'Biochemical analysis of non- standard fluids: clinical ...
106
'Biochemical analysis of non- standard fluids: clinical and analytical considerations. Presentation by: Dr Peadar McGing, FRCPath EuSpLM, Principal Clinical Biochemist, Department of Clinical Chemistry and Diagnostic Endocrinology, Mater Misericordiae University Hospital, Eccles Street, Dublin 7, D07R2WY, Ireland.
Transcript of 'Biochemical analysis of non- standard fluids: clinical ...

'Biochemical analysis of non-standard fluids: clinical and analytical considerations.
Presentation by:
Dr Peadar McGing, FRCPath EuSpLM, Principal Clinical Biochemist, Department of Clinical Chemistry and Diagnostic Endocrinology, Mater Misericordiae University Hospital, Eccles Street, Dublin 7, D07R2WY, Ireland.

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
2

My first fluid testing case
• 12 year old male patient
• Acute pains lasting only seconds in different part of abdomen.
• Increased frequency of pain.
• Multiple negative blood and radiology tests (over 3 weeks as in-patient).
• Lumbar puncture performed – CSF tests negative.
• What next?
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
3

My first fluid testing case
• What next? Pain frequency decreased post LP
• Second LP performed. Pain disappeared
• ?Long term outcome.
• Patient is currently 50 years symptom free.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
4

5 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
6

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
7
“Instruction does much, but encouragement everything.”
– Johann Wolfgang von Goethe, writer and statesman

Lecture Outline
• Reference Books
• Body fluids
– Types of fluids
– Some physiology and pathology
• Pre-analytical
• Analytical
• Post-analytical
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
8

9 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

10 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

11 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

• Copyright: 2015; ISBN: 9781594251801
• Pages: 56; Price: $22.00; Member Price: $18.00
12 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

From ACB Mailbase
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
13

Clinical Significance
Sodium = 125 mmol/L
versus
Sodium = 141 mmol/L
• Is there a clinical difference in these results?
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
14

Clinical Significance
Sodium = 125 mmol/L
versus
Sodium = 141 mmol/L
• Is there a clinical difference in these results?
• YES if serum / plasma
• NO if urine
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
15

Let’s talk about fluids
• Fluid formation
• Fluid function
• Fluid accumulation
• Fluid removal
• Fluid analysis
Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing 16

Types of Fluids for Analysis
• Cerebral Spinal Fluid
– Query CSF
• Pleural Fluid
• Pericardial Fluid
• Ascitic / Peritoneal Fluid
– PET Dialysis Fluid
• Saliva
• Sweat
• Amniotic Fluid
• Seminal Fluid
• Synovial Fluid
• Cyst Fluids
– Pancreatic cyst fluid
• Faecal Water
• Vitreous humour
• Drain fluids
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
17

The age-old question
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
18
fluids

Body Fluids
• Body fluid / body water – c60% of body wt
• Two-thirds Intracellular Fluid (ICF)
• One-third Extracellular Fluid (ECF)
• One quarter of ECF is Intravascular (plasma)
• Three quarters is Extravascular.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
19

Origin of Fluids
• Body fluid / body water – c60% of body wt Two-thirds Intracellular Fluid (ICF), One-third Extracellular Fluid (ECF)
• One quarter of ECF is Intravascular (plasma), three quarters Extravascular.
• Extravascular fluid:
– Three quarters interstitial fluid
– One quarter transcellular fluid
• Separated from plasma by additional epithelial layer
• Incl CSF, pleural fl, pericardial fl, peritoneal fl, synovial fl, intraoccular fl, …
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
20

Fluid collection for testing
• Blood readily available, but minimally invasive,
• Urine can be readily available (timing-dependent)
• Transcellular fluid may be difficult – – Increasingly Ultrasound guided,
– Sometimes just diagnostic tap
– Often fluid drainage is therapeutic
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
21

Body Fluids
• Fluid function: – Protection (e.g. CSF, amniotic fluid)
– Waste removal (e.g. CSF)
– Lubrication (e.g. pleural, pericardial fluid)
• Fluid accumulation: – Increased production
• Raised hydrostatic pressure (e.g. heart failure),
• Increased permeability (e.g. infection, malignancy)
– Decreased removal
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
22

