BIOFILMS IN SURGICAL SITE INFECTIONSsoreillydesignportfolio.com/LINKS/digital-design... ·...
16
© 2015 American Academy of Orthopaedic Surgeons 1 KEYWORDS: biofilm; surgical site infection; bacterial life cycle; antibiotic resistance Dr. Shirtliff or an immediate family member has stock or stock options held in difusion. Dr. McLaren or an immediate family member has stock or stock options held in Sonoran Biosciences; has received research or institutional support from Astellas Pharma; has received nonincome support (such as equipment or services), commercially derived honoraria, or other non-research–related funding (such as paid travel) from Synthes, the Research Recovery Institute, Stryker, and Smith & Nephew; and serves as a board member, owner, officer, or committee member of the Musculoskeletal Infection Society and the Arizona Orthopaedic Society. INTRODUCTION The life cycle of infecting microorganisms and their interactions with both the host and each other are important in the understanding of orthopaedic surgical site infections (SSIs). Although this biology is highly complex with intricate molecular details, this chapter presents a functional understanding that is important for clinical practice. Commensal microorganisms coexist on almost all healthy body surfaces that are covered by epithelial cells and exposed to the external environment (integumentary, gastrointestinal, respiratory, and urogenital). 1 These human microbiomes are fre- quently polymicrobial, bacterial, and fungal. The effects that each organism induces on surrounding organisms and the host are collectively considered its extended phe- notype, 2 which is encoded in a self-refining pangenome distributed across multiple strains for each microbial species. 3 The resulting biosystems have diverse symbiotic interactions between microbial communities 4 and the host. In the sustained battle be- tween microbes and the host, microbes encounter innate, adaptive immune respon- ses that prevent infection in most interactions. However, surgical incisions disrupt patient defenses, providing opportunity for SSI. Surgical sites lack the host defenses specific to the locations where commensal organisms exist, and innate immunity is disrupted by tissue injury and hematoma formation. In addition, implanted medical 1 BIOFILMS IN SURGICAL SITE INFECTIONS Mark E. Shirtliff, PhD Alex C. McLaren, MD
Transcript of BIOFILMS IN SURGICAL SITE INFECTIONSsoreillydesignportfolio.com/LINKS/digital-design... ·...

© 2015 American Academy of Orthopaedic Surgeons 1
KEYWORDS: biofilm; surgical site infection; bacterial life cycle; antibiotic resistance
Dr. Shirtliff or an immediate family member has stock or stock options held in difusion. Dr. McLaren or an immediate family member has stock or stock options held in Sonoran Biosciences; has received research or institutional support from Astellas Pharma; has received nonincome support (such as equipment or services), commercially derived honoraria, or other non-research–related funding (such as paid travel) from Synthes, the Research Recovery Institute, Stryker, and Smith & Nephew; and serves as a board member, owner, officer, or committee member of the Musculoskeletal Infection Society and the Arizona Orthopaedic Society.
INTRODUCTIONThe life cycle of infecting microorganisms and their interactions with both the host and each other are important in the understanding of orthopaedic surgical site infections (SSIs). Although this biology is highly complex with intricate molecular details, this chapter presents a functional understanding that is important for clinical practice.
Commensal microorganisms coexist on almost all healthy body surfaces that are covered by epithelial cells and exposed to the external environment (integumentary, gastrointestinal, respiratory, and urogenital).1 These human microbiomes are fre-quently polymicrobial, bacterial, and fungal. The effects that each organism induces on surrounding organisms and the host are collectively considered its extended phe-notype,2 which is encoded in a self-refining pangenome distributed across multiple strains for each microbial species.3 The resulting biosystems have diverse symbiotic interactions between microbial communities4 and the host. In the sustained battle be-tween microbes and the host, microbes encounter innate, adaptive immune respon-ses that prevent infection in most interactions. However, surgical incisions disrupt patient defenses, providing opportunity for SSI. Surgical sites lack the host defenses specific to the locations where commensal organisms exist, and innate immunity is disrupted by tissue injury and hematoma formation. In addition, implanted medical
1 BIOFILMS IN SURGICAL SITE INFECTIONSMark E. Shirtliff, PhDAlex C. McLaren, MD

