Buletin 82014

of 19
Transcript of Buletin 82014
-
8/11/2019 Buletin 82014
1/19
Definition
Bipolar Disorder is a se-rious brain disorder that
limits ones ability to
function and to feel a
normal range of moods.
Bipolar disorder is also
known as manic depres-
sion. This serious mental
illness involves mood
swings that range any-
where from depression
to mania.
H i s t o r y
Bipolar Disorder is actu-ally one of the worldsoldest diseases. Usingearly medical records,researchers have found
symptomsof this disease recorded
from since the secondcentury. Aretaeus of Cap-padocia (a medical phi-losopher) first recog-nized and linked symp-toms of mania and de-pression, but his findings
were ignored. Then, in1650, scientist RichardBurton wrote a bookcalled The Anatomy ofMelancholia. Even to-day, he is credited as
being the founding fa-ther of depression as amental illness.
Pr eva l ence
About 4% of people suf-fer from bipolar disor-der. Prevalence is similarin men and women and,
broadly, across differentcultures and ethnicgroups .
I n t r o d u c t i o n
Si g n & sy mpt o ms o f bi po l a r
Bipo l ar bDiso r d er
Bipolar Spectrum 1
Criteria & Subtypes 1
Causes 2
Bipolar Spectrum& Criteria 2
Management 3
Electroconvelsive Therapy 3
BD in specific Population 4,5
HomeRemedies & Life 7
Conclusion & Refer- 7
Aktiviti Farmasi PKDTumpat
8-19
Inside this issue:
Dep r e ssi o n Fo r m
Constantly feeling sad orworthless
Sleep too much or too little
Feeling tired or lackingenergy
Appetite & weight changes
M a n i a F or m
increase in energy level- less need for sleep- easily distracted- nonstop talking
- increased self confidence
- focused on getting thingsdone, but does not accom-plish much
PHARMACY BULLETIN , OCT 2013
Unit Farm asi, Pejabat Kesihatan daerah Tum pat
-
8/11/2019 Buletin 82014
2/19
Gene t i c
BD tends to be familial
meaning that it runs withinfamilies. About 50% of peo-ples with BD have a familymember with a mood disor-ders, such as depression.
Neu r o c hem i c a l
Brain imaging studiesshowed dysfunction of cer-tain neurotransmitters suchas norepinephrine , seroto-nin and probably many oth-ers in people with BD.
E n v i r o nm e n t a l
There is fairly consistent evi-dence from prospective studiesthat recent life events and inter-personal relationships contributeto the likelihood of onsets andrecurrences of bipolar mood epi-sodes. There have been repeated
findings that between a thirdand a half of adults diagnosedwith bipolar disorder reporttraumatic/abusive experiencesin childhood.
Subs t ances /D r ugs
Drugs can trigger a manic epi-sode in people who are suscepti-ble to BD. For examples:
o Antidepresants
o llicit Drus such as cocaine,amphatemines, etc
o Excessive of appetite sup-presants, and cold prepara-tion.
o Nonantiphychiatric drugssuch as medicine for thyroidproblem or corticosteroid
o Excessive caffeine
PAGE2
c au ses
PHARMACY BULLETIN ,
A third and a half of adults diagnosed
with BD reports traumatic / abusive
experience in childhood
Bi po l a r spec t r u m
Msevere maniaDsevere depres-
sion (unipolar depres-sion)
mless severe mania(hypomania)
dless severe depression
http://en.wikipedia.org/wiki/Severe_depressionhttp://en.wikipedia.org/wiki/Severe_depressionhttp://en.wikipedia.org/wiki/Hypomaniahttp://en.wikipedia.org/wiki/Hypomaniahttp://en.wikipedia.org/wiki/Severe_depressionhttp://en.wikipedia.org/wiki/Severe_depression -
8/11/2019 Buletin 82014
3/19
Psychosoc i a l
Psychotherapy is aimed atalleviating core symptoms,recognizing episode triggers,reducing negative expressedemotion in relationships, rec-ognizing prodro-mal symptoms before full-blown recurrence, and, prac-ticing the factors that lead to
maintenance of remission
In general Cognitive behav-ioural therapy,family-focused therapy,andpsychoeducationhavethe most evidence for efficacyin regard to relapse preven-tion, while interpersonal andsocial rhythm therapy andcognitive-behavioural therapyappear the most effective inregard to residual depressivesymptoms.
promote brain to correct im-balances in the brain centersthat are responsible forsleep, appetite, mood andthought processes.
