
by cardiomyopathy: a - Heartheart.bmj.com/content/heartjnl/63/1/26.full.pdf · W 1020 30 50 70 90...
6
Br Heart J 1990;63:26-31 Short term haemodynamic effects of converting enzyme inhibition before and after eating in patients with moderate heart failure caused by dilated cardiomyopathy: a double blind study Bo Herrlin, Christer Sylven, Olof Nyquist, Olof Edhag Abstract The haemodynamic changes that follow a meal can mimic the response to a vasodilator drug. To avoid overestimat- ing the beneficial effects of treatment in uncontrolled studies, measurements of haemodynamic function are usually performed with patients in the fasting postabsorptive state. But such recordings are not representative of the resting patient during daily life. In this double blind placebo controlled study the short term haemodynamic effects of enalapril were assessed during 12 hours in 19 patients with moderate heart failure caused by dilated cardiomyopathy. The patients ate lunch and dinner and were studied in the absorptive and postabsorp- tive phases. In the placebo group systemic vascular resistance, mean arterial pres- sure, and the rate-pressure product fell significantly (5-16%) after lunch. Four hours after lunch the haemodynamic function had returned to baseline-that is the postabsorptive state. Enalapril, accentuated the haemodynamic effects during the absorptive state producing a larger post-prandial fall in mean arterial blood pressure and rate-pressure product and changes in the absorptive phase were maintained into the post- absorptive phase. Pulmonary wedge pressure fell significantly after treatment with enalapril. These overall changes during the study period indicated that enalapril reduced the preload and after- load on the heart-over and above the reduction produced by eating. These findings suggest that the effects of enalapril given at rest to patients with moderate heart failure unload the heart and enhance the reduction of afterload induced by meals. Cardiac Division, Department of Medicine, Huddinge University Hospital, Huddinge, Sweden B Herrlin C Sylven O Nyquist O Edhag Correspondence to Dr Bo Herrlin, Department of Medicine, Huddinge Hospital, S-141 86 Huddinge, Sweden. Accepted for publication 20 July 1989 The haemodynamic effects of drugs are usually studied in fasting patients. Such recordings do not represent the effects in resting patients who are eating normally. Splanchnic vasodilatation in the absorptive phase may change central haemodynamic function'` by reducing the sys- temic afterload. Activation of the renin-angiotensin system, which increases systemic vascular resistance,4 is an important compensatory mechanism in treated heart failure. Angiotensin-converting enzyme inhibitors cause systemic vasodilata- tion and reduce the load on the heart.56 In heart failure such drugs may enhance the haemo- dynamic effects seen in the absorptive phase. We investigated the complex haemodynamic effects of enalapril and eating and absorption in a double blind, controlled, randomised study in a homogeneous group of patients with treated moderate heart failure caused by dilated cardiomyopathy. We studied the angiotensin- converting enzyme inhibitor, enalapril, because its bioavailability was reported not to be influenced by food intake7 and because a single oral dose gives therapeutic serum con- centrations throughout a 12 hour study period. Patients and methods PATIENTS We studied 19 patients (16 men and three women (41-62 years old (mean (SD)) 51 (6) years)), with moderate heart failure caused by dilated cardiomyopathy, which was treated with digoxin and frusemide. None of the patients had oedema and all had been clinically stable for at least two weeks. Inclusion criteria were an echocardiographically determined left ventricular end diastolic dimension of >30 mm/m2, a left ventricular shortening fraction of < 20%, and an exercise capacity of > stage III and < stage IX according to a revised Naugh- ton protocol.8 We excluded patients with primary valve disease, suspected ischaemic heart disease, or congenital valve disease; those taking concomitant vasodilating agents; and those with right sided heart failure caused by pulmonary disease. The study protocol was approved by the local ethics committee. All patients gave their informed consent before entering the study. PROTOCOL The patient was admitted to hospital and served meals containing a known concentration of sodium. The daily doses of digoxin and frusemide remained unchanged. On the first day the blood volume was determined and echocardiography, a chest x ray, and an exer- cise test were performed. Serum albumin labelled with iodine-131 was used to measure the total blood volume. Echocardiography was performed on patients in the left lateral position (ATL Mark III, 13 mm and 3 MHz transducer). The transducer position and cardiographic gain were adjusted to obtain optimal recordings of 26 on 27 June 2018 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.63.1.26 on 1 January 1990. Downloaded from
Transcript of by cardiomyopathy: a - Heartheart.bmj.com/content/heartjnl/63/1/26.full.pdf · W 1020 30 50 70 90...

