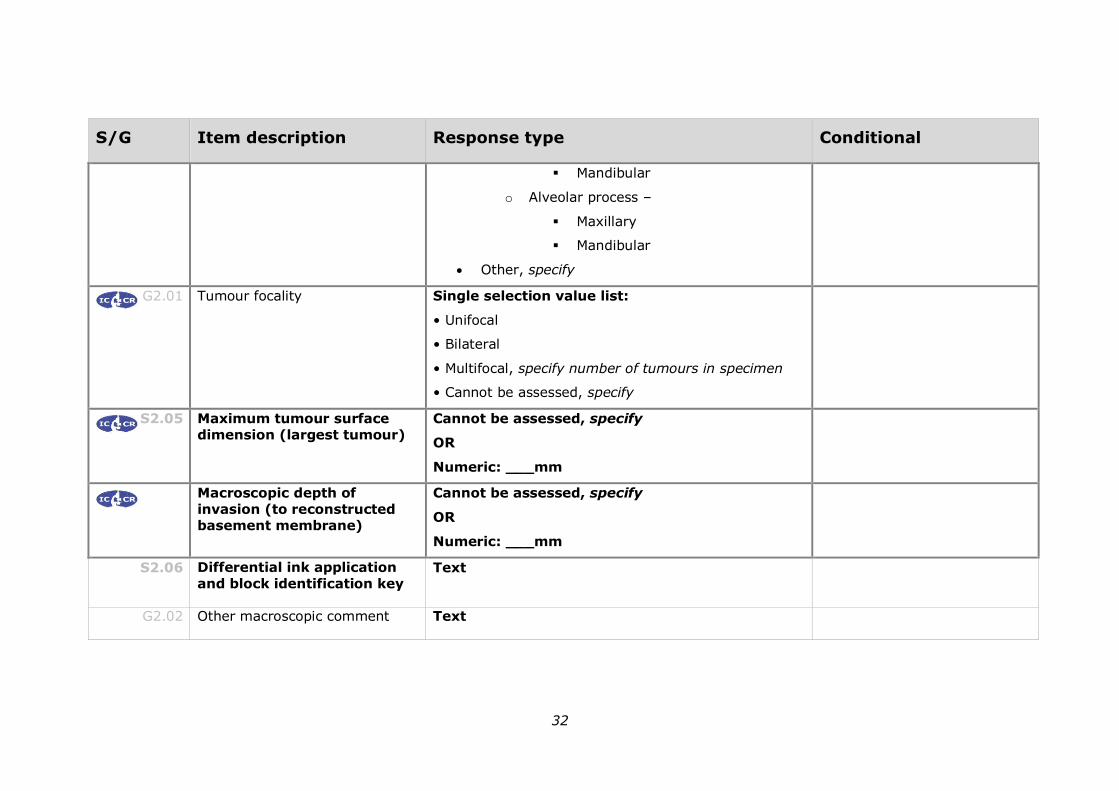
S/G Item description Response type Conditional
▪ Mandibular
o Alveolar process –
▪ Maxillary
▪ Mandibular
• Other, specify
G2.01 Tumour focality Single selection value list:
• Unifocal
• Bilateral
• Multifocal, specify number of tumours in specimen
• Cannot be assessed, specify
S2.05 Maximum tumour surface dimension (largest tumour)
Cannot be assessed, specify
OR
Numeric: ___mm
Macroscopic depth of
invasion (to reconstructed basement membrane)
Cannot be assessed, specify
OR
Numeric: ___mm
S2.06 Differential ink application
and block identification key Text
G2.02 Other macroscopic comment Text

33
S/G Item description Response type Conditional
Microscopic findings
S3.01 Tumour type Select value: Squamous cell carcinoma
OR
Salivary gland neoplasm
OR
Other
If other is specified, record the specific tumour type
If Squamous cell carcinoma
is selected record the tumour subtype.
Tumour type Text
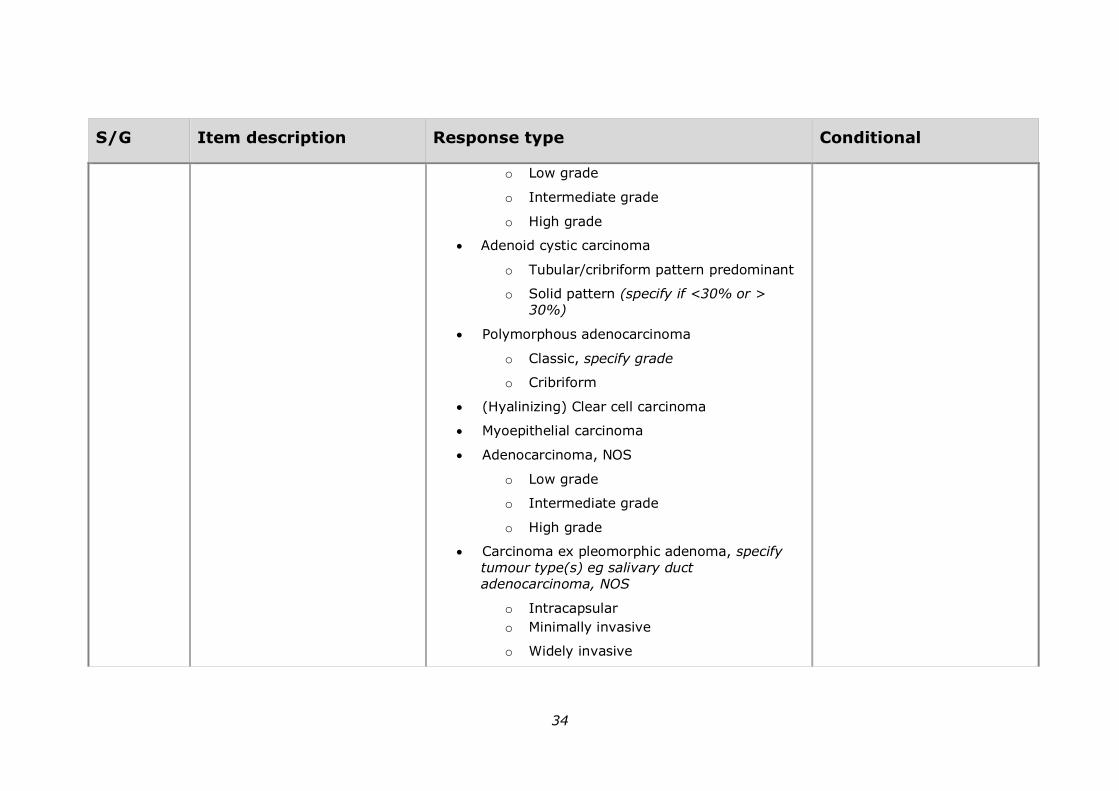
Tumour subtype Single selection value list:
• Squamous cell carcinoma
o Conventional
o Verrucous carcinoma
o Basaloid squamous cell carcinoma
o Papillary squamous cell carcinoma
o Spindle cell carcinoma
o Acantholytic squamous cell carcinoma
o Adenosquamous carcinoma
o Carcinoma cuniculatum
• Neuroendocrine carcinoma, specify type
• Secretory carcinoma
• Mucoepidermoid carcinoma
If other is specified, record the specific tumour subtype
34
S/G Item description Response type Conditional
o Low grade
o Intermediate grade
o High grade
• Adenoid cystic carcinoma
o Tubular/cribriform pattern predominant
o Solid pattern (specify if <30% or > 30%)
• Polymorphous adenocarcinoma
o Classic, specify grade
o Cribriform
• (Hyalinizing) Clear cell carcinoma
• Myoepithelial carcinoma
• Adenocarcinoma, NOS
o Low grade
o Intermediate grade
o High grade
• Carcinoma ex pleomorphic adenoma, specify tumour type(s) eg salivary duct
adenocarcinoma, NOS
o Intracapsular
o Minimally invasive
o Widely invasive
35
S/G Item description Response type Conditional
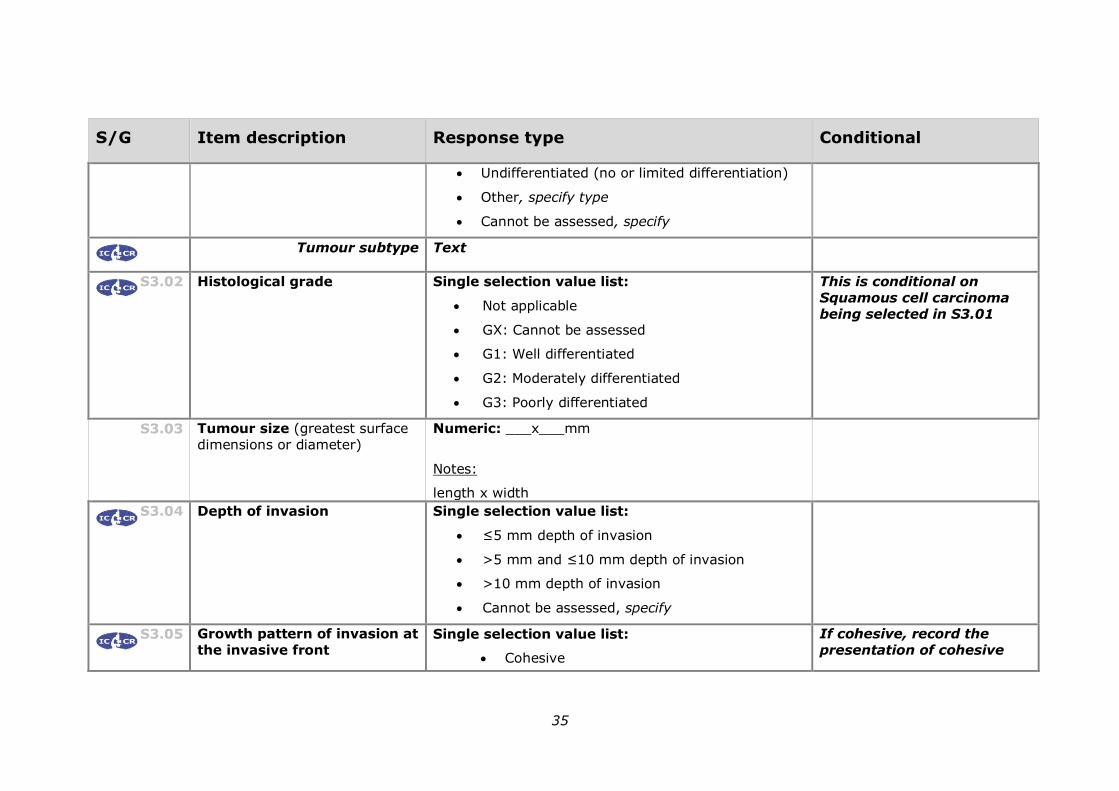
• Undifferentiated (no or limited differentiation)
• Other, specify type
• Cannot be assessed, specify
Tumour subtype Text
S3.02 Histological grade Single selection value list:
• Not applicable
• GX: Cannot be assessed
• G1: Well differentiated
• G2: Moderately differentiated
• G3: Poorly differentiated
This is conditional on Squamous cell carcinoma being selected in S3.01
S3.03 Tumour size (greatest surface dimensions or diameter)
Numeric: ___x___mm
Notes:
length x width
S3.04 Depth of invasion Single selection value list:
• ≤5 mm depth of invasion
• >5 mm and ≤10 mm depth of invasion
• >10 mm depth of invasion
• Cannot be assessed, specify
S3.05 Growth pattern of invasion at
the invasive front Single selection value list:
• Cohesive
If cohesive, record the
presentation of cohesive

