
Breakthrough medicines targeting the growing global medicines targeting the growing global health...
29
Breakthrough medicines targeting the growing global health threat of antibiotic resistance Jefferies Healthcare Conference June 2017 June 2017
Transcript of Breakthrough medicines targeting the growing global medicines targeting the growing global health...

Breakthrough medicines targeting the growing global health threat of antibiotic resistance
Jefferies Healthcare Conference
June 2017
June 2017

2
Our Mission
To build an enduring biopharmaceutical company focused on medicines that target the growing global threat of drug-resistant
bacterial infections affecting millions of people worldwide

3
Building an enduring antibacterial company
• Multi-product, Gram-negative infectious disease discovery and development company, with 2 clinical-stage assets and a 3rd entering the clinic by 1Q 2018
• Highly-differentiated products targeting drug resistant pathogens with high medical need and significant revenue potential
• All products wholly-owned
• Discovery engine capable of delivering continued pipeline
• Experienced team with deep expertise in antibiotic discovery and development

4
7%
20%
27%30%
34%
9%
23%
44% 43%
50%
13%
17%20%
25%
20%
0%
10%
20%
30%
40%
50%
60%
2000 2005 2010 2012 2014
Fluoroquinolone-resistant E. coli
Carbapenem-resistant A. baumannii
Carbapenem-resistant P. aeruginosa
Resistance trends in Gram-negative bacteria5
Increasing drug resistance results in large unmet need….
• U.S.: 2 MM drug-resistant infections/year1
– >23,000 direct deaths1
• High mortality and morbidity
– CRE (carbapenem resistant Enterobacteriaceae) 75% mortality2,3
– Acinetobacter baumannii mortality 43%4 and 63% multi-drug resistant (MDR)2,3
– 14%5 of Pseudomonas aeruginosa are MDR, occasional reports of resistance to last resort antibiotics4
• Resistance trends increase the urgency of the medical need
• Entasis pipeline aims to effectively address medical need caused by each of these Gram-negative pathogens
1 Antibiotic Resistance Threats in the Unites States, 2013; Centers for Disease Control2 Nat. Rev. Drug Discov. 12:963.3 Clin. Microbiol. 48:2271. 4 Expert Rev. Anti Infect. Ther. 10(8), 917-934 (2012)5 CDC Antibiotic Resistance Patient Safety ATLAS; Center for Disease Dynamics, Economics & Policy

5
Which has prompted a global call to action
• Non-dilutive funding for R&D– NIAID, BARDA, DARPA, CARB-X(US)– IMI (Europe)
• New regulatory pathways, accelerated approvals
• QIDP & fast track designations• Improved biological insights• Rapid molecular diagnostics
• Next generation antibiotics – Tailored to target key pathogens – Highly effective– Well tolerated– Priced to reflect value-add

