Blood Pressure and Blood Flow Variation during Postural Change … · 2005-05-12 · 1 Blood...
20
1 Blood Pressure and Blood Flow Variation during Postural Change from Sitting to Standing: Model Development and Validation Mette S. Olufsen Department of Mathematics & Center for Resarch in Scientific Computation North Carolina State University Raleigh, NC 27695 email: [email protected] Phone: (919) 515 2678, Fax: (919) 513 7336 Johnny T. Ottesen Department of Mathematics and Physics Roskilde University, Roskilde, Denmark Hien T. Tran and Laura M. Ellwein Department of Mathematics & Center for Resarch in Scientific Computation North Carolina State University, Raleigh, NC 27695 Lewis A. Lipsitz Hebrew SeniorLife, Research and Training Institute, Division of Gerontology, Beth Israel Deaconess Medical Center, and Harvard Medical School, Boston, MA 02215 Vera Novak Division of Gerontology Beth Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA 02215 Abstract— Short term cardiovascular responses to pos- tural change from sitting to standing involve complex interactions between the autonomic nervous system that regulates blood pressure, and cerebral autoregulation that maintains cerebral perfusion. We present a mathematical model that can predict dynamic changes observed in beat-to-beat arterial blood pressure and middle cerebral artery blood flow velocity during postural change from sitting to standing. Our cardiovascular model utilizes 11 compartments to describe blood pressure, blood flow, compliance and resistance in the heart and systemic circulation. To include dynamics due to the pulsatile nature of blood pressure and blood flow, resistances in the large systemic arteries are modeled using nonlinear functions of pressure. A physiologically based sub-model is used to describe effects of gravity on venous blood pooling during postural change. Two types of control mechanisms are included: (i) Autonomic regulation mediated by sym- pathetic and parasympathetic responses that affect heart rate, cardiac contractility, resistance, and compliance. (ii) Autoregulation mediated by responses to local changes in myogenic tone, metabolic demand, and concentration of carbon dioxide (CO 2 ) that affect cerebrovascular re- sistance. Finally, we formulate an inverse least squares problem for parameter estimation and to demonstrate that our mathematical model is in agreement with physiological data obtained from a young subject during postural change from sitting to standing. Keywords: Cardiovascular system; Mathematical modeling; Cerebral blood flow; Gravitational effect; Autonomic regulation; Cerebral Autoregulation
Transcript of Blood Pressure and Blood Flow Variation during Postural Change … · 2005-05-12 · 1 Blood...

1
Blood Pressure and Blood Flow Variation duringPostural Change from Sitting to Standing: Model
Development and ValidationMette S. Olufsen
Department of Mathematics &Center for Resarch in Scientific Computation
North Carolina State UniversityRaleigh, NC 27695
email: [email protected]: (919) 515 2678, Fax: (919) 513 7336
Johnny T. OttesenDepartment of Mathematics and PhysicsRoskilde University, Roskilde, DenmarkHien T. Tran and Laura M. Ellwein
Department of Mathematics &Center for Resarch in Scientific Computation
North Carolina State University, Raleigh, NC 27695Lewis A. Lipsitz
Hebrew SeniorLife, Research and Training Institute,Division of Gerontology, Beth Israel Deaconess Medical Center,
and Harvard Medical School, Boston, MA 02215Vera Novak
Division of Gerontology Beth Beth Israel Deaconess Medical Centerand Harvard Medical School, Boston, MA 02215
Abstract— Short term cardiovascular responses to pos-tural change from sitting to standing involve complexinteractions between the autonomic nervous system thatregulates blood pressure, and cerebral autoregulation thatmaintains cerebral perfusion. We present a mathematicalmodel that can predict dynamic changes observed inbeat-to-beat arterial blood pressure and middle cerebralartery blood flow velocity during postural change fromsitting to standing. Our cardiovascular model utilizes 11compartments to describe blood pressure, blood flow,compliance and resistance in the heart and systemiccirculation. To include dynamics due to the pulsatile natureof blood pressure and blood flow, resistances in the largesystemic arteries are modeled using nonlinear functionsof pressure. A physiologically based sub-model is usedto describe effects of gravity on venous blood poolingduring postural change. Two types of control mechanismsare included: (i) Autonomic regulation mediated by sym-pathetic and parasympathetic responses that affect heartrate, cardiac contractility, resistance, and compliance. (ii)Autoregulation mediated by responses to local changesin myogenic tone, metabolic demand, and concentration
of carbon dioxide (CO2) that affect cerebrovascular re-sistance. Finally, we formulate an inverse least squaresproblem for parameter estimation and to demonstrate thatour mathematical model is in agreement with physiologicaldata obtained from a young subject during postural changefrom sitting to standing.
Keywords: Cardiovascular system; Mathematicalmodeling; Cerebral blood flow; Gravitational effect;Autonomic regulation; Cerebral Autoregulation

2
I. INTRODUCTION
Orthostatic intolerance disorders, which are commonin every age, are difficult to diagnose and treat. Typi-cally, these disorders whose clinical manifestations in-clude dizziness, syncope, orthostatic hypotension, falls,and cognitive decline are a result of several biologicalmechanisms. To develop better strategies to treat anddiagnose orthostatic intolerance, it is important to un-derstand the underlying mechanisms leading to thesedisorders. One of the main mechanisms involved is theshort term cardiovascular regulation of blood flow tothe brain, which include both autonomic regulation andcerebral autoregulation. The overall goal of this workis to develop a mathematical model that can predictdynamics in observed cerebral blood flow and peripheralblood pressure data, and to propose mechanisms that canexplain the interaction between autonomic regulation andcerebral autoregulation. To this end we have developed amathematical model that can predict these two regulatorymechanisms. To validate the model we compare modelpredictions with arterial finger blood pressure paf , andmiddle cerebral artery blood flow velocity vacp measure-ments from a young subject.
Upon standing from a chair, blood is pooled in thelower extremities due to gravitational forces. As a result,venous return is reduced, which lead to a decreasein cardiac stroke volume, a decline in arterial bloodpressure, and an immediate decrease of blood flow tothe brain. The reduction in arterial blood pressure un-loads the baroreceptors located in the carotid and aorticwalls, which leads to parasympathetic withdrawal andsympathetic activation through baroreflex-mediated au-tonomic regulation. Parasympathetic withdrawal inducesfast (within 1-2 cardiac cycles) increases in heart rate,while sympathetic activation yields a slower (within 6-8cardiac cycles) increase in vascular resistance, vasculartone, cardiac contractility, and a further increase in heartrate [4], [7], [37]. Simultaneously, cerebral autoregula-tion, mediated by changes in CO2, myogenic tone, andmetabolic demand leads to vasodilation of the cerebralarterioles [2], [18], [34], [38].
Our mathematical model includes two sub-models: (i)a cardiovascular model that can predict blood pressureand blood flow velocity during sitting (for t ≤ 60 sec.),and (ii) a control model that can predict autonomic andcerebral regulatory mechanisms during postural changefrom sitting to standing. Both sub-models are basedon the same closed-loop compartmental model with11 compartments that represent the heart and systemiccirculation. Our previous work [27], [29] also usedcompartmental models to describe the dynamics of the
cardiovascular system. The model in [27] used an open-loop model (the 3-element windkessel model) to analyzedynamics of cardiovascular control. This model usedarterial blood pressure measured in the finger as an inputto predict model parameters that describe dynamics ofcerebral vascular regulation for young people. Theseparameters were obtained by minimizing the error be-tween computed and measured middle cerebral arterialblood flow velocity. Consequently, no equations wereused to describe possible mechanisms of the underlyingregulation. To further advance this study, we recentlydeveloped a 7 compartmental closed-loop model, thatcan predict the dynamics observed in the data. Thismodel did not rely on an external input, but includeda model that describe the pumping of the left ventricle.In addition, the 7 compartmental model included simpleequations that describe the short term regulation. Thismodel was able to accurately predict dynamics of bothcerebral blood flow velocity and arterial blood pressureduring sitting (for t < 60 sec.) and standing (for t > 80sec), as well as the mean values during the transition (for60 < t < 80 sec.), but it was not able to predict detaileddynamics during the transition region. Furthermore, wewere not able to obtain adequate filling of the left ventri-cle. To obtain a more accurate model we developed the11 compartmental model described in this work, whichovercome limitations of the 7 compartmental model asdescribed below.
To obtain adequate filling of the left ventricle weadded a compartment that represents the left atrium. Inthe 7 compartmental model we used the blood pressurein the upper body to validate the model against data,which are measured in the finger. The pulse pressure(systolic minus diastolic pressure) in the upper body istoo wide and very sensitive to parameter changes. Hence,to improve our model we included a compartment thatrepresents the arteries in the finger. In addition, we addedtwo small compartments that represent the aorta andvena cava. These compartments were primarily addedto improve model simulation stability. In summary, theimprovements discussed above have led to the addition of4 additional compartments. Furthermore, the 7 compart-mental model was not able to predict pulse pressure reg-ulation immediately following standing. To compensatefor this we have modeled resistance of the large arteriesusing nonlinear functions of pressure. Finally, to obtainaccurate widening of the blood flow velocity, a featurethat our 7 compartmental model was not able to predict,we devised an empirical model of autoregulation, and aphysiological model that can predict pooling of blood inlower extremities, due to effects of gravity.
A large body of work that describe cardiovascular