36
S/G Item description Response type Conditional
• Non-cohesive
• Widely dispersed
cells.
If non-cohesive record the presentation of noncohesive cells.
Presentation of cohesive cells
Multi select value list (select all that apply):
• Broad bulbous islands of cells
• Strands of cells (>15 cells across)
Presentation of non-cohesive cells
Multi select value list (select all that apply):
• Narrow strands or small islands of infiltrating cells
• Single infiltrating keratinocytes
G3.01 Response to neoadjuvant therapy
Single selection value list:
• No prior treatment
• Incomplete response
• Complete response
• Response cannot be assessed, explain reasons
S3.06 Lymphovascular invasion Single selection value list:
• Not identified
• Present
• Cannot be assessed, specify
37
S/G Item description Response type Conditional
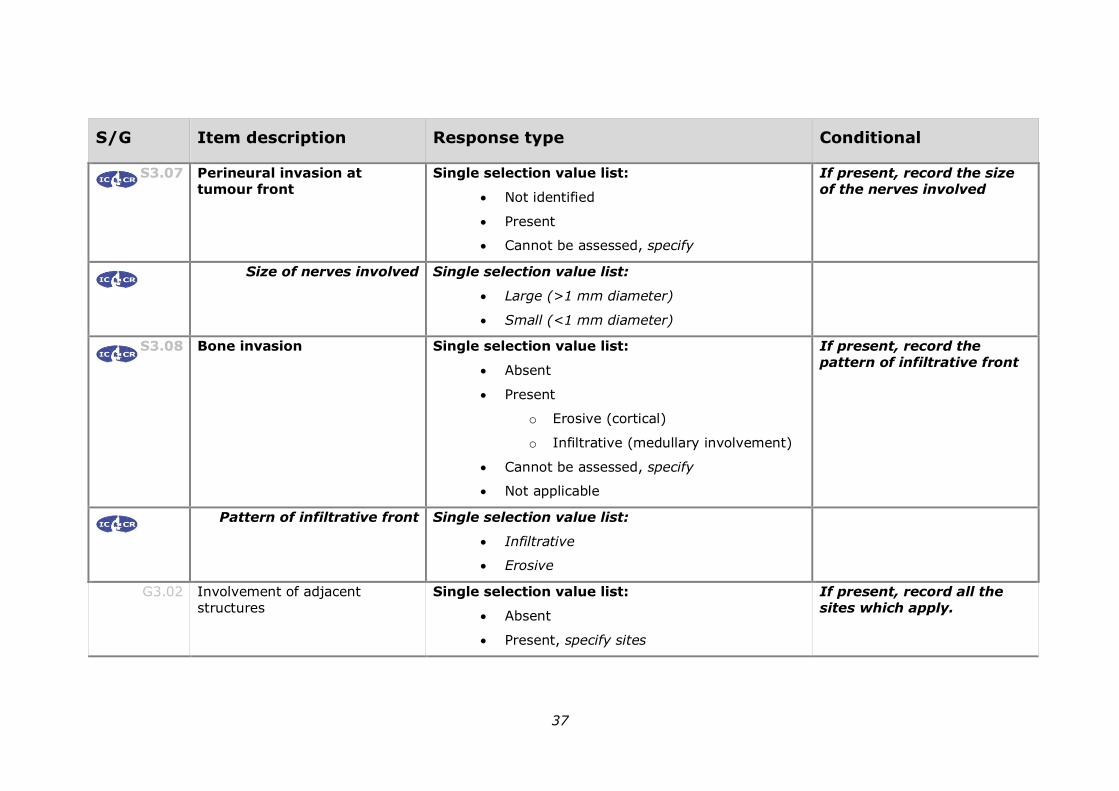
S3.07 Perineural invasion at
tumour front
Single selection value list:
• Not identified
• Present
• Cannot be assessed, specify
If present, record the size
of the nerves involved
Size of nerves involved Single selection value list:
• Large (>1 mm diameter)
• Small (<1 mm diameter)
S3.08 Bone invasion Single selection value list:
• Absent
• Present
o Erosive (cortical)
o Infiltrative (medullary involvement)
• Cannot be assessed, specify
• Not applicable
If present, record the pattern of infiltrative front
Pattern of infiltrative front Single selection value list:
• Infiltrative
• Erosive
G3.02 Involvement of adjacent structures
Single selection value list:
• Absent
• Present, specify sites
If present, record all the sites which apply.
38
S/G Item description Response type Conditional
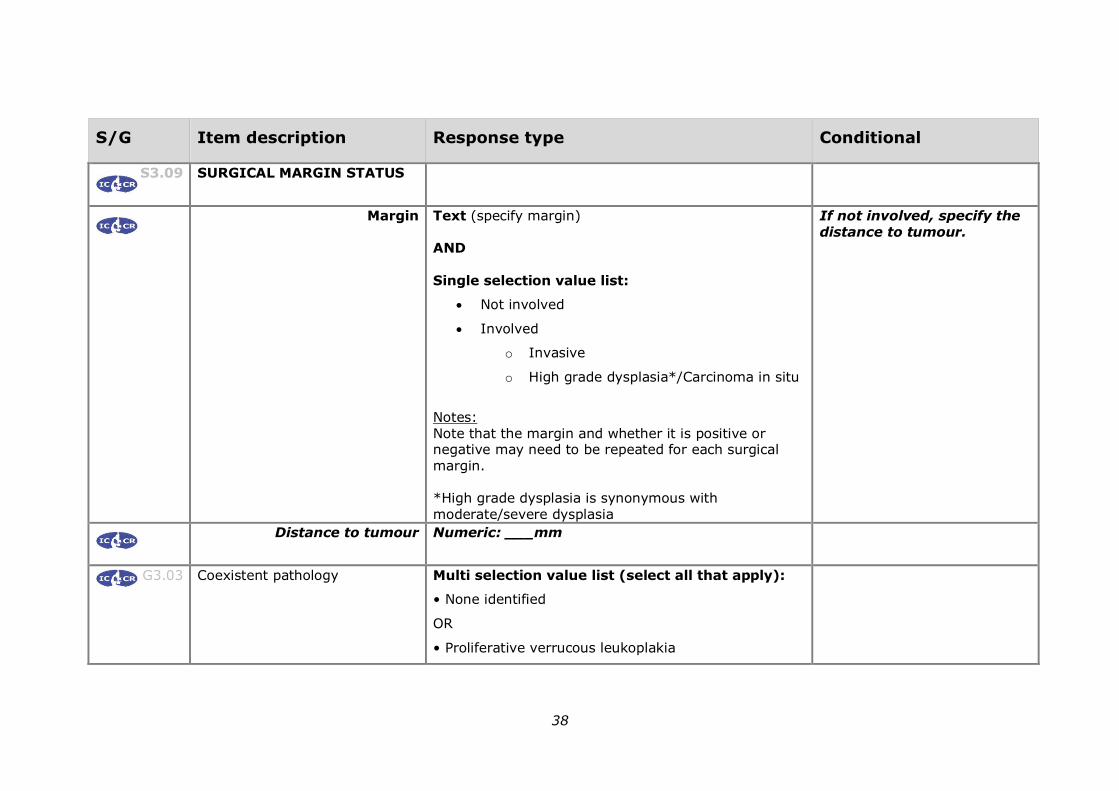
S3.09 SURGICAL MARGIN STATUS
Margin Text (specify margin) AND
Single selection value list:
• Not involved
• Involved
o Invasive
o High grade dysplasia*/Carcinoma in situ
Notes: Note that the margin and whether it is positive or negative may need to be repeated for each surgical margin. *High grade dysplasia is synonymous with moderate/severe dysplasia
If not involved, specify the distance to tumour.
Distance to tumour Numeric: ___mm
G3.03 Coexistent pathology Multi selection value list (select all that apply):
• None identified
OR
• Proliferative verrucous leukoplakia

