bRAIN HEAMMORAGE
56
View with images and charts SUBARACHNOID HAEMORRHAGE -A BRIEF REVIEW INTRODUCTION Cerebrovascular diseases include some of the most common and devastating disorders: ischemic stroke, haemorrhagic stroke, and cerebrovascular anomalies such as intracranial aneurysms and arteriovenous malformations (AVMs). Most cerebrovascular diseases are manifest by the abrupt onset of a focal neurologic deficit, as if the patient was "struck by the hand of God" (Smith et al 2008). Between 5% and 10% of stroke are due to subarachnoid haemorrhage (Aminoff 2007). Subarachnoid haemorrhage typically presents with a sudden severe "thunder clap" headache (often occipital) which lasts for hours or even days, often accompanied by vomiting. There may be loss of consciousness at the onset, so subarachnoid haemorrhage should be considered if a patient is found comatose. Since 1 patient in 8 with a sudden severe headache has had a subarachnoid haemorrhage, clinical vigilance is necessary to avoid a missed diagnosis. All patients with a sudden severe headache require investigation to exclude a subarachnoid haemorrhage (Allen et al 2006). Forty five percent of patients die with in the first 30 days following subarachnoid haemorrhage, nearly two third die as a result of the initial haemorrhage and most within first two days (Parr et al 1996). Of those who survive more than half are left with major neurologic deficits as a result of the initial haemorrhage, cerebral vasospasm with infraction or hydrocephalus. If the patient survives but the aneurysm is not obliterated the annual rebleed rate is about 3% (Smith et al 2001). Despite vigorous therapeutic efforts, the mortality rate from subarachnoid haemorrhage remains high. So the major therapeutic emphasis is on preventing the predictable early complications of the rupture which in turn depends upon early diagnosis and prompt therapeutic intervention. A greater understanding of the basic mechanisms and pathology of subarachnoid haemorrhage may lead to more effective prevention
-
Upload
regan-ahmed -
Category
Documents
-
view
216 -
download
1
description
Â
Transcript of bRAIN HEAMMORAGE

View with images and charts
SUBARACHNOID HAEMORRHAGE-A BRIEF REVIEW
INTRODUCTION
Cerebrovascular diseases include some of the most common and devastating disorders: ischemic stroke, haemorrhagic stroke, and cerebrovascular anomalies such as intracranial aneurysms and arteriovenous malformations (AVMs). Most cerebrovascular diseases are manifest by the abrupt onset of a focal neurologic deficit, as if the patient was "struck by the hand of God" (Smith et al 2008).Between 5% and 10% of stroke are due to subarachnoid haemorrhage (Aminoff 2007). Subarachnoid haemorrhage typically presents with a sudden severe "thunder clap" headache (often occipital) which lasts for hours or even days, often accompanied by vomiting. There may be loss of consciousness at the onset, so subarachnoid haemorrhage should be considered if a patient is found comatose. Since 1 patient in 8 with a sudden severe headache has had a subarachnoid haemorrhage, clinical vigilance is necessary to avoid a missed diagnosis. All patients with a sudden severe headache require investigation to exclude a subarachnoid haemorrhage (Allen et al 2006).Forty five percent of patients die with in the first 30 days following subarachnoid haemorrhage, nearly two third die as a result of the initial haemorrhage and most within first two days (Parr et al 1996). Of those who survive more than half are left with major neurologic deficits as a result of the initial haemorrhage, cerebral vasospasm with infraction or hydrocephalus. If the patient survives but the aneurysm is not obliterated the annual rebleed rate is about 3% (Smith et al 2001).Despite vigorous therapeutic efforts, the mortality rate from subarachnoid haemorrhage remains high. So the major therapeutic emphasis is on preventing the predictable early complications of the rupture which in turn depends upon early diagnosis and prompt therapeutic intervention. A greater understanding of the basic mechanisms and pathology of subarachnoid haemorrhage may lead to more effective prevention and therapeutic strategies. Early diagnosis of subarachnoid haemorrhage requires good knowledge about clinical features and using necessary investigating tools at an earlier and appropriate time.
The aim of writing this review article on subarachnoid haemorrhage is to understand the details of subarachnoid haemorrhage including its pathophysiology, disease presentation, management of such patients and future thinking.
ARTERIES OF THE BRAIN (Snell 1997)
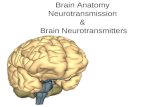
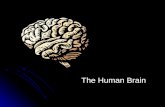
The brain is supplied by the two internal carotid and the two vertebral arteries (Fig.1). Four arteries remain within the subarachnoid space and their branches anatomies on the inferior surface of the brain to form the circle of Willis.

Fig.1. The arteries at the base of the brain. The right temporal pole and most of the right hemisphere of the cerebellum have been removed. Verifications in the pattern of these vessels are common. Source: Gray's anatomy (38th edn).
INTERNAL CAROTID ARTERY
Branches of the cerebral portion:1. The opthalmic artery: It supplies the eye and other orbital structures, frontal area of
the scalp, the ethmoid and frontal sinus and the dorsum of the nose.
2. Posterior communicating artery: It is a small vessel, forming part of the circle of Willis.
3. Choroidal artery: It is a small artery, ends in the choroid plexus also gives off small branches to crus cerebri, the lateral geniculate body, the optic tract, and the internal capsule.
4. Anterior cerebral artery: It is connected with it opposite anterior cerebral artery by anterior communicating artery, The cortical branches supply all the medial surface of the cerebral cortex as far back as the parieto-occipital sulcus. They also supply a strip of cortex about 1 inch wide on the adjoining lateral surface. A group of central branches supply parts of the lentiform, caudate nuclei and the internal capsule.
5. Middle cerebral artery: It is the largest branch of the internal carotid, cortical branches supply the entire lateral surface of the hemisphere, except for the narrow strip supplied by the anterior cerebral artery, the occipital pole, and the inferolateral

surface of the hemisphere which are supply by the posterior cerebral artery. Central branches supply the lentiform and caudate nuclei and the internal capsule.
VERTEBRAL ARTERY
The vertebral artery is a branch of the first part of the subclavian artery. It inters the skull through the foramen magnum. At the lower border of the pons, it joins the vessel of the opposite side to form the basilar artery.
Branches of the cranial portion:1. Meningial branches
2. Posterior spinal artery
3. Anterior spinal artery
4. Posterior inferior cerebellar artery: It supplies the inferior surface of the vermis. The central nuclei of the cerebellum and the under surface of the cereballar hemisphere, it also supplies the medulla oblongata and the choroid plexus of the fourth ventricle.
5. Medullary arteries are very small branches that are distributed to the medulla oblongata.
BASILAR ARTERY1. The pontine arteries are numerous small vessels that enter the substances of the
pons.
2. The labyrinthine artery.
3. The anterior inferior cereballar artery: It supplies the superior surface of the cerebellum. It also supplies the pons, the pineal gland and the superior medullary velum.
4. The superior cerebellar artery: It supplies the superior surface of the cerebellum. It also supplies the pons, the pineal gland, and the superior medullary velum.
5. Posterior cerebral artery: Cortical branches supply the infero-lateral and medial surfaces of the temporal lobe and the lateral and medial surfaces of the occipital lobe. Central branches pierce the brain substance and supply parts of the thalamus and the lentiform nucleus and the midbrain, the pineal and the medial geniculate bodies.
SUBARACHNOID SPACE
This is the space between the subarachnoid and the pia mater, which contains CSF and the larger arteries and veins which traverse the surface of the brain (Fig.2). Arteries and veins are coated by a thin layer of lepto-meninges. The pia and arachnoid mater are connects by collagenous trabecule and sheets. The piamater is reflected from the surface of the brain and pass along with vessels in the brain substance and disappear as the vessels become capillaries (Berry et al 1995).

Wherever the brain and the cranium are not close to each other, there is a wide interval between pia and arachnoid matter and form subarachnoid cisterns, like cerebellomedullary cistern, pontine cistern, interpeduncular cistern,cistern of lateral fossa etc. the interpeduncular cistern contains circle of Willis (Berry et al 1995).
The cerebrospinal fluid subarachnoid space is a modified tissue fluid and amount is about 150 ml. The cerebrospinal fluid gives buoyancy to the brain and protects the nervous tissue from mechanical forces applied to the skull. Inferiorly, the subarachnoid space extends beyond the lower end of the spinal cord and invests the cauda equina. The subarachnoid space ends below at the level of the interval between the second and third sacral vertebrae (Snell 1997).
Fig.2. Relationships of pia and arachnoid mater to the dura, brain and vessels. (modified from Alcolado et al 1988 according to Zhang, Inman & Weller 1990).Source: Grays' Anatomy (38th edn).
CIRCLE OF WILLIS
The circle of Willis lies in the interpeduncular fossa at the base of the brain. It extends from the superior border of the pons to the longitudinal fissure. It is formed by the anastomosis between the two internal carotid arteries and the two vertebral arteries. The anterior communicating, anterior carotid, posterior communicating, posterior cerebral, and basilar arteries all contribute to the circle. The circle of Willis allows blood that enters by either internal carotid or vertebral arteries lobe distributed to any part of both cerebral hemispheres (Snell 1997).
Two types of branches arise from the circle and its major branches; these are arbitrarily divided into cortical and central and they differ from each other in the extent of their anastomosis. The central branches are very numerous and slender; they tend to arise in groups and immediately pierce the surface of the brain to supply its internal parts. The largest collections of these pass through the anterior and posterior perforated substances. They do not anatomies to a significant extent within the brain substance. The cortical branches ramify over the surface of the cortex and anatomies fairly freely on the piameter. They give rise to numerous small branches which enter the cortex at right angles and like central branches, do not anatomies in it. It follows that blockage of an artery on the piameter may produce little if

any damage to the brain but damage to branches entering the substances of the brain leads to destruction of brain tissue (Romanes 1986).
The arteries of brain are liberally supplied by sympathetic nerves which run on to them from the carotid and vertebral plexuses. They are extremely sensitive to injury and readily react by passing into prolong spasm. This of itself may be sufficient to cause damage to brain tissue since even the least of neurons can not withstand absolute loss of blood supply for a period exceeding seven minutes (Romanes 1986).
Fig.3. Diagram of the arteries at the base of the brain, showing the constitution of the arterial circle. The arteries constituting this so called arterial 'circle' are commonly asymmetrical and sometimes a constituent vessel is missing. AL= anterolateral central branches; AM= anteromedial central branches; PL= posterolateral central branches;PM= posteromedial central branches. Source: Gray's Anatomy(38th edn)

