BURN TO CD NEW (1)
52
1 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND… OUR LADY OF FATIMA COLLEGE OF NURSING Antecedents and Consequences of Nicotine Dependence and Readiness to Quit among Student Smokers of the Allied Health Programs in the Philippines Jade P. Mojica 1,2,3 , John Gerald A. Calisay 1,2,3 , Jason M. Franco 1,2,3 , Owoh Joshua Amobi 1,2,3 Vikhuli Hansen 1,2,3 , Jenica A. Rivero 1,2,3,4 1 College of Nursing 2 Research Development and Innovation Center 3 Our Lady of Fatima University 4 Research Adviser October 2015
-
Upload
joshua-owoh -
Category
Documents
-
view
56 -
download
0
Transcript of BURN TO CD NEW (1)

1 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Antecedents and Consequences of Nicotine Dependence and Readiness to Quit
among Student Smokers of the Allied Health Programs in the Philippines
Jade P. Mojica1,2,3, John Gerald A. Calisay1,2,3, Jason M. Franco1,2,3, Owoh Joshua
Amobi1,2,3 Vikhuli Hansen1,2,3, Jenica A. Rivero1,2,3,4
1College of Nursing
2Research Development and Innovation Center
3Our Lady of Fatima University
4Research Adviser
October 2015

2 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Endorsement
This research entitled “Antecedents and Consequences of Nicotine Dependence
and Readiness to Quit among Student Smokers of the Allied Health Programs in the
Philippines” prepared by Jade P. Mojica et al. of section 4Y1-1, in partial fulfillment of the
requirements for the degree Bachelors of Science in Nursing has been examined and now
recommended for Oral Examination.
This is to certify that Jade P. Mojica et al. are ready for the Oral Examination.
Jenica A. Rivero
Adviser
This is to certify that the thesis: “Antecedents and Consequences of Nicotine
Dependence and Readiness to Quit among Student Smokers of the Allied Health Programs
in the Philippines” prepared and submitted by Jade P. Mojica et al. of section 4Y1-1, is
recommended for Oral Examination.
Christian V. Del Rosalio
Chair
Caesardo A. Nicolas RN, MAN Shawn B. Cajayan RN, MAN
Member Member
Lurceli L. Santos MAN, RN, RM
Dean, Our Lady of Fatima University

3 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Certificate of Originality
We hereby declare that this thesis is our own work and that, to the best of our knowledge
and belief, it contains no material previously published or written by another person nor
material to which to a substantial extent has been accepted for award of any other degree
or diploma of a university or other institute of higher learning, except where due
acknowledgement is made in the text.
We also declare that the intellectual content of this thesis is the product of our work, even
though we may have received assistance from others on style, presentation and language
expression.
Jade P. Mojica
Principle Investigator
Members:
John Gerald A. Calisay
Jason M. Franco
Owoh Joshua Amobi
Vikhuli Hansen
Jenica A. Rivero RN, MAN
Adviser
Date

4 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Table of content
Endorsement 2
Certificate of Originality 3
List of Tables 6
List of Figures 7
List of Appendices 8
Abstract 9
1.0 Introduction 10
2.0 Literature Review 11
2.1 Theoretical Framework 11
2.2 Variable Discussion 12
2.2.6 Problem Statement and Hypothesis 15
2.3 Research Simulacrum 17
3.0 Research Methods 17
3.1 Research Design 17
3.2 Research Locale 18
3.3 Population and Sampling 18
3.4 Research Ethics 18
3.5 Research Instrument 19
3.6 Data Collection 20
3.7 Data Analysis 21
4.0 Results 21
4.1 Demographic Profile of the Respondents 21
4.2 Nicotine Dependency, Intention to Quit, and Health Related
Quality of Life
23
4.3 Demographic Difference on Nicotine Dependency 24
4.4 Demographic Differences on Readiness to Quit 25
4.5 Impact of Nicotine Dependency to Health Related Quality of life 26
4.6 Impact of Readiness to Quit on Health Related Quality of Life 27
5.0 Discussion 28
6.0 Conclusion 33
5 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
7.0 Recommendation 34
Reference 35
Appendices 39
Acknowledgement 52

6 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
List of Tables
Table 1 Demographic Profile of the Respondents 22
Table 2 Nicotine Dependency, Readiness to Quit, and Health Related Quality
of Life
23
Table 3 Demographic Differences on Nicotine Dependency 24
Table 4 Demographic Differences on Readiness to Quit 25
Table 5 Impact of Nicotine Dependency on Health Related Quality of Life 27
Table 6 Impact of Readiness to Quit on Health Related Quality of Life 27

7 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
List of Figures
Figure 1 Research Simulacrum 17
8 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
List of Appendices
Appendix A: Ethics Approval 39
Appendix B: Permission to Use Questionnaire 40
Appendix C: Consent 41
Appendix D: Questionnaire 42
Appendix E: Fagerstrom Test of Nicotine Dependency 43
Appendix F: Quit Ladder 44
Appendix G: EQ-5D-5L 45
Appendix H: Statistics Certificate 47
Appendix I: Budget 48
Appendix J: Timeline 49
Appendix K: About the Researchers 50

9 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Abstract
Smoking is associated with most of the health related condition worldwide, and which this
research is done to elicit the level of nicotine dependency, readiness to quit, and the
perception of smoking related to age, health related quality of life, social acceptance, socio
economic, gender and religion. Consequences of Nicotine Dependence and Readiness to
Quit was conducted in a tertiary institute with a corresponded of 262 in Valenzuela city,
Philippines. We conducted a quantitative and descriptive correlational study on the student
smokers in the Allied Health Programs in the Philippines. It helps show a relation between
4 fields of study; demographic, nicotine dependency, readiness to quit, and health related
quality of life. The study is based on a target population of 262 college student smokers
who are enrolled for the school year 2015-2016 in a Higher Educational Institution in the
Philippines. Pearson’s correlation shows that there’s a weak negative association between
the readiness to quit smoking and level of pain/discomfort (r=-0.146, p-value=0.018; and
between readiness to quit smoking and anxiety or depression (r=-0.247, p-value<0.001)
which are both statistically significant. However, weak negative association but not
statistically significant were observed between readiness to quit smoking and mobility (r=-
0.059, p-value=0.338); self-care (r=-0.059, p-value=0.344) and usual activities (r=-0.099,
p-value=0.11). Pearson’s correlation shows that there is significant association between the
nicotine dependency and health related quality of life namely mobility, self-care and
pain/discomfort. There is a weak inverse relationship between nicotine dependency and
mobility (r=0.141, p-value=0.022). Nicotine dependency and self-care(r=0.152, p-
value=0.014) and nicotine dependency and pain/discomfort (r=0.145, p-value=0.019).
Nevertheless, result shows that there is weak positive association between nicotine
dependency and usual activities(r=0.05, p-value=0.423) and nicotine dependency and
anxiety/discomfort (r=0.094, p-value=0.128) which both not statistically significant.
Keywords: Nicotine Dependence, Age, Religion, Socio-economic, Gender, Cigarette
Smoking, Intention to quit smoking, college student, cigarette, nicotine.

10 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
1.0 Introduction
The increase in tobacco smoking through the use of cigarette remain one of the
most significant causes of preventable diseases worldwide. Health related quality of life is
decreased in people who are more nicotine dependent compared to others who are less
nicotine dependent, despite the understanding of the negative health effect associated with
smoking, some people still continue to smoke as long as the cigarette meet there pleasure
need and ignoring the negative effect of respiratory problem, metabolic problem, malignant
problem and other ill health associated with smoking. The negative effect of smoking does
not begins to manifest on one’s health immediately, rather it gradually destroys the normal
cell of vital organs in the human body resulting to latter life organ impairment and
sometime manifest early in middle life.
Smoker’s perception and lifestyle is an aspect to systematically evaluate the habit
of smokers, and their readiness to quit smoking. Some people who smoke more cigarette
per day find it more difficult to quit compare to those who smoke occasionally because the
more dependent a person is to nicotine the more he or she crave to smoke compared to
those who smoke occasionally. Some occasional smokers have not yet reach the peak of
craving, so there will stand a better chance to quit compare to a chronic smoker who is
already dependent to it.
Most developing countries have started to combat the rate at which their citizen
smoke through the use of media awareness of the associated negative health and evaluating
their readiness to quit smoking. Readiness to quit could be associated with the perceived
negative health of the individual or due to medical diagnosis as a motivation to quit
smoking. Religion also could be motivation to cigarette cessation because of the
steadfastness in religious practice and activity which one is associated with in daily life.
the more close one is to his religious practice will gradually reduce the consumption of
cigarette per day and gradually stop smoking even when religion do not generally prohibit
the use of tobacco else 80 to 90 % of the world population will be free from most of the
diseases caused by the use of tobacco product through the smoking of cigarette.
In gender and social acceptance related to cigarette smoking, Gender is commonly
seen with as stereotyping attitude which male are accepted to smoke while female smokers

