
Bleeding during pregnancy
70
Early Pregnancy Bleeding
-
Upload
manalhaija -
Category
Health & Medicine
-
view
77 -
download
3
Transcript of Bleeding during pregnancy

Early Pregnancy Bleeding
Abortion Abortion: ending of the pregnancy before 20
weeks of gestation. Expulsion of the uterine contents either spontaneously or induced before the point of viability 24 or 20 weeks and weight less than 500g.
Incidence: 10-15% of all pregnancies. The majority of spontaneous abortion occur between the 8th and 12th weeks when the level of progesterone secreted by the corpus luteum falls and the placental hormone has not reached a sufficiently high level to sustain the conception.
Causes
Maternal causes: Rh incompatibility and ABO
incompatibility. Defective ovum or sperm. Endocrine deficiencies. Abnormalities of maternal reproductive
organ ( bicornate uterus). Chronic illness, nutritional deficiencies,
and acute infections. Uterine fibriods.

Fetal causes: Chromosomal abnormalities. Poor implantation.

Types of abortion Threatened Miscarriage Inevitable Miscarriage Incomplete Miscarriage Complete Miscarriage Missed Miscarriage Septic Miscarriage Habitual Miscarriage Therapeutic Abortion

Threatened Miscarriage Threatened miscarriage affects one in five
pregnancies. Signs & SymptomsCervical os close , membrane intact ,mild
cramping ,spotting of blood. Management bed rest ,sedative , avoid sexual intercourse,
good observation for amount of bleeding ,V/S , check fetal H.R . Give Anti D within 72 hrs if indicated.
Although there is no definite evidence that bed rest can affect the course of pregnancy abstinence from active environment for a couple of days may help women feel safer

Inevitable Miscarriage
Signs & SymptomsModerate cramping, moderate to sever amount of bleeding ,cervical os dilated and membrane bulging.
Bed rest, sedation, blood transfusion may be indicated, observe amount of bleeding, color, give anti D if indicated.
Incomplete Miscarriage S&S Parts of the products of conception are expelled ( fetus expelled from uterus placenta and membranes are still inside ), severe
bleeding ,cervical os open, severe pain. Management V/S, sedation, bed rest.May or may not additional dilation needed before
curettage (D&E) .Anti D if indicated .
Complete Miscarriage
S&SAll contents expelled without assistance, minimal bleeding ,cervix is closed and
uterus is empty ,pain is stopped. Management
No further interventions needed.
Anti D if indicated .

Missed Miscarriage S&SFetus dies and retained in uterus, signs of pregnancy disappear, pregnancy test negative, fundal height not increase in size, FHR absent, cervix os is closed, ultrasound confirm fetal death ,may spotting blood present ManagementIf spontaneous evacuation of uterus not occur within one month, pregnancy is terminated .blood clotting factors are monitored ,DIC may develop in cases of fetal death after 12th weeks ,if products of conception are retained for longer than 5 weeks .D&C or misoprostol is the treatment.Mother may develop hypofibrinogenaemia.
Septic Miscarriage S&SFever ,abdominal tenderness, vaginal bleeding
and chills, Nausea, Vomiting. ManagementAntibiotics , clinical bacteriological and
hematological investigation to identify the infectious organism ,electrolyte control ,the pads correctly collected and discarded ,accurate observation of temp & Bp
Habitual miscarriage
When women have three or more consecutive spontaneous abortion.
May due to:
Cervical incompetent ,poor nutritional status, hormonal disturbance, defective ova or spermatozoa, RH incompatibilityPain and bleeding are absent or minimal.
Recurrent premature dilation of the cervix
(Incompetent cervix)
Passive and painless dilation of cervix os without labor or contraction of uterus. it occurs in second or early in third trimester. As a result miscarriage or preterm birth
may occur .

Etiology
Etiologic factors include : hx of previous cervical trauma such as laceration during childbirth ,excessive cervical dilation for curettage or biopsy ,congenitally short cervix ,cervical or uterine anomalies. exposed to the drug diethylstilbestrol (DES) by the woman’s mother while pregnant with the woman.
Diagnosis Diagnostic criteria for U/S are:1-short cervix (less than 20 mm in length ).2- effacement 30%-40% of the internal Os of the cervix. Management1. Bed rest , hydration ,progesterone ,anti-inflammatory
drugs and antibiotics. McDonald (cervical cerclage) procedure done .it is performed in 11-15 week ,not done after 25 week because of complications such as PROM ,preterm labor ,and chorioamnionitis
2. Post op and follow up care include :observe for S&S of infection ,uterine contraction ,ROM ,educate women about importance of limited activity and signs of complications .
3. Anti D.


