BrHeart J Streptokinase thrombin stenosis · Ranjadayalan,Stevenson,Marchant,...
5
Br Heart J 1992;68:171-5 Streptokinase induced defibrination assessed by thrombin time: effects on residual coronary stenosis and left ventricular ejection fraction Kulasegaram Ranjadayalan, Robert Stevenson, Bradley Marchant, Velaitham Umachandran, Simon W Davies, Denise Syndercombe-Court, Charles N Gutteridge, Adam D Timmis Department of Cardiology, Newham General Hospital, London K Ranjadayalan V Umachandran Department of Haematology, The Royal London Hospital, London D Syndercombe-Court C N Gutteridge Department of Cardiology, The London Chest Hospital, London R Stevenson B Marchant S W Davies A D Timmis Correspondence to Dr Adam D Timmis, Department of Cardiology, The London Chest Hospital, Bonner Road, London E2 9JX Accepted for publication 13 February 1992 Abstract Objective-To evaluate laboratory markers of defibrination early after thrombolytic therapy and to determine their relation to residual stenosis and left ventricular ejection fraction measured angiographically before dis- charge from hospital. Design-Prospective analysis of defibrination after streptokinase measured by fibrinogen assay and thrombin time to provide a comparison of these coagulation variables for predic- ting angiographic responses to treat- ment in patients with acute myocardial infarction. Setting-The coronary care unit of a district general hospital. Patients-44 patients with acute myocardial infarction treated by streptokinase infusion, all of whom underwent paired blood sampling before and one hour after streptokinase and cardiac catheterisation at a median of six (interquartile range 3-9) days later. Main outcome measures-Assay of thrombin time and plasma fibrinogen concentrations one hour after strepto- kinase infusion. Relations between these coagulation variables and residual sten- osis in the infarct related coronary artery and left ventricular ejection frac- tion. Separate analyses are presented for all patients (n = 44) and those with patency of the infarct related artery (n = 35). Results-Streptokinase infusion produced profound defibrination in every patient as shown by changes in thrombin time and circulating fibrinogen. Throm- bin time after streptokinase infusion correlated significantly with both residual stenosis (r = -0-43, p < 0 005) and left ventricular ejection fraction (r = 0-38, p < 0 02). The importance of these correlations was emphasised by the interquartile group comparison which showed that a thrombin time > 49 seconds predicted a residual stenosis of 74% and an ejection fraction of 65%, compared with 90% and 49% for a thrombin time <31 seconds (p < 0 01). When the analysis was restricted to patients with patency of the infarct related artery, the correlation between thrombin time and residual stenosis remained significant and group compar- isons continued to show that patients in the highest quartile range had more widely patent arteries and better preservation of ejection fraction. Analysis of the fibrinogen data, on the other hand, showed insignificant or only marginally significant correlations with these angiographic variables. Conclusions-Early after streptokin- ase infusion for acute myocardial infarc- tion, the level of defibrination measured by thrombin time has an important in- fluence on residual coronary stenosis and left ventricular ejection fraction at dis- charge from hospital, values above 49 seconds being associated with the best angiographic result. (Br Heart J 1992;68:171-5) Reduction in circulating fibrinogen has been regarded as a major requirement for success- ful thrombolytic therapy and some,' 2 though not all,3 investigators have confirmed that high residual plasma concentrations are often as- sociated with non-patency of the infarct related coronary artery. Non-patency of the infarct related coronary artery at discharge from hospital has an adverse effect on one year mortality,4 and there is an empirical but unproved assumption that a high grade residual stenosis may also increase the risk of recurrent events. Left ventricular ejection fraction at discharge from hospital is recog- nised as an important determinant of long term outcome,56 but it remains unknown to what extent these angiographic variables are affected by the level of defibrination after thrombolytic therapy. The purpose of our study, therefore, was to evaluate laboratory markers of defibrination early after throm- bolytic therapy and to determine their relation to residual stenosis and left ventricular ejection fraction found before discharge from hospital. Defibrination was estimated by fibrinogen assay and also by thrombin time (a measure of the functional integrity of circulating fibrinogen) to provide a compari- son of these coagulation variables for pre- dicting angiographic responses to infusion of streptokinase.7 171 on July 12, 2020 by guest. Protected by copyright. http://heart.bmj.com/ Br Heart J: first published as 10.1136/hrt.68.8.171 on 1 August 1992. Downloaded from
Transcript of BrHeart J Streptokinase thrombin stenosis · Ranjadayalan,Stevenson,Marchant,...