CAUSES OF SUBARACHNOID HAEMORRHAGE
In 85% of cases of spontaneous SAH, the cause is rupture of a cerebral aneurysm—a weakness in the wall of one of the arteries in the brain that becomes enlarged. They tend to be located in the circle of Willis and its branches. While most cases of SAH are due to bleeding from small aneurysms, larger aneurysms (which are less common) are more likely to rupture (Van Gijn et al 2007).
In 15–20% of cases of spontaneous SAH, no aneurysm is detected on the first angiogram (Rinkel et al 1993). About half of these are attributed to non-aneurysmal perimesencephalic hemorrhage, in which the blood is limited to the subarachnoid spaces around the midbrain (i.e. mesencephalon). In these, the origin of the blood is uncertain (Van Gijn et al 2007).The remainder are due to other disorders affecting the blood vessels (such as arteriovenous malformations), disorders of the blood vessels in the spinal cord, and bleeding into various tumors (Van Gijn et al 2007). Cocaine abuse and sickle cell anemia (usually in children) and, rarely, anticoagulant therapy, problems with blood clotting and pituitary apoplexy can also result in SAH (Warrell et al 2003; Rinkel et al 1993).
INTRACRANIAL ANEURYSM
EPIDEMIOLOGY
The incidence and prevalence of unruptured intracranial aneurysms and aneurysmal SAH should be considered separately. Intracranial aneurysms are found on postmortem examination in between 1% and 6% of adults in large autopsy series (Schievink 1997). The frequency of intracranial aneurysm seen during angiography for patients not suspected of harboring an aneurysm is between 0.5% and 1.0%. The overall incidence of SAH from aneurysms is approximately 7-10 per 100,000 people per year (Menghini et al 1998), but this figure includes children, who have a very low incidence of rupture. The mean age of rupture is approximately 50 years. Among adults older than 30 years of age, the incidence of SAH is approximately 40-50 per 100,000 per year, and nearly one half of these individuals die from their SAH. Various reviews have noted a slight female predominance of SAH from aneurysms, with a mean age of haemorrhage of approximately 50 years. Ruptured aneurysms rarely occur in children, and there is a steady increase in the incidence of rupture from 0.3 per 10,000 persons per year between 25 and 34 years of age to 3.7 per 10,000 persons per year for patients 65 years of age or older.
A special category of patients are those who have a family history of aneurysms and SAH. Familial occurrence of intracranial aneurysms is defined by the presence of aneurysms in two or more first to third degree relatives without any known hereditary disease. It is not known whether the pathogenesis of familial intracranial aneurysms differs from that of the general population (Ronkainen et al 1998). In a community-based study from Rochester, MN, the relative risk of SAH among first-degree relatives of patients with the familial form of SAH was four times higher than the general population. Other studies have shown that in patients with familial intracranial aneurysms, there is a lower mean age at the time of rupture compared with SAH in the general population (Ronkainen et al 1998). Screening studies, with MRA, CT angiography, for the presence of aneurysms in this group of patients appears warranted.
ANEURYSM PATHOGENESIS AND CAUSE:

Several classifications of aneurysms have been proposed. This was suggested by Weir (1985). Morphology
SaccularFusiformDissecting
Size<3mm 3-6 mm 7-10 mm 11-25 mm >25 mm(giant)
Location (Ropper & Brown 2005)
Approximately 90 to 95 percent of saccular aneurysm lies on the anterior part of the circle of Willis. The four most common sites are 1. The proximal portions of the anterior communicating artery. 2. At the origin of the posterior communicating artery from the stem of the internal carotid, 3. At the first major bifurcation of the middle cerebral artery, and 4. At the bifurcation of the internal carotid into middle and anterior cerebral arteries.
Other sites include the internal carotid artery in the cavernous sinus, at the origin of the ophthalmic artery, the junction of the posterior communicating and posterior cerebral arteries, the bifurcation of the basilar artery, and the origins of the three cerebeller arteries. Aneurysms that rupture in the cavernous sinus may give rise to an arteriovenous fistula.
Fig.4. Common sites of berry aneurysms in the circle of WillisSource: Robin's Patholgy ( 6th edn.)

Saccular Aneurysms(Selman et al 2004)
Saccular, or berry, aneurysms are the most common form of aneurysms and are most often responsible for aneurysmal subarachnoid haemorrhage. Saccular aneurysms may arise from defects in the muscular layer of cerebral arteries that occur at vessel bifurcations and from degenerative changes that damage the internal elastic membrane, resulting in weakness of the vessel wall. They usually occur on the first or second order arterial branches of the vessel emanating from the circle of Willis. Evidence suggests that both genetic and environmental factors contribute to the development of saccular aneurysms. The evidence that genetic factors are important comes from the documented association of intracranial aneurysms with heritable connective tissue disorders such as autosomal dominant polycystic kidney disease, Ehlers-Danlos syndrome type IV, neurofibromatosis type 1, and Marfans syndrome. The familial occurrence of intracranial aneurysms also points to a role for genetic factors. In those patients who have a first degree relative with an aneurysmal SAH, the risk of a ruptured aneurysm is four times higher than the risk in the general population. A role for acquired factors in the pathogenesis of saccular aneurysm is suggested by the mean age of 50 for patients with aneurysmal SAH, and the increased incidence of haemorrhage occurring with age. Cigarette smoking is a risk factor in all population studies, and a role for systemic hypertension, although not as strong as that of cigarette smoking, in the cause of aneurysm formation appears likely.
Saccular aneurysms may also be caused by infection, trauma, or neoplasm. Mycotic aneurysms results from infected emboli that lodge in the arterial intima or the vasa vasorum and account for approximately 5% of all intracranial aneurysms. They occur most frequently in patients with subacute bacterial endocarditis, congenital heart disease, or a history of intravenous drug use, and are usually located on more distal branches of the cerebral vasculature. Proper management includes appropriate intravenous antibiotic therapy, with surgery in selected cases. Fungal aneurysms, which are much rarer than bacterial, usually are associated with arteritis and thrombosis and have been uniformly fatal.Traumatic aneurysms are rare but can be caused by either blunt or penetrating head injury. Such aneurysms occur at sites other than bifurcations. Angiograms are not routinely performed following head trauma, and these lesions may not be detected, but they should be considered in patients who suffer delayed deterioration. Early operative repair is recommended because of the high mortality associated with these lesions.
Neoplastic embolization, in rare cases, may produce an aneurysm in patients with choriocarcinoma, atrial myxoma, and undifferentiated carcinoma. In forming an aneurysm, the tumor embolus may remain viable, penetrate the endothelium, grow subintimally, and eventually destroy the arterial wall.
Morphology(girolami et al 1999)
An unruptured berry aneurysm is a thin-walled out pouching at arterial branch points along the circle of Willis or major vessels just beyond. Berry aneurysms measure a few mm to 2 to 3 cm and have a bright red, shiny surface and a thin translucent wall. Demonstration of the site of rupture requires careful dissection and removal of blood in the unfixed brain. Atheromatous plaques, calcification, or thrombotic occlusion of the sac may be found in the wall or lumen of the aneurysm. Brownish discoloration of the adjacent brain and meninges is evidence of prior haemorrhage. The neck of the aneurysm may be their wide or narrow. Rupture usually occurs at the apex of the sac with extravasation of blood into the

subarachnoid space, the substances of the brain, or both. The arterial wall adjacent to the neck of the aneurysm often shows some intimal thicking and gradual attenuation of the media as it approaches the neck. At the neck of the aneurysm, the muscular wall and intimal elastic lamina are usually absent or fragmented, and the wall of the sac is made up of thickened hyalinized intima. The adventitia covering the sac is continuous with that of the parent artery.
Fusiform Aneurysms(Selman et al 2004)
Fusiform or dolichoectatic aneurysms are classified separately from saccular aneurysms, although in some patients these types may overlap. The basilar artery is most commonly affected, although these aneurysms also can be seen in the anterior circulation. Only rarely are these lesions associated with SAH. Their presentation is characterized by cranial nerve or brainstem dysfunction secondary to direct compression or by embolization from intraluminal thrombus.
Dissecting Aneurysms(Selman et al 2004)
Dissecting aneurysms result from cystic medial necrosis or a traumatic tear in the endothelium and sub adjacent layers of the artery, allowing the formation of a false lumen. The false lumen may connect with the true lumen distally or may rupture through the remaining external arterial wall. Such aneurysms can occur in any portion of the extra cranial or intracranial arterial circulation. Trauma is a common cause in the neck and anterior circulation, but is a rare cause in the posterior circulation. Connective tissue diseases such as Marfans syndrome and other disorders such as fibromuscular dysplasia predispose to arterial dissections.
PATHOLOGY AND PATHOGENESIS OF SAH
At necropsy, subarachnoid haemorrhage is seen as a thin coating of blood in the subarachnoid space over the surface over the surface of the brain and as a rather thicker layer of blood around the ruptured aneurysm. The basal CSF cisterns are often filled with blood which can be visualized by CT scan. If bleeding is focal, it may indicate the location of an aneurysm but false localization may occur if haemorrhage is intraventricular and has leaked through the foramen of Luschka into the pontine cisterna around the basilar artery. Preliminary removal of fresh blood clot from around the circle of Willis may reveal the aneurysm or may facilitate dissection of the aneuryum in the fixed brain. If the blood clot around the aneurysm is allowed to harden by fixation the aneurysm may be difficult to locate or it may be damaged during the removal of the solidified blood clot (Sloam et al 1990).
In many cases of ruptured saccular aneurysm there is significant intraventricular or intracerebral haemorrhage. In a necropsy study of 133 patients with rupture saccular aneurysms ( Sloam et al 1990) intraventricular haemorrhage was observed in 40%, half of which are caused by rupture of an anterior communicating artery aneurysm either through the inferior medial portion of the frontal lobe or through the corpus collosum. Intracerebral haemorrhage was seen in 39% of cases caused by middle cerebral artery aneurysms in half of these (Sheffield & Weller 1980).
SAH can alter mechanisms that control cerebral blood flow and metabolism. Chemical control of blood flow by CO2 is altered in SAH patients (Graham 1990). Auto regulation is commonly lost after SAH. Because the degree of impairment of auto regulation may be different in different regions of the brain, a reduction in cerebral perfusion pressure may

cause extreme ischemia in some areas but not others. These changes in the intrinsic control of cerebral blood flow are particularly deleterious because several factors may operate to reduce cerebral blood flow after SAH, including decreased cerebral perfusion pressure from the raised intracranial pressure from the raised intracranial pressure caused by acute hydrocephalus or clot formation (Hirashima et al 1999).
Blood in the subarachnoid space triggers a pathological process that results in a spasm of the vessels of the major branches of the circle of Willis. Increased plasma platelet activating factor and antiphospholipids may contribute to the pathogenesis of cerebral vasospasm after SAH (Endo et al 1995). In Japan, there is a study at Tokayama, to evaluate the usefulness of measuring anti-phospholipid antibodies (aPLs) for the occurrence of symptomatic vasospasm and the outcome after SAH. They explained the association of antiphospholipids with worse outcome, aPLs were detected between 7 and 13 days after SAH. The mechanism of transient aPLs is unclear but it is more likely to occur in the severer grade patients. The reduction in platelet count, the increased platelet factor 4 concentration were also observed in aPLs-positive patients with symptomatic vasospasm (Endo et al 1995).
Delayed cerebral vasospasm that occurs after SAH seems to be associated with both impaired dilator and increased constrictor mechanisms in cerebral arteries. Mechanisms contributing arteries after SAH have been intensively investigated in recent years. Nitric oxide is produced by the endothelium and is an important regulator of cerebral vascular tone by tonic ally maintaining the vasculature in a dilated state. Endothelial injury after SAH may interfere with Nitric oxide (NO) production and lead to vasoconstriction and impaired responses to endothelium vasodilators (Sobey et al 1998).
Inactivation of NO by Oxyhaemoglobin or superoxide from erythrocytes may also occur in the subarachnoid space after SAH. Nitric oxide stimulates activity of soluble guanylate cyclase in vascular in vascular muscle leading generation of cGMP and relaxation. Subarachnoid haemorrhage appears to cause impaired activity of soluble granylate cyclase, resulting in reduced basal levels of cGMPin cerebral arteries to nitric oxide. Endothelin(ET) is a potent, long lasting vasoconstrictor that may contribute to the spasm of cerebral arteries after SAH. Endothelin is present in increased levels in the cerebrospinal fluid of SAH patients. Pharmacological inhibition of ET synthesis or ET receptors has been reported to attenuate cerebral vasospasm. Production of and vasoconstriction by Endothelin may be due, in part, to the decreased activity of Nitric oxide and formation of cGMP (Sobey et al 1998).
Protine kinase C (PKC) is an important enzyme involved in the contraction of vascular muscle in response to several agonists, including ET, activity of the PKC appears to be increased in the cerebral arteries after SAH indicating that PKC may be critical in the development of cerebral vasospasm. Recent evidence suggests that PKC activation may occur in cerebral arteries after SAH as a result of decreased negative feedback influence of NO/cGMP. Cerebral arteries are depolarize after SAH, possibly due to decreased activity of potassium channels may be due to several mechanisms, including impaired activity of Nitric oxide (and/or cGMP) or increased activity of PKC. Thus endothelial damage and reduced activity of Nitric oxide may contribute cerebral vascular dysfunction after SAH (Sobey et al 1998).
Because cerebral blood flow is inversely proportional to the fourth power of the radius, small changes in vessel caliber can have profound effects. If regional flow falls below the critical thresholds for membrane integrity, ischemic edema formation and infraction can occur. Focal