Pleural Effusion
• “Pleural fluid is not just there to annoy respiratory physicians but has a purpose. It allows us to breathe.”
– Opening remark of Consultant Respiratory Physician at Medical Grand Rounds presentation ‘A fluid situation. Myths, pearls, and reality of pleural effusions’.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
23

Pleural Effusion
• Pleural effusion → fluid formation exceeds removal → accumulation of excess fluid in the pleural space.
• Fluid accumulation can be due to – increased fluid production or – decreased fluid removal.
• Etiology is related to the underlying condition • – congestive cardiac failure causes increased fluid due
to raised hydrostatic pressure gradient • – malignancy or infection, the increased production is
usually the result of increased permeability of capillary vessels.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
24

Pleural fluid- physical characteristics
Fluid Appearance/ Odour
Necessary Fluid Study
Differential
Bloody Hematocrit and RBC count
Malignancy, trauma, PE, hemothorax
Cloudy Triglycerides Chylothorax
Putrid odour Gram stain and culture
Anaerobic infection
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
25

Fluid appearance
26 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Fluid appearance
27 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Pleural Effusions
• The most common causes of exudative pleural effusions are – parapneumonic effusions (particularly bacterial
pneumonia), and
– malignancy.
• The most common causes of transudative pleural effusions are – left ventricular failure (very common) and
– cirrhosis.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
28

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
29

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
30
Lapworth R and Tarn AC. Commentary on the British Thoracic Society guidelines for the investigation of unilateral pleural effusion in adults. Ann Clin Biochem 2006; 43: 17-22.

Transudate v Exudate
• Fluid Protein strongly suggests
Transudate if Fluid Protein <25 g/L
Exudate if Fluid Protein >35 g/L
• Fluid Protein equivocal if 25-35 g/L
Further testing required, including Fluid LDH, or
Light’s Criteria
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
31

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
32
Clin Chest Med 34 (2013) 21-26.
Light’s criteria (Pleural Fluid)
• Pleural fluid is an exudate if one or more of the following criteria are met:
– Pleural fluid protein divided by serum protein is >0.5
– Pleural fluid lactate dehydrogenase (LDH) divided by serum LDH is >0.6
– Pleural fluid LDH >2/3 the upper limits of laboratory normal value for serum LDH.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
33

Pleural Effusions
• Where clinical suggests transudate but Light Criteria suggest exudate:
• Serum:fluid protein gradient >31 g/L suggests Transudate,
• If protein gradient <31 g/L then
– Fluid NT-Pro BNP >1300ng/L, or
– Serum:fluid Albumin gradient >12 g/L
suggests Transudate.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
34

CONCLUSIONS: Regardless of the daily drainage, chest tubes can safely be removed earlier than anticipated in most patients after lobectomy if the protein content of the draining fluid is low. [Def’n of Low: Drains were removed if the pleural fluid to blood protein ratio (PrRPl/B) was ≤0.5.]
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
35

Pleural Fluid Report
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
36
Reference ranges are not reported for fluid biochemistry. Fluid biochemistry should be interpreted in light of the clinical question being asked, comparison with blood results, and/or appropriate clinical guidelines.
Biochemical Tests performed in specific clinical circumstances.
• Query Chylothorax
– triglycerides and cholesterol +/- chylomicrons
• Query TB
– (Adenosine deaminase)
• Query Malignancy
– value of tumour markers is questionable.
• Query Pancreatitis
– amylase.
Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing 37

Patient A.
• b/g end-stage ischaemic cardiomyopathy.
• Chest drain inserted
• Sample: Pleural Fluid
• Test requested: TRIGFL (Fluid Triglyceride)
• Clinical Details: Query chylothorax
• Result: TRIGFL = 4.01 mmol/L
• Query re interpretation.
• Biochemist added CHOLFL (Fluid Cholesterol)
• Result: CHOLFL = 1.40 mmol/L Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing 38

Interpretation
Chylothorax Pseudo-chylothorax
Trig (mmol/L) >1.24 <0.56
Chol (mmol/L) <5.18 >5.18
Fl to Ser Chol Ratio <1
Fl to Ser Trig Ratio >1
Chylomicrons Present Absent
Cholesterol Crystals Not seen Often seen
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
39
Ref: adapted from McGrath et al. Respiratory Medicine (2010) 104, 1-8.

