cancer the facts
52
-
Upload
carlos-alberto-trapani -
Category
Health & Medicine
-
view
57 -
download
1
Transcript of cancer the facts


Cancer is not just one diseaseMore than 200 different types of cancer have been identified
What is cancer?
CANCER

Defining cancer
Cancer is an accumulation of abnormal cells that multiply through uncontrolled cell division and spread to other parts of the body by invasion and/or distant
metastasis via the blood and lymphatic system
MetastasisTumour growthNormal cells Abnormal cells
Invasion into surrounding tissues
Uncontrolled cell division
Spread via blood or lymphatic system

Incidence of cancer across the globe (2008, estimate)1
Estimated number of new cancer cases (% of total)
Africa (6%)Asia (48%)Europe (25%)Latin America and Caribbean (7%)Northern (13%)Oceania (1%)
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C and Parkin DM. GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No.10 [Internet]. Lyon, France: International Agency
for Research on Cancer; 2010. Available from: http://globocan.iarc.fr, accessed on 06/06/2013.

Changing prevalence of cancer
Global cancer incidence and mortality rates continue to rise1
21.3 M
12.7 M
13.1 M
7.6 M
CASES DEATHS
2030
2008
20302002
25 M people living
with cancer*2
75 M predicted to be living with
cancer2
*Diagnosed in last 5 years
GROWING AND AGEING POPULATION
ADOPTION OF UNHEALTHY LIFESTYLES
IMPROVEMENT IN DIAGNOSIS/SCREENING
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C and Parkin DM. GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No.10 [Internet]. Lyon, France: International
Agency for Research on Cancer; 2010. Available from: http://globocan.iarc.fr, accessed on 14/01/2013. 2. The International Agency for Research on Cancer. World Cancer Report 2008. Available from:
http://www.iarc.fr/en/publications/pdfs-online/wcr/, accessed on 06/06/2013.

Common cancers in men and women worldwide1
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C and Parkin DM. GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No.10 [Internet]. Lyon, France: International
Agency for Research on Cancer; 2010. Available from: http://globocan.iarc.fr, accessed on 06/06/2013.
16.5
13.6
109.77.9
4.94.4
3
3
27
Men (%) Lung (16.5)
Prostate (13.6)
Colorectum (10.0)
Stomach (9.7)
Liver (7.9)
Oesophagus (4.9)
Bladder (4.4)
Non-Hodgkin lymphoma (3.0)
Leukaemia (3.0)
Other and unspecified (27.0)
8.5
22.9
9.45.83.78.84.8
3.72.7
29.7
Women (%) Lung (8.5)
Breast (22.9)
Colorectum (9.4)
Stomach (5.8)
Liver (3.7)
Cervix uteri (8.8)
Corpus uteri (4.8)
Ovary (3.7)
Thyroid (2.7)
Other and unspecified (29.7)

1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C and Parkin DM. GLOBOCAN 2008 v2.0, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No.10 [Internet]. Lyon, France: International Agency for Research on
Cancer; 2010. Available from: http://globocan.iarc.fr, accessed on 06/06/2013. 2. American Cancer Society. Global Cancer Facts and Figures 2nd Edition. Atlanta: American Cancer Society; 2011.
Global cancer mortality
Both sexes Men Women0
5
10
15
20
25
Lung
Stomach
Liver
Colorectal
Female breastM
ort
ality
(%
of
all c
ance
r ty
pe
s)
Approximately 7.56 million people died from
cancer in 2008,1 accounting for 13% of all deaths (from any cause)2
Lung, stomach, liver, colorectal and female
breast cancers cause 50% of all cancer deaths1


Common terms
Localisedthe cancer is still confined to the site of origin and has
not yet invaded the surrounding tissues or spread to other sites
Invasivethe cancer has spread
from the site of origin into the surrounding tissues
Metastatic the cancer has spread to distant sites in the body to
form new tumours
Stage classification of the cancer,
important for treatment decisions, based on the
size, presence or absence of metastasis and involve-
ment of lymph nodes
Gradehow abnormal cancer cells appear in comparison to normal cells and how aggressive the cancer is
Low grade – nearly normal in appearance; slow rate of growth and metastasis
High grade – very abnormal-looking cells; high rate of growth and metastasis

Cancer categories
Carcinomacancer of the skin or tissues that line or cover the internal
organs
Sarcomacancer of bone,
cartilage, muscle, fat, blood vessels, and connective tissues
Leukaemia cancer of the bone
marrow affecting the white blood cells
Lymphoma cancer arising in the
lymph glands
Central nervous system cancerscancer of the brain or
spinal cord

Making sense of cancer names
Artwork originally created for the National Cancer Institute. Reprinted with permission of the artist, Jeanne Kelly. Copyright 2013.