Br Heart J 1990;63:26-31
Short term haemodynamic effects of convertingenzyme inhibition before and after eating inpatients with moderate heart failure caused bydilated cardiomyopathy: a double blind study
Bo Herrlin, Christer Sylven, Olof Nyquist, Olof Edhag
AbstractThe haemodynamic changes that follow ameal can mimic the response to avasodilator drug. To avoid overestimat-ing the beneficial effects of treatment inuncontrolled studies, measurements ofhaemodynamic function are usuallyperformed with patients in the fastingpostabsorptive state. But such recordingsare not representative of the restingpatient during daily life. In this doubleblind placebo controlled study the shortterm haemodynamic effects of enalaprilwere assessed during 12 hours in 19patients with moderate heart failurecaused by dilated cardiomyopathy. Thepatients ate lunch and dinner and werestudied in the absorptive and postabsorp-tive phases. In the placebo group systemicvascular resistance, mean arterial pres-sure, and the rate-pressure product fellsignificantly (5-16%) after lunch. Fourhours after lunch the haemodynamicfunction had returned to baseline-thatis the postabsorptive state. Enalapril,accentuated the haemodynamic effectsduring the absorptive state producing alarger post-prandial fall in mean arterialblood pressure and rate-pressureproduct and changes in the absorptivephase were maintained into the post-absorptive phase. Pulmonary wedgepressure fell significantly after treatmentwith enalapril. These overall changesduring the study period indicated thatenalapril reduced the preload and after-load on the heart-over and above thereduction produced by eating.These findings suggest that the effects
of enalapril given at rest to patients withmoderate heart failure unload the heartand enhance the reduction of afterloadinduced by meals.
Cardiac Division,Department ofMedicine, HuddingeUniversity Hospital,Huddinge, SwedenB HerrlinC SylvenO NyquistO EdhagCorrespondence toDr Bo Herrlin, Departmentof Medicine, HuddingeHospital, S-141 86Huddinge, Sweden.
Accepted for publication20 July 1989
The haemodynamic effects of drugs are usuallystudied in fasting patients. Such recordings donot represent the effects in resting patients whoare eating normally. Splanchnic vasodilatationin the absorptive phase may change centralhaemodynamic function'` by reducing the sys-temic afterload.
Activation of the renin-angiotensin system,which increases systemic vascular resistance,4is an important compensatory mechanism intreated heart failure. Angiotensin-converting
enzyme inhibitors cause systemic vasodilata-tion and reduce the load on the heart.56 In heartfailure such drugs may enhance the haemo-dynamic effects seen in the absorptive phase.We investigated the complex haemodynamic
effects of enalapril and eating and absorption ina double blind, controlled, randomised study ina homogeneous group of patients with treatedmoderate heart failure caused by dilatedcardiomyopathy. We studied the angiotensin-converting enzyme inhibitor, enalapril,because its bioavailability was reported not tobe influenced by food intake7 and because asingle oral dose gives therapeutic serum con-centrations throughout a 12 hour study period.
Patients and methodsPATIENTSWe studied 19 patients (16 men and threewomen (41-62 years old (mean (SD)) 51 (6)years)), with moderate heart failure caused bydilated cardiomyopathy, which was treatedwith digoxin and frusemide. None of thepatients had oedema and all had been clinicallystable for at least two weeks. Inclusion criteriawere an echocardiographically determined leftventricular end diastolic dimension of >30mm/m2, a left ventricular shortening fraction of< 20%, and an exercise capacity of > stage IIIand < stage IX according to a revised Naugh-ton protocol.8 We excluded patients withprimary valve disease, suspected ischaemicheart disease, or congenital valve disease; thosetaking concomitant vasodilating agents; andthose with right sided heart failure caused bypulmonary disease. The study protocol wasapproved by the local ethics committee. Allpatients gave their informed consent beforeentering the study.
PROTOCOLThe patient was admitted to hospital andserved meals containing a known concentrationof sodium. The daily doses of digoxin andfrusemide remained unchanged. On the firstday the blood volume was determined andechocardiography, a chest x ray, and an exer-cise test were performed. Serum albuminlabelled with iodine-131 was used to measurethe total blood volume.Echocardiography was performed on
patients in the left lateral position (ATL MarkIII, 13 mm and 3 MHz transducer). Thetransducer position and cardiographic gainwere adjusted to obtain optimal recordings of
26
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.63.1.26 on 1 January 1990. D
ownloaded from
Short term haemodynamic effects of enalapril before and after eating
left ventricular dimensions in the short axis.We measured the left ventricular end diastolicdiameter (LVEDD) and left ventricular endsystolic diameter (LVESD).9 The mean valuefor five consecutive beats was calculated. Theleft ventricular shortening fraction was derivedfrom the difference between LVEDD andLVESD divided by LVEDD.