11 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
are seen as inappropriate. Socio acceptance of female smokers is marred with wildness and
unsuitable to some people despite that female smokers are known to be occasional smokers
compared to male smokers who are habitual smokers. Female smokers commonly smoke
for the fun of it or trying to create a gesture of belongingness in an environment where
mostly everyone smokes so as not to be left out. Nevertheless, female smokers who smoke
as the same quantity as male are twice dependent to nicotine than men, and will find it
more difficult to quit.
2.0 Literature Review
2.1 Theoretical Framework
Two theories was used to describe the study framework. These theories are Dorothy
Johnson’s Behavioral Systems Theory and Albert Bandura’s Self-Efficacy theory. The
Behavioral Systems theory allows the giving of efficient and effective behavioral
functioning in the patient to prevent illness. While the Self-Efficacy theory explains the
change of human behavior, both theories are patient centered and based on behavior.
Dorothy Johnson’s Behavioral System Theory. This theory gives more importance
on the connection of the patient to the environment than the patient to environment alone.
“The patient is identified as a behavioral system composed of seven subsystems:
attachment, dependency, ingestion, eliminative, sexual, aggression, (Gonzalo. A). the
subsystems are interrelated, meaning that if one is altered then the other subsystems will
also be altered. According to Johnson “each of the behavioral subsystems are influenced
by events in the environment” (Octaviano & Balita). Johnson focuses on two areas, “first,
nursing care should lessen stimuli that are stressors, and second, nursing care should offer
support of the client’s normal defenses and adaptive processes” (Octaviano & Balita).
Albert Bandura’s Self-Efficacy Theory. This theory focuses more on changing
behavior of a person’s perception of their ability to reach a goal. “Self-efficacy beliefs
12 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
provide the foundation for human motivation, well-being, and personal accomplishment”
(Pajares, F.). Self-efficacy explains the change of human behavior.
These both support our study because they are both patient centered and based on
the behavior. The study is about factors relating to smoking cessation, whereas quitting is
a decision made by the individual. In Bandura’s theory, he studied the way behaviors
change, such as the research question used, what influences college students to quit?
Johnson’s Behavioral Theory states that if one subsystem is altered, the others will be
altered. This research is not trying to elicit the reason why college student smoke but rather
to understand if there are some reason or effort put in place to quit smoking, also, to
ascertain the level of nicotine dependency among the participant of the research.
Variable Discussion
2.2 Literature Review
The research conducted used a descriptive correlational nonexperimental method.
The variables that were examined include age, religion, socioeconomic status, heavy
smoking, and health issues relating to quitting smoking. We believed that these variables
would important in influencing smokers to either quit or continue smoking.
2.2.1 Age
The relationship of Age to nicotine dependency is a characteristics that cannot be
undermine because age stand as the quantitative aspect of human development, and at some
time in life where curiosity is heightened one will tend to explore the world he lives in, and
the good and bad that goes with it. Hence cigarette consumption will come into exploration.
The increase in cigarette dependency is commonly seen in teenagers of 19 years and above
when anxiety and exploration play more role to cigarette consumption to sometime in
middle adulthood of 25 to 27 years old when decision making has started to set in. These
put some young adult in pressure and depression to relieve themselves with a puff of a stick
or two to more in the subsequent days.
13 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Young adults are majority of college students in most country in the world today, and the
increased in cigarette consumption are commonly seen among this set of individuals.
Smoking rates are declining in the United States, except for young adults (age 18 to 24)
(Ling 2004.). In a study, it was found that there is an increase in smoking prevalence from
adolescence to young adulthood and then a decline after the mid 20's (Paavola 2000.). This
study was conducted on the same group when they were 14 years, 20 years, and 27 years
to compare the difference in smoking. They were able to find that the desire to quit does
not differ much among different age groups. In all age groups one tenth of smokers want
to continue smoking and half of smokers would like to quit (Paavola 2000.) In a study
about tobacco industry recapturing young adults concluded that in 1986 many of the
smokers most likely to quit, such as intermittent smokers or brand switchers, were young
adults (Ling 2004.) Also that, tobacco companies attempted to recapture younger quitters
by developing products that appeared to be less addictive or more socially acceptable. This
suggests that smoking menthol cigarettes are popular among young adults, making it more
difficult to successfully quit (Fagan 2007.). With a large increase in smoking among the
young adults this also be the hypothesis for our research.
2.2.2 Religion
The Relationship between Religious Activities and Cigarette Smoking in Older
Adults has concluded that religiously active people were less likely to smoke cigarettes. If
the religious person does smoke they smoke fewer than those less religiously active. Those
who never attended religious activities had a higher percentage of smoking and a higher
amount of pack per year. This is compared to the people who attend religious activities
more than 1 times a week who have a low percentage of smokers. For those who do smoke
they have a lower amount of packs smoked per year.
2.2.3 Socioeconomics
14 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Socioeconomics is a factor that hasn’t adequately been assessed in most studies
(Siahpush 2004.). But even then, it can be a predictor of smoking cessation when actually
being assessed. There is an increasing prevalence of smoking with a decreasing
socioeconomic status (Gilman 2003.). In a study it was observed that socioeconomically
disadvantaged smokers find quitting more difficult, possible because lack of support for
quit attempts, greater addiction to tobacco, less motivation to quit and less compliance to
treatment (Hiscock 2010.). This lack of support has been identified as a reason for low quit
rates among disadvantaged smokers (Hiscock 2010.). These disadvantaged smokers are
most commonly in developing countries making it difficult to quit among these countries.
2.2.4 Nicotine Dependency
Nicotine addiction is believed to be a major impediment for many people in quitting
smoking, but measures of nicotine dependence such as the heaviness of smoking index
have mixed success in predicting cessation. The level of nicotine dependence is important
in assessing the effectiveness of smoking prevention and control programs. There are
several scales available for measuring addiction level such as the Fagerstrom tolerance of
nicotine dependence, the cigarette dependence scale, and the nicotine dependence scale. A
study in Canada found that heaviness of smoking index is associated with reported changes
in smoking. The result of this study says smokers who had low heaviness of smoking index
scores quit earlier than those with higher score but the long term cessation rates were
similar (Kozlowski 1994) more like quitting smoking at follow-up. But the data did not
indicate a constant relationship between increasing heaviness of smoking index scores and
a decreasing probability of cessation at follow-up. In this study people with low levels of
nicotine dependence as measured by heaviness of smoking index consistently to report
quitting, highly nicotine dependent smokers, particularly older and wealthier also reported
a substantial likelihood of cessation. Other research found that for the majority of smokers,
dependence is only one factor in making, and succeeding to quit attempt with cognitive,
affective, and environment influences being other important factors (McDonald 2003;
Kenford t al., 2002).

15 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
The heaviness of smoking can be considered the degree to which an individual is
attached to cigarette smoking, this conception of dependence only partially related to actual
chances of quitting. The affective model of nicotine dependence is related to individual
capacity to experience negative affect and an individual’s expectations that quitting
nicotine would improve this effect, is a better predictor of smoking cessation.
There is increasing recognition that the two measures in the heaviness of Smoking
Index, time to first cigarette of the day and daily consumption (cigarettes per day), are
strongly predictors of quitting behavior. Study found out that both time to first cigarette of
the day and cigarettes per day are fairly reliable and important predictors of quitting
outcomes. The study demonstrate that the categorical scoring method adequate for many
purposes. One of the advantage in relative meaning of consumption changes as a result of
reduced opportunities to smoke (e.g., result of smoke-free policy; Husten, 2009)
2.2.5 Health Related Quality of Life
Several decades of research have established the causal relationship between
tobacco smoking and a variety of adverse health effects. The health benefits of smoking
cessation include a reduction of the risk of lung and other cancers, heart attack, stroke, and
chronic lung disease. The dynamics of smoking cessation are complicated, and the struggle
to quit permanently can be prolonged, involving several attempts (and relapses) before
permanent cessation is achieved. As well, it may take years of abstinence for disease risk
to be similar to that of people who never smoked. Therefore, research aimed at studying
the relationship between smoking status and health outcomes by using the EQ-5D-5L a
generic preference-based measure that reflects the subjective values assigned to specific
health-related outcomes was to assess health-related quality of life and outcomes.
2.2.6 Problem statement and hypothesis
Cigarettes smoking is one of the most recognized cause associated with different
kind of health related problem around the world ranging from metabolic diseases,
16 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
respiratory and malignant diseases. The problem statement of the research is identifying
whether if health related quality of life of individual smokers has a relationship to why the
correspondents decide to quit smoking cigarette, this research is made to believe that
anyone who is suffering from a health condition whereby smoking of cigarette will
exacerbate the condition of the individual might want to consider quitting smoking.
Religion in the other hand might have a significant relationship to why anyone would
consider to quit smoking even though religion does not entirely prohibit the use of cigarette
but still value human existence and as such will encourage cessation. Social acceptance is
another aspect to the relationship to why smoking cessation is encourage to most people,
if in a group of friends and only one person smokes, the influence of the other friends who
perceive cigarette as a bad habit or practice that might give the smoking friend the
perception that the other friends are not always comfortable when he is around them and
might be the significant relationship to smoking cessation. In some research, smoking
cessation related to nicotine dependence show some significant relationship to quitting in
accordance to the heaviness of cigarette smoking, and so as in social acceptance. Socio
acceptance related to smoking is the stereotyping associated with practice or behavior that
is unacceptable to others and as such will deem it inappropriate as perceived by the people
who feel affected or in close contact with primary perpetrator of the perceived
inappropriate character.
Hypothesis
1) How does demographic differences relate to nicotine dependence and readiness to quit?
2) What is the impact of nicotine dependency to health related quality of life?
3) What is the impact of readiness to quit to health related quality of life?
i. We believe that, age, sex, religion and Social Economics is another significance
that could enhance the readiness to quit smoking cigarette due to low financial
status or not having enough to spare for a stick of cigarette or more compare to
quantity per day and how low socioeconomic increase the rate of smoking and
dependence to nicotine.

17 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
ii. Nicotine dependency to health related quality of life is another significance that we
believe will have a relationship to readiness to quit smoking due to the health
related perception of chronic smoking.
iii. The researchers believe that there will be significance with readiness to quit
smoking and Heath Related Quality of Life among the smoking correspondent.
2.3 Research Simulacrum
Figure 1. Research Simulacrum
3.0 Research Methodology
3.1 Research design
The design used for the research was a quantitative approach, and descriptive
correlation. This design uses the dependent variables and independent variables to find a
relationship of the data. This was done by self-evaluation through the use of questionnaires
for the correspondent to provide information regarding steps taking to quit smoking and