2 © 2015 American Academy of Orthopaedic Surgeons
devices provide a particularly problematic niche for bacterial growth. Staphylococcus epidermidis and Propionibacterium acnes are commensal organisms that are condition-ally pathogenic when introduced directly into the surgical site via the incision. Com-mensal organisms from sites remote to orthopaedic procedures, such as Enterococcus faecalis in the bowel, are also conditional pathogens for SSI. Pathogenic microorgan-isms such as Pseudomonas aeruginosa or Aeromonas hydrophila, which do not normally coexist on healthy epithelial surfaces, can be introduced directly through the incision from a contaminated surgical field or hematogenously from remote sites.
Progression to infection is determined by the interplay between bacterial virulence, inoculum, the host’s immunologic status, and the presence of an attachment surface. The importance of devitalized tissue and abiotic surfaces in this interplay has long been known. In 1956, Elek5 found that a 106 inoculum of Staphylococcus aureus in the dermis was not sufficient to produce a localized infection, but 7.5 × 106 had a 50% likelihood of causing infection, and as few as 100 S aureus cells on suture material had a 100% likelihood of causing infection. Furthermore, antibacterials were ineffective at clearing the infection without removing the suture. The presence of an abiotic attach-ment surface caused a greater than 75,000-fold increase in the ability of S aureus to cause infection and produced a chronic infection that resisted antimicrobial therapy.
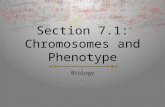
THE BIOFILM MODE OF GROWTHConventional wisdom over the past 150 years focused on planktonic pathogens.6 Isolation in culture, susceptibility to antimicrobials, clinical course, and treatment were all based on the biology of microorganisms thriving individually, free floating in the planktonic phase, inducing acute illness.3 Modern antimicrobial therapy and vaccine development have effectively controlled these diseases in the developed world. Currently, most infections are no longer acute, planktonic phase infections. The US Centers for Disease Control and Prevention and the National Institutes of Health have respectively estimated that 56% and 80% of infections in modern health-care facilities in the United States are associated with biofilms: 17,000,000 infections and 550,000 deaths costing $90 billion annually. Biofilms are polymicrobial, sessile, community-based aggregations within a self-secreted matrix7-9 (Figure 1). Such microbial communities exhibit a radically altered phenotype regarding growth, gene expression, and protein production compared with taxonomically identical microor-ganisms growing planktonically.10,11 Biofilm thickness can vary from a single cell
Let’s Discuss: Surgical Site Infections

© 2015 American Academy of Orthopaedic Surgeons 3
FIGURE 1 Illustration depicts the biofilm life cycle. (Copyright P. Dirckx, Montana State University, Bozeman, MT.)
layer to a thick community of cells. Structural analyses have demonstrated that thick biofilms possess a sophisticated architecture in which microcolonies can exist in dis-crete pillar- or mushroom-shaped structures.12 Between these structures, an intricate network of channels provides access to environmental nutrients.
Planktonic microorganisms are a transient population that replicates successfully only in limited conditions. They are exposed to environmental threats, including host defenses, desiccation, and antimicrobial agents, which limit their survival. Alternatively, biofilms provide a safe environment for microbes and have several advantages over the free-floating lifestyle of planktonic microorganisms. One major benefit is resistance to antimicrobial agents13 and to cellular and humoral host im-mune effectors.14-16 Biofilm-embedded bacteria are up to 1,000 times more tolerant to antimicrobials. Therefore, after a surface is infected, the only successful strategy to resolve the infection is surgical removal of the implant and débridement of the de-vitalized tissue. Another advantage to the biofilm mode of growth is dispersion via detachment. Microcolonies may detach under the influence of fluid mechanical shear or through a genetically programmed response that mediates the detachment pro-cess.17 As a result, growth in the biofilm mode allows an enduring bacterial source
Biofilms in Surgical Site Infections