Electroconvulsive Therapay(ECT)formerly known aselectroshock .
During ECT, a small amountof electrical current is sent tothe brain, producing seizureactivity. This seizure activity
PAGE3
P h a rm am a c o t h e r a p y
BIPOLARBD I SORDER
man ag emen t
ELECTROCONVULSIVE THERAPY
o Lithium
Treating acute manic episodes,and preventing relaps
es, more so for manic than for depressive episodes .
o Anticonvulsants as Mood Stabilizerssuch as Car-bamazepine,(CBZ) Valproic Acid(VPA),Lamotrigin(LTG) often prescribed for people with rapid cycling
four or more episodes of mania and depression in ayear.CBZ and VPA tends to be more effective in treatingmania than depressive symptoms, however, LTG ap-pears to have stronger antidepressant than antimaniceffects
o Antipsychotic
Antipsychotics used to control phychotic symptom likedelusions or hallucination or mania symptoms. Neweragents eg Quetiapine ( Seroquel),Olanzapine(Zyprexa) help provide mood stabilizing effect ontheir own.
o Benzodiazepines (eg Diazepam, Clonazepam)
Short courses ofbenzodiazepines may be used as ad-junct to medications until mood stabilizing become ef-fective
http://en.wikipedia.org/wiki/Psychotherapyhttp://en.wikipedia.org/wiki/Prodromalhttp://en.wikipedia.org/wiki/Prodromalhttp://en.wikipedia.org/wiki/Cognitive_behavioural_therapyhttp://en.wikipedia.org/wiki/Cognitive_behavioural_therapyhttp://en.wikipedia.org/wiki/Family_therapyhttp://en.wikipedia.org/wiki/Family_therapyhttp://en.wikipedia.org/wiki/Psychoeducationhttp://en.wikipedia.org/wiki/Psychoeducationhttp://en.wikipedia.org/wiki/Interpersonal_and_social_rhythm_therapyhttp://en.wikipedia.org/wiki/Interpersonal_and_social_rhythm_therapyhttp://en.wikipedia.org/wiki/Benzodiazepineshttp://en.wikipedia.org/wiki/Benzodiazepineshttp://en.wikipedia.org/wiki/Benzodiazepineshttp://en.wikipedia.org/wiki/Benzodiazepineshttp://en.wikipedia.org/wiki/Interpersonal_and_social_rhythm_therapyhttp://en.wikipedia.org/wiki/Interpersonal_and_social_rhythm_therapyhttp://en.wikipedia.org/wiki/Psychoeducationhttp://en.wikipedia.org/wiki/Family_therapyhttp://en.wikipedia.org/wiki/Cognitive_behavioural_therapyhttp://en.wikipedia.org/wiki/Cognitive_behavioural_therapyhttp://en.wikipedia.org/wiki/Prodromalhttp://en.wikipedia.org/wiki/Prodromalhttp://en.wikipedia.org/wiki/Psychotherapy -
8/11/2019 Buletin 82014
4/19
with BD abuse alcoholand drugs as a way to es-cape. If addiction devel-ops, treatment become
complicated as bothmental health disordersand substance abusehave to be treated at the
Ch i l d r en / a do l escen t
Many parents are chal-lenged by a child who hasextreme changes inmood, energy, thinking,and behavior.