39
S/G Item description Response type Conditional
• Fungal infection
• Dysplasia, specify grade
• HPV positive dysplasia
• Submucous fibrosis
• Inflammation
• Other, specify
G3.04 Radiation induced tissue damage Single selection value list:
• Not identified
• Identified, specify
• Cannot be assessed, specify
If identified, specify a description of induced
damage, if possible.
If cannot be assessed, specify a reason, if possible.
G3.05 Other microscopic comment Text
Ancillary test findings
G4.01 IMMUNOHISTOCHEMICAL STAINS
Performed Single selection value list:
• No
• Yes
If yes, record antibodies, interpretation and clinical significance.
Antibodies List (as applicable):

40
S/G Item description Response type Conditional
• Positive
• Negative
• Equivocal
Interpretation Text
Clinical significance Text
IN SITU HYBRIDISATION
Performed Single selection value list:
• No
• Yes
If yes, record performing lab, results, conclusions and person responsible for reporting.
Performing laboratory Text
Result Text
Conclusion Text
Person responsible for reporting Text
CYTOGENETICS
Performed Single selection value list:
• No
• Yes
If yes, record performing lab, results, conclusions and person responsible for
reporting.

41
S/G Item description Response type Conditional
Performing laboratory Text
Result Text
Conclusion Text
Person responsible for reporting Text
Synthesis and overview
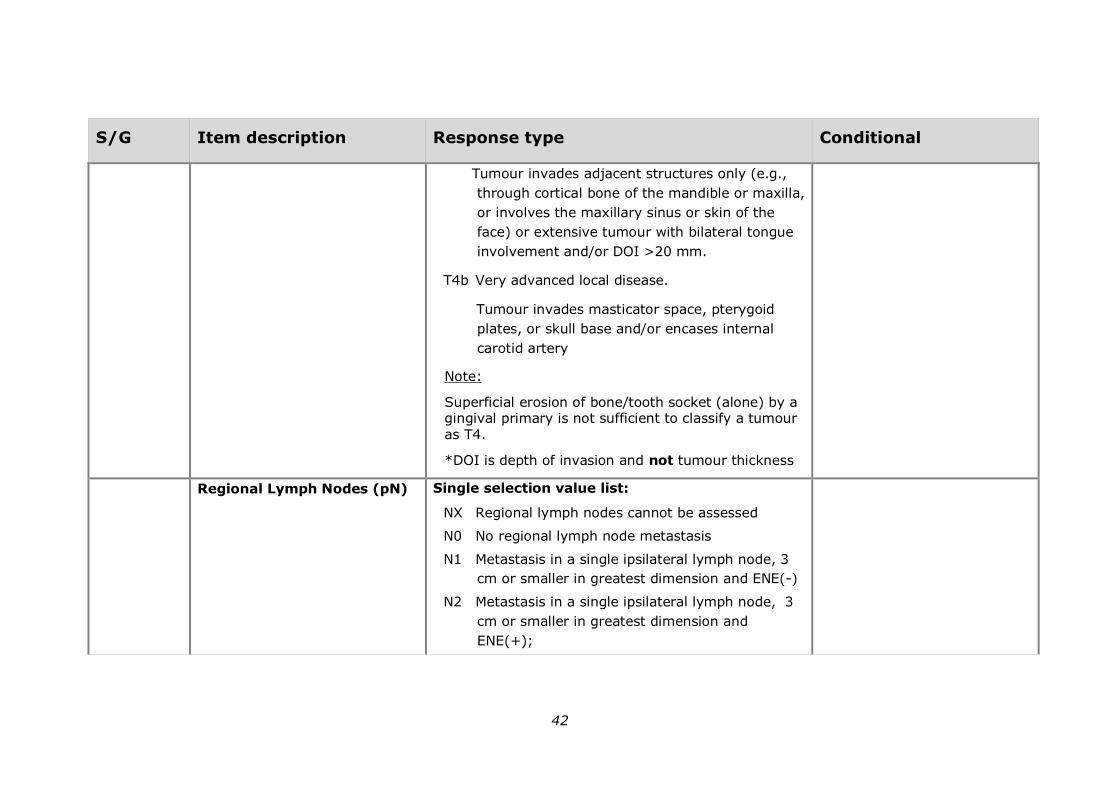
S5.01 AJCC TUMOUR STAGING (AJCC 8TH EDITION)
Primary Tumour (pT) Single selection value list:
TX Primary tumour cannot be assessed
Tis Carcinoma in situ
T1 Tumour <2 cm with depth of invasion (DOI)*
<5mm
T2 Tumour <2 cm, with DOI* >5 mm or tumour >2
cm and <4cm, with DOI* <10mm
T3 Tumour >4 cm
or any tumour with DOI >10 mm but <20 mm
T4 Moderately advanced or very advanced local
disease
T4a Moderately advanced local disease.
42
S/G Item description Response type Conditional
Tumour invades adjacent structures only (e.g.,
through cortical bone of the mandible or maxilla,
or involves the maxillary sinus or skin of the
face) or extensive tumour with bilateral tongue
involvement and/or DOI >20 mm.
T4b Very advanced local disease.
Tumour invades masticator space, pterygoid
plates, or skull base and/or encases internal
carotid artery
Note:
Superficial erosion of bone/tooth socket (alone) by a gingival primary is not sufficient to classify a tumour as T4.
*DOI is depth of invasion and not tumour thickness
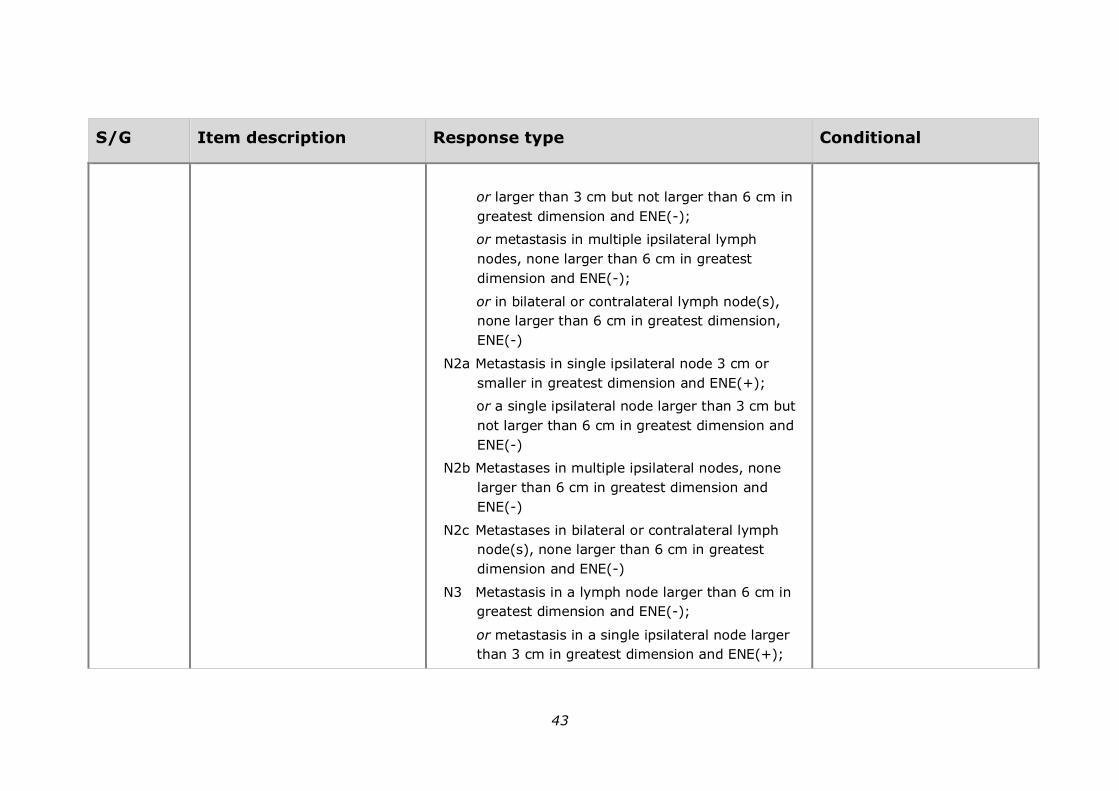