18 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
the motivating factors regarding their decision, or they don’t have the intention to quit, of
which shows how dependent they are to nicotine, also, the method used will help show the
quantity of cigarette consumption per day, and the onset of smoking from getting up from
bed in the morning.
3.2 Research locale
The research was carried out in a tertiary institution and one of the many
universities with the most accredited courses in the Philippines. It is an ISO certify school
and one of the few university granted the right to offer medical courses, and with a level
four (LEVEL 4 PACUCOA) accreditation in nursing in the Philippines. The institution is
located in Manila. It comprises of five section of the campus that possess the different
colleges, and the main campus comprises the allied health programs where the data was
collected.
3.3 Population and sampling
In order for the respondent to participate he/she must have the following
characteristics; be of age meaning 19 years or older, currently enrolled in an HEI in NCR
as a student of the Allied Health Program, and must be of sound mind without any
neurologic disorders. This is to prevent errors and incorrect input into the research data.
Our sampling technique used was a snowball sampling to prevent violation of individual
confidentiality. After the respondent participates in the question we asked them if they may
refer us to other smokers that also fit the characteristics of our target population.
3.4 Research Ethics
This research paper went through review with the ethics committee of the
University and was approved before the research was conducted. The research also
obtained an informed consent from every participant to ensure their knowledge of the
research and to help clarify their understanding that their participation is voluntary with no
19 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
benefits or losses. Confidentiality and anonymity is ensured that no harm will be brought
upon the participant, and if the participant feels the need or desired to stop even after they
might have attempted the question on the questionnaire, they may do so without any
penalties.
3.5 Research instruments
Demographics. The questionnaire is divided into 4 sets of questions; 1demographic
profile, 2currently smoking, 3quitting smoking, and 4have already quit. The demographic
profile consists of five significance; age, gender, religion, socio economic status, and
education attainment. Currently smoking asks how long the participant has been smoking,
how many sticks they smoke per day, and how soon after they wake they smoke. The
quitting smoking set asks the participants if they want to quit, how many times they had
tried, how long they have abstained from smoking, and what they think is the one most
important reason they would quit smoking. The last section of the questionnaire is for those
participants who have already quit smoking. It asks how long they have quit smoking and
if they are tempted to start again. The purpose of this questionnaire is to explore their
history in smoking and desire to quit.
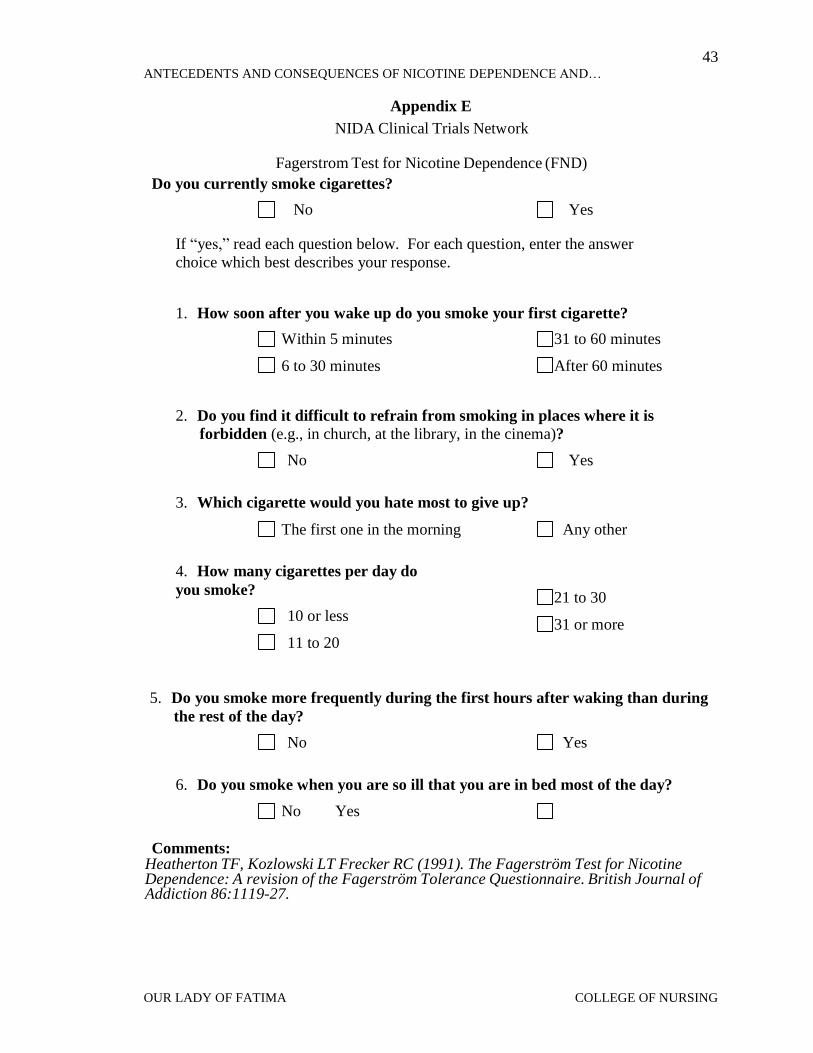
Fagerstrom Test for Nicotine Dependence (FND). The Fagerstrom Test is an
instrument used to measure the participants’ dependency to nicotine by asking six different
questions. These questions includes how soon is it to the smoker’s first cigarette, if they
have difficulty to refrain from smoking, which they would not like to give up, how many
sticks per day, if they smoke more frequently in the first hour of the day or any other time,
and if they smoke even if they are ill. Each answer choice has a score that would be added
to find the outcome of the test which can be low, low to moderate, moderate, or high. This
test has been used in other researches to measure smoker’s dependency for after they quit.
It helps to indicate the appropriate treatment for withdrawal symptoms in certain
researches. If the participants score between 1-2 they have a low dependency to nicotine.
A score of 3-4 indicated low to moderate, 5-7 indicates moderate level, and 8 or high is
considered high dependency.