Children with BD are atgreater risk for anxietydisorders and attention-
deficit hyperactivity dis-orders.(ADHD) Thesecooccurring disorderscomplicate diagnosis ofBD and contribute to thelack recognition of ill-ness.
Moreover, many teen
same time.
L i t h i u m is the onl yrug approved by FDAfor children.
Psychological treatmentcombines normal-ly education on the dis-ease,group thera-
PAGE4
Bipo l a r in spec if ic po pu l at io n
Caption describing picture or graphic.
others drugs such as diuret-ics, angiotensinconvertingenzyme inhibitor(ACEIs),nonsteroidal anti inflammatorydrugs(NSAIDs),theophyllineand etc that may cause inef-ficacy and toxicity due to in-creased or decreased in levelof Lithium.
Issues affecting treatment
for elderly patient that
should be considered by clini-cians including access totransportation, financial diffi-culties, and recognition forthe need of treatment.
Sign/ Symptoms of Acute Lithi-um toxicity includes:
o Diarea
o Nausea
o Vomiting
o Ataxia
o Tremor
E l d e r l y
BD in later life is a complex
and confounding neuropsychi-atric syndromes with diagnos-tic and therapeutic challenges.
It is because metabolism of
drug can change with aging,and dramatic pharmacokineticdifferences resulting from thechange in adipose tissue, free
water, protein binding anddrug distribution.
For example in elderly taking
lithium, decreased renal clear-ance lead to a half life that isdouble the adult patient.
Moreover, there is a lot of in-
teraction between antipsy-chotics eg.Lithium with many
PHARMACY BULLETIN ,
There is a lot of interaction between
antipsychotics with many other drug that
may cause inefficacy and toxicity
http://en.wikipedia.org/wiki/Psychoeducationhttp://en.wikipedia.org/wiki/Psychoeducationhttp://en.wikipedia.org/wiki/Psychoeducationhttp://en.wikipedia.org/wiki/Group_psychotherapyhttp://en.wikipedia.org/wiki/Group_psychotherapyhttp://en.wikipedia.org/wiki/Psychoeducationhttp://en.wikipedia.org/wiki/Psychoeducation -
8/11/2019 Buletin 82014
5/19
Managing BD throughout a
pregnancy is a delicate bal-ance of the risks and benefitsof the illness versus treatment.
Lithium and first generationantipsychotics (Haloperidol)are preferred mood stabilizers
because they consistentlyshow minimal risk to the fe-tus.
Some convulsants such as
Valproic Acid and Carbamaze-pine have been proven harm-ful to fetus, possibly contrib-uting to birth defects.
Bear in mind, while takingLithium, it is important thatthe pregnant mother stay hy-drated to prevent Lithiumtoxicity .
prevent premature contrac-tion.
PAGE5
When Electroconvulsive Ther-
apy (ECT) was used in preg-nancy, it poses fewer risks andcomplications are uncommon.
However, it is important ofpregnant women to stay nour-ished and hydrated to help
BIPOLARBD I SORDER
Bipo l a r d iso r d er in pr eg n a n c y
DID YOU KNOW
Olanzapine (Zyprexa) has beenapproved by FDA for the treat-ment of acute mania is not associ-ated with birth defects.. However,Zyprexa has been asscociatedwith weight gain, gestational dia-
betes, Thus, blood sugar levelsand blood pressure should becarefully monitored in all pregnantwomen takeing Zyprexa.
Bipolar disorder can causesuicidal ideation that leadsto suicidal attempts.
One out of three people withbipolar disorder report pastattempts of suicide or com-plete it,and the annual aver-
age suicide rate is 0.4%,which is 10 to 20 times thatof the general population.
The depressed phase in BDlinked to about 80% of sui-cide attempts and completedsuicides.