4 © 2015 American Academy of Orthopaedic Surgeons
population that is resilient to challenge by both antimicrobial agents and the host immune response, simultaneously enabling the continuous shedding that spreads bacteria.
LIFE CYCLE OF A MICROORGANISM
VIDEO 1 Microbial life cycle.Shirtliff ME: Video. Excerpt. Biology of Biofilms. Baltimore, MD, 2015.
Abiotic and devitalized biotic surfaces are quickly coated in host extracellular matrix proteins (collagen, elastin, osteopontin, fibronectin, and fibrinogen). When planktonic microbes encounter a protein-covered surface, they adhere to it and begin replication. Depending on the infecting species, the host is often complicit in the infectious process by promoting an early Th2 cell humoral response (in the case of P aeruginosa) that fails to clear the infecting microbe or an overly activated and misdirected Th1 and Th17 inflammatory response (in the case of S aureus) that causes tissue damage, thereby increasing adhesion surfaces.
As the microbial population increases, quorum-sensing compounds (for example, homoserine lactones of gram-negative bacteria or autoinducing peptides of gram- positive bacteria) reach a threshold. The microbes respond by altering their gene expression to promote biofilm formation in a species-specific manner. Extracellular polymeric substance production is initiated to generate an autogenously produced matrix with a composition that depends on the microbial species and strain. The quorum-sensing system also activates the production of toxins that lyse the lead re-sponse cells of the immune response (such as neutrophils), further contributing to the biofilm mass and localized tissue destruction. Other microbes (strains, species, and kingdoms) are actively incorporated into the biofilm when encountered, increasing its diversity.
As the biofilm thickness expands, nutrients (carbohydrates, nucleic acids, amino acids, and terminal electron acceptors such as oxygen) become limited, reducing the metabolic activity of the biofilm-embedded microbes. At this point, redox and pH homeostasis as well as amino acid and nucleic acid acquisition become priorities.
Let’s Discuss: Surgical Site Infections

© 2015 American Academy of Orthopaedic Surgeons 5
This reduced rate of cell division and low metabolic activity of microbes within the biofilm cause tolerance to antimicrobial agents that inhibit the synthesis of cell walls, DNA, RNA, protein, or folic acid of rapidly dividing microbes. In addition, up to 10% of the microbes within the biofilm population become persister cells. These micro-organisms are a subset of the biofilm population that express almost no metabolic activity, protein production, or replication. Antimicrobials are completely ineffective against these population subsets. Antimicrobial susceptibility progressively reduces as the biofilm becomes progressively more sessile. Antimicrobial agents effectively control the rapidly dividing planktonic populations that cause the clinical manifes-tations; however, the persister cell populations remain. After the antimicrobial levels are reduced, viable persister cells can repopulate the matrix, resulting in reactivation of the infection.
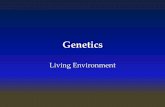
EXTRACELLULAR MATRIXSurface attached microbes produce multiple extracellular polymeric substances that include exopolysaccharides, eDNA, proteins, and lipids. This extracellular matrix, termed slime, acts as a protective physical barrier for the microbes.3 Quantum packets released for intercellular signaling must be transported through the matrix; the ma-trix supports nanotubes that conduct cell-to-cell electric signals (Figure 2). In addi-tion, the microbes are physically stabilized, facilitating the transfer of genetic material.
VIDEO 2 Communication by quorum sensing and electrical signaling through nanotubes.Shirtliff ME: Video. Excerpt. Biology of Biofilms. Baltimore, MD, 2015.
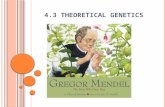
Slime is viscoelastic, providing biofilm the ability to deform and flow in response to mechanical loads, notably to shear from flow in adjacent fluid (Figure 3). The material properties of slime depend on the composition of the extracellular polymeric substance produced by the microbe community.3 Coupled with microbially induced fluid produced by the host, microbe-controlled rheologic properties help determine the biofilm’s three-dimensional morphology (pillars, mushrooms, interconnecting channels).
Biofilms in Surgical Site Infections

6 © 2015 American Academy of Orthopaedic Surgeons
FIGURE 2 Scanning electron microscopic image of polymicrobial biofilm demonstrates nanotubes. (Reproduced with permission from Schaudinn C, Carr G, Gorur A, Jaramillo D, Costerton JW, Webster P: Imaging of endoontic biofilms by combined microscopy [FISH/cLSM-SEM]. J Microsc 2009;235[2]:124-127.)
FIGURE 3 Phase contrast microscopy demonstrates flow-induced movement of a 10-µm clump (white outline). Arrows indicate direction of fluid flow. (Copyright Paul Stoodley, MD, Columbus, OH.)
Let’s Discuss: Surgical Site Infections