regions of edema can further impair local blood flow despite on overall normal intracranial pressure. AVP (Arginine vasopressin) plays an important role in the development of antidiuersis and disturbance of the brain water and electrolyte imbalance after SAH ( Laszi et al 1995).
CLINICAL SYNDROMES
UNRUPTURED ANEURYSMS
Most unruptured intracranial aneurysms are completely asymptomatic. Aneurysms may demonstrate evidence of their presence or of growth, before rupture, in other ways besides headache. Premonitory manifestations depend on the location of the aneurysm and include diplopia, visual field deficits, or facial pain (Weir 1994).
PHYSICAL FINDINGS
Because aneurysms can produce catastrophic haemorrhage before they reach a size that would produce neurological deficits, the lack of clinical findings should not preclude further diagnostic evaluation. The physical findings in patients with unruptured aneurysms are determined in part by the size and location of the aneurysm, although few aneurysms can be diagnosed with confidence on the basis of clinical presentation alone. Thus aneurysms arising from the anterior communicating artery can produce visual field defects, endocrine dysfunction, or localized frontal headache. Aneurysms of the internal carotid artery can produce oculomotor paresis, visual field deficits, impaired visual acuity, endocrine dysfunction, and localized facial pain. Aneurysms of the internal carotid artery in the cavernous sinus can produce a cavernous sinus syndrome when they reach a sufficient size. Those of the middle cerebral artery can produce aphasia, focal arm weakness, or paresthesias. Basilar bifurcation aneurysm can be associated with oculomotor paresis, although the clinical features of posterior circulation aneurysms seldom permit diagnosis before they rupture (Selman et al 2004).
RUPTURED SACCULAR ANEURYSMS
With rupture of the aneurysm, blood under high pressure is forced into the subarachnoid space (usually in relation to the circle of Willis), and the resulting clinical events assume one of the three patterns:(1) The patient is stricken with an excruciating generalized headache and vomiting and falls unconscious almost immediately; (2) Headache develops in the same manner but the patient remains relatively lucid- the most common syndrome;(3) Rarely consciousness is lost quickly without any preceding complaint. Decerebrate rigidity and brief clonic jerking of the limbs may occur at the onset of the haemorrhage, in association with unconsciousness. If the haemorrhage is massive, death may ensue in a matter of minutes or hours, so that ruptured aneurysm must be considered in the differential diagnosis of sudden death. A considerable proportion of such patients probably never reach a hospital. Persistent deep coma is accompanied by irregular respirations, attacks of extensor rigidity, and finally respiratory arrest and circulatory collapse. In these rapidly fatal cases, the subarachnoid blood has greatly increased the intracranial pressure to a level that approaches arterial pressure and caused a marked reduction in cerebral perfusion. In some instances the

haemorrhage has dissected intracerebrally and entered the ventricular system (Ropper & Brown 2005).
Ruptured of the aneurysm usually occurs while the patient is active rather during sleep, and in a few instances during sexual intercourse, straining at stool, lifting heavy objects, or other sustained exertion. Momentary valsalva maneuvers, as in coughing or sneezing, have generally not caused aneurysmal rupture. In patients who survive the initial rupture, the most feared complication is rerupture, an event that may occur at any time from minutes up to 2 or 3 weeks (Ropper & Brown 2005).
In less severe cases, consciousness, if lost, may be regained within a few minutes or hours, but a residuum of drowsiness, confusion, and amnesia accompanied by severe headache and stiff neck persists for several days. It is not uncommon for the drowsiness and confusion to last 10 days or longer. Since the haemorrhage is confined to the subarachnoid space, there are few if any focal neurologic signs. That is to say, gross lateralizing signs in the form of hemiplegia, hemiparesis, homonymous hemianopia, or aphasia are absent in the majority of cases. On occasion, a jet of blood emanating from an aneurysm may rupture into the adjacent brain or clot in the insular cistern and produce a hemiparesis or other focal syndrome. There may also be a focal syndrome from acute or delayed ischemia in the territory of the aneurysm-bearing artery. Usually this occurs several days after a large subarachnoid hemorrhage. The pathogenesis of such manifestations is not fully understood, but a transitory fall in pressure in the circulation distal to the aneurysm is postulated in early cases and vasospasm is responsible for the later focal signs. Transient deficits are not common, but they do constitute reliable indicators of the site of the ruptured aneurysm (Ropper & Brown 2005).
Convulsive seizures, usually brief and generalized, occur in 10 to 25 percent of cases according to Hart et al (but far less often in our experience) in relation to acute bleeding or rebleeding. These early seizures do not correlate with the location of the aneurysm and do not appear to alter the prognosis (Ropper & Brown 2005).
In most patients the neurologic manifestations do not point to the exact sight of the aneurysm, but it can often be inferred from the location of the main clot on CT scan. A collection of blood in the anterior interhemispheric fissure indicates rupture of an anterior communicating artery aneurysm; in the sylvian fissure, a middle cerebral artery aneurysm; in the anterior perimesencephalic cistern, a posterior communicating or distal basilar artery aneurysm; and so on. In some instances clinical signs provide clues to its localization, as follows:
Third nerve palsy (ptosis, diplopia, dilation of pupil, and divergent strabismus), as stated above, usually indicates an aneurysm at the junction of the posterior communicating artery and the internal carotid artery- the third nerve passes immediately lateral to this point;
Transient paresis of one or both of the lower limbs at the onset of the haemorrhage suggests an anterior communicating aneurysm that has interfered with the circulation in the anterior cerebral arteries;
Hemisparesis or aphasia points to an aneurysm at the first major bifurcation of the middle cerebral artery;
Unilateral blindness indicates an aneurysm lying anteromedially in the circle of Willis (at the origin of the ophthalmic artery or at the bifurcation of the internal carotid artery);
A state of retained consciousness with akinetic mutism or abulia (sometimes associated with paraparesis) favors a location on the anterior communicating

artery, with ischemia of or haemorrhage into one or both of the frontal lobes or hypothalamus (with or without acute hydrocephalus);
The side on which the aneurysm lies may be indicated by a unilateral preponderance of headache or preretinal haemorrhage, the occurrence of monocular pain, or, rarely, lateralization of an intracranial sound heard at the time of rupture of the aneurysm. Sixth nerve palsy, unilateral or bilateral, is usually attributable to raised intracranial pressure and is seldom of localizing value (Ropper & Brown 2005).
In summary, the clinical sequence of sudden severe headache, vomiting, collapse, relative preservation of consciousness with few or no laterlizing signs, and neck stiffness is diagnostic of subarachniod haemorrhage due to a ruptured saccular aneyrysm (Ropper & Brown 2005).The initial clinical manifestations of SAH can be graded using the Hunt-Hess or World Federation of Neurosurgical Societies classification schemes. For ruptured aneurysms, prognosis for good outcomes falls as the grade increases. For example it is unusual for a Hunt-Hess grade 1 patient to die if the aneurysm is treated, but the mortality for grade 4 and 5 patients may be high as 80%.
Table: Grading Scales for Subarchnoid Hemorrage (Hemphill & Smith 2008)
Grade Hunt-Hess Scale World Federation of Neurosurgical societies (WFNS) Scale
1 Mild headache, normal mental status, no cranial nerve or motor findings
Glasgow Coma Scale score 15, no motor deficits
2 Severe headache, normal mental status, may have cranial nerve deficit
GCS 13-14, no motor deficits
3 Somnolent, confused, may have cranial nerve or mild motor deficit
GCS 13-14, with motor deficits
4 Stupor, moderate to severe motor deficit, may have intermittent reflex posturing
GCS 7-12, with or without motor deficits
5 Coma, reflex posturing or flaccid GCS 3-6, with or without motor deficits
INVESTIGATIONSThe laboratory evaluation of patients suspected of having a rupture aneurysmal SAH uses a combination of CT scan, magnetic resonance imaging, lumber puncture and angiography.
CT Scan A CT scan will detect blood locally or diffusely in the subarachniod spaces or within the brain or ventricular system in more than 90 percent of cases (if within 48 hours of bleed) and in practically all cases in which the hemorrhage has been severe enough to cause momentary or persistent loss of consciousness. This should therefore be the initial investigative

procedure. The sooner the CT scan is performed in relation to the suspected hemorrhage the greater the likelihood of visualizing blood (Ropper & Brown 2005).
The blood may appear as a subtle shadow along the tentorium or in the sylvian or adjacent fissures. A large collection of subarachnoid blood or a hematoma in brain tissue or within the sylvian fissure indicates the adjacent location of the aneurysm and the likely region of subsequent vasospasm, as already noted. A high incidence of symptomatic vasospasm in the middle and anterior cerebral arteries has been found when early CT scan shows sudarachnoid clots larger than 5*3 mm in the basal cisterns or layers of blood more than 1 mm thick in the cerebral fissures. CT scan less reliably predicts vasospasm in the vertebral, basilar, or posterior cerebral arteries (Ropper & Brown 2005). Also, coexistent hydrocephalus will be demonstrable. If the CT scan documents subarachnoid blood with certainty, a spinal tap is not necessary.
In all other cases, where subarachnoid hemorrhage is suspected but not apparent on imaging studies or computed tomography is unavailable but the patient is oriented and obeying commands, a lumber puncture should be undertaken. Lumber puncture should not be performed in patients with papilloedema or focal neurological signs (Duffy 1982). Usually the CSF becomes grossly bloody within 30 min of the hemorrhage, with red blood cell counts up to 1 million/mm3 or even higher. With a relatively mild hemorrhage, there may be only a few thousand cells, but it is unlikely that a severe headache syndrome from subarachnoid hemorrhage would be associated with less than a several hundred cells. It is also probably not possible for an aneurysm to rupture entirely into the brain tissue without some leakage of blood into the subarachnoid fluid. In other words, the diagnosis of ruptured saccular aneurysm (by lumber puncture) is essentially excluded if blood is not present in the CSF. Xanthochromia is found after centrifugation if several hours or more have elapsed from the moment of the ictus. In a patient who reports a headache that is consistent with subarachnoid hemorrhage but the occurrence was several days earlier, the CT scan may be normal and xanthrochromia the only diagnostic finding. Also helpful after several days is the MRI taken with the FLAIR sequence, with will demonstrate blood (Ropper & Brown 2005).
Fig. 5. CT scan of the brain showing subarachnoid hemorrhage as a white area in the center