Br Heart J 1992;68:171-5
Streptokinase induced defibrination assessed bythrombin time: effects on residual coronarystenosis and left ventricular ejection fraction
Kulasegaram Ranjadayalan, Robert Stevenson, Bradley Marchant,Velaitham Umachandran, Simon W Davies, Denise Syndercombe-Court,Charles N Gutteridge, Adam D Timmis
Department ofCardiology, NewhamGeneral Hospital,LondonK RanjadayalanV UmachandranDepartment ofHaematology, TheRoyal LondonHospital, LondonD Syndercombe-CourtC N GutteridgeDepartment ofCardiology, TheLondon ChestHospital, LondonR StevensonB MarchantSW DaviesA D TimmisCorrespondence toDr Adam D Timmis,Department of Cardiology,The London Chest Hospital,Bonner Road, LondonE2 9JXAccepted for publication13 February 1992
AbstractObjective-To evaluate laboratorymarkers of defibrination early afterthrombolytic therapy and to determinetheir relation to residual stenosis andleft ventricular ejection fractionmeasured angiographically before dis-charge from hospital.Design-Prospective analysis of
defibrination after streptokinasemeasured by fibrinogen assay andthrombin time to provide a comparisonof these coagulation variables for predic-ting angiographic responses to treat-ment in patients with acute myocardialinfarction.Setting-The coronary care unit of a
district general hospital.Patients-44 patients with acute
myocardial infarction treated bystreptokinase infusion, all of whomunderwent paired blood sampling beforeand one hour after streptokinase andcardiac catheterisation at a median ofsix (interquartile range 3-9) days later.Main outcome measures-Assay of
thrombin time and plasma fibrinogenconcentrations one hour after strepto-kinase infusion. Relations between thesecoagulation variables and residual sten-osis in the infarct related coronaryartery and left ventricular ejection frac-tion. Separate analyses are presented forall patients (n = 44) and those withpatency of the infarct related artery(n = 35).Results-Streptokinase infusion
produced profound defibrination in everypatient as shown by changes in thrombintime and circulating fibrinogen. Throm-bin time after streptokinase infusioncorrelated significantly with bothresidual stenosis (r = -0-43, p < 0 005)and left ventricular ejection fraction(r = 0-38, p < 0 02). The importance ofthese correlations was emphasised by theinterquartile group comparison whichshowed that a thrombin time > 49seconds predicted a residual stenosis of74% and an ejection fraction of 65%,compared with 90% and 49% for athrombin time <31 seconds (p < 0 01).When the analysis was restricted topatients with patency of the infarct
related artery, the correlation betweenthrombin time and residual stenosisremained significant and group compar-isons continued to show that patients inthe highest quartile range had morewidely patent arteries and betterpreservation of ejection fraction.Analysis of the fibrinogen data, on theother hand, showed insignificant or onlymarginally significant correlations withthese angiographic variables.Conclusions-Early after streptokin-
ase infusion for acute myocardial infarc-tion, the level of defibrination measuredby thrombin time has an important in-fluence on residual coronary stenosis andleft ventricular ejection fraction at dis-charge from hospital, values above 49seconds being associated with the bestangiographic result.
(Br Heart J 1992;68:171-5)
Reduction in circulating fibrinogen has beenregarded as a major requirement for success-ful thrombolytic therapy and some,' 2 thoughnot all,3 investigators have confirmed that highresidual plasma concentrations are often as-sociated with non-patency of the infarctrelated coronary artery. Non-patency of theinfarct related coronary artery at dischargefrom hospital has an adverse effect on one yearmortality,4 and there is an empirical butunproved assumption that a high graderesidual stenosis may also increase the risk ofrecurrent events. Left ventricular ejectionfraction at discharge from hospital is recog-nised as an important determinant of longterm outcome,56 but it remains unknown towhat extent these angiographic variables areaffected by the level of defibrination afterthrombolytic therapy. The purpose of ourstudy, therefore, was to evaluate laboratorymarkers of defibrination early after throm-bolytic therapy and to determine their relationto residual stenosis and left ventricularejection fraction found before discharge fromhospital. Defibrination was estimated byfibrinogen assay and also by thrombin time (ameasure of the functional integrity ofcirculating fibrinogen) to provide a compari-son of these coagulation variables for pre-dicting angiographic responses to infusion ofstreptokinase.7
171
on July 12, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.68.8.171 on 1 A
ugust 1992. Dow
nloaded from

Ranjadayalan, Stevenson, Marchant, Umachandran, Davies, Syndercombe-Court, Gutteridge, Timmis
Patients and methodsPATIENTSTable 1 shows demographic data of thepatients. We studied 44 patients with acutemyocardial infarction treated with 1-5 mU ofstreptokinase infused intravenously over onehour. Two hours after completion of strepto-kinase, the patients were anticoagulated withheparin infused at 1000 units/hour for 48hours and thereafter were started on 75 mg ofaspirin daily according to treatment policy atthe time this study was undertaken.
