
Understanding Developmental-Behavioral Screening Measures ...
13
DOI: 10.1542/pir.33-10-448 2012;33;448 Pediatrics in Review Kevin P. Marks and Angela C. LaRosa Understanding Developmental-Behavioral Screening Measures http://pedsinreview.aappublications.org/content/33/10/448 located on the World Wide Web at: The online version of this article, along with updated information and services, is http://pedsinreview.aappublications.org/content/suppl/2012/09/26/33.10.448.DC2.html http://pedsinreview.aappublications.org/content/suppl/2012/09/26/33.10.448.DC1.html tml http://pedsinreview.aappublications.org/content/suppl/2012/09/17/33.10.448.DCSupplementary_Data.h Data Supplement (unedited) at: Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly by Kevin Marks on October 1, 2012 http://pedsinreview.aappublications.org/ Downloaded from
Transcript of Understanding Developmental-Behavioral Screening Measures ...

DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
httppedsinreviewaappublicationsorgcontent3310448located on the World Wide Web at
The online version of this article along with updated information and services is
httppedsinreviewaappublicationsorgcontentsuppl201209263310448DC2htmlhttppedsinreviewaappublicationsorgcontentsuppl201209263310448DC1html
tmlhttppedsinreviewaappublicationsorgcontentsuppl201209173310448DCSupplementary_Datah
Data Supplement (unedited) at
Pediatrics All rights reserved Print ISSN 0191-9601 Boulevard Elk Grove Village Illinois 60007 Copyright copy 2012 by the American Academy of published and trademarked by the American Academy of Pediatrics 141 Northwest Pointpublication it has been published continuously since 1979 Pediatrics in Review is owned Pediatrics in Review is the official journal of the American Academy of Pediatrics A monthly
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
Understanding Developmental-BehavioralScreening MeasuresKevin P Marks MDdagger
Angela C LaRosa MDDagger
Author Disclosure
Drs Marks and LaRosa
have disclosed no
financial relationships
relevant to this article
This commentary
does not contain
a discussion of an
unapproved
investigative use of
a commercial product
device
Educational Gap
With nearly half of pediatricians still not using standardized screening tools primary care
clinicians should know that the periodic use of general developmental and social-emotional
screening tools has been proven to identify promptly two to six times more children (age 0ndash
5 years) with suspected delays than a clinicianrsquos unstructured surveillance alone
Objectives After completing this article readers should be able to
1 Recognize the many methods available to detect a wide spectrum of developmental
and behavioral conditions with screening tools and the screening schedule
recommended by the AAP
2 Recognize that universal periodic screening with psychometrically sound
developmental-behavioral instruments greatly enhances a clinicianrsquos ability to detect
refer and monitor children who have evolving developmental and behavioral
problems A pediatric providerrsquos impression has good specificity but poor sensitivity
and thus has difficulty identifying the less obvious delays
3 Know that children who have false-positive screens (screening test concerning but
subsequently ineligible for early intervention or early childhood special education
services) are a high-risk group in need of close monitoring and other community
services such as evidence-based parenting programs and Head Start
4 Know the main limitations of applying standardized screening tools into a primary
care setting
5 Be aware that screening measures which adhere to core psychometric and feasibility
standards are more likely to perform consistently well and be found sustainable in
a primary care setting
IntroductionDevelopmental and behavioral problems are among the mostcommon conditions of childhood and adolescence 15 ofchildren have a developmental disability and 21 have a men-tal health disorder If intervention is instituted before kinder-garten entrance many problems can be prevented and thelarge majority can be ameliorated In the United States earlydetection depends heavily on primary care providers Primarycare clinicians should know that the periodic use of generaldevelopmental (1)(2)(3)(4) and social-emotional (5) screen-ing tools has been proven to identify promptly two to six timesmore children (age 0ndash5 years) who have suspected delays thana clinicianrsquos surveillance alone (1)(2)(3)(4)(5) This differencein outcome includes foster care populations in whom pedia-tricians possess knowledge of children being at higher risk fora developmental delay or social-emotional disorder (4)(5)
Abbreviations
ASQ Ages and Stages QuestionnaireASQ-3 Ages amp Stages Questionnaire Third EditionASD autism spectrum disorderECSE early childhood special educationEI early interventionM-CHAT Modified Checklist for Autism in ToddlersNPV negative predictive valuePEDS Parentsrsquo Evaluation of Developmental StatusPEDSDM Parentsrsquo Evaluation of Developmental Statusndash
Developmental MilestonesPPV positive predictive value
Department of Pediatrics PeaceHealth Medical Group Eugene ORdaggerDivision of General Pediatrics School of Medicine Oregon Health amp Science University Portland ORDaggerDepartment of Genetics and Developmental-Behavioral Pediatrics Medical University South Carolina Charleston SC
Article growth and development
448 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
Periodic screening leads to substantial increases inearly intervention (EI) and early childhood special educa-tion (ECSE) eligibility rates (1)(2) Interestingly the per-centage of pediatricians ldquowho self-reported alwaysalmost always using Dagger1 screening toolsrdquo has increased sig-nificantly from 230 to 477 from 2002 to 2009 (6)With greater numbers of clinicians incorporating stan-dardized screening tools into their practices a better un-derstanding of how to optimize their performance isneeded With nearly half of pediatricians still not rou-tinely using standardized tools further education is war-ranted about which tools are feasible for use in primarycare with attention paid to which tools are psychometri-cally sound Education also is warranted on how practi-tioners can better employ screens in a 1) safe 2)equitable 3) effective 4) timely 5) patient- and parent-centered and 6) efficient manner These are the Instituteof Medicinersquos six quality aims
Surveillance is the process in which clinicians watch forsigns of developmental or behavioral problems in thecourse of caring for children Screening refers to the useof brief standardized tools to differentiate those who needa further evaluation for potential problems from those whoprobably do not Although screening measures help to
refine the pattern of delays in children who have detectableproblems they are meant primarily for children perceivedto be asymptomatic by the clinician and for those in whomsurveillance demonstrates risk
Developmental-behavioral screens are different frommany othermedical screens which seek to identify a strictlypositive or negative condition (eg cystic fibrosis congen-ital hypothyroidism phenylketonuria) In fact researchindicates that children who have false-positive screens(screening test positiveconcerning but subsequentlyineligible for EIECSE services) are a high-risk groupin need of diligent monitoring and other community re-sources (2)(7)
There are numerous categories of developmental-behavioral screening instruments (Table 1) used to iden-tify a wide spectrum of developmental-behavioral condi-tions with variable prevalence rates at different ages(Table 2) Parent-report screens (Figs 1ndash3) typically aredesigned to measure one of the first three componentsof developmental-behavioral surveillance 1) elicitingand addressing parentsrsquo concerns 2)maintaining a develop-mental-behavioral history (reviewing milestones and be-haviors) and 3) identifying developmental-behavioralrisk and protective factors (biological and environmental)