6
Unique innovative platform sets foundation for repeated success
Structure-based Design
Novel TherapeuticsStructure-based Design
No Rx
After RxTreatment
0
24
1150
0
128
44,522
Nu
mb
er of
Map
ped
Read
s
Bacterial Genomics
Molecular Dynamics
Medicinal Chemistry
7
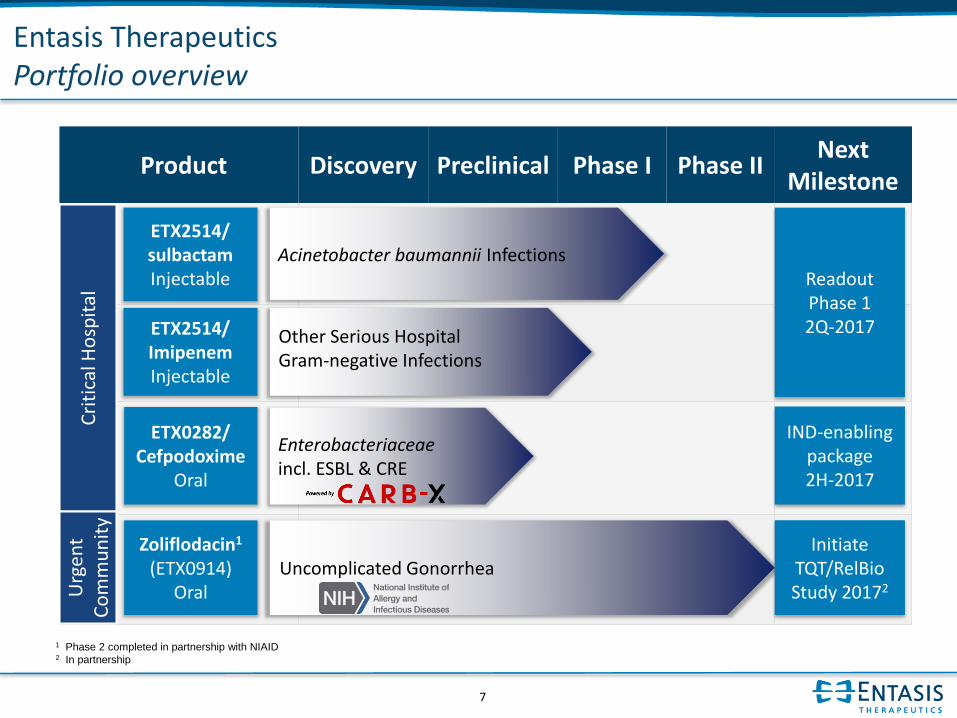
Entasis TherapeuticsPortfolio overview
Product Discovery Preclinical Phase I Phase IINext
Milestone
Uncomplicated Gonorrhea
Readout Phase 12Q-2017ETX2514/
ImipenemInjectable
Zoliflodacin1
(ETX0914)Oral
Initiate TQT/RelBio Study 20172
Acinetobacter baumannii Infections
Other Serious Hospital Gram-negative Infections
Cri
tica
l Ho
spit
alU
rgen
t C
om
mu
nit
y
ETX2514/sulbactamInjectable
ETX0282/ Cefpodoxime
Oral
IND-enabling package2H-2017
1 Phase 2 completed in partnership with NIAID2 In partnership
Enterobacteriaceaeincl. ESBL & CRE

8
Entasis TherapeuticsPortfolio overview
Product Discovery Preclinical Phase I Phase IINext
Milestone
Uncomplicated Gonorrhea
ETX2514/ ImipenemInjectable
Zoliflodacin1
(ETX0914)Oral
Initiate TQT/RelBio Study 20172
Acinetobacter baumannii Infections
Other Serious Hospital Gram-negative Infections
Cri
tica
l Ho
spit
alU
rgen
t C
om
mu
nit
y
ETX2514/sulbactamInjectable
1 Phase 2 completed in partnership with NIAID2 In partnership
ETX0282/ Cefpodoxime
Oral
IND-enabling package2H-2017
Readout Phase 12Q-2017
Enterobacteriaceaeincl. ESBL & CRE

9
What is a b-lactamase inhibitor (BLI)?
PBPs required
for bacterial cell
wall synthesis
BLs inactivate b-lactams
No inhibition of
cell wall synthesis
Bacterial growth
MDR
pathogen
BLI inhibits BLs,
b-lactam inhibits PBPs
Deadbacteria
b-lactamalone
b
b-lactam
+ BLI
b Inhibition of
cell wall synthesisb
b
b
b
b
b
b
b
b
b
b
b-lactamases (BLs)
expressed in periplasm

10
Emerging Threat
Entasis’ programs address unmet opportunity in b-lactamase inhibitors
Class C Class D Class B
b-lactamases
Metallo-enzymesSerine Enzymes
Originally marketed BLIs, generic
Major new opportunity Acinetobacter &
PseudomonasETX2514
KPCCarbapenemase
Class A

11
ETX2514 combinations offer the broadest spectrum Gram-negative coverage amongst leading competitors
ETX
25
14
+
Sulb
acta
m
ETX
25
14
+
imip
en
em
Avy
caz
(AZ/
All
erg
an)
Zerb
axa
(Me
rck)
Car
bav
ance
(Me
dC
o)
Erav
acyc
line
(Te
trap
has
e)
Imip
en
em
/ re
leb
acta
m(M
erc
k)
Pla
zom
icin
(Ah
cao
gen
)
S-6
49
26
6(S
hio
no
gi)
WC
K 5
99
9(W
ock
har
dt)
ESBL ExpressingEnterobacteriaceae +/- + + +/- + + + + + +
Carbapenem-Resistant Enterobacteriaceae
+/- + +/- - + + + + + +
Pseudomonas - ++ + ++ + - + - + -
Acinetobacter ++ +/- - - - +* - +/- +/- +/-
* Activity measured in vitro, concerns about plasma exposure in vivo
Source: Tetraphase Needham Investor presentation, Karen Bush “Has the Antibiotic Pipeline been Sufficiently Replenished?”.