MRI Scan
Not routinely used, but in patients with multiple aneurysms, MRI performed several days after the bleed may provide greater sensitivity than CT in detecting small areas of subarachnoid clots and help determine the particular lesion responsible (Yadav et al 1998). Angiography
A rupture of an intracerebral haemorrhage due to hypertension, into the subarachnoid space or the ventricles may be difficult to distinguish from a subarachnoid haemorrhage occurring in a hypertensive patient and invading one cerebral hemisphere. When the diagnosis of subarachnoid haemorrhage has been confirmed by CT scan or examination of cerebral fluid, therefore, it is necessary to exclude a ruptured aneurysm or a bleeding angioma as its cause. This may call for angiography, which raises the question of whether this should be done in every case, and if so when (Yadav et al 1998).
There is a difference of opinion about this, some surgeons recommending that carotid angiography should be performed in every case of subarachnoid haemorrhage as soon as the diagnosis is made while others are more selective. The rational answer seems to be that if there is possibility that a life saving operation may be carried out as the result of information yielded by angiography, angiography should be performed. If on the hand this is not the case because it is thought that the patient is too ill to stand operation or that either angiography or the operation is fraught with greater risks than expected treatment. As may be the case particularly in patients over the age of 60 with evident atheroma, angiography should be postponed. There is no doubt, however, that surgery carried out sufficient early may save lives which would otherwise be lost (Pathirana et al 1994).
Angiography is usually carried out at the earliest convenience, although in patients in poor clinical condition, the clinician may prefer to delay investigation until improvement has occurred. If a patient deteriorates from the mass effect of an intracranial haematoma, then emergency angiography is required prior to any decompressive operation .Four vessels angiography is usually performed in all patients. Anterior-posterior, lateral and oblique views are requires for each vessel. Carotid angiography may show not only the site, size and shape of the aneurysm but also whether as sometimes happens there is an associated spasm of important arteries which may be contributing to the clinical picture (Lindsay et al 1997).
Magnetic resonance angiography
Magnetic resonance angiography is a useful non-invasive technique for demonstrating intracranial aneurysms but the resolution is still insufficient to ensure that small aneurysms are not missed.
MRA is less sensitive than conventional arteriography to visualize anomalies (Anzalone 1995). MRA is not sensitive enough to serve as a screening procedure after SAH. It can be used however to detect unruptured aneurysms in selected patients (Brust 1995).
Negative angiography

Angiography fails to reveal a source of the subarachnoid haemorrhage in approximately 20% of patients. In the presence of arterial spasm, reduction in flow may prevent the demonstration of an aneurysm and repeat angiography may be required at a later date (Jose et al 1996).Four vessels angiography confirms the presence of an AVM and delineates the feeding and draining vessels. Reasonably small AVMs are difficult to detect and only early venous filling may draw attention to their presence. In the presence of a haematoma, angiography should be delayed until the haematoma resolves, otherwise local pressure may mask demonstration of AVM. If the angiogram is subsequently negative, then MRI is required to exclude the presence of a cavernous malformation (Lindsay et al 1997).Transcranial droppler ultrasound assessment of proximal middle, anterior and posterior cerebral and basilar artery flow is helpful in detecting the onset of vasospasm, even prior to symptoms and following its course and response to therapy (Donald et al 2001).Skull radiographs sometimes reveal calcification in the AVM or increased vascular markings in the overlying bone (Brust 1995).
Associated Systemic Changes
Acute subarachnoid haemorrhage is associated with several characteristic responses in the systemic circulation, water balance, and cardiac function. The ECG changes include symmetrically large peaked T waves and other alterations suggesting subendocardial ischemia. Also there is a tendency to develop hyponatremia; this abnormality and its relationship to intravascular volume depletion plays a key role in treatment. Albuminuria and glycosuria may be present for a few days. Rarely, diabetes insipidus occurs in the acute stages, but water retention or a natriuresis is more frequent. There may be a leukocytosis of 15,000 to 18,000 cells per cubic millimeter, but the sedimentation rate is usually normal (Ropper & Brown 2005).
COMPLICATIONS OF ANEURYSMAL SAH(Mohr et al 2004)
Intracranial complications:
1. Recurrent haemorrhage.2. Vasospasm- induced ischemic stroke.3. Hydrocephalus.4. Seizures.5. Brain edema.
Extra cranial complications:
1. Systemica. Arterial hypotension or hypertensionb. Electrolyte disturbances (hyponatremia, hypernatremia, hypokalemia)c. Cardiac (myocardial infraction, arrhythmia, congestive heart failure)
2. Pulmonary (neurogenic pulmonary edema, adult respiratory distress syndrome, atelectasis, pneumonia)
3. Gastrointestinal bleeding.
4. Sepsis5. Renal or hepatic dysfunction6. Venous thromboembolism

7. Bleeding disorders, including thrombocytopenia
Vasospasm (Ropper & Brown 2005)
Delayed hemiplegia and other focal deficits usually appear 3 to 12 days after rupture and rarely before or after this period. These delayed syndromes and the focal narrowing of a large artery or arteries, seen on angiography, are referred to as vasospasm. Fisher and coworkers(1975) have shown that spasm is most frequent in arteries surrounded by the largest collections of clotted subarachnoid blood. The vasospasm appears to be a direct effect of blood or some blood product, possibly hematin or a platelet product, on the adventitia of the artery. Areas of ischemic infraction in the territory of the vessel bearing the aneurysm, without thrombosis or other changes in the vessel, is the usual finding in such cases. These ischemic lesions are often multiple and occur with great frequency, according to Hijdra and associates (1986).
After a few days, arteries in chronic spasm undergo a series of morphologic changes. The smooth muscle cells of the media become necrotic, and the adventitia is infiltrated with neutrophilic leukocytes, mast cells, and red blood corpuscles, some of which have migrated to a subendothelial position (Chyatte and Sundt). These changes are caused by products of hemolyzed blood seeping inward from the pia-arachnoid into the muscularis of the artery (Ropper & Brown 2005).
The clinical features of cerebral vasospasm depend on the affected blood vessel but typically include a fluctuating hemiparesis or aphasia and increasing confusion that must be distinguished from the effects of hydrocephalus. In the past, an arteriogram was required to verify the diagnosis, although it is not often performed now because of the slight associated risk of worsening vascular spasm and the ease with which the condition can be visualized with MRA and spiral CT techniques. Transcranial Doppler measurements are an indirect and easier way of following, by observations of blood flow velocity, the caliber of the main vessels at the base of the brain. Almost all patients have a greatly increased velocity of blood flow in the affected vessel that can be detected by this method in the days after haemorrhage. However, progressive elevation of flow velocity in any vessel (especially if over 175 cm/s) suggests that focal vasospasm is occurring. There is a reasonable correlation between these findings and the radiographic appearance of vasospasm, but the clinical manifestations of ischemia depend on additional factors such as collateral blood supply and the cerebral perfusion pressure (Ropper & Brown 2005).
Recurrent Hemorrhage Recurrent hemorrhage is a feared complication of SAH because it is a leading cause of death or neurologic morbidity during the first 2 weeks after SAH (Roos et al 2000; Hillman et al 1998). The cumulative rate of rebleeding during the first 2 weeks after SAH is approximately 15% to 20% (Torner et al 1981). Torner and colleagues (1981) found that the period of greatest risk for rebleeding is the first 24 hours after the ictus; the risk peaked at approximately 4% during that time.
Several clinical features identify those patients at the highest risk for early rebleeding. The most important is the level of consciousness at admission; patient admitted in coma at the greatest risk. Rebleeding is also more common among older people, women, and people

whose systolic blood pressure exceeds 170 mm Hg. The results of the baseline CT do not predict recurrent hemorrhage.
Recurrent haemorrhage usually causes a sudden headache and a rapid change in neurologic condition, including a drop in consciousness. Extensor spasm s and posturing are important early signs. A "convulsion" that occurs immediately after SAH also can mark a recurrent haemorrhage (Hart et al 1981). However, rebleeding in a comatose patient may be overlooked. It may be manifested only by a sudden change in respiratory pattern or vital signs. Recurrent haemorrhage should be sought whenever a patient experiences a new headache or worsens neurologically (Mohr et al 2004).
The differential diagnosis of rebleeding are vasospasm-induced brain ischemia, subacute hydrocephalus, seizure, electrolyte imbalance, hypotension, hypoxia, medication effects, systemic complication etc. The diagnosis of rebleeding should not be solely on clinical features, because this approach leads to over diagnosis. Recurrent haemorrhage can be proved most easily by the detection of additional blood on CT scans (Mohr et al 2004).
HydrcephalusHydrocephalus is a common complication of SAH, resulting from the massive collections of blood that fill the ventricles, block the aqueduct of sylvius, or obstruct the fourth ventricle. Blood can fill the subarachnoid cisterns or coat the arachnoid villi (Mohr et al 2004).
Sheehan and associates (1999) reported that hydrocephalus developed in approximately one fourth of their patients during the acute treatment period. Hydrocephalus is more common among patients who, upon admission, have severe neurologic impairments or CT evidence of ventricular dilation or intraventricular haemorrhage. In addition, women, patients with preexisting hypertension, and patients with a history of alcohol abuse have higher rates of hydrocephalus (Sheehan et al 1999).
The hydrocephalus after SAH may be classified according to its time of appearance as (1) acute- appearing within 12 hours after aneurysmal rupture, (2) sub acute- developing a few days after the ictus, or (3) delayed- noted as ventricular dilation week to years later. Acute hydrocephalus is an important cause of increased intracranial pressure and coma. Sub acute hydrocephalus is a cause of a gradual decline in consciousness that can occur approximately 7 to 10 days after SAH. In this situation, intracranial pressure may be modestly elevated. Delayed hydrocephalus often manifests as a subacute dementia, gait apraxia, and bladder incontinence. In the setting, intracranial pressure often fluctuates and may not be consistently elevated (Mohr et al 2004).
Approximately 16% to 34% of patients have CT findings consistent with acute hydrocephalus. Some patients with ventricular enlargement may be asymptotic, but most have decreased consciousness. Symptoms of acute hydrocephalus in addition to decline in alertness are bilateral motor signs, miosis, and downward deviation of the eyes. Acute hydrocephalus predicts increased mortality and morbidity and is correlated with subsequent development of vasospasm and ischemic stroke (Mohr et al 2004).
MANAGEMENT OF SAH
Table 1. Factors Predicting Less Favorable Outcome after Subarachnoid Hemorrhage (Mohr et al 2004)

Clinical factors 1. Admitting level of consciousness( coma)2. Interval from subarachnoid haemorrhage(<3 days)3. Age(>65years)4. Prior unrecognized hemorrhage or warning leak5. Presence of local neurologic signs on admission6. Presence of severe co morbid disease or extraneural organ
involvementDiagnostic results
1. Hyponatremia or hypovolemia2. Abnormal CT scan
Local, thick, or diffuse collection of subarachnoid bloodIntracerebral or intraventricular blood
3. Mass effect4. Hydrocephalus5. Evidence of rebleeding detected by sequential CT scan6. Vasospasm detected by arteriography or by
transcranial Doppler ultrasonography 7. Aneurysm located on anterior cerebral or vertebrobasilar
arteries8. Size of aneurysm(>10mm)
ACUTE MANAGEMENT
The patient with recent SAH is critically ill and should be evaluated and treated urgently (Mayberg et al 1994; Wijdicks 1995). He or she should be transported rapidly to a medical center that has the expertise to treat a patient with a ruptured aneurysm. Acute, potentially life-threatening complications should be anticipated. Personnel should assess the patient quickly and should measure vital signs and assess neurologic status frequently. The heart rate and rhythm should be monitored. The airway, breathing, and circulation should be supported, and if necessary, supplemental oxygen, endotracheal intubation, or ventilatory assistance should be given (Wijdicks 1995). Intravenous access is established to expedite emergency administration of medications. Normal saline can be given at a slow rate to maintain patency of the intravenous line. Unfortunately, the urgent approach to acute management of SAH is often suboptimal in emergency departments (Thomson et al 2000). Each institution should develop a protocol for the management of SAH in the emergency department, including plans for both acute treatment and urgent evaluation.
The initial evaluation should include CT scan, chest radiograph, electrocardiogram, and blood studies. CT can demonstrate subarachnoid blood and a number of other acute intracranial complications. When CT shows intracranial bleeding, a lumber puncture can be avoided. The findings of CT that is performed within 24 hours after onset of symptoms with the use of third-generation scanners are normal in approximately 2% to 7% of cases (Zouaoui 1997). If the CT findings are normal, a cerebrospinal fluid specimen should be obtained.
Patients should be admitted to a unit that has monitoring equipment and is staffed by neurologically trained nurses. Acute care can be divided into general supportive efforts and therapies aimed at preventing or controlling specific complications (Mayberg et al 1994; Wijdicks 1995). For the first 24 hours, blood pressure, vital signs, and neurologic status should be assessed hourly. Thereafter, examinations can be spaced further apart in stable