Table 1 Common Developmental-Behavioral Screening Tool Categories
I Parent-report measures parental concerns versus milestonesskills and behaviors versus developmental-behavioral(biological and environmental) risk andor protective factors versus a history of parentndashchild interactions versusa combination of all of the aboveII Practitioner-administered directly eliciting andor observing milestonesskills and behaviors about the child andor theparentndashchild interactions In reality many practitioner-administered tools have parent-report items
Broad-band Screening Measures Narrow-band Screening MeasuresA Broad-band family psychosocial 1 Parental mood disorderdepression-specifica
2 Parental substance abusendashspecific3 Domestic violencendashspecific4 Parental adverse childhood experiencendashspecific
B Broad-band (general) developmentala 1 Social-emotional2 Language- and cognitive-specific3 Communicationndashspecific4 Autism-specifica
5 Motor-specificC Broad-band mental healthbehavioralpsychosocial
functiona1 ADHD- oppositional defiant- conduct disorderndashspecific2 Academic- andor literacy-specific3 Anxiety disorderndashspecific4 Depressionmood disorderndashspecificb
5 Substance abusendashspecifica
6 Suicide-specific
ADHDfrac14attention-deficithyperactivity disorderaThe AAP recommends universal postpartum maternal mood disorder screening in the first year (experts recommend 2 4 andor 6 months) generaldevelopmental screening at 9 18 and 30 (or 24) months (AAP experts also recommend a ldquokindergarten readinessrdquo screening at 4 years) autism-specificscreening at 18 and 24 months mental healthpsychosocial function screening at every health supervision visit Dagger5 years and substance abusendashspecificscreening at every health supervision visit throughout adolescencebThe US Prevention Service Task Force recommends depression-specific screening at every health supervision visit throughout adolescence
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 449
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
Practitioner-administered screens (Fig 4) which di-rectly elicit or make observations about the childrsquos skillsand behavior generally measure another component ofsurveillance making accurate and informed observa-tions about the child and parentndashchild interactionsScreens may be broad-band (general) (Figs 1 and 4)meaning they tap all or most developmental-behavioral do-mains (expressive speech and language receptive languagegross motor fine motor cognitiveproblem-solving self-help and adaptive skills social-emotionalbehavior) ornarrow-band (Fig 2) meaning domain- disorder- or dis-ability-specific Narrow-band screens may partially tap oneor more domains but are not designed to assess the widespectrum of development-behavioral conditions at variousages (Table 2) and therefore ideally should always beused in conjunction with a broad-band screen
Current RecommendationsThe American Academy of Pediatrics (AAP) currently rec-ommends universal postpartum mood disorder screeningin the first year after birth general developmental screen-ing at 9 18 and 30 (or 24) months autism-specificscreening at 18 and 24months social-emotional screening
whenever a general or autism-specific instrument is abnor-mal ldquokindergarten readinessrdquo screening at 4 years social-emotionalmental healthpsychosocial function screeningat every health supervision visit from ages 5 to 18 yearsand substance abusendashspecific screening at every healthsupervision visit throughout adolescence
In addition according to the AAP an appropriatescreen should be administered whenever a clinicianrsquos sur-veillance determines ldquoriskrdquo All of these screening recom-mendations have heightened the need for clinicians toimplement office-based and community-based systemsthat are simultaneously effective and efficient especiallyfor those for whom research suggests interventions aremost effective the 257 million children in the UnitedStates who are age lt5 years (projected population in2012 per httpwwwchildstatsgov)
Incorporating Periodic Screening Into OngoingSurveillanceFigure 5 provides a collaborative model for screening andsurveillance in a medical home setting and is a combina-tion of the 2006 developmental 2007 autism spec-trum disorders (ASDs) and 2010 mental health AAP
Table 2 Prevalence of Developmental-Behavioral Conditions in Childrena
Any developmental disability 150 (3ndash17 y in 2006ndash2008)Condition Prevalence ( most studies conducted in the United States)Common conditions (Dagger1)1 Social-emotionalbehavioral disorders bull 21 (children and adolescents who meet criteria for a mental
health disorder with at least minimal impairment in 1999)bull 95ndash142 (ldquoserious emotional disturbancerdquo 0ndash5 y in2006)
2 Speech and language impairment bull 135 (expressive speech delays 18ndash23 mo in 1996ndash2000)bull 175 (expressive speech delays 30ndash36 mo in 1996ndash2000)bull 74 (language impairment kindergarten in 1997)
3 Attention-deficithyperactivity disorder bull 76 (3ndash17 y in 2006ndash2008)bull 41 (4ndash8 y in 2006ndash2008)
4 Learning disability bull 72 (3ndash17 y in 2006ndash2008)5 Developmental coordination disorder bull 6 (5ndash11 y in 2000) 17 (7ndash8 y in 2009)6 Intellectual disabilitymental retardation bull 12 (3ndash10 y in 1991)
bull 067 (3ndash17 y in 2006ndash2008)7 ASDs bull 066 (8 y and 3ndash10 y in 1998)
bull 11b (3ndash17 y in 2006ndash2008)Less common conditions (lt 1)8 Cerebral palsy bull 024 (3ndash10 y in 1991)9 Hearing impairmentc bull 038 (3ndash17 y in 2006ndash2008)10 Vision impairmentd bull 013 (3ndash17 y in 2006ndash2008)
ASDfrac14autism spectrum disorderaPlease note that all of these developmental-behavioral conditions have high rates of comorbiditybIn 2007 the ASD point prevalence was 110 per 10000 (11) Diagnosis of ASD was defined by 1) a physician or other health-care provider who said thatthe child had ASD and 2) that the child currently had the condition Nearly 40 of those ever diagnosed with ASD did not currently have the condition at thetime of a random-digit-dial telephone National Survey of Childrenrsquos Health (sample size frac14 78037)cDefined by the Centers for Disease Control and Prevention as moderate hearing loss (40 dB) or worse unaided in the better eardDefined by the Centers for Disease Control and Prevention as 2070 visual acuity or worse with correction in the better eye
growth and development developmental-behavioral screening measures
450 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
algorithms (8) When a psychometrically sound screen rai-ses concerns the algorithm emphasizes system-widereferral care coordination and a secondary screening orassessment which in a primary care setting is best ac-complished with the help of an EIECSE agency andan early return (pound1 month) office visit
In this algorithm pediatric clinicians are encouragedto refer automatically when their clinical impressionconfidently detects a developmental delay or if the childpossesses a biological or environmental condition associatedwith a sufficiently high probability of a delay developmental-behavioral promotion has been formally incorporated as acomponent of surveillance to make the process safer more
effective and parent-centered plusgreater detail has been providedabout the decisions and actionsteps that should reliably occur af-ter a screening test is administered(ie postscreening surveillance) (8)
ldquoStructured surveillancerdquo meansthat the process and decision-makingare enhanced with periodic screeningby using evidence-based measures(8) ldquoUnstructured surveillancerdquomeans that the process and decision-making are reliant on subjective im-pressions or casual observations (8)In a systematic review a pediatricclinicianrsquos unstructured surveillancewhen compared with a validatedscreening tool or a diagnostic inter-view has good specificity (the propor-tion of children correctly identifiedas not having a developmental-behavioral problem) ranging from69 to 100 but poor sensitivity(the proportion of children correctlyidentified as having a developmental-behavioral problem) ranging from14 to 54 (9)