Cardiac volume was measured radiologicallyby Jonsell's method.'0 Patients performed theexercise test sitting on an electrically brakedergometer. The load was increased every twominutes according to a modified Naughtonprotocol':Stage I II III IV V VI VII VIII IXW 10 20 30 50 70 90 110 130 150The patients exercised until limiting symp-
toms developed-that is dyspnoea or fatigue orboth.On the third day at 5.30 am the patient was
given a light breakfast and his or her daily doseof digoxin and frusemide. The right ventriclewas catheterised at 8 am. A triple lumenballoon tipped thermodilution catheter(Edwards Laboratory, USA) was introducedvia an antecubital or femoral vein underfluoroscopic guidance and was used to measurethe right atrial, pulmonary arterial, andpulmonary capillary wedge pressures. A poly-ethylene arterial catheter was introduced intothe brachial or femoral artery to measuresystemic pressure. The patient was placed inbed and transported to the coronary care unitfor haemodynamic monitoring for 12 hoursafter two hours of rest. We used Hewlett-Packard transducers (HP 1290) and a Hewlett-Packard patient monitoring system (Model HP78342A). All haemodynamic measurementswere done by the same physician (BH). Themeasurements ofhaemodynamic function weremade with the zero reference level at themidaxillary line with the patient supine and thebed in a horizontal position. Before eachhaemodynamic measurement we checked thatthe zero transducer pressure was the sameas atmospheric pressure; calibration scaleswere displayed electronically. Cardiac outputwas measured by a bedside cardiac outputcomputer (Cardiac Computer, EdwardsLaboratories, model 9520) with the use of an
iced injectate. Heart rate was derived from a
continuously recorded electrocardiogram. Thepatients were randomised double blindly toenalapril 10 mg or placebo, and drugs were
given at 0 hours. Recordings were made at 0, 1,2, 3, 4, 5, 6, 8, and 12 hours. The patients ateportions of meals of their own choice after oneand five hours. Snacks and coffee or tea were
not allowed but water was available.Serum concentrations of enalaprilat were
measured by radioimmunoassay."
ANALYSES
Mean right atrial pressure (RAP), mean
pulmonary artery pressure (MPAP), mean pul-monary capillary wedge pressure (PCWP),systolic systemic arterial pressure (SAP), andmean systemic arterial pressure (MAP) weremeasured by electronic integration. The mean
of at least six determinations was calculated;each was the average for 12 seconds. Cardiacoutput (CO) was determined in triplicate.Heart rate (HR) was determined for one min-ute. Derived haemodynamic variables werecalculated as follows:
Cardiac index (CI) (1/min/m2) = CO/body surface area
Stroke volume index (SVI) (ml/beat/m2) =CI/HR
Systemic vascular resistance (SVR)(dyn.s.cmn5)
= 80 x (MAP-RAP)/COPulmonary vascular resistance (PVR)
(dyn.s.cm5) = 80 x (MPAP-PCWP)/CORate-pressure product (RPP) (beats.mm Hg
min) = HR x SAP
STATISTICAL ANALYSISValues are given as means (SD). Unpaired ttests were used to evaluate differences betweentwo groups. Multiple comparisons of repeatedmeasurements were tested by analysis ofvariance and Fisher's protected least squaresignificance test. A p value of <0 05 wasregarded as significant.
ResultsTen patients were randomly allocated toenalapril and nine to placebo. One patientbecame symptomatically hypotensive six hoursafter administration of enalapril and was suc-cessfully treated with an infusion of saline.This patient was excluded from further study.The remaining 18 patients completed the studywithout complications.Table 1 shows the clinical characteristics and
non-invasive findings. The mean heart volumeand the daily dose of frusemide were signifi-cantly larger in the group receiving enalaprilthan in the placebo group (p < 0-05). Othercharacteristics were similar in the two groups.All patients had concentrations of serumsodium within the normal range.There were no significant differences in
haemodynamic variables between the twogroups at baseline (0 hour, table 2).
Table 1 Clinical characteristics, non-invasivefindings,blood volume, and serum sodium
Placebo group Enalapril group(n= 9) (n= 9) pvalue
Age (yr) 53 (3) 50 (7) NSSex (F/M) 2/7 1/8 NSDuration of symptoms
(mnth) 21 (12) 41 (30) NSFrusemide dosage
(mg/day) 98 (45) 158 (65) <0 05ECG (AF/SR) 2/7 3/6 NSExercise duration (s) 701 (93) 692 (173) NSChest x ray, heartvolume (ml/m') 712 (144) 872 (168) <0-05
Echocardiography:LVEDD (mm/m') 37 (5) 39 (3) NSFS (%) 11 (4) 11 (3) NS
Bloodvolume(1) 5-8 (1-4) 6-3 (1 3) NSSerum sodium (mmol/l) 140 (2) 142 (2) NS
AF, atrial fibrillation; FS, left ventricular fractional shortening;LVEDD, left ventricular end diastolic diameter; SR, sinusrhythm.