patients. Cardiac monitoring and, if necessary, continuous intra-arterial or noninvasive blood pressure monitoring are extended for at least 24 to 48 hours after admission.
Forced bed rest is a traditional part of management. Visitors and external stimuli are restricted. Passive range-of-motion exercises and frequent turning are performed. A water mattress or an alternating- pressure pneumatic bed can reduce the risk of pressure sores and atelectasis. Patients are assisted with self-care activities, such as bathing and eating. Black and associates (1986) showed that external pneumatic calf compression stocking and devices reduce the incidence of deep vein thrombosis. The use of heparin as a prophylaxis against deep venous thrombosis is generally avoided until the ruptured aneurysm is treated.
Gentle pulmonary suctioning and nursing care are important for avoiding pneumonia. The value of absolute bed rest in preventing rebleeding was tested by the cooperative study of Intracranial Aneurysms and Subarachnoid Heamorrhage; the cumulative rate of rebleeding was 25% during the first 14 days after SAH (Nishioka 1981). In general, the prognosis of patients treated only with absolute bed rest now represents the natural history of SAH.
Because intravenously administered medications are often needed, a slow infusion of saline is continued. Alert patients are usually given a soft, high-fiber diet supplemented by stool softeners (Wijdicks 1995). Caffeinated beverages are avoided. Stuporous and comatose patients are not fed during the acute treatment period. If a seriously ill person is stable several days after SAH and the airway is secured, nasogastric feedings can be instituted.
SYMPTOMATIC TREATMENT
Patients with SAH are often confused or agitated as a result of brain injury, hydrocephalus, or increased intracranial pressure. Pain or nausea can also lead to irritability. Agitation raises the risk of rebleeding and aggravates increased intracranial pressure. Control of pain or nausea can calm an upset patient. Regular administration of diazepam or phenobarbital may be useful in providing sedation for agitated patients.
The headache of SAH is intense, and patients should receive ample doses of analgesics (Mayberg et al 1994; Wijdicks 1995). Most alert patients require a medication such as codeine, meperidine, or morphine. The agent is usually administered parenterally. These medications can be combined with acetaminophen, hydroxyzine hydrochloride, or promethazine. Some patients have photophobia; a quiet, dark environment can help relieve some of these conditions, which otherwise might worsen the head pain. Sedation and sleep might also help control pain. Aspirin affects platelet aggregation and prolongs the bleeding time; there is concern that aspirin might potentiate rebleeding.
Severe nausea and vomiting are common and important complaints, particularly during the first 24 hours after SAH. Nauseated patients should receive an antiemetic, such as ondansetron, trimethobenzamide, or prochlorperazine, to control these complaints.
ANTICONVULSANTS
Approximately 25% of patients have seizures, most of which occur within the first 24 hours (Hart et al 1981; Rhoney et al 2000; Sundaram et al 1986). Rhoney and colleagues (2000) reported that seizures were most common among patients with thick cisternal clots. Most seizures happen before the patient reaches the hospital. Hart and associates (1981) noted that

63% of the seizures happened at the time of aneurymal rupture. However, some of these 'seizures' may not be truly epileptic phenomena but may represent transient decerebrate posturing secondary to increased intracranial pressure (Hart et al 1981; Fisher 1975).
Although seizures occurring after hospitalization are uncommon, they can be associated with recurrent haemorrhage. Physicians prescribe anticonvulsants to patients who have experienced a seizure as part of SAH, but the prophylactic use of these agents in treatment of patients who have not had a seizure is controversial. The rationale for prophylactic of anticonvulsants is that a seizure is a dangerous event in a person with a recent SAH. Because of the low rate of seizures after admission, however, Hart and associates (1981) and sundaram and chow (1986) question the necessity for routine prescription of anticonvulsants to patients with recent SAH. However, regular use of phenytion or another parentrally administered anticonvulsant is recommended to reduce the likelihood of seizures. No trial has tested the value of anticonvulsants in management of patients with recent SAH. Pending such a trail, the decision to prescribe these medications is individualized. If a patient has had or is having convulsions, intravenous doses of anticonvulsants are given.
TREATMENT OF MYOCARDIAL ISCHEMIA AND CARDIAC ARRHYTHMIAS
Cardiac arrhythmias can be detected in almost all patients during the first few hours after SAH; in approximately 20% of cases, the arrhythmias can be severe or life-threatening (Di Pasquale et al 1988, Manninen et al 1995, Oppenheimer et al 1994, Randell et al 1999). Ventricular arrhythmias are a potential cause of sudden death after SAH. Di Pasquale and coworkers (1988) noted torsades de points in 3.8% of 132 patients with SAH who underwent Holter monitoring. Increased QT dispersion is a common electrocardiographic finding after SAH (Randell et al 1997).
Changes resembling those seen in acute myocardial ischemia can be noted in 25% to 80% of patients ( Zouaoui et al 1997, Gascon et al 1983). In fact, many people with SAH have secondary myocardial ischemia and left ventricular dysfunction (Sakka et al 1999, Yuki et al 1991). An elevation of the cardiac isoenzyme creatine kinase necrosis are found among patients who died of SAH even those without prior history of coronary artery disease. Abnormal left ventricular function is seen most commonly among patients with elevated creatine kinase levels. Severe left ventricular dysfunction after SAH may necessitate a delay in aneurysm surgery. In addition, the reduction of cardiac output after severe SAH might increase the risk of cerebral ischemia secondary to vasospasm.
Brouwers and associates (1995) correlated elevated plasma levels of norepinephrine with a poor outcome after SAH. The release of catecholamines by the posterior hypothalamus is key to the development of the cardiovascular complications of SAH. Presumably, the markedly elevated levels of norepinephrine lead to hypokalemia, systemic hypertensive effects, left ventricular strain, coronary artery vasospasm, a "stunned" myocardium, or cardiac toxicity(Oppenheimer et al 1995, Yuki et al 1991, Donaldson et al 2001). Administration of a B-blocking medication might reduce the number and severity of cardiac sequelae ( Hamann et al 1993, Neil-Dwyer et al 1978).
ANTIHYPERTENSIVE TREATMENT
Arterial hypertension is common in SAH, resulting from elevations of catecholamines and renin produced by hypothalamic disturbances(Neil-Dwyer et al 1980, Toftdahl et al 1995) .

Additionally, increased intracranial pressure can induce arterial hypertension as a means to maintain adequate cerebral perfusion pressure. Arterial hypertension also can be secondary to seizures, vomiting, agitation, or pain. In addition, the patient may have preexisting hypertension.
Hypertension after SAH has been found to correlate with increases in the risk of vasospasm and mortality (Toftdahl et al 1995). Arterial hypertension also puts patients at high risk for recurrent haemorrhage. Administration of antihypertensive agents is a traditional component of early medical management of SAH (Mayberg et al 1994, Wijdicks et al 1995). However, rapid or steep reductions in blood pressure might be dangerous. Patients with vasospasm or increased intracranial pressure may experience a drop in cerebral perfusion in conjunction with a decline in blood pressure; neurologic deterrioration can result. Some antihypertensive agents (nitroglycerin, sodium nitroprusside, fenoldopam) are potent cerebral vasodilators, and enlargement of the cerebrovascular bed secondary to their administration could further increase intracranial pressure.
The blood pressure often returns to normal after the patients with SAH is admitted to the hospital or when symptoms such as headache are treated; thus, aggressive antihypertensive therapy might be avoided in some cases. The levels of arterial hypertension that mandates treatment is not known. Patients with moderate hypertension (mean arterial blood pressure lower than 120 mm Hg) probably do not need to be treated. On the other hand, patients whose mean blood pressure is 120 mm Hg or higher or whose systolic blood pressure is higher than 180 mm Hg should receive medication. The goal should be to cautiously lower the blood pressure to levels normal for the patient and to avoid inducing hypertension.
Although alert patients with elevated blood pressures can receive oral medications, parenteral agents have the advantage of a prompt response. Antihypertensive agents that were used before SAH are usually continued, and they should not be stopped abruptly. Short-acting antihypertensive agents are desirable because of the rapid resolution of the unwanted effects of an excessive decline in blood pressure. Because patients are often dehydrated or hyponatremic, diuretics are avoided. B-blockers, calcium channel blockers, and angiotensin-converting enzyme inhibitors are the oral most commonly prescribed. Nimodipine or nicardipine may be useful antihypertensive agents in the patient with SAH.
The patient with a markedly elevated or unstable arterial blood pressure reading may require a continuous intravenous infusion of labetalol, sodium nitroprusside, or fenolopam. The rate of infusion is adjusted in response to blood pressure values. The dosage must be individuelized, because a patient may be very sensitive to a medication, and the resulting drop in blood pressure may exceed expectations. Doses required in patients with SAH can be lower than those required for other hypertensive emergencies.
MANAGEMENT OF ELECTROLYTE AND FLUID BALANCE
Disturbances in water and sodium balance occur in approximately one third of patients with SAH (Wijdicks et al 1985). These complications are most likely to develop in critically ill patients with large hemorrhages. Hyponatremia and volume depletion correlate with a poor prognosis and the subsequent development of hydrocephalus, vasospasm, and ischemic stroke (Wijdicks et al 1985). Severe hyponatremia can cause convulsions and is potential cause of coma.

The primary indication for rapid correction of hyponatremia is the development of seizures in a patient without neurologic disease, however, this indication becomes blurred in patients with recent SAH. In the past, hyponatremia after SAH was attributed to the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) and was treated with fluid restriction. It is now recognized, that a more common cause of hyponatremia in patients with SAH is cerebral salt wasting (CSW). The mechanism of water and sodium loss in CSW has been correlated with disturbances in levels of artial natriuretic peptide, brain natriuretic peptide, and c-type natriuretic peptide, as well as with direct neural effects of renal function (Harrigan 2001, Sviri et al 2000, Wijdicks 1997).
The key to diagnosis of this syndrome is the urinary excretion of large amounts of sodium and chloride at a time when the extracellular fluid volume is contracted. Declines in plasma volume, red blood cell mass, and total blood volume occur (Wijdicks et al 1985, Sato et al 1999) these findings are unlike those in SIADH, in which the patient is euvolemic or hypervolemic. In contrast to therapy for SIADH, the appropriate therapy for CSW is replacement of salt and water rather than fluid restriction. Assessment of volume status by means of careful recording of inputs and outputs to calculate sodium and chloride balance, daily body weights, or laboratory test results suggesting dehydration, such as elevated hematocrit or blood urea nitrogen-creatinine ratio, can be useful in choosing therapy ( Harrigan 2001, Carlotti et al 2001).
If the serum sodium concentration does not normalize despite a euvolemic status, modest fluid restriction or an infusion of a hyperosmolar solution containing sodium can be started. The serum sodium concentration should be corrected no more rapidly than 0.7mEq/hour to avoid central pontine myelinolysis (Harrigan 2001). In 39 patients with recent SAH, Wijdicks and associates(1988) administered 0.2 mg of fludrocortisone twice a day, combined with daily fluid intake of at least 3L, and noted improvements in plasma volume and sodium balance. As a result, these investigators recommend that frudrocortisone be added to the fluid management regimen if the serum concentration of sodium is less than 125 mmol/l. Hypokalemia after SAH probably results from vomiting but can be secondary to elevated levels of corticosteroids, renin, or catecholamines. Because cardiac arrhythmias can be associated with hypokalemia, this imbalance should be corrected promptly.
Treatment of other medical complications
Gastrointestinal bleeding can result from hemorrhage gastritis, tress gastric ulcers, or an esophageal tear secondary to vomiting. Because of the risk of bleeding, patients are often given intravenous histamine2-receptor antagonists or proton pump inhibitors via nasogastric tube (Mayberg et al 1994). Sucralfate does not have central nervous system side effects, so it has potential advantages in preventing gastrointestinal side effects among critically ill patients prone to depression in consciousness (Wijdicks 1988).
Obtunded patients are at high risk for adult respiratory distress syndrome, atelectasis, pulmonary hypoventilation, and aspiration pneumonia. Securing of the airway, careful bronchopulmonary management, and ventilatory assistance may be required. Events such as renal failure, hepatic dysfunction, and urinary tract infections as well as other illness should be treated. Measures to avoid pressure sores or orthopedic complications also are important.
Treatment of increased intracranial pressure

