The Brain The Brain _______ ___________ ______________ ___________.
Upload
rendy-santosoCategory
view
215download
2
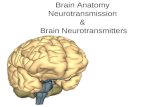
Brain Trauma
Fanny Indarto,dr.,Sp.B
Mechanisms
• Blunt and Penetrating Traumaoccurs from motor vehicle accidents, falls, assault, and
industrial accidents. Gunshot or missile wounds and stab wounds result in penetrating trauma.• Primary Brain Injury
Primary brain injury occurs at impact and is irreversible.• Secondary or Delayed Brain Injury
a result of several factors, including development of intracranial hematomas, contusions, cerebral edema, anoxia and other
metabolic abnormalities, hydrocephalus, infections, pneumocephalus, seizures, and so forth.
Secondary injury is often preventable and, in many cases, reversible.
Classification
• Mild: GCS of 14 to 15; loss of consciousness, if present, is brief (<5 minutes)
• Moderate GCS of 9 to 13• Severe: GCS of ≤8, which, by definition, is
coma

Glasgow Coma Scale
History• Mechanism of Injury
information on the speed at which the motor vehicle accident (MVA) occurred, vehicular damage, restraints, ejection from vehicle, assault weapon, type of missile or firearm, alcohol or substance use, and so on. • On-Scene Neurologic Examination
Information from emergency personnel must be obtained, when available. Loss of consciousness, changes in neurologic examination while en route to the ER, history of nausea or vomiting, side of the pupil to dilate first, and so on must be elicited.• Time Course of Events
Determine the possibility of multisystem trauma and so on.• Neurologic Symptoms
Consider any neurologic symptoms described by patient (headache, changes in vision, speech, hearing, motor strength or sensation, pain in neck or spine).• Alcohol or Substance Use

Examination• Vital signs• Dilated pupil• Level of Consciousness or Cognition (Glasgow Coma Scale)• Inspection• Cranial nerve exam• Pupil• Vision• Ocular movement• Facial motor and sensory functions• Hearing and equilibrium• Limbs• Spine
• A combination of hypertension, bradycardia, and respiratory irregularity (Cushing reflex) indicates transtentorial herniation.
• Hypotension is unlikely to result from head injury, except: neonates or infants who can lose significant proportion of total blood volume in an intracranial hemorrhage and adults with significant loss of blood from scalp injuries or associated spinal cord injury with neurogenic shock.
• Hypothermia needs to be treated because it will worsen coagulopathy and alter neurologic status.
• Unilateral or bilateral, a dilated pupil is a surgical emergency.
• lacerations or defects in scalp, periorbital ecchymoses (raccoon eyes), and retroauricular ecchymoses (Battle's sign) indicative of anterior cranial skull base and petrous temporal fractures
• Bleeding in the ear canals or cerebrospinal fluid (CSF) otorhinorrhea can also indicate skull fractures and increased risk of ascending infection.

Diagnostic studies
• Skull radiograph• Head CT scan• MRI• Cerebral angiogram• Nuclear cerebral perfusion studies

Management
• Head elevation• Avoid Hypothermia• Maintain Normovolemia• Nothing by Mouth• Orotracheal Intubation and Assisted Ventilation• Avoid Jugular Venous Compression• Serial Monitoring• Electrolytes, blood gasses, osmolality, serum levels of
antiepileptic drugs, and coagulation parameters must be monitored serially.
• Maintain Normotension
• Continuous Intracranial Pressure Monitoring• Steroids• Antiemetics and Mild Analgesics• Antiepileptic Treatment• Intravenous Mannitol• Hypertonic Saline• Short-Acting Sedatives and Paralytics• Hyperventilation
• Decompressive Surgery in Severe Refractory Intracranial Hypertension
• Pentobarbital Therapy