When pediatric health-care pro-viders detect a problem they usuallyare correct however they struggleto identify the majority of delaysmost likely because they over-relyon psychometrically unsound mile-stone checklists with vague referralcriteria (1)(2)(8) As a result thelarge majority of children who haveevolving developmental-behavioralproblems can be deprived of the ben-
efits of EI ECSE or other evidence-based communityservices before kindergarten entrance
Periodic screening (ie structured surveillance) has beenproven repeatedly to enhance a clinicianrsquos ability todetect refer and monitor children who have evolvingdevelopmental-behavioral problems (1)(2)(3)(4)(5)(8)
Limitations of Screening in Primary CareAlthough standardized screening improves the quality ofcare at health supervision visits increases parental satisfac-tion leads to substantial cost savings for society and pos-itively affects the lives of children and families via the
Figure 1 Broad-band (general) developmental parent-report screening measures Corestandards are highlighted in yellow See text to explain shading and see Table 3 forabbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 451
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
benefits of EI and ECSE clinicians should be aware thatscreening has its limitations No single instrument willsuffice to identify every developmental-behavioral prob-lem and match the needs of every population or practicesetting The population screened and the method of im-plementation affect the psychometric properties ofa screening measure Screens can be falsely negative(ie they can yield negative or borderline results butthe child could be promptly deemed eligible for EIECSE services) or falsely positive (ie the screening testis positive or concerning but the child is subsequentlydeemed EIECSE ineligible) However a clinicianrsquos
longitudinal surveillance can beused to better interpret the typicalor borderline results of a screeningtest
For example when a pediatri-cian confidently suspects a delayand simultaneously a screen suchas the Ages and Stages Question-naire (ASQ) is found to be typicalor borderline 92 of pediatrician-referred children (blind to ASQ re-sults) promptly receive some formof EI services (40 are found to beEI-eligible 52 are placed on anEI-monitoring list) (1) Howeverthere is no evidence to support theconcept that unstructured surveil-lance should be used to overridethe concerning results of a psycho-metrically sound screen and negatethe need for a community-basedreferral (8) Children who failscreening tests and subsequentlyare not promptly found to have adevelopmental-behavioral diagno-sis (false-positives) nonethelesstend to have numerous psychoso-cial risk factors and exhibit perfor-mance well below average in thebetter predictors of school suc-cess pre-academics languageand intelligence (7) Indeed chil-dren found to have false-positivescreening results are a high-riskgroup in need of closer monitoringrepeat screenings at subsequentvisits and other community re-sources (eg evidence-based par-enting programs nurse home visit
programs high-quality child care structured preschoolssuch as Head Start)
Evaluating Specific Characteristics ofScreening MeasuresAlthough experts agree that no single screening instrumentwill suffice to identify every developmental-behavioralproblem in every practice setting it is also true thatall screening tools are not constructed equal In 2008Drotar et al (10) provided guidelines to help pediatri-cians select which screening tools were best-suited totheir practices based on their populationrsquos risk level
Figure 2 Narrow-band parent-report social-emotional (SE) communication amp autism-specific screens Data not included for the M-CHAT Follow-up Interview (FI) which isrecommended for any failed M-CHAT Core standards are highlighted in yellow See textto explain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
452 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
For general developmental parent-report tools Drotaret al recommended the ASQ and Parentsrsquo Evaluation ofDevelopmental Status (PEDS) for general primary carepopulations and the ASQ specifically for high-risk popula-tions For ASD-specific screening tools the ModifiedChecklist for Autism in Toddlers (M-CHAT) was recom-mended for general primary care populations For furtherdetails and recommendations refer to httpwwwcmwforgContentPublicationsFund-Manuals2008FebPediatric-Developmental-ScreeningndashUnderstanding-and-Selecting-Screening-Instrumentsaspx
Since 2008 new tools have been developed (eg Pa-rentsrsquo Evaluation of Developmental StatusndashDevelopmental
Milestones [PEDSDM] Quantita-tive Checklist for Autism in Tod-dlers) and others have undergonerevisions (eg Ages amp Stages Ques-tionnaire Third Edition [ASQ-3])In 2009 an AAP periodic surveyin concert with the screening toolselection trends in national andstatewide implementation initiativescollectively suggested that the ASQPEDS and M-CHAT have emergedas the three most commonly selectedscreening instruments for childrenage 0 to 5 years in US primary caresettings (6)
For broad-band developmentalscreening tools from 2002 to2009 pediatriciansrsquo use of the ASQincreased from 73 to 224 anduse of the PEDS increased from24 to 159 (6) In 2011 a well-designed study indicated that theASQ (second edition) was signifi-cantly more accurate than the PEDSespecially for children over age 30months in the identification of de-velopmental delays in a primary caresetting (11) The strengths of theASQ include its accuracy (both over-all and across all age ranges) and itsability to be used as a developmentalpromotion tool When caregiversmark ldquonot yetrdquo to an item becausethey have never tried that particulardevelopmental task with their childthis is considered a ldquoteachable mo-mentrdquo where clinicians can promotea new developmental activity
Although multiple primary care studies suggest thatthe paper-based ASQ is feasible it does require gettingall items on the correct age-interval ASQ thoughtfullycompleted by caregivers (and then correctly scored) beforethe health supervision visit In contrast the strength ofthe PEDS is its feasibility as a previsit screen with its 2- to5-minute administration time fourth- to fifth-grade read-ing level and single questionnaire format for all ages
Interestingly the PEDS has been designed to detecta broader array of ldquoat-riskrdquo (not just ldquodelayedrdquo) childrenand can be used not only as a screening and surveillancemeasure but also as a scaffold to enhance parentndashprovidercommunication Compared with the ASQ a higher
Figure 3 Mental healthbehavior screening amp assessment measures (used mostly inschool age children) Commonly used ADHD tools were included per the editorrsquos requesthowever an exhaustive list of depression- anxiety- and substance abuse-specificscreening tools was not included Core standards are highlighted in yellow See text toexplain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 453
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
percentage of children who have concerning or positivescreens on the PEDS which casts a ldquobroad netrdquo willbe found ineligible for EIECSE services and a higherpercentage of children who have delays will be missed be-cause of a negative screening result (although this findingvaries by age)
Of note the accuracy and feasibility of the ASQ andPEDS theoretically improve with online modalities that au-tomatically correct for prematurity foster a more thought-ful at-homeprevisit implementation approach and scoreresults without interference from human error Also withits online modality the PEDS can be used in combinationwith the PEDSDM
For autism-specific screening tools research now indi-cates that the M-CHAT follow-up interview should be
administered routinely for any pos-itive or borderline M-CHAT resultdue to a high false-positive rate(w90 are not subsequently diag-nosed as having ASD) when usingthe M-CHAT at 18 and 24 monthsin a general primary care popula-tion (8)