Patient A - Interpretation
Chylothorax Pseudo-chylothorax
Trig (mmol/L) >1.24 <0.56
Chol (mmol/L) <5.18 >5.18
Fl to Ser Chol Ratio <1
Fl to Ser Trig Ratio >1
Chylomicrons Present Absent
Cholesterol Crystals Not seen Often seen
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
40
TRIGFL = 4.01 mmol/L CHOLFL = 1.40 mmol/L

Clinical Audit (Bio / Respiratory)
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
41

Audit findings
• 34 consecutive pleural fluids
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
42
Fluid test n %
Culture 32 94
LDH 29 85
Gram stain 29 85
Protein + albumin 27 79
pH 26 76
Glucose 21 62
Cytology 14 41
Serum / Plasma n %
Blood with fluid 17 50
Protein + albumin 14 41
LDH 8 24
Glucose 7 21

Pre-analytical
• The correct sample
• Correctly labelled – Including fluid source
• All tests requested – Including paired blood tests
• All test samples taken – and in correct tubes
• All samples presented in timely manner
• All samples processed in timely manner
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
43

Pre-analytical
• Some examples of MMUH communications and procedures aimed at reducing pre-analytical issues
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
44

45 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Fluid Analysis
The Following Sample Containers are required for Collection of Fluid
(Pleural/Ascites/Peritoneal) to ensure appropriate Test Analysis
Product No: 75.9922.745. 70ml MSU container Laboratory: Microbiology Test Request: FL C/S & Gram stain; FL ZN/TB Culture (Pleural Fluid only)
N. B. Please send separate Pleural Fluid sample for each test request -------------------------------------------------------------------------------------------------------
Product No: 05-1167-001. 2.7 ml EDTA KE Pink capped tube OR
Product No: 05.1167.901. 2.7 ml EDTA KE Grey capped tube Laboratory: Microbiology Test Request: Fluid Cell Count Mix well by inverting gently 4-5 times -------------------------------------------------------------------------------------------------------
Product No.75.9922.745 70ml MSU Laboratory: Cellular Pathology Test Request: Diagnostic Cytology N. B. Please do not add any fixative to this sample. Deliver fresh to lab ASAP. 50mls aliquot deliver as soon as possible. Place 3 IU heparin per ml of fluid to prevent clot formation
46 Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing

Mater Misericordiae University Hospital MI-GEN-011 Pathology Laboratory Edition 1.03
Product No: 04.1940.001. 4.9 ml ORANGE capped Lithium-Heparin gel Tube Laboratory: Clinical Chemistry & Diagnostic Endocrinology Test Requests [Routine]: Fluid Protein(PROTFL), Fluid Albumin(ALBFL), Test Requests [Occasional]: Fluid Cholesterol(CHOLFL), Fluid Triglycerides(TRIGFL), Fluid Amylase(AMYLFL), Fluid Bilirubin(BILIFL), Fluid CA125(CA125F), Fluid Urea(UREAFL), Fluid Creatinine(CREAFL), Fluid CA19.9(CA199F), Fluid CEA(CEAFL) Mix well by inverting gently 4-5 times N. B. Please ensure blood sample is also collected -------------------------------------------------------------------------------------------------------
Product No: 04.1935.001. 4.9 ml BROWN capped Serum gel Tube Laboratory: Clinical Chemistry & Diagnostic Endocrinology Test Request: Fluid LDH (LDHFL) Mix well by inverting gently 4-5 times N. B. Please ensure blood sample is also collected -------------------------------------------------------------------------------------------------------
Product No: 04-1903-001. 2.6 ml Fluoride EDTA YELLOW capped tube. Laboratory: Clinical Chemistry & Diagnostic Endocrinology
Test Request: Fluid Glucose (GLUFL) Mix well by inverting gently 4-5 times N. B. Please ensure blood sample is also collected ---------------------------------------------------------------------------------------
Product No: 956-622. safePICO Aspirator Arterial Blood Sampler Laboratory: Clinical Chemistry & Diagnostic Endocrinology: Test Request [Routine]: Fluid pH (PHFL), Test Request [Occasional]: Fluid Lactate (LACTFL) Mix well by inverting gently 4-5 times
47 Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing

Pleural fluid sampling instruction. -for clinical staff, available on hospital intranet
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
48

Laboratory guide to fluid sample types Mater Misericordiae University Hospital LI-CCE-0051 Clinical Chemistry and Endocrinology Laboratory Edition 1.02
Clinical Chemistry/Endocrinology - Processing Chart for Fluids This refers to Fluid samples only; refer to LI-CCE-0012 and LI-CCE-0050 for Blood and urine processing charts respectively
Subscript numbers refer to Tube type e.g. 2 is Brown serum gel tube.
TEST Telepath Code Tube Type Fluid type allowed for assay (for entering as specimen type on Telepath)
CSF Protein CPROT Plain aliquot CSF
CSF Glucose CGLU Plain aliquot CSF
CSF Xanthochromia XAN Plain aliquot protected from light
SF2
Fluid Protein PROTFL Orange Top Gel PF, PER, PAF, PC, FL
Fluid Albumin ALBFL Orange Top Gel PF, PER, PAF, PC, FL
Fluid LDH LDHFL Brown Top Gel PF2, PER2, PAF2, FL2
Fluid Cholesterol CHOFL Orange Top Gel PF, PER, PAF, PC, FL
Fluid Triglycerides TRIGFL Orange Top Gel PF, PER, PAF, PC, FL
Fluid Amylase AMYFL Orange Top Gel DR, PAF, FL
Fluid Bilirubin BILIFL Orange Top Gel DR, FL
Fluid CA125 CA125F Orange Top Gel PF, PER, FL
Fluid Urea UREAFL Orange Top Gel PET, FL
Fluid Creatinine CREAFL Orange Top Gel PET, DR, FL
Fluid CA199 CA199F Orange Top Gel PAF, FL
Fluid pH PHFL Blood Gas Monovette PF4, PER4, PAF4, FL4
Fluid Lactate LACTFL Blood Gas Monovette DR4, CSF, FL4
Fluid Glucose GLUFL Yellow Top PF3, PER3, PAF3, FL3, PET3, DR3
Fluid CEA CEAFL Orange Top Gel PF, PER, PAF, FL
Stability: CSF XAN – see special protocol. All other tests: stability as for plasma / serum, once in correct containers.
Fluid Types Code
CSF (Cerebral Spinal Fluid) CSF
CSF for Xanthochromia SF2
Pleural Fluid PF
Ascitic / Peritoneal Fluid PER
Dialysis Fluids PET
Fluid Types Code
Drain Fluids DR
Pancreatic Cyst Fluids. PAF
Pericardial Fluids PC
All other Fluids FL
49 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

50 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Fluids SOP
Procedure for Body Fluids other than Blood and Urine
Mater Misericordiae University Hospital
REVISION DESCRIPTION
Added comment re use ‘off-label’ (1.0) Added re salivary cortisol (1.0, 2.0, 3.4) Added section on Stability (3.3) [CR5018] Added Pericardial Fluid as specimen type (4.0, 5.0) Re-formatted pages.
51 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Fluids – Pre-analytical
• 3.3 Stability
• Provided samples are collected into appropriate tubes, or transferred to such tubes soon after collection (e.g. Fluoride EDTA for fluid glucose), then stability is the same as for that test in plasma. For stability times see LI-CCE-0009 [ANALYTE STABILITY CHART].
• CSF for glucose should be analysed within one hour if significant cells present.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
52

Procedure for Body Fluids other than Blood and Urine
Mater Misericordiae University Hospital
REVISION DESCRIPTION
Added comment re use ‘off-label’ (1.0) Added re salivary cortisol (1.0, 2.0, 3.4) Added section on Stability (3.3) [CR5018] Added Pericardial Fluid as specimen type (4.0, 5.0) Re-formatted pages.
Most testing described in this SOP is ‘off-label’, i.e. testing is carried out in a fluid not validated by the manufacturer. All reports carry a statement to this effect.
53 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing
Email to ACB mailbase, Jan 2016 Subject: UKAS accreditation for pleural and ascitic fluid
• ‘It is my understanding that measurements of certain analytes in fluids such as ascitic and pleural fluid cannot be UKAS accredited for several reasons including CE marking, lack of fluid EQA, standardisation issues in non-recommended matrix etc. These include: albumin, amylase, bicarbonate, calcium, creatinine, glucose, LDH, potassium, sodium, triglyceride, total protein and urea in pleural and ascitic fluid …. ’
• ‘We let our users know that these are non-accreditable tests.’
• ‘Is anyone tempted to drop them due to UKAS, or not bother with UKAS for fluids or has anyone overcome this by local verification?’
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
54