© 2015 American Academy of Orthopaedic Surgeons 7
As the biofilm matures, flow induces shear-detached clumps of biofilm-embedded microbes, and the genetically programmed dispersion of single planktonic cells oc-curs. These processes allow the infection to spread to new host niches.
THE DISTRIBUTED PANGENOMEA biofilm can be seen as a collective response to environmental conditions, as though it was a single living “organism.”3 Multiple species, often multiple kingdoms, coexist within close, spatially structured regions that allow more robust signaling and exchange of genetic material through horizontal gene transfer. This exchange occurs at rates more than 10,000 times faster in a biofilm mode of growth than in those between planktonic microbes.
VIDEO 3 Exchange of genetic material in biofilm.Shirtliff ME: Video. Excerpt. Biology of Biofilms. Baltimore, MD, 2015.
The number of new strains with unique combinations of genetic characteristics increases, some with increased survival ability, which prevents the host from build-ing an effective adaptive immune response.3 The genetic material distributed across the many strains in each species and kingdom within the biofilm organism functions as a de facto genome larger than that of any one strain, termed a pangenome.3 The biofilm becomes progressively more advanced in its ability to coexist with the host.
PHENOTYPE AND EXTENDED PHENOTYPEBiofilms are the dominant phase in the life cycle of bacteria and fungi, starting as a single cell attaching to a surface, progressing to mature biofilm over time.
Incipient (Immature) BiofilmSessile biology begins in organisms within 15 minutes of surface attachment.8 When signaling molecules reach a threshold, cell-to-cell communication causes “crowd behavior.” The excretion of extracellular polysaccharide substance, also known as slime, begins. The surface binding becomes irreversible. Cell surface proteins, meta-bolic rate, and replication are still similar to those of planktonic microbes.
Biofilms in Surgical Site Infections

8 © 2015 American Academy of Orthopaedic Surgeons
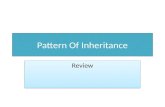
FIGURE 4 Fluorescent staining for glucosaminidase of a cross-section of Staphylococcus aureus biofilm demonstrates heterogeneity. (Reproduced with permission from Brady RA, Leid JG, Kofonow J, Costerton JW, Shirtlift ME: Immunoglobins to surface-associated biofilm immunogens provide a novel means of visualization of methicillin-resistant Staphylococcus aureus biofilms. Appl Environ Microbial 2007;73[20]:6612-6619.)
Mature Biofilm (Sessile)Within 48 hours, the molecular and cellular behaviors of the microbes change with altered expression of cell surface proteins, decreased metabolic activity, and decreased cell replication. Vertical and horizontal heterogeneity develop over time (Figure 4). Thickness increases from a single cell layer to a complex ultrastructure with interconnecting fluid channels, towers, and mushroom formations (Figure 1). Streamers and shedding develop at the surface. Gradients develop in pH, O2 tension, ion concentrations, and nutrients.
Mature Biofilm (Genetic Diversity)Extensive genetic diversity develops over time as horizontal gene transfer across multiple strains of the same species progresses to a pangenome. Incorporation of other bacterial species and fungi establish the polymicrobial nature of many mature biofilms. Biologic behavior of mature biofilm becomes analogous to a multicellular
Let’s Discuss: Surgical Site Infections

© 2015 American Academy of Orthopaedic Surgeons 9
organism with population-level virulence traits that are more resistant to host de-fenses than individual planktonic microorganisms.3
Extended PhenotypeThe propagation and survival of the biofilm is enhanced by changes that the biofilm induces in the local environment and the changes it induces in adjacent host tissues.2 Signaling molecules induce host tissues to increase extracellular fluid (effusions, exudates, edema), thereby increasing the flow of nutrients available to the biofilm.3 Neutrophils are attracted and penetrate the biofilm but their capability for phago-cytosis is lost.8 Biofilm induces local environment pH, O2 tension, and ion concen-trations that are favorable to the biofilm and hostile to the host immune cells. These alterations in the host and the environment are the extended phenotype. The pan-genome of the biofilm ultimately results in these changes even though the molecular pathways in the host are not necessarily exclusive to the biofilm.18
Surface DispersionMicroorganisms near the surface tend to be less sessile when the local environment is less threatening.8 Extensions develop in the fluid adjacent to the surface, and flow causes streaming. Fragments of biofilm8 and planktonic organisms that are shed and transported can potentially establish new biofilms on remote surfaces.
ANTIMICROBIAL TOLERANCEOne of the most important clinical aspects of the biofilm mode of growth is the tol-erance of the resident microbes to antimicrobial agents. Biofilm-embedded microbes can resist the bactericidal action of antimicrobial agents at 100 to 1,000 times the lev-els that would easily kill their planktonic counterparts. This should not be confused with genetically encoded antimicrobial resistance mechanisms such as inactivation or modification of the antimicrobial, alteration or replacement of the antimicrobial target site that reduces its binding capacity, modification of metabolic pathways to circumvent the antimicrobial effect, or reduced intracellular antimicrobial accumula-tion by decreasing permeability and/or increasing active efflux of the antimicrobial. Instead, biofilm antimicrobial tolerance is a result of the biofilm mode of growth. Susceptibility returns when the microbes return to a planktonic state.
Biofilms in Surgical Site Infections