Regional Lymph Nodes (pN)
Single selection value list:
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node, 3
cm or smaller in greatest dimension and ENE(-)
N2 Metastasis in a single ipsilateral lymph node, 3
cm or smaller in greatest dimension and
ENE(+);
43
S/G Item description Response type Conditional
or larger than 3 cm but not larger than 6 cm in
greatest dimension and ENE(-);
or metastasis in multiple ipsilateral lymph
nodes, none larger than 6 cm in greatest
dimension and ENE(-);
or in bilateral or contralateral lymph node(s),
none larger than 6 cm in greatest dimension,
ENE(-)
N2a Metastasis in single ipsilateral node 3 cm or
smaller in greatest dimension and ENE(+);
or a single ipsilateral node larger than 3 cm but
not larger than 6 cm in greatest dimension and
ENE(-)
N2b Metastases in multiple ipsilateral nodes, none
larger than 6 cm in greatest dimension and
ENE(-)
N2c Metastases in bilateral or contralateral lymph
node(s), none larger than 6 cm in greatest
dimension and ENE(-)
N3 Metastasis in a lymph node larger than 6 cm in
greatest dimension and ENE(-);
or metastasis in a single ipsilateral node larger
than 3 cm in greatest dimension and ENE(+);
44
S/G Item description Response type Conditional
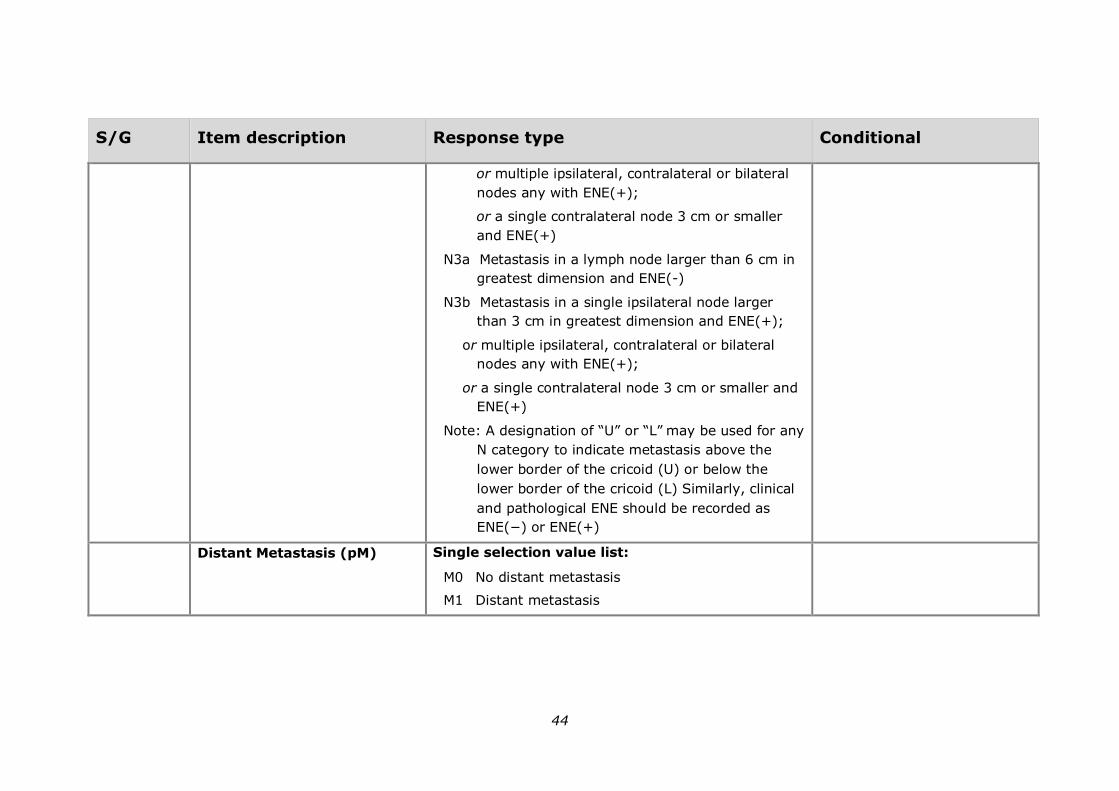
or multiple ipsilateral, contralateral or bilateral
nodes any with ENE(+);
or a single contralateral node 3 cm or smaller
and ENE(+)
N3a Metastasis in a lymph node larger than 6 cm in
greatest dimension and ENE(-)
N3b Metastasis in a single ipsilateral node larger
than 3 cm in greatest dimension and ENE(+);
or multiple ipsilateral, contralateral or bilateral
nodes any with ENE(+);
or a single contralateral node 3 cm or smaller and
ENE(+)
Note: A designation of “U” or “L” may be used for any
N category to indicate metastasis above the
lower border of the cricoid (U) or below the
lower border of the cricoid (L) Similarly, clinical
and pathological ENE should be recorded as
ENE(−) or ENE(+)
Distant Metastasis (pM)
Single selection value list:
M0 No distant metastasis
M1 Distant metastasis
45
S/G Item description Response type Conditional
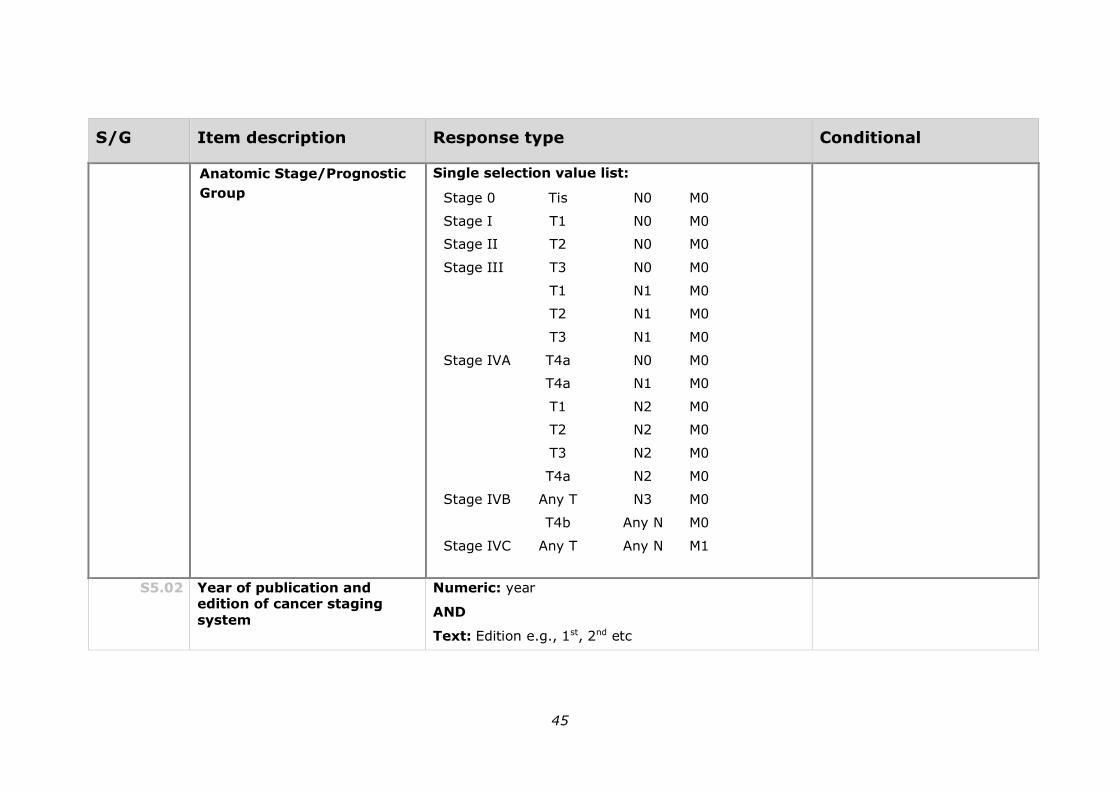
Anatomic Stage/Prognostic
Group
Single selection value list:
Stage 0 Tis N0 M0
Stage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB Any T N3 M0
T4b Any N M0
Stage IVC Any T Any N M1
S5.02 Year of publication and edition of cancer staging system
Numeric: year
AND
Text: Edition e.g., 1st, 2nd etc