Email to ACB mailbase, Jan 2016 Subject: UKAS accreditation for pleural and ascitic fluid
• Feedback:
• ‘The replies can be split into 2 groups:’
• ‘We have removed these from our AC6. Seems the easiest way to deal with the issue’
• ‘Just go for "this report is not UKAS-accredited“.’
• Concern:
• ‘We are now in the realm of having “UKAS accredited tests” and “non-UKAS Accredited tests”, which is an accreditation place that I did not want to be. For example once we accept that we are going to provide a clinical service with some “non-UKAS accredited tests” where do we draw the line?’
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
55

The inspector?
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
56

The fluids biochemist?
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
57

Types of Fluids for Analysis
• Cerebral Spinal Fluid
– Query CSF
• Pleural Fluid
• Pericardial Fluid
• Ascitic / Peritoneal Fluid
– PET Dialysis Fluid
• Saliva • Sweat
• Amniotic Fluid
• Seminal Fluid
• Synovial Fluid
• Cyst Fluids
– Pancreatic cyst fluid
• Faecal Water
• Vitreous humour
• Drain fluids
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
58

Ascitic / Peritoneal Fluid
• Common clinical finding – wide range of causes.
• Conditions that may be associated with ascites include – increased hydrostatic pressure associated with portal
hypertension (e.g cirrhosis, alcoholic hepatitis) – decreased colloid osmotic pressure secondary to
hypoalbuminaemia (e.g. ESLD, nephrotic syndrome) – increased permeability of peritoneal capillaries (TB
peritonitis, HIV peritinotis) – leakage of fluid into the peritoneal cavity (e.g. bile, urine) – malignant conditions (e.g. peritoneal carcinomatosis) – miscellaneous causes (e.g. myxoedema, chronic HD)
Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing 59

SAAG
• SAAG = [S-Alb]– [F-Alb]; all in g/L
• SAAG greater or equal to 11 predicts that the patient has portal hypertension with 97% accuracy.
• Runyon BA1, Montano AA, Akriviadis EA, Antillon MR, Irving MA, McHutchison JG. The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites. Ann Intern Med. 1992 Aug 1;117(3):215-20.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
60

Remember effect on serum assays
• Type of comment I sometimes add to report of raised plasma CA125 in patient with fluid accumulation –
Noted receipt of peritoneal fluid for analysis, indicating presence of ascites. Ascites can of itself cause marked rise in plasma CA125 (to higher than level seen in this case).
Interpret with caution.
61
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
62

• “Your tests reveal you are retaining fluids.”
63 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Could this fluid be leaked CSF?
• Pt B.
• Male in late 50s.
• Fluid noted on scan, and removed
• Surgeons keen to know origin of fluid before doing exploratory operation.
• Could be CSF
• What test?
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
64

Could this fluid be leaked CSF?
• Pt B.
• Male in late 50s.
• Surgeons keen to know origin of fluid before doing exploratory operation.
• Could be CSF
• What test?
• Measure Beta Trace Protein – We use Health Services Laboratories in London
• Beta Trace Protein now preferred to Beta-2-Transferrin (Asialotransferrin)
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
65

Could this fluid be leaked CSF?
• Measure Beta Trace Protein (BTP) • Fluid:
– appearance = straw coloured – BTP = 1.61 mg/L (ref: <1.30 = negative, 1.31-8.88
=intermediate positive, >8.89 = raised positive) – Suggests possible CSF leak
• Serum: – BTP = 0. 61 mg/L (ref: <1.30 = normal)
• Fluid to serum ratio: – Ratio = 2.63 (>2.0 indicates probably fluid is CSF).
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
66