Risk factor definitions
013
RISK FACTOR
Something that increases the chances of getting
a disease
Intrinsic risk factor
…is an integral part of the individual and
cannot be changed (genetics, age, etc.)
Extrinsicrisk factor
…is related to an individual’s own actions
and environment(tobacco, pollution,
diet, etc.)

Risk factors are multiple and differ according to the cancer type
RISK FACTORS
Age
ObesityBacteriaH.pylori
Hormones
Radiation
Diet
Smoking tobacco
General health
Hereditary
Chemicals
VirusesHPV
HBV
EBV
Sunexposure

Absolute risk vs. Relative risk
Absolute risk
The risk of an individual
developing cancer during
their entire lifetime
Relative risk
The risk of a group of people
developing cancer in
comparison to another group

Benefits of assessing risk
Allows the individual at risk to undertake prevention strategies (e.g. stop smoking, avoid radiation)!
Alerts physicians to those individuals at risk of developing cancer!
Early detection enables physicians to initiate treatment, whist the tumour is still in the initial stages!
Enables screening procedures to detect cancer at an early stage!


1. Nowell, PC. The clonal evolution of tumor cell populations. Science (1976) 194:23-28. 2. Cavenee, WK & White, RL. The genetic basis of cancer. Scientific American (1995) 272:72-79.
Emergence of a cancer cell
Malignant cell
Cancers originate from a single cell1,2
A series of mutations accumulate in successive generations of the cell in a process known as
clonal evolution
Eventually, a cell accumulates enough mutations to become
cancerousFirst
mutationSecond mutation
Third mutation
Fourth orlater mutation
Genetic mutations, i.e. changes to the normal base sequence of DNA, contribute to
the emergence of a cancer cell

In order for cancerous cells to develop and form a tumour, mutations and other alterations that allow the cell to acquire a succession of the
following biological capabilities must occur:1,2
The hallmarks of cancer
1. Hanahan D & Weinberg RA. The hallmarks of cancer. Cell (2000) 100:57-70. 2. Hanahan D & Weinberg RA. Hallmarks of cancer: the next generation. Cell (2011) 144:646-674
Sustaining proliferative signalling
Evading growth suppressors
Activating invasion & metastasis
Enabling replicative immortality
Inducingangiogenesis
Resisting cell death

Normal cells rely on positive growth signals from other cellsCancer cells can reduce their dependence on growth signals by:1,2
- Production of their own extracellular growth factors -- Overexpression of growth factor receptors -
- Alterations to intracellular components of signalling pathways -
Sustaining proliferative signalling
Cell wallIntracellular signalling
Growth factor receptors
Growth factors
1. Hanahan D & Weinberg RA. The hallmarks of cancer. Cell (2000) 100:57-70. 2. Hanahan D & Weinberg RA. Hallmarks of cancer: the next generation. Cell (2011) 144:646-674

• Normal cells rely on antigrowth signals to regulate cell growth1,2
• Cancer cells can become insensitive to these signals
• One way that this can happen is by disruption of the retinoblastoma protein (pRb) pathway1
• pRb prevents inappropriate transition from the G1 phase of the cell cycle to the synthesis (S) phase1
• In cancer cells, pRB may be damaged, allowing the cell to divide uncontrollably1
Celldivision
cycleG1
S
G2M
1. Hanahan D & Weinberg RA. The hallmarks of cancer. Cell (2000) 100:57-70. 2. Hanahan D & Weinberg RA. Hallmarks of cancer: the next generation. Cell (2011) 144:646-674
Evading growth suppressors

