CAGPO 2018: Cancer Associated Thrombosis · uOttawa.ca Objectives To develop a modern understanding...
75
CAGPO 2018: Cancer Associated Thrombosis Dr. Marc Carriere (thrombosis) and Dr. Sandy Sehdev (medical oncology) uOttawa.ca Faculté de médecine | Faculty of Medicine
Transcript of CAGPO 2018: Cancer Associated Thrombosis · uOttawa.ca Objectives To develop a modern understanding...

uOttawa.ca
CAGPO 2018: Cancer Associated Thrombosis
Dr. Marc Carriere (thrombosis) and Dr. Sandy Sehdev (medical oncology)
uOttawa.ca
Faculté de médecine | Faculty of Medicine
uOttawa.ca
Objectives
To develop a modern understanding of the approach to the treatment of cancer associated thrombosis in the setting of
novel cancer treatmentsnewer anticoagulant choices for Rx
uOttawa.ca
Faculté de médecine | Faculty of Medicine
uOttawa.ca
Evaluation
Were the concepts presented clearly and logically?Do you feel comfortable managing CAT patients in the clinic?
uOttawa.ca
Faculté de médecine | Faculty of Medicine

uOttawa.ca
Disclosure: Dr. Sehdev
Grants/research support: noneHonoraria: Leo advisory board 2014, CAGPO presentation 2018Consulting fees: nonePatents: noneOther: travel support for this meeting
uOttawa.ca
Faculté de médecine | Faculty of Medicine

uOttawa.ca
Disclosure: Dr. Carrier
Grants/research support: BMS, Pfizer and Leo Pharma Honoraria: CAGPO presentation 2018, Bayer, Sanofi, BMS, Servier, Leo Pharma and Pfizer.Consulting fees: Patents: NoneOther: travel support for this meeting
uOttawa.ca
Faculté de médecine | Faculty of Medicine

uOttawa.ca
Mitigating potential bias
Neither Leo nor any other industry source has had direct input into the development of our contentOnly generic names will be used, without logosThe evidence basis for recommendations will be highlighted
uOttawa.ca
Faculté de médecine | Faculty of Medicine
uOttawa.ca
OverviewOverviewRisk factors — changing dynamic of patient populations
Rx factorsDisease factors
Current guidelines for Rx (guidance statement)Choice of agents — LMWH, oral DOACsPractical issues in management
bleedingreversalfailurethrombocytopeniabridging around proceduresdrug drug interactions
uOttawa.ca
Faculté de médecine | Faculty of Medicine

uOttawa.ca
Changing Landscape in Oncology: Patient Factors
Aging demographicNewer Rx: targeted Rx, biologics, immunotherapy
allow consideration in older, sicker patientsLonger survival / longer time on therapiesComorbidities
often on ASA or anticoagulants for cardiac indicationsTumoral bleeding risks: CNS mets, in-situ GI/GU malignancies
uOttawa.ca
Faculté de médecine | Faculty of Medicine

uOttawa.ca
Changing Landscape in Oncology: Treatment Factors
Thrombocytopenia: gemcitabine, carboplatin, T-DM1More complex protocols: FOLFIRINOX (pancreatic ca), …Myeloma: lenalidomide (VTE risk), hyperviscosityImmunotherapies: risk of bleeding from complications (colitis)Multiple new oral targeted Rxs: potential for drug interactions (cytochrome p450, P-glycoprotein,…)
uOttawa.ca
Faculté de médecine | Faculty of Medicine

uOttawa.ca
Changing Landscape in Oncology: Clinic Impact
Busy! How to handle prophylaxis, acute management of CATSpecialized thrombosis teams — not always availableSupport for home sc injection teaching / administration variesReview of renal function, drug interactionsPt education
uOttawa.ca
Faculté de médecine | Faculty of Medicine

uOttawa.ca
Format today: Discussion around a case
Lung cancerStage IIIPICC DVT issuesBumpy road: Rx and disease complications !Practical discussion around real issues !
uOttawa.ca
Faculté de médecine | Faculty of Medicine
42 F with cough, SOBpT3N2M0 NSCLC (squamous) of LUL — stage IIIa, unresectableRx: combined modality chemotherapy and radiationPET scans negative elswhere, brain MRI negativeStill smokingOtherwise well, no past hx of VTE
Rx: Cisplatin and etoposide chemotherapy daily iv x first 5 days and last 5 days of XRTXRT: 60 Gy over 5 weeksAdjuvant durvalumab immunotherapy iv q 2 wk - planned for 12 monthsPICC line required for iv access
CASE PRESENTATION
During week 2: swollen R arm (PICC side)
U/S confirms proximal arm DVT
CBC unremarkable, eGFR 65 mL/min
Risk factors: obese, sedentary, cancer, smoking, chemo, PICC line
Quits smoking!
Given 1 dose of LMWH in ER and next day F/U consultation arranged
CASE PRESENTATION