Medical Grand Rounds - case presented by Consultant Endocrinologist
• Patient C: 59 yrs male
• May 2012 to Apr 2016 had 6 admissions
• Adm Apr’16 w drowsiness + ataxia.
• Hx included Hashimoto’s thyroiditis and left hemi-thyroidectomy.
• Adm bloods – TFTs=N (FT4=18.2, TSH=2.19), Anti-TPO=38.5 (ref<5); mild anaemia.
• ?EATTD (Encephalopath Autoimmune Associated Thyroid Disease)
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
67

Medical Grand Rounds - case presented by Consultant Endocrinologist
• 59 yrs male with possible diagnosis of EATTD (Encephalopath Autoimmune Associated Thyroid Disease).
• Exclude other causes of encephalopathy
• Test that could maybe be helpful
CSF Anti-TPO
• But is the assay validated / verified for CSF?
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
68

Medical Grand Rounds - case presented by Consultant Endocrinologist
• As our assay was not validated Neurology Dept had sent CSF to USA for TPO analysis
• Result not available
• Deemed clinically that dx did = EATTD
• Post Grand Round, I decided to do very basic verification
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
69

TPO mini-verification
• Samples used:
• CSF – old samples from freezer storage (next samples due for routine disposal); anonymised.
• Plasma – aliquots of samples from routine TPO assay; TPO<1 or TPO>200 IU/mL.
• Test sample: 50µL plasma + 950 µL CSF
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
70
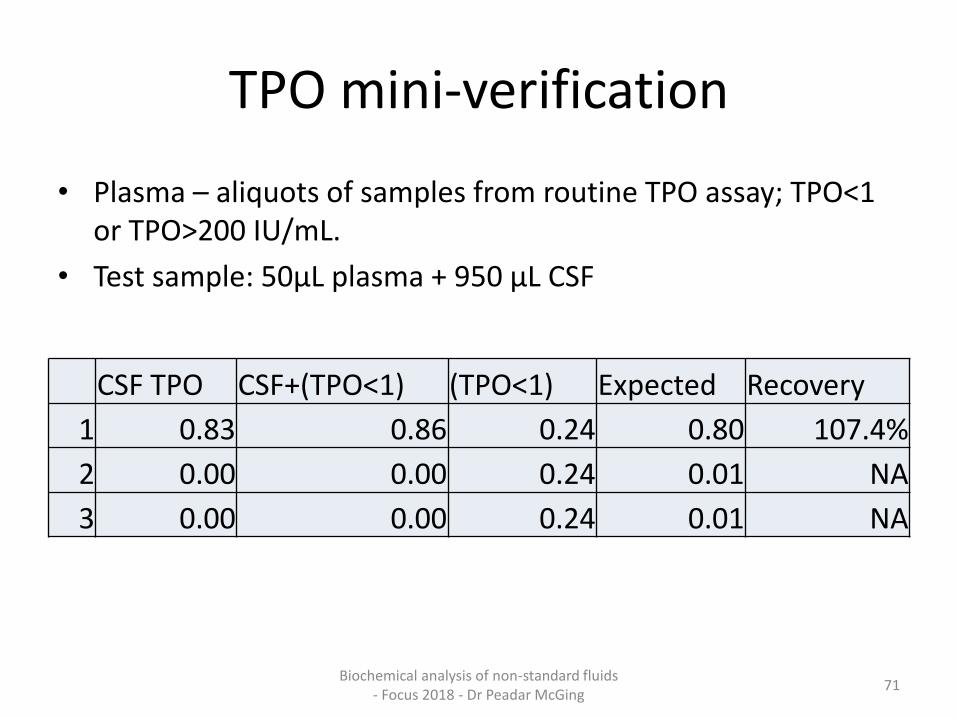
TPO mini-verification
• Plasma – aliquots of samples from routine TPO assay; TPO<1 or TPO>200 IU/mL.
• Test sample: 50µL plasma + 950 µL CSF
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
71
CSF TPO CSF+(TPO<1) (TPO<1) Expected Recovery
1 0.83 0.86 0.24 0.80 107.4%
2 0.00 0.00 0.24 0.01 NA
3 0.00 0.00 0.24 0.01 NA

TPO CSF TPO CSF+(TPO pos) (TPO pos) Expected Recovery
1 0.83 43.11 756 38.59 111.7% 2 0.00 44.94 756 37.80 118.9% 3 0.00 37.88 756 37.80 100.2% 4 0.83 70.33 1246 63.09 111.5% 5 0.00 63.83 1246 62.30 102.5% 6 0.00 63.64 1246 62.30 102.2% 7 0.83 12.14 209 11.24 108.0% 8 0.00 10.55 209 10.45 101.0% 9 0.00 10.74 209 10.45 102.8%
mean 106.5% SD 6.4%
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
72

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
73
Tamagno et al. BMC Neurology 2010, 10:27
In the CSF, anti-TPO and anti-TG Abs were positive in 5/5 (Patient 2,
6, 7, 10, and 14) and 2/2 (Patient 6 and 7) cases, respectively.