A decline in consciousness is the hallmark of increased intracranial pressure, which, in turn, can result from a large intracerebral or intraventricular hematoma, the mass effects of a secondary ischemic lesion, cerebral edema, or hydrocephalus. SAH also causes vasoparalysis and loss of autoregulation; secondary dilation of intracranial vessels might aggravate intracranial pressure by expanding the vascular compartment. Intracranial pressure is markedly elevated within a few minutes of aneurysmal rupture; the sudden increase in pressure may help halt the bleeding. In addition, the elevated intracranial pressure may transiently equal mean arterial blood pressure. A massive rise in intracranial pressure is probably one of the causes of sudden death after SAH. High intracranial pressure may also lead to hypoperfusion, which induces brain ischemia. Prompt aggressive treatment of increased intracranial pressure is one of the keys to successful management of SAH (Wijdicks 1995).
Several medical and surgical measures are available to treat brain edema or increased intracranial pressure. Continuous monitoring of intracranial pressure is indicated for many patients; the results might guide the timing of surgical or medical interventions. Continuous intraventricular drainage combined with monitoring is an option if the patient has intraventricular haemorrhage or acute hydrocephalus. Treatment of increased intracranial pressure consists of (1) elevation of the head of the bed to promote venous drainage, (2) fluid restriction, (3) correction of hyponatremia, (4) treatment of fever or agitation, and (5) prevention of hypoventilation and secondary hypercarbia.
Intubation and hyperventilation are indicated if a patient's condition is deteriorating. There is no evidence that dexamethasone is useful in managing brain edema after intracranial hemorrhage. Furosemide, which can reduce intracranial pressure by limiting the production of CSF, can be given in an emergency. However, the diuretic effects of furosemide can lead to electrolyte disturbances and hypovolemia. Mannitol is an osmotic agent that can be given to control increased intracranial pressure. A response is noted within minutes, and the duration of effect is approximately 4 to 6 hours. The dosage can be repeated as needed. Secondary dehydration, hyperosmolarity, and a rebound increase in brain edema are possible complications. Measurements of serum osmolality and serum electrolytes should be performed often, especially if repeated doses of mannitol are prescribed. Measurement of central venous or pulmonary artery wedge pressure might be needed. Hypertonic saline has also been used in refractory cases to lower intracranial pressure and has the advantage of expanding intravascular volume (Qureshi & Suarez 2000).
Management of hydrocephalus
A patient with acute hydrocephalus can be observed, medically managed, monitored with sequential CT studies, and treated with serial lumber punctures. Although acute hydrocephalus may resolve spontaneously, most cases require placement of a temporary ventriculocaval or ventriculoperitoneal catheter (Graff- Radford et al 1989; Heros 1989). Insertion of a ventricular catheter may be difficult in a patient with an intraventricular clot, because blood can occlude the catheter. Continuous cisternal drainage might relieve intracranial and expedite lavage of blood from the subarachnoid space. Placement of a shunt is recommended for any patient with depressed consciousness and enlarging ventricles. Shunting is not always effective.
PREVENTION OF RECURRENT HEMORRHAGE

Measures to ameliorate recurrent hemorrhage are not effective; therefore treatment is aimed at prevention. Choices include prolonged bed rest, induced hypotension, antifibrinolytic agents, carotid ligation, intracranial clipping of the aneurysm, and endovascular obliteration of the aneurysm. Occlusion of the aneurysm is the best method for preventing rebleeding (van Gjin & Rinkel 2001). Neither absolute bed rest nor induced hypotension has been successful in improving outcomes after SAH or in reducing the risk of recurrent haemorrhage. Carotid ligation can be performed to prevent rebleeding from aneurysms of the distal internal carotid artery, but because of the advances in intracranial operative techniques and development of invasive neuroradiologic procedures, carotid ligation now is rarely performed (Perret & Nibbelink 1981).
Antifibrinolytic therapy
The rationale for the use of antifibrinolytic agents (aminocaproic acidor tranexamic acid) is that the perianeurysmal clot that formed the initial haemorrhage abuts and supports the aneurysm, thus helping to prevent its re-rupture. Treatment would be given before surgery, to prevent rebleeding while the patient was recovering from the acute effects of SAH. Antifibrinolttic agents cross the blood brain barrier, but peak CSF levels of these agents are lower than plasma levels and are also delayed. When the agents are administered as a constant intravenous infusion, a steady state in CSF is reached only after 36 hours. Therefore, the possible therapeutic level of agent in the CSF may not be achieved during the period of highest risk for recurrent haemorrhage.
Clinicians are concerned about the safety of antifibrinolytic agents. A fulminant myopathy, rhabdomyolysis, or myoglobulinuria can complicate prolonged use of these medications (Brown et al 1983). Antifibrinilytic agents accentuate the development of hydrocephalus (Graff-Radford et al 1989). Ischemic stroke is the most feared side effects. The high rate of ischemic stroke is the primary reason that antifibrinolytic agents are not established as effective in the acute management of SAH (Vermeulen et al 1984).
INTRACRANIAL OPERATION
Surgery is an important component of management of SAH. Surgical repair involves placing a metal clip across the aneurysm neck, thereby immediately eliminating the risk of rebleeding. This approach requires craniotomy and brain retraction, which is associated with neurologic morbidity. Currently, surgery is the preferred treatment for the aneurysm, but the recommendation for surgery must still be made on a case-by-case basis. For example, the patient's age, the severity of neurologic injury, or the presence of a serious comorbid disease may weigh against an intracranial operation. Although people older than 60 years tolerate intracranial operation less well than younger people, age alone is not a reason for excluding surgery from the treatment regimen, because outcomes in the elderly have improved over time (Johansson et al 2001).
For most patients, the question is not whether the aneurysm should be clipped but, rather, when is the ideal time for the operation. Some neurosurgeons advocate delaying surgery until a patient's condition has stabilized (Maurice-williams et al 1997), but most neurosurgeons now favor early operation (Findlay 1997). Early operation is preferred because the risk of rebleeding is elimination and the operation is performed before vasospasm appears. The primary reason for delaying surgery has been that a lag permits the patient's condition to recover from the initial event before the patient is subjected to the stresses associated with

early surgery. Delayed surgery leaves the aneurysm untreated during the period of highest risk of rebleeding. In addition, the potential of recurrent rupture of an unsecured aneurysm can complicate hypervolumic hemodilution and induced hypertension for treatment of ischemia secondary to vasospasm. Surgeons rightfully point out that the overall results of management, and not just postoperative statistics, should be compared. The overall results of early medical treatment followed by a delayed operation are not satisfactory.
Several groups described favorable results of early operation combined with a variety of interventions, including calcium channel blockers (Juvela et l989, LeRoux et al1995, Nishimoto et al 1985). A small trial in Finland, demonstrated better outcomes for early operation (Ohman and Heiskanen 1989). Although the data favored early operation, the results were distorted by a simultaneous random assignment of patients to receive either placebo or active treatment with calcium channel blocking agents. Miyaoka and associates (1993) reported better management results with early surgery in patients who were in good condition and better results with delayed operation in patients who were seriously ill. A large international epidemiologic study evaluated outcomes of 3521 patients hospitalized within 3 calendar days of SAH (Kassellet al 1990). Although it was not a randomized trial, the large numbers assured that prognostic factors were similar in the groups that underwent early and delayed operations. Overall management results (favorable outcomes) were similar in the two treatment groups, but early surgery did reduce the overall risk of rebleeding. Early surgery was not associated with a high rate of intraoperative complication, such as a re-rupture of the aneurysm or worsening of brain edema.
ENDOVASCULAR TREATMENT
Endovascular obliteration of the aneurysm or the parent artery is used to treat aneurysms of the intracavernous or proximal portions of the internal carotid artery, even in patients who have a carotid-cavernous fistula. Tandem placement of balloons in the parent artery (trapping) can shrink the aneurysm or lead to its occlusion (Findlay 1997). This procedure is relatively effective, and the risk of ischemic stroke is low (Larson et al 1995). However, detachable balloons can be relatively difficult to place within the aneurysm. The sizes and shapes of the balloons might not correspond to the contour of the aneurysmal sac. Occasionally, the balloons can be lost and migrate into distal arteries. In addition, the balloons can deflate, and the aneurysm can become recanalized. Finally, the balloons might place pressure on the aneurysm's wall and promote recurrent rupture.
Endovascular placement of adhesive materials can be used to occlude smaller intracranial aneurysms. Kinugasa and associates(1995) reported success with the placement of cellulose acetate polymer for occlusion in 9 of 12 patients with aneurysms. Obliteration of the aneurysmal sac expedited treatment of vasospasm and allowed the patients to become stable before the aneurysm was surgically repaired.
Development of microcatheters and detachable coils has stimulated greater interest in direct endovascular treatment of intracranial aneurysms (McDougall 1996). Aneurysms that are not easily approached for direct clipping might be occluded with endovascular treatment (McDougall 1996, Casasco et al 1993, Sinson et al 1996). In particular, aneurysms of the posterior circulation and the basilar bifurcation can be treated with placement of coils (Birchall et al 2001). In one multicenter trail comprising 150 patients, basilar tip aneurysms were treated with detachable platinum coils; approximately 75% of the aneurysms were successfully treated (Eskridge & Song 1998). The periprocedural mortality rate was 2.7%.

Complications included rupture of the aneurysm and occlution of the parent artery. Cognard and colleagues (1998) treated 208 patients with aneurysms (150 with SAH), achieving total occlusion of the aneurysms in 81% of cases, and subtotal occlusion in 17%. In another study, 75 seriously ill patients with ruptured aneurysms were treated with coils (Raymond and Roy 1997). Success was achieved in most patients, although procedure-related mortality and morbidity occurred in 8% of cases. Lefkowtz and coworkers (1999) placed coils in wide-necked aneurysms in 23 patients; complete or nearly complete occlusion was achieved in all cases. Three patients had complications. Although the usefulness of endovascular placement of coils has not been compared with that of surgery, this therapy has gained popularity and likely will continue to increase in popularity in the future.
VASOSPASM AND ISCHEMIC STROKE
Removal of the subarachnoid clots
Early intracranial operation and lavage of the subarachnoid space can remove clots and might prevent development of vasospasm. The rationale for this procedure is that evacuation of the clots might prevent the release of substances that induce the arterial narrowing. Surgical removal of the clots can be difficult in critically ill patients, however, and some of the blood collects in areas far from the operative field. Extensive manipulation of the brain to remove the subarachnoid clots may also injure penetrating vessels, leading to ischemic deficits. Despite promising study did not show any reduction in the severity or incidence of vasospasm (Kassell et al 1990). It appears that vigorous lavage of the subarachnoid space is not a feasible way to prevent vasospasm in most patients.
Several small studies report the potential usefulness of intrathecal thrombolytic therapy in the setting of acute surgical treatment of a ruptured aneurysm (Brinker et al 1992, Mizoi et al 1993, Sasaki et al 1994, Usui et al 1994) . Most of these studies treated only patients judged to be at very high risk for vasospasm and ischemia. Outcomes were generally favorable, consisting of a lower frequency of severe vasospasm and ischemic impairments (Treggiari-Venzi et al 2001). Kodama and associates (2000) performed cisternal irrigation with urokinase and ascorbic acid in 217 high-risk patients, and observed subsequent symptomatic vasospasm in 6 patients. Thrombolytic agents can be instilled safely into the basal cisterns. Thrombolytic agents can be instilled safely into the basal cisterns. The risk of major bleeding complications, in particular brain haemorrhage, thrombolytic agents should not be administered until the aneurysm has been occluded. The optimal timing of treatment, the duration of treatment, the best agent, and the best dose are not known. Considerable research, including prospective controlled trials, is needed before intrathecal thrombolytic agents are added to the usual care of patients with recently ruptured aneurysms.
CALCIUM CHANNEL BLOCKING AGENTS
Influx of extracellular calcium, an important component in sustaining contraction of smooth muscle, is critical in the process of cellular ischemia. An agent that inhibits calcium entry might prevent vasospasm or its cerebral ischemic consequences. The diyhdropyridine derivatives nimodipine and nicardipine have been tested. Although these agents can reduce the arterial blood pressure, they also increase cerebral blood flow, including in ischemic regions. Small studies testing the utility of oral nimodipine found that the medication reduced mortality but it did not prevent vasospasm (Allen et al 1983, Ohman et al 1991). A British trail established the utility of nimodipine to improve outcomes after SAH (Pickard et al