Resisting cell death
Hanahan D & Weinberg RA. The hallmarks of cancer. Cell (2000) 100:57-70. 2. National Cancer Institute, What is Cancer, 2010. 3. Hanahan D & Weinberg RA. Hallmarks of cancer: the next generation. Cell (2011) 144:646-674. Artwork originally created for
the National Cancer Institute. Reprinted with permission of the artist, Jeanne Kelly. Copyright 2013.
An important hallmark of many cancers is resistance to apoptosis,
which contributes to the ability of the cells to divide uncontrollably1,2
When normal cells become old/damaged, they go through
apoptosis (programmed cell death)
Normal celldivision
Cell damage –no repair
Apoptosis
Cancer celldivision
First mutation
Second mutation
Third mutation
Fourth orlater mutation
Uncontrolledgrowth

Another important hallmark of cancer is the ability of the cell to overcome the boundaries on how many times a cell can divide1
These limits are usually set by telomeres (the ends of chromosomes):1,2
• In normal cells, telomeres get shorter with each cell division until they become so short that the cell can no longer divide
• In cancer cells, telomeres are maintained, allowing the cell to divide an unlimited number of times
Enabling replicative immortality
Normal cells Cell division Cancer cells
Telomeres
No apoptosis
Apoptosis
Chromosomes
1. Hanahan D & Weinberg RA. The hallmarks of cancer. Cell (2000) 100:57-70. 2. Hanahan D & Weinberg RA. Hallmarks of cancer: the next generation. Cell (2011) 144:646-674
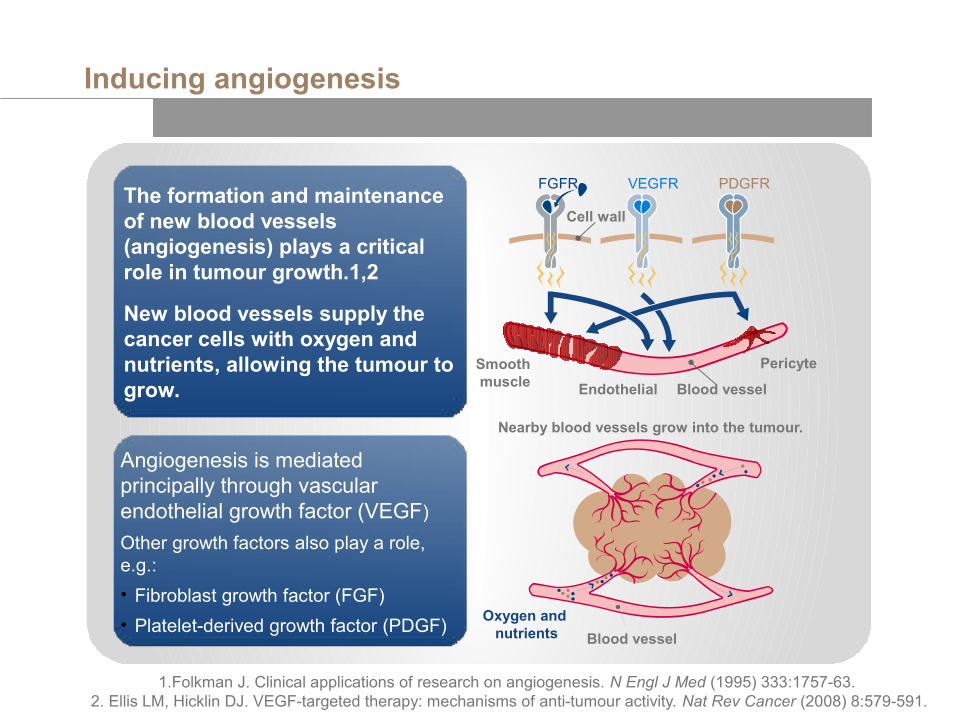
1.Folkman J. Clinical applications of research on angiogenesis. N Engl J Med (1995) 333:1757-63. 2. Ellis LM, Hicklin DJ. VEGF-targeted therapy: mechanisms of anti-tumour activity. Nat Rev Cancer (2008) 8:579-591.
Inducing angiogenesis
The formation and maintenance of new blood vessels (angiogenesis) plays a critical role in tumour growth.1,2
New blood vessels supply the cancer cells with oxygen and nutrients, allowing the tumour to grow.
Angiogenesis is mediated principally through vascular endothelial growth factor (VEGF)
Other growth factors also play a role, e.g.:
• Fibroblast growth factor (FGF)
• Platelet-derived growth factor (PDGF)
Nearby blood vessels grow into the tumour.
Oxygen and nutrients Blood vessel
Blood vessel
Pericyte
Endothelial
Smooth muscle
Cell wall
VEGFRFGFR PDGFR