Should we have considered prophylactic anticoagulation before her chemotherapy?
1. Yes
2. No
INTERACTIVE QUESTIONS

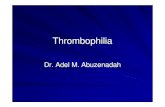
PREVALENCE OF CAT

Cumulative risk for VTE in patients with cancer undergoing chemotherapy.
Pancreas
StomachLungAllColon/rectumOvaryBladder
Adapted from Lyman GH, et al. The Oncologist. 2013;18:1321-1329.
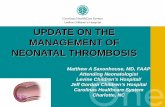
CHEMOTHERAPY FURTHER INCREASES RISK FOR VTE

Adapted from Lyman GH, et al. ASCO Update. J Clin Oncol. 2013;31:2189-204.

Kreuziger LB et al, Thrombosis Research 2017;157:64-71
• CRT represents approximately 70% of all upper extremity DVTs and 10% of all DVTs/PEs
• Risk factors include:
– Type of Central Venous Catheters
• PICC > implanted ports
– Location (i.e., junction of the superior vena cava and the right atrium)
– Insertion site
• femoral > subclavian > jugular
– Prior history of DVT/PE
– Metastatic disease
HOW COMMON ARE CATHETER-RELATED THROMBOSIS (CRT)
Kreuziger LB et al, Thrombosis Research 2017;157:64-71
• Mean duration from catheter insertion to a CRT diagnosis is 10 days
• Large majority of CRTs will occur in the initial 100 days following the insertion
WHEN TO THEY OCCUR?
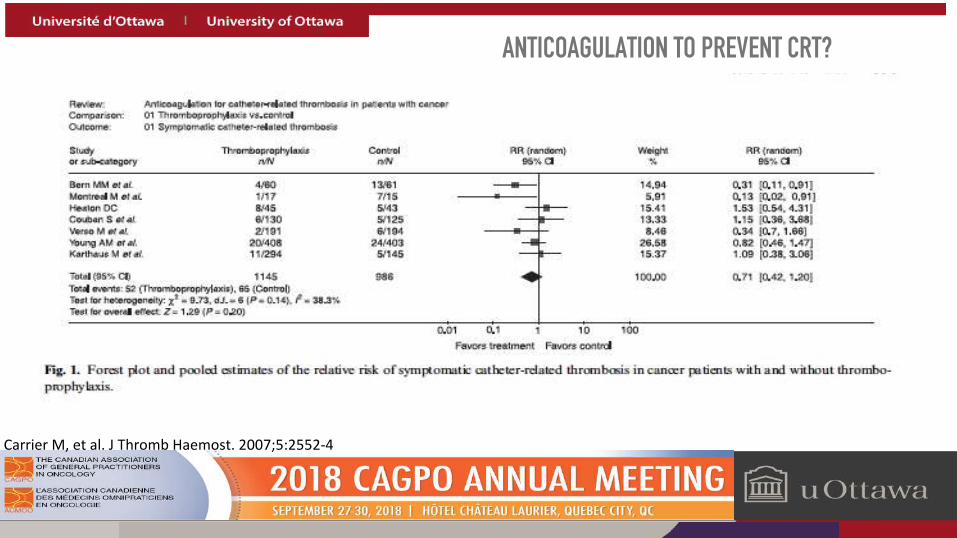
Carrier M, et al. J Thromb Haemost. 2007;5:2552-4
ANTICOAGULATION TO PREVENT CRT?

What would you prescribe?
1. LMWH long term — tinzaparin, dalteparin, enoxaparin
2. Oral direct oral anticoagulant
INTERACTIVE QUESTIONS

Zwicker JI et al, J Thromb Haemost 2014;12:796–800
ISTH Scientific and Standardization Committee guidance
• Therapeutic dose of anticoagulation without removal of the catheter is recommended if the CVC is functional and required for ongoing therapy
• If CVC needs to be removed (i.e., non-functioning), a short duration of anticoagulation (3–5 days) prior to removal is recommended
INITIAL MANAGEMENT OF CRT
Zwicker JI et al, J Thromb Haemost 2014;12:796–800 Carrier M, et al. Current Oncology 2015;22(1):49-59.
• No comparative studies between anticoagulant agents exist in any population of patients
• Borrowing from other cancer data, LMWH is typically recommended in those with active cancer
ACUTE AND LONG-TERM TREATMENT OF CRT