1989). The rate of favorable outcome was increased from 67% to 80.2% with treatment. Meta-analyses confirm the efficacy of nimodipine in treating patients with recent SAH (Barker and Ogilvy 1996, Feigin et al 2000,Tettenborn and Dycka 1990). Although a significant reduction in mortality is not achieved, the calcium channel antagonists reduce the proportion of patients with ischemic deficits secondary to vasospasm.
In general, nimodipine is safe, and complications of its use are few. Hypotension is a potential side effect. The exact mechanism of nimodipine's efficacy is unclear, but it may be neuroprotective. Patients with recently ruptured aneurysms should receive nimodipine as part of their general medical care (Mayberg et al 1994, Ven Gijn and Rinkel 2001). The U.S. Food and Drug Administration have approved the use of nimodipine for this indication. The usual oral dosage of nimodipine is 60 mg every 4 hours. Comatose patients can receive the medication via a nasogastic tube. The usual duration of treatment is 3 weeks after SAH, although a shorter course (10 to 14days) may be all that is needed. If the SAH is not diagnosed until 10 to 14 days after it has occurred, the patient has already survived the period of greatest risk for ischemia, and nimodipine might not be needed. Nicardipine has similar potential theraputic actions, and it can be given parenterally. Use of the agent in SAH was tested in a large clinical trial (Haley et al 1993). At 3 months, the actively treated and control groups had comparable rates of favorable outcomes, but the frequency of symptomatic vasospasm was reduced with the use of nicardipine. In another study comparing two different doses of nicardipine, the same investigators found that the lower dose of medication was associated with a slightly higher rate of severe vasospasm but that outcomes were similar in the two groups (Haley et al 1994). Shibuya and colleagues (1994), who administered nicardipine intrathecally to 50 patients with SAH, noted declines in both symptomatic and arteriographic vasospasm. These studies suggest that nicardipine is effective in preventing ischemic sequelae of SAH but that the combination of aggressive volume expansion and induced hypertension is also effective. These additional data support the use of calcium channel blockers supplemented by hypervolemic hemodilution and induced hypertension for prevention of ischemic stroke after SAH.
OTHER MEDICATION TO PREVENT VASOSPASM OR ISCHEMIC STROKE
Calcitonin gene-related peptide (CGRP), a potent vasodilator, was tested in a small clinical trial (Lancet 339:891-834, 1992). Hypotension was a common side effect, and two thirds of the treated patients did not complete of the course of treatment. Although this study was reported as having negative results for the use of CGRP, largely because of its small size, favorable outcomes were noted in 60% of treated patients and 60% of controls.
Clinical studies of superselective intra-arterial administration of papaverine that this potent vasodilator may be helpful (Clouston et al 1995). Firlik and coworkers (1999) found that intraarterial papaverine can reverse the arterial narrowing of vasospasm. In their series of 15 patients (32 treated arteries), pavaverine therapy increased cerebral blood flow in 46% of cases and led to major clinical improvement in 26%. Kaku and associates(1992) reported that this agent should be given before the arteries lose their ability to respond. Hypotension does not appear to be a complication of local intra-arterial infusions. Seizures have been reported as a complication of this therapy(Carhuapoma et al 2001). Arakawa and colleagues(2001) reported that the vasodilator milrinone might be helpful in dilating vasospastic vessels.

Finfer and associates(1999) used barbiturate- induced coma to protect the brain in 11 patients with severe vasospasm, 10 of whom had good outcomes. These investigators proposed this therapy for patients who show no response to other medical interventions. Although barbiturate-induced coma does offer benefit, it is a very vigorous therapy that requires intensive adjunctive care. It utility has not been established.
The 21-aminosteroids can scavenge free radicals and inhibit lipid peroxidation, features that promote stabilization of the membranes of ischemic tissues. Clinical trails have been conducted to test intravenously administered tirilazed given as a supplement to oral nimodipine (Haley et al 1997, Kassell et al 1996, Lanzino and Kassell 1999). Although the medication was well tolerated, no major improvement in favorable outcomes was noted with treatment. The medication has not been approved for management of patients with SAH.
HYPERVOLEMIC HEMODILUTION AND INDUCED HYPERTENSION
Increasing cerebral blood flow can ease ischemic symptoms and can prevent permanent neurologic sequelae (Mayberg et al 1994, Kassell et al 1982, Mori et al 1995). Reduction in the diameter of the vascular lumen affects the blood's rheologic characteristies and, thus, influences flow. Severe losses of water and sodium result in hemoconcertration, which in turn increases viscosity and reduces blood flow. Measures to prevent infarction by correcting the losses of sodium and water are initiated upon the patient's admission to the hospital. A small randomized trial of prophylactic therapy with hypervolemic hypertensive hemodilution therapy did not demonstrate benefit in preventing vasospasm (Mori et al 1995).
Because autoregulation is impaired, cerebral blood flow becomes pressure-dependent. Cerebral perfusion pressure is altered by changes in the mean arterial blood pressure and intracranial pressure. Improvement of venous drainage by positioning and elevation of the head, treatment of brain edema, and control of hydrocephalus lowers intracranial pressure and improves perfusion. When feasible, antihypertensive agents are avoided. Nimodipine may have to be discontinued so that the blood pressure can be effectively raised. After the diagnosis of symptomatic vasospasm is made, more aggressive treatment of increased intracranial pressure, including hyperventilation and mannitol, might help. Antifibrinolytic agents should be discontinued.
Several groups report reversal of ischemic symptoms with the combination of volume expansion and drug induced hypertension (Kassell et al 1982, Mori et al 1995). In some cases, neurologic signs can reappear when the therapy is discontinued (Kassell et al 1982) Although no controlled trials of this regimen have been conducted, the previously described trial of nicardipine demonstrates a benefit from this aggressive therapy(Haley et al1993). Qureshi and associates (2000) found that patients with a depressed level of consciousness at the initiation of volume expansion therapy on blood flow and cardiac function (Lennihan et al 2000). The investigators found that hypervolemic therapy raised cardiac filling pressures but it did not increase cerebral blood flow. A meta -analysis of published data found that there is no sound evidence for or against the use of volume expansion therapy in patients with SAH (Feigin et al 2000).
If improvement is not observed after volume expansion, a vasopressor (most commonly dopamine or phenylephrine) is added in an attempt to increase mean arterial blood pressure. Darby and coworkers (Darby et al 1994) noted that the increase in cerebral blood flow after use of dopamine may be independent of changes in blood pressure, because the dopamine

might have direct cerebrovascular effects. Although there is some disagreement about the utility of hypervolemic hemodilution and induced hypertension to prevent ischemia after SAH, the regimen is commonly prescribed (van Gijn & Rinkel. 2001,Oropellet et al 1996, Ullman & Bedersom 1996).
This therapy is vigorous, and patients need intensive observation. Arterial pressure, cardiac rhythm, central venous pressure, or pulmonary artery wedge pressure should be continuously monitored (Mori et al 1995). Continuous intracranial pressure monitoring may be also needed. Frequent laboratory assessments of serum electrolytes, serum osmolarity, blood gases, and blood counts are needed. Complications of the therapy include congestive heart failure, pulmonary edema, acute myocardial infraction, and cardiac arrhythmias. Worsening of brain edema, hypertensive intracerebral hemorrhage, haemorrhagic transformation of the infraction, and re-rupture of the aneurysm can also occur(Kassell et al 1996). Shimoda and colleagues (1993) reported worsening of brain edema in 18 of their 94 patients undergoing hypervolemic hemodilution; 8 others had haemorrhagic infractions. These investigators advised against the use of hypervolemic hemodilution if a patient's CT scan shows an ischemic lesion in the brain, particularly if the abnormality is found within 6 days of SAH.
ANGIOPLASTY
Transluminal angioplasty successfully dilates vasospastic arteries (Coyne et al 1994). The development of microballoons allows for catheterization in small- to medium-sized arteries at the base of the brain. Angioplasty does stretch and disrupt the arterial wall (Honma et al 1995). Bejjani and associates (1998) performed angioplasty at approximately 7 days after SAH in 31 patients, treating a total of 81 vessels. These investigators noted major clinical improvements in 12 cases and moderate improvements in another 11. They encountered no major neurologic complications and concluded that angioplasty is a potentially useful treatment for patients who show no response to other therapies. Polin and coworkers (2000) found that angioplasty is effective in reversing angiographically confirmed vasospasm, but they did not observe clinical improvements with treatment. At present, angioplasty is usually reserved for treatment of SAH that does not respond to medical measures.
ARTERIOVENOUS MALFORMATIONS OF THE BRAIN:(ROPPER & BROWN 2005)
An arteriovenous malformation (AVM) consists of a tangle of dilated vessels that from an abnormal communication between the arterial and venous systems, really an arteriovenous fistula. It is a developmental persistence of an embryonic pattern of blood vessels and is not a neoplasm, but the constituent vessels may proliferate and enlarge with the passage of time. Arteriovenous malformations have been designated by a number of other terms, such as angioma and arteriovenous aneurysm, but these are less appropriate; angioma suggests a tumor, and the term aneurysm is generally reserved for the lesions described in the preceding section. Venous malformations, consisting purely of distended veins deep in the white matter, are a separate entity; they may be the cause of seizures and headaches but seldom of haemorrhage. When a small haemorrhage occurs in relation to venous malformation, it is due to an associated cavernous malformation.
Vascular malformations vary in size from a small blemish a few millimeters in diameter lying in the cortex or white mater to a huge mass of tortuous channels constituting an AV shunt of sufficient magnitude, in rare instances, to raise cardiac output. Hypertrophic dilated arterial feeders can be seen approaching the main lesion and to break up into a network of thin-walled blood vessels that connect directly with draining veins. The latter often from greatly