46
S/G Item description Response type Conditional
G5.01 Diagnostic summary
Include:
a) Type of specimen
b) Anatomical site
c) Tumour type
d) Histological grade
e) Tumour dimensions
f) Depth of invasion
g) Pattern of invasion
h) Lymphovascular invasion
i) Perineural invasion
j) Bone invasion
k) Involved or close margins with measurements
Text
S5.03 Overarching comment Text
G5.02 Edition/version number of the RCPA protocol on which the
report is based
Text

47
7 Formatting of pathology reports
Good formatting of the pathology report is essential for optimising communication with the clinician, and will be an important contributor to the success of cancer reporting protocols. The report should be formatted to provide information clearly and unambiguously to the treating doctors, and should be organised with their use of the report in mind. In this sense, the report differs from the structured checklist, which is organised with the pathologists’ workflow as a priority.
Uniformity in the format as well as in the data items of cancer reports between laboratories makes it easier for treating doctors to understand the reports; it is therefore seen as an important element of the systematic reporting of cancer. For guidance on formatting pathology reports, please refer to Appendix 2.
48
Appendix 1 Pathology request form
This appendix describes the information that should be collected before the pathology test. Some of this information can be provided on generic pathology request forms; any additional information required specifically for the reporting of Carcinoma of the oral cavity may be provided by the clinician on a separate request information sheet. An example request information sheet is included below. Elements which are in bold text are those which pathologists consider to
be required information. Those in non-bold text are recommended.
Also included in this appendix are the procedures that are recommended before handover of specimens to the laboratory.
Patient information
➢ Adequate demographic and request information should be provided with the specimen.
• Items relevant to cancer reporting protocols include:
• patient name
• date of birth
• sex
• identification and contact details of requesting doctor
• date of request
• Document whether or not the patient identifies as Aboriginal and/ or Torres Strait Islander in Australia, or Māori in New Zealand. This is in support of government initiatives to monitor the health of those who identify as indigenous, particularly in relation to cancer.
➢ The patient’s health identifiers should be provided.
• The patient’s health identifiers may include the patient’s Medical Record Number as well as a national health number such as a patient’s Individual Healthcare Identifier (IHI) (Australia) or the National Healthcare Identifier (New Zealand).
➢ The Australian Healthcare identifiers i.e., Healthcare Provider Identifier - Individual (HPI-I) and Healthcare Provider Identifier - Organisation (HPI-O) should be use, where possible, to identify the requesting doctor.
Clinical Information
➢ The anatomical site of the biopsy or resection must be recorded.

49
• Site is an important identifier especially when multiple biopsies are performed. For carcinomas that may involve more than one site it is recommended that the clinician
identify all sites involved and that if possible the principal site of involvement be recorded.
Sufficient information is required to localise the lesion for subsequent therapy. A diagram or photograph can facilitate this.
Prognostic significance – the association between anatomical
site and survival may be explained by the tumours site’s influence on metastasis to cervical lymph nodes.15-16
➢ The laterality of the lesion must be recorded.
• Laterality information is needed for identification purposes
➢ Clinical history should be recorded.
➢ The clinical diagnosis or differential diagnosis should be recorded.
• Providing the provisional clinical diagnosis or differential diagnosis improves clinico-pathological correlation and
improves diagnostic accuracy.
➢ The type of operation performed must be recorded.
• The type of operation performed will influence the subsequent handling of the specimen in the laboratory.
➢ Preoperative radiological/imaging reports should ideally be
available for review during pathological reporting of the surgical specimen, and key elements should be included with the clinical details (e.g., site and size).
➢ Any involvement of adjacent structures must be recorded.
• With regard to extension of disease into areas which either
have or have not been resected (i.e., involvement of other tissues such as salivary glands by direct spread), it is the responsibility of the surgeon to report these deposits and, if indicated, mark these areas with a suture or other marker.
➢ Any neoadjuvant therapy administered should be recorded.
• There is no agreed upon system for grading tumour regression in oral squamous cell carcinoma that has been treated with neoadjuvant therapy. However, a history of previous radiotherapy and/or chemotherapy should be included as histologic changes related to the therapy such as necrosis may affect interpretation of the tumour.
➢ Record if this is a new primary cancer or a recurrence of a previous cancer, if known
• The term recurrence defines the return, reappearance or metastasis of cancer (of the same histology) after a disease-
50
free period.
Recurrence should be classified as distant metastases or regional (local) recurrence.
Regional (local) recurrence refers to the recurrence of cancer cells at the same site as the original (primary) tumour or the regional lymph nodes.
Distant metastasis refers to the spread of cancer of the same histologic type as the original (primary) tumour to distant organs or distant lymph nodes.
This information will provide an opportunity for previous reports to be reviewed during the reporting process, which may provide valuable information to the pathologist. This information also has implications for recording cancer incidence and evidence-based research.
➢ Comments should be included, if appropriate.
• Space for free text should be included to encourage reporting of ambiguity, or for the addition of other comments.
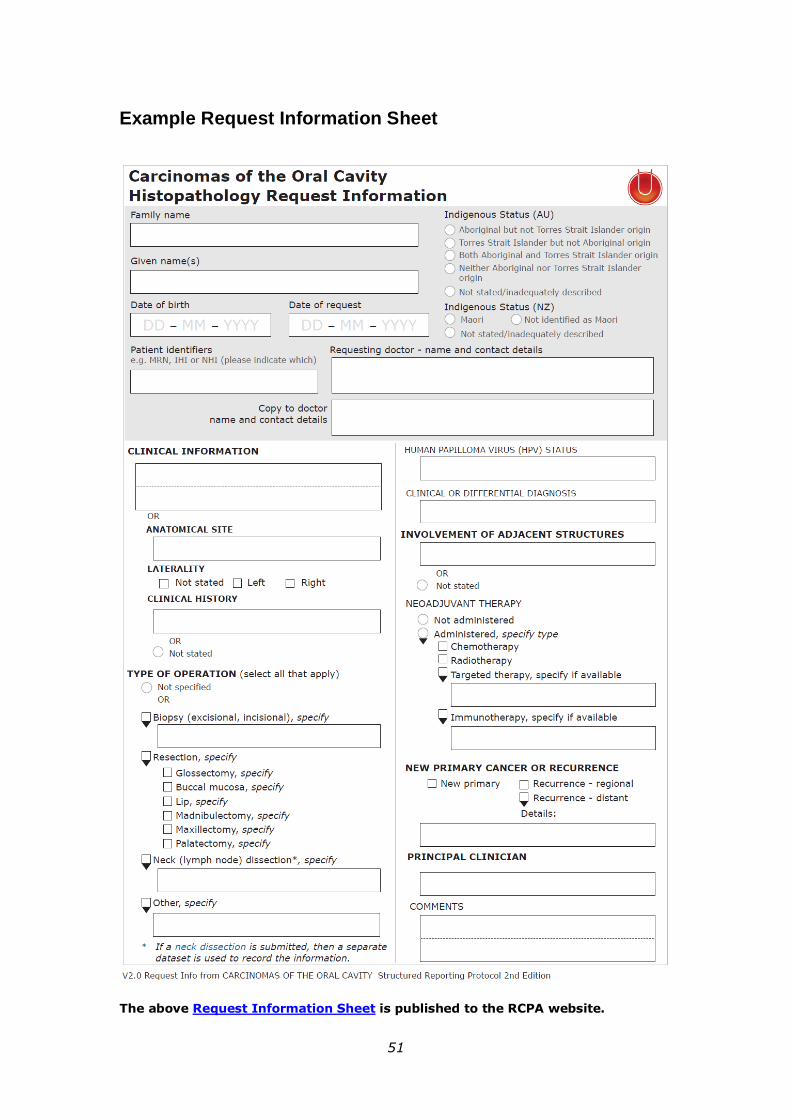
51
Example Request Information Sheet
The above Request Information Sheet is published to the RCPA website.