The strength of the M-CHAT isits feasibility and that it is far less likelyto miss a case of autism comparedwith a clinicianrsquos unstructured surveil-lance (8) Any positive M-CHAT re-sult should lead to an EIECSEagency referral and ideally an earlyreturn office visit for further as-sessment Unfortunately a positiveM-CHATdoes not necessarily justifyan expensive comprehensive ASD-specific evaluation and EI plan in allcases Children who screen positiveon the M-CHAT plus Follow-up In-terview should be referred for anASD-specific EI plan and compre-hensive evaluation Although somechildren will not be diagnosed as hav-ing ASD ultimately over-referralsare not a major concern becausethose not diagnosed as having ASDgenerally have other developmentaldisorders predominantly languageimpairment or cognitive disabilities
Of note unstructured surveillance(eg caregiver concerns about ASDworrisome social-communicationdeficits or behavioral observations
or having a sibling who has ASD) still should be usedin combination with the interpretation of a screening tool(eg a number of ldquocriticalrdquo M-CHAT items failed) to de-termine the need for an ASD-specific comprehensive eval-uation and EI plan without need for the follow-upinterview
To develop a deeper understanding about thestrengths and weaknesses of various screening tools anunderstanding is needed about the basic precepts behindpsychometric and feasibility standards Core standards af-fect a screening toolrsquos application to a primary care setting(eg performance on a wide variety of populations screen-ing tool completion rates sustainability over time) Thequestion arises what is a core standard Throughout thisarticle a core standard is defined as an inflexible property
Figure 4 Broad-band (general) developmental practitioner-administered screening andassessment measures Core standards are highlighted in yellow See text to explainshading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
454 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

Understanding Developmental-BehavioralScreening MeasuresKevin P Marks MDdagger
Angela C LaRosa MDDagger
Author Disclosure
Drs Marks and LaRosa
have disclosed no
financial relationships
relevant to this article
This commentary
does not contain
a discussion of an
unapproved
investigative use of
a commercial product
device
Educational Gap
With nearly half of pediatricians still not using standardized screening tools primary care
clinicians should know that the periodic use of general developmental and social-emotional
screening tools has been proven to identify promptly two to six times more children (age 0ndash
5 years) with suspected delays than a clinicianrsquos unstructured surveillance alone
Objectives After completing this article readers should be able to
1 Recognize the many methods available to detect a wide spectrum of developmental
and behavioral conditions with screening tools and the screening schedule
recommended by the AAP
2 Recognize that universal periodic screening with psychometrically sound
developmental-behavioral instruments greatly enhances a clinicianrsquos ability to detect
refer and monitor children who have evolving developmental and behavioral
problems A pediatric providerrsquos impression has good specificity but poor sensitivity
and thus has difficulty identifying the less obvious delays
3 Know that children who have false-positive screens (screening test concerning but
subsequently ineligible for early intervention or early childhood special education
services) are a high-risk group in need of close monitoring and other community
services such as evidence-based parenting programs and Head Start
4 Know the main limitations of applying standardized screening tools into a primary
care setting
5 Be aware that screening measures which adhere to core psychometric and feasibility
standards are more likely to perform consistently well and be found sustainable in
a primary care setting
IntroductionDevelopmental and behavioral problems are among the mostcommon conditions of childhood and adolescence 15 ofchildren have a developmental disability and 21 have a men-tal health disorder If intervention is instituted before kinder-garten entrance many problems can be prevented and thelarge majority can be ameliorated In the United States earlydetection depends heavily on primary care providers Primarycare clinicians should know that the periodic use of generaldevelopmental (1)(2)(3)(4) and social-emotional (5) screen-ing tools has been proven to identify promptly two to six timesmore children (age 0ndash5 years) who have suspected delays thana clinicianrsquos surveillance alone (1)(2)(3)(4)(5) This differencein outcome includes foster care populations in whom pedia-tricians possess knowledge of children being at higher risk fora developmental delay or social-emotional disorder (4)(5)
Abbreviations
ASQ Ages and Stages QuestionnaireASQ-3 Ages amp Stages Questionnaire Third EditionASD autism spectrum disorderECSE early childhood special educationEI early interventionM-CHAT Modified Checklist for Autism in ToddlersNPV negative predictive valuePEDS Parentsrsquo Evaluation of Developmental StatusPEDSDM Parentsrsquo Evaluation of Developmental Statusndash
Developmental MilestonesPPV positive predictive value
Department of Pediatrics PeaceHealth Medical Group Eugene ORdaggerDivision of General Pediatrics School of Medicine Oregon Health amp Science University Portland ORDaggerDepartment of Genetics and Developmental-Behavioral Pediatrics Medical University South Carolina Charleston SC
Article growth and development
448 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
Periodic screening leads to substantial increases inearly intervention (EI) and early childhood special educa-tion (ECSE) eligibility rates (1)(2) Interestingly the per-centage of pediatricians ldquowho self-reported alwaysalmost always using Dagger1 screening toolsrdquo has increased sig-nificantly from 230 to 477 from 2002 to 2009 (6)With greater numbers of clinicians incorporating stan-dardized screening tools into their practices a better un-derstanding of how to optimize their performance isneeded With nearly half of pediatricians still not rou-tinely using standardized tools further education is war-ranted about which tools are feasible for use in primarycare with attention paid to which tools are psychometri-cally sound Education also is warranted on how practi-tioners can better employ screens in a 1) safe 2)equitable 3) effective 4) timely 5) patient- and parent-centered and 6) efficient manner These are the Instituteof Medicinersquos six quality aims
Surveillance is the process in which clinicians watch forsigns of developmental or behavioral problems in thecourse of caring for children Screening refers to the useof brief standardized tools to differentiate those who needa further evaluation for potential problems from those whoprobably do not Although screening measures help to
refine the pattern of delays in children who have detectableproblems they are meant primarily for children perceivedto be asymptomatic by the clinician and for those in whomsurveillance demonstrates risk
Developmental-behavioral screens are different frommany othermedical screens which seek to identify a strictlypositive or negative condition (eg cystic fibrosis congen-ital hypothyroidism phenylketonuria) In fact researchindicates that children who have false-positive screens(screening test positiveconcerning but subsequentlyineligible for EIECSE services) are a high-risk groupin need of diligent monitoring and other community re-sources (2)(7)
There are numerous categories of developmental-behavioral screening instruments (Table 1) used to iden-tify a wide spectrum of developmental-behavioral condi-tions with variable prevalence rates at different ages(Table 2) Parent-report screens (Figs 1ndash3) typically aredesigned to measure one of the first three componentsof developmental-behavioral surveillance 1) elicitingand addressing parentsrsquo concerns 2)maintaining a develop-mental-behavioral history (reviewing milestones and be-haviors) and 3) identifying developmental-behavioralrisk and protective factors (biological and environmental)