12
Multi-Drug Resistant Acinetobacter baumannii is growing in prevalence and is associated with high mortality
• Between 60,000 and 100,000 infections per year in the US, ~100,000-140,000 per year in EU51
– forecast to grow over the next decade
• A. baumannii causes infections among critically ill patients. Mortality rates as high as 43%2
• Class D b-lactamases in A. baumannii are responsible for failure of many b-lactams3-5
• About 63% of A. baumannii isolates are MDR2
1. Decision Resources2. Am. J. Respir. Crit. Care Med. 2011.1409; Int. J. Antimicrob. Agents 2009.5753. M.M. Ehlers, et. Al. 2012. Prevalence of Carbapenemases in Acinetobacter baumannii, Antibiotic Resistant Bacteria – A Continuous Challenge in the New Millennium,
InTech, DOI: 10.5772/303794. Poirel, L. 2010. Diversity, Epidemiology & Genetics of Class D b-lactamases. AAC. 54: 24-38.5. Lancet 2008.751; J. Glob. Infect. Dis. 2010.291
A. baumannii

13
ETX2514+sulbactam for Acinetobacter baumannii infections
Drug Profile
• Novel I.V. antibiotic to treat serious A. baumannii infections• b-lactamase inhibitor with novel mode-of-action and expanded
spectrum, including Class D b-lactamases
Market Opportunity
• A. baumannii infections associated with high mortality• Resistance rates to one or more antibiotic >60%
Label / Indications
• Demonstrated or suspected A. baumannii infection• Multiple body sites • I.V. infusion q6h
Data to Date• Pre-clinical safety and DMPK complete• Extensive PK/PD to project clinical exposure and safety
Status • Phase 1 initiated October 2016
Next Steps • Readout Phase 1 2Q-2017, Phase 2 start 4Q-2017

14
ETX2514 + sulbactam: A novel combination against multi-drug resistant A. baumannii
• ETX2514 + sulbactam maintains excellent activity over time
• ETX2514 + sulbactam activity remains unchanged in carbapenem-resistant, colistin-resistant and multidrug resistant strains
MIC (mg/L) ≤0.06 0.12 0.25 0.5 1 2 4 8 16 32 >64
2011N=195
Cumul % 1 3.1 13.8 41.5 65.6 89.7 96.9 97.9 99.5 100 100
2012 N=209
Cumul % 0 0.5 2.9 20.1 46.9 79 98.6 100 100 100 100
2013N=207
Cumul % 0 0 4.3 15.9 43.4 73.8 96.5 97.5 99 99 100
2014N=1131
Cumul % 1 1.6 7.8 27.9 63.7 88.9 99.6 99.6 99.7 100 100
2015*N=202
Cumul % 0 1.0 7.4 43.1 78.7 97.0 99.5 99.5 100 100 100
MIC distributions for globally diverse A. baumannii clinical strains
*2015 study performed at JMI

15
ETX2514 + sulbactam exhibits excellent in vivo activity
Strong bacterial load suppression of XDR* A. baumannii infections at clinically relevant doses
7.40
9.40
8.408.03
6.636.19
4.854.61
4.19
2
3
4
5
6
7
8
9
10
Pre-treatment
Vehicle 2.5 /0.625
5 / 1.25 10 / 2.5 20 / 5 30 / 7.5 40 / 10 80 / 20
Log(
CFU
/g)
Lung
Stasis
sulbactam/ETX2514 (mg/kg) q3h
6.36
8.03 8.02
6.72
4.39 4.243.97 4.01 4.07
2
3
4
5
6
7
8
9
10
Pre-treatment
Vehicle 2.5 /0.625
5 / 1.25 10 / 2.5 20 / 5 30 / 7.5 40 / 10 80 / 20
Log(
CFU
/g)
Thigh
Stasis
sulbactam/ETX2514 (mg/kg) q3h
* Extensively drug resistant A. baumannii ARC3486 (OXA-72, OXA-66, TEM-1, AmpC) in neutropenic mice; MIC(sulbactam) ≥ 32 mg/L, MIC(sulbactam/ETX2514) = 0.5 mg/L
Human dose projected to be 500-1000mg/QID based on PK, efficacy and hollow fiber work