dilated, pulsating channels, carrying away arterial blood. The tangled blood vessels interposed between arteries and veins are abnormally thin and do not have the structure of normal arteries or veins. Arteriovenous malformations occur in all parts of the cerebrum, brainstem, and cerebellum (and spinal cord), but the larger ones are more frequently found in the central part of a cerebral hemisphere, commonly forming a wedge-shape lesion extending from the cortex to the ventricle. Some lie on the dural surface of the brain or spinal cord, but these most often turn out to be direct arteriovenous fistulas.
When heamorrhage occurs, blood may enter the subarachniod space, producing a picture almost identical to that of ruptured saccular aneurysm, but generally less severe; since most AVMs lie within cerebral tissue, bleeding is more than likely to be intracerebral as well, causing a hemiparesis, hemiplegia, and so forth, or even death.
Arteriovenous malformations are about one-tenth as common as saccular aneurysms and about equally frequent in males and females. The two lesions-AVM and saccular aneurysm are associated in about 5 percent of cases; the conjunction increases with the size of the AVM and the age of the patient (Miyasaka et al 1982). Rarely, AVMs occur in more than one member of a family in the same generation or successive ones.
CLINICAL FEATURES
Bleeding or seizures are the main modes of presentation. Most AVMs are clinically silent for a long time, but sooner or later they bleed. The first haemorrhage may be fatal, but in more than 90 percent of cases the bleeding stops and the patient survives. The rate of haemorrhage in untreated patients is established to be 2 to 4 percent per year, far lower than aneurysms. The mortality rate in two major series (Crawford et al 1986, Ondra et al 1994 ) has been 1 to 2 percent per year but as high as 6 to 9 percent in the immediate year following a first haemorrhage. The matter of an increased risk of AVM rupture during pregnancy has been disputed. The weight of evidence suggests that the risk is not raised by pregnancy alone, but -as with saccular aneurysm- that parturition and Valsalva activity is always a source of concern. Before rupture, chronic, recurrent headache may be a complaint; usually the headache is of a nondescript type, but a classic migraine with or without neurologic accompaniment occurs in about 10 percent of patients-probably with greater frequency than it does in the general population. Most of the lesions associated with migraine-like headaches lie in the parietal-occipital region of one cerebral hemisphere, and about two-thirds of such patients have a family history of migraine.
Huge AVMs may produce a slowly progressive neurologic deficit because of compression of neighboring structures by the enlarging mass of vessels and by shunting of blood through greatly dilated vascular channels ("intracerebral steal"), resulting in hypoperfusion of the surrounding brain(Homan et al 1986). When the vein of Galen is enlarged as a result of drainage from an adjacent AVM, hydrocephalus may result. Not infrequently one or both carotid arteries pulsate unusually forcefully in the neck. A systolic bruit heard over the carotid in the neck or over the mastoid process or the eyeballs in a young adult is almost pathognomonic of an AVM. However, such bruits have been heard in fewer than 25 percent of our patients. Exercise that increases the pulse pressure may bring out a bruit if none is present at rest.
Fully 95 percent of AVMs are disclosed by CT scans if enhanced and an ever larger number by MRI. Magnetic susceptibility MRI shows small areas of previous bleeding around AVMs.

Arteriography is usually necessary to establish the diagnosis with certainty and will demonstrate AVMs larger than 5 mm in diameter; MRI may fail to reveal smaller lesions. Small ones may be obscured by haemorrhage; even at autopsy, a careful search under the dissecting microscope may be necessary to find them.
Treatment
The preferred approach in most centers is surgical excision. Some 20 to 40 percent of AVMs are amenable to block dissection, with an operative mortality rate of 2 to 5 percent and a morbidity of 5 to 25 percent. In the others, which are inaccessible, attempts have been made to obliterate the malformed vessels by ligation of feeding arteries or by the use of endovascular embolization with liquid adhesives or particular material that are injected via a balloon catheter that has been navigated into a feeding vessel. Complete obliteration of large AVMs is usually not possible by these methods but, they are highly effective in reducing the size of the AVM prior to surgery.
Kjellberg and Chapman (1983) pioneered the treatment of AVMs at the Massachusetts General Hospital using a single dose subnecrotizing stereotactically directed proton radiation. The technique of radiosurgery has been adopted by others using photon radiation sources, such as a linear accelerator, gamma knife, and other modes of focused x-ray radiation, as an accepted alternative to operative treatment of lesions situated in deep regions, including the brainstem, or in 'eloquent', areas of the cortex. Generally, malformations smaller than 3 cm diameter are treatable in this way. Radiosurgical obliteration of AVM occurs in a delayed manner, usually with a latency of at least 18 to 24 months after treatment. During this early period the patient is unprotected from rebleeding.
The likelihood of successful treatment and the nature of the risks depend on the location and size of the AVM and the radiation dose delivered. After 2 years, 75 to 80 percent of AVMs smaller than 2.5 cm in diameter have been obliterated. Even for those AVMs that have not been totally eliminated, the radiation effect appears to confer some long-term protection from bleeding. Of the larger ones, a majority are shrunken or appear less dense. The rest have shown no change at this low dose level, but even in this group, the morbidity and mortality are lower than in the untreated group. However, a proportion of larger AVMs that are obliterated will recanalize, and many of these will subsequently bleed. Among more than 250 patients whose AVMs disappeared following proton beam therapy, there has been no recurrence of hemorrhage for up to 10 years; in larger AVMs (approximately the last 1000 cases) treated in this way, the frequency and severity of hemorrhage have been significantly reduced. The results of treatment with focused gamma radiation have been about the same. In one study, the risk of hemorrhage was reduced by 54 percent between the time of radiation and obliteration of the malformation and by 88 percent thereafter (Maruyama et al 2005).
Two types of complications of radiation occur at a combined rate of approximately 2 to 4 percent. The first is delayed radiation necrosis, which is predictable based on the radiation dose, and the second is a venous congestion that occurs several weeks or months after treatment. The latter is indicative of the desired effect of thrombosis of the malformation. Both cause local symptoms for weeks or months. Radiation necrosis may be reduced by the administration of corticosteroids but the vascular problem generally is not helped.

The treatment of AVMs by endovascular techniques is increasingly popular but has not been fully evaluated. Nearly every AVM has several feeding arteries, some not reachable by catheter and some part of the AVM remains after treatment. In most series, 25 percentor more of AVMs, mostly of small and medium size, could be completely obliterated, with a mortality rate below 3 percent and morbidity of 5 to 7 percent, which compares favorably with surgical outcomes. These techniques are also particularly well adapted to lesions of a combined AVM and an aneurysm on the feeding vessel.
Most recently, combined therapy that begins with endovascular reduction of the lesion and is followed by either surgery or radiation has been viewed most favorably. In series of patients using this approach, over 90 percent of lesions could be obliterated with a very low rebleeding rate over several years. What is clear is that the plan for each patient must be individualized based on the size, location, nature of feeding vessels, the presence of other vascular lesions (aneurysm or additional AVM), and the age of the patient. Even then, there will be differences of opinion based on local resources and experience.
Finally, if the primary problem is recurrent seizure successful treatment with reduction or cessation of seizures is achieved in a very high proportion of cases. The results are comparable to those from surgery and radiation, even if the AVM is not entirely obliterated.
Dural Arteriovenous Fistulas
These curious vascular abnormalities, occurring in both the cranial and spinal dura, have different presentations at each site. The cranial type is being detected with increasing frequency as refinements continue to be made in imaging of the cerebral vessels, but its true incidence and pathogenesis are not fully known. The defining features are radiologic -a nidus of abnormal arteries and veins with arteriovenous shunting contained entirely within the leaflets of the dura. The lesion is fed by dural arterial vessels derived from the internal cranial circulation and often more prolifically, from the external cranial circulation (external carotid artery and muscular branches of the vertebral artery). The venous drainage is complex and is largely into the dural venous sinuses. The rapid transit of injected angiographic dye through these fistulas account, for the early opacification of the draining venous structures; in the case of high-flow connections, this may not be seen unless images are taken almost immediately after the injection. A number of potential feeding vessels must be injected to demonstrate all the conduits into the lesion. On CT scanning and MRI, the fistula is sometimes detected as a thickening or enhancement of a region of dura, generally close to a large dural venous sinus. In other cases, the dilated draining vessels may be seen only with the injection of dye or gadolinium. Probably, many are not detected by these techniques.
The origin of these vascular lesions has not been settled- several mechanisms may be involved. Most evidence suggests that some of these lesions, unlike conventional cerebral AVMs and aneurysms, are not developmental in origin. The best-defined examples are those that arise adjacent to a venous sinus thrombosis or in association with a vascular atresia, most often in the transverse sigmoid sinus or adjacent to the cavernous sinus. However, it is not clear whether the abnormality of the dural sinus is the cause or the result of the dural fistula. In a number of cases, a dural fistula has appeared after a forceful head injury, often in a region remote from the site of impact. A small group is associated with the Klippel-Trenaunay or Osler-Weber-Rendu syndromes, diseases in which frequent conjunction with AVMs is well known. Usually all of these causes can be excluded and the largest group remains idiopathic.

Subdural hemorrhage is an infrequent mode of presentation, sometimes creating a large and fatal clot; another syndrome is a cerebral-subarachnoid hemorrhage, although this occurs with not nearly the frequency or severity as bleeding from brain AVMs. However, our knowledge of the risk of bleeding from dural fistulas and the evolution of the lesions is far less precise than it is for cerebral AVMs. It appears that the dural lesions most at risk of bleeding are those located in the anterior cranial fossa and at the tentorial incisura. Seizures are distinctly uncommon. A special syndrome linked to dural AVMs, although it may occur also with high-flow cerebral malformations, is of headache, vomiting, and papilledema -namely, pseudotumor cerebri. A cranial bruit is infrequent. In small children the high-flow lesions may shunt so much blood as to cause congestive heart failure, similar to malformations of the vein of Galen.
Treatment is by surgical extirpation or endovascular embolization, a painstaking procedure because of the multitude of potential feeding vessels. Surgery seems preferable for the smaller lesions and embolization for larger and inaccessible ones. The issue of anticoagulation, when there is slowed flow in a venous sinus draining a malformation, is unsettled.
Cavernous Malformafions
Vascular malformations composed mainly of clusters of thin walled veins without important arterial feeders and with little or no intervening nervous tissue make up a significant group, some 7 to 8 percent of our series of AVMs. Conventional subdivisions of this group into cavernous, venous, and telangiectatic types have not proven useful. We have, therefore, roughly designated them all as cavernous. They have several attributes that set them apart. Their tendency to bleed is probably no less than that of the more common AVMs, but far more often the haemorrhages are small and clinically silent. The exact incidence of bleeding is uncertain but is estimated to be less than 1 percent per year per lesion. Often there are multiple lesions. They are generally not seen in arteriograms. The diagnosis is based on their clinical manifestations and MRI, which discloses a cluster of vessels surround by a zone of hypodense feritin in the T1- weight images, the product of previous small episodes of bleeding. A small but uncertain number are associated with adjacent venous malformations, visualized by imaging studies. The lack of formation of a mass over long period of time separates this lesion from a malignant tumor that has bled. About one-half of all cavernous angiomas lie in the brainstem, and in the past (before the availability of MRI), many of them were misdiagnosed as multiple sclerosis because of a stepwise accumulation of neurologic deficits with each haemorrhage.
About 10 percent of these lesions are multiple and 5 percent are familiar. In one of the families we have followed of Italian-American origin, there were 29 affected members in there generations. The inheritance followed an autosomal dominant pattern; Marchuk and coworkers (1995) have localized the abnormal gene in other kindreds to the long arm of chromosome 7. One interesting characteristic of this group, as pointed out by Labauge and colleagues (2001), is the appearance over time of new lesions in one- third of patients. The follow- up of some of our patients has documented this.
Treatment

Cavernous angiomas on the surface of the brain, within reach of the neurosurgeon, even those in the brainstem, can be plucked out, like clusters of grapes, with low morbidity and mortality. Kjellberg and colleagues(1983) have treated 89 deeply situated cavernous angiomas with low-dose proton radiation. Our impression is that these vascular malformations, like the hemangioblastoma, respond poorly to radiation and are not amenable to treatment by endovascular techniques.
Lesions that cause recurrent bleeding and are surgically accessible with little risk are often removed, but incidentally discovered angiomas and those that are inaccessible may be left alone. Although this is the approach usually taken, there is not adequate data on the rate and risk of bleeding to determine proper approach. CONCLUSION
Considerable progress is being made in the management of SAH. Medical and surgical therapies that effectively prevent rebreeding and vasospasm are reflected by declines in mortality and morbidity. Still, there is considerable room for improvement. Several promising therapies are being tested; one or more of these interventions likely will be shown to further improve outcomes after SAH. However, most successful therapies are based on early treatment. Thus, the medical community must give greater attention to the early diagnosis of SAH and the acute care of patients with SAH who are critically ill.