52
Appendix 2 Guidelines for formatting of a pathology report
Layout
Headings and spaces should be used to indicate subsections of the report, and heading hierarchies should be used where the Laboratory Information System
(LIS) allows it. Heading hierarchies may be defined by a combination of case, font size, style and, if necessary, indentation.
• Grouping similar data elements under headings and using ‘white space’ assists in rapid transfer of information.82
Descriptive titles and headings should be consistent across the protocol, checklist
and report.
When reporting on different tumour types, similar layout of headings and blocks of data should be used, and this layout should be maintained over time.
• Consistent positioning speeds data transfer and, over time, may reduce the need for field descriptions or headings, thus reducing unnecessary information or ‘clutter’.
Within any given subsection, information density should be optimised to assist in data assimilation and recall.
• Configuring reports in such a way that they ‘chunk’ data elements into a single unit will help to improve recall for the clinician.82
• ‘Clutter’ should be reduced to a minimum.82 Thus, information that is
not part of the protocol (e.g. billing information, Snomed codes, etc) should not appear on the reports or should be minimized.
• Injudicious use of formatting elements (e.g. too much bold, underlining or use of footnotes) constitutes clutter and may distract the reader from the key information.
Where a structured report checklist is used as a template for the actual report, any values provided in the checklist but not applying to the case in question must be deleted from the formatted report.
Reports should be formatted with an understanding of the potential for the information to mutate or be degraded as the report is transferred from the LIS to other health information systems.
As a report is transferred between systems:
• text characteristics such as font type, size, bold, italics and colour are often lost
• tables are likely to be corrupted as vertical alignment of text is lost when fixed font widths of the LIS are rendered as proportional fonts on
screen or in print
• spaces, tabs and blank lines may be stripped from the report, disrupting the formatting
• supplementary reports may merge into the initial report.
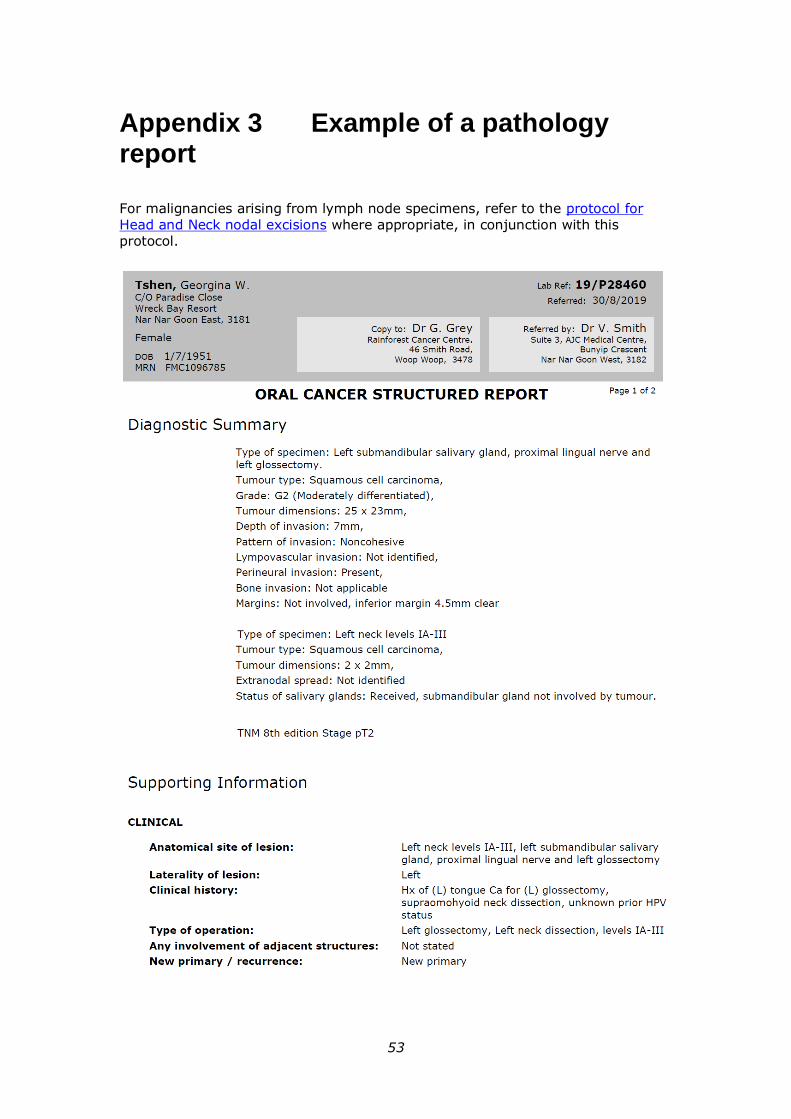
53
Appendix 3 Example of a pathology report
For malignancies arising from lymph node specimens, refer to the protocol for Head and Neck nodal excisions where appropriate, in conjunction with this protocol.
54

55

56
Appendix 4 WHO classification of tumours
WHO classification of tumours of the oral cavity and mobile tongue46a
Descriptor ICD-O
codes
Epithelial tumours and lesions
Squamous cell carcinoma 8070/3
Oral epithelial dysplasia
Low grade 8077/0
High grade 8077/2
a The morphology codes are from the International Classification of Diseases for Oncology (ICD-O). Behaviour is coded /0 for benign tumours; /1 for unspecified, borderline, or uncertain behaviour; /2 for carcinoma in situ and grade III intraepithelial neoplasia; and /3 for malignant tumours
© WHO/International Agency for Research on Cancer (IARC). Reproduced with permission.

57
References
1 Merlin T, Weston A and Tooher R (2009). Extending an evidence hierarchy to include topics other than treatment: revising the Australian 'levels of evidence'. BMC Med Res Methodol 9:34.
2 Macfarlane G, Sharp L, Porter S, Franceschi S and (1996). Trends in
survival from cancer of the oral cavity and pharynx in Scotland: A clue to why the disease is becoming more common. Br J Cancer 73:805-808.
3 Australian Institute of Health and Welfare (2014). Head and neck cancers in Australia. AIHW Cancer series no. 83. https://www.aihw.gov.au/getmedia/bdccebf2-dbe6-44e2-9104-
8461d7e7c165/16933.pdf.aspx?inline=true
4 Australian Cancer Network Colorectal Cancer Guidelines Revision Committee (2005). Guidelines for the Prevention, Early Detection and Management of Colorectal Cancer. The Cancer Council Australia and Australian Cancer Network, Sydney.
5 Maughan NJ, Morris E, Forman D and Quirke P (2007). The validity of the Royal College of Pathologists' colorectal cancer minimum dataset within a population. Br J Cancer 97(10):1393–1398.
6 Royal College of Pathologists (2017). Cancer datasets and tissue pathways. Available from: https://www.rcpath.org/profession/publications/cancer-datasets.html. (Accessed 19th Dec 2017).
7 CAP (College of American Pathologists) (2015). Cancer protocol templates. Available from: https://www.cap.org/protocols-and-guidelines/cancer-reporting-tools/cancer-protocol-templates. (Accessed 19th Feb 2019).
8 Cross SS, Feeley KM and Angel CA (1998). The effect of four interventions on the informational content of histopathology reports of resected colorectal carcinomas. J Clin Oncol 51(6):481–482.
9 Mathers M, Shrimankar J, Scott D, Charlton F, Griffith C and Angus B (2001). The use of a standard proforma in breast cancer reporting. J Clin Pathol 54(10):809–811.
10 Srigley JR, McGowan T, MacLean A, Raby M, Ross J, Kramer S and Sawka C (2009). Standardized synoptic cancer pathology reporting: A population-based approach. J Surg Oncol 99(8):517–524.
58
11 Gill AJ, Johns AL, Eckstein R, Samra JS, Kaufman A, Chang DK, Merrett ND, Cosman PH, Smith RC, Biankin AV and Kench JG (2009). Synoptic reporting improves histopathological assessment of pancreatic resection specimens. Pathology 41(2):161–167.
12 RCPA (Royal College of Pathologists of Australasia (2009). Guidelines for Authors of Structured Cancer Pathology Reporting Protocols. RCPA, Surry Hills NSW.
13 World Health Organization (WHO) (2017). Classification of Head and Neck Tumours, 4th Edition. El-Naggar AK, Chan JKC, Grandis JR, Takata T and Slootweg PJ. IARC, Lyon.
14 Amin MB, Edge SB, Greene FL, Byrd DR, Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR, Sullivan DC, Jessup JM, Brierley JD, Gaspar LE, Schilsky RL, Balch CM, Winchester DP, Asare EA, Madera M, Gress DM and Meyer LR (eds) (2017). AJCC Cancer Staging Manual. 8th ed., Springer, New York.
15 RCPA (Royal College of Pathologists of Australasia) (2004). Chain of Information Custody for the Pathology Request-Test-Report Cycle — Guidelines for Requesters and Pathology Providers. RCPA, Surry Hills, NSW.
16 Jerjes W, Upile T, Petrie A, Riskalla A, Hamdoon Z, Vourvachis M, Karavidas K, Jay A, Sandison A, Thomas GJ, Kalavrezos N and Hopper C (2010).
Clinicopathological parameters, recurrence, locoregional and distant metastasis in 115 T1-T2 oral squamous cell carcinoma patients. Head Neck Oncol 2:9.
17 Rapidis AD, Gullane P, Langdon JD, Lefebvre JL, Scully C and Shah JP (2009). Major advances in the knowledge and understanding of the epidemiology, aetiopathogenesis, diagnosis, management and prognosis of oral cancer. Oral
Oncol 45(4-5):299-300.
18 Shah JP and Gil Z (2009). Current concepts in management of oral cancer--surgery. Oral Oncol 45(4-5):394-401.
19 Nakhleh RE (2011). Quality in surgical pathology communication and reporting. Arch Pathol Lab Med 135(11):1394-1397.
20 Nakhleh RE, Myers JL, Allen TC, DeYoung BR, Fitzgibbons PL, Funkhouser WK, Mody DR, Lynn A, Fatheree LA, Smith AT, Lal A and Silverman JF (2012). Consensus statement on effective communication of urgent diagnoses and significant, unexpected diagnoses in surgical pathology and cytopathology from the College of American Pathologists and Association of Directors of Anatomic and Surgical Pathology. Arch Pathol Lab Med 136(2):148-154.