3
control modeling, e.g., [10], [11], [12], [30], [44] isbased on predictions of mean values for arterial bloodpressure and cerebral blood flow velocity. Consequently,these models can not predict the pulsatile dynamicsof the cardiovascular system. These models use opti-mal control to minimize the deviation between someobserved quantity (e.g., arterial blood pressure) and agiven set-point. While this strategy can provide goodparameter estimates, optimal control models do not de-scribe the underlying physiological mechanisms. Othermodeling strategies have been proposed in the work byMelchior [19], [20] and Heldt [8], who devise pulsatilemodels that include pulsatility, autonomic regulation, andeffects of gravity. The latter was done by changing thereference pressure outside the compartments. However,these models do not include effects of autoregulation.One way to model the effect of autoregulation is to letthe cerebrovascular resistance be a function of time assuggested by Ursino [39]. However, this work does notinclude the effects of autonomic regulation.
A second group of models has described parts ofthe control system without validation against experi-mental data, e.g., [5], [19], [20], [21], [31], [32], [35],[40], [41], [42], [43]. These models used a closed-loopcompartmental description of the cardiovascular systemcombined with physiological descriptions of the control.While these models can provide qualitative analysis ofthe system they cannot be used for quantitative compar-isons with data. Furthermore, most of the models in thesecond group describe the effects of autonomic regula-tion without including the effects of cerebral autoregu-lation. In contrast, our model includes both autonomicand cerebrovascular regulations and provides quantitativecomparisons with physiological data.
II. MODELING BLOOD PRESSURE AND BLOOD FLOW
VELOCITY
A. A Compartmental Model for the Cardiovascular Sys-tem
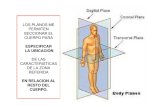
Our cardiovascular model is based on a closed-loopmodel with 11 compartments. This model is designedto predict blood pressure and volumetric blood in theleft atrium, the left ventricle, aorta, vena cava, arteriesand veins in the upper body, the lower body, and thehead, as well as arteries in the finger, see Fig. 1. Eachcompartment represents all vessels in areas of similarpressure. Hence, in its simplest form the systemic circuitcould consist of one arterial compartment (high pressure)and one venous compartment (low pressure). In ourmodel, we include 5 arterial compartments and 4 venouscompartments.
The 11 compartments depicted in Fig. 1 are chosen toensure that the level of detail in the model is adequateto describe the complex dynamics observed in the dataand at the same time not too complex to be solvedcomputationally. Four compartments that represent theupper body and the legs are included to model venouspooling of blood and sympathetic contraction of thevascular bed. Two compartments that represent the brainare included to model effects of cerebral autoregulationand to enable model validation against cerebral arterialblood flow velocity measurements. One compartmentthat represents the finger is included to enable modelvalidation against arterial blood pressure measured in thefinger. To determine cardiac output and venous return,two compartments are included to represent the aortaand vena cava. Finally, to obtain a closed-loop model itis necessary to include a source (the heart) that pumpsblood through the system. Consequently, two compart-ments are included to represent the left atrium and theleft ventricle. Our previous work [29] only included theleft ventricle, but without an atrium it is not possible toobtain adequate filling of the heart.
The major system not included in our model is thepulmonary circulation. Addition of compartments thatrepresent the pulmonary circulation would require moreparameters, which would increase the computationalcomplexity. Instead, the pulmonary circulation is rep-resented as a resistance between vena cava and the leftatrium.
To study dynamics of postural change from sittingto standing it is not important to know how blood isdistributed among various inner organs. Hence, the upperbody is simply represented by an arterial and a venouscompartment. Each compartment is represented by acompliance element (inverse elasticity) and is separatedby resistance to flow. The design of the systemic cir-culation with arteries and veins separated by capillariesprovides some resistance and inertia to the volumetricflow rate. In our model we include effects of resistancebetween compartments but neglect effects due to inertia.The major resistance to flow is located in peripheralregions between compartments that represent arteriesand veins. Compartments that represent large conduitvessels are also separated by resistances that representthe overall resistance of the compartment. Resistancesbetween conduit vessels are very small compared withthe peripheral resistances.
The description of blood pressure and volumetric flowrate in a system comprised of compliant compartments(capacitors) and resistors are equivalent to that of anelectrical circuit, see Fig. 1, where blood pressure p[mmHg] plays the role of voltage and volumetric flow

4
Finger Art
Veins (legs)
Vena cava Atrium
Sys Art (legs)
Sys Art (up)
Cer Art
Sys Aorta
Cer Veins
Veins (up)
Left ventricle
qal
qafp
Raup
Racp
qacp
Rac
Rav
qav
Caf
Vaf
Raf
qaf
qau Rau
Cau
pv
Vvl
Cvl
pvu
pvc
Vv
pvl
Cal
pac
Val
Vau
pal
pla paplv
Clv(t)
qac
qalp
qaup
Vac
Cvc
Cv
Vvc
Vla
Cla(t)
Cvu
Vvu
Cac
Ca
Va
paf
pau
Ralp
Ral
Rvc qvc
qvuRvu
qvlRvl
RmvRv
qmvqv
Vlv
Rafp
Fig. 1. Compartmental model of the systemic circulation. The model contains 11 compartments. 5 compartments represent systemic arteries(the brain, upper body, lower body, aorta and the finger), 4 compartments represent the systemic veins (the brain, upper body, lower body,and vena cava), and 2 compartments represent the left atrium and left ventricle. Since the pulmonary system is not included, the systemicveins are directly attached to the left ventricle. Each compartment includes a capacitor to represent the compliant volume of the arteriesor veins. All compartments are separated by resistors representing resistance of the vessels. Furthermore, the compartment representing theleft ventricle has two valves (the aortic valve and the mitral valve). Following terminology from electrical circuit theory, the flow betweencompartments is equivalent to electrical current and the pressure inside each compartment is analogous to voltage. Resistors R [mmHgsec/cm3] are marked with zigzag lines, capacitors C [cm3/mmHg] are marked with dashed parallel lines inside the compartments, whilethe aortic and mitral valves are marked with short lines inside the compartment that represents the left ventricle. The abbreviations are laleft atrium, lv left ventricle, av aortic valve, mv mitral valve, a aorta, au arteries in the upper body, al arteries in the lower body, aupperipheral arteries in the upper body, alp peripheral arteries in the lower body, ac cerebral arteries (in the brain), acp peripheral cerebralarteries, af finger arteries, afp peripheral finger arteries, vl veins in the lower body, vu veins in the trunk and upper body, v vena cava,and vc cerebral veins.
rate q [cm3/sec] plays the role of current. To compareour model with data we assume that the diameter ofthe middle cerebral artery remains constant, such thatblood flow velocity can be obtained by scaling volu-metric blood flow by a constant factor that representsthe area of the vessel. Recent measurements of middlecerebral artery diameter by magnetic resonance imaging(MRI) combined with transcranial Doppler assessment ofcerebral blood flow velocity have demonstrated that themiddle cerebral artery diameter does not change despitelarge changes in cerebral blood flow velocity elicited bystimuli such as lower body negative pressure and CO2
changes [36].
To predict blood pressure and blood flow in andbetween the compartments we base our model on volumeconservation laws [41]. Blood pressure and volumetricblood flow can be found by computing the volume andchange of volume for each compartment. The equationsthat represent the arterial and venous compartments are
similar. For each of these compartments the stressed vol-ume V = Cp [cm3] (volume pumped out during one car-diac cycle), where C [cm3/mmHg] is the compliance andp [mmHg] is the blood pressure. The cardiac output fromthe heart is given by CO = HVstroke [cm3/sec], whereH [beats/sec] is the heart rate and Vstroke [cm3/beat] isthe stroke volume. For each compartment, the net changeof volume is given by
dV
dt= qin − qout, q =
pin − pout
R, (1)
where q [cm3/sec] is determined analogously to Kirch-hoff’s current law and R is the resistance to flow. Severalcompartments have more than one inflow or outflow.For example, the compartment that represent the aortahas 3 outflows (qout = qaf + qau + qac) while thecompartment that represent vena cava has 3 inflows(qin = qafp + qvu + qvc), see Fig. 1.
To model the left ventricle as a pump, the positionof the mitral and the aortic valves must be included.