16
When combined with a carbapenem, ETX2514 has excellent microbiological potency against Pseudomonas
MIC50
(mg/L)MIC90
(mg/L)
CLSI Breakpoint
(mg/L)
1 16 2 (IPM)
0.25 1 2 (IPM)
0.5 16 8 (MEM)
0.25 8 8 (MEM)
Activity vs. 602 P. aeruginosa StrainsJMI 2013-2015
0%
20%
40%
60%
80%
100%
% S
us
ce
pti
ble
Str
ain
s
MIC (mg/L)
Imipenem (IPM)
IPM:ETX2514
Meropenem (MEM)
MEM:ETX2514
MIC90

17
ETX2514: Rapid and broad development strategy
• Currently in Phase 1– Compelling preclinical safety and toleration profile
– SAD, MAD, drug-drug interaction studies with multiple partners completed
– Data will be prepared for presentation at upcoming ID conference
• Phase 2 will be initiated by the end of 2017, pivotal trials in 2018
• Anticipate NDA filing against A. baumannii in 2020– Rapid path to licensure reflects high medical need
• Opportunity to expand label to additional pathogens/indications

18
Entasis TherapeuticsPortfolio overview
Product Discovery Preclinical Phase I Phase IINext
Milestone
Uncomplicated Gonorrhea
Readout Phase 12Q-2017ETX2514/
ImipenemInjectable
Zoliflodacin1
(ETX0914)Oral
Initiate TQT/RelBio Study 20172
Acinetobacter baumannii Infections
Other Serious Hospital Gram-negative Infections
Cri
tica
l Ho
spit
alU
rgen
t C
om
mu
nit
y
ETX2514/sulbactamInjectable
1 Phase 2 completed in partnership with NIAID2 In partnership
ETX0282/ Cefpodoxime
Oral
IND-enabling package2H-2017
Enterobacteriaceaeincl. ESBL & CRE

19
Emerging Threat
Entasis’ programs address unmet opportunity in b-lactamase inhibitors
Class C Class D Class B
b-lactamases
Metallo-enzymesSerine Enzymes
Originally marketed BLIs, generic
KPCCarbapenemase
Class A
I.V. Gram-(avibactam)Oral ETX0282

20
ETX0282 in combination with cefpodoxime addresses a significant unmet medical need
• MDR community urinary tract infections (UTIs) are a major concern in the medical community
• Category has been subject to an increase in resistance to SOCs (fluoroquinolones, TMP-SMX)*
• Uncomplicated UTI patients (typically treated in the community) require hospitalization for I.V. treatment when infected with MDR strains
• 95% of community UTIs are caused by Enterobacteriaceae, >75% by E. coli
Our vision: To create an oral agent for MDR Enterobacteriaceae (Class A and C)
• Outpatient setting (PCP or ER): Treatment for MDR cystitis, pyelonephritis patients who failed initial oral therapy (prevent hospitalization)
• Hospital setting: Oral step-down from IV - extend utility well beyond UTI (early discharge)
Urinary Tract
* Spellberg, B. & Y. Doi. The Rise of Fluoroquinolone-Resistant Escherichia coli in the Community: Scarier Than
We Thought. J Infect Dis. 2015. 212(12):1853-5..

21
• Combination of ETX0282 with cefpodoxime-proxetil (prodrug of cefpodoxime) has excellent microbiological potency– MIC90 ≤ 0.5 µg/ml against a panel of relevant Enterobacteriaceae clinical
isolates, including ESBL and CRE
• Favorable ADME, robust oral efficacy in neutropenic mouse thigh infection model– PK/PD requirements defined for projected clinical efficacy
• Excellent safety profile in non-GLP toxicology
ETX0282 with cefpodoxime is only oral BL/BLI combination with activity against ESBL and CRE bacteria

22
Our novel combination provides best-in-class coverage of contemporary clinical UTI isolates
Activity vs. ~900 global, diverse, ESBL-enriched Enterobacteriaceae isolates
(from UTI in 2013-2015)
MIC90
(mg/L)
CLSI Breakpoint
(mg/L)
Cefpodoxime (CPD) >32 2
ETX1317 32 ND
CPD/ETX1317 0.03 2 (CPD)
Levofloxacin 32 2
Piperacillin/tazobactam >32 16
Note: BLIs tested at a fixed concentration of 4 mg/L in combinations.
MIC90

23
ETX0282 delivers high bioavailability in preclinical species
Rat PK : Oral Bioavailability = 98% Dog PK : Oral Bioavailability = 97%
1
10
100
1000
10000
100000
0 5 10
Time, hr
1
10
100
1000
10000
100000
0 5 10 15
Co
nc,
ng/
mL
Time, hr
ETX0282 PO
ETX1317 IV
• Excellent bioavailability achieved in both rats and dogs
• PK profile similar to cefpodoxime proxetil