59
21 Dissanayaka WL, Jayasooriya PR, Kumarasiri PV and Tilakaratne WM (2010). A histopathologic comparison between synchronous and single primary oral squamous cell carcinomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109(5):732-738.
22 Bedi GC, Westra WH, Gabrielson E, Koch W and Sidransky D (1996). Multiple head and neck tumors: evidence for a common clonal origin. Cancer Res 56(11):2484-2487.
23 Feng Z, Xu QS, Niu QF, Qin LZ, Li JZ, Su M, Li H and Han Z (2016). Risk factors for patients with multiple synchronous primary cancers involving oral and oropharyngeal subsites. Oral Surg Oral Med Oral Pathol Oral Radiol 121(4):360-366.
24 Bagan JV, Murillo J, Poveda R, Gavalda C, Jimenez Y and Scully C (2004). Proliferative verrucous leukoplakia: unusual locations of oral squamous cell carcinomas, and field cancerization as shown by the appearance of multiple OSCCs. Oral Oncol 40(4):440-443.
25 Spiro RH, Huvos AG, Wong GY, Spiro JD, Gnecco CA and Strong EW (1986). Predictive value of tumor thickness in squamous carcinoma confined to the tongue and floor of the mouth. Am J Surg 152(4):345-350.
26 Dhanda J, Uppal N, Chowlia H, Opie N, Al-Qamachi L, Shelat D, Aslam A, Yuffa A, Martin T, Risk J, Triantafyllou A, Shaw R, Parmar S and Mehanna H
(2016). Features and prognostic utility of biopsy in oral squamous cell carcinoma. Head Neck 38 Suppl 1:E1857-1862.
27 Ebrahimi A, Murali R, Gao K, Elliott MS and Clark JR (2011). The prognostic and staging implications of bone invasion in oral squamous cell carcinoma. Cancer 117(19):4460-4467.
28 Shim SJ, Cha J, Koom WS, Kim GE, Lee CG, Choi EC and Keum KC (2010). Clinical outcomes for T1-2N0-1 oral tongue cancer patients underwent surgery with and without postoperative radiotherapy. Radiat Oncol 5:43.
29 D'Cruz AK, Vaish R, Kapre N, Dandekar M, Gupta S, Hawaldar R, Agarwal JP, Pantvaidya G, Chaukar D, Deshmukh A, Kane S, Arya S, Ghosh-Laskar S, Chaturvedi P, Pai P, Nair S, Nair D and Badwe R (2015). Elective versus Therapeutic Neck Dissection in Node-Negative Oral Cancer. N Engl J Med 373(6):521-529.
30 Byers RM, El-Naggar AK, Lee YY, Rao B, Fornage B, Terry NH, Sample D, Hankins P, Smith TL and Wolf PJ (1998). Can we detect or predict the presence of occult nodal metastases in patients with squamous carcinoma of the oral tongue? Head Neck 20(2):138-144.
60
31 Tan WJ, Chia CS, Tan HK, Soo KC and Iyer NG (2012). Prognostic significance of invasion depth in oral tongue squamous cell carcinoma. ORL J
Otorhinolaryngol Relat Spec 74(5):264-270.
32 Kang CJ, Lin CY, Wang HM, Fan KH, Ng SH, Lee LY, Chen IH, Huang SF, Liao CT and Yen TC (2011). The number of pathologically positive lymph nodes and pathological tumor depth predicts prognosis in patients with poorly differentiated squamous cell carcinoma of the oral cavity. Int J Radiat Oncol Biol
Phys 81(4):e223-230.
33 Pentenero M, Gandolfo S and Carrozzo M (2005). Importance of tumor thickness and depth of invasion in nodal involvement and prognosis of oral squamous cell carcinoma: a review of the literature. Head Neck 27(12):1080-1091.
34 Patel KR, Chernock RD, Sinha P, Muller S, El-Mofty SK and Lewis JS, Jr. (2015). Verrucous carcinoma with dysplasia or minimal invasion: a variant of verrucous carcinoma with extremely favorable prognosis. Head Neck Pathol 9(1):65-73.
35 Jayasooriya PR, Tilakaratne WM, Mendis BR and Lombardi T (2013). A literature review on oral basaloid squamous cell carcinomas, with special emphasis on etiology. Ann Diagn Pathol 17(6):547-551.
36 Schick U, Pusztaszeri M, Betz M, Ghadjar P, Demiroz C, Kaanders JH and
Ozsahin M (2013). Adenosquamous carcinoma of the head and neck: report of 20 cases and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol 116(3):313-320.
37 Thavaraj S, Cobb A, Kalavrezos N, Beale T, Walker DM and Jay A (2012). Carcinoma cuniculatum arising in the tongue. Head Neck Pathol 6(1):130-134.
38 Seethala RR (2011). Histologic grading and prognostic biomarkers in salivary gland carcinomas. Adv Anat Pathol 18(1):29-45.
39 Brandwein M, Huvos AG, Dardick I, Thomas MJ and Theise ND (1996).
Noninvasive and minimally invasive carcinoma ex mixed tumor: a clinicopathologic and ploidy study of 12 patients with major salivary tumors of low (or no?) malignant potential. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 81(6):655-664.
40 Jakobsson PA, Eneroth CM, Killander D, Moberger G and Martensson B (1973). Histologic classification and grading of malignancy in carcinoma of the larynx. Acta Radiol Ther Phys Biol 12(1):1-8.