Risk factors associated withcompleted suicide in BD in-clude:
o History of attempted sui-cideo Co-morbid anxiety disor-dero Hopelessness
o Alcohol/Substance Abuse
o Younger age of onset
The suicide rate is 10-20 times that of
the general population
20-50% of bipolar patients have at least
one suicide attempt
MORTALITY
http://en.wikipedia.org/wiki/Suicidalhttp://en.wikipedia.org/wiki/Suicidal -
8/11/2019 Buletin 82014
6/19
Quit drinking or usingillegal drugs.
Steer clear of un-
healthy relation-
ships.Surround yourself
with people who are a pos-
itive influence and won't
encourage unhealthy be-
havior or attitudes that canworsen your bipolar disor-
der.
PAGE6
Get regular exer-cise.Moderate, regular
exercise can help steady
your mood. Working out
releases brain chemicals
that make you feel good
(endorphins), can help
you sleep
Get plenty ofsleep.managing your
mood.
BIPOLARBD I SORDER
Al t er n at iv e t r eat men t
HO ME REMEDIES & l i f est y l es c h a n g es
Omega-3 fatty
acids.These oils may help improve brain function and depression associated
with bipolar disorder.
Magnesium. Several small studies have suggested that magnesium supplements may
lessen mania and the rapid cycling of bipolar symptoms.
St. John s wort This herb may be helpful with depression. However, it can also interactwith antidepressants and other medications, and it has the potential to
trigger mania in some people.
Acupuncture This ancient Chinese practice of inserting tiny needles into the skin mayrelieve depression, but more studies are needed to confirm its benefits
Yoga. Yoga may help ease depression and mood swings associated with bipo-lar disorder. It also has a number of other health benefits.
Massage therapy. Massage may also help relieve anxiety and stress, which can worsenbipolar symptoms.
Sts John Wort
-
8/11/2019 Buletin 82014
7/19
Bipolar Disorder ia a major public health problem associated with
significant morbidity and a high mortality risk. Several factors
make treatment complex, including the fluctuation of mood episodes
and the effects of these episodes on patient well being , drug non ad-
herences and co morbid conditions.
http://en.wikipedia.org/wiki/Bipolar_disorder (accessed on29/9/2013)
http://www.medicinenet.com/bipolar_disorder/article.htm(accessedon 29/9/2013)
http://www.webmd.com/bipolar-disorder/(accessed on 29/9/2013)
http://www.moh.gov.my/attachments/3897.pdf (CPG Major Depres-sive Disorder)(accessed on 29/9/2013)
http://www.psychiatry-malaysia.org/file_dir/144334708246e4d861559b8.pdf (Bipolar Disor-der)(accessed on 29/9/2013)
http://www.nimh.nih.gov/health/topics/bipolar-disorder(accessed on29/9/2013)
References
CONCLUSION
PAGE7
Editorial Board:
Supervisor
Pn Rohaya Hussin
Peg. Farmasi U48,KKWakaf Bharu
ditor
Cik Canthira a/p Eh Di Pn.Lim Yoke Kuan
Peg. Far,masi U44, Peg. Farmasi U44,KKWB
KK Pgkln Kubor KK Wakaf Bharu
-
8/11/2019 Buletin 82014
8/19
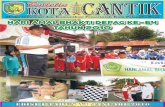
AKTIVITI UNT FARMASI PKD TUMPAT
Pelbagai Aktivitivi Penggunaan Ubat bBerkualiti dijalankan seperti ceramah dan pameranuntuk memastikan pengguna mengambil ubatubatan secara rasional.
PROGRAM KENALI UBAT ANDA
Pameran KENALI UBAT ANDA sempena Program Kelab Koperasi Negeri Kelantan
di Sekolah Kebangsaan Getting, Pengkalan Kubor pada 13 Mac 2013
-
8/11/2019 Buletin 82014
9/19
Ceramah KENALI UBAT ANDA disampaikan kepada kakitangan
Perhutannan Bukit Bakar pada 9th Oct 2013.