10 © 2015 American Academy of Orthopaedic Surgeons
Antimicrobial tolerance is mediated by means of low metabolic levels and drastically downregulated rates of cell division of the deeply entrenched microbes,19 including nondividing persister cells.20,21 Although low metabolic rates can sub-stantially explain the antimicrobial resistance properties of biofilms, other factors can also play a role. For example, biofilms can act as a diffusion barrier, slowing the infiltration of some antimicrobial agents or the production of stress response genes that resist antimicrobial action.13
DIAGNOSTIC IMPLICATIONSCurrently, pathogen identification and antimicrobial susceptibility require propaga-tion in microbial culture followed by diagnostic analyses that normally involve addi-tional rounds of replication in culture, purification of specific bacterial products, or biochemical tests. At best, microbe recovery and identification can occur within days to weeks, depending on the growth rate of a specific pathogen. Biofilm infections are particularly difficult to culture. Small foci of microbes in the biofilm (< 0.1 mm3) can cause inflammation in large areas of tissue because of secreted toxins and inflam-matory mediators. If a biopsy misses the small biofilm population among the larger volume of involved tissue, then microbial cultures will be negative. Also, substan-tial difficulty exists in liberating the bacteria from the biofilm to grow in culture media. Sonication can increase the yield from biofilm on implant surfaces,22 but the recovered microbes are phenotypically planktonic, with virulence and susceptibility characteristics that do not represent their behavior from within the biofilm. Last, conventional cultures and subcultures that can readily grow planktonic organisms8 are often not able to detect microbes in the sessile phenotype, especially persister cells, which almost never yield positive culture results. False-negative cultures can delay appropriate therapy and allow the biofilm time to mature further and be-come even more resistant to antimicrobial agents. Even with positive cultures, the microbes must be transformed into their planktonic form to be detected. The number of organisms and their biologic characteristics, including antimicrobial susceptibil-ity and toxin production, do not represent the original sessile form.8 Because of the high false-negative culture rate for biofilm microbes, many indolent biofilm infec-tions were previously thought to be chronic inflammatory disorders.3 Sophisticated molecular techniques are needed to identify the microorganisms present.23,24
The methods used for direct identification of microbes in biofilm (polymerase chain
Let’s Discuss: Surgical Site Infections