Table 1 Common Developmental-Behavioral Screening Tool Categories
I Parent-report measures parental concerns versus milestonesskills and behaviors versus developmental-behavioral(biological and environmental) risk andor protective factors versus a history of parentndashchild interactions versusa combination of all of the aboveII Practitioner-administered directly eliciting andor observing milestonesskills and behaviors about the child andor theparentndashchild interactions In reality many practitioner-administered tools have parent-report items
Broad-band Screening Measures Narrow-band Screening MeasuresA Broad-band family psychosocial 1 Parental mood disorderdepression-specifica
2 Parental substance abusendashspecific3 Domestic violencendashspecific4 Parental adverse childhood experiencendashspecific
B Broad-band (general) developmentala 1 Social-emotional2 Language- and cognitive-specific3 Communicationndashspecific4 Autism-specifica
5 Motor-specificC Broad-band mental healthbehavioralpsychosocial
functiona1 ADHD- oppositional defiant- conduct disorderndashspecific2 Academic- andor literacy-specific3 Anxiety disorderndashspecific4 Depressionmood disorderndashspecificb
5 Substance abusendashspecifica
6 Suicide-specific
ADHDfrac14attention-deficithyperactivity disorderaThe AAP recommends universal postpartum maternal mood disorder screening in the first year (experts recommend 2 4 andor 6 months) generaldevelopmental screening at 9 18 and 30 (or 24) months (AAP experts also recommend a ldquokindergarten readinessrdquo screening at 4 years) autism-specificscreening at 18 and 24 months mental healthpsychosocial function screening at every health supervision visit Dagger5 years and substance abusendashspecificscreening at every health supervision visit throughout adolescencebThe US Prevention Service Task Force recommends depression-specific screening at every health supervision visit throughout adolescence
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 449
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
Practitioner-administered screens (Fig 4) which di-rectly elicit or make observations about the childrsquos skillsand behavior generally measure another component ofsurveillance making accurate and informed observa-tions about the child and parentndashchild interactionsScreens may be broad-band (general) (Figs 1 and 4)meaning they tap all or most developmental-behavioral do-mains (expressive speech and language receptive languagegross motor fine motor cognitiveproblem-solving self-help and adaptive skills social-emotionalbehavior) ornarrow-band (Fig 2) meaning domain- disorder- or dis-ability-specific Narrow-band screens may partially tap oneor more domains but are not designed to assess the widespectrum of development-behavioral conditions at variousages (Table 2) and therefore ideally should always beused in conjunction with a broad-band screen
Current RecommendationsThe American Academy of Pediatrics (AAP) currently rec-ommends universal postpartum mood disorder screeningin the first year after birth general developmental screen-ing at 9 18 and 30 (or 24) months autism-specificscreening at 18 and 24months social-emotional screening
whenever a general or autism-specific instrument is abnor-mal ldquokindergarten readinessrdquo screening at 4 years social-emotionalmental healthpsychosocial function screeningat every health supervision visit from ages 5 to 18 yearsand substance abusendashspecific screening at every healthsupervision visit throughout adolescence
In addition according to the AAP an appropriatescreen should be administered whenever a clinicianrsquos sur-veillance determines ldquoriskrdquo All of these screening recom-mendations have heightened the need for clinicians toimplement office-based and community-based systemsthat are simultaneously effective and efficient especiallyfor those for whom research suggests interventions aremost effective the 257 million children in the UnitedStates who are age lt5 years (projected population in2012 per httpwwwchildstatsgov)
Incorporating Periodic Screening Into OngoingSurveillanceFigure 5 provides a collaborative model for screening andsurveillance in a medical home setting and is a combina-tion of the 2006 developmental 2007 autism spec-trum disorders (ASDs) and 2010 mental health AAP
Table 2 Prevalence of Developmental-Behavioral Conditions in Childrena
Any developmental disability 150 (3ndash17 y in 2006ndash2008)Condition Prevalence ( most studies conducted in the United States)Common conditions (Dagger1)1 Social-emotionalbehavioral disorders bull 21 (children and adolescents who meet criteria for a mental
health disorder with at least minimal impairment in 1999)bull 95ndash142 (ldquoserious emotional disturbancerdquo 0ndash5 y in2006)
2 Speech and language impairment bull 135 (expressive speech delays 18ndash23 mo in 1996ndash2000)bull 175 (expressive speech delays 30ndash36 mo in 1996ndash2000)bull 74 (language impairment kindergarten in 1997)
3 Attention-deficithyperactivity disorder bull 76 (3ndash17 y in 2006ndash2008)bull 41 (4ndash8 y in 2006ndash2008)
4 Learning disability bull 72 (3ndash17 y in 2006ndash2008)5 Developmental coordination disorder bull 6 (5ndash11 y in 2000) 17 (7ndash8 y in 2009)6 Intellectual disabilitymental retardation bull 12 (3ndash10 y in 1991)
bull 067 (3ndash17 y in 2006ndash2008)7 ASDs bull 066 (8 y and 3ndash10 y in 1998)
bull 11b (3ndash17 y in 2006ndash2008)Less common conditions (lt 1)8 Cerebral palsy bull 024 (3ndash10 y in 1991)9 Hearing impairmentc bull 038 (3ndash17 y in 2006ndash2008)10 Vision impairmentd bull 013 (3ndash17 y in 2006ndash2008)
ASDfrac14autism spectrum disorderaPlease note that all of these developmental-behavioral conditions have high rates of comorbiditybIn 2007 the ASD point prevalence was 110 per 10000 (11) Diagnosis of ASD was defined by 1) a physician or other health-care provider who said thatthe child had ASD and 2) that the child currently had the condition Nearly 40 of those ever diagnosed with ASD did not currently have the condition at thetime of a random-digit-dial telephone National Survey of Childrenrsquos Health (sample size frac14 78037)cDefined by the Centers for Disease Control and Prevention as moderate hearing loss (40 dB) or worse unaided in the better eardDefined by the Centers for Disease Control and Prevention as 2070 visual acuity or worse with correction in the better eye
growth and development developmental-behavioral screening measures
450 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
algorithms (8) When a psychometrically sound screen rai-ses concerns the algorithm emphasizes system-widereferral care coordination and a secondary screening orassessment which in a primary care setting is best ac-complished with the help of an EIECSE agency andan early return (pound1 month) office visit
In this algorithm pediatric clinicians are encouragedto refer automatically when their clinical impressionconfidently detects a developmental delay or if the childpossesses a biological or environmental condition associatedwith a sufficiently high probability of a delay developmental-behavioral promotion has been formally incorporated as acomponent of surveillance to make the process safer more
effective and parent-centered plusgreater detail has been providedabout the decisions and actionsteps that should reliably occur af-ter a screening test is administered(ie postscreening surveillance) (8)
ldquoStructured surveillancerdquo meansthat the process and decision-makingare enhanced with periodic screeningby using evidence-based measures(8) ldquoUnstructured surveillancerdquomeans that the process and decision-making are reliant on subjective im-pressions or casual observations (8)In a systematic review a pediatricclinicianrsquos unstructured surveillancewhen compared with a validatedscreening tool or a diagnostic inter-view has good specificity (the propor-tion of children correctly identifiedas not having a developmental-behavioral problem) ranging from69 to 100 but poor sensitivity(the proportion of children correctlyidentified as having a developmental-behavioral problem) ranging from14 to 54 (9)