20 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
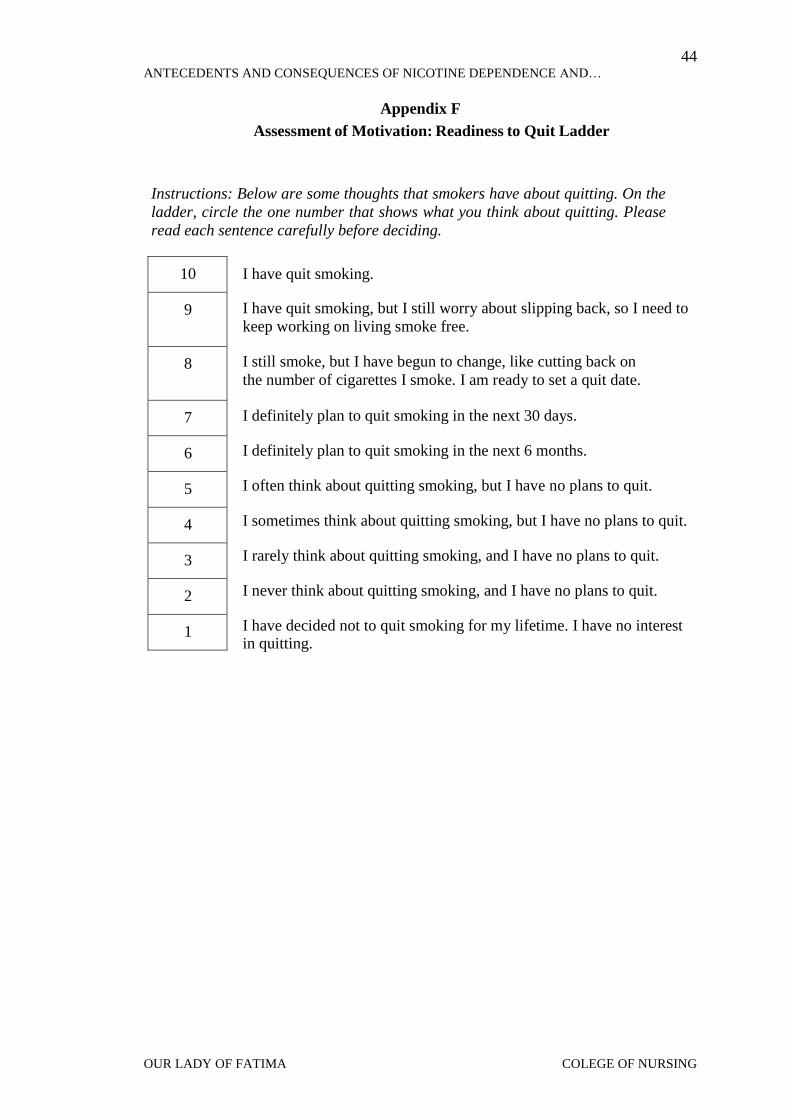
Quit Ladder. The Readiness to Quit Ladder is a 1-10 scale that provides statements
or thoughts that the smoker may have to indicate their readiness to quit tobacco smoking.
This tool was created to help know when the appropriate time to start treatment. If the
smoker chooses 7, “I definitely plan to quit smoking in the next 30days,” treatment would
be best to start. The individual’s readiness may change over time meaning those who
indicate they do not want to quit may later want to quit and those who say they are ready
may later not want to quit anyone. In other research, treatment are applied to such
individual to help them reframe from smoking, but this research does not subject the
participant to any treatment to stop smoking, rather, it evaluate the participant level of
dependent to cigarette smoking and the factors which may cause the individuals readiness
to quit
EQ-5D-5L. The EQ-5D-5L is a European questionnaire that has 5 dimensions;
mobility, self-care, usual activities, pain/ discomfort, and anxiety/ depression. Within these
dimensions there are 5 different statements or levels which includes no, slight, moderate,
severe, and unable or extreme. This instrument is used for the individual to rate his health
on the current day. The second part of the tool is a scale of 0-100 with 100 being the best
health imaginable and 0 meaning the worst health imaginable. This perception of their
health is also for the current day. This questionnaire was used for this study to evaluate the
participants health related quality of life.
3.6 Data Collection
Before the study was carried out, the researchers went through the University’s
research department for review and ethical approval to prevent any errors in the paper. Data
was collected by explaining the goal of the study to the participants and making sure that
participation is voluntary. Afterword, the questionnaire was given to the participant
together with a consent form to be signed with their name printed as a sign of approval.
Any questions asked by the participants were well explained to prevent error in data
gathering. As soon as they completed all section of the questionnaire, we kindly asked the
21 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
participants if they had anyone they may refer us to that fits the characteristics of our target
goal and so doing, prevent public embarrassment of our participants.
3.7 Data Analysis
For analyzing the data the T-Test and Analysis of Variance (ANOVA) was used to
compare the difference between the variables. T-Test is an analysis that uses 2 groups to
be compared most commonly used when the data findings are considered categories. In
analysis of variance, it uses more than two groups that are numerically scaled. For example,
in our research when we compare the difference of the sexes we use the T-Test, but when
we compare the impact of nicotine dependence to health related quality of life we use the
ANOVA because each score is a numeric value. Pearson correlation was used to compare
the strength and the weakness of the variables, the level of significant was set 0.05 to accept
result less than the level of significance, and any valur above the level of significance was
rejected.
4.0 Results
4.1 Demographic Profile of the Respondents
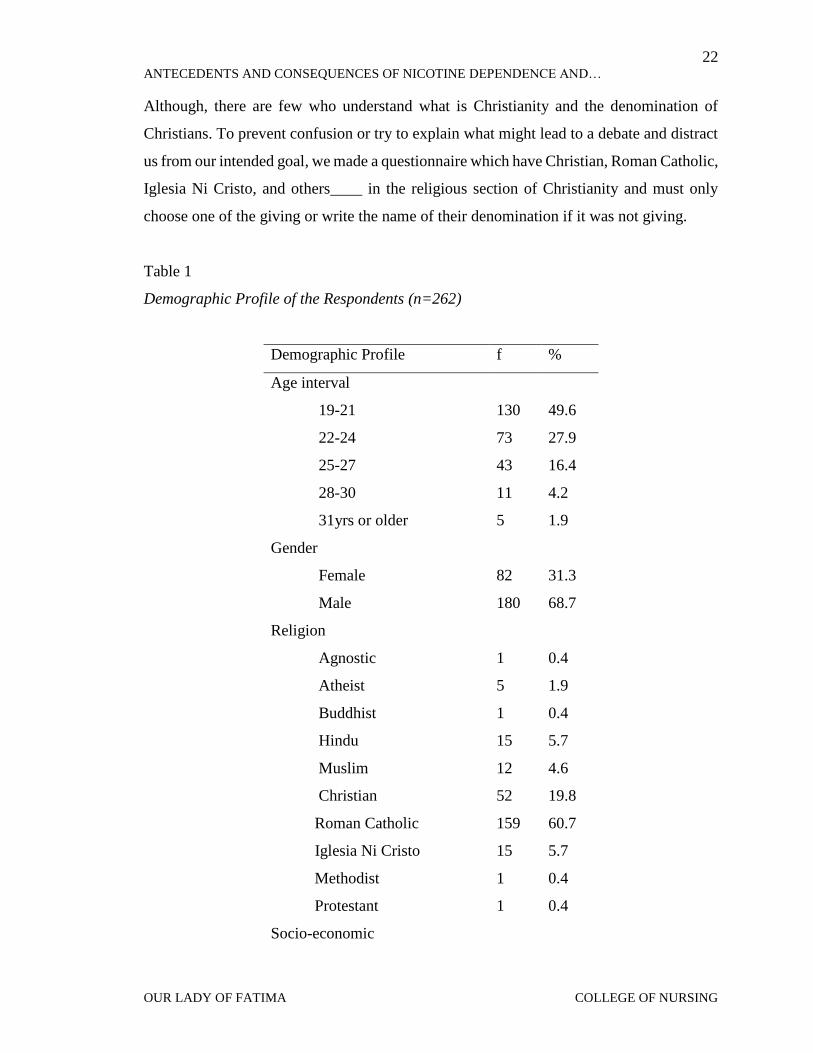
Table 1 presents the demographic profile of the respondents. Majority of the
respondents are 19 to 21 years old, males, middle class, Roman Catholic and in the
undergraduate level.
This might seem strange to some readers but it is the reality that most people do not
understand what is Christianity and the denominated churches under Christian doctrine in
the Philippines. Roman Catholic Church is a denomination under Christianity. In the
Philippines, most people believe that Christian is a religion where the people are born again
and differ from Roman Catholic Church as well as Iglesia Ni Christo Church. So when you
say that you are a Christian most people take you for a born again. Example of a born again
person in the Philippines, you are a member of Victory Church, Redeem Christian Church,
and if you are a Roman Catholic you are not a Christian but just only a Roman Catholic.
22 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Although, there are few who understand what is Christianity and the denomination of
Christians. To prevent confusion or try to explain what might lead to a debate and distract
us from our intended goal, we made a questionnaire which have Christian, Roman Catholic,
Iglesia Ni Cristo, and others____ in the religious section of Christianity and must only
choose one of the giving or write the name of their denomination if it was not giving.
Table 1
Demographic Profile of the Respondents (n=262)
Demographic Profile f %
Age interval
19-21 130 49.6
22-24 73 27.9
25-27 43 16.4
28-30 11 4.2
31yrs or older 5 1.9
Gender
Female 82 31.3
Male 180 68.7
Religion
Agnostic 1 0.4
Atheist 5 1.9
Buddhist 1 0.4
Hindu 15 5.7
Muslim 12 4.6
Christian 52 19.8
Roman Catholic 159 60.7
Iglesia Ni Cristo 15 5.7
Methodist 1 0.4
Protestant 1 0.4
Socio-economic
23 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
high 8 3.1
low 7 2.7
middle 131 50
no response 116 44.3
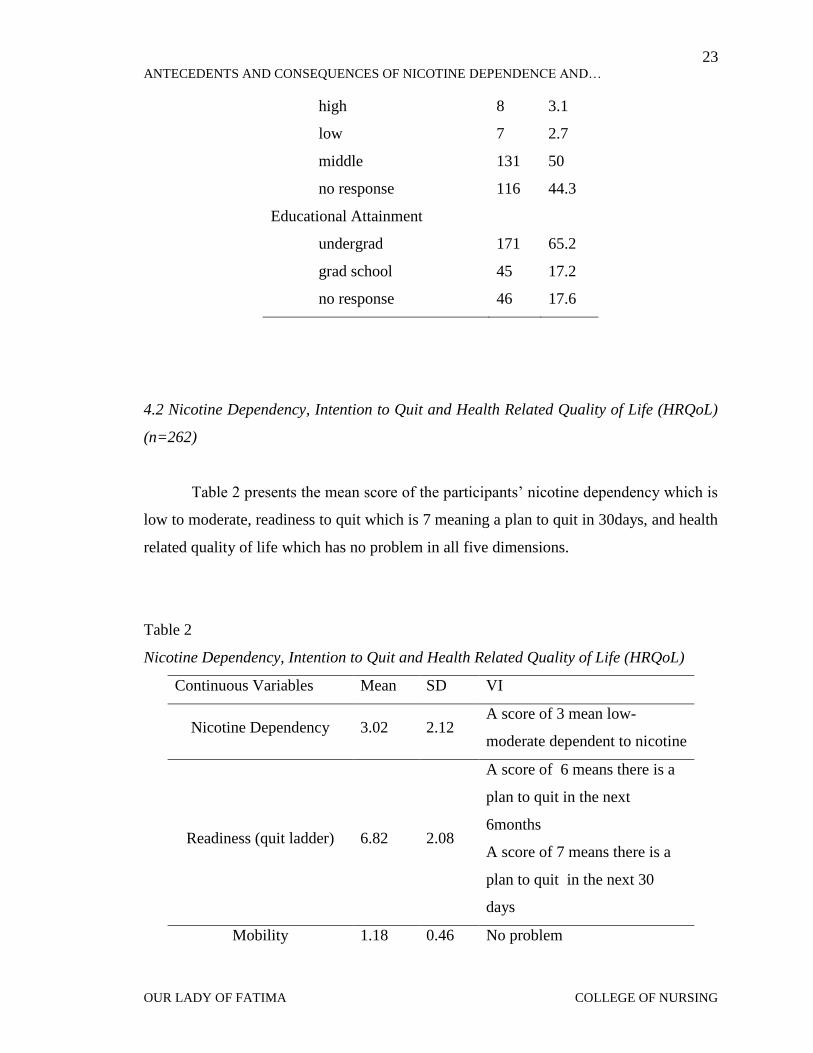
Educational Attainment
undergrad 171 65.2
grad school 45 17.2
no response 46 17.6
4.2 Nicotine Dependency, Intention to Quit and Health Related Quality of Life (HRQoL)
(n=262)
Table 2 presents the mean score of the participants’ nicotine dependency which is
low to moderate, readiness to quit which is 7 meaning a plan to quit in 30days, and health
related quality of life which has no problem in all five dimensions.
Table 2
Nicotine Dependency, Intention to Quit and Health Related Quality of Life (HRQoL)
Continuous Variables Mean SD VI
Nicotine Dependency 3.02 2.12 A score of 3 mean low-
moderate dependent to nicotine
Readiness (quit ladder) 6.82 2.08
A score of 6 means there is a
plan to quit in the next
6months
A score of 7 means there is a
plan to quit in the next 30
days
Mobility 1.18 0.46 No problem

24 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Self-Care 1.16 0.53 No problem
Usual Activities 1.27 0.61 No problem
Pain/ Discomfort 1.31 0.58 No problem
Anxiety/ Depression 1.46 0.82 No problem
Range for HRQoL: 1.0 -1.49 No problem; 1.5-2.49 Slight problem, 2.5-3.49 Moderate
problem, 3.5 – 4.49 Severe problem, 4.5 – 5.0 Extreme Problem
4.3 Demographic Differences on Nicotine Dependency
Table 3 shows that no significant difference exist in the nicotine dependence of the
respondents when grouped according to age, religion, social class, and educational
attainment. However, a significant difference exists when respondents are grouped
according to gender (p=0.048).
Table 3
Demographic Differences on Nicotine Dependency
Demographic vs Nicotine
Dependency mean(SD)
test
statistic p-value interpretation
age interval(n=257)
19-21yrs 2.99(2.06)
F=0.414 0.743 no difference 22-24yrs 2.93(2.06)
25-27yrs 3.21(2.26)
28-30yrs 2.45(2.16)
gender(n=262)
female 3.4(2.21) t=1.989 0.048
with
difference male 2.84(2.06)
religion(n=258)
Roman catholic 3.04(2.05) F=0.35 0.93 no difference
Muslim 3.17(2.29)
25 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Christian 2.81(2.13)
Hinduism 2.87(2.39)
INC 3.33(2.41)
Atheist 3.6(2.70)
socio-economic status(n=146)
low 2.14(1.46)
F=0.498 0.609 no difference middle 2.85(2.06)
high 3.13(1.81)
educational attainment (n=216)
undergrad 3.01(2.15) t=0.948 0.344 no difference
grad school 2.67(2.06)
*significant at 0.05
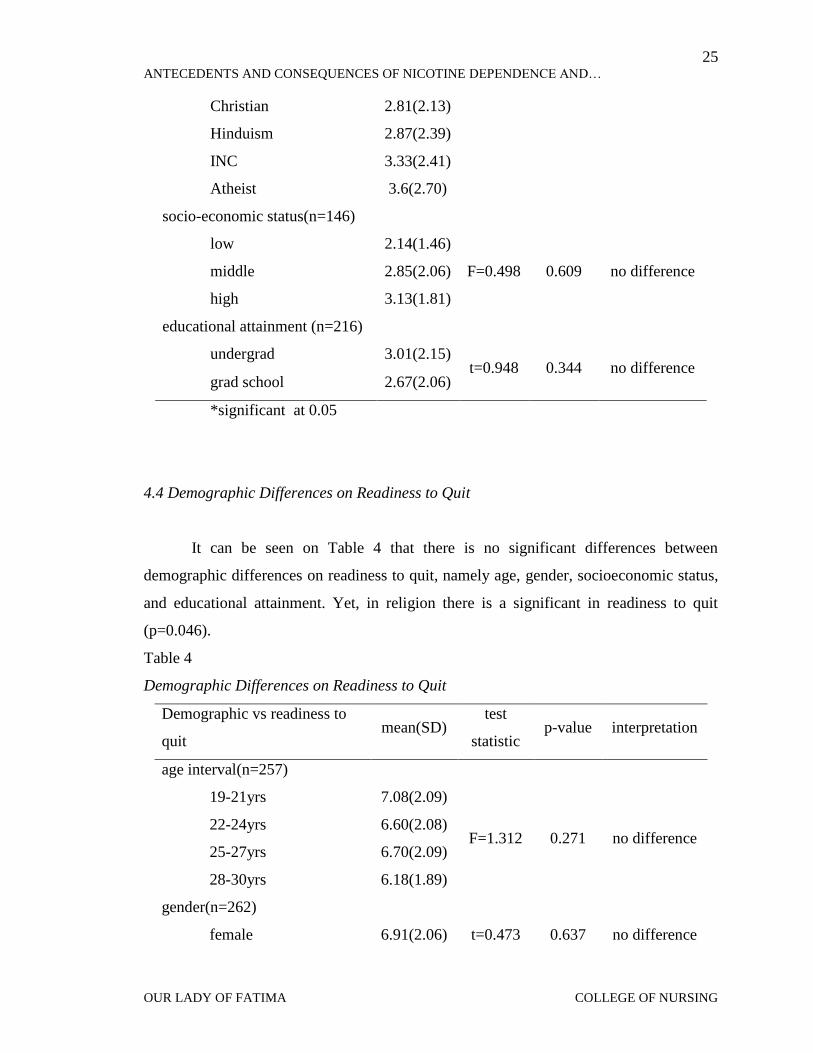
4.4 Demographic Differences on Readiness to Quit
It can be seen on Table 4 that there is no significant differences between
demographic differences on readiness to quit, namely age, gender, socioeconomic status,
and educational attainment. Yet, in religion there is a significant in readiness to quit
(p=0.046).
Table 4
Demographic Differences on Readiness to Quit
Demographic vs readiness to
quit mean(SD)
test
statistic p-value interpretation
age interval(n=257)
19-21yrs 7.08(2.09)
F=1.312 0.271 no difference 22-24yrs 6.60(2.08)
25-27yrs 6.70(2.09)
28-30yrs 6.18(1.89)
gender(n=262)
female 6.91(2.06) t=0.473 0.637 no difference