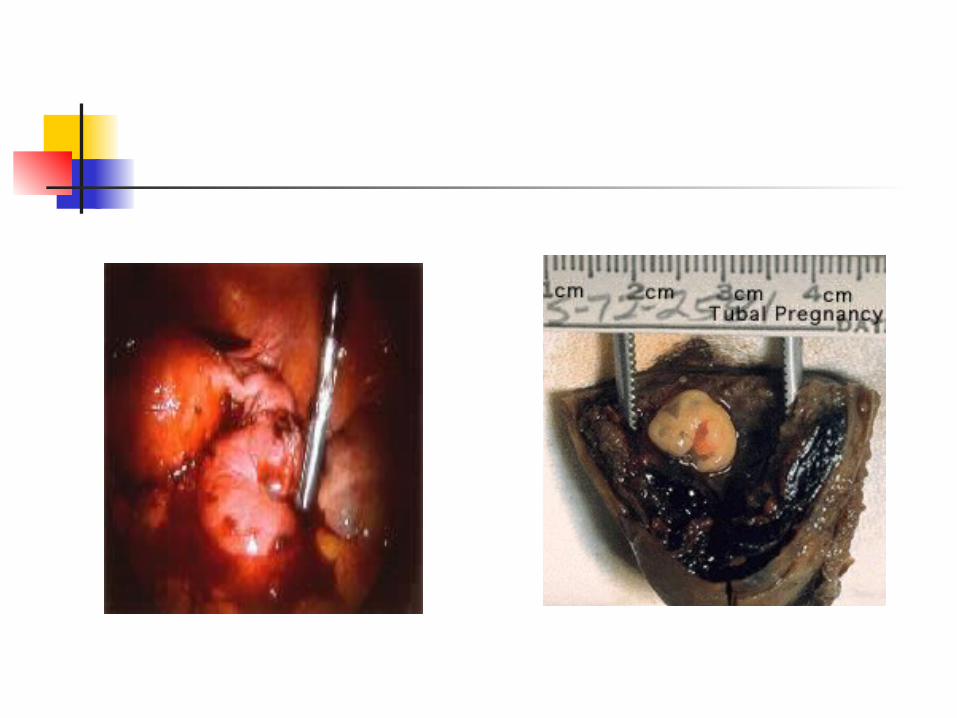
Ectopic pregnancy
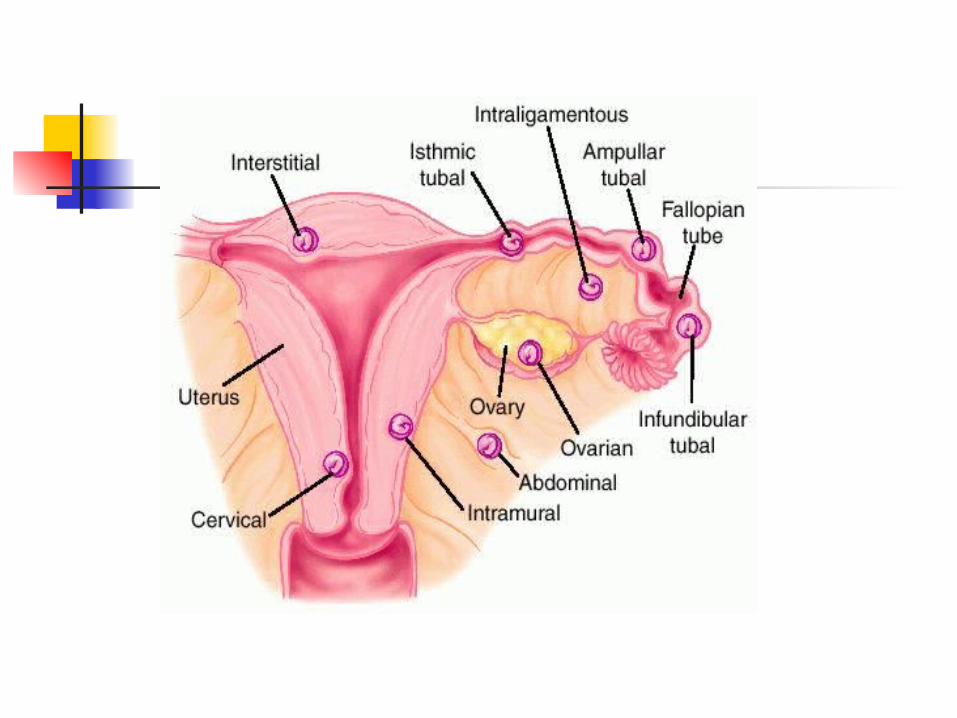
Ectopic pregnancy refers to an abnormal implantation of the fertilized ovum outside the uterine cavity.
Approximately 95% of ectopic pregnancy occur in the uterine ( fallopian) tube, with most located on the ambullar portion. Other sites include the abdominal cavity (3-4%), ovary (1%), and cervix (1%).