Delluc A, et al. Thromb Res. 2015;135:298-302.
• Recent retrospective cohort of ~100 patients with CRT and active cancer mostly treated with therapeutic LMWH as per CLOT trial regimens reported the following outcomes:
• No recurrent events in those on therapeutic LMWH
• Incidence of major bleeding was 3.7 per 100 patients years (2 required stopping anticoagulation)
LMWH FOR THE TREATMENT OF CRT

Davies et al, Thromb Res 2018 162:88-92.
DOAC FOR THE TREATMENT OF CRT
• Catheter-2 study• N=70 cancer patients with CRT• Rivaroxaban 15 mg PO BID X 21 days then 20 mg PO daily X 3 mo
• 100% Preservation of line function• 1 (1.4%) recurrent CAT – Fatal PE• 9 (12.5%) patients had 11 bleeding events
Carrier M, et al. Current Oncology 2015;22(1):49-59.
DOAC FOR THE TREATMENT OF CRT
• Catheter-2 study• N=70 cancer patients with CRT• Rivaroxaban 15 mg PO BID X 21 days then 20 mg PO daily X 3 mo
• 100% Preservation of line function• 1 (1.4%) recurrent CAT – Fatal PE• 9 (12.5%) patients had 11 bleeding events
What if she was elderly and arthritic, unable to self-inject?

What if her eGFR was 30 mL/min?

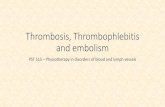
0
2
4
6
8
>60 mL/min 30-60 mL/min <30 mL/min
Multivariate Analysis of RisksFatal PE Fatal Bleed
Odd
s Rat
io
Monreal M, et al. Am J Med. 2006;119(12):1073-9
RENAL FAILURE INCREASES RISK OFFATAL PE AND FATAL BLEEDING

Woodruff S et al. J Thromb Thrombolysis 2016;42(4):494–505 Bauersachs R et al. Thromb Haemost 2018 May;118(5):914-921. .
Variable TreatmentEventsn/N %
Hazard ratio(95% CI)
p – value
VTE (ITT)(N = 162)
Dalteparin 2/74 2.7 0.15(0.03, 0.65)
0.01VKA 15/88 17.0
Major bleeding(N = 161)
Dalteparin 7/74 9.5 1.29(0.43, 3.83)
0.65VKA 6/87 6.9
Variable TreatmentEventsn/N %
Hazard ratio(95% CI)
p – value
VTE (ITT)(N = 131)
Tinzaparin 9/69 13.0 0.90(0.38, 2.12)
NSVKA 9/62 14.5
Major bleeding(N = 131)
Tinzaparin 3/69 4.3 0.54(0.13, 2.16)
NSVKA 5/62 8.1
CATCH patients with CrCl 20–59 mL/min
CLOT patients with CrCl <60 mL/min
LMWH FOR CAT IN PATIENTS WITH RENAL DYSFUNCTION

What if she has moderate daily gross hemoptysis from her tumour?

ISTH Scientific and Standardization Committee guidanceCVC removal without anticoagulation is only suggested if therapeutic anticoagulation cannot be safely administered due to active risk of haemorrhage
– On-going bleeding– Thrombocytopenic (low platelet count)
Close clinical follow-up. Serial US?
WHAT IF SHE HAD GROSS HEMOPTYSIS?
Zwicker JI et al, J Thromb Haemost 2014;12:796–800

Post Rx, her Hb is 86 and PLT 57 (ANC 0.9)
No active bleeding noted
Should we:
1. Hold anticoagulation until PLT > 100 then resume?
2. Discontinue Rx permanently?
3. Continue?
INTERACTIVE QUESTIONS

• Full anticoagulation (DOACs or LMWH) does not pose excessive risk when platelet count remains above 50 x 109/l
• Factors to consider:1. Time since index CAT
• Highest risk of recurrent VTE in initial 3 months
2. Thrombus burden: Massive PE vs. distal DVT
3. Severity of thrombocytopenia (< 50; 20-50; < 20)
ANTICOAGULATION DURING THROMBOCYTOPENIA
Samuelson Bannow BT et al. J Thromb Haemost. 2018 16:1246-1249.