26 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
male 6.78(2.10)
religion(n=258)
Roman catholic 6.92(1.91)
F=2.083* 0.046 with
difference
Muslim 6.67(2.54)
Christian 6.96(2.260
Hinduism 7.0(1.69)
INC 6.1392.450
Atheist 6.2(2.07)
socio-economic status(n=146)
low 7.29(1.70)
F=0.345 0.709 no difference middle 6.91(1.91)
high 7.38(1.69)
educational attainment (n=216)
undergrad 6.87(2.12) t=0.143 0.886 no difference
grad school 6.82(1.74)
*significant at 0.05
4.5 Impact of Nicotine Dependency to Health Related Quality of Life (HRQoL)
Table 5 presents that there is significant association between the nicotine
dependency and health related quality of life namely mobility, self-care and
pain/discomfort. There is a weak inverse relationship between nicotine dependency and
mobility (r=0.141, p-value=0.022) This could probably be that the correspondent do not
experience any discomfort because that there are still in the early stage of smoking and
have not yet experience the impact of health problem associated to nicotine dependence,
Nicotine dependency and self-care(r=0.152, p-value=0.014) and nicotine dependency and
pain/discomfort (r=0.145, p-value=0.019).
However, result shows that there is weak positive association between nicotine
dependency and usual activities(r=0.05, p-value=0.423) and nicotine dependency and
anxiety/discomfort (r=0.094, p-value=0.128) which both are not statistically significant.

27 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Table 5
Impact of Nicotine Dependency to Health Related Quality of Life (HRQoL)
Quality of Life R p-value Interpretation
Mobility 0.141* 0.022 significant( weak positive)
Self-care 0.152* 0.014 significant(weak positive)
Usual activities 0.05 0.423 not significant
Pain/Discomfort 0.145* 0.019 significant(weak positive)
Anxiety/Depression 0.094 0.128 not significant
* Correlation is significant at the 0.05 level
4.6 Impact of Readiness to Quit to Health Related Quality of Life (HRQoL)
Table 6 shows that there’s a weak negative association between the
readiness to quit smoking and level of pain/discomfort (r=-0.146, p-value=0.018; and
between readiness to quit smoking and anxiety or depression (r=-0.247, p-value<0.001)
which are both statistically significant.
However, weak negative association but not statistically significant were observed
between readiness to quit smoking and mobility (r=-0.059, p-value=0.338); self-care (r=-
0.059, p-value=0.344) and usual activities (r=-0.099, p-value=0.11).
Table 6
Impact of Readiness to Quit to Health Related Quality of Life (HRQoL)
Quality of Life r p-value Interpretation
Mobility -0.059 0.338 not significant
Self-care -0.059 0.344 not significant
Usual activities -0.099 0.110 not significant
Pain/Discomfort -.146* 0.018 significant (weak negative association)

28 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Anxiety/Depression -0.247* 0.000 significant (weak negative association)
* Correlation is significant at the 0.05 level
5.0 Discussion
5.1 Table 1
The age relationship of increased smoking is mostly found among young adult of
age 19 to 21 years old and middle adult 25 to 27 shows the increased of nicotine
dependence according to the collected data, this is possibly that the increased result of
nicotine dependence among young adult of 19 to 21 years old could be associated to the
their young intuitive age were exploring is mostly common and as such will want to get
the feeling and experience of smoking. Contrast to the middle age group were increased
dependence of nicotine was found could lead to result of depression which is mostly
common to young adult of this age group possibly due to the fact that this is the stage of
young adult to adult life where decision making is common. In other studies young adults
are found to be majority of the smoking population. In agreement to our findings, young
adults are found to be most of the smoking population in the United States and Canada due
to the fact that they start around this age (Freedman et al. 2012). As stated by this article,
“Young adulthood represents a critical time in the transition from adolescence to
adulthood, when changes in risk-taking behaviors such as experimenting with smoking
become apparent.” Males in this population are greater than females which are in relation
to other study findings. Gender in this study comprises of the community perception
regarding gender smokers and acceptance, in female smokers, stereotyping is mostly
common compared to male smoker who the community give the most acceptance. Smoking
in female as it is compared to male smokers smoke for the possible reason of style, and
occasionally compare to men who already associating the practice as a habit, and could be
seen smoking in the public without stereotyping from other people like it is seen in the
female smokers. A study done in Bangladeshi and Pakistani adults, it was noted that men
smoke more than women for a number of reasons. It was found that men smoke more

29 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
because it is socially acceptable. According to Bush et al., if women smoking it is a shamed
upon society, so if women do smoke in these cultures they usually do it in secret. Possibly
it could be seen that some women still believe it to be shameful so they may not be smoking
regularly as men do.
Middle class people are the most common group of people in society, this group of
people are commonly found in every works of life and places, and are the most sociable.
Middle class is a state of financial being where the individual is not poor nor wealthy, and
this type of people have little or nothing to worry about like the poor who probably might
be thinking of what to eat after they get up in the morning, and the rich who are more
conscious with their security and social slandered in the society. Middle class individual as
we understand from the study has no problem buying a stick of cigarette nor trying to
maintain a social standard and isolating themselves from community perception. Middle
class is the majority of the respondents gathered. According to Katainen, the working class,
also known as the middle class, is increasing in the smoking population. They had found
that it is becoming a cultural practice and work habit among blue collar workers. Results
indicate that the middle class is increasing in smoking numbers, but are also still greater to
quit as compared to the high class smokers (Barbeau et al. 2004). As stated by Barbeau et
al., smoking can provide a means of coping with frustration,” which is an understanding
statement to possible findings of our frequency findings. Smoking could be a coping
method for some student who find college work as a stressor. As for religion differences
we resulted to almost half being catholic. Reason for this is because Philippines is a
predominantly catholic denomination of Christian country, and will be a bias statement if
we say that the possibility of smoking is more among the catholic denomination. Religion
frequencies has a great deal with location in many researches.
5.2 Table 2
The average nicotine dependency score among all the participants is a low to
moderate. “Nicotine dependence is a substance abuse disorder involving compulsive drug
use in spite of known health risks” (Mendelsohn 2011). The population had an overall low

30 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
score because they are students and probably only smoke because of the stress from school.
Another reason why they are not highly addicted is because the population sample are
enrolled in health related courses where they learn the effects of cigarette smoking. Though
they are not highly dependent but they are still dependent. Table 2 shows that the mean
average of our respondents score is almost 7, they plan to quit in the next 30 days.
“Everyone has their own reasons for quitting smoking but not everyone has made plan to
quit. Factors increasing the participants’ readiness to quit smoking could be further
understood in future studies.
Mobility, self-care, usual activities, pain/discomfort, and anxiety/depression are all
different dimensions in the health related quality of life. These mean scores are low due to
the fact that nicotine dependency is also low. It was similar in Lima et al (2014) study
where it was also found a relationship between nicotine dependence and health related
quality of life.
5.3 Table 3
Demographic profile on nicotine dependency shows significance in gender (table
3). Among the sexes, females happen to have a higher nicotine dependency than men in
this research. Possible reason why is because women feel more and handle there stresses
differently than men, but we could not really ascertain the main reason why they are more
dependent to men. Women smoking are also becoming acceptable in society according to
Waldron (2002). After the nineteen twenties equality among the sexes includes smoking
unintentionally. However, the increase in female smokers in the study is because women
as men have equal right and responsibility in the Philippines and as such society does not
totally shun the habit of female smokers to cigarette, their acceptance could be another
reason of the increase in cigarette consumption and together with other factors that may
lead to them been more dependent than men as seen in the study.