Activating invasion & metastasis
1. Hanahan D & Weinberg RA. The hallmarks of cancer. Cell (2000) 100:57-70. 2. Gupta GP & Massagué J. Cancer metastasis: Building a framework. Cell (2006) 127: 679-695
Eventually, tumours may spawn pioneer cells that can invade adjacent tissues and
travel to other sites in the body to form new tumours
(metastasis)1
This capability allows cancerous cells to colonise
new areas where oxygen and nutrients are not
limiting1
Metastasis causes 90% of deaths from solid tumours2
Nearby blood vessels grow into the tumour.
Oxygen and nutrients
Cells escape and metastasiseBlood vessel

There is evidence that a further two emerging hallmarks are involved in the pathogenesis of cancer1
The acquisition of these hallmarks of cancer is made possible by two enabling characteristics1
Enabling characteristics and emerging hallmarks
1. Hanahan D & Weinberg RA. Hallmarks of cancer: the next generation. Cell (2011) 144:646-674
Evading immune destruction
Enabling characteristics
Genome instability and mutation
Deregulating cellular energetics
Tumour-promoting inflammation
Emerging hallmarksThe immune system is responsible for
recognising and eliminating cancer cells, and therefore preventing tumour
formation. Evasion of this immune surveillance by weakly immunogenic cancer cells is an important emerging
hallmark of cancer.
Cancer cells achieve genome instability by increasing their mutability, or rates
of mutation, through increased sensitivity to mutagenic agents or
breakdown of genomic maintenance machinery.
The uncontrolled growth and division of cancer cells relies not only on the
deregulation of cell proliferation, but also on the reprogramming of cellular
metabolism, including increased aerobic glycolysis (known as the
Warburg effect)
Immune cells infiltrate tumours and produce inflammatory responses, which
can paradoxically enhance tumourigenesis, helping tumours acquire the hallmarks of cancer
Click on each hallmark or enabling characteristic for more information


Diagnostic tests include:
• Physical examination
• Laboratory tests
• Imaging
• Endoscopic examination
• Biopsy
• Surgery
• Molecular testing
How is cancer diagnosed?
‘Cancer’ is an umbrella term for a broad group of diseases
There is no single test that can diagnose all cancers1
1. Stanford Cancer Institute, Cancer Diagnosis, 2012
If there are symptoms suggestive of cancer a broad range of tests allow HCPs to make an accurate and detailed diagnosis

Laboratory tests
Assess the general health of the body and levels of certain compounds
Typically, blood and/or urine samples
Blood is assessed for its composition, and can give an indication of liver and renal function
Blood, proteins and other compounds in the urine indicate there could be a problem
Tumour markers detected in blood or urine are substances created by the body in response to cancer cells
• Currently, markers are used to monitor treatment efficacy and recurrence
• May become more important in diagnosis in the future
1. Stanford Cancer Institute, Cancer Diagnosis, 2012.
CEA, carcinoembryonic antigen, several cancers can raise CEA levels; AFP, alpha-fetoprotein; HCG, human chorionic gonadotropin; CA 15-3 and CA 27-29 are most useful in assessing advanced breast cancer treatment
Marker Cancer
CA 125 Ovarian
CEA Colorectal
AFP Liver, ovarian, testicular
HCGTesticular, ovarian, liver,stomach, pancreatic, lung
CA 19-9 Colon, stomach, bile duct
CA 15-3 Ovarian, lung, prostate
CA 27-29Colon, stomach, kidney, lung, ovarian, pancreatic, uterus, and liver

Imaging
1. Stanford Cancer Institute, Cancer Diagnosis, 2012.
Produce images of the organs and structures
Reveal location and extent of disease
Three main types:
• Transmission imaging: high-energy photons beamed through body – the ‘opacity’ of different structures/tissues varies > X-ray, CT scan, bone scan, mammogram, lymphangiogram
• Reflection imaging: high frequency sound reflected differentially depending on structures/tissues > Ultrasound
• Emission imaging: atoms excited to emit energy waves detected by a scanner > MRI, PET
magnetic field direction
Imaging
Transmittedradio waves
Emittedradio waves