© 2015 American Academy of Orthopaedic Surgeons 11
reaction, DNA array, RNA, fluorescent in situ hybridization probes, enzyme-linked immunosorbent assay, phase contrast microscopy, and fluorescence staining)8 are sophisticated, sensitive, and specific, but are largely investigational. These technolo-gies are not yet cost effective for clinical use, although polymerase chain reaction has been used clinically on a limited basis. Therefore, clinicians have no reliable modali-ty to help diagnose biofilm infections and must use clinical experience and consider clinical presentation and consensus results from multiple diagnostic strategies. How-ever, the unique properties of biofilms could be exploited by researchers to develop diagnostic tests specific for antigenic markers of the biofilm phenotype. Two prom-ising modalities being explored for the diagnosis of biofilm infections in laboratories include the detection of biofilm-directed, labeled probes25 or the detection of host antibodies against biofilm-specific antigens.26
CLINICAL IMPLICATIONSThe biologic behavior of the biofilm can change over time with genetic, phenotypic, and species diversity,8 which can make diagnosis and management challenging. Microorganisms that cause SSIs are initially planktonic. Planktonic microorganisms are well understood based on centuries of isolation; identification; and antimicro-bial susceptibility testing, vaccine development, and clinical experience. Acute, superficial, and deep SSIs present quickly, particularly when the infecting agent is highly virulent. The constellation of symptoms (pain, swelling, and fever), local and systemic findings (redness, warmth, edema, drainage, tenderness, elevated tempera-ture, and tachycardia), leukocytosis, and elevated acute reactive indices (erythrocyte sedimentation rate, C-reactive protein, and interleukin-6) are associated with the host response to uncontrolled growth of planktonic microorganisms. With timely diagno-sis and treatment, clinical outcomes with systemic antimicrobials are predictable and consistent with soft-tissue SSIs encountered in other specialties. However, when abi-otic surfaces or the surfaces of compromised tissue are present, microbes can quickly and actively transform to the sessile phase of their life cycle.4,8,27 After a biofilm is es-tablished, antimicrobial susceptibility can be decreased by 100- to 1,000-fold; surgical removal of all infected surfaces, both implant and compromised tissue, is required for infection resolution. Chronic SSI can either result from incompletely treated acute infections with residual biofilm or can be indolent from the outset, especially with low-virulence microbial species such as S epidermidis or P acnes. Indolent cases may
Biofilms in Surgical Site Infections

12 © 2015 American Academy of Orthopaedic Surgeons
have minimal local response with no purulence. The symptoms and findings of a host response are limited to periods of planktonic exacerbation. Quiescent periods as long as 75 years can occur.28 Systemic administration of susceptibility-directed antimicrobials is effective against planktonic microorganisms during exacerbation but do not completely clear the sessile-phase microorganisms.
New therapies that exploit biofilm biology are still being investigated. Antibiofilm- signaling analogs that prevent attachment, interrupt quorum sensing, and disperse the biofilm are under investigation and are not known to develop resistance.8 Inter-ventions that target genetic modifications are also being explored. One example is specific targeted antimicrobial peptides, which use a bifunctional peptide with a generic bacteriolytic segment and a species-specific ligand.8 One method with the greatest potential to treat biofilms may be prevention, either by means of prophy-lactic vaccination or with passive immunization using antibodies directed against antigens expressed early in the biofilm mode of growth.29,30
SUMMARYBacteria and fungi form sessile microbial communities termed biofilms, which is the dominant mode of growth of microbes and phenotypically distinct from their free-floating, planktonic counterparts. While in a biofilm, bacteria are tolerant to antimicrobial removal strategies and are inherently difficult to diagnose. Therefore, these microbial communities are of the utmost importance to orthopaedics because infections of devitalized tissue and bone as well as all indwelling medical devices will require surgical removal of the infectious nidus for resolution.
ACKNOWLEDGMENTSThe authors thank Michael A. Saubolle, MD, and Paul Stoodley, MD, for their contri-butions to this chapter.
• The dominant phase in the life cycle of bacteria and fungi is the sessile phenotype in communities (biofilms), not individual, free-floating planktonic microorganisms.
• A biofilm infection should be suspected when a hydrated attachment surface is present, either abiotic implant surfaces or devitalized tissue.
KEY POINTS
Let’s Discuss: Surgical Site Infections

© 2015 American Academy of Orthopaedic Surgeons 13
• Diagnosis of a biofilm using a culture is difficult and often fails because of localized microbial populations that are missed during biopsy and persister cells that cannot be cultivated.
• Biofilms are recalcitrant to effective antimicrobial therapy because the microbes are hundreds of times less susceptible to antimicrobials.
• Systemic antimicrobial treatment may eliminate planktonic microorganisms and resolve the systemic response, but does not eliminate cells in biofilm; surgical excision is required to eradicate established biofilm infection.
• The staphylococcal biofilm that colonizes skin is not eliminated by the skin prep; an implant should not touch the skin edges during insertion.
• Vascular catheters are all covered in biofilm within 1 week in situ; guidewires transfer biofilm during catheter exchange; indwelling vascular access catheters should be removed before implanting a permanent prosthesis.
KEY POINTS (continued)
Høiby N, Bjarnsholt T, Moser C, et al: ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin Microbiol Infect 2015 Jan 14 [Epub ahead of print]. pii: S1198-743X(14)00090-1. doi: 10.1016/j.cmi.2014.10.024.
McConoughey SJ, Howlin R, Granger JF, et al: Biofilms in periprosthetic orthopedic infections. Future Microbiol 2014;9(8):987-1007.
Brady RA, Leid JG, Calhoun JH, Costerton JW, Shirtliff ME: Osteomyelitis and the role of biofilms in chronic infection. FEMS Immunol Med Microbiol 2008;52(1):13-22.
Donlan RM, Costerton JW: Biofilms: survival mechanisms of clinically relevant microorganisms. Clin Microbiol Rev 2002;15(2):167-193.
SUGGESTED READING LIST
Biofilms in Surgical Site Infections