Risk Factors
1. previous ectopic pregnancy, tubal damage from infection or surgery, history of infertility, treatment for in vitro fertilization, increased age, and smoking.
2. history of pelvic inflammatory disease is particularly important after acute salpingitis the incidence of ectopic pregnancy increased
sevenfold.


The incidence of ectopic pregnancy is increasing but mortality is decreasing due to better diagnostic methods and technology.
Incidence about 2% (medscape, 2010) Ectopic pregnancy is responsible for
10% of all maternal mortality, and it is the leading pregnancy related cause of first trimester maternal mortality.
Moreover ectopic pregnancy is a leading cause of infertility.
Ectopic pregnancy is classified according to site of implantation.
The uterus is the only organ capable of containing and sustaining a term pregnancy.
However, abdominal pregnancy with birth by laparotomy may result in a living infant in 5%-25% of such pregnancies.
Clinical manifestation
A missed period. Adnexal fullness. Tenderness may suggest an unruptured
tubal pregnancy. Tenderness may progress from a dull
pain to a colicky pain when the tube stretches.
Pain may be unilateral, bilateral, or diffuse over the abdomen.

Dark red or brown abnormal vaginal bleeding occurs in 50%-80% of women.
If ectopic pregnancy ruptures, pain increases. Pain may be generalized, unilateral, or acute deep lower quadrant pain caused by blood irritating the peritoneum.
Referred shoulder pain can occur as a result of diaphragmatic irritation caused by blood in the peritoneal cavity.

An ecchymotic blueness around the umbilicus (Cullen’s sign), indicating hematoperitoneum. May develop in an undiagnosed ruptured intraabdominal ectopic pregnancy.
The woman may exhibit signs of shock related to the amount of bleeding.

Assessment and management
The differential diagnosis of ectopic pregnancy involves consideration of numerous disorders that share many signs and symptoms.
Miscarriage, appendicitis, salpingitis, ovarian cysts, UTI.
Laboratory screening includes determination of serum progesterone and beta hCG levels.
The woman is also undergo transvaginal ultrasound to confirm intrauterine or tubal pregnancy.

Management of tubal pregnancy depends on whether the tube is intact or ruptured.
If the tube is intact and hCG levels are declining, its indicate spontaneous regression of the tubal pregnancy.
Methotrexate is a folic acid analogue that destroys the rapidly dividing cells, may be used in a single dose intramuscular injection to treat unruptured pregnancies.
The primary reason for medical management is preserving the fallopian tube to increase the chance of future pregnancy.
Methotrexate therapy avoids surgery and is a safe, effective.

The Medical Management of Ectopic Pregnancy: A Meta-analysis Comparing "Single Dose" and "Multidose" Regimens
The overall success rate for women treated with methotrexate for an ectopic pregnancy was 89%. The single dose was much more commonly used. The use of single dose was associated with a significantly greater chance of failed medical management than the use of the multidose. The single-dose regimen was associated with fewer side effects. Women who experienced side effects were more likely to have successful treatment regardless of regimen.(Kurt, 2003)
Surgical management of an unruptured tubal pregnancy involve salpingostomy.
Salpingectomy is performed when the tube is ruptured to control bleeding and prevent hypovolemic shock.
If internal bleeding is present, assessment may reveal vertigo, shoulder pain, hypotension, and tachycardia.
If surgery is planned, general preoperative and postoperative care.
Blood transfusion may be necessary.
Anti D. IV fluid, electrolytes.

Future pregnancy can occur with one tube remaining.
Future fertility should be discussed.
Increased risk for recurrent ectopic pregnancy.