5
During diastole the mitral valve is open while the aorticvalve is closed allowing blood to enter the left ventricle.Then, isometric contraction begins, increasing the ven-tricular pressure. Once, the ventricular pressure exceedsthe aortic pressure, the aortic valve opens, propellingthe pulse wave through the vascular system. Note, forhealthy young people, both valves cannot be open si-multaneously. To incorporate the state of the valves wehave modeled the resistances (Rav and Rmv , see Fig. 1)as follows
Rv = min(
Rv + e−10(pin−pout), 5000)
,
where v = mv, av. This equation result in a largeresistance (and no flow) while the valve is closed anda small resistance (and normal flow) while the valveis open. The minimum value is introduced to avoidnumerical problems due to large numbers.
A system of differential equations is obtained by dif-ferentiating the volume equation V = Cp and inserting(1), i.e.,
dV
dt= C
dp
dt+ p
dC
dt= qin − qout. (2)
The circuit in Fig. 1 gives rise to a total of 9 differentialequations in dp/dt, one for each of the arterial andvenous compartments. For the two compartments thatrepresent the atrium and the ventricle, differential equa-tions are kept as dV/dt. For these two compartments,blood pressure is computed explicitly as a function ofvolume, see next section. A complete list of equationscan be found in the Appendix.
B. Ventricular and Atrial Contraction
Atrial and ventricular contraction leads to an increasein blood pressure from low values observed in the venoussystem to high values observed in the arterial system.Our model is based on the work by Ottesen [6], [33].This model predicts atrial (pla) and ventricular (plv)pressure as a function volume and cardiac activation ofthe form
p = a(V (t)− b)2 +(c(t)V (t)− d)g(t), p = pla, plv.(3)
The parameter a [mmHg/cm3] is related to elastanceduring relaxation and b [cm3] represents volume at zerodiastolic pressure, c(t) [mmHg/cm3] represents contrac-tility, and d [mmHg] is related to the volume dependentand volume independent components of the developedpressure. The activation function g(t), which is definedover the length of one cardiac cycle, is described by a
polynomial of degree (n,m): g(t) = f(t)/f(tp) with
f(t̃) =
ppt̃n(β − t̃)m
nnmm[
βm+n
]m+n 0 ≤ t̃ ≤ β
0 β < t̃ ≤ T.
(4)
T [sec] is the duration of the cardiac cycle, t̃ =mod(t, T ) [sec], β(H) [sec] denotes the onset of relax-ation, H = 1/T [1/sec] denotes the heart rate, n and mcharacterize the contraction and relaxation phases, andpp is the peak value of the activation. The ability to varyheart rate is included in the isovolumic pressure equation(3) by scaling time and peak values of the activationfunction f . The time for peak value of the contraction,tp [sec], is scaled by introducing a sigmoidal function,that depend on the heart rate H , of the form
tp = tm +θν
Hν + θν(tM − tm), (5)
where θ represents the median and ν represents the steep-ness, and tm [sec] and tM [sec] denote the minimumand maximum values, respectively. The peak ventricularpressure pp [mmHg] is scaled similarly using a sigmoidalfunction of the form
pp = pm +Hη
Hη + φη(pM − pm), (6)
where φ represents the median and η represents thesteepness, pm [mmHg] and pM [mmHg] denote theminimum and maximum values, respectively.
Finally, the time for onset of relaxation β is modeledby
β =n+m
ntp(H). (7)
This equation is obtained by recognizing that the timefor peak pressure, tp, is related to the parameter β inthe isovolumic pressure model (3). Initial values for allparameters were obtained from the work by Ottesen andDanielsen [33]. In this work, parameters were basedon canine data. To obtain human values for the youngsubject studied in this work, we identified parametersduring our model validation. Resulting parameters canbe found in Table I.
C. Nonlinear Resistances
To our knowledge, previous modeling contributions,discussed in the introduction, assume that during steadystate (during sitting, for t ≤ 60 sec.) the small resistancesbetween compartments that represent large conduit ves-sels are constant. Nevertheless, from the theory of fluidmechanics it is well known that the resistance dependson the radii of the vessels, and that the radii themselvesdepend on the corresponding transmural pressure.

6
Rest. Initial Optimized Heart Initial OptimizedComp.
Rav 0.030 0.1149 av 0.0003 0.0009Rau 0.072 0.1853 bv 5 4.9122Ral 0.087 0.0043 cv 6.4 6.9100Raf 0.183 0.5456 dv 1 0.8310Rac 0.409 0.3177 nv 2 3.6659Raup 1.565 1.8565 mv 2.2 1.7369Ralp 6.522 7.5854 νv 9.9 11.0201Rapf 17.5 17.8953 θv 0.951 0.9213Racp 6.696 7.0838 ηv 17.5 17.6658Rmv 0.007 0.0164 φv 1 1.1560Rv 0.033 0.0368 tm,v 0.186 0.1310Rvu 0.001 0.000 tM,v 0.280 0.2305Rvl 0.174 0.1193 pm,v 0.842 1.1074Rvc 0.957 1.2875 pm,v 1.158 1.2385Ca 0.084 0.0732 aa 0.002 0.0002Cau 0.6160 0.7255 ba 5 4.1074Cal 0.940 0.9881 ca 6.4 6.4325Caf 0.174 0.2353 da 1 1.1668Cac 0.159 0.0892 na 1.9 1.9501Cv 2.931 2.5181 ma 2.2 1.9767Cvu 15.276 15.4531 νa 9.9 10.8595Cvl 6.038 6.2778 θa 1 1.9998Cvc 2.847 2.3007 ηa 17.5 16.5386
φa 1 2.1152fact 0.1415 0.2079 tm,a 0.186 0.2487α 1.4287 2.3220 tM,a 0.280 0.3560
pm,a 0.842 1.0065pM,a 0.990 1.2100
TABLE I
STEADY STATE PARAMETERS BEFORE AND AFTER OPTIMIZATION. RESISTANCES [MMHG SEC/CM3] ARE USED IN EQUATION (1),
COMPLIANCES [CM3/MMHG] IN EQUATION (2), AND HEART PARAMETERS ARE USED IN EQUATION (3).
Our investigation has shown that such dependenciesare important to include in regions that represent vesselswith large diameters and high blood pressure (in thelarge arteries), while they are less important in regionsof low blood pressure (in the venous system). Further-more, these “passive” changes in diameters are alsonegligible in regions with small vessels (in the smallarteries and arterioles) where autonomic responses areactive and dominate the change in vessel diameters. Ourprevious work [29] did not include nonlinear arterialresistances and as a result we were not able to obtaina sufficiently wide pulse pressure immediately followingpostural change from sitting to standing.
To model nonlinearities for these resistances, we baseour derivation on Poiseuille’s law. For flow in a cylinderwith circular cross-sectional area, Poiseuille’s law pre-
dicts the resistance to flow [14] as
R =8ηl
πr4,
where R [mmHg sec/cm3] is the resistance, r [cm] is theradius of the vessel, and η [mmHg sec] is the viscosity ofblood, and l [cm] is the length of the cylindrical vessel.Assume a constant length of the vessel, then
1
R∝ r4 ∝ V 2
∝ p2. (8)
The first relation comes from Poiseuille’s law, the secondcan be obtained by assuming a fixed length l, and thethird by assuming the validity of the pressure volumerelation V = Cp. In the compartmental model discussedabove each compartment lumps a number of vesselstogether and as a result we do not have any specificinformation about r. The relationship in (8) impliesthat the resistance is inversely proportional to pressure

7
squared. For real arteries and veins, the resistance willhave maximum and minimum values. Hence, we havechosen to model this nonlinear relation using a sig-moidally decreasing function of the form
R = (RM −Rm)αk
2
pk + αk2
+Rm, (9)
where RM [mmHg sec/cm3] and Rm [mmHg sec/cm3]are the maximum and minimum values that the resis-tances can have, p [mmHg] is the blood pressure in thecompartment that precede the resistance (in our imple-mentation the actual blood pressure oscillates too muchand as a consequence, for numerical stability, we base theprediction of R on the corresponding mean arterial bloodpressure p̄(t) [mmHg]), resulting ressitance can be seenin Figure 2. As shown in Fig. 3 the mean arterial bloodpressure oscillates with the same frequency but with asmaller amplitude than pa. k represents the steepness ofthe sigmoid, and the parameter α2 is calculated to ensurethat R returns the value of the controlled parameterfound during steady state. For k = 2, the slope of thesigmoid approximates the relation in (8). However, therelation in (8) is only valid for a steady flow. Bloodflow in arteries is unsteady and the flow through a givenvessel depends on the state of the vessel. Consequently,as shown in Table II, we should not expect that k = 2.
In our model 3 resistances are computed as functionsof pressure: Ral(p̄au), Rac(p̄a), Raf (p̄a). The resistanceof the aorta Rau could also be modeled using thismethod. Initial investigations showed that other mecha-nisms, e.g., autoregulation or autonomic regulation, mayalso affect Rau. As a consequence, we have used anempirical model to estimate Rau, see Section III-B.
D. Gravitational Effect
Gravitational effects are essential during posturalchange from sitting to standing. Consider a cylindricalvessel with length ∆z [cm] and time invariant cross-sectional area A [cm2], i.e., dA/dt = 0. Assume thatthere is no velocity across the vessel and that the bloodpressure is only a function position along the vessel.Hence, dv/dr = 0, v [cm/sec] and r [cm] denotes thevelocity and radii, respectively, and the volumetric flowrate becomes q = Av [cm3/sec]. Finally, assume thatthe drag force due to viscous shear is proportional toq. Thus, the drag force per cross-sectional area unit isproportional to q, i.e., the drag force can be written as−RAq, where R [mmHg s/cm3] may be interpreted asthe resistance. In steady state, the resistance R is givenby Poiseuille’s law
R =8πη∆z
A2,
where η represents the fluid viscosity [23].To derive the mathematical model we proceed by
balancing inertial forces with the drag force, the pressureforce, and the gravitational force. The inertial force isgiven by
Mdv
dt= ρA∆z
d
dt
(
q
A
)
= ρ∆zdq
dt,
where ρ = 1.055 [g/cm3] is the density of the fluid andM [g] is the mass of the fluid contained in a piece ofthe vessel with length ∆z [cm] and cross-sectional areaA [cm2], see Fig. 4. Thus, Newton’s second law thatdescribes balancing of forces gives
ρ∆zdq
dt= (pin − pout)A+Mg cos(ψ)−RAq,
where g = 981 [cm/sec2] is the gravitational accelera-tion. From this it follows that
Ldq
dt= pin − pout + ρg∆h−Rq, (10)
where L = ρ∆z/A [1/sec2] is the inertance and ∆h =∆z cos(ψ) = hin − hout [cm] is the vertical differenceof the vessel inlet (at hin where pin is the inlet pressureand pout is the outlet pressure. During steady state (10)reduces to
q =(pin + ρghin)− (pout + ρghout)
R. (11)
When modeling postural change from sitting to standingwe substitute (11) for Kirchhoff’s current law. Notice,in the limit g → 0, (11) approaches the normal form ofKirchhoff’s current law given in (1). Also note, in thecase of energy conservation (R → 0) Bernoulli’s lawfor steady flow is recovered; as a result pin + ρghin =pout +ρghout. Thus Kirchhoff’s current law is still validif we interpret p as the hydrostatic pressure p+ ρgh.
To capture the transition from sitting to standing,h is defined for the lower-body compartments as theexponentially increasing function
h(t) =hM
1 + e−k(t−Tup−δ), (12)
where Tup [sec] is the time at which the subject standsup, hM [cm] is the maximum height needed for themean arterial blood pressure in the finger to drop asindicated by the data, and δ [sec] is the latency forstanding up. In our experiments, the subjects sits withtheir legs elevated and the hand, in which pressure ismeasured, is held by a sling at the level of the heart.Therefore, compartments that represent the heart and thefinger are not affected by gravity. Compartments thatrepresent the brain and the upper-body are exposed toconstant hydrostatic conditions, which are neglected in

