C. Michael Gibson, MS, MD Beth Israel Deaconess Medical Center Boston, MA The Benefit of Statin...
23
C. Michael Gibson, MS, MD Beth Israel Deaconess Medical Center Boston, MA The Benefit of Statin Therapy Before and After Coronary Revascularization
-
Upload
elfreda-riley -
Category
Documents
-
view
220 -
download
0
Transcript of C. Michael Gibson, MS, MD Beth Israel Deaconess Medical Center Boston, MA The Benefit of Statin...

C. Michael Gibson, MS, MD Beth Israel Deaconess Medical Center
Boston, MA
The Benefit of Statin Therapy Before and After Coronary
Revascularization

ARMYDA Trial
Peak CK-MBp = 0.007
Peak Troponin I p = 0.0008
Circulation 2004;110:674-8
ng
/mL
ng
/mL
Atorvastatin AtorvastatinPlacebo Placebo

ARMYDA-ACS Trial: BackgroundARMYDA-ACS Trial: Background
• The original ARMYDA study showed a reduction in The original ARMYDA study showed a reduction in peri-procedural MI with atorvastatin pre-treatment peri-procedural MI with atorvastatin pre-treatment in a low-risk, stable angina, elective PCI in a low-risk, stable angina, elective PCI population.population.
• The goal of the trial was to evaluate the effect of The goal of the trial was to evaluate the effect of atorvastatin compared with placebo among atorvastatin compared with placebo among patients with acute coronary syndromes (ACS) patients with acute coronary syndromes (ACS) undergoing percutaneous coronary intervention undergoing percutaneous coronary intervention (PCI).(PCI).
ACC 2007

ARMYDA-ACS Trial: Study DesignARMYDA-ACS Trial: Study Design
Primary Endpoint: 30 day major adverse cardiac events (MACE), defined Primary Endpoint: 30 day major adverse cardiac events (MACE), defined as death, myocardial infarction (MI), or unplanned revascularizationas death, myocardial infarction (MI), or unplanned revascularization
Secondary Endpoint: Post-procedural increase of markers of myocardial Secondary Endpoint: Post-procedural increase of markers of myocardial injury above the upper limit of normal (CK-MB, troponin-I, myoglobin); post-injury above the upper limit of normal (CK-MB, troponin-I, myoglobin); post-procedural variations from baseline CRP levels.procedural variations from baseline CRP levels.
Atorvastatin Atorvastatin (80mg 12h pre-PCI; 40mg (80mg 12h pre-PCI; 40mg
immediately pre-PCI)immediately pre-PCI)n=86n=86
Matching PlaceboMatching Placebo(80mg 12h pre-PCI; 40mg (80mg 12h pre-PCI; 40mg
immediately pre-PCI)immediately pre-PCI)n=85n=85
171 patients with non-ST-segment elevation ACS sent to early coronary angiography 171 patients with non-ST-segment elevation ACS sent to early coronary angiography within 48 hours. within 48 hours.
Placebo-controlled. Double-blind. Randomized. Mean follow-up 30 days.Placebo-controlled. Double-blind. Randomized. Mean follow-up 30 days.
Atorvastatin (40mg) indefinitely; Clopidogrel (75mg/day) 6 mos. post-PCI; Aspirin (100mg/day) indefinitelyMean age 66 years. 21% femaleMean age 66 years. 21% female
RR
30 day follow-up30 day follow-up
ACC 2007
Clopidogrel (600mg) loading Clopidogrel (600mg) loading dose at least 3h pre-PCI dose at least 3h pre-PCI

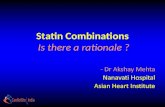
• Death, MI, or Death, MI, or unplanned unplanned revascularization revascularization was lower in the was lower in the atorvastatin (5%) atorvastatin (5%) group vs. placebo group vs. placebo group (17%) (p=0.01). group (17%) (p=0.01).
• This was driven by a This was driven by a reduction in peri-reduction in peri-procedural MI for the procedural MI for the atorvastatin group atorvastatin group (5% vs. 15%, p=0.04).(5% vs. 15%, p=0.04).
MA
CE
(%
)M
AC
E
(%)
ARMYDA-ACS Trial: Primary EndpointARMYDA-ACS Trial: Primary Endpoint
n = 86n = 86 n = 85n = 85
p = 0.01 p = 0.01
ACC 2007ACC 2007
Occurrence of MACE at 30 daysOccurrence of MACE at 30 days

ARMYDA-ACS Trial: Secondary EndpointARMYDA-ACS Trial: Secondary Endpoint
Patients (%) with elevated levels Patients (%) with elevated levels of CKMB and Troponin-I post-PCIof CKMB and Troponin-I post-PCI • Post-PCI CKMB Post-PCI CKMB
elevations occurred elevations occurred in fewer patients in in fewer patients in the atorvastatin the atorvastatin group than in the group than in the placebo group (7% placebo group (7% vs. 27%, p=0.001).vs. 27%, p=0.001).
•Troponin-I elevation Troponin-I elevation also occurred in also occurred in fewer patients in the fewer patients in the atorvastatin group atorvastatin group than in the placebo than in the placebo group (41% vs. 58%, group (41% vs. 58%, p=0.039).p=0.039).
n = 86n = 86 n = 85 n = 85 n = 86 n = 86 n = 85 n = 85 Pat
ien
ts w
ith
Po
st-P
CI
Pat
ien
ts w
ith
Po
st-P
CI
elev
atio
n
(%)
elev
atio
n
(%)
p = 0.039p = 0.039p = 0.039p = 0.039
p = 0.001p = 0.001
ACC 2007ACC 2007