27
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.63.1.26 on 1 January 1990. D
ownloaded from
Herrlin, Sylven, Nyquist, Edhag
Table 2 Haemodynamic measurements (mean (SD)) in the placebo and enalapril groups
Placebo group
Baseline Absorptive phase Postabsorptive phase
Oh 2h 3h Sh
HR 82 (14) 81 (11) 82 (8) 83 (12)RAP 4 (3) 5 (3) 5 (4) 5 (4)*MPAP 20 (8) 19 (6) 19 (5) 21 (8)PCWP 1 1 (8) 10 (7) 10 (6) 12 (8)MAP 85 (9) 81 (9)* 80 (12)* 84 (10)CI 2 5 (0-5) 2-8 (0.5)** 2-7 (0 6)* 2-5 (0 6)SVI 31 (8) 35 (8)*** 33 (9) 30 (9)SVR 1402 (308) 1176 (245)*** 1194 (230)*** 1371 (268)PVR 159 (37) 144 (38) 136 (46)** 158 (53)RPP 9422 (1729) 8914 (1567)* 8915 (1605)* 9227 (1621)
Statistical differences within groups compared with baseline are indicated as *p < 0 05, **p < 0-01, ***p < 0-001.Statistical differences in changes from baseline between groups are indicated as tp < 0-05, ttp < 0-01.HR, heart rate (beats/min); RAP, right atrial pressure (mm Hg); MPAP, mean pulmonary artery pressure (mm Hg); PCWP, pulmonary capillarywedge pressure (mm Hg); MAP, mean arterial pressure (mm Hg); CI, cardiac index (1/min/m2); SVI, stroke volume index (ml/m2); SVR, systemicvascular resistance (dyn.s.cm'); PVR, pulmonary vascular resistance (dyn.s.cmnf); RPP, rate-pressure product (beats. mm Hg/min).
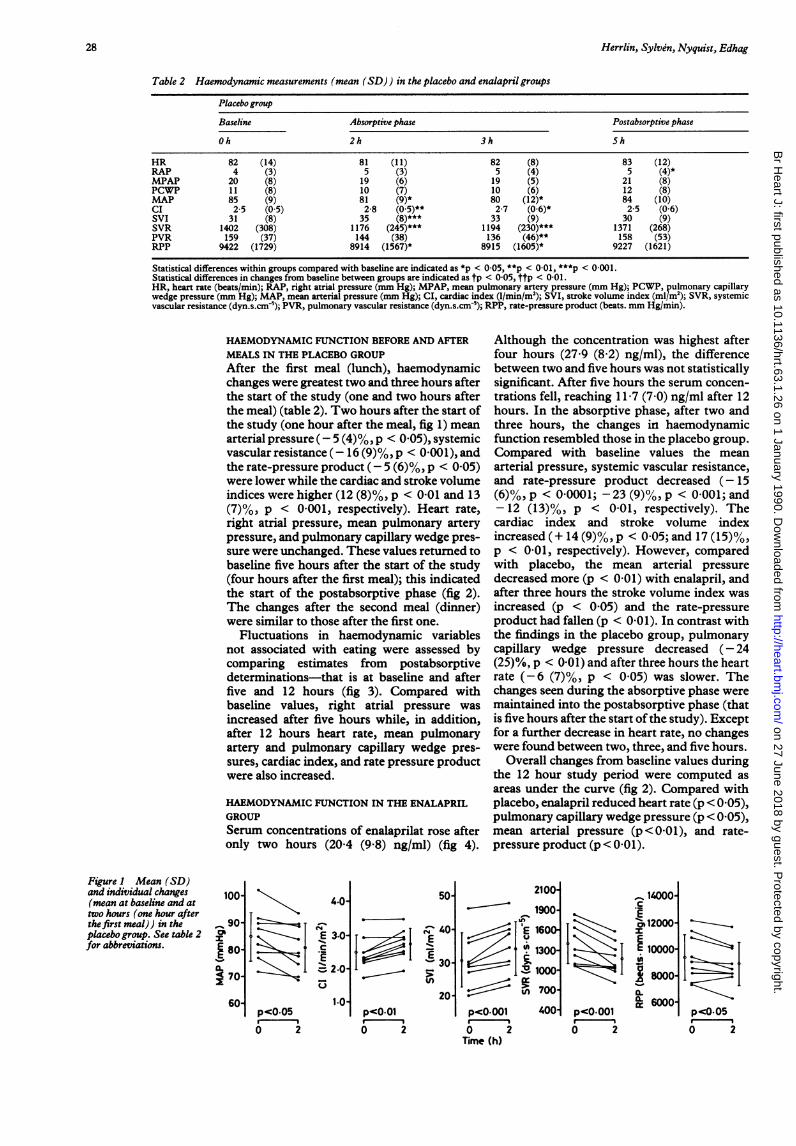
HAEMODYNAMIC FUNCTION BEFORE AND AFTERMEALS IN THE PLACEBO GROUPAfter the first meal (lunch), haemodynamicchanges were greatest two and three hours afterthe start of the study (one and two hours afterthe meal) (table 2). Two hours after the start ofthe study (one hour after the meal, fig 1) meanarterial pressure (- 5 (4)%, p < 0 05), systemicvascular resistance (- 16 (9)%, p < 0-001), andthe rate-pressure product (-5 (6)%, p < 0 05)were lower while the cardiac and stroke volumeindices were higher (12 (8)%, p < 0-01 and 13(7)%, p < 0-001, respectively). Heart rate,right atrial pressure, mean pulmonary arterypressure, and pulmonary capillary wedge pres-sure were unchanged. These values returned tobaseline five hours after the start of the study(four hours after the first meal); this indicatedthe start of the postabsorptive phase (fig 2).The changes after the second meal (dinner)were similar to those after the first one.