8
A
45 50 55 60 65 70 75 80 85 900
0.1
0.2
0.3
0.4
0.5
time [sec]
Rau
[mm
Hg
s/cm
3 ]
B
45 50 55 60 65 70 75 80 85 900
0.5
1
1.5
2
2.5
time [sec]
Rac
[mm
Hg
sec/
cm3]
Fig. 2. “Passive” resistances between compartments that represent the large arteries. The top panel shows Rau(t) (fitted, using (19) with26 values, marked with stars on the figure) and the bottom panel shows Rac(t) [mmHg sec/cm2] (computed using (9)). Both resistances aredepicted for 45 ≤ t ≤ 90. Both resistances increase as a response to the decreasing pressure and then decrease to a new steady state value.The resistances Ral(t) and Raf (t) [mmHg sec/cm2] are modeled similar to Rac(t) and show similar trends.
45 50 55 60 65 70 75 80 85 9055
60
65
70
75
80
85
90
95
100
time [sec]
pam
[mm
Hg]
Fig. 3. The graph shows the mean arterial pressure pa(t) (written as “pam” on the y-axis) [mmHg] for 45 ≤ t ≤ 90. The mean arterialpressure is computed as a continuous function by solving the differential equation in (16). Similar results were obtained for p̄au(t).

9
Initial and optimized regulation parametersParam. Init. Opt. Param. Init. Opt.
p̄a 92.8 - k(catr) 2.0 4.58p̄au 90.0 - RM (catr) 4× css
vtr 11.99τCv 10.0 18.57 Rm(catr) css
vtr/4 0.94τCa 10.0 13.67 k(Ca) 2.0 0.38τR 5.0 23.03 CM (Ca) 4× Css
a 4.3× 10−2
τS 5.0 0.076 Cm(Ca) Cssa /4 4.8× 10−4
hH 50.0 46.73 k(Cau) 2.0 17.22hk 3.0 3.92 CM (Cau) 4× Css
au 1.01δ 0.4 1.26 Cm(Cau) Css
au/4 0.42k(Ral) 5.0 1.48 k(Cal) 2.0 13.90RM (Ral) 10×Rss
al 1.69 CM (Cal) 4× Cssal 15.25
Rm(Ral) Rssal/10 1.1× 10−3 Cm(Cal) Css
al /4 0.82k(Rac) 5.0 8.79 k(Cac) 2.0 4.05RM (Rac) 10×Rss
ac 2.49 CM (Cac) 4× Cssac 0.23
Rm(Rac) Rssac/10 1.3× 10−2 Cm(Cac) Css
ac/4 7.0× 10−2
k(Raf ) 5.0 3.83 k(Caf ) 2.0 81.34RM (Raf ) 10×Rss
af 1.5× 10−1 CM (Caf ) 4× Cssaf 0.46
Rm(Raf ) Rssaf/10 2.9× 10−5 Cm(Caf ) Css
af/4 1.7× 10−2
k(Raup) 2.0 5.74 k(Cv) 3.0 0.47RM (Raup) 4×Rss
aup 14.58 CM (Cv) 5× Cssv 15.32
Rm(Raup) Rssaup/4 0.13 Cm(Cv) Css
v /5 0.52k(Ralp) 5.0 10.57 k(Cvu) 3.0 12.90RM (Ralp) 10×Rss
alp 145.19 CM (Cvu) 5× Cssvu 55.86
Rm(Ralp) Rssalp/10 0.41 Cm(Cvu) Css
vu/5 1.93k(Rafp) 2.0 3.69 k(Cvl) 3.0 47.93RM (Rafp) 4×Rss
afp 64.81 CM (Cvl) 5× Cssvl 277.94
Rm(Rafp) Rssafp/4 0.16 Cm(Cvl) Css
vl /5 0.17k(cvtr) 2.0 4.62 k(Cvc) 3.0 15.71RM (cvtr) 4× css
vtr 17.27 CM (Cvc) 5× Cssvc 13.89
Rm(cvtr) cssvtr/4 1.04 Cm(Cvc) Css
vc/5 0.19
TABLE II
OPTIMIZED PARAMETERS. CONSTANTS p̄a AND p̄au DENOTE PRESSURE SET-POINTS USED IN CONTROL-EQUATIONS. TIME-CONSTANTS
τi DENOTE THE TIME DELAY INVOLVED WITH THE CONTROLLED VARIABLES, PARAMETERS FOR GRAVITY DENOTE THE MAX HEIGHT
NEEDED TO OBTAIN OBSERVED PRESSURE DROP, AND A SMALL DELAY δ FROM WHICH THE SUBJECTS STANDS UP. α REPRESENTS THE
WEIGHT FOR THE EXPONENTIAL NEEDED TO COMPUTE THE MEAN ARTERIAL PRESSURE. OPTIMIZED VALUES FOR THE RESISTANCES
AND CAPACITORS INCLUDE ki THAT REPRESENT THE STEEPNESS OF THE SIGMOID, A MAXIMUM (RM OR CM ) AND A MINIMUM (Rm
OR Cm) VALUE. OPTIMIZED VALUES FOR Rau AND Racp ARE SHOWN IN FIGS. 6 AND 2.
the current formulation. The height difference relative tothe increases for compartments that represent the legs.Consequently, equations for the flows qal and qvl will bemodified as described in (11), that is,
qal =pau − (pal + ρgh)
Ral
qvl =(pvl + ρgh) − pvu
Rvl
.
In the top equation hin = 0 and hout = h, where h iscomputed using (12). In the bottom equation hin = hand hout = 0.
III. MODELING AUTONOMIC REGULATION AND
CEREBRAL AUTOREGULATION
Two main control mechanisms play a role; autonomicregulation and cerebral autoregulation. Autonomic regu-lation is mediated via the autonomic nervous system andcauses changes of resistances in the vascular bed, com-pliance, heart rate, and cardiac contractility. Autoregula-tion is a local control that maintains cerebral perfusiondespite changes in systemic pressure. Autoregulationis mediated via changes in myogenic tone, metabolicdemands, and CO2 concentration.

10
∆h =
∆z cos(ψ) =g cos(ψ)
= g sin(θ)= g cos(π/2− θ)
θ
g
pin
∆z
∆z sin(θ) =
pout
ψ
Fig. 4. A vessel segment with cross-sectional area A [cm2] and length ∆z [cm]. At one end the pressure is pin [mmHg] and at theother end the pressure is pout [mmHg]. The vessel is at an angle ψ with respect to gravity g [g/cm2] and at an angle θ with respect to thehorizontal axis. As indicated on the graph, the difference in vertical latitude is ∆h = ∆z cos(ψ) [cm].
A. Autonomic Regulation
Autonomic regulation is modeled as a pressure reg-ulation where heart rate (H [beats/sec]), cardiac con-tractility (ca, cv [mmHg/cm3]), peripheral systemic re-sistance (Raup, Ralp [mmHg sec/cm3]), and systemiccompliance (Ca, Cau, Cal, Cac, Caf , Cv , Cvu, Cvl,Cvc [cm3/mmHg]) are functions of mean arterial bloodpressure pa [mmHg].
The change in the controlled parameters are modeledusing a first order differential equation with a set-pointfunction dependent on the mean arterial blood pressurep̄a. This simple model is able to predict the observeddynamics. In future work we plan to model effects ofchanges in sympathetic and parasympathetic tone.
dx(t)
dt=−x(t) + xctr(pa)
τ. (13)
The parameter x(t) is controlled, xctr(pa) is the set-pointfunction, and τ [sec] is a time constant that characterizesthe time it takes for the controlled variable to obtain itsfull effect. Different values of τ were used for control ofcardiac contractility, compliance, and resistances, see Ta-ble II. As described earlier, autonomic regulation yieldsincreases in peripheral vascular resistance, heart rate, andcardiac contractility. Heart rate is directly obtained fromdata. Hence, it is not modeled using the set-point func-tion (13). To obtain increases in peripheral resistances(Raup, Ralp, and Rafp) and cardiac contractility (cla andclv) in response to the decrease in arterial blood pressure,
the following set-point function has been used:
xctr(p̄a) = (xM − xm)αk
2
p̄ka + αk
2
+ xm. (14)
A sigmoidal function was used, since it displays satura-tion, i.e., the function has a maximum and a minimumvalue corresponding to maximum dilation and maximumconstriction of the vessels. In addition, vascular toneis increased, leading to a decrease in compliance inresponse to a decrease in arterial blood pressure. Hence,for compliance, the set-point function has the form
xctr(p̄a) = (xM − xm)p̄k
a
p̄ka + αk
2
+ xm. (15)
Equation (14) gives rise to a decreasing sigmoidal curve(i.e., for a decreasing pressure the value of xctr willincrese), while equation (15) gives rise to an increasingsigmoidal curve (i.e., for a decreasing pressure the valueof xctr will decrease). The parameters xm and xM areminimum and maximum values for the controlled param-eter x(t). The parameter α2 is calculated to ensure thatx(t) returns the value of the controlled parameter foundduring steady state optimization. Initial values of param-eters for k, xm, and xM are taken from Danielsen [5],see Table II.
The above control equations are formulated as func-tions of mean arterial blood pressure. However, ourmodel describes the instantaneous (pulsatile) pressure.Mean values are computed as weighted averages where