BLOOD SAMPLING AND ANALYSISPaired venous blood samples were takenimmediately before streptokinase infusion andagain one hour afterwards, before infusion ofheparin had been started. Samples weredrawn without venous occlusion,anticoagulated in sodium citrate, centrifuged,and the plasma frozen to -20°C within 30minutes of drawing the blood. The plasmawas thereafter stored at -80°C until analysisin one batch for measurement of fibrinogenconcentration and thrombin time. Fibrinogenwas measured by the method of Clauss8 andthrombin time by automated photoden-sitometry in an ACL-2000.
CARDIAC CATHETERISATIONAll patients gave written informed consent forcardiac catheterisation by either Judkins orSones techniques involving coronary arterio-graphy with at least five views of the leftsystem and three of the right, and single plane(right anterior oblique) left ventriculography.Studies were performed at a median of six(interquartile range 3-9) days after hospitaladmission to determine the patency of theinfarct related coronary artery, the degree ofresidual stenosis, and left ventricular function.The infarct related artery was identified as theartery subtending the ventriculographic dys-kinetic segment that corresponded to the areaof acute injury on the admission electrocar-diogram. In this study we encountered noambiguity between circumflex and rightcoronary arteries in patients with inferiorinfarction. The coronary lesions wereanalysed for patency by two experienced
Table 1 Patient characteristics
Characteristic No
No of patients 44Age (median (interquartile range)) (y) 59 (52-65)SexMen 36Women 8
Infarct locationAnterior 22Inferior 22
History of previous infarction 5Time to streptokinase
(median (interquartile range)) (min) 210 (155-278)Time to cardiac catheterisation
(median (interquartile range)) (days) 6 (3-9)Infarct related coronary artery
Patent 35Non-patent 9
Coronary artery diseaseSingle vessel 18Multivessel 26
Left ventricular ejection fraction(median (interquartile range)) (%) 58 (50-62)
observers (ADT, RS), the quantitativeanalysis being performed by RS alone. Bothobservers were blinded to the results of thecoagulation analysis. For quantitativeanalysis, two views were selected that weremost nearly orthogonal to the diseased seg-ment and to one another with the least overlapof other coronary branches. The two viewswere projected with magnification onto whitepaper and traced by hand. Patency of theinfarct related coronary artery was assessed bythe thrombolysis in myocardial infarction(TIMI) criteria.9 Residual stenosis was takenat the narrowest point within the lesion re-lated to the calibre of the normal segmentimmediately proximal to the lesion. Theinterobserver reproducibility of this techniquehas previously been reported.'0 Left ven-tricular ejection fraction was measured by themethod of Sandler and Dodge."
STATISTICAL ANALYSISIn all analyses, non-parametric statistics wereused. Averaged values are expressed asmedian with the interquartile range in paren-theses. Unpaired comparisons were made withthe Mann-Whitney U test, paired compar-isons with the Wilcoxon test, and correlationswere examined with the Spearman rank cor-relation coefficient. Statistical significance wastaken as p < 0 05 although marginal values(>0.05-<0 1) have been recorded in themanuscript.
ResultsRESPONSES TO STREPTOKINASEStreptokinase infusion produced profounddefibrination in every patient as reflected byreductions in circulating fibrinogen andincreases in thrombin time. Bleeding complica-tions occurred in two patients, one of whomsufferedgastrointestinalhaemorrhage requiringblood transfusion and the other frank hae-maturia. In both cases the baseline fibrinogenconcentrations were high (3 7 and 4 0 g/l)compared with the remainder of the group, andshowed an exaggerated decline (- 3-6 and-3 9 g/l) in response to streptokinase. Table 2shows responses to streptokinase.