Fluctuations in haemodynamic variablesnot associated with eating were assessed bycomparing estimates from postabsorptivedeterminations-that is at baseline and afterfive and 12 hours (fig 3). Compared withbaseline values, right atrial pressure wasincreased after five hours while, in addition,after 12 hours heart rate, mean pulmonaryartery and pulmonary capillary wedge pres-sures, cardiac index, and rate pressure productwere also increased.
HAEMODYNAMIC FUNCTION IN THE ENALAPRILGROUPSerum concentrations of enalaprilat rose afteronly two hours (20'4 (9'8) ng/ml) (fig 4).
Although the concentration was highest afterfour hours (27-9 (8-2) ng/ml), the differencebetween two and five hours was not statisticallysignificant. After five hours the serum concen-trations fell, reaching 1 1 7 (7 0) ng/ml after 12hours. In the absorptive phase, after two andthree hours, the changes in haemodynamicfunction resembled those in the placebo group.Compared with baseline values the meanarterial pressure, systemic vascular resistance,and rate-pressure product decreased (- 15(6)%, p < 0-0001; -23 (9)%, p < 0 001; and- 12 (13)%, p < 0-01, respectively). Thecardiac index and stroke volume indexincreased (+ 14 (9)%, p < 0 05; and 17 (15)%,p < 0-01, respectively). However, comparedwith placebo, the mean arterial pressuredecreased more (p < 0-01) with enalapril, andafter three hours the stroke volume index wasincreased (p < 005) and the rate-pressureproduct had fallen (p < 0O01). In contrast withthe findings in the placebo group, pulmonarycapillary wedge pressure decreased (- 24(25)%, p < 0-01) and after three hours the heartrate (-6 (7)%, p < 0-05) was slower. Thechanges seen during the absorptive phase weremaintained into the postabsorptive phase (thatis five hours after the start ofthe study). Exceptfor a further decrease in heart rate, no changeswere found between two, three, and five hours.
Overall changes from baseline values duringthe 12 hour study period were computed asareas under the curve (fig 2). Compared withplacebo, enalapril reduced heart rate (p < 0 05),pulmonary capillary wedge pressure (p < 0 05),mean arterial pressure (p < 0-01), and rate-pressure product (p < 0 01).
Figure I Mean (SD)and individual changes(mean at baseline and attwo hours (one hour afterthe first meal)) in theplacebo group. See table 2for abbreviations.
100-
_ 90
I S.80-
4 70-
60-
4.0-
-0-
E 3.0-
.
0 2
50
4~ ~ 40
i~1S 30
20-p<0.01
0 2
2100-
1900-
IE1t600-T 1300-
,R 1700-
tn 700-
_ 14000-.9c, 12000-IEEE 1000-
0-L 6000-
14Lp<0.OOt0 2
p<O-OOl
2Time (h)
400I Ip<0.050 2
28
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.63.1.26 on 1 January 1990. D
ownloaded from

Short term haemodynamic effects of enalapril before and after eating
Enalapril group
Baseline Absorptive phase Postabsorptive phase
Oh 2h 3h 5h
87 (20) 85 (18) 81 (19)* 80 (15)**5 (3) 4 (2) 5 (2) 4 (2)tt
25 (7) 22 (5) 22 (5) 22 (5)t15 (7) 1 1 (4)** 12 (4)* 12 (6)*tt83 (7) 71 (8)***tt 69 (8)***t 70 (6)***tt2-3 (0-4) 2-6 (0-3)* 2-5 (0-3) 2-4 (0-7)
28 (9) 32 (9)** 33 (9)**t 31 (10)*t1416 (288) 1067 (192)*** 1035 (212)*** 1150 (223)**174 (63) 187 (44) 187 (48) 168 (39)
9833 (2077) 8522 (1779)** 7774 (1440)***tt 7687 (978)***tt
DiscussionThis is the first placebo controlled, randomiseddouble blind study showing the short termhaemodynamic effects of an angiotensin-con-verting enzyme inhibitor in heart failure andthe extent to which these effects are affected byeating, absorption, and postabsorption. In agroup of patients with treated moderate heartfailure caused by dilated cardiomyopathy,enalapril reduced left ventricular preload andafterload during both the absorptive and post-absorptive phases and hence throughout the 12hour study period. Heart rate and the leftventricular metabolic cost, estimated as therate-pressure product, decreased.The principal features of central haemody-
namic function during the absorptive phase(one hour after ingestion) were similar incontrols and patients with varying degrees of
heart failure."2"6 Systemic vascular resistancedecreased with or without decreases in meanarterial blood pressure and heart rate while thecardiac index increased. These systemic effectsreflect absorptive splanchnic hyperaemia andare the result of a locally mediated vascularresponse to digested nutrients in the lumen17and their composition.8 19 The hyperaemiaseems to be limited to tissues that are active indigestion and was maximal after 30-90 minuteswhen the local blood flow increased 30-150%."32O2 In healthy individuals splanchnichyperaemia was paralleled by an increase inrenal blood flow, but this haemodynamic re-sponse to food seemed to be specific to protein-rich meals.22 Information on blood flowdistribution to other vascular beds during theabsorptive phase is scarce. Studies in animalssuggest that blood flow to the brain and heart
0 2 4 6 8 10 12
,%0.6-
c 0.4-
c 02-
-0-2
IIII I .I i I .