Samuelson Bannow BT et al. J Thromb Haemost. 2018 16:1246-1249.
Platelets < 50 X 109/L
Able to maintain plateletswith transfusion (≥ 50)
Therapeutic doses
Unable to maintainplatelets
20-50
50% doseLMWH
< 20
Hold LMWH
THROMBOCYTOPENIA (< 1 MONTH)

Samuelson Bannow BT et al. J Thromb Haemost. 2018;16:1246-1249.
THROMBOCYTOPENIA (≥ 1 MONTH)
• ISTH SSC suggest reducing the dose of LMWH to 50% of the therapeutic dose or using a prophylactic dose of LMWH in patients with a platelet count of 20–50 X 109/L
• ISTH SSC suggest discontinuing anticoagulation in patients with a platelet count of < 20 X 109/L

Rx completed
Anticoagulation continued
CBC normalizes 4 wks later
Begins durvalumab (via private drug plan): 10 mg/kg iv q 2wk x up to 1 year for consolidation Rx
NEXT STEPS
IMMUNOTHERAPY

IMMUNOTHERAPY

Risk of colitis / GI bleeding
Newer anti PD-1 (nivolumab, pembrolizumab) or PD-L1 antibodies (atezolizumab, durvalumab): risks of diarrhea ~ 20% but grade 3-4 < 5$
ITP — rare
Pneumonitis, thyroid dysfunction, rash
IMMUNOTHERAPY ; ISSUES
At week 14, develops grade 3 diarrhea and hematochezia
Admitted to hospital
Anticoagulation held
INTERACTIVE QUESTIONS
Should we:
1. Stop anticoagulation for now and manage medically ?
2. Stop anticoagulation and reverse ?
3. Continue anticoagulation given importance ?
4. Stop anticoagulation permanently and d/c PICC?
INTERACTIVE QUESTIONS


MANAGEMENT OF BLEEDING
• Identify and stop all oral anticoagulants, parenteral anticoagulants and antiplatelet agents.
• Identify source of bleeding (if not already done)
• Supportive measures (Volume replacement and blood products as needed) to maintain hemodynamic stability and urine output.
• Consider tranaxemic acid (1 g IV)

thrombosiscanada.ca ON-LINE TOOL

Started on methylprednisolone 1 mg/kg iv q12h, iv hydration
Still diarrhea 8/d, watery and bloody
Anticoagulation discontinued
GI consulted: colonoscopy, biopsy = inflammatory colitis
On day 3, infliximab given iv
Diarrhea and bleeding resolved, oral prednisone 50 mg/d and tapered over 6 weeks
COLITIS

Rx discontinued, anticoagulation d/c’d after PICC outPost Rx CT = response in tumour, resolved nodes but primary still 2.3 cm
F/U CT at 3 mos = new bone (ribs, T6, L3, iliac crest) and liver mets (4, up to 3 cm)Started on chemotherapy with carboplatin (AUC 5) d1 and gemcitabine 1000 mg/m2 on d1,d8 q 3 wk, palliative intent
No further plans for immunotherapyCycle 2b — new 2+ L leg swelling
extensive proximal leg DVT confirmed on doppler U/Sno further hemoptysis or GI bleeding
FOLLOW UP

Choice of Rx?
1. LMWH agent for 6 mos ?
2. LMWH indefinitely ?
3. Oral DOAC for 6 mos ?
4. Oral DOAC indefinitely ?
INTERACTIVE QUESTIONS

Raskob et al. N Engl J Med 2018 Feb 15;378(7):615-624.
HOKUSAI VTE - CANCER STUDY DESIGN

Raskob et al. N Engl J Med 2018 Feb 15;378(7):615-624.
TIME TO VTE OR MAJOR BLEEDING

Recurrent VTE Major Bleeding Event-free Survival
HR 0.71 (0.48 – 1.06) HR 1.77 (1.03 – 3.04) HR 0.93 (0.77 – 1.11)p = 0.09 p = 0.04 p = NS
E 7.9% vs D 11.3% E 6.9% vs D 4.0% E 55.0% vs D 56.5%
COMPONENTS OF PRIMARY OUTCOME