Endoscopy
1. Stanford Cancer Institute, Cancer Diagnosis 2012.
• BronchoscopyUsed to examine the airways and obtain tissue samples from the lungs
• Colonoscopy and sigmoidoscopyUsed to view the large intestine or just the sigmoid colon
• Endoscopic retrograde cholangiopancreatography (ERCP)Combined with X-ray to examine the liver, gallbladder, bile ducts, and pancreas
• Oesophagogastroduodenoscopy (upper endoscopy)Used to view the inside of the oesophagus, stomach, and duodenum
• Cystoscopy (cystourethroscopy)Device inserted through the urethra to examine the bladder and urinary tract
Oesophagus
Endoscope
Stomach
Light
Interior of stomach
Endoscope
Light
Stomachlining
Biopsy sample
An endoscope is a small, flexible tube with a light, lens and tools

Biopsy
1. Stanford Cancer Institute, Cancer Diagnosis, 2012.
Biopsy type Description
Endoscopic Tissue sample removed via an endoscopy
Bone marrow
Bone chip or cells aspirated from the sternum or hip
Excisional or incisional
Full thickness of skin even whole tumour removed
Fine needle aspiration (FNA)
Tiny pieces of tumour extracted via a thin needle
PunchShort cylinder of tissue taken
Shave Top layer of skin removed
Skin Small sample of skin taken
Tissue or cells from the body for examination under a microscope
Performed in the doctor’s office or hospital, depending on the type of biopsy and location of the tumour

Pathology
1. National Cancer Institute, Understanding Cancer, 2009.Artwork originally created for the National Cancer Institute.
Reprinted with permission of the artist, Jeanne Kelly. Copyright 2013.
Tests on biopsies and samples of patient tissue or body fluids reveal a great deal about the cancer
Microscopic examination can reveal the presence of cancer cells, the origin of the cancer cells (sub-type), and information on stage, etc.
Biopsy
Blood sampleor
tissue sample
Pathology
Proteomic profile
Genomic profile


What is TNM?
TNM is a system for classifying malignant tumours!
It is a cancer staging system, which describes the extent of a person's cancer!
Most medical facilities use this system as their main method for cancer reporting1!
Most types of cancer have TNM designations, but some do not1!
1. National Cancer Institute, Cancer Staging, 2010

How does the TNM system work?
The 3 parameters of the TNM system1:
T = extent of the tumour
N = the extent of spread to the lymph nodes
M = presence of distant metastases
A number is added to each letter
to indicate1:
the size or extent of the primary tumour
the extent of cancer spread
1. National Cancer Institute, Cancer Staging, 2010