14 © 2015 American Academy of Orthopaedic Surgeons
REFERENCES1. Tlaskalová-Hogenová H, Stepánková R, Hudcovic T, et al: Commensal bacteria (normal micro-
flora), mucosal immunity and chronic inflammatory and autoimmune diseases. Immunol Lett 2004;93(2-3):97-108. Medline http://dx.doi.org/10.1016/j.imlet.2004.02.005
2. Dawkins R: The Extended Phenotype: The Long Reach of the Gene, Revised Edition. Oxford, England, Oxford University Press, 1999, p 336.
3. Ehrlich GD, Ahmed A, Earl J, et al: The distributed genome hypothesis as a rubric for under-standing evolution in situ during chronic bacterial biofilm infectious processes. FEMS Immunol Med Microbiol 2010;59(3):269-279. Medline
4. Wolcott RD, Rhoads DD, Bennett ME, et al: Chronic wounds and the medical biofilm paradigm. J Wound Care 2010;19(2):45-53. Medline http://dx.doi.org/10.12968/jowc.2010.19.2.46966
5. Elek SD: Experimental staphylococcal infections in the skin of man. Ann N Y Acad Sci 1956;65(3):85-90. Medline http://dx.doi.org/10.1111/j.1749-6632.1956.tb36626.x
6. Wolcott RD, Ehrlich GD: Biofilms and chronic infections. JAMA 2008;299(22):2682-2684. Medline http://dx.doi.org/10.1001/jama.299.22.2682
7. Costerton JW, Stewart PS, Greenberg EP: Bacterial biofilms: A common cause of persistent infec-tions. Science 1999;284(5418):1318-1322. Medline http://dx.doi.org/10.1126/science.284.5418.1318
8. Costerton W, Veeh R, Shirtliff M, Pasmore M, Post C, Ehrlich G: The application of biofilm sci-ence to the study and control of chronic bacterial infections. J Clin Invest 2003;112(10):1466-1477. Medline http://dx.doi.org/10.1172/JCI200320365
9. US National Institutes of Health: Research on Microbial Biofilms, PA-03-047. Available at: http://grants.nih.gov/grants/guide/pa-files/PA-03-047.html. Accessed December 10, 2014.
10. Resch A, Leicht S, Saric M, et al: Comparative proteome analysis of Staphylococcus aureus bio-film and planktonic cells and correlation with transcriptome profiling. Proteomics 2006;6(6):1867-1877. Medline http://dx.doi.org/10.1002/pmic.200500531
11. Donlan RM, Costerton JW: Biofilms: Survival mechanisms of clinically relevant microorganisms. Clin Microbiol Rev 2002;15(2):167-193. Medline http://dx.doi.org/10.1128/CMR.15.2.167-193.2002
12. Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lappin-Scott HM: Microbial bio-films. Annu Rev Microbiol 1995;49:711-745. Medline http://dx.doi.org/10.1146/annurev.mi.49.100195.003431
13. Xu KD, McFeters GA, Stewart PS: Biofilm resistance to antimicrobial agents. Microbiology 2000;146(Pt 3):547-549. Medline
Let’s Discuss: Surgical Site Infections