Edoxaban (N = 522)
Dalteparin(N = 524)
Hazard Ratio(95% CI)
Major bleeding 36 (6.9%) 21 (4.0%) 1.77(1.03 – 3.04)
Fatal 0 2ICH 2 4
Upper GI 17 3Lower GI 3 3
TIME to VTE or Major bleeding
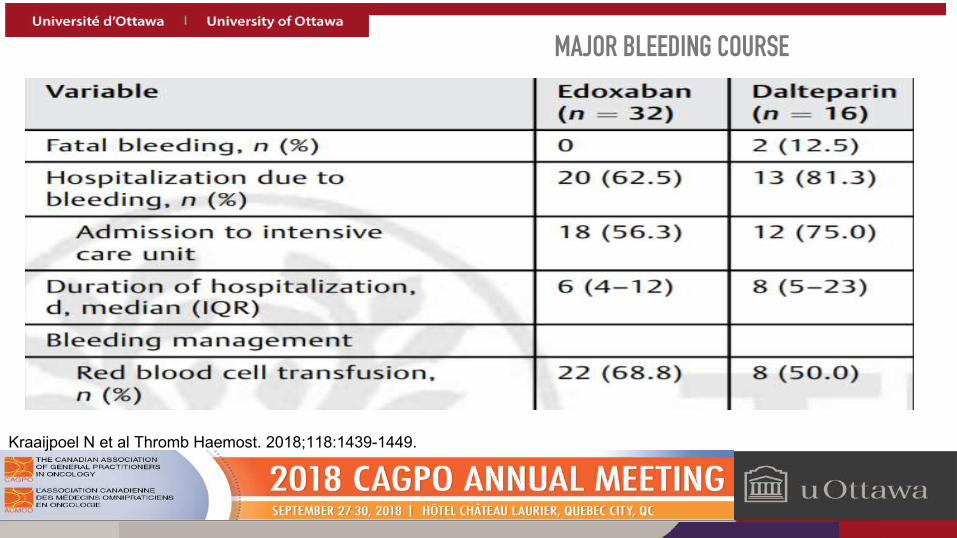
Kraaijpoel N et al Thromb Haemost. 2018;118:1439-1449.
MAJOR BLEEDING COURSE
Kraaijpoel N et al Thromb Haemost. 2018;118:1439-1449.
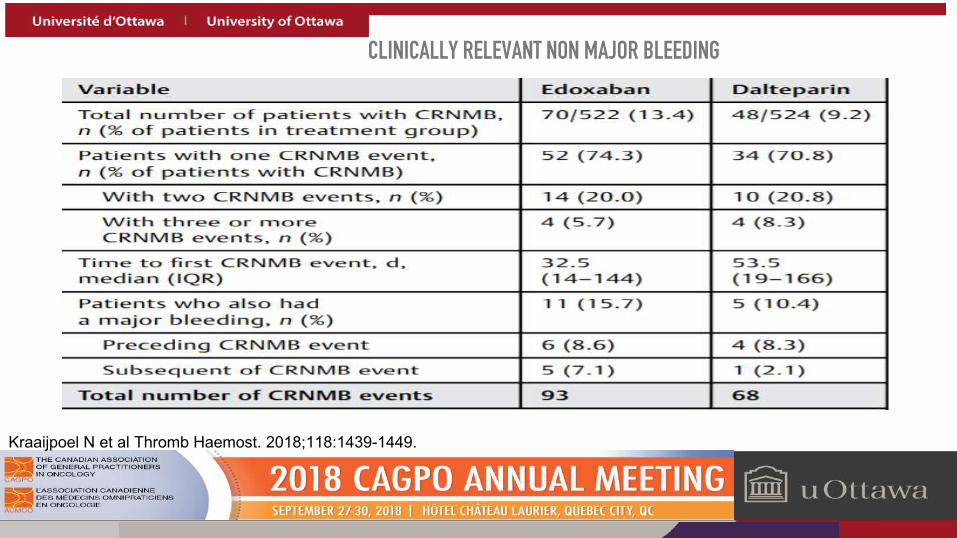
CLINICALLY RELEVANT NON MAJOR BLEEDING
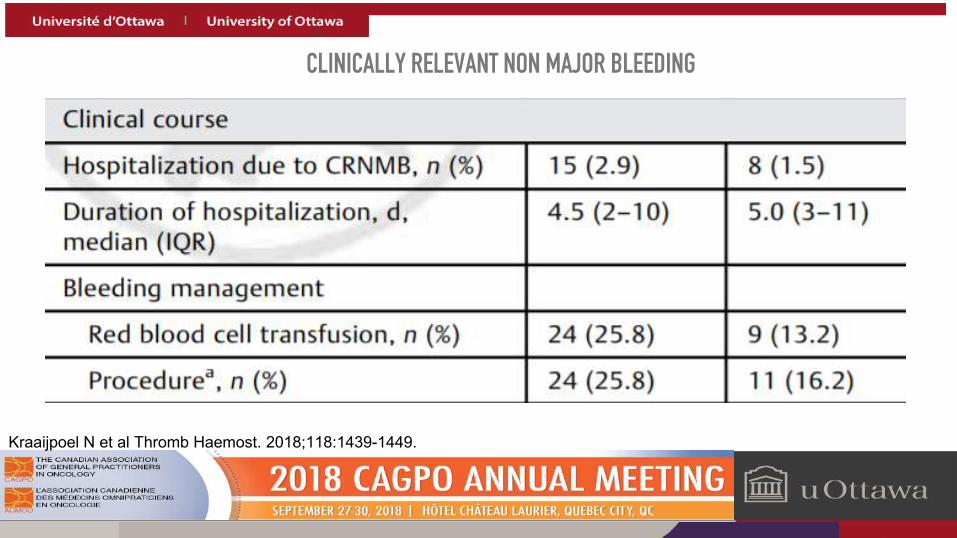
Kraaijpoel N et al Thromb Haemost. 2018;118:1439-1449.
CLINICALLY RELEVANT NON MAJOR BLEEDING