Subdural Hematomas
• which occurs in 20% to 40% of severely head-injured patients.
• This lesion originates in the space between the dura and arachnoidal meningeal layer on the surface of the brain and is a result of injury to the bridging veins and the brain parenchyma beneath it.
• As it layers on the surface of the brain it forms a crescent shape
• The morbidity of subdural hematomas is due to the rapid onset of mass effect as well as injury to the brain parenchyma beneath the subdural

Subdural hematoma
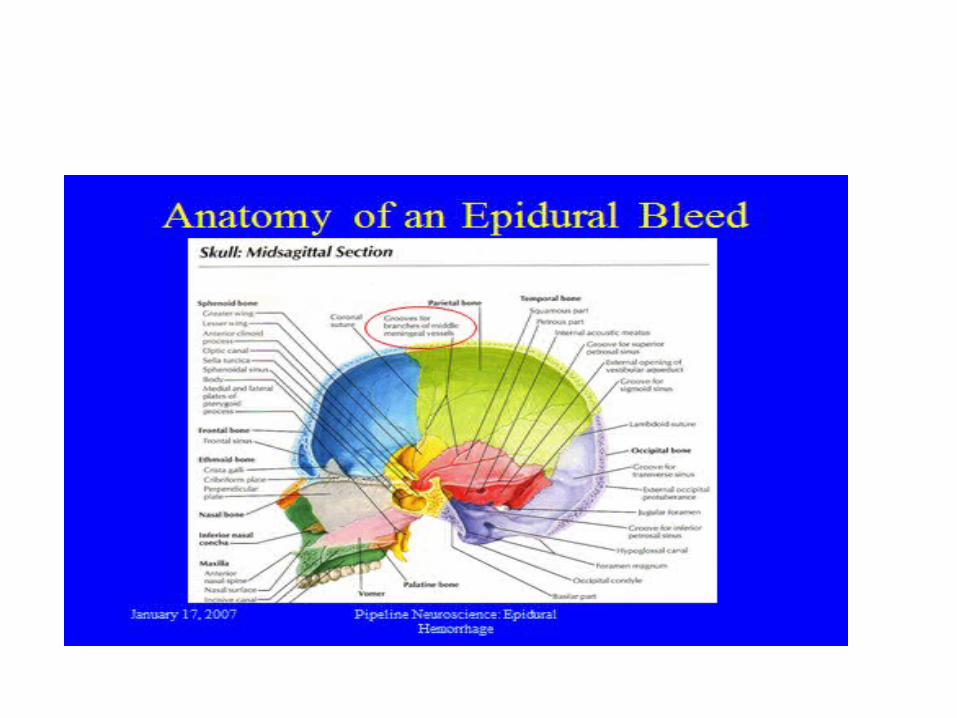
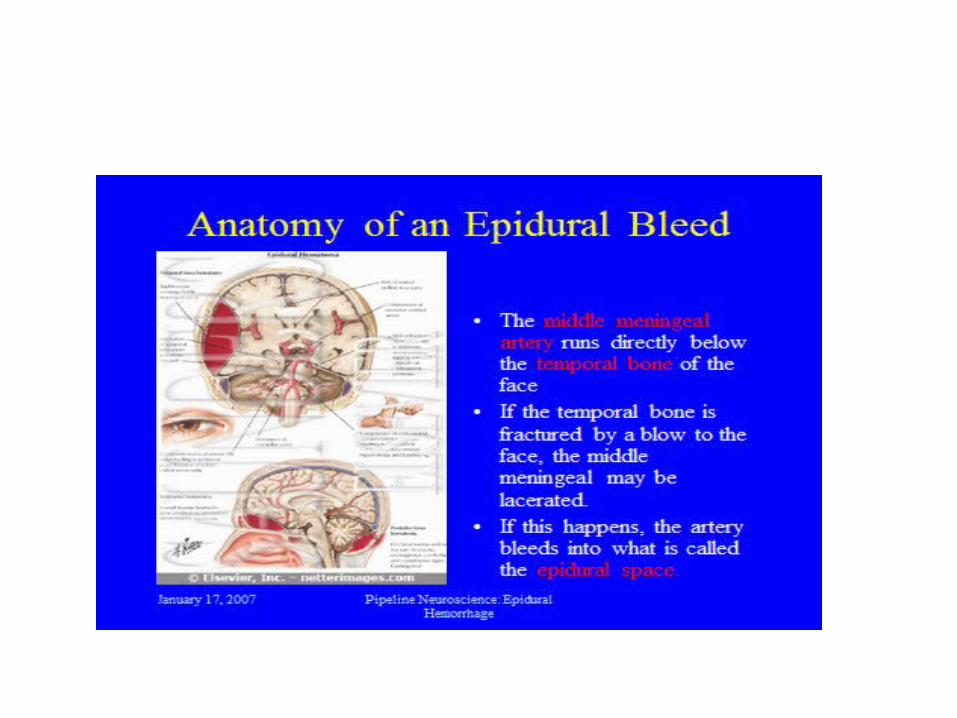
Epidural hematomas
• epidural hematomas have a lens shape, formed as the blood peels the dura back, creating a pocket of blood trapped between the inner table and the dura.
• caused by lacerations of the middle meningeal artery caused by fractures in the temporal bone, which is extremely thin and susceptible to fracture.
• can also be caused by lacerations to the dural sinuses or fractures through the diploic spaces, causing venous bleeding into the epidural space.
• Epidural hematomas are more the result of skull injury than of brain injury
• In fact, only about 1/3 of patients with epidural hematomas actually experience this “lucid interval” and it may also occur with other intracranial bleeds, making it an alarming but nonspecific finding.