When pediatric health-care pro-viders detect a problem they usuallyare correct however they struggleto identify the majority of delaysmost likely because they over-relyon psychometrically unsound mile-stone checklists with vague referralcriteria (1)(2)(8) As a result thelarge majority of children who haveevolving developmental-behavioralproblems can be deprived of the ben-
efits of EI ECSE or other evidence-based communityservices before kindergarten entrance
Periodic screening (ie structured surveillance) has beenproven repeatedly to enhance a clinicianrsquos ability todetect refer and monitor children who have evolvingdevelopmental-behavioral problems (1)(2)(3)(4)(5)(8)
Limitations of Screening in Primary CareAlthough standardized screening improves the quality ofcare at health supervision visits increases parental satisfac-tion leads to substantial cost savings for society and pos-itively affects the lives of children and families via the
Figure 1 Broad-band (general) developmental parent-report screening measures Corestandards are highlighted in yellow See text to explain shading and see Table 3 forabbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 451
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
benefits of EI and ECSE clinicians should be aware thatscreening has its limitations No single instrument willsuffice to identify every developmental-behavioral prob-lem and match the needs of every population or practicesetting The population screened and the method of im-plementation affect the psychometric properties ofa screening measure Screens can be falsely negative(ie they can yield negative or borderline results butthe child could be promptly deemed eligible for EIECSE services) or falsely positive (ie the screening testis positive or concerning but the child is subsequentlydeemed EIECSE ineligible) However a clinicianrsquos
longitudinal surveillance can beused to better interpret the typicalor borderline results of a screeningtest
For example when a pediatri-cian confidently suspects a delayand simultaneously a screen suchas the Ages and Stages Question-naire (ASQ) is found to be typicalor borderline 92 of pediatrician-referred children (blind to ASQ re-sults) promptly receive some formof EI services (40 are found to beEI-eligible 52 are placed on anEI-monitoring list) (1) Howeverthere is no evidence to support theconcept that unstructured surveil-lance should be used to overridethe concerning results of a psycho-metrically sound screen and negatethe need for a community-basedreferral (8) Children who failscreening tests and subsequentlyare not promptly found to have adevelopmental-behavioral diagno-sis (false-positives) nonethelesstend to have numerous psychoso-cial risk factors and exhibit perfor-mance well below average in thebetter predictors of school suc-cess pre-academics languageand intelligence (7) Indeed chil-dren found to have false-positivescreening results are a high-riskgroup in need of closer monitoringrepeat screenings at subsequentvisits and other community re-sources (eg evidence-based par-enting programs nurse home visit
programs high-quality child care structured preschoolssuch as Head Start)
Evaluating Specific Characteristics ofScreening MeasuresAlthough experts agree that no single screening instrumentwill suffice to identify every developmental-behavioralproblem in every practice setting it is also true thatall screening tools are not constructed equal In 2008Drotar et al (10) provided guidelines to help pediatri-cians select which screening tools were best-suited totheir practices based on their populationrsquos risk level
Figure 2 Narrow-band parent-report social-emotional (SE) communication amp autism-specific screens Data not included for the M-CHAT Follow-up Interview (FI) which isrecommended for any failed M-CHAT Core standards are highlighted in yellow See textto explain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
452 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
For general developmental parent-report tools Drotaret al recommended the ASQ and Parentsrsquo Evaluation ofDevelopmental Status (PEDS) for general primary carepopulations and the ASQ specifically for high-risk popula-tions For ASD-specific screening tools the ModifiedChecklist for Autism in Toddlers (M-CHAT) was recom-mended for general primary care populations For furtherdetails and recommendations refer to httpwwwcmwforgContentPublicationsFund-Manuals2008FebPediatric-Developmental-ScreeningndashUnderstanding-and-Selecting-Screening-Instrumentsaspx
Since 2008 new tools have been developed (eg Pa-rentsrsquo Evaluation of Developmental StatusndashDevelopmental
Milestones [PEDSDM] Quantita-tive Checklist for Autism in Tod-dlers) and others have undergonerevisions (eg Ages amp Stages Ques-tionnaire Third Edition [ASQ-3])In 2009 an AAP periodic surveyin concert with the screening toolselection trends in national andstatewide implementation initiativescollectively suggested that the ASQPEDS and M-CHAT have emergedas the three most commonly selectedscreening instruments for childrenage 0 to 5 years in US primary caresettings (6)
For broad-band developmentalscreening tools from 2002 to2009 pediatriciansrsquo use of the ASQincreased from 73 to 224 anduse of the PEDS increased from24 to 159 (6) In 2011 a well-designed study indicated that theASQ (second edition) was signifi-cantly more accurate than the PEDSespecially for children over age 30months in the identification of de-velopmental delays in a primary caresetting (11) The strengths of theASQ include its accuracy (both over-all and across all age ranges) and itsability to be used as a developmentalpromotion tool When caregiversmark ldquonot yetrdquo to an item becausethey have never tried that particulardevelopmental task with their childthis is considered a ldquoteachable mo-mentrdquo where clinicians can promotea new developmental activity
Although multiple primary care studies suggest thatthe paper-based ASQ is feasible it does require gettingall items on the correct age-interval ASQ thoughtfullycompleted by caregivers (and then correctly scored) beforethe health supervision visit In contrast the strength ofthe PEDS is its feasibility as a previsit screen with its 2- to5-minute administration time fourth- to fifth-grade read-ing level and single questionnaire format for all ages
Interestingly the PEDS has been designed to detecta broader array of ldquoat-riskrdquo (not just ldquodelayedrdquo) childrenand can be used not only as a screening and surveillancemeasure but also as a scaffold to enhance parentndashprovidercommunication Compared with the ASQ a higher
Figure 3 Mental healthbehavior screening amp assessment measures (used mostly inschool age children) Commonly used ADHD tools were included per the editorrsquos requesthowever an exhaustive list of depression- anxiety- and substance abuse-specificscreening tools was not included Core standards are highlighted in yellow See text toexplain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 453
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
percentage of children who have concerning or positivescreens on the PEDS which casts a ldquobroad netrdquo willbe found ineligible for EIECSE services and a higherpercentage of children who have delays will be missed be-cause of a negative screening result (although this findingvaries by age)
Of note the accuracy and feasibility of the ASQ andPEDS theoretically improve with online modalities that au-tomatically correct for prematurity foster a more thought-ful at-homeprevisit implementation approach and scoreresults without interference from human error Also withits online modality the PEDS can be used in combinationwith the PEDSDM