Carrier M et al. Current Oncol. 2018
ACUTE AND LONG-TERM TREATMENT OF CAT
uOttawa.ca
Patient is on multiple other drugs:
Importance of drug interactions ?Practicalities of assessment, pharmacy reviewMultiple new oral targeted Rxs: potential for drug interactions (cytochrome p450, P-glycoprotein,…)
uOttawa.ca
Faculté de médecine | Faculty of Medicine

Anticoagulant CYP3A4(metabolic)
P-gp(transport)
Other CYP metabolizing enzymes (2C9, 2C19, 2C8, 2C18, 1A2)
LMWH No No No
VKA Major No/Minor All (Major: CYP2C9)
Apixaban Major Major Minor: 1A2, 2C8, 2C9, 2C19
Edoxaban Minor Major No
Rivaroxaban Major Major No
Dabigatran No Moderate No
• DOACs and warfarin are substrates of key metabolic and transport pathways.
DRUG-DRUG INTERACTIONS

Kinase inhibitors CYP3A4 P-gpAfatinib ↓Alectinib ↓Ceritinib ↓Crizotinib ↓Dasatinib ↓Ibrutinib ↓Idelalisib ↓ ↓Imatinib ↓Lapatinib ↓ ↓Nilotinib ↓ ↓Osimertinib ↓Vemurafenib ↑ ↓Lenvatinib ↑ ↑
Chemotherapies CYP3A4 P-gpDoxurubicin ↓Topotecan ↓Vinblastine ↓Mitotane ↑Venetoclax ↓
Supportive care CYP3A4 P-gpAprepitant ↓Methylprednisolone ↓
Dexamethasone ↑ ↑
Inhibitors of CYP3A4 and/or P-gp may increase risk of bleeding on DOACs.
DRUG-DRUG INTERACTIONS
After cycle 3b, doppler and physical exam confirm more extensive DVTAsymptomatic segmental PE RLL noted on CT
FOLLOW UP

Given failure of anticoagulation:
1. Raise dose?
2. Change anticoagulation for DOAC (if started on LMWH) or LMWH (if started on DOAC)?
3. Continue same dose and same type of anticoagulation and hope for the best ?
4. Add anti platelet agent (ASA or clopidogrel) ?
INTERACTIVE QUESTIONS

RECURRENT CAT DESPITE ANTICOAGULATION
Antithrombotic Therapy for VTE Disease: CHEST Guidelines
In patients who have recurrent VTE on long-term LMWH (and are believed to be compliant), we suggest increasing the dose of LMWH by about one-quarter to one-third (Grade 2C).
Kearon C, et al. Chest. 2016 Feb;149(2):315-52.

Kearon C, et al. Chest. 2016 Feb;149(2):315-52.
RECURENT CAT DESPITE ANTICOAGULATION
Antithrombotic Therapy for VTE Disease: CHEST Guidelines
In patients who have recurrent VTE on VKA therapy (in the therapeutic range) or on dabigatran, rivaroxaban, apixaban, or edoxaban (and are believed to be compliant), we suggest switching to treatment with LMWH at least temporarily (Grade 2C).

Ihaddadene R, et al. Thromb Res. 2014;134(1):93-5; Carrier M, et al. J Thromb Haemost. 2009;7(5):760-765.
Ihaddadene et al. 2014 Carrier et al. 2009
Sample 55 70
Recurrent VTE 7.3%95% CI: 2.0-17.6%
8.6% 95% CI: 4.1-17.5%
Major bleeding 5.5%95% CI: 1.1-15.1%
4.3%95% CI: 1.5-11.9%
RECURRENT CAT DESPITE ANTICOAGULATION

Schulman S, et al. J Thromb Haemost. 2015;13:1010-1018.
• 212 patients with recurrent cancer-associated thrombosis despite anticoagulation followed for 3 months
• 70% LMWH; 30% VKA.• Acute phase:
▪ 25% switched anticoagulant (VKA → LMWH)▪ 31% dose escalation and 25% same dose
• Overall risk of recurrent VTE 11% (3 months)• ↔ risk of recurrent VTE: dose escalation vs. same dose
RECURRENT CAT DESPITE ANTICOAGULATION