T = extent of primary tumour
organlocal tissues
T0 T1 T2 T3
T is classified as follows:1
Tx: Primary tumour cannot be evaluated | T0: No evidence of primary tumour
Tis: Carcinoma in situ (CIS)2 | T1, T2, T3, T4: Size and/or extent of the primary tumour
1. National Cancer Institute, Cancer Staging, 20102. CIS – abnormal cells are present but have not spread to neighbouring tissue; although not cancer, CIS
may become cancer and is sometimes called pre-invasive cancer
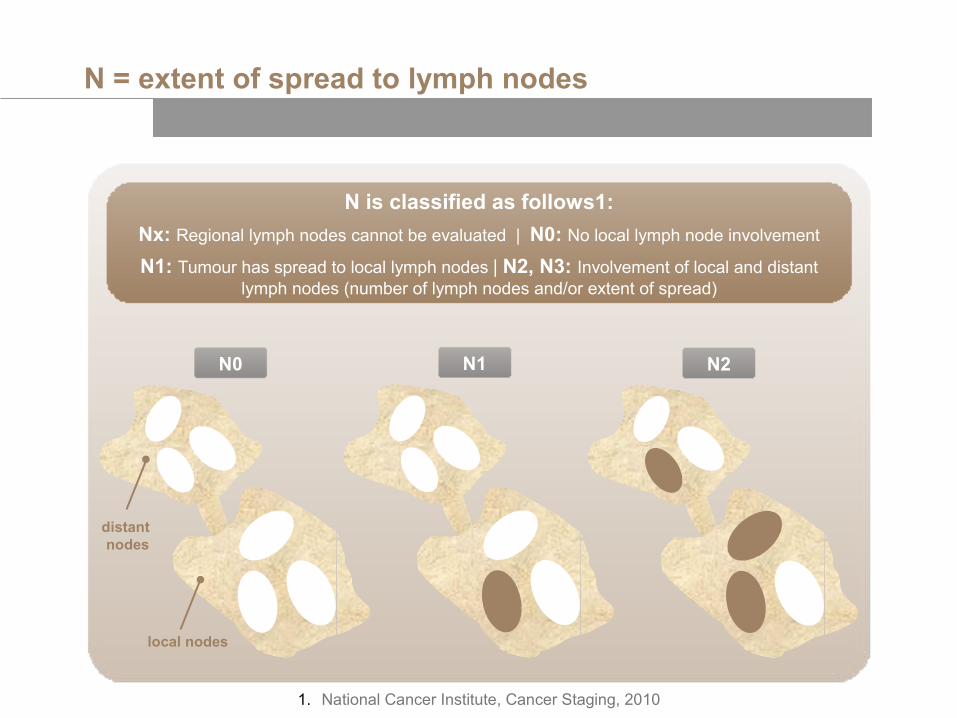
N = extent of spread to lymph nodes
distant nodes
local nodes
N0
N is classified as follows1:
Nx: Regional lymph nodes cannot be evaluated | N0: No local lymph node involvement
N1: Tumour has spread to local lymph nodes | N2, N3: Involvement of local and distant lymph nodes (number of lymph nodes and/or extent of spread)
1. National Cancer Institute, Cancer Staging, 2010
N1 N2

M0
M = presence of distant metastases
M is classified as follows1:
Mx: Distant metastasis cannot be evaluated | M0: No distant metastasis
M1: Distant metastasis is present
1. National Cancer Institute, Cancer Staging, 2010
bone
lung
liver
M1 Mx
?


Intrinsic vs. extrinsic factors
Cancer caused by intrinsic factors, i.e. inherited mutations, can only be prevented by screening and appropriate early intervention
Cancer Prevention
1. National Cancer Institute, Understanding Cancer, 2009.
Cancer caused by extrinsic factors can be prevented by reducing or eliminating exposure to these factors (e.g. chemicals, tobacco, radiation, viruses)
Radiation
Viruses or bacteria
Carcinogenicchemicals

Tobacco products
1. National Cancer Institute, Understanding Cancer, 2009. 2. WHO Fact Sheet 339, 2012.Artwork originally created for the National Cancer Institute.
Reprinted with permission of the artist, Jeanne Kelly. Copyright 2013.
The use of tobacco products is implicated in ~33% of all cancer deaths1
~1 person dies every 6 seconds due to tobacco2
The combination of tobacco and alcohol products appears to be particularly dangerous1
As well as lung cancer, tobacco products have also been implicated in cancer of the mouth, larynx, oesophagus, stomach, pancreas, kidney, and bladder1
Avoiding tobacco is the single most important factor in reducing cancer risk
Lung Cancer Risk Increases with Cigarette Consumption1
15x
10x
5x
0 15 30
LungCancerRisk
Cigarettes Smoked per DayNon-smoker

Excessive exposure to UV radiation
1. WHO Fact Sheet 305, 2009.
Excessive UV exposure, particularly in fair-skinned individuals can cause:1• cutaneous malignant
melanoma• squamous cell carcinoma• basal cell carcinoma
In 2000, >200,000 cases of melanoma were diagnosed worldwide1
Stratosphere
Sunexposure
Ozone
Epidermis
Dermis
Hypodermis
UV-A
UV-B
UV-C

Diet
National Cancer Institute, Understanding Cancer, 2009. Artwork originally created for the National Cancer Institute.
Reprinted with permission of the artist, Jeanne Kelly. Copyright 2013.
Unlike tobacco products, UV radiation and alcohol, dietary components that influence cancer risk have been difficult to determine1
Limiting fat and calorie intake appears to reduce cancer risk1
A diet rich in meat increases cancer risk, especially colon cancer1
Nu
mb
er o
f C
ases
(p
er 1
00,
00 P
eop
le)
Correlation Between Meat Consumption and Colon Cancer Rates in Different Countries1
40
30
15
Grams (per person per day)
N.Z.
20
10
0 80 100 200 300
U.S.A.
DEN. CANG.B.
SWENOR NETH
GERMANYICE
ISRJAMFIN P.R.
HUNGROM
COLNIG
JAPAN
YUG POL
CHILE