0 24 68 10 12
O 2 4 6 8 10 12
N
E 4-'j---- ------ O- 2-
i1 -2-
NS
0 2 4 6 8 10 12
6 2 .4 6 8 1 12
-7 - ---
NS
6 2 ..6 8 1 12Time (h)
$E 2000
1000-
I IE 0- I--; -1000
0 -2000
NS 4 -3000-
O 2 4 6 8 10 12Time (h)
4 I
---Ic
pc Ol0
-;c-IIc'0
6 2 .6 8 10 12Time (h)
Figure 2 Absolute changes in haemodynamic measurements compared with baseline (mean (SEM)) after enalapril(a) and placebo ( x ). Arrows indicate meals. p values indicate differences between the two groups in the respectiveareas under the curve calculatedfrom zero. See table 2for abbreviations.
200-100-~
EU 0
c -100--200-
x -300-l -400-
-500-'
29
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.63.1.26 on 1 January 1990. D
ownloaded from

Herrlin, Sylvin, Nyquist, Edhag
*
-_ _E~
E
.4
-2-Sh 12h
L ** 8-
3- - 62--1-~ -2
051 L 2"
.4
0- 0.
-1 -2-5h 12h
**
I
30.
.4
I
Sh 12h
08
0-6
.fi 0*'4
E~0 2E02D-u
5h 12h-0-4
* _..1600E 1200
l 8001400-
in
4,0
a.-I.00-0-
Ir--8004
-1200Sh 12h 5h 12h
Figure 3 Spontaneous haemodynamic changes compared with baseline (mean (SD)) in the placebogroup during postabsorptive phases atfive and12 hours. Significant differencesfrom baseline as tested by analysis of variance are indicated as *p < 005 and **p < 0-01. See table 2forabbreviations.
is unaltered and that to skeletal muscle isunaltered or reduced.2' Although the centralhaemodynamic changes during the absorptivephase are similar in individuals with or withoutvarying degrees of heart failure, the distribu-tion of blood flow to other organs may differwith the cardiac capacity.
Packer et al' and Siemienczuk et al16reported a decrease in pulmonary capillarywedge pressure during the absorptive phase inpatients with heart failure, but we found nochange. This difference might be because ourpatients had a lower filling pressure. Differ-ences in the selection of patients, study design,and spontaneous haemodynamic changes maybe relevant.We did not standardise the amount and
composition of the meals eaten by our patients,who ate as much as they wanted and probablythe same as they normally did.
In the placebo group we saw increases inheart rate, pressures, and cardiac index after 12hours and in the postabsorptive phase. Theseresults are at variance with those reported byPacker et al, who found a gradual decrease inpulmonary capillary wedge pressure during 24hours after right heart catheterisation. 5 Massieet al reported similar results.23 In contrast, wefound increases in right atrial and pulmonarycapillary wedge pressures after 12 hours and inthe postabsorptive state, but we did not stopdiuretics on the day of investigation. Diuresisduring the morning could have added to lowerfilling pressures at baseline. Such differencesin basal haemodynamic conditions underscorethe importance of well defined basal conditionsin order to avoid bias introduced by the designof a clinical trial.Two hours after the oral administration of
Figure 4 Concentrationcurve of serum enalaprilat(mean (SD)).