• The percent The percent increase in CRP increase in CRP from baseline from baseline was lower in the was lower in the atorvastatin atorvastatin group (63%) than group (63%) than in the placebo in the placebo group (147%) group (147%) (p=0.01).(p=0.01).
Incr
ease
in C
RP
from
bas
elin
e (
%)
Incr
ease
in C
RP
from
bas
elin
e (
%)
ARMYDA-ACS Trial: Secondary EndpointARMYDA-ACS Trial: Secondary Endpoint
n = 86n = 86 n = 85n = 85
p = 0.01 p = 0.01
ACC 2007
Percent increase in CRP from pre to post-PCIPercent increase in CRP from pre to post-PCI

ARMYDA-ACS Trial: LimitationsARMYDA-ACS Trial: Limitations
• The optimal timing of a pre-treatment atorvastatin The optimal timing of a pre-treatment atorvastatin load is unknown, as is the impact of delaying PCI load is unknown, as is the impact of delaying PCI to pre-treat with atorvastatin in an ACS to pre-treat with atorvastatin in an ACS population.population.
• Pre-treatment in the present study was for 12 Pre-treatment in the present study was for 12 hours, with a mean time to PCI of 23 hours. hours, with a mean time to PCI of 23 hours. However, in an unstable population, time to However, in an unstable population, time to revascularization is often shorter.revascularization is often shorter.
ACC 2007ACC 2007

Meta-Analysis of the Role of Statin Therapy in Reducing Myocardial
Infarction Following Elective Percutaneous Coronary
Intervention
Meta-Analysis of the Role of Statin Therapy in Reducing Myocardial
Infarction Following Elective Percutaneous Coronary
Intervention
Girish R. Mood, MD; Anthony A. Bavry, MD, MPH; Henri Roukoz, MD; and Deepak L. Bhatt, MD
Girish R. Mood, MD; Anthony A. Bavry, MD, MPH; Henri Roukoz, MD; and Deepak L. Bhatt, MD

Methods
• Mood et al. selected studies that randomized patients who underwent elective PCI to statin therapy versus placebo / usual care.
• To be included, statin therapy was required to be initiated around the time of coronary intervention, and individual outcome data were required to be collected.
• The primary end point was MI.
• The secondary end points were all-cause mortality, cardiovascular mortality, surgical or percutaneous revascularization, and stroke.
Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23 Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23

• 6 studies were selected: PREDICT- Prevention of Restenosis by Elisor After
Transluminal Coronary Angioplasty FLARE- Fluvastatin Angioplasty Restenosis GAIN- German Atorvastatin Intravascular
Ultrasound LIPS- Lescol Intervention Prevention Study ARMYDA- Atorvastatin for Reduction of
Myocardial Damage During Angioplasty Briguori et al- Randomized 3,941 patients (1,967 to
statins and 1,974 to placebos)
Studies Included in Meta-Analysis
Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23 Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23

Cholesterol Data of Study Participants (Statin Arm/ Placebo Arm)
Variable PREDICT FLARE GAIN LIPS ARMYDA Briguori et al
Baseline Total cholesterol
(mg/dl)228/231 222/223 228/242 200/199 -- 197/196
LDL cholesterol
(mg/dl)155/157 153/153 155/166 131/132 -- 121/122
Follow-up Total cholesterol
(mg/dl)195/239 -- 156/215 -- -- 168/193*
LDL cholesterol
(mg/dl)119/159 102/149 86/140 95/147 -- 93/121*
* Level at index procedure
LDL = low-density lipoprotein
* Level at index procedure
LDL = low-density lipoprotein
Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23 Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23

Odds Ratio Odds Ratio 95% CI95% CI
OR=0.57
(0.42-0.78)
PREDICTPREDICT
FLAREFLARE
GAINGAIN
LIPSLIPS
BriguoriBriguori
ARMYDAARMYDA
OverallOverall
Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23 Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23
Odds of MI after PCIOdds of MI after PCI

Cumulative Cardiovascular Mortality Results
• The cumulative incidence of cardiovascular mortality in patients among the statin group vs placebo group was 0.71% vs 1.2%, respectively (OR 0.58, 95% CI 0.30 to 1.11, p=0.10).
• The weighted mean duration of follow-up was 20.6 months, and the absolute difference between the groups was 0.8% ( p = 0.10).
Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23 Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23