AKTIVITI UNT FARMASI PKD TUMPAT
-
8/11/2019 Buletin 82014
10/19
AKTI VI TI 5S
Objektif Amalan 5S:
o Mewujudkan persekitaran tempat kerja yangberkualiti dan produktif
o Hasil kebersihan, kekemasan, & keselamatan yang
nyatao Lebih banyak idea kreatif & inovatif diketengahkan
oleh pekerja untuk penyelesaikan masalah&penambahbaikan
o Operasi di tempat kerja lebih senang, pantas, &selamat.
AKTIVITI UNT FARMASI PKD TUMPAT
-
8/11/2019 Buletin 82014
11/19
Aktiviti S KK BANDAR
TUMPAT
UbatUbatan dilabel dengan kemas dan menggunakan TALL MAN lettering un-
tukubat LOOK ALIKE
-
8/11/2019 Buletin 82014
12/19
Gambar SEBELUM & SELEPAS Aktiviti 5S KK Pengkalan Kubor
BEFORE
BEFORE
AFTERBEFORE
AFTER
AFTER
-
8/11/2019 Buletin 82014
13/19
Gambar SEBELUM & SELEPAS aktiviti 5S KK Wakaf Bharu
-
8/11/2019 Buletin 82014
14/19
SAMBUNG...
-
8/11/2019 Buletin 82014
15/19
G a m b a r SE BE L U M & SE L E PA S
a k t i v i t i 5S K K B u n o h a n
BEFORE
BEFORE
AFTER
AFTER
Kaunt er yang cer i a dan kondusi f
-
8/11/2019 Buletin 82014
16/19
J AM UAN PERPI SAHAN
E N N I K M O H D N O R (P P F U 32)
JASAMU dikenang...
AKTIVITI UNT FARMASI PKD TUMPAT
Di Restauran KAFI, Wakaf Bharu
Di Restauran Horizon, Wakaf Cheyeh
-
8/11/2019 Buletin 82014
17/19
Siti Zulaikha Binti Ramly
Pegawai Farmasi U41
Graduated with a Bachelor of Pharmacy with Honors,
University Sains Malaysia (2008-2012)
PRP of HRPZ II,Kota Bharu, Kelantan.(2012-2013)
FRP of PKD Tumpat, Kelantan (KK Tumpat)
Tarikh lapor diri: 27th Jan 2014
Nur Alyaa Bajana Binti Abd Malik
Pegawai Farmasi U41
Graduated with a Bachelor of Pharmacy with Honors,
University Sains Malaysia (2008-2012)
PRP of Hospital Besut, Terengganu( 2012-2013)
FRP of PKD Tumpat, Kelantan (KK Wakaf Bharu)
Tarikh lapor diri: 3th Mac 2014
WELLCOM I NG NEW STAFFS
AKTIVITI UNT FARMASI PKD TUMPAT
-
8/11/2019 Buletin 82014
18/19
Bibi Norazilah Binti Azuratmi
Pegawai Farmasi U44
Graduated with a Bachelor of Pharmacy with Honors,
Universitiy Teknologi Mara (2006-2010)
PRP of HTAA, Kuantan , Pahang (2019-2011)
FRP of PKD Tumpat, Kelantan (KK Wakaf Bharu)
Tarikh lapor diri: 3th Mac 2014
Nur Syamimi Binti Mamat
Pegawai Farmasi U41
Graduated with a Bachelor of Pharmacy with Honors,
University Kebangsaan Malaysia(2008-2012)
PRP of HRPZ II, Kota Bharu , Kelantan.(2012-2013)
FRP of PKD Tumpat, Kelantan (KK Sg. Pinang)Tarikh lapor diri: 10th Apr 2014
WELLCOM I NG NEW STAFFS
AKTIVITI UNT FARMASI PKD TUMPAT
-
8/11/2019 Buletin 82014
19/19
Menimangcahaya mata
T HNI H
Pn Rohaya Bt Hussin Pegawai Farm asi U48
- Melahirkan bayi perempuan ke-5 pada 7 Nov 2013
A khi rn