31 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
5.4 Table 4
Table 4 shows that among the demographic differences age, gender, socio-
economic status, and educational attainment have no difference with the readiness to quit
smoking. This means that these are not statistically significant to the research. However,
religion has a difference to readiness to quit with a result of F=2.083 and a p-value of 0.046.
Religion is an important factor in some people. In some religions it is frowned upon to
smoke because it is disrespectful, in others it is considered a sin to harm and damage your
own body. Religion could be the motivation to quit smoking. It was found in this study that
the respondents that are Hindu are more ready to quit with Roman Catholics and other
Christian denomination with similar perceptions of their readiness. Other studies (Bash et
al., 2003; Koenig et al., 1998) have similar findings. Smoking is religiously unacceptable
(Bash et al., 2003) and that religions activities influence individuals to quit smoking
(Koenig et al., 1998).
5.5 Table 5
Our research indicates that under health related quality of life mobility, self-care,
and pain/discomfort have a weak inverse relationship to nicotine dependency. In other
words, among the participants that have a low dependency to nicotine they have a better
perception of health and vice versa. The results conclude that there is an increase in
difficulty with mobility which may be due to the fact that there is lack of oxygen to the
body. There is also the possibility that the reason the participants feel a difficulty in
mobility is because cigarettes give a relaxed feeling to some and making it difficult to
actively walk about. To conclude, the more one smokes the more he may have a relaxed
feeling. The results in the ‘Tobacco Use among Adults with Disabilities in Massachusetts’
research concludes that adults with disabilities were more likely to have ever smoked and
to be current smokers (Brawarsky et al). Smoking may be continued in these participants
possibly because a decrease in mobility influences smoking. With self-care, there was also
a decrease which also may be due to the relaxed feeling. Another probability is that when
one smokes there becomes a buildup of plaque along the teeth as seen by many dentist.
32 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
This makes it difficult to keep the oral cavity always clean. Therefore when one smokes
more, one should also clean more and take more care of his hygiene. There was not enough
supporting evidence to how smokers with high nicotine dependency have a relationship to
self-care. Pain/discomfort maybe seen in smokers that have high nicotine dependency
because the more one smokes the less oxygen they are supplying to their bodies. Cigarettes
have many substances in just one stick, after lighting it and inhaling it, it causes suffocation
to the lungs. Those smokers that are not smoking as often possibly have better lungs that
can adjust to the lack of oxygen unlike those who are highly dependent. Lack of oxygen
can cause chest pains at first because that is the first system that is affected in the body, but
later lack of oxygen will start affecting different cells within the body. In other studies
frequent headaches or frequent tiredness and stress were reported in current smokers. “Also
some people might have taken up or resumed smoking because of pain” (Palmer et al.
2003).
5.6 Table 6
Table 6 express that participant’s level of pain/discomfort and anxiety/depression
are decreased and shows that there is an increase in their readiness to quit smoking.
Participants may be using this as a motivation to quit smoking because smoking may also
be the cause of pain. Smoking, especially deep inhaled smoke causes pain in the chest
because of the many substance in smoke and the lack of oxygen which leads to cell
proliferation. Since the participants are students in the Allied Health Program, anxiety and
depression may occur in the college life because of the possibility of developing lung
cancer. Depression may be used as a motivation to quit because smoking is frowned upon
especially to these types of students. As future doctors, dentist, nurses and others of the
health team, they learn the predisposing factors of many harmful diseases which smoking
happens to be one of the main cause. Possibly feelings shamed on from being a bad
example to others who is supposed to promote a healthy lifestyle. Similarly seen in a study
from Brawarsky et al, where it was found that the adults with disabilities that are smokers
feel more pain than the adults with disabilities that don’t smoke. It was also concluded in
this study that the more pain they felt the more likely to be planning to quit smoking. Also

33 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
the participants that felt more depressed were ready to quit as similar to a study that also
found that higher depressed smokers had a greater motivation to quit smoking among
females (Haukkala et al 2000).
6.0 Conclusion
The study aims to identify the differences in demographic profiles to nicotine
dependency and to readiness to quit. Also its target is to find the impact of nicotine
dependency and readiness to quit on the health related quality of life. It involved 262
purposively selected students from a Higher Educational Institution in the National Capital
Region in Philippines. The results pose that there are significant differences with
demographic profile and nicotine dependency, namely gender and educational attainment
differences. The test used indicate that female are more dependent to nicotine compared to
male who show less dependent to nicotine. Religion was another difference between
demographic profile and readiness to quit and which the Hindus shows more readiness
compare to other religion. As for the impact of nicotine dependence on health related
quality of life, there was a significant inverse relationship with mobility, self-care, and
pain, meaning that the more one is dependent to nicotine he or she may feel more
discomfort, and less discomfort if he or she is less dependent to nicotine. Lastly, it was
seen that in readiness to quit there was also an inverse relationship on health related quality
life with pain and anxiety meaning that does with decreased anxiety/depression show more
readiness to quit smoking and decrease level of pain/discomfort, and most of the
correspondent who feel anxious/depressed smoke more and show less readiness to quit and
also feel pain/discomfort sometimes when they smoke. Therefore, the more
anxious/depressed they are the more they smoke and sometime they feel pan/discomfort
after. These results highlight that nicotine dependency and readiness to quit both have an
impact on one’s health and should be considered in further research.

34 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
7.0 Recommendation
The researchers were able to answer the questions and accomplish their
goals with this study, however, future studies could further improve this by focusing on the
results from this research. In our research we found that pain and anxiety are inversely
related to readiness to quit, future studies can discover reasons why smokers are motivated
to quit. We will also recommend that other researchers to focus on the barriers to quit
smoking among the different levels of nicotine dependence. Similar studies should be
conducted correlating to antecedents and consequences of nicotine dependence and
readiness to quit with other variables in terms of environmental factors, peer pressure,
organization affiliation, family orientation and health perception.

35 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Reference
Barbeau, E. M.; Leavy-Sperounis, A.; Balbach, E. D. (2004). Smoking, social class, and
gender: what can public health learn from the tobacco industry about disparities in
smoking? Tob Control 13(2): 115-120. doi: 10.1136/tc.2003.006098
Borland, Ph.D, R., Yong, Ph.D, H., O'Connor, Ph. D, R., Hyland, Ph. D, A., & Thompson,
Ph. D, M. (2010). The Reliability and Predictive Validity of the Heaviness of
Smoking Index and Its Two Components: Findings from the International Tobacco
Control Four Country Study. Nicotine Tob Res, 12(Suppl 1), S45–S50. doi:
10.1093/ntr/ntq038
Brawarsky, P.; Brooks, D.R.; wilber, N.; Gertz, Jr. R. E.; walker, D. K. (2002.) Tobacco
Use Among Adults with Disablities in Massachusetts. Tob Control 2002; 11:ii329-
ii33 doi: 10.1136/tc.11.suppl_2.ii29
Bush, J.; White, M.; Kai, J.; Rankin, J.; Bhopal, R.; Usher, B.; Usher, J. (2003).
Understanding Influences on smoking in Bangladeshi and Pakistani adults:
community based, qualitative study. BMJ 2003; 326
doi:http://dx.doi.org/10.1136/bmj.326.7396.962
Chaiton, M., Cohen, J., McDonald, P., & Bondy, S. (2006). The Heaviness of Smoking
Index as a Predictor of Smoking Cessation in Canada. Addictive Behaviors, 32(5),
1031-1041. http://www.sciencedirect.com/science/article/pii/S0306460306002474
Coste, J., Quinquis, L., D'Almeida, S., & Audureau, E. (2014). Smoking and Health-
Related Quality of Life in the General Population. Independent Relationships and
Large Differences According to Patterns and Quantity of Smoking and to Gender.
PLoS ONE 9(3): e91562. doi:10.1371/journal.pone.0091562
Fagan PhD MPH, P., Augustson PhD MPH, E., Backinger PhD MPH, C. L., O'Connell
MA, M. E., Vollinger Jr MSPH, R. E., Kaufman BA, A., & Gibson BS, J. T. (2007).
Quit Attempts and Intention to Quit Cigarette Smoking Among Young Adults in
the United States. Am J Public Health, 97(8), 1412-1420. Doi:
10.2105/AJPH.2006.103697
Freedman, K. S.; Nelson MS, N. M.; Feldman EdS, L. L. (2012). Smoking Initiatoin
Among Young Adults in the United Sates and Canada, 1998-2010: A Systemic
Review. Prev Chronic Dis 2012; 9:110037. doi:
36 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
5. Katainen, A. (2010). Social class differences in the accounts of smoking - striving for
distinction? Sociology of Health and Illness Vol. 32 No. 7 2010, ISSN 0141-9889,
PP. 187-1101 DOI: 10.1111/J.1467-9566.2012.01267
Gilman, S. E., Abrams, D. B., & Buka, S. L. (2003). Socioeconomic status over the life
course and stages of cigarette use: initiation, regular use, and cessation. J Epidemiol
Community Health 57(10), 802-808. doi: 10.1136/jech.57.10.802
Gilman, S. E.; Martin, L. T.; Abrams, D. B.; Kawachi, I.; Kubzansky, L.; Loucks, E. B.;
Rende, R.; Rudd, R;.; Buka, S. L. (2008).Educational attainment and cigarette
smoking: a causal association. Int. J. Epidemiol. 2008; 37 (3): 615-624. doi:
10.1093/ije/dym250
Haukkala, A., Uutela, A., Vartiainen, E., Mcalister, A., Knekt, P. (2000) Depression and
Smoking Cessation: The role of Motivation and Self-efficacy. Addictive Behaviors,
vol 25(1), pp 311-316. Doi: 10.1016/S0306-4603(98)00125-7
Hiscock, R., Judge, K., & Bauld, L. (2010). Social inequalities in quitting smoking: what
factors mediate the relationship between socioeconomic position and smoking
cessation? Journal of Public Health, 23(1), 39-47. Doi:10.1093/pubmed/fdq097
Koenig, H.G., George, L. K., Cohen, H. J., Hays, J. C., Larson, D. B., & Blazer, D. G.
(1998). The Relationship Between Religious Activities and Cigarette Smoking in
Older Adults. Journal of Gerontology: MEDICAL SCIENCE, 53A (6): M426-
M434. http://biomedgerontology.oxfordjournals.org/
Lim K. H., Idzwan M. F., Sumarni M. G., Kee C. C., Amal N. M., Lim K. K., Gurpreet K.
(2012). Heaviness of smoking index, number of cigarettes smoked and the
Fagerstrom test for nicotine dependence among adult male Malaysians. Asian
Pacific Journal of Cancer Prevention, 13, 343–346.
Doi:10.7314/apjcp.2012.13.1.343
Lima, M. G., Borim, F. S. A., de Azeredo Barros, M. B. (2014) Smoking and Health-
Related Quality of Life (SF-36). A Population-Based Study in Campinas, Sp,
Brazil. Health, 6,1539-1548. http://dx.doi.org/10.4236/health.2014.612189
Ling MD MPH, P. M., & Glantz PhD, S. A. (2004). Tobacco Industry Research on
Smoking Cessation. Recapturing Young Adults and Other Recent Quitters. Journal
37 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
of General Internal Medicine, 19(5), 419–426. Doi: 10.1111/j.1525–
1497.2004.30358.x
Mendelsohn MB BS, C. (2011) Nicotine Dependence: Why is it so hard to quit? Medicine
Today 2011, 12(10): 35-40. http://medicinetoday.com.au/2011/october/feature-
article/nicotine-dependence-why-it-so-hard-quit
Paavola, M., Vartiainen, E., & Puska, P. (2000). Smoking cessation between teenage years
and adulthood. Health Education Research (2001) 16(1), 49–57. Doi:
10.1093/her/16.1.49
Palmer, K. T.; Syddall, H.; Cooper, C.; Coggon, D. (2003). Smoking and Musculoskeletal
Disorders: Findings from a British National Survey. Ann Rheum Disorder 2003;
62: 33-36 doi: 10.1136/ard.62.1.33
Sharma, M. K., Suman L. N., Manjula M., Marimuthu P., & Ahmad, M. (2011). Exploring
the Role of Religion in Smoking Cessation. Delhi Psychiatry Journal 14(1), 129-
132. http://medind.nic.in/daa/t11/i1/daat11i1p129.pdf
Shields, M., Garner, R. E., & Wilkin, K. (2013). Dynamics of smoking cessation and
health–related quality of life among Canadians. Health Reports, 24(2), 3–11.
http://www.statcan.gc.ca/pub/82003x/2013002/article/11769eng.htm
Siahpush, M., McNeill, A., Borland, R, & Fong, G.T. (2004). Socioeconomic variations in
nicotine dependence, self-efficacy, and intention to quit across four countries:
findings from the International Tobacco Control (ITC) Four Country Survey.
Tobacco Control 2006;15(Suppl III):iii71–iii75. doi: 10.1136/tc.2004.008763
Siahpish, M., Spittal, M., & Singh, G. K. (2007). Smoking cessation and financial stress.
Journal of Public Health, 29(4), 338-342. Doi:10.1093/pubmed/fdm070
Tammemägi, M. C., Berg, C. D., Riley, T. L., Cunningham, C. R., & Taylor K. L. (2014).
Impact of Lung Cancer Screening Results on Smoking Cessation. Journal of
National Cancer Institute, 106(6), 1–8. Doi: 10.1093/jnci/dju084
Tomioka, H., Sekiya, R., Nishio, C., & Ishimoto, G. (2014). Impact of smoking cessation
therapy on health–related quality of life. BMJ Open Respiratory Research, 1. 1–10.
Doi: 10.1136/bmjresp–2014–000047