The challenge of fluid analyses
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
74
“In life, there is always a hurdle.”
– Gail Devers, track and field athlete
• Photo courtesy of IAAF

Safety
• Options – Reject – Treat as do for plasma / serum/urine – Prepare in fume cupboard – Use special category high-risk fume cupboard
• Sample dependent • Local availability of facilities • Safety considerations for in-house AND for
referral • Rem CSF for Xanthochromia
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
75

MMUH Fluids SOP
• 6.2 External QA • Other than for CSF (and the schemes for blood and
urine) there is no EQA scheme covering analysis of biochemical parameters in Body Fluids.
• Details of the EQA scheme for CSF are to be found in the SOP for EQA [QP-CCE-0001]
• CSF Protein is also specifically covered by RIQAS Urine Scheme (as well as CSF-specific scheme).
• We use the EQA schemes for blood and urine to monitor quality of performance for all other tests carried out on miscellaneous body fluids.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
76

EQA of Fluids - Options
• EQA of specific fluid
– Plasma / serum
– CSF
– Other
• Assurance from plasma/serum
– Testing the analyte
– Testing the system
• EQA by sample exchange
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
77

78 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

79 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Glucose EQA
• MMUH Routine Glucose assay = Hexokinase/G-6-PDH (on Abbott Architect)
– EQA in Plasma / Serum – Good
– EQA in Urine – Good
– EQA in CSF – Good
• MMUH POCT Glucose assay = Glucose sensor (electrode) (on ABG machine)
– EQA in Whole Blood – Good
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
80
Lactate EQA
• MMUH lactate assay = Lactate sensor (electrode) (on ABL90 ‘blood gas’ machine)
– EQA in Whole Blood – Good
– EQA in Plasma / Serum – Good
• Used CSF EQA as initial test of validity of our Lactate assay if applied to CSF.
– EQA in CSF – Poor Decision = refer CSF Lact
Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing 81

Saliva
• Mouth fluid possessing several functions
– Oral health and homeostasis
– Taste perception
– Oral mucosa protection against mechanical damage
– α-amylase
– Teeth enamel mineralisation
– Defence functions
• Mouth fluid as test medium
– Significant Advantage….non-invasive collection
– Free hormones
Slides on Salivary Cortisol method courtesy of Keith Mulready, MMUH.

Production and composition
• 500 – 1500 ml/day
• Modified by several physiological and pathological influences
• Autonomic nervous system controls output and composition
• Serous…sympathetic nervous system
• Mucous…both para- and sympathetic
• Clearance of compounds from plasma into saliva involves
– Ultrafiltration…only molecules MW<1900 Da involved • Small polar molecules
– Transudation • Albumin
– Selective transport through cellular membranes • Passive diffusion of lipophilic molecules
• Free, non-protein bound unconjugated steroids
Slides on Salivary Cortisol method courtesy of Keith Mulready, MMUH

Cortisol analysis by Immunoassay
CBG
80-90%
Albumin
10-15%
Free Cortisol
5-10%
• Large intra + inter-platform variability
• New Roche II 25% lower than Roche I
• Numerous CRMs in use • Diff antibodies to different
epitopes • No consensus for diagnostic
cut-offs • Displacement steps are
manufacturer specific Use of another steroid, a change
in pH or use of a high affinity antibody to compete for binding
Cortisol Transport + Binding (Plasma)
Slides on Salivary Cortisol method courtesy of Keith Mulready, MMUH

LC-MS/MS is 10-100 times more sensitive when compared with IA-based methodology and is capable of eliminating many of the inherent
flaws encountered with immunoassays