10 mg of enalapril the serum concentration ofenalaprilat was 20-4 (9-8) ng/ml. After 12 hoursit was 117 (7 0) ng/ml. The serum concentra-tion curve resembled that found in controls6and the time to peak concentration was notdelayed, as has been reported in severe heartfailure.24 Angiotensin-converting enzymeinhibition in the 90% range was reported atonly 10 ng/ml.25 Therefore, angiotensin-converting enzyme inhibition was likely to beeffective from the second to the twelfth hour ofthis study.During the absorptive phase the reduction of
afterload was more pronounced with enalaprilthan with placebo. Though the reduction ofafterload during the absorptive phase in theplacebo group was transient, it was maintainedinto the postabsorptive phase after enalapril. Inaddition, enalapril reduced heart rate andpreload as expressed by a decreased pulmonarycapillary wedge pressure while no change wasseen in the placebo group. These enalaprilinduced changes increased from recordingsduring the absorptive phase to those of thepostabsorptive phase, in keeping with shortterm pharmacodynamic studies on heart failurein which maximal haemodynamic effects,including heart rate and afterload reduction,were seen 4-8 hours after administration of asingle oral dose.6 So we would not expect themaximal afterload reduction in the enalaprilgroup to occur as early as two and three hoursafter administration. Indices measured aftertwo and three hours, however, resembled thosemeasured five hours after administration. Thisindicates that after two and three hours, duringthe absorptive phase, the total reduction ofafterload is a summation of enalapril-inducedand meal-induced vasodilatation.The patients were given diuretics on the day
of investigation and this may have potentiatedthe haemodynamic changes produced byenalapril owing to complex interactionsbetween diuretics and converting enzymeinhibitors.26 Notwithstanding this fact, theaim of the study was to describe the shortterm haemodynamic effects of enalapril in anexperimental situation that resembled, as far aspossible, the daily routine of the patient at rest.In addition to meals, this routine also includes acontinuation of long term medication.
In short term studies of congestive heartfailure, inhibition of angiotensin-convertingenzyme activity reduced systemic arterial pres-sure and systemic peripheral resistance and
161L4-
- 12E 10-a 8Z 6-
4 2-0
30
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.63.1.26 on 1 January 1990. D
ownloaded from

Short term haemodynamic effects of enalapril before and after eating
increased the cardiac index. In most vascularbeds (limbs, 27-29 brain,30 liver,29 and coron-aries27 31) tissue flow is maintained throughhomoeostatic vasodilatation. Information on
splanchnic blood flow was ambiguous. Theincrease in the cardiac index was directedmainly to the kidneys where the regional bloodflow was increased.2729 During the absorptivephase splanchnic vasodilatation induced byenalapril was supplemented by physiologicalsplanchnic vasodilatation, which was probablycaused by regionally active vasodilating agents.
CONCLUSIONS(a) The principal haemodynamic effects ofeating and absorption seemed to be similar incontrols and patients with varying degrees ofheart failure. After a meal there was a transientreduction of afterload and an increase incardiac index. (b) When meals were beingeaten regularly angiotensin-converting enzymeinhibition by enalapril in patients withmoderate heart failure caused by dilatedcardiomyopathy produced signs of a balancedreduction in preload and afterload with a
decreased rate-pressure product. The afterloadreduction was additional to that induced bymeals. (c) To avoid bias in clinical trials thestudy design should be double blind with wellcontrolled basal conditions.
This study was supported by funds from the KarolinskaInstitute and the Swedish Heart and Lung Foundation.
1 Grollman A. Physiological variations in the cardiac output ofman. III. The effect ofthe ingestion offood on the cardiacoutput, pulse rate, blood pressure and oxygen consump-tion ofman. Am JPhysiol 1929;89:366-70.
2 Burns GP, Schenck WG. Effect of digestion and exercise onintestinal blood flow and cardiac output. Arch Surg1969;98:790-4.
3 Norryd C, Denker H, Lunderquist A, Olin T, Tylen U.Superior mesenteric blood flow during digestion in man.Acta Chir Scand 1975;141:197-202.
4 Francis GS. Neuroendocrine manifestations of congestiveheart failure. Am J Cardiol 1988;62:9A-13A.
5 Romankiewicz JA, Brogden RN, Heel RC, Speight TM,Avery GS. Captopril: an update review of its pharma-cological properties and therapeutic efficacy in congestiveheart failure. Drugs 1983;25:6-40.
6 Todd PA, Heel RC. Enalapril. A review of its pharma-codynamic and pharmacokinetic properties andtherapeutic use in hypertension and congestive heartfailure. Drugs 1986;31:198-248.
7 Swanson BN, Vlasses PH, Ferguson RK, et al. Influence offood on the bioavailability of enalapril. J Pharm Sci1984;73:1655-7.
8 Patterson JA, Naughton J, Pietras RJ, Gunnar RM. Tread-mill exercise in assessment of the functional capacity ofpatients with cardiac disease. Am J Cardiol 1972;30:757-62.