RECURRENT CAT DESPITE ANTICOAGULATION

After cycle 4b chemotherapy:Partial response noted, all liver mets smaller (up to 2.1 cm), bones unchanged but pain improved and ALKP normalizedBrain MRI on restaging = 3 new brain mets: 1 cerebellar 1.2 cm and 2 cerebral (up to 2 cm with mild edema, mildly hemorrhagic)
Stereotactic XRT planned to CNS metsPLT now 47, Hb 92, ANC 1.2, eGFR 50 mL/min
CANCER RX

Now what to do?
1. D/C anticoagulant and place IVC umbrella filter
2. LMWH indefinitely ?
3. Oral DOAC for 6 mos ?
4. Oral DOAC indefinitely ?
INTERACTIVE QUESTIONS
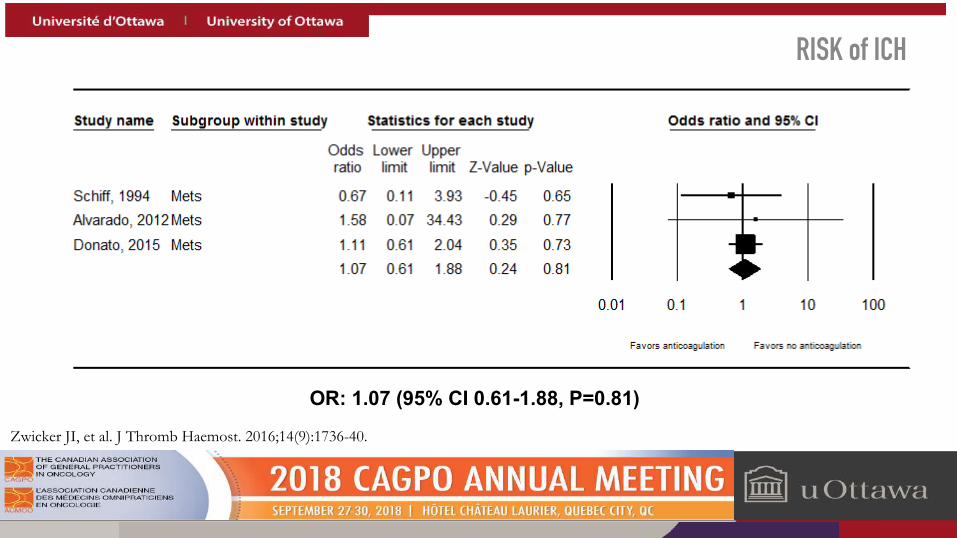
Zwicker JI, et al. J Thromb Haemost. 2016;14(9):1736-40.
OR: 1.07 (95% CI 0.61-1.88, P=0.81)
RISK of ICH