HPV Infection Increases Risk for Cervical Cancer2
Viruses
1. Liao JB. Viruses and Human Cancer. YJBM 2006 (79);115-122. 2.National Cancer Institute, Understanding Cancer, 2009. Artwork originally created for the National Cancer Institute. Reprinted with permission of the artist, Jeanne Kelly. Copyright 2013.
Worldwide, 15% of all cancers may be caused by viruses, including:1
• Epstein-Barr virus
• Human papilloma virus (HPV)
• Hepatitis B virus
• Human herpes virus-8
• Human T lymphotrophic virus type 1
• Hepatitis C virus
Reducing exposure to these viruses reduces cancer risk
In the case of HPV, avoiding unprotected sex with many partners reduces the risk of contracting this virus2
High
LowNon-infected
women
CervicalCancerRisk
Women infected with HPV

Strategies for prevention
about cancer and risk factors (warnings on cigarette packets, campaigns about sun and exposure to UV radiation)
pink ribbons for breast cancer, world cancer day
don’t smoke, stay out of the sun, avoid toxic chemicals and polluted areas
cervical smear, mammography, colonoscopy
HPV vaccine to reduce risk of cervical cancer; Hep B vaccine to reduce risk of liver cancer
normal weight, healthy diet, exercise
regular check-ups, seek medical attention early
Education
Awareness campaigns
Risk avoidance
Screening
Vaccines
Lifestyle
Healthcare


Breast Cancer Screening
What is screening?
Screening is the name given to a range of tests that can detect cancer at an early stage before symptoms appear
Finding cancer early usually means it is easier to treat/cure
By the time symptoms appear, the cancer may have grown and spread and therefore be more difficult to treat/cure
1. National Cancer Institute, Cancer Screening Overview, 2012.

Screening: the rationale
For screening to be effective, two requirements must be met:
A test or procedure must be available to detect cancers earlier than if the cancer were detected as a result of the development of symptoms
!
Evidence must be available that treatment initiated earlier as a consequence of screening results in an improved outcome
!
1. National Cancer Institute, Cancer Screening HCP, 2012.

Cervical Cancer Screening
Screening tests
National Cancer Institute, Cancer Screening Overview, 2012. Artwork originally created for the National Cancer Institute. Reprinted with permission of the artist, Jeanne Kelly. Copyright 2013.
A variety of tests are used in cancer screening:
• Physical exam and history: check general health and review medical history
• Laboratory tests: investigate samples of tissue, blood, urine, etc.
• Imaging: visualise the insides of the body using e.g. x-ray, ultrasound, CT, MRI, etc
• Molecular tests: look for specific mutations that are linked to some types of cancer
Biopsy
NormalPap smear
AbnormalPap smear
Patient‘s blood sampleor
tissue sample
Pathology
Proteomic profile
Genomic profile

Screening: pros and cons
Pros• Reduction in cancer deaths
• 3–35% of premature deaths due to cancer could be avoided with screening
• Improved outcomes (does not apply in all cases)
Cons• Some screening
procedures carry their own risks
• False negative results – patient wrongly assured there is no problem
• False positive results – patient may receive treatment they do not need
1. National Cancer Institute, Cancer Screening HCP, 2012.

Heredity and cancer
Screening and high risk populations
By focusing on high-risk populations, screening resources can be better applied
Patients with a personal history/strong family history of cancer are deemed to be high-risk
The ability to test for specific genetic mutations has further refined the identification of high-risk patients
National Cancer Institute, Cancer Screening HCP, 2012. Artwork originally created for the National Cancer Institute. Reprinted with permission of the artist, Jeanne Kelly. Copyright 2013.
All Breast Cancer Patients
Inherited factor(s) Other factor(s)
Genes and Cancer
RadiationViruses
Chemicals
Heredity
Chromosomesare DNA molecules