11
the present time is weighted higher than the past time:
p̄a =1
N
∫ t
0pa(s) exp(−ψ(t− s)) ds. (16)
The normalization factor N is introduced to ensure thatthe correct mean arterial blood pressure is obtained forpa = 1, i.e.,
N =
∫ t
0exp(−ψ(t− s)) ds =
1− exp(−ψt)
ψ. (17)
Since our mathematical model is described by differ-ential equations, it is more efficient to implement adifferential equation to compute the mean arterial bloodpressure. Hence, we differentiate (16) to obtain
dp̄a
dt=−p̄a + pa(t)
N. (18)
A similar equation is used to calculate p̄au.
B. Cerebral Autoregulation
Upon standing, cerebral autoregulation mediates adecline in cerebrovascular resistance (Racp) in responseto the decrease in arterial blood pressure. In addition,the autonomic system may also play a role, eitherby a decrease the cerebrovascular resistance due tocholinergic vasodilation or by an increase the resistancedue to release of noradrenaline [7]. Consequently, it isnot trivial to develop an accurate physiological modelthat describes cerebral autoregulation. Our strategy inthis work has been to use a piecewise linear functionwith unknown coefficients to obtain a representativefunction that describes the time varying response ofthe cerebrovascular resistance. Once such a function isobtained we can interpret the result in terms of theunderlying physiology. To obtain such a function, wehave parameterized the cerebrovascular resistance Racp
using piecewise linear functions of the form
Racp(t) =n∑
i=1
γiHi(t), (19)
where Hi are the standard “hat” functions given by
Hi(t) =
t− ti−1
ti − ti−1, ti−1 ≤ t ≤ ti
ti+1 − t
ti+1 − ti, ti ≤ t ≤ ti+1
0, otherwise.
(20)
The unknown coefficients γi will be estimated togetherwith the other control parameters given in Table II. Asdescribed earlier, we have used a similar method toestimate the resistance Rau, which may be affected bypassive nonlinear-resistances and autonomic regulation.
IV. PARAMETER ESTIMATION
Estimation of model parameters has been done in anumber of steps. First we used physiological propertiesof the system to determine initial values for all param-eters and variables, see Table I. Then we solved thesteady state problem (without including effects of gravityand regulation), i.e., we solved 11 equations of the form(2), one for each compartment. During steady state allresistances and capacitors were kept constant, henceterms that involve pdC/dt = 0. These equations arecombined with equations (3-7) that determine pressuresin the left atrium and ventricle, and equation (18) that de-termines the mean arterial pressures p̄a and p̄au. Finally,we estimated a constant fact used to calculate cerebralblood flow velocity vacp = qacp/fact [cm/sec]. We haveused a constant factor, since we assume that the cross-sectional area of the middle cerebral artery does notchange significantly [36]. These equations involve a totalof 53 parameters that were estimated using the nonlinearoptimization method Nelder-Mead algorithm, which isbased on function information computed on sequencesof simplexes [13]. Estimated parameter values are showntogether with initial values in Table I. To obtain the bestpossible parameter values we used the following costfunction to minimize the difference between measuredand computed values of cerebral blood flow velocity vacp
and finger pressure paf .
J =1
N
(
∑Ni=1 (vd,i − vc,i)
2
v̄d+
∑Ni=1 (pd,i − pc,i)
2
p̄d
)
+
1
M
∑Mi=1
(
vdiad,i − v
diac,i
)2
v̄diad
+
∑Mi=1
(
vsysd,i − v
sysc,i
)2
v̄sysd
+
1
M
∑Mi=1
(
pdiad,i − p
diac,i
)2
p̄diad
+
∑Mi=1
(
psysd,i − p
sysc,i
)2
p̄sysd
where v = vacp and p = paf . Subscript d refers to dataand subscript c to the corresponding computed values.In the first two sums i = [1 : N ], where N is thenumber of data points. To compare the computed xc
and the measured xd values (x = v, p), interpolation isused to evaluate the computed at the same points in timewhere the data is obtained. Each term is divided by thenumber of points and the mean value of the measureddata. As shown in Fig. 5B our model is not able topredict second order oscillations. The error due to poorresolution of second order oscillations is of the sameorder of magnitude as the error due to poor resolutionof the maximum and minimum values. However, forour modeling purpose, it is important to resolve themaximum and minimum value, but it is not important

12
A
30 35 40 45 50 55 60
80
100
120
paf [
mm
Hg]
30 35 40 45 50 55 6020
40
60
80
100
vacp
[cm
/s]
B
30 31 32 33 34
80
100
120
paf [
mm
Hg]
30 31 32 33 3420
40
60
80
time [sec]
vacp
[cm
/s]
Fig. 5. A shows the middle cerebral blood flow velocity (vacp(t) [cm/sec]) and arterial finger blood pressure (paf (t) [mmHg]). Bothgraphs are depicted while the subject is sitting down, i.e., for 0 ≤ t ≤ 60. B shows zoomed versions of the same plots for 29.4 ≤ t ≤ 34.2.During steady state, vacp(t) and paf (t) are obtained by solving the differential equations of the form (2), the appendix lists all equations.On all graphs, the dark lines represent the result of our computations and the underlying light grey lines represent the corresponding data.The figure shows that our model can accurately predict blood flow velocity and blood pressure profiles while the subject is sitting. However,as shown on the zoomed plot in B, our model is not able to capture secondary oscillations observed in the data.
to resolve second order oscillations. To reward goodresolution of the maximum and minimum values, wehave added four additional sums predicting the errorbetween systolic and diastolic computed and measuredvalues (indicated by superscripts sys and dia) of vacp
and paf . Due to the nature of the pulse-wave, only oneminimum and maximum value is obtained per period,hence i = [1 : M ] where M is the number of periodsfor 45 ≤ t ≤ 90.
After the steady state parameters (constant valuesof all resistances and compliances) were obtained weincluded all equations that describe the control and rananother optimization to fit parameters that describe thecontrol functions. This second optimization included 27ordinary differential equations, 11 equations of the form(2), two equations of the form (18), and 14 equations ofthe form (13). These equations are solved together withthe heart model described in equations (3-7), equationsfor passive nonlinear resistances (9), equation (12) that
determines the height used to calculate gravitationalpooling in the veins, and the piecewise linear functionsused to parameterize Racp and Rau. This second opti-mization gave rise to a total of 111 parameters that wereoptimized. Fifty nine parameters are shown in Table IIand Fig. 6 and 2 show the 52 parameters used to parame-terize Racp and Rau. During this second optimization allparameters found during steady state (i.e., during sitting,for t < 60 sec.) optimization remained constant (at theoptimized values). In general, the inverse problem forparameter estimation does not provide a unique solution.In addition, the optimized parameters depend both on theinitial guesses and on the optimization algorithm.
The differential equations from our mathematicalmodel, (2), (13), and (18), are solved using MATLAB’s(The Math Works, Inc., Natick, MA) differential equa-tions solver “ode15s”. Initial values for the resistance andcompliance parameters were found from the distributionof the total blood volume between compartments and