DEFIBRINATION AND CORONARY PATENCYCoronary arteriography after three to nine daysshowed patency of the infarct related artery in35 cases (80%). Comparison of coagulationvariables in patients with and without coronaryarterypatencyshowedno significantdifferences.Quantitative analysis, however, ofthe degree ofresidual stenosis (range 39%-100%) showed ahighly significant correlation with the thrombintime one hour after streptokinase. Whenanalysis was confined to the 35. patients withpatency of the infarct related artery, thecorrelation between residual stenosis (range39%-99%) and thrombin time remainedstatistically significant. Correlations with cir-culating fibrinogen, on the other hand, were notsignificant.The relation between defibrination and the
efficacy of treatment is emphasised in figures 1and 2 where residual stenoses of patients in the
172
on July 12, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.68.8.171 on 1 A
ugust 1992. Dow
nloaded from

Defibrination after streptokinase
Table 2 Coagulation variables before and one hour after streptokinase infusion
Before streptokinase I hour after streptokinase(median (interquartile range)) (median (interquartile range)) p Value
Fibrinogen (g/1) 2-8 (2 3-3 3) 0-21 (0-160-27) <0-001Thrombin time (s) 137 (116-157) 371 (307-489) <0-001
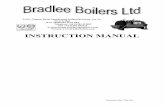
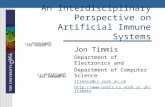
highest and lowest quartile ranges for thrombintime and fibrinogen are compared. Patients inthe highest quartile range for thrombin timehad more widely patent arteries with sig-nificantly less severe residual stenoses thanpatients in the lowest quartile range, regardlessofwhether the analysis included all patients (fig1) or only those with a patent infarct relatedartery (fig 2). Fibrinogen analysis, on the otherhand, was less helpful and failed to separatepatients on the basis of residual stenosis.
DEFIBRINATION AND LEFT VENTRICULAREJECTION FRACTIONDefibrination after streptokinase was an impor-tant determinant of residual left ventricularejection fraction shortly before discharge fromhospital. Thus the thrombin time one hourafter treatment correlated significantly with leftventricular ejection fraction, although whenthe analysis was confined to patients with apatent infarct related artery the correlation wasweaker and just failed to reach statistical sig-nificance (table 3). Nevertheless, the interquar-tile group comparisons confirmed that patientsin the highest range for thrombin time hadsignificantly better preservation of left ven-tricular ejection fraction than patients in thelodwest range, regardless of whether all patientswere included or only those with a patentinfarct related artery (figs 1 and 2).
Figure I The effects ofthrombin time and plasmafibrinogen one hour afterstreptokinase on residualcoronary stenosis and leftventricular ejectionfraction (LVEF). Thesedata arefor all of the 44patients and compare thehighest (n = 11) andlowest (n = 11) quartileranges for each coagulationvariable. Each box plotdisplays the 10th, 25th,50th, 75th and 90thpercentile values. Notchesrepresent 95% confidenceintervals about themedian.
110
g- 100.T 90cno 80ca,4, 70coXu 60
n 50
= 40znI
-
LL
Ji
Figure 2 The effects ofthrombin time and plasmafibrinogen one hour afterstreptokinase on residualcoronary stenosis and leftventricular ejectionfraction (LVEF). Thesedata arefor the 35patients with patency ofthe infarct related arteryand compare the highest(n = 9) and lowest(n = 9) quartile rangesfor each coagulationvariable. Each box plotdisplays the 10th, 25th,50th, 75th and 90thpercentile values. Notchesrepresent 95% confidenceintervals about themedian.
o
0.U_0)
a)
co
LL
-J_n
cr
0-0R
-i
Thrombin time at 1 h
T
110
100
90
8070
60
50
40n.