61
41 Roland NJ, Caslin AW, Nash J and Stell PM (1992). Value of grading squamous cell carcinoma of the head and neck. Head Neck 14(3):224-229.
42 Kearsley JH and Thomas S (1993). Prognostic markers in cancers of the head and neck region. Anticancer Drugs 4(4):419-429.
43 Snow GB, Annyas AA, van Slooten EA, Bartelink H and Hart AA (1982). Prognostic factors of neck node metastasis. Clin Otolaryngol Allied Sci 7(3):185-
192.
44 Henson DE (1988). The histological grading of neoplasms. Arch Pathol Lab Med 112(11):1091-1096.
45 Sethi S, Lu M, Kapke A, Benninger MS and Worsham MJ (2009). Patient and tumor factors at diagnosis in a multi-ethnic primary head and neck squamous cell carcinoma cohort. J Surg Oncol 99(2):104-108.
46 El-Naggar AK CJ, Grandis JR, Takata T, Slootweg PJ Eds. (2017). WHO Classification of Head and Neck Tumours (4th Edition). IARC, Lyon, France.
47 Woolgar JA and Triantafyllou A (2009). Pitfalls and procedures in the histopathological diagnosis of oral and oropharyngeal squamous cell carcinoma and a review of the role of pathology in prognosis. Oral Oncol 45(4-5):361-385.
48 Woolgar JA (2006). Histopathological prognosticators in oral and oropharyngeal squamous cell carcinoma. Oral Oncol 42(3):229-239.
49 Kademani D, Bell RB, Bagheri S, Holmgren E, Dierks E, Potter B and Homer L (2005). Prognostic factors in intraoral squamous cell carcinoma: the influence of histologic grade. J Oral Maxillofac Surg 63(11):1599-1605.
50 Adel M, Kao HK, Hsu CL, Huang JJ, Lee LY, Huang Y, Browne T, Tsang NM, Chang YL and Chang KP (2015). Evaluation of Lymphatic and Vascular Invasion in Relation to Clinicopathological Factors and Treatment Outcome in Oral Cavity Squamous Cell Carcinoma. Medicine (Baltimore) 94(43):e1510.
51 Seethala RR (2009). An update on grading of salivary gland carcinomas. Head Neck Pathol 3(1):69-77.
52 Brierley JD, Gospodarowicz MK and Wittekind C (eds) (2016). UICC TNM Classification of Malignant Tumours, 8th Edition, Wiley-Blackwell.
53 Almangush A, Bello IO, Coletta RD, Makitie AA, Makinen LK, Kauppila JH, Pukkila M, Hagstrom J, Laranne J, Soini Y, Kosma VM, Koivunen P, Kelner N,
62
Kowalski LP, Grenman R, Leivo I, Laara E and Salo T (2015). For early-stage oral tongue cancer, depth of invasion and worst pattern of invasion are the strongest pathological predictors for locoregional recurrence and mortality. Virchows Arch
467(1):39-46.
54 Almangush A, Bello IO, Keski-Santti H, Makinen LK, Kauppila JH, Pukkila M, Hagstrom J, Laranne J, Tommola S, Nieminen O, Soini Y, Kosma VM, Koivunen P, Grenman R, Leivo I and Salo T (2014). Depth of invasion, tumor budding, and worst pattern of invasion: prognostic indicators in early-stage oral tongue cancer.
Head Neck 36(6):811-818.
55 Li Y, Bai S, Carroll W, Dayan D, Dort JC, Heller K, Jour G, Lau H, Penner C, Prystowsky M, Rosenthal E, Schlecht NF, Smith RV, Urken M, Vered M, Wang B, Wenig B, Negassa A and Brandwein-Gensler M (2013). Validation of the risk model: high-risk classification and tumor pattern of invasion predict outcome for
patients with low-stage oral cavity squamous cell carcinoma. Head Neck Pathol 7(3):211-223.
56 Kuan EC, Mallen-St Clair J, Badran KW and St John MA (2016). How does depth of invasion influence the decision to do a neck dissection in clinically N0 oral cavity cancer? Laryngoscope 126(3):547-548.
57 Brandwein-Gensler M, Teixeira MS, Lewis CM, Lee B, Rolnitzky L, Hille JJ, Genden E, Urken ML and Wang BY (2005). Oral squamous cell carcinoma: histologic risk assessment, but not margin status, is strongly predictive of local disease-free and overall survival. Am J Surg Pathol 29(2):167-178.
58 Fives C, Feeley L, O'Leary G and Sheahan P (2016). Importance of lymphovascular invasion and invasive front on survival in floor of mouth cancer. Head Neck 38 Suppl 1:E1528-1534.
59 Chatzistefanou I, Lubek J, Markou K and Ord RA (2014). The role of neck
dissection and postoperative adjuvant radiotherapy in cN0 patients with PNI-positive squamous cell carcinoma of the oral cavity. Oral Oncol 50(8):753-758.
60 Chinn SB, Spector ME, Bellile EL, McHugh JB, Gernon TJ, Bradford CR, Wolf GT, Eisbruch A and Chepeha DB (2013). Impact of perineural invasion in the pathologically N0 neck in oral cavity squamous cell carcinoma. Otolaryngol Head
Neck Surg 149(6):893-899.
61 Miller ME, Palla B, Chen Q, Elashoff DA, Abemayor E, St John MA and Lai CK (2012). A novel classification system for perineural invasion in noncutaneous head and neck squamous cell carcinoma: histologic subcategories and patient
outcomes. Am J Otolaryngol 33(2):212-215.
62 Hinni ML, Ferlito A, Brandwein-Gensler MS, Takes RP, Silver CE, Westra WH, Seethala RR, Rodrigo JP, Corry J, Bradford CR, Hunt JL, Strojan P, Devaney
63
KO, Gnepp DR, Hartl DM, Kowalski LP, Rinaldo A and Barnes L (2013). Surgical margins in head and neck cancer: a contemporary review. Head Neck 35(9):1362-1370.
63 Meier JD, Oliver DA and Varvares MA (2005). Surgical margin determination in head and neck oncology: current clinical practice. The results of an International American Head and Neck Society Member Survey. Head Neck 27(11):952-958.
64 Maxwell JH, Thompson LD, Brandwein-Gensler MS, Weiss BG, Canis M, Purgina B, Prabhu AV, Lai C, Shuai Y, Carroll WR, Morlandt A, Duvvuri U, Kim S, Johnson JT, Ferris RL, Seethala R and Chiosea SI (2015). Early Oral Tongue Squamous Cell Carcinoma: Sampling of Margins From Tumor Bed and Worse Local Control. JAMA Otolaryngol Head Neck Surg 141(12):1104-1110.
65 Chang AM, Kim SW, Duvvuri U, Johnson JT, Myers EN, Ferris RL, Gooding WE, Seethala RR and Chiosea SI (2013). Early squamous cell carcinoma of the oral tongue: comparing margins obtained from the glossectomy specimen to margins from the tumor bed. Oral Oncol 49(11):1077-1082.
66 Chen CH, Hsu MY, Jiang RS, Wu SH, Chen FJ and Liu SA (2012). Shrinkage of head and neck cancer specimens after formalin fixation. J Chin Med Assoc 75(3):109-113.
67 Seoane J, Caballero TG, Urizar JM, Almagro M, Mosquera AG and Varela-Centelles P (2010). Pseudodysplastic epithelial artefacts associated with oral
mucosa CO2 laser excision: an assessment of margin status. Int J Oral Maxillofac Surg 39(8):783-787.
68 Gonzalez-Mosquera A, Seoane J, Garcia-Caballero L, Lopez-Jornet P, Garcia-Caballero T and Varela-Centelles P (2012). Er,CR:YSGG lasers induce fewer dysplastic-like epithelial artefacts than CO2 lasers: an in vivo experimental
study on oral mucosa. Br J Oral Maxillofac Surg 50(6):508-512.
69 Buchanan MA, Coleman HG, Daley J, Digges J, Sandler M, Riffat F and Palme CE (2016). Relationship between CO2 laser-induced artifact and glottic cancer surgical margins at variable power doses. Head Neck 38 Suppl 1:E712-716.
70 Speight PM, Abram TJ, Floriano PN, James R, Vick J, Thornhill MH, Murdoch C, Freeman C, Hegarty AM, D'Apice K, Kerr AR, Phelan J, Corby P, Khouly I, Vigneswaran N, Bouquot J, Demian NM, Weinstock YE, Redding SW, Rowan S, Yeh CK, McGuff HS, Miller FR and McDevitt JT (2015). Interobserver
agreement in dysplasia grading: toward an enhanced gold standard for clinical pathology trials. Oral Surg Oral Med Oral Pathol Oral Radiol 120(4):474-482.e472.

64
71 Stojanov IJ and Woo SB (2015). Human papillomavirus and Epstein-Barr virus associated conditions of the oral mucosa. Semin Diagn Pathol 32(1):3-11.
72 Akrish S, Ben-Izhak O, Sabo E and Rachmiel A (2015). Oral squamous cell carcinoma associated with proliferative verrucous leukoplakia compared with conventional squamous cell carcinoma--a clinical, histologic and immunohistochemical study. Oral Surg Oral Med Oral Pathol Oral Radiol 119(3):318-325.
73 Gillenwater AM, Vigneswaran N, Fatani H, Saintigny P and El-Naggar AK (2013). Proliferative verrucous leukoplakia (PVL): a review of an elusive pathologic entity! Adv Anat Pathol 20(6):416-423.
74 Jayasooriya PR, Nadeeka Jayasinghe KA and Mudiyanselage Tilakaratne W (2011). Relationship between thickness of fibrosis and epithelial dysplasia in oral submucous fibrosis. J Investig Clin Dent 2(3):171-175.
75 Bice TC, Tran V, Merkley MA, Newlands SD, van der Sloot PG, Wu S and Miller MC (2015). Disease-Specific Survival with Spindle Cell Carcinoma of the Head and Neck. Otolaryngol Head Neck Surg 153(6):973-980.
76 Rytkonen AE, Hirvikoski PP and Salo TA (2011). Lymphoepithelial carcinoma: two case reports and a systematic review of oral and sinonasal cases. Head Neck Pathol 5(4):327-334.
77 Sgaramella N, Coates PJ, Strindlund K, Loljung L, Colella G, Laurell G, Rossiello R, Muzio LL, Loizou C, Tartaro G, Olofsson K, Danielsson K, Fahraeus R and Nylander K (2015). Expression of p16 in squamous cell carcinoma of the mobile tongue is independent of HPV infection despite presence of the HPV-receptor syndecan-1. Br J Cancer 113(2):321-326.
78 Reuschenbach M, Kansy K, Garbe K, Vinokurova S, Flechtenmacher C, Toth C, Prigge ES, Thiele OC, Reinert S, Hoffmann J, von Knebel Doeberitz M and Freier K (2013). Lack of evidence of human papillomavirus-induced squamous cell carcinomas of the oral cavity in southern Germany. Oral Oncol 49(9):937-942.
79 Zafereo ME, Xu L, Dahlstrom KR, Viamonte CA, El-Naggar AK, Wei Q, Li G
and Sturgis EM (2016). Squamous cell carcinoma of the oral cavity often overexpresses p16 but is rarely driven by human papillomavirus. Oral Oncol 56:47-53.
80 Ebrahimi A, Gil Z, Amit M, Yen TC, Liao CT, Chaturvedi P, Agarwal JP, Kowalski LP, Kreppel M, Cernea CR, Brandao J, Bachar G, Bolzoni Villaret A, Fliss D, Fridman E, Robbins KT, Shah JP, Patel SG and Clark JR (2014). Primary tumor staging for oral cancer and a proposed modification incorporating depth of invasion: an international multicenter retrospective study. JAMA Otolaryngol Head Neck Surg 140(12):1138-1148.
65
81 Royal College of Pathologists of Australasia (2011). Functional Requirements for Laboratory Information Systems to support Structured Pathology Reporting of Cancer Protocols https://www.rcpa.edu.au/Library/Practising-Pathology/Structured-Pathology-Reporting-of-Cancer/Implementation.
82 Valenstein PN (2008). Formatting pathology reports: applying four design principles to improve communication and patient safety. Arch Path Lab Med.
132(1):84–94.


