PREPIC Study Group. Circulation 2005;112:416-22; Mismetti P, et al. JAMA. 2015;313(16):1627-35.
IVC FILTERS
• PREPIC 1: Permanent filters and anticoagulation• N= 400• ↓ PE; ↑ DVT; ↔ survival
• PREPIC 2: Temporary filters and anticoagulation• N= 398• ↔ PE; ↔ DVT; ↔ survival; ↔ bleeding
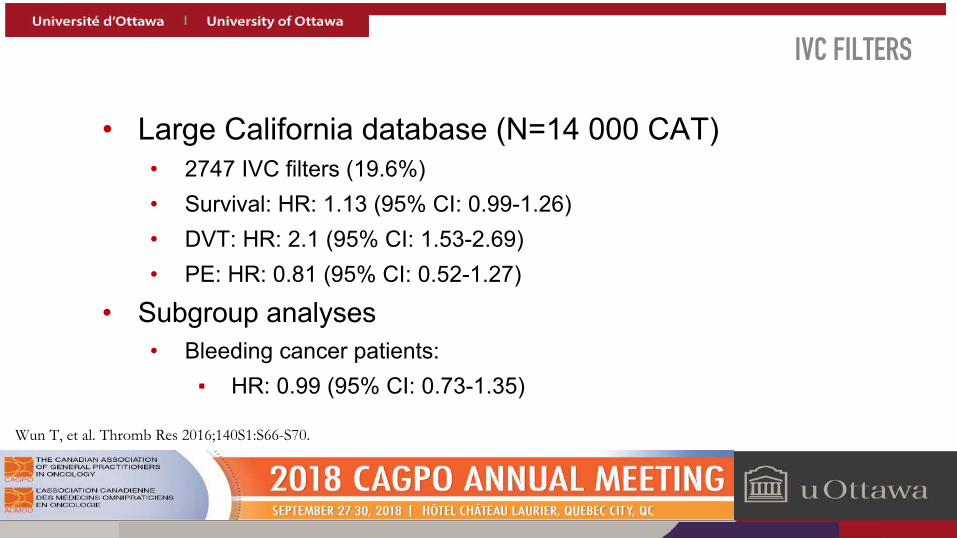
Wun T, et al. Thromb Res 2016;140S1:S66-S70.
• Large California database (N=14 000 CAT)• 2747 IVC filters (19.6%)• Survival: HR: 1.13 (95% CI: 0.99-1.26)• DVT: HR: 2.1 (95% CI: 1.53-2.69)• PE: HR: 0.81 (95% CI: 0.52-1.27)
• Subgroup analyses• Bleeding cancer patients:
▪ HR: 0.99 (95% CI: 0.73-1.35)
IVC FILTERS
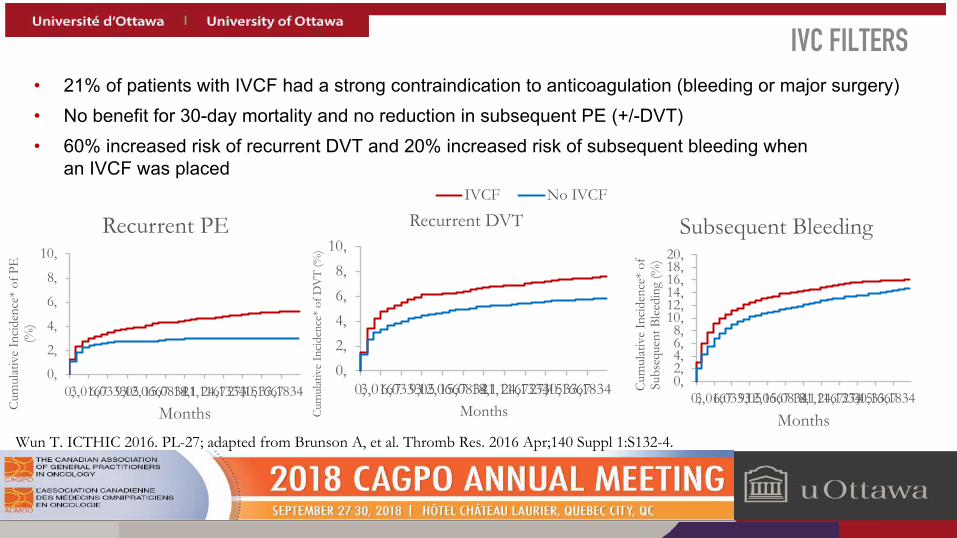
• 21% of patients with IVCF had a strong contraindication to anticoagulation (bleeding or major surgery)
• No benefit for 30-day mortality and no reduction in subsequent PE (+/-DVT)
• 60% increased risk of recurrent DVT and 20% increased risk of subsequent bleeding when an IVCF was placed
Wun T. ICTHIC 2016. PL-27; adapted from Brunson A, et al. Thromb Res. 2016 Apr;140 Suppl 1:S132-4.
0,
2,
4,
6,
8,
10,
0,3,01676,03339,0512,066715,083418,121,116724,133427,1530,166733,1834
Cum
ulat
ive
Inci
denc
e* o
f PE
(%
)
Months
Recurrent PE
0,2,4,6,8,
10,
0,3,01676,03339,0512,066715,083418,121,116724,133427,1530,166733,1834
Cum
ulat
ive
Inci
denc
e* o
f DV
T (%
)
Months
Recurrent DVTIVCF No IVCF
0,2,4,6,8,
10,12,14,16,18,20,
0,3,01676,03339,0512,066715,083418,121,116724,133427,1530,166733,1834
Cum
ulat
ive
Inci
denc
e* o
f Su
bseq
uent
Ble
edin
g (%
)
Months
Subsequent Bleeding
IVC FILTERS
Carrier M, et al. J Thromb Haemost. 2014 Jan;12(1):116-7.
ISTH Scientific and Standardization Committee guidance
• Recommend against IVC filter insertion in the absence of contraindications to anticoagulation
• Suggest IVC filter insertion in cancer patients with contraindications to anticoagulationand a high risk of potentially fatal PE
• Recommend resuming anticoagulation with LMWH and removing the retrievable filter in cancer patients when the contraindication has resolved
IVC FILTERS

uOttawa.ca
Evaluation
Were the concepts presented clearly and logically?Do you feel comfortable managing CAT patients in the clinic?
uOttawa.ca
Faculté de médecine | Faculty of Medicine
uOttawa.ca
CAGPO 2018: Cancer Associated ThrombosisTHANK YOU !
Dr. Marc Carriere (thrombosis) and Dr. Sandy Sehdev (medical oncology)
uOttawa.ca
Faculté de médecine | Faculty of Medicine