38 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Waldron, I. (2002) Patterns and Causes of Gender Differences in Smoking. Social
Science and Medicine 13(9), 989-1005.
http://www.sciencedirect.com/science/article/pii/0277953691901578
Wang, Z., Koenig, H.G., & Shohalb, S. A. (2015). Religious involvement and tobacco use
in mainland China: a preliminary study. BMC Public Health 15.
Doi:10.1186/s12889-015-1478-y
Yong, H. H., Hamann, Ph. D, S. L., Borland, Ph. D, R., Fong, Ph. D, G. T., & Omar, Ph.
D, M. (2009). Adult Smokers' Perception of the Role of Religion and Religious
Leadership on Smoking and Association with Quitting: A Comparison between
Thai Buddhists and Malaysian Muslims. Social Science & Medicine, 69(7), 1025–
1031. doi:10.1016/j.socscimed.2009.07.042
39 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Appendix A Ethics Approval
40 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Appendix B
Permission to Use Questionnaire
41 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Appendix C
Consent Form
Dear Sir/Ma’am,
Greetings.
The name of the research is Antecedents and Consequences of Nicotine
Dependence and Readiness to Quit among Student Smokers of Allied Health Programs in
the Philippines. This research study is envisioned to identify the relationship of
demographic profile to nicotine dependency and readiness to quit, also to identify the
relationship of nicotine dependency and readiness to quit to health related quality of life.
The research will be given in a survey question that will take no longer than 10 minutes
to answer. There are no benefits or losses that will come to the participants. The
researchers will protect the confidentiality of the participant’s data, which includes name,
age, and other information about smoking. If the participant does not wish to answer the
research questions even after saying they would participate, there will be no penalty to
the participant.
Very truly yours,
Jade P. Mojica
(Principle Investigator)
“I have read the foregoing information, or it has been read to me. I have had the
opportunity to ask questions about it and any questions I have asked have been answered
to my satisfaction. I consent voluntarily to participate as a subject in this study and
understand that I have the right to withdraw from the study at any time without in any
way it affecting my further medical care.”
Signature over Printed name
(Participant)

42 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Appendix D Questionnaire of Demographic
Demographic Profile
1. Age:
□ 19yrs 21yrs □ 22yrs24yrs □ 25yrs 27yrs □ 28yrs 30yrs □ 31yrs or older
2. Sex (Gender):
□Male □Female
3. Religion:
□ Roman Catholic □ Christian □ Iglesia ni Cristo □ Muslim
□ Others_________________
4. Socio Economic Status:
5. Educational Attainment:
Currently Smoking
1. About how long have you been smoking?
_______Year(s) ______Month(s) ______Days
2. How many cigarettes do you usually smoke per day? (1 pack = 20 cigarettes).
_____Cigarettes
3. How soon after you wake up do you smoke?
□ Within 30 minutes □ After 30 minutes
Quitting Smoking
1. Do you want to quit smoking?
□ Yes □ No □ Unsure
2. How many times have you tried to quit smoking in the past?
_____ Times
3. What is the longest time that you have gone without smoking?
_____Year(s) _____Month(s) _____Day(s)
4. What is the ONE MOST IMPORTANT reason you want to quit smoking? (Check
ONE)
□ Health □Money □Significant others
□Social Acceptability □Religion
□Others (please describe) ________________________________________ Have Already Quit
1. Are you tempted to start again after you have quit?
□Yes □No 2. How long has it been since you stopped smoking?
_____ Year(s) _____Month(s) _____Days
43 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Appendix E
NIDA Clinical Trials Network
Fagerstrom Test for Nicotine Dependence (FND)
Do you currently smoke cigarettes?
No Yes
If “yes,” read each question below. For each question, enter the answer
choice which best describes your response.
1. How soon after you wake up do you smoke your first cigarette?
Within 5 minutes
6 to 30 minutes
31 to 60 minutes After 60 minutes
2. Do you find it difficult to refrain from smoking in places where it is
forbidden (e.g., in church, at the library, in the cinema)?
No Yes
3. Which cigarette would you hate most to give up?
The first one in the morning Any other
4. How many cigarettes per day do
you smoke?
10 or less
11 to 20
21 to 30 31 or more
5. Do you smoke more frequently during the first hours after waking than during
the rest of the day?
No Yes
6. Do you smoke when you are so ill that you are in bed most of the day?
No Yes
Comments: Heatherton TF, Kozlowski LT Frecker RC (1991). The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. British Journal of Addiction 86:1119-27.
44 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLEGE OF NURSING
10
9
8
7
6
5
4
3
2
1
Appendix F
Assessment of Motivation: Readiness to Quit Ladder Instructions: Below are some thoughts that smokers have about quitting. On the
ladder, circle the one number that shows what you think about quitting. Please
read each sentence carefully before deciding.
I have quit smoking.
I have quit smoking, but I still worry about slipping back, so I need to
keep working on living smoke free.
I still smoke, but I have begun to change, like cutting back on
the number of cigarettes I smoke. I am ready to set a quit date.
I definitely plan to quit smoking in the next 30 days.
I definitely plan to quit smoking in the next 6 months.
I often think about quitting smoking, but I have no plans to quit.
I sometimes think about quitting smoking, but I have no plans to quit.
I rarely think about quitting smoking, and I have no plans to quit.
I never think about quitting smoking, and I have no plans to quit.
I have decided not to quit smoking for my lifetime. I have no interest in quitting.