Gestational Trophoblastic Disease

Gestational trophoblastic disease includes hydatidiform mole, invasive mole, and choricarcinoma.
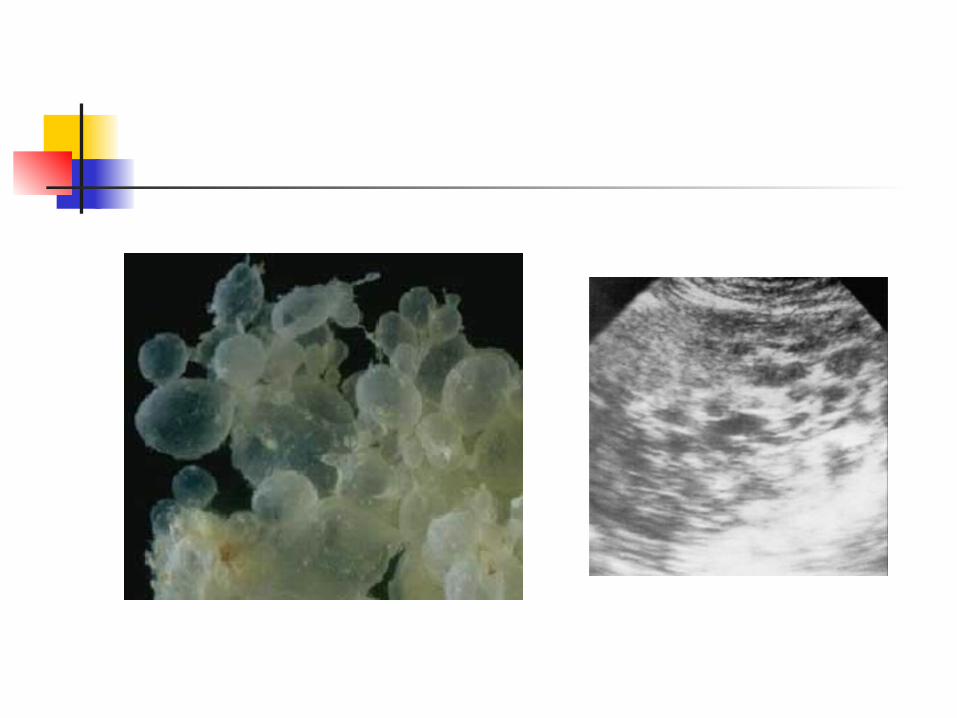
hydatidiform mole (molar prenancy) is a condition in which the trophoblastic tissue proliferates and the chorionic villi of the placenta become swollen and fluid filled, taking on the appearance of grapelike clusters.
The etiology is unknown, although there may be an ovular defect or nutritional deficiency.
Higher risk who have undergone ovulation stimulation with clomiphene., early teens, older than 40 years.
The risk of a second mole is 1%- 2%.

Risk of recurrent hydatidiform mole and subsequent pregnancy outcome following complete or partial hydatidiform molar pregnancy
Overall recurrence risk for molar pregnancy was 1.8%.
is about 1 in about 1 in 60 and if this were to
occur, the majority of cases will be of the same type of mole as the preceding pregnancy. (Sebire, 2003).
Molar pregnancy and husband’soccupation: do soil and dust haveany role?
Comparing all occupations that had exposure to soil and dust with all those who did not have this exposure (physical and non-physical) resulted in a statistically significant difference in the occurrence of molar pregnancy. (Milani,2008)
Types Complete mole: results from fertilization
of an egg with a lost or inactive nucleus. The nucleus of a sperm duplicates itself.
The hydropic vesicles grow rapidly, causing the uterus to be larger than expected for the duration of the pregnancy.
Complete mole contains no fetus, placenta, amniotic membranes, or fluid.
20 %of cases progression toward choricarcinoma.

Partial mole results of two sperm fertilizing an apparently normal ovum.
karyotype of 69,XXX; 69,XXY;69,XYY. Partial mole often have embryonic or
fetal parts and an amniotic sac. Congenital anomalies are usually present.

Clinical manifestations Complete mole cannot be
distinguished from those of normal pregnancy.
Vaginal bleeding occurs later in almost 95% of cases.
The vaginal discharge may be dark brown (prune juice) or bright red, either scant or profuse, continuing for only a few days or intermittently for weeks.

Clinical manifestations Anemia from blood loss. Excessive nausea and vomiting. Abdominal cramps--- uterine distention. Preeclampsia in 15% of causes usually
between 9-12 weeks of gestation. Hyperthyroidism, pulmonary embolism . Partial mole cause few of these
symptoms and may be mistaken for an incomplete or missed miscarriage.

Management Serial beta hCG levels and ultrasound
are the primary diagnostic tools. Treatment begins with evacuation of
the mole. Anti D. Follow up includes frequent physical
and pelvic examination along with biweekly measurement of beta hCG level until the level decrease to normal and remains normal for 3 weeks.
Monthly measurements are taken for 6 months and then every 2 months for a total of 1 year.
A rising titer and enlarged uterus may indicate choriocarcinoma.
Chemotherapy may be started.

Bleeding In Late Pregnancy

Placenta Previa
Placenta previa occurs when the placenta abnormally implants near or over the cervical os instead of in the fundus of the uterus.
Placenta previa occurred in approximately 1 in 200 live births (2007).