© 2015 American Academy of Orthopaedic Surgeons 15
14. Meluleni GJ, Grout M, Evans DJ, Pier GB: Mucoid Pseudomonas aeruginosa growing in a biofilm in vitro are killed by opsonic antibodies to the mucoid exopolysaccharide capsule but not by antibodies produced during chronic lung infection in cystic fibrosis patients. J Immunol 1995;155(4):2029-2038. Medline
15. Ward KH, Olson ME, Lam K, Costerton JW: Mechanism of persistent infection associ-ated with peritoneal implants. J Med Microbiol 1992;36(6):406-413. Medline http://dx.doi.org/10.1099/00222615-36-6-406
16. Yasuda H, Ajiki Y, Aoyama J, Yokota T: Interaction between human polymorphonuclear leuco-cytes and bacteria released from in-vitro bacterial biofilm models. J Med Microbiol 1994;41(5):359-367. Medline http://dx.doi.org/10.1099/00222615-41-5-359
17. Boyd A, Chakrabarty AM: Role of alginate lyase in cell detachment of Pseudomonas aeruginosa. Appl Environ Microbiol 1994;60(7):2355-2359. Medline
18. Cator LJ, George J, Blanford S, et al: ‘Manipulation’ without the parasite: Altered feeding behaviour of mosquitoes is not dependent on infection with malaria parasites. Proc Biol Sci 2013;280(1763):20130711.
19. Brown MR, Allison DG, Gilbert P: Resistance of bacterial biofilms to antibiotics: A growth-rate related effect? J Antimicrob Chemother 1988;22(6):777-780. Medline http://dx.doi.org/10.1093/jac/22.6.777
20. Harrison JJ, Turner RJ, Ceri H: Persister cells, the biofilm matrix and tolerance to metal cations in biofilm and planktonic Pseudomonas aeruginosa. Environ Microbiol 2005;7(7):981-994. Medline http://dx.doi.org/10.1111/j.1462-2920.2005.00777.x
21. Lewis K: Multidrug tolerance of biofilms and persister cells. Curr Top Microbiol Immunol 2008;322:107-131. Medline
22. Zhai Z, Li H, Qin A, et al: Meta-analysis of sonication fluid samples from prosthetic components for diagnosis of infection after total joint arthroplasty. J Clin Microbiol 2014;52(5):1730-1736. Med-line http://dx.doi.org/10.1128/JCM.03138-13
23. Hall-Stoodley L, Hu FZ, Gieseke A, et al: Direct detection of bacterial biofilms on the middle-ear mucosa of children with chronic otitis media. JAMA 2006;296(2):202-211. Medline http://dx.doi.org/10.1001/jama.296.2.202
24. Costerton JW, Post JC, Ehrlich GD, et al: New methods for the detection of orthopedic and other biofilm infections. FEMS Immunol Med Microbiol 2011;61(2):133-140. Medline http://dx.doi.org/10.1111/j.1574-695X.2010.00766.x
Biofilms in Surgical Site Infections
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7636254&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1613780&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7966209&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8074516&dopt=Abstract

16 © 2015 American Academy of Orthopaedic Surgeons
25. Shirtliff ME, Brady RA, Leid JG, Vail TL, Kofonow JM: In vivo biofilm infection diagnosis and treatment. US8697375 B2, 2014. Available at: http://www.google.com/patents/US8697375. Accessed December 15, 2014.
26. Leid JG, Vail TL, Kofonow JM, Shirtliff ME, Brady RA: Methods and devices for the detection of biofilm. US8541006 B2, 2013. Available at: http://www.google.com/patents/US8541006. Accessed December 15, 2014.
27. Peters BM, Jabra-Rizk MA, O’May GA, Costerton JW, Shirtliff ME: Polymicrobial interactions: Impact on pathogenesis and human disease. Clin Microbiol Rev 2012;25(1):193-213. Medline http://dx.doi.org/10.1128/CMR.00013-11
28. Libraty DH, Patkar C, Torres B: Staphylococcus aureus reactivation osteomyelitis after 75 years. N Engl J Med 2012;366(5):481-482. Medline http://dx.doi.org/10.1056/NEJMc1111493
29. Brady RA, O’May GA, Leid JG, Prior ML, Costerton JW, Shirtliff ME: Resolution of Staphy-lococcus aureus biofilm infection using vaccination and antibiotic treatment. Infect Immun 2011;79(4):1797-1803. Medline http://dx.doi.org/10.1128/IAI.00451-10
30. DiGiandomenico A, Keller AE, Gao C, et al: A multifunctional bispecific antibody protects against Pseudomonas aeruginosa. Sci Transl Med 2014;6(262):262ra155. Medline http://dx.doi.org/10.1126/scitranslmed.3009655
VIDEO REFERENCEShirtliff ME: Video. Excerpt. Biology of Biofilms. Baltimore, MD, 2015.
Let’s Discuss: Surgical Site Infections