i p < 0.01
Ju
90 _80 - T70
60-504030
p < 0.00520
10Thrombin time Thrombin time
49s .31 s
110 Thrombin time at 1 h
100 _90 - T80 -
70
6050 p < 0.054030
90 _
80
70 L60 - <T50
4030 p<0.0220
Thrombin time Thrombin time¢ 50 s 31 s
Fibrinogen at 1 h
p = 0.06
90 _80
70 T60 _- < T,..,,.950 _ b40-
30 - p < 0.0052010
Fibrinogen Fibrinogena 0.27 g/l > 0.16 g/l
110 Fibrinogen at 1 h100 _90
807060 _
50
40 NS30F
90
80
70
60
50 -
40 NS
30,Fibrinogen) 0.27 g/l
Fibrinogen> 0.15 g/l
173
-rl
I
on July 12, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.68.8.171 on 1 A
ugust 1992. Dow
nloaded from

Ranjadayalan, Stevenson, Marchant, Umachandran, Davies, Syndercombe-Court, Gutteridge, Timmis
Table 3 Relation between coagulation variables, residual coronary stenosis, and leftventricular ejection fraction
Coagulation variable I hour after streptokinase
Thrombin time (s) Fibrinogen (g/l)
r* p Value r* p Value
All patients (n = 44):Residual stenosis (%) -043 <0-005 0-28 0 07LVEF (%) 0-38 <0-02 -0-29 0 05
Patients with patent IRCA (n = 35):Residual stenosis (%) -038 <0 05 - NSLVEF (%) 0-32 0-06 - NS
*Correlation coefficient (Spearman's rank method). IRCA, infarct related coronary artery.
Plasma fibrinogen concentrations one hourafter streptokinase also correlated weakly withleft ventricular ejection fraction when data forall patients were analysed. The interquartilegroup comparison confirmed that patients inthe lowest range for fibrinogen concentrationhad significantly better preservation of ejectionfraction (fig 1). When the analysis was confinedto patients with a patent infarct related arteryneither the correlation with ejection fractionnor the interquartile group comparison was
significant.
DiscussionHigh plasma fibrinogen concentrations afterthrombolytic therapy are often associated withnon-patency of the infarct related coronary
artery.' 2 In our study, however, this associa-tion could not be tested because all the patientsshowed profound reductions in circulatingfibrinogen that exceeded 80% in every case.
Nevertheless, quantitative analysis of residualcoronary stenosis showed that the degree ofarterial patency correlated significantly with thelevel of defibrination when this was assessed bymeasurement of thrombin time. The impor-tance of this correlation was emphasised by theinterquartile group comparison which showedthat a thrombin time of more than 49 secondsafter streptokinase was associated with a
median residual stenosis of 74%, comparedwith 90% for a thrombin time of less than 31seconds. Part of this difference might beexplained by non-patency of the infarct relatedartery in patients who did not defibrinate suf-ficiently in response to streptokinase. This doesnot, however, provide the full explanationbecause the difference, though more weaklysignificant, persisted even when patients withnon-patency were excluded from analysis in-dicating that the association between highgrade residual stenosis and attenuation of thethrombin time response was not merely theresult of failed thrombolysis. The data suggest,therefore, that vigorous defibrination early afterstreptokinase, as indicated by significantprolongation of the thrombin time, ensures
more effective thrombolysis and a more widelypatent infarct related artery.
Arterial patency is a major goal of throm-bolytic therapy that may have an importantindependent influence on long term prognosis.4The degree of arterial patency, however, as
reflected by residual stenosis, has received lessattention as a predictor ofoutcome although, ininterventional studies, patients treated bydirect angioplasty have been shown to havemore widely patent arteries and better preser-vation of ventricular function than thosetreated by intracoronary streptokinase."' Thefindings in our study are to some extentanalogous, in that an exaggerated thrombintime response was associated not only with amore widely patent coronary artery but alsowith better preservation of left ventricularejection fraction. Although correlations be-tween thrombin time and left ventricular ejec-tion fraction were generally weak, and justfailed to reach statistical significance, in thesubgroup with coronary patency interquartilegroup comparison with data on thrombin timeshowed highly significant differences betweenresidual ejection fractions for patients in thehighest and lowest quartile ranges. Thus athrombin time of more than 49 seconds wasassociated with a median ejection fraction of65% compared with only 49% for a thrombintime of less than 31 seconds. Similar differenceswere shown when patients with non-patency ofthe infarct related artery were excluded fromthe analysis, again indicating that these findingswere not merely a reflection of the knownassociation between failed thrombolytictherapy and more extensive myocardial injury.Thus the data suggest that the level of defibrin-ation, as shown by the thrombin time one hourafter streptokinase infusion, may have animportant influence on the residual left ven-tricular ejection fraction after acute myocardialinfarction.Although mechanisms relating defibrination