For autism-specific screening tools research now indi-cates that the M-CHAT follow-up interview should be
administered routinely for any pos-itive or borderline M-CHAT resultdue to a high false-positive rate(w90 are not subsequently diag-nosed as having ASD) when usingthe M-CHAT at 18 and 24 monthsin a general primary care popula-tion (8)
The strength of the M-CHAT isits feasibility and that it is far less likelyto miss a case of autism comparedwith a clinicianrsquos unstructured surveil-lance (8) Any positive M-CHAT re-sult should lead to an EIECSEagency referral and ideally an earlyreturn office visit for further as-sessment Unfortunately a positiveM-CHATdoes not necessarily justifyan expensive comprehensive ASD-specific evaluation and EI plan in allcases Children who screen positiveon the M-CHAT plus Follow-up In-terview should be referred for anASD-specific EI plan and compre-hensive evaluation Although somechildren will not be diagnosed as hav-ing ASD ultimately over-referralsare not a major concern becausethose not diagnosed as having ASDgenerally have other developmentaldisorders predominantly languageimpairment or cognitive disabilities
Of note unstructured surveillance(eg caregiver concerns about ASDworrisome social-communicationdeficits or behavioral observations
or having a sibling who has ASD) still should be usedin combination with the interpretation of a screening tool(eg a number of ldquocriticalrdquo M-CHAT items failed) to de-termine the need for an ASD-specific comprehensive eval-uation and EI plan without need for the follow-upinterview
To develop a deeper understanding about thestrengths and weaknesses of various screening tools anunderstanding is needed about the basic precepts behindpsychometric and feasibility standards Core standards af-fect a screening toolrsquos application to a primary care setting(eg performance on a wide variety of populations screen-ing tool completion rates sustainability over time) Thequestion arises what is a core standard Throughout thisarticle a core standard is defined as an inflexible property
Figure 4 Broad-band (general) developmental practitioner-administered screening andassessment measures Core standards are highlighted in yellow See text to explainshading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
454 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

Periodic screening leads to substantial increases inearly intervention (EI) and early childhood special educa-tion (ECSE) eligibility rates (1)(2) Interestingly the per-centage of pediatricians ldquowho self-reported alwaysalmost always using Dagger1 screening toolsrdquo has increased sig-nificantly from 230 to 477 from 2002 to 2009 (6)With greater numbers of clinicians incorporating stan-dardized screening tools into their practices a better un-derstanding of how to optimize their performance isneeded With nearly half of pediatricians still not rou-tinely using standardized tools further education is war-ranted about which tools are feasible for use in primarycare with attention paid to which tools are psychometri-cally sound Education also is warranted on how practi-tioners can better employ screens in a 1) safe 2)equitable 3) effective 4) timely 5) patient- and parent-centered and 6) efficient manner These are the Instituteof Medicinersquos six quality aims
Surveillance is the process in which clinicians watch forsigns of developmental or behavioral problems in thecourse of caring for children Screening refers to the useof brief standardized tools to differentiate those who needa further evaluation for potential problems from those whoprobably do not Although screening measures help to
refine the pattern of delays in children who have detectableproblems they are meant primarily for children perceivedto be asymptomatic by the clinician and for those in whomsurveillance demonstrates risk
Developmental-behavioral screens are different frommany othermedical screens which seek to identify a strictlypositive or negative condition (eg cystic fibrosis congen-ital hypothyroidism phenylketonuria) In fact researchindicates that children who have false-positive screens(screening test positiveconcerning but subsequentlyineligible for EIECSE services) are a high-risk groupin need of diligent monitoring and other community re-sources (2)(7)
There are numerous categories of developmental-behavioral screening instruments (Table 1) used to iden-tify a wide spectrum of developmental-behavioral condi-tions with variable prevalence rates at different ages(Table 2) Parent-report screens (Figs 1ndash3) typically aredesigned to measure one of the first three componentsof developmental-behavioral surveillance 1) elicitingand addressing parentsrsquo concerns 2)maintaining a develop-mental-behavioral history (reviewing milestones and be-haviors) and 3) identifying developmental-behavioralrisk and protective factors (biological and environmental)
Table 1 Common Developmental-Behavioral Screening Tool Categories
I Parent-report measures parental concerns versus milestonesskills and behaviors versus developmental-behavioral(biological and environmental) risk andor protective factors versus a history of parentndashchild interactions versusa combination of all of the aboveII Practitioner-administered directly eliciting andor observing milestonesskills and behaviors about the child andor theparentndashchild interactions In reality many practitioner-administered tools have parent-report items
Broad-band Screening Measures Narrow-band Screening MeasuresA Broad-band family psychosocial 1 Parental mood disorderdepression-specifica
2 Parental substance abusendashspecific3 Domestic violencendashspecific4 Parental adverse childhood experiencendashspecific
B Broad-band (general) developmentala 1 Social-emotional2 Language- and cognitive-specific3 Communicationndashspecific4 Autism-specifica
5 Motor-specificC Broad-band mental healthbehavioralpsychosocial
functiona1 ADHD- oppositional defiant- conduct disorderndashspecific2 Academic- andor literacy-specific3 Anxiety disorderndashspecific4 Depressionmood disorderndashspecificb
5 Substance abusendashspecifica
6 Suicide-specific
ADHDfrac14attention-deficithyperactivity disorderaThe AAP recommends universal postpartum maternal mood disorder screening in the first year (experts recommend 2 4 andor 6 months) generaldevelopmental screening at 9 18 and 30 (or 24) months (AAP experts also recommend a ldquokindergarten readinessrdquo screening at 4 years) autism-specificscreening at 18 and 24 months mental healthpsychosocial function screening at every health supervision visit Dagger5 years and substance abusendashspecificscreening at every health supervision visit throughout adolescencebThe US Prevention Service Task Force recommends depression-specific screening at every health supervision visit throughout adolescence
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 449
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
Practitioner-administered screens (Fig 4) which di-rectly elicit or make observations about the childrsquos skillsand behavior generally measure another component ofsurveillance making accurate and informed observa-tions about the child and parentndashchild interactionsScreens may be broad-band (general) (Figs 1 and 4)meaning they tap all or most developmental-behavioral do-mains (expressive speech and language receptive languagegross motor fine motor cognitiveproblem-solving self-help and adaptive skills social-emotionalbehavior) ornarrow-band (Fig 2) meaning domain- disorder- or dis-ability-specific Narrow-band screens may partially tap oneor more domains but are not designed to assess the widespectrum of development-behavioral conditions at variousages (Table 2) and therefore ideally should always beused in conjunction with a broad-band screen
Current RecommendationsThe American Academy of Pediatrics (AAP) currently rec-ommends universal postpartum mood disorder screeningin the first year after birth general developmental screen-ing at 9 18 and 30 (or 24) months autism-specificscreening at 18 and 24months social-emotional screening