13
45 50 55 60 65 70 75 80 85 900
1
2
3
4
5
6
time [sec]
Rac
p [m
mH
g s/
cm3 ]
Fig. 6. Cerebral vascular resistance Racp(t) [mmHg sec/cm3] for 45 ≤ t ≤ 90. The cerebral vascular resistance is computed using thepiecewise linear equation described in (19). We used 26 values (indicated by stars on the figure) to estimate the cerebrovascular resistance.Our results show that shortly after standing, at t = 60 sec., cerebral autoregulation leads to a decrease in cerebrovascular resistance. Thisdecrease is followed by an increase to a new steady state value slightly higher than the steady state value during sitting (for t ≤ 60 sec.).
steady state estimates for the pressure values in thevarious compartments. The blood volume distribution isobtained using the quantities suggested by [3]. Initialvalues for the resistances and compliances were based onpreviously reported values for blood volumes and flowrates [3], while blood pressure values were obtained fromstandard physiology literature, e.g., [4]. Volumes for eachcompartment are given by
V = Cp+ Vunstr.
where Vunstr is the unstressed volume, i.e., the part of thevolume that is not pumped out during the cardiac cycle.Therefore initial values for compliances and resistancesare calculated by
C =V − Vunstr
p,
R =pin − pout
q.
These initial values are given in Table I. Initial values forpressures and unstressed volumes are given in Table III.
V. EXPERIMENTAL DATA
Our model was validated against continuous phys-iological data obtained from a young subject duringtransition from sitting to standing. In particular, we usedarterial blood pressure measurements from the finger andarterial blood flow velocity measurements from the mid-dle cerebral artery; [15]. Each subject was instrumentedwith a 3-lead echocardiogram (ECG) (Collins, TX, USA)to obtain heart rate and a photoplethysmographic cuff
on the middle finger of the right hand supported at thelevel of the right atrium to obtain non-invasive beat-by-beat blood pressure (Finapres, Ohmeda, CO, USA). Themiddle cerebral artery was insonated by placing a 2 MHzDoppler probe (Nicolet Companion, WI, USA) over thetemporal window to obtain continuous measurementsof blood flow velocity. The envelope of the velocitywaveform was derived from the fast Fourier transform ofthe Doppler signal as described by Aaslid et al. [1]. Allphysiological signals were digitized at 500 Hz (Windaq,Dataq Instruments, OH, USA) and stored for off-lineanalysis. Blood pressure reduction of approximately 30mmHg upon standing up was used as a challenge forcerebral autoregulation. Subjects sat in a straight-backedchair with their legs elevated at 90 degrees in front ofthem. They were then asked to stand. Standing wasdefined as the moment both feet touched the floor.Subjects performed two trials of a 5 minute sit followedby standing for one minute, and one trial of a 5 minutesit followed by a 6 minute stand.
VI. RESULTS
Results from our modeling effort, discussed in theprevious sections, are described below. First, it shouldbe noted that we were able to obtain excellent agreementbetween simulations and measured data. Fig. 7 shows thecharacteristic features of the measured data. After stand-ing up at t = 60 sec., the blood pressure (both systolic,diastolic, and mean values) dropped significantly. Atthe same time, the mean blood flow velocity decreasedduring the transition from sitting to standing (dark line

14
Total UnstressedParam. [mmHg] volume [cm3] volume [cm3]
pa 70.0 Va 40.0 V unstra 32.0
pau 72.0 Vau 300.0 V unstrau 240.0
pal 73.0 Val 233.7 V unstral 151.9
paf 70.0 Vaf 80.0 V unstraf 64.0
pac 70.0 Vac 70.0 V unstrac 56.0
pv 2.0 Vv 183.2 V unstrv 168.5
pvu 2.1 Vvu 1909.5 V unstrvu 1756.7
pvl 2.2 Vvl 724.6 V unstrvl 652.1
pvc 43.0 Vvc 391.4 V unstrvc 360.1
Vlv 68.0Vla 172.0
TABLE III
INITIAL VALUES FOR PRESSURES, TOTAL AND UNSTRESSED VOLUMES. INITIAL PRESSURES ARE ESTIMATED BASED ON STANDARD
PHYSIOLOGICAL TEXTS [4], [7]. INITIAL VOLUMES ARE ESTIMATED BASED ON THE WORK BY BENEKEN [3].
45 50 55 60 65 70 75 80 85 90
50
100
150
paf [
mm
Hg]
45 50 55 60 65 70 75 80 85 900
50
100
vacp
[cm
/sec
]
45 50 55 60 65 70 75 80 85 900.5
1
1.5
time [sec]
H [b
eats
/sec
]
Fig. 7. Measured arterial blood pressure paf (t) [mmHg] in the middle finger (top graph), cerebral blood flow velocity vacp(t) [cm/sec](middle graph), and heart rate H(t) [beats/sec] (bottom graph) for a young subject. All graphs are depicted for 45 ≤ t ≤ 90. In the top twographs, the light grey lines show the time-varying values, and the solid dark lines show the corresponding beat-to-beat mean values. Theheart rate is obtained by H = 1/T , where T [sec] is the duration of the cardiac cycle. Immediately after standing (at t = 60 sec.), bothpulsatile and mean blood pressure dropped significantly, at the same time the mean blood flow velocity dropped while the pulsatile bloodflow velocity widened (i.e., the systolic value increased and the diastolic value decreased). Initially, the heart rate increased followed by anew steady state at a higher level than during sitting.
through pulsatile velocity data). However, while bothsystolic and diastolic values of pressure decreased, onlydiastolic value of the blood flow velocity is diminished.The systolic values remain at baseline or is even slightlyincreased. This yields a significant widening of thepulsatile flow, a feature typical for young people withnormal regulatory responses [15].
First, we evaluated our models ability to reproducethe dynamics during steady state (i.e., during sitting,for t ≤ 60 sec.). We applied initial parameter valuesfrom physiological considerations as described above.
Then, we fitted our model (without including equationsthat describe resistances of large arteries as non-linearfunctions of pressure (9) equations that describe activecontrol (13) and (19)) to the data-set. The duration ofthe cardiac cycles was obtained from the ECG, seeFig. 7. Simulation results are shown in Fig. 5. This figureshows that we have obtained an excellent agreementbetween our model and the data during steady state.However, note that our model is not able to resolvedetails the secondary oscillations observed within eachcardiac cycle, see Fig. 5B, a feature that at present is not

15
included in our heart model.The second step in validating our model is to illustrate
that we can model effects of venous pooling after stand-ing up. Venous pooling results in dramatic reductions ofboth cerebral blood flow velocity and arterial pressure,see Fig. 8. This figure shows that with the parameterslisted in Tables I and II it is possible to decreaseboth blood flow velocity and pressure. Two observationsshould be noted. First, while we did not include effectsof the control, we still see an increase in heart rate,because heart rate information is obtained from the data,see Fig. 7. Second, even though both blood flow velocityand pressure drops, immediately after standing (at t = 60sec.) the pulse amplitude for both blood flow velocity andpressure remain very narrow.
Next, we demonstrate the impact of the nonlinear rela-tionship between pressure and the vascular resistance ofthe large arteries as described in Section II-C, i.e., we letRal(p̄au), Rau(p̄a), Rac(p̄a), and Raf (p̄a) be functionsof pressure. Using the same values for all remainingparameters, the result of this simulation is shown inFig. 8B. Note that the pulse pressure amplitude is higherimmediately after standing (from 60 ≤ t ≤ 65 sec.)and thus the model better represents measured values(compare dark lines in Fig. 8A and B in the transitionregion, for 60 ≤ t ≤ 65 sec.).
The third step is to incorporate all active controlmechanisms. Results that include effects of both auto-nomic regulation and autoregulation are shown in Fig. 9.Our model is able to predict the change in the overallprofile during the transition from sitting to standing. Theonly minor difference is that the data include a slightovershoot in pressure while the subject stands up.
Autonomic regulation was included using a modelthat predicts parameters as a function of pressure. Whilethis method does not incorporate effects of sympatheticversus parasympathetic activation it does include neteffects of neurogenic regulation. In future work, weplan to develop a model that separates sympathetic andparasympathetic responses. Effects of cerebral autoregu-lation are modeled using the empirical model describedin equation (19). We have chosen to include 26 points torepresent the dynamics of the cerebral vascular resistanceRacp, see Figs. 6. This figure shows that Racp decreasesdue to autoregulation as a response to the decrease inpressure. From earlier work [27] we expected an initialincrease before the decrease, however, the model usedin our previous work was much simpler than the modelused in the current work. In particular, the parameterthat represent the peripheral resistance Rp in [27] lumpsthe peripheral resistance from the entire body, i.e., itcombines Racp, Raup, Rafp, and Ralp. Consequently, it
can be difficult to use Rp to describe the dynamics ofthe cerebrovascular resistance Racp, as we attempted todo in [27].
The resistance of the upper body Rau was alsomodeled using a piecewise linear model with unknownparameters as described by (19). We expected that Rau
may depend both on autonomic regulation and be a non-linear passive function of pressure. This resistance doesfollow trends predicted by remaining resistances thatrepresent the large arteries, see Fig. 2. Hence, in futurework we plan to model this resistance using the passivenon-linear model discussed in Section II-C.
Finally, Fig. 10 depicts the dynamics of some ofthe controlled variables. The figure shows the arterialresistance Raup, the cardiac contractility of the left ven-tricle clv , and the venous compliance in the upper bodyCvu. These results do display quite different dynamicsof the three types of variables. In particular, note thatthe compliance and peripheral resistance do not reach asteady state during the 10 sec. following the transitionfrom sitting to standing (from 80 ≤ t ≤ 90 sec.). Thismay be caused by the fact that the dynamics that changethe ventricular contractility occurs over a much fastertime-scale than changes that affect resistances and com-pliances. Finally, it should be noted that the dynamics ofother resistances, capacitors, and atrial contractility aresimilar to the parameters shown in this figure.
VII. CONCLUSION
In summary, we have developed a 11 compartmentalmodel that can predict cerebral blood flow velocity andfinger blood pressure. This model includes physiologicaldescription of dynamics as a response to hydrostaticpressure changes obtained during postural change fromsitting to standing. Furthermore, our model includesnon-linear functions describing resistances of the largesystemic arteries as functions of pressure. To regulateblood pressure and cerebral blood flow velocity follow-ing postural change from sitting to standing, our modelincludes autonomic regulation using first-order differen-tial equations regulating cardiac contractility, peripheralresistance, and vascular tone (compliance). Furthermore,we have included an empirical model describing thedynamics of cerebral vascular resistance. Validation ofour model against one dataset showed that, by includingthe mechanisms described above our model is able toreproduce the dynamics of blood flow velocity and bloodpressure needed to compensate for hypotension observedduring postural change from sitting to standing.
Modeling of physiological responses to standing en-ables a better understanding of physiological mechan-