to ejection fraction are not clear, the degree ofarterial patency may play a contributory part.Thus vigorous defibrination produces a morewidely patent infarct related artery that maypermit more effective and perhaps earlier reper-fusion leading to greater myocardial salvage. Aless vigorous response, on the other hand,associated with high grade residual stenosis, isunlikely to restore adequate perfusion, par-ticularly after thrombolytic therapy when thedynamics ofcoronary flow are adversely affectedby plaque rupture and intraluminal thromboticdebris.'0 Nevertheless, residual stenosis andejection fraction were not significantly cor-related in our study indicating that other fac-tors may also play a part in the associationbetween defibrination and left ventricular func-tion. Recent experimental data suggest thatthrombolytic therapy may reduce infarct sizeindependently of reperfusion and,'3 '4 if thesame applies clinically, defibrination mayinfluence myocardial salvage directly; althoughwhether this contributed to the findings in ourstudy remains speculative.Although the level of defibrination as
measured by thrombin time correlated withresidual stenosis and left ventricular ejectionfraction, plasma fibrinogen itself correlatedonly weakly with these variables, and not at allwhen patients with non-patency of the infarctrelated artery were excluded from the analysis.This may reflect the relative inaccuracy of the
174
on July 12, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.68.8.171 on 1 A
ugust 1992. Dow
nloaded from

Defibrination after streptokinase
Clauss method,8 which, although widely usedfor assessment of fibrinogen responses tothrombolytic therapy,'13 may give falsely lowvalues if fibrin degradation products arepresent. Indeed, there has been some inconsis-tency about the value of fibrinogen assay by thismethod for assessing responses to thrombolytictherapy and at least one group of investigatorshas reported no relation with coronarypatency.3 It is perhaps not surprising,therefore, that when defibrination wasmeasured by plasma fibrinogen, it failed tocorrelate with residual stenosis because thiswould demand of the assay a level of accuracybeyond that required for an all or none predic-tion of patency. Thrombin time, on the otherhand, measures the functional integrity ofcirculating fibrinogen and is not affected byfibrin degradation products. Probably for thisreason it provided a better test of the throm-bolytic efficacy of streptokinase in our study.
It was our specific purpose to evaluatelaboratory measurements of defibrination earlyafter thrombolytic therapy for predictingcoronary patency and left ventricular fractionat discharge from hospital when decisionsabout further management are usually made.Thus angiography was delayed from three tonine days when recovery from the acute phaseof infarction was complete. Even at this fairlylate stage, however, reversible myocardialstunning continues to make a variable con-tribution to alterations in ejection fraction.'5Moreover, any time delay between treatmentand angiography is associated with continuedremodelling of the lesion within the infarctrelated artery, driven partly by the ongoinglytic effects of treatment, and partly byendogenous mechanisms.'0 Taken togetherthese factors may have blunted the predictivevalue of our measurements by weakeningcorrelations between defibrination and theangiographic data. Indeed, the fact that throm-bin time one hour after streptokinase infusionremained significantly related to both residualstenosis and ejection fraction about a week laterconfirms the potential value of this test formonitoring responses to treatment.The potential benefits of exaggerated
defibrination must be set against the risk ofbleeding, which affected two patients in ourstudy. Fibrinogen degradation products havecomplex adverse effects on haemostasis,'6 and itis noteworthy that both patients with bleedingcomplications had high baseline fibrinogen con-centrations that declined by 96% in response tostreptokinase infusion. This may well havecontributed towards their tendency to hae-morrhage although in general the magnitude ofsystemic defibrination and its laboratory de-rangements have not been shown to correlatewith bleeding.'718 Thus neither patient whobled had prolongation of the thrombin timebeyond 40 seconds indicating that this par-ticular measure of defibrination may not helpidentify patients at risk.
The findings in this study may have implica-tions for clinical practice. Thus whereas someprevious investigators have found that fibrin-ogen depletion encourages coronary patencyafter thrombolytic therapy'2 our studyindicates that the more exaggerated the de-fibrination, the greater the coronary patencyand the better the preservation of ventricularejection fraction at the time of discharge fromhospital. Simple measurement of thrombintime one hour after treatment seems par-ticularly useful for assessing responses to treat-ment, values above 49 seconds being associatedwith the best angiographic results.