45 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLEGE OF NURSING
Appendix G
EQ-5D-5L
Figure 1: EQ-5D-5L (UK English sample version) Under each heading, please tick the ONE box that best describes your health
TODAY
MOBILITY
I have no problems in walking about
I have slight problems in walking about
I have moderate problems in walking about
I have severe problems in walking about
I am unable to walk about
SELF CARE
I have no problems washing or dressing myself
I have slight problems washing or dressing myself
I have moderate problems washing or dressing myself
I have severe problems washing or dressing myself
I am unable to wash or dress myself
USUAL ACTIVITIES (e.g. work, study, housework, family or
leisure activities)
I have no problems doing my usual activities
I have slight problems doing my usual activities
I have moderate problems doing my usual activities
I have severe problems doing my usual activities
I am unable to do my usual activities
PAIN / DISCOMFORT
I have no pain or discomfort
I have slight pain or discomfort
have moderate pain or discomfort
I have severe pain or discomfort
I have extreme pain or discomfort
ANXIETY / DEPRESSION
I am not anxious or depressed
I am slightly anxious or depressed
I am moderately anxious or depressed
I am severely anxious or depressed
I am extremely anxious or depressed
46 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
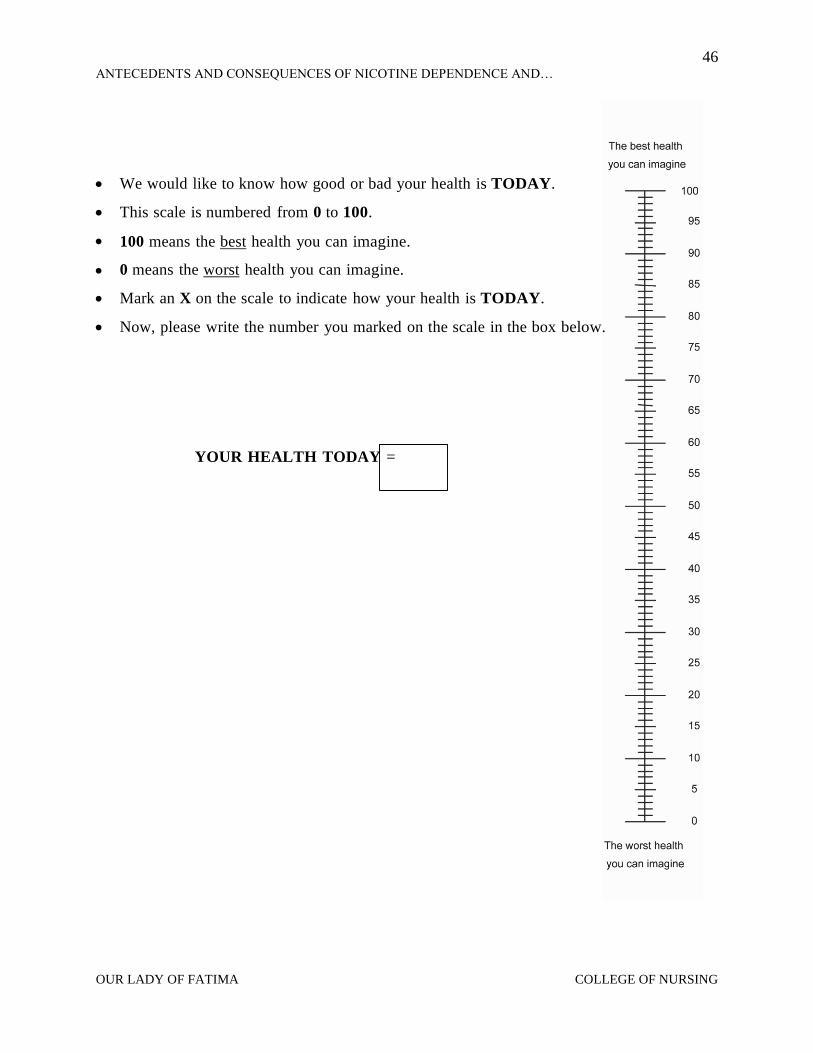
We would like to know how good or bad your health is TODAY.
This scale is numbered from 0 to 100.
100 means the best health you can imagine.
0 means the worst health you can imagine.
Mark an X on the scale to indicate how your health is TODAY.
Now, please write the number you marked on the scale in the box below.
YOUR HEALTH TODAY =
47 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Appendix H
Statistics Certificate
48 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
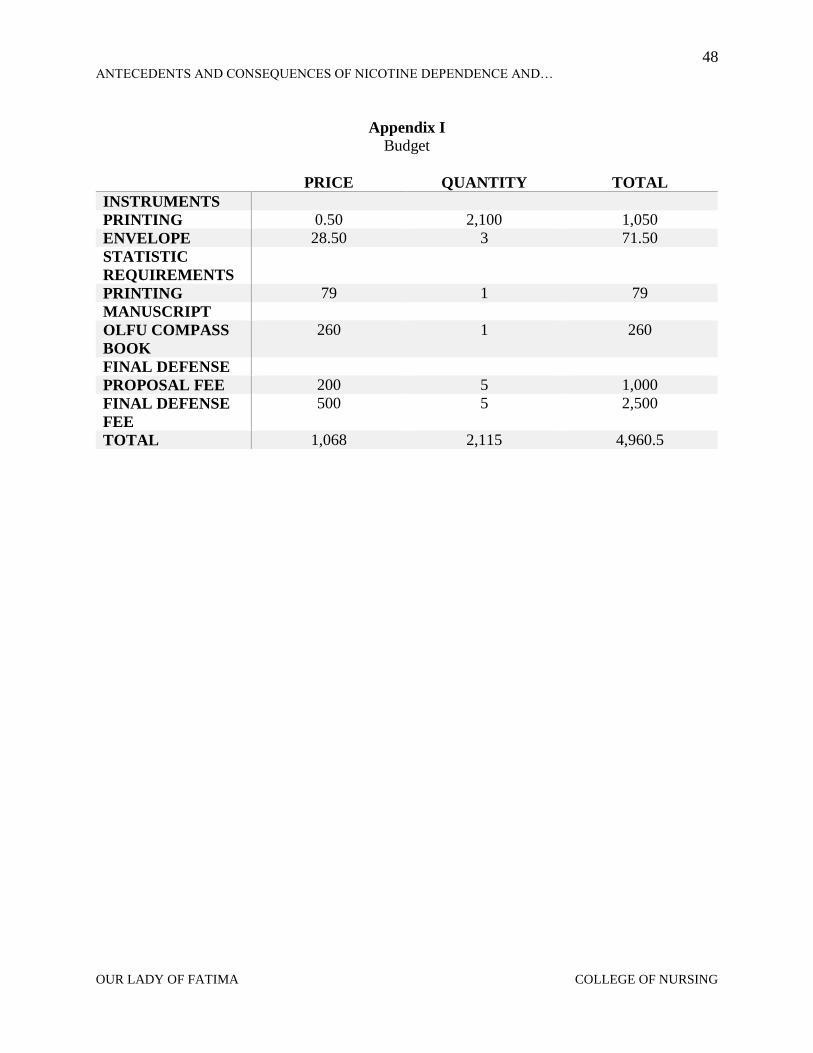
Appendix I
Budget
PRICE QUANTITY TOTAL
INSTRUMENTS
PRINTING 0.50 2,100 1,050
ENVELOPE 28.50 3 71.50
STATISTIC
REQUIREMENTS
PRINTING 79 1 79
MANUSCRIPT
OLFU COMPASS
BOOK
260 1 260
FINAL DEFENSE
PROPOSAL FEE 200 5 1,000
FINAL DEFENSE
FEE
500 5 2,500
TOTAL 1,068 2,115 4,960.5
49 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
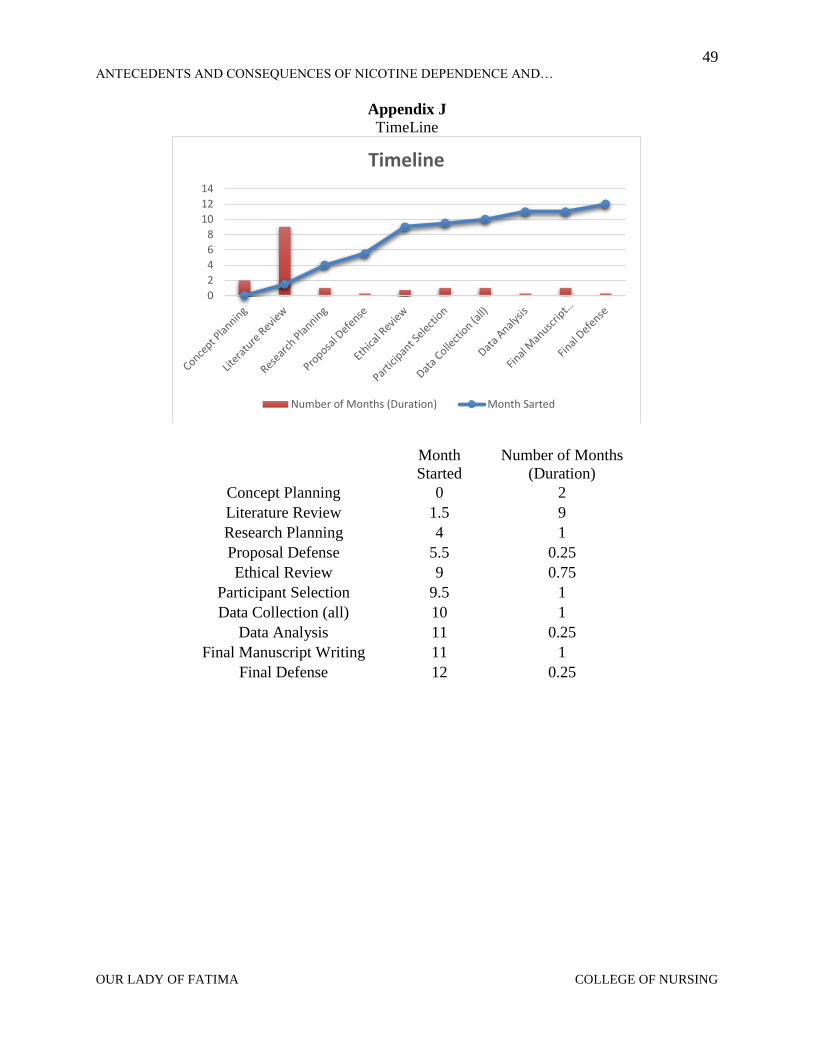
Appendix J
TimeLine
0
2
4
6
8
10
12
14
Timeline
Number of Months (Duration) Month Sarted
Month
Started
Number of Months
(Duration)
Concept Planning 0 2
Literature Review 1.5 9
Research Planning 4 1
Proposal Defense 5.5 0.25
Ethical Review 9 0.75
Participant Selection 9.5 1
Data Collection (all) 10 1
Data Analysis 11 0.25
Final Manuscript Writing 11 1
Final Defense 12 0.25
50 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Appendix K
About the Researchers
Jade Pohaku Maikai Mojica, the principal investigator of the study.
She is a hard working student who is kind and willing to help anyone
in need. She graduated high school in California where she was
enrolled in the Biomedical Careers Academy program where she was
CPR and first aid certified. She volunteered in school and sporting
events such as blood drives, fundraisers, and trash pickup. She started
her first year in college at Lyceum of the Philippines University and
later transferred to Our Lady of Fatima University. Her fourth year she
became emergency first aid certified, BLS- adult CPR for lay rescuers
certificate and became a member of the PRC. She plans to finish her
course in nursing and prepare herself for the licensure exam.
John Gerald A. Calisay, a co-investigator in the study. He is a kind
person who is friendly to all. He is a good listener and a student who
actively participates in class discussions. He sometimes plays
basketball, which reflects his team effort. His goals in life is to finish
his education to gain as much knowledge and skills to be an active
helper to the needs in his home place Samar.
Jason M. Franco, a coinvestigator in the study, is a former member and
officer of the Nightingale Civic Action Group. He is also a member of
Church of Christ (Iglesias Ni Cristo), and a former choir member. As a
member he helped in community clean up drives, and participated in
blood donations. In high school in New York, he was a member of the
photography club and cross country he also learned CPR in his health
class.
51 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Vikhuli Hansen, a coinvestigator of the study. She was one of the
International Students Organization Executive officers in the previous
college. She was a social worker in India and sent by her church leaders to
china and Thailand for Christian work. She was a nursing assistant in an
old care center in America and got best care giver appreciation award. After
graduating from Fatima, she plans to go back to America where she will
achieve her goal of opening a care center for the elderly so she may help
the poor and needy.
Owoh Joshua Amobi, a co-investigator in the study and the
presenter of the research paper. He is known with a character of
goal oriented and a strong will of achieving success in any event
of life even when the path to obtaining it is stiff, and as such drove
him toward obtaining the award of the best performing foreign
student in his former school, Lyceum of the Philippines University
Batangas. After his transfer to Our Lady of Fatima University, he
also obtained the certificate of the best case presenter in all third
year level interclass case presentation he is also a member of the
RED CROSS Valenzuela City Chapter Philippines. He obtains a
certificate in Disaster Nursing, and a Certified Emergency First
Aide Personnel, and a certified Basic Life Support-Adult CPR for Lay Rescuer PRC-Valenzuela
City Chapter. Joshua is a Senior Consultant with Edibongus Global LMT. He is a kind of student
who finds education as the key toward confidence of self-expression, and acquiring vast
knowledge. And God willing, he hope to further his education to becoming a medical doctor in the
nearest future, hence, giving back to the community the sense of vision if.

52 ANTECEDENTS AND CONSEQUENCES OF NICOTINE DEPENDENCE AND…
OUR LADY OF FATIMA COLLEGE OF NURSING
Acknowledgment
We would like to express our special thanks of gratitude to our advisers, Sir Clarence and
Jenica A. Rivero, who gave us the knowledge and guidance to conduct and put together this
study. We are now ready for future studies of our own from the understanding you had given us.
Secondly, we would like to thank the Research Development and Innovation Center for
helping, improving our study. We would like to give a special thank you to Dianna Eraphie A.
Tao-on and Michael Joseph Dino for statistical results and for enhancing our understanding of
research.
Thirdly, we would like to thank the students of the Allied Health Programs enrolled in
Our Lady of Fatima University for participating in our research because without you we would
not have an understanding to our study.
Lastly, we would like to thank our family and friends for being supportive during our
research by reminding us to focus on our goal and achievement.