whenever a general or autism-specific instrument is abnor-mal ldquokindergarten readinessrdquo screening at 4 years social-emotionalmental healthpsychosocial function screeningat every health supervision visit from ages 5 to 18 yearsand substance abusendashspecific screening at every healthsupervision visit throughout adolescence
In addition according to the AAP an appropriatescreen should be administered whenever a clinicianrsquos sur-veillance determines ldquoriskrdquo All of these screening recom-mendations have heightened the need for clinicians toimplement office-based and community-based systemsthat are simultaneously effective and efficient especiallyfor those for whom research suggests interventions aremost effective the 257 million children in the UnitedStates who are age lt5 years (projected population in2012 per httpwwwchildstatsgov)
Incorporating Periodic Screening Into OngoingSurveillanceFigure 5 provides a collaborative model for screening andsurveillance in a medical home setting and is a combina-tion of the 2006 developmental 2007 autism spec-trum disorders (ASDs) and 2010 mental health AAP
Table 2 Prevalence of Developmental-Behavioral Conditions in Childrena
Any developmental disability 150 (3ndash17 y in 2006ndash2008)Condition Prevalence ( most studies conducted in the United States)Common conditions (Dagger1)1 Social-emotionalbehavioral disorders bull 21 (children and adolescents who meet criteria for a mental
health disorder with at least minimal impairment in 1999)bull 95ndash142 (ldquoserious emotional disturbancerdquo 0ndash5 y in2006)
2 Speech and language impairment bull 135 (expressive speech delays 18ndash23 mo in 1996ndash2000)bull 175 (expressive speech delays 30ndash36 mo in 1996ndash2000)bull 74 (language impairment kindergarten in 1997)
3 Attention-deficithyperactivity disorder bull 76 (3ndash17 y in 2006ndash2008)bull 41 (4ndash8 y in 2006ndash2008)
4 Learning disability bull 72 (3ndash17 y in 2006ndash2008)5 Developmental coordination disorder bull 6 (5ndash11 y in 2000) 17 (7ndash8 y in 2009)6 Intellectual disabilitymental retardation bull 12 (3ndash10 y in 1991)
bull 067 (3ndash17 y in 2006ndash2008)7 ASDs bull 066 (8 y and 3ndash10 y in 1998)
bull 11b (3ndash17 y in 2006ndash2008)Less common conditions (lt 1)8 Cerebral palsy bull 024 (3ndash10 y in 1991)9 Hearing impairmentc bull 038 (3ndash17 y in 2006ndash2008)10 Vision impairmentd bull 013 (3ndash17 y in 2006ndash2008)
ASDfrac14autism spectrum disorderaPlease note that all of these developmental-behavioral conditions have high rates of comorbiditybIn 2007 the ASD point prevalence was 110 per 10000 (11) Diagnosis of ASD was defined by 1) a physician or other health-care provider who said thatthe child had ASD and 2) that the child currently had the condition Nearly 40 of those ever diagnosed with ASD did not currently have the condition at thetime of a random-digit-dial telephone National Survey of Childrenrsquos Health (sample size frac14 78037)cDefined by the Centers for Disease Control and Prevention as moderate hearing loss (40 dB) or worse unaided in the better eardDefined by the Centers for Disease Control and Prevention as 2070 visual acuity or worse with correction in the better eye
growth and development developmental-behavioral screening measures
450 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
algorithms (8) When a psychometrically sound screen rai-ses concerns the algorithm emphasizes system-widereferral care coordination and a secondary screening orassessment which in a primary care setting is best ac-complished with the help of an EIECSE agency andan early return (pound1 month) office visit
In this algorithm pediatric clinicians are encouragedto refer automatically when their clinical impressionconfidently detects a developmental delay or if the childpossesses a biological or environmental condition associatedwith a sufficiently high probability of a delay developmental-behavioral promotion has been formally incorporated as acomponent of surveillance to make the process safer more
effective and parent-centered plusgreater detail has been providedabout the decisions and actionsteps that should reliably occur af-ter a screening test is administered(ie postscreening surveillance) (8)
ldquoStructured surveillancerdquo meansthat the process and decision-makingare enhanced with periodic screeningby using evidence-based measures(8) ldquoUnstructured surveillancerdquomeans that the process and decision-making are reliant on subjective im-pressions or casual observations (8)In a systematic review a pediatricclinicianrsquos unstructured surveillancewhen compared with a validatedscreening tool or a diagnostic inter-view has good specificity (the propor-tion of children correctly identifiedas not having a developmental-behavioral problem) ranging from69 to 100 but poor sensitivity(the proportion of children correctlyidentified as having a developmental-behavioral problem) ranging from14 to 54 (9)
When pediatric health-care pro-viders detect a problem they usuallyare correct however they struggleto identify the majority of delaysmost likely because they over-relyon psychometrically unsound mile-stone checklists with vague referralcriteria (1)(2)(8) As a result thelarge majority of children who haveevolving developmental-behavioralproblems can be deprived of the ben-
efits of EI ECSE or other evidence-based communityservices before kindergarten entrance
Periodic screening (ie structured surveillance) has beenproven repeatedly to enhance a clinicianrsquos ability todetect refer and monitor children who have evolvingdevelopmental-behavioral problems (1)(2)(3)(4)(5)(8)
Limitations of Screening in Primary CareAlthough standardized screening improves the quality ofcare at health supervision visits increases parental satisfac-tion leads to substantial cost savings for society and pos-itively affects the lives of children and families via the
Figure 1 Broad-band (general) developmental parent-report screening measures Corestandards are highlighted in yellow See text to explain shading and see Table 3 forabbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 451
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
benefits of EI and ECSE clinicians should be aware thatscreening has its limitations No single instrument willsuffice to identify every developmental-behavioral prob-lem and match the needs of every population or practicesetting The population screened and the method of im-plementation affect the psychometric properties ofa screening measure Screens can be falsely negative(ie they can yield negative or borderline results butthe child could be promptly deemed eligible for EIECSE services) or falsely positive (ie the screening testis positive or concerning but the child is subsequentlydeemed EIECSE ineligible) However a clinicianrsquos
longitudinal surveillance can beused to better interpret the typicalor borderline results of a screeningtest
For example when a pediatri-cian confidently suspects a delayand simultaneously a screen suchas the Ages and Stages Question-naire (ASQ) is found to be typicalor borderline 92 of pediatrician-referred children (blind to ASQ re-sults) promptly receive some formof EI services (40 are found to beEI-eligible 52 are placed on anEI-monitoring list) (1) Howeverthere is no evidence to support theconcept that unstructured surveil-lance should be used to overridethe concerning results of a psycho-metrically sound screen and negatethe need for a community-basedreferral (8) Children who failscreening tests and subsequentlyare not promptly found to have adevelopmental-behavioral diagno-sis (false-positives) nonethelesstend to have numerous psychoso-cial risk factors and exhibit perfor-mance well below average in thebetter predictors of school suc-cess pre-academics languageand intelligence (7) Indeed chil-dren found to have false-positivescreening results are a high-riskgroup in need of closer monitoringrepeat screenings at subsequentvisits and other community re-sources (eg