24
Entasis TherapeuticsPortfolio overview
Product Discovery Preclinical Phase I Phase IINext
Milestone
Uncomplicated Gonorrhea
Readout Phase 12Q-2017ETX2514/
ImipenemInjectable
Zoliflodacin1
(ETX0914)Oral
Initiate TQT/RelBio Study 20172
Acinetobacter baumannii Infections
Other Serious Hospital Gram-negative Infections
Cri
tica
l Ho
spit
alU
rgen
t C
om
mu
nit
y
ETX2514/sulbactamInjectable
1 Phase 2 completed in partnership with NIAID2 In partnership
ETX0282/ Cefpodoxime
Oral
IND-enabling package2H-2017
Enterobacteriaceaeincl. ESBL & CRE

25
Gonorrhea is an area of significant unmet need
• N. gonorrhoeae is an immediate public health threat
– Highly contagious with low rates of resistance sufficient to drive new treatment recommendations
– Resistance to cefixime (oral cephalosporin) >1%1; not recommended since 2012
– Resistance to ceftriaxone (injectable cephalosporin, current standard-of-care) is growing
– Cluster of MDR infections recently reported in Hawaii, but already an everyday reality in Europe and Asia
• In 2013, 333,000 cases of gonorrhea were reported, but CDC estimates that more than 820,000 cases occur annually in the U.S.3
1 CDC 2013 STD surveillance, susceptibility rates in the United States2 Cole MJ, et al. Euro surveill 2014;19(45) ; 3 Zheng H, et al. Japan J Infect Dis 2014;67:288-91; Hamasuna R, et al Japan J Infect Dis 203;19:571-8; Hamasuna R, et al. J Infect
Chemother 2015;21:1-6; CDC. STD Surveillance 2013.Atlanta, US Department of HHS 2014
http://www.cdc.gov/std/gisp2013/default.htm4 Includes oral cefixime and ceftriaxone
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
2009 2010 2011
China Japan Europe US
% of N. gonorrhoeae Isolates with Reduced Susceptibility to Extended-spectrum
Cephalosporins2,3,4

26
Zoliflodacin (ETX0914): Phase 2 POC
Open-label, multi-center, randomized
• NIAID sponsored
• 3 study arms (N=180 total patients with gonorrhea)– 2:2:1 ETX0914 2000mg or 3000mg once, or ceftriaxone 500mg I.M. once
– ETX0914 dosed as an oral suspension
Zoliflodacin has achieved POC
• Microbiological eradication and clinical cure in urogenital and anal infections comparable to high-dose ceftriaxone (100% at high dose)
• Potentially numerically slightly inferior in pharyngeal infections (4/6 and 7/9 respectively) but small numbers
• Generally well tolerated, no drug-related SAEs
Progression to Phase 3
• Relative bioavailability and TQT required prior to initiation of Phase 3
• Phase 3 initiation planned in 2H-2018

27
2017 2018 2019 2020
ETX2514End of Ph1
2Q2017
ETX2514Ph3-ready
2Q2018
ETX2514Ph3 start3Q2018
ETX2514DBL for NDA
1Q2020
ETX0282End of Ph1
4Q2018
ETX0282POC
1Q2020
ETX2514NDA filing3Q2020
zoliflodacinend of Phase 3
1H2020
ETX0282Ph1 start1Q2018
ETX25142nd Ph3 start
2H2019
ETX25142nd Ph3 DBL
2021
ETX2514Approval
2021
Project 4Ph1 start4Q2019
zoliflodacinApproval
2021
Multiple near-term value generating milestones
2021
zoliflodacinPh3 start2H2018
ETX0282Ph2 start1Q2019
ETX0282Ph3 start4Q2020
Project 4End of Ph1
4Q2020
ETX2514Ph2 start4Q2017

28
Building an enduring antibacterial company
Building value with a differentiated pipeline and favorable
clinical and regulatory strategy
Two clinical programs and a compelling preclinical pipeline
addressing critical unmet medical needs
Proven team and strong investors
Upcoming Milestones
ETX2514 ETX0282 Zoliflodacin
Phase 2 initiates 4Q2017 Phase 1 initiates 1Q2018 Initiate TQT/RelBio study in 2017*
* Dependent on partner funding.

29
Thank you
• Patients & volunteers, their families
• Study investigators for zoliflodacin & ETX2514
• Entasis employees and collaborators


