Risk factors Defective vascularity of the decidua. previous infection in the upper uterine
segment. Uterine scarring from previous C/S. Previous placenta previa. Endometritis. Multifetal gestation.
Because the lower uterine segment is not as well vascularized as the upper segment, the placenta must cover a large area for adequate function.
Types of placenta previa
Complete: the internal os is completely covered by the placenta.
Partial: incomplete cover of the internal os.
Marginal: only an edge of the placenta extends to the internal os.
Low lying placenta: placenta is implanted in the lower uterine segment but does not reach the os.

Assessment and management Placenta previa can be diagnosed before
bleeding occurs in the third trimester because of performing routine U/S.
Placenta previa should be suspected with onset of painless bleeding occur after 24 weeks.
Abdominal examination reveals a soft, relaxed, nontender uterus with normal tone.
Painless bleeding results from the separation of the placenta that is near , or covering , the internal cervical os.
Bleeding may be intermittent or in gush. The bleeding can be extensive and can prove to be fatal.

The woman diagnosed with placenta previa must be closely monitored for the amount and character of blood loss.
Vital signs, fetal heart rate, and activity are documented.
PV exam is contraindicated.
Management is depend on the classification of previa and gestational age of the fetus.
If the gestational age is less than 36 weeks and bleeding is slight, the woman is hospitalized for observation.
Blood count, type, cross match are performed.

If bleeding is heavy, an urgent C/S is performed.

complication The main complication is hemorrhage for
the woman and prematurity hypoxia or death of the fetus.
Immediate pp hemorrhage often accompanies this condition because the surface area of attachment is greater than usual and the site of placental implantation in the lower uterine segment dose not contract well after the placenta is expelled.

Dose the number of the previous C/S affect maternal outcome and complication rates?
Dose the number of the previous C/S deliveries affect maternal outcome and complication rates?
(Alchalabi, 2007)
PP infection may also occur because of the closeness of the placental site to the cervix and vagina.

Abruptio placenta
)Premature separation of placenta (is the detachment of part or all of the placenta from its implantation site.
Separation occur in the area of decidua basalis after 20 week of gestation.

Incidence & Etiology 1 in 200 of all pregnancies is
complicated by Abruptio placenta Hypertension is the most
consistently identified risk factor for Abruptio placenta.
cocaine use , Abdominal trauma, smoking ,previous Abruptio placenta, PROM ,Twin gestation.
Placental Abruption and Perinatal Mortality in the United States
Abruption was recorded in 6.5 per 1,000 births. Perinatal mortality was 119 per 1,000 births with abruption compared with 8.2 per 1,000 among all other births.
The high mortality with abruption was due, in part, to its strong association with preterm delivery; 55% of the excess perinatal deaths with abruption were due to early delivery. (Ananth and Wilcox, 2001)
Clinical Manifestations
Vaginal bleeding Abdominal pain Uterine tenderness.

Maternal &Fetal outcomes It is a leading cause of maternal death The mother's prognosis depend on the extent
of placental detachment. ,blood loss ,degree of DIC, time between placental detachment and birth.
Maternal complications: Hemorrhage, hypovolemic shock ,renal failure,
DIC. Fetus complications Death as a result of hypoxia , SGA , preterm
birth .

Management It depends on severity of blood loss and
fetus status. Women with Abruptio placenta not
managed outside hospital . Woman less than 36 week and have
mild Abruptio placenta and fetus not in distress, close observation for S&S of bleeding and labor is needed .other wise the choice of treatment is C/S.

Disseminated intravascular coagulation (DIC)
DIC is a condition in which coagulation defect prevents blood from clotting. This result from overstimulation of the normal coagulation process.
Massive rapid fibrin formation results. This condition causes the widespread appearance of small thrombi in the small blood vessels.
Factors that prevent coagulation and factors that stimulate coagulation are activated at the same time.
Assessment and management Because of the amount of intravascular
clotting, the blood platelets and clotting factors are depleted.
The following clinical problems may occur:
1. Tendency toward generalized bleeding.2. Ischemia of the vital organs caused by
thrombi obstruction in the blood vessels.3. Sever anemia resulting from excessive
bleeding.

It should be suspected in woman with placenta abruptio, retained dead fetus, molar pregnancy, hemorrhagic shock, and septic abortion.
This disorder can often be resolved by correcting the underlying cause which may require termination the pregnancy to stop the production of thromboplastin, administering blood products, monitor V/S, intake and output, administer O2, platelet count and fibrinogen level, replace depleting clotting factors
The nurse should be alert to the S&S of DIC bleeding from gum, epistaxis, and petechiae, provide emotional support.


