Intracerebral Hematoma
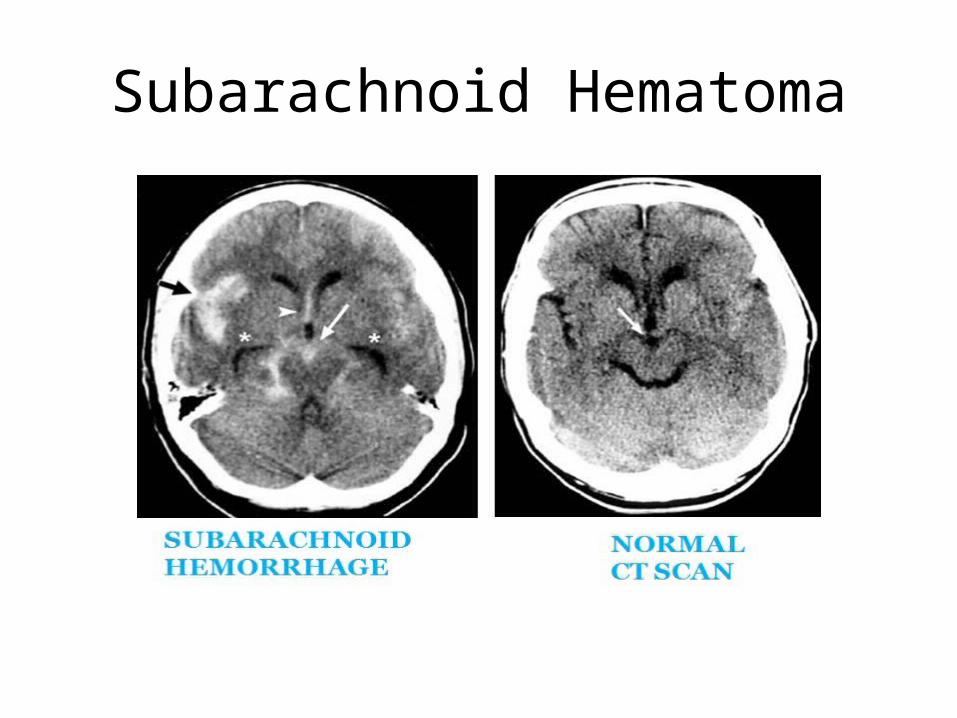
Subarachnoid Hematoma