Metrological Traceability
Need to fulfil the requirements of the IVD directive and ISO15189
Minimum of 6 certified reference materials for Cortisol ERM-DA 192 and 193
ERM-DA 451/IFCC
SRM 921
SRM 971
U.S. Pharmacopeia Hydrocortisone Reference Standard
NIST standard reference material 921 was used for cortisol calibrators
Cerilliant CRM for calibrators and IQC Cortisone
The traceability chain is maintained

Validation
• FDA Guidance for Industry Bioanalytical Method Validation
• Honour, J.W., 2011. Development and validation of a quantitative assay based on tandem mass spectrometry. Annals of Clinical Biochemistry, 48(Pt 2), pp.97–111.
Assessment
Intra-precision
Inter-precision
Accuracy
Post Extract Stability
Injection Precision
Ion Suppression
(Post Column Infusion)
Carryover
LC-MS/MS Referral
Peer Comparison
Linearity
Analyte Recovery
Dilutional Studies
Sample stability Slides on Salivary Cortisol method courtesy of
Keith Mulready, MMUH

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
88

Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
89

Types of Fluids for Analysis
• Cerebral Spinal Fluid
– Query CSF
• Pleural Fluid
• Pericardial Fluid
• Ascitic / Peritoneal Fluid
– PET Dialysis Fluid
• Saliva
• Sweat
• Amniotic Fluid
• Seminal Fluid
• Synovial Fluid
• Cyst Fluids
– Pancreatic cyst fluid
• Faecal Water • Vitreous humour
• Drain fluids
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
90

91
‘Father of Microbiology’
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
92

Antonie van Leeuwenhoek (1632 – 1723)
• Dutch merchant
• First to see microorganisms (‘animalicules’),
• First to see Sperm, and describe fertilisation,
• First to describe Urate crystals.
• [Figure from original drawing]
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
93

Synovial Fluid
• Gold standard for diagnosis of gout is identification of MSU (monosodium urate) crystals in synovial fluid.
• Differentiate MSU from CPPD (calcium pyrophosphate dihydrate) crystals.
• Polarised light microscope is required. – MSU crystals have negative birefringence (rotate
beam of polarised light clockwise).
– CPPD crystals have positive birefringence (rotate beam of polarised light anti-clockwise).
Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing 94

95 Biochemical analysis of non-standard fluids
- Focus 2018 - Dr Peadar McGing

Pancreatic Cyst Fluid
• Pancreatic cyst fluid analysis for differential diagnosis between benign and malignant lesions.
• Renata Talar-Wojnarowska et al. Oncol Lett. 2013 Feb; 5(2): 613–616
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
96

Pancreatic Cyst Fluid
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
97

Copyrights apply

Copyrights apply
Typical carcinoembryonic antigen (CEA) level: <5 to 20 ng/mL in majority of lesions. Relative malignant potential: Negligible
Typical carcinoembryonic antigen (CEA) level: >200 ng/mL in approximately 75% of lesions. Relative malignant potential :Moderate, High, Low to moderate respectively

Faeces / Faecal Water
• Faecal calprotectin
• Faecal elastase
• Faecal electrolytes
– Sodium
– Potassium
– Magnesium
• Faecal Osmolality
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
100

Copyrights apply

Copyrights apply

Remember testing may not be always appropriate.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing 103

Summary (1)
• Many body fluids can accumulate in disease
• In some cases laboratory testing, including biochemical, may be of value.
• Testing of other fluids (not pathological accumulations) can also be helpful.
• The number of samples and analytes so tested is a very small part of our workload
• Despite this, fluid analyses can be difficult and labour intensive.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
104

Summary (2)
• Matrix differences versus serum/plasma/urine means some verification needed
• Full verification / validation is probably not clinically necessary (usually),
• Matrix effect MUST be tested.
• Some interpretation should be provided either on report, via electronic link, or via reference to hospital intranet /internet.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
105
Summary (3)
• Message that test is used off-label must be attached to report (unless not appropriate)
• The difficulties associated with verification of fluid analyses should not deter laboratories from using them.
• Biochemists should – carry out verification of any assays likely to be of
value, where possible, – Refer tests only if referral lab has verified assay, – Refuse to assay where could mislead – Refuse to assay where cannot stand over result.
Biochemical analysis of non-standard fluids - Focus 2018 - Dr Peadar McGing
106