16
A
45 50 55 60 65 70 75 80 85 90
50
100
150
paf [
mm
Hg]
45 50 55 60 65 70 75 80 85 900
50
100
vacp
[cm
/s]
B
45 50 55 60 65 70 75 80 85 90
50
100
150
paf [
mm
Hg]
45 50 55 60 65 70 75 80 85 900
50
100
time [sec]
vacp
[cm
/s]
Fig. 8. Cerebral blood flow velocity (vacp(t) [cm/sec]) and arterial finger blood pressure (paf (t) [mmHg]) for 45 ≤ t ≤ 90. This figureshows the effect of standing up without including active control mechanisms. A shows that both blood flow velocity and blood pressure(dark lines) decrease due to the redistribution of volumes obtained by changes in hydrostatic pressure. This graph is obtained by solvingequations of the form (2), where gravity is included as shown in (11). B shows the effect of including nonlinear functions of pressure forlarge arterial resistances as described in (9). Note, immediately after standing (from 60 ≤ t ≤ 65 sec.) the pulse-pressure is much wider. Inboth figures the dark lines represent the simulated model results while the light grey lines represent the data.
45 50 55 60 65 70 75 80 85 90
50
100
150
paf [
mm
Hg]
45 50 55 60 65 70 75 80 85 900
50
100
time [sec]
vacp
[cm
/s]
Fig. 9. Autonomic regulation and cerebral autoregulation of arterial finger blood pressure paf (t) [mmHg] and cerebral blood flow velocityvacp(t) [cm/sec] for 45 ≤ t ≤ 60. This figure shows that our model is able to reproduce data well, as before dark lines represent modelsimulations while the underlying light grey lines represent the data. This graph is obtained by solving cardiovascular equations of the form(2), including gravity as described in (11), passive resistances (9), and autonomic and autoregulatory (13) and (19). Notice, the main region,where the model does not capture the dynamics of the data is just before returning to steady state during standing, i.e., for t ≈ 80 sec.

17
45 50 55 60 65 70 75 80 85 902.5
3
3.5
4
4.5
5
Rau
p [m
mH
g se
c/cm
3]
45 50 55 60 65 70 75 80 85 905
6
7
8
9
10
11
12
13
14
15
clv
[mm
Hg/
sec]
45 50 55 60 65 70 75 80 85 909
10
11
12
13
14
15
16
17
time [sec]
Cvu
[cm
3 /mm
Hg]
Fig. 10. Dynamics of the controlled variables. The figure shows the peripheral resistance in the upper body Raup(t) [mmHg sec/cm3], thecardiac contractility of the left ventricle clv(t) [mmHg/sec], and the compliance of the veins in the upper body Cvu(t) [cm3/mmHg], for45 ≤ t ≤ 90. These results are obtained by solving (13) together with equations for the cardiovascular system (2). Autonomic regulationyields increase in peripheral resistance, cardiac contractility and vascular tone. The latter yields a decrease in compliance as shown on thefigure. The timing of the different controls vary, especially, note that the cardiac contractility changes faster than resistances and capacitors.Regulation of the remaining resistances, contractility, and compliances showed similar responses.

18
imsms underlying disorders related to orthostatic tol-erance, e.g., orthostatic hypotension and syncope. Ourmodel predicts that in the absence of regulatory mecha-nisms (as shown in Fig. 8) blood pressure and blood flowvelocity declined upon standing up, and did not recoverto baseline in the upright position. This modeling resulthas not been validated against data. However, similar re-sponses have been observed clinically. For example, sus-tained blood pressure reduction in the upright position isseen in clinical syndromes with orthostatic hypotensionassociated with autonomic failure [16], [17]. Differentetiologies and severity of autonomic failure may leadto differences in pathophysiological responses duringstanding up. For example, severe peripheral autonomicfailure, such as pure autonomic failure or diabetic neu-ropathy, may be associated with orthostatic hypotensionwith no heart rate increment. Cerebral autoregulationthat maintains cerebral perfusion over a wide range ofpressure [25] may be preserved, expanded or reduced inorthostatic hypotension. However, cerebral blood flowwould decline with impairment of autoregulation and/orwhen blood pressure is diminished below the autoreg-ulated range. A transient impairment of autonomic andcerebral blood flow control is common in young peoplewith vasodepressor syncope. This is associated with awithdrawal of sympathetic tone followed by a decline ofblood pressure and cerebral perfusion [9], [22], [24].
Furthermore, our results show that by including pas-sive nonlinear responses of resistances in the large ar-teries we can obtain sufficient widening of the pulsepressure amplitude observed immediately after standingup. This response is immediate, and is thus not aregulatory response, but rather a purely passive responsethat occurs due to the nature of the underlying fluiddynamics. In the current work we described an elaboratemodel for predicting effects of hydrostatic changes,even though this model was only validated for sit-to-stand, i.e., cos(ψ) = 1. The advantage of the modelderived in the present paper is that it may be applicableto predict hydrostatic effects observed during tilt-tableexperiments. This is a topic that we plan to explorefurther in future work.
The main accomplishment of this work is that ourmodel describes how autonomic regulation and cerebralautoregulation play a synergistic role in the control of ar-terial blood pressure and cerebral blood flow velocity. Inparticular it should be noticed that the cerebral resistancefirst decreases, then increases during active standing.This result is different from previous findings in [27],that suggested an initial increase followed by a decrease.However, the new result is not surprising, since thecurrent study is performed with a more complex closed-
loop model. The main advantage of the closed-loop 11compartmental model presented in this study is that thecerebrovascular resistance offers a more accurate repre-sentation of the brain, which does not include aspectsof the rest of the body. For example, previous work [27]used the measured pressure as an input and included onlyone compartment. Hence, the peripheral resistance wasnot distinguished between resistance of the body and thebrain. Furthermore, it should be noticed that the curvefor Racp display hysteresis effects: Immediately afterstanding the decrease of Racp is faster, than the increase,observed for t ≥ 70 during the phase where blood flowvelocity is returning to its normal value. Hysteresis invascular resistance in response to decreasing and increas-ing pressures may reflect differences between cerebraland peripheral vasculature that account for time lagsbetween central and peripheral responses. With normalautoregulation, blood flow velocity precedes changes inperipheral blood pressure, reflecting local adjustmentsto intracranial pressure [26]. In future work we plan tostudy these effects in more detail, by proposing a phys-iological model for autoregulation, separating effects oflocal regulation and autonomic regulation. Finally, itshould be noticed that to obtain a blood flow velocityduring standing that is equivalent to sitting, the resistancereaches a set-point that is higher during standing thanduring sitting.
Results for parameters representative of autonomicregulation shows that theese parameters react as ex-pected: peripheral resistance and cardiac contractilityincreases, while compliance decreases, see Fig. 10. Asdescribed in our results the contractility increases muchfaster than the peripheral resistance. This could be dueto the more rapid effects of parasympathetic withdrawalacting on contractility, compared to sympathetic activa-tion, which has a later effect on contractility, peripheralresistance, and compliance. In future work, we plan touse these observations to develop a physiological modelthat can predict autonomic regulation by introducing sep-arate models of both sympathetic and parasympatheticresponses.
Finally, the optimized parameters depend both on theinitial estimates and on the optimization algorithm. Inparticular, it should be noted that some of the maxi-mum values for the resistances and compliances havelarge values, which are physiologically unrealistic. Inthe future, more work will be done to estimate theunknown parameters that lie within physiological ranges.One approach would be to bound the parameters withinlower and upper limits. This would lead to a constrainedoptimization problem, which is more difficult to solvethan the unconstrained problem used for the investigation