9 Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommenda-
tions regarding quantitation in m-mode echocardio-graphy: results of a survey of echocardiographicmeasurements. Circulation 1978;58:1072-83.
10 Jonsell S. A method for the determination of the heart sizeby teleroentgenography (a heart volume index). ActaRadwilogica 1939;20:325-40.
11 Hichens M, Hand EL, Mulcahy WS. Radioimmunoassayfor angiotensin converting enzyme inhibitors [Abstract].Ligand Quarterly 1981;4:43.
12 Fagan TC, Sawyer PR, Gourley LA, Lee JT, Gaffney TE.Postprandial alterations in hemodynamics and bloodpressure in normal subjects. Am J Cardiol 1986;58:636-41.
13 Jarvis RC, Green JA, Nara AR, Pospisil R, Kasmer RJ.Effects of food ingestion on hemodynamics in chroniccongestive heart failure. Crit Care Med 1988;16:491-4.
14 Cornyn JW, Massie BM, Unverferth DV, Leier CV.Hemodynamic changes after meals and placebo treatmentin chronic congestive heart failure. Am J Cardiol 1986;57:238-41.
15 Packer M, Medina N, Yushak M. Hemodynamic changesmimicking a vasodilator drug response in the absence ofdrug therapy after right heart catheterization in patientswith chronic heart failure. Circulation 1985;71:761-6.
16 Siemienczuk D, Greenberg B, Broudy DR. Effects of eatingon cardiac performance in congestive heart failure. Chest1986;90:193-7.
17 Gallavan RH, Chou CC. Possible mechanisms for theinitiation and maintenance of postprandial intestinalhyperemia. Am J Physiol 1985;249:G301-8.
18 Brandt JL, Castleman L, Ruskin HD, Greenwald JJ, KellyJ. The effect of oral protein and glucose feeding onsplanchnic blood flow and oxygen utilization in normaland cirrhotic subjects. J Clin Invest 1955;34:1017-25.
19 Siregar H, Chou CC. Relative contribution of fat, protein,carbohydrate and ethanol to intestinal hyperemia. Am JPhysiol 1982;242:G27-31.
20 Gallavan RH, Chou CC, Kvietys PR, Sit SP. Regional bloodflow during digestion in the conscious dog. Am J Physiol1980;238:H220-5.
21 Chou CC. Splanchnic and overall cardiovascular hemo-dynamics during eating and digestion. Fed Proc1983;42:1658-61.
22 Premen AJ. Protein-mediated elevations in renal hemo-dynamics: existence of a hepato-renal axis? Med Hypoth-eses 1986;19:295-309.
23 Massie BM, Leier CV, Unverferth DV. Hemodynamicchanges following placebo administration: implicationsfor drug studies [Abstract]. Circulation 1984;70(supplII):1 12.
24 Dickstein K, Till AE, Aarsland T, et al. The pharma-cokinetics of enalapril in hospitalized patients with con-gestive heart failure. Br J ClinPharmacol 1987;23:403-10.
25 Biollaz J, Schelling JL, Jacot des Combes B, Brunner DB,Desponds G, Brunner HR. Enalapril maleate and a lysineanalogue (MK-521) in normal volunteers; relationshipbetween plasma drug levels and the renin angiotensinsystem. Br J Clin Pharmacol 1982;14:363-8.
26 Cleland JG, Gillen G, Dargie HJ. The effects of frusemideand angiotensin-converting enzyme inhibitors and theircombination on cardiac and renal haemodynamics in heartfailure. Eur Heart J 1988;9:132-41.
27 Faxon DP, Creager MA, Halperin JL, Bernard DB, RyanTJ. Redistribution of regional blood flow followingangiotensin-converting enzyme inhibition. Comparisonof normal subjects and patients with heart failure. Am JMed 1984;76:104s-10.
28 Levine TB, Olivari MT, Cohn JN. Hemodynamic andregional blood flow response to captopril in congestiveheart failure. Am JMed 1984;76:38-42.
29 Levine TB, Olivari MT, Garberg V, Sharkey SW, Cohn JN.Hemodynamic and clinical response to enalapril, a long-acting converting-enzyme inhibitor, in patients withcongestive heart failure. Circulation 1984;69:548-53.
30 PaulsonOB, Jarden JO, Vorstrup S, Holm S, Godtfredsen J.Effect of captopril on the cerebral circulation in chronicheart failure. Eur J Clin Invest 1986;16:124-32.
31 De Marco T, Daly PA, Liu M, Kayser S, Parmley WW,Chatterjee K. Enalaprilat, a new parenteral angiotensin-converting enzyme inhibitor: rapid changes in systemicand coronary hemodynamics and humoral profile inchronic heart failure. JAm Coll Cardiol 1987;9:1131-8.
31
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.63.1.26 on 1 January 1990. D
ownloaded from


