Cumulative Repeat Surgical or Percutaneous Revascularization
• Among the patients randomized to statin therapy versus placebo, the cumulative incidence of repeat surgical or percutaneous revascularization was 19.6% vs 21.9%, respectively (OR 0.89, 95% CI 0.78 to 1.02, p = 0.098).
• The weighted mean duration of follow-up was 22.7 months, and the absolute difference between the groups was 2.3% ( p = 0.098).
Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23 Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23

Limitations
• The follow-up periods ranged from 1 day to 45 months, making it difficult to assess the long-term benefits of statin therapy.
Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23 Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23

Conclusion
• Statin therapy initiated at the time of elective PCI significantly reduces myocardial infarction.
• The reduction in MI appeared to occur early and was sustained late after PCI. It is possible that the initiation of statin therapy before PCI may be preferential to initiation after the procedure.
Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23 Mood et al. Am J Cardiol. 2007 Sep 15;100(6):919-23

Intensive Lipid Lowering and TVR (Clinical Restenosis) Intensive Lipid Lowering and TVR (Clinical Restenosis) and Non-TVR (Lesion Progression) and Non-TVR (Lesion Progression)
TVRp = 0.001
MV O.R. 0.63, p=0.001*
Non-TVRp = 0.012
MV O.R. 0.87, p=0.364*
% %
* MV model adjusted for on treatment LDL
11.6%
16.0%
8.5%
11.3%
Atorva 80 mg Atorva 80 mgPrava 40 mg Prava 40 mg
(167/1440) (227/1420) (122/1440) (227/1420)
Gibson CM, ACC 2005

%
p=0.004p=0.004 p=0.003p=0.003
N=367N=367 N=44N=44N= 429 N= 429 N= 49 N= 49
* Statin use within 2 weeks
Association of Statin Use with Myocardial Association of Statin Use with Myocardial Perfusion After FibrinolysisPerfusion After Fibrinolysis
Gibson CM 2004Gibson CM 2004

Simvastatin Prior to CABG is Associated with Improved Post Operative Flow on PET Scanning
Imp
rov
eme
nt
in P
ET
Blo
od
Flo
w
1.3
9.6
3.8
48.6
PlaceboDotani, … Gibson Am J Cardio 2003; 91: 1107-9
Simvastatin
Bypassed Segment
Bypassed Segment
Non- Bypassed Segment
Non- Bypassed Segment
p<0.001

1 Year MACE After CABG: Comparison of Statin vs Other Lipid- 1 Year MACE After CABG: Comparison of Statin vs Other Lipid- Lowering Agent Before CABGLowering Agent Before CABG
Post-operative incidence of Death, MI, Post-operative incidence of Death, MI, Unstable angina, Arrhythmia, CHF, StrokeUnstable angina, Arrhythmia, CHF, Stroke
% O
ccu
rren
ce A
E%
Occ
urr
ence
AE
The risk of The risk of Death/MI was Death/MI was reduced from 8% reduced from 8% to 0% (p=0.01)to 0% (p=0.01)
18%
57%
p<0.0001p<0.0001
Dotani, … Gibson et al Am J Cardio 2003
No statinNo statin StatinStatin

ARMYDA-3 Trial: Primary EndpointARMYDA-3 Trial: Primary Endpoint
Post-operative occurrence of atrial Post-operative occurrence of atrial fibrillation (%) p=0.003fibrillation (%) p=0.003
% O
ccu
rren
ce A
F%
Occ
urr
ence
AF
Presented at ACC 2006Presented at ACC 2006
200 patients200 patients undergoing undergoing elective cardiac surgery elective cardiac surgery were randomized to were randomized to either atorvastatin or either atorvastatin or placeboplacebo beginning 7 beginning 7 days before the days before the operation operation Placebo-controlled. Placebo-controlled. Randomized. BlindedRandomized. BlindedPatients had no previous Patients had no previous history of statin history of statin treatment or atrial treatment or atrial fibrillationfibrillation

Mechanisms by Which Statins Reduce Reperfusion InjuryMechanisms by Which Statins Reduce Reperfusion Injury
• Reduce monocyte CD11b expression and monocyte adhesion to Reduce monocyte CD11b expression and monocyte adhesion to the endothelium in patients independent of cholesterol-lowering the endothelium in patients independent of cholesterol-lowering effect CD11b is the effect CD11b is the αα-chain of the -chain of the ββ2-integrins, which promote 2-integrins, which promote firm adhesion of leukocytes to the endotheliumfirm adhesion of leukocytes to the endothelium
• Inhibit neutrophil and monocyte chemotaxisInhibit neutrophil and monocyte chemotaxis
• Upregulation of endothelial NO synthesis or inhibit hypoxia-Upregulation of endothelial NO synthesis or inhibit hypoxia-mediated inhibition of NOS mediated inhibition of NOS
NO has been shown to act as a physiological inhibitor of NO has been shown to act as a physiological inhibitor of leukocyte– endothelial cell interaction by suppressing leukocyte– endothelial cell interaction by suppressing upregulation of several endothelial cell adhesion molecules, upregulation of several endothelial cell adhesion molecules, including P-selectin,VCAM-1, and ICAM-1including P-selectin,VCAM-1, and ICAM-1