19
reported in this paper. Furthermore, we plan to improvethe parameter identification method so that it becomesfeasible to use the proposed model to analyze datasetsfrom a larger population of people. In particular, weplan to use the proposed model to study the effectsof aging and cardiovascular diseases on autonomic andautoregulatory responses to postural change.
VIII. ACKNOWLEDGMENTS
This work was supported by a US Austria-DenmarkCooperative Research: Modeling and Control of theCardiovascular-Respiratory System Grant 0437037 fromthe National Science Foundation (NSF). Work performedat Beth Israel Deaconess Medical Center General Clin-ical Research Center was supported by the NationalInstitute of Health (NIH) under grants M01-RR01302,R01 NS045745-01A2, and P60 AG08812. Laura Ellwein(MS) was supported by a predoctoral NRSA trainingaward supported by TR32-AG023480 and a SAMSIgraduate fellowship. Data collection and analysis wassupported by a Joseph Paresky Men’s Associates grantfrom the Hebrew Rehabilitation Center for Aged, a Re-search Nursing Home Grant AG04390 and AlzheimersDisease Research Center Grant AG05134. Hien Tran wassupported in part by the National Institute of Health(NIH) under grant RO1 GM067299-03.
APPENDIX
The complete system of differential equations neededto describe all flows and pressures shown in Fig. 1consist of 11 ordinary differential equations. For each ofthe 9 compartments that represent the arteries and veinswe obtain differential equations of the form (2). These9 equations are given by
Cadpa
dt= qav − qac − qaf − qau − pa
dCa
dt
Caudpau
dt= qa − qal − qaup − pau
dCau
dt
Caldpal
dt= qau − qalp − pal
dCal
dt
Cafdpaf
dt= qa − qafp − paf
dCaf
dt
Cacdpac
dt= qac − qacp − pac
dCac
dt
Cvldpvl
dt= qalp − qvl − pvl
dCvl
dt
Cvudpvu
dt= qvl + qaup − qvu − pvu
dCvu
dt
Cvdpv
dt= qvu + qafp + qvc − qv − pv
dCv
dt
Cvcdpvc
dt= qacp − qvc − pvc
dCvc
dt,
where each of the flows are determined using Kirchoff’scurrent law. The list of flows are given by
qav =plv − pa
Rav
qau =pa − pau
Rau
qal =pau − pal − ρgh
Ral
qaf =pa − paf
Raf
qac =pa − pac
Rac
qaup =pau − pvu
Raup
qalp =pal − pvl
Ralp
qafp =paf − pv
Rafp
qacp =pac − pvc
Racp
qv =pv − pla
Rv
qvu =pvu − pv
Rvu
qvl =pvl − pvu + ρgh
Rvl
qvc =pvc − pv
Rvc
qmv =pla − plv
Rmv.
Finally, differential equations for the two compartmentsthat represent the left atrium and ventricle are given by
dVlv
dt= qmv − qav
dVla
dt= qv − qmv.
For these compartments, pressures are computed usingthe heart model discussed in Section II-B.
REFERENCES
[1] Aaslid R. and Markwalder T.M. and Nornes H. Noninvasivetranscranial Doppler ultrasound recording of flow velocity in basalcerebral arteries J Neurosurg 57:769-774, 1982.
[2] Aaslid R. Cerebral hemodynamics. In Newell DW, Aaslid R(eds), Transcranial Doppler, Raven Press, New York, 49-55, 1992.
[3] Beneken J.E.W. and DeWit B. A physical approach to hemody-namic aspects of the human cardiovascular system. In Guyton ACand Reeve EB (eds), Physical Basis of Circulatory Transport:Regulation and Exchange. Philadelphia, PA: Saunders, 1966, pp.1-45, 1966.
[4] Bullock J. and Boyle J. and Wang M. Physiology. 4th ed.Philadelphia: Lippincott Williams & Wilkins, 2001.

20
[5] Danielsen M. Modeling of feedback mechanisms which controlthe heart function in a view to an implementation in cardiovascu-lar models. PhD Thesis, Roskilde University, Denmark. Text No358, 1998.
[6] Danielsen M. and Ottesen J.T. Describing the pumping heart asa pressure source. J Theor Biol 212:71-81, 2001.
[7] Guyton A.C. and Hall J.E. Textbook of medical physiology. WBSaunders, Philadelphia, PE, 9th ed, 1996.
[8] Heldt T. and Shim E.B. and Kamm R.D. and Mark R.D.Computational modeling of cardiovascular response to orthostaticstress. J Appl Physiol, 92:1239-1254, 2002.
[9] Kaufmann H. Syncope. A neurologist’s viewpoint. CardiologyClinics, 15(2):177-194, 1997.
[10] Kappel F. and Peer R.O. A mathematical model for fundamentalregulation processes in the cardiovascular system. J Math Biol,31:611-631, 1993.
[11] Kappel F. and Lafer S. and Peer R.O. A model for thecardiovascular system under an ergometric workload. Surv MathInd, 7:239-250, 1997.
[12] Kappel F. and Batzel J.J. Survey of research in modelingthe human respiratory and cardiovascular systems. In R.C. Smithand M.A. Demetriou (eds) Research Directions in DistributedParameter Systems, SIAM, Philadelphia, PE, pp. 187-218, 2003.
[13] Kelley C. Iterative methods for optimization. SIAM, Philadel-phia, PE, 1999.
[14] Landau L.D. and Lifshitz E.M. Fluid mechanics. PergamonPress, Oxford, 2nd ed, pp. 57, 1993.
[15] Lipsitz L.A. and Mukai S. and Hamner J. and Gagnon M. andBabikian V. Dynamic regulation of middle cerebral artery bloodflow velocity in aging and hypertension. Stroke, 31(8):1897-1903,2000.
[16] Low P.A. Autonomic nervous system function. J Clin Neuro-physiol, 10(1):14-27, 1993.
[17] Low P.A. and Bannister R.G. Multiple System Atrophy andPure Autonomic Failure. In: Low P.A.(eds). Clinical AutonomicDisorders. Lippincott-Raven Publishers, Philadelphia, PE, pp.555-575, 1997.
[18] Low P.A. and Novak V. and Spies J.M. and and Petty G.Cerebrovascular regulation in the postural tachycardia syndrome(POTS). Am J Med Sci, 317(2),124-133, 1999.
[19] Melchior F.M. and Scrinivasen R.S. and Charles J.B. Mathe-matical modeling of the human response to LBNP. Physiologist,35 Suppl1:S204-S205, 1992.
[20] Melchior F.M. and Scrinivasen R.S. and Clere J.M. Simulationof cardiovascular response to lower body negative pressure from0 mmHg to -40 mmHg. J Appl Physiol, 77:630-640, 1994.
[21] Neumann S. Modeling acute hemorrhage in the human car-diovascular system. PhD thesis, University of Pennsylvania, PA,1996.
[22] Njemanze P.C. Cerebral circulation dysfunction and hemody-namic abnormalities in syncope during upright tilt test. Can JCardiol, 9(3):238-242, 1993.
[23] Noordergraaf A. Circulatory system dynamics. Academic Press,New York, NY, pp. 24, 1978.
[24] Novak V and Honos G and Schondorf R. Is the heart ’empty’at syncope? J Auton Nerv Syst, 60:83-92, 1996.
[25] Novak V and Novak P and Spies J.M. and Low P.A. Cerebralblood flow autoregulation in orthostatic hypotension. Clin AutonRes, 7:238, 1997.
[26] Novak V and Yang A.C.C. and Lepicovsky L. and Gold-beger A.L. and Lipsitz L.A. and Peng C.K. Multimodal pressure-flow method to assess dynamics of cerebral autoregulation instroke and hypertension. BioMed Eng Online, 3(1):39, 2004.
[27] Olufsen M.S. and Nadim A. and Lipsitz L.A. Dynamics ofcerebral blood flow regulation explained using a lumped parametermodel. Am J Physiol, 282:R611-R622, 2002.
[28] Olufsen M.S. and Nadim A. On deriving lumped models forblood flow and pressure in the systemic arteries. Math Biosci Eng,1:61-80, 2004.
[29] Olufsen M.S. and Tran A and Ottesen J.T. Modeling cerebralblood flow control during posture change from sitting to standing.Cardiovasc Eng, 4(1):47-58, 2004.
[30] Ono K. and Uozumi T. and Yoshimoto C and Kenner T. Theoptimal cardiovascular regulation of the arterial blood pressure.In Kenner T, Busse R, Hinghofer-Szalkay (eds), Cardiovascularsystem dynamics; Model and measurements. Plenum Press, pp.119-139, 1982.
[31] Ottesen J.T. Modeling of the baroreflex-feedback mechanismwith time-delay. J Math Biol, 36:41-63, 1997.
[32] Ottesen J.T. Nonlinearity of baroreceptor nerves. Surv MathInd, 7:187-201, 1997.
[33] Ottesen J.T. and Danielsen M. Modeling ventricular contractionwith heart rate changes. em J Theor Biol, 222:337-346, 2003.
[34] Panerai R.B. Assessment of cerebral pressure autoregulationin humans - a review of measurement methods. Physiol Meas,19:305-338, 1998.
[35] Rideout V. Mathematical and computer modeling of physiolog-ical systems. Medical Physics Publishing, 1991.
[36] Serrador J.M. and Picot P.A. and Rutt B.K. and Shoemaker J.K.and Bondar R.L. MRI measures of middle cerebral artery diam-eter in conscious humans during simulated orthostasis. Stroke,31:1672-1678, 2000.
[37] Smith J.J. and Kampine J.T. Circulatory physiology, theessentials. Williams and Wilkins, Baltimore, MD, 3rd ed, 1990.
[38] Tiecks F.P. and Lam A.M.and Aaslid R. and Newell D.W.Comparison of static and dynamic cerebral autoregulation mea-surements. Stroke, 26:1014-1019, 1995.
[39] Ursino M. and Lodi C.A. Interaction among autoregulation,CO2 reactivity, and intercranial pressure: a mathematical model.Am J Physiol, 43:H1715-H1728, 1998.
[40] Ursino M. Interaction between carotid baroregulation and thepulsating heart: a mathematical model. Am J Physiol, 44:H1733-H1747, 1998.
[41] Warner H.R. The Frequency-dependent nature of blood pressureregulation by carotid sinus studied with an electric analog. CircRes, VI:35-40, 1958.
[42] Warner H.R. Use of analogue computers in the study of controlmechanisms in the circulation. Federation Proc, 21:Jan-Feb, 1962.
[43] Warner H.R. and Cox A. A mathematical model of heart ratecontrol by sympathetic and vagus efferent information. J ApplPhysiol, 17:349-358, 1962.
[44] Wesseling K.H and Stettels J.J. and Walstra G. and VanEsch H.J. and Donders J.H. Baromodulation as the cause of shortterm blood pressure variability. In Alberi G, Bajzer Z, Baxa P(eds), Application of physics to medicine and biology. WorldScientific, pp.247-276, 1982.