1 Lew AS, Cercek B, Hod H, Shah PK, Ganz W. Usefulness ofresidual plasma fibrinogen after intravenous streptokinasefor predicting delay or failure of reperfusion in acutemyocardial infarction. Am J Cardiol 1986;58:680-5.
2 Brugemann J, Van der Meer J, Takens BH, Hillege H, LieKI. A systemic non-lytic state and local thrombolyticfailure of anistreplase (anisoylated plasminogen strepto-kinase activator complex, APSAC) in acute myocardialinfarction. Br Heart J 1990;64:355-8.
3 White CW, Schwartz JL, Ferguson DW, Brayden CW,Kelly KJ, Kioschos JM, et al. Systemic markers offibrinolysis after unsuccessful intracoronary streptokinasethrombolysis for acute myocardial infarction: does non-reperfusion indicate failure to achieve a systemic lyticstate? Am J Cardiol 1984;54:712-7.
4 Kennedy JW, Ritchie JL, Davis KB, Stadius ML, MaynardC, Fritz JK. The Western Washington randomized trial ofintracoronary streptokinase in acute myocardial infarc-tion: a 12 month follow-up report. N Engl J Med1985;312: 1073-8.
5 Risk stratification and survival after myocardial infarction:The Multicenter Postinfarction Research Group. N EnglJMed 1983;309:331-6.
6 Mukharji J, Rude RE, PooleWK, Gustafson N, Thomas LJ,Strauss HW, et al. Risk factors for sudden death afteracute myocardial infarction; two-year follow-up. Am JCardiol 1984;54:31-6.
7 Shafer KE, Santoro SA, Sobel BE, Jaffe AS. Monitoringactivity of fibrinolytic agents: a therapeutic challenge. AmJ Med 1984;76:879-86.
8 Clauss A. Gerinnungsphysiologische Schnellmethode zurBestimmung des Fibrinogens. Acta Haematol 1957;17:237-46.
9 Chesebro JH, Knatterud G, Roberts R, Borer J, Cohen LS,Dalen J, et al. Thrombolysis in myocardial infarction(TIMI) trial, phase 1: a comparison between intravenoustissue plasminogen activator and intravenous strepto-kinase. Circulation 1987;76:142-54.
10 Davies SW, Marchant B, Lyons JP, Timmis AD, RothmanMT, Layton CA, et al. Coronary lesion morphology inacute myocardial infarction: demonstration of earlyremodelling after streptokinase treatment. JAm CollCardiol 1990;16:1079-86.
11 Sandler H, Dodge HT. The use of single plane angio-cardiograms for the calculation of left ventricular volumein man. Am Heart J 1968;75:325-34.
12 O'Neill W, Timmis GC, Bourdillon PC, Lai P, Ganghadar-han V, Walton Jr J, et al. A prospective randomizedclinical trial of intracoronary streptokinase versus coron-ary angioplasty for acute myocardial infarction. N Engl JMed 1986;314:812-8.
13 Hochman JS, Choo H. Limitation of myocardial infarctexpansion by reperfusion independent of myocardialsalvage. Circulation 1987;75:299-306.
14 Chakrabarty S, Flores NA, Sheridan DJ. Can thrombolytictreatment produce beneficial effects in the absence ofcoronary recanalisation during acute myocardial infarc-tion? [abstract]. Br Heart J 1991;66:92.
15 Braunwald E, Kloner RA. The stunned myocardium: pro-longed postischemic ventricular dysfunction. Circulation1982;66:1 146-9.
16 Arnold AER, Brower RW, Collen D, Gerrit-Anne Van ES,Lubsen J, Serruys PW, et al. Increased serum levels offibrinogen degradation products due to treatment withrecombinant tissue-type plasminogen activator for acutemyocardial infarction are related to bleeding complica-tions, but not to coronary patency. JAm Coll Cardiol1989;14:581-8.
17 Bell WR, Meek AG. Guidelines for the use of thrombolyticagents. N Engl JMed 1979;301:1266-70.
18 Sharma GVRK, Cella G, Parisi AF, Sasahara AA.Thrombolytic therapy. N Engl JMed 1982;306:1268-76.
175
on July 12, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.68.8.171 on 1 A
ugust 1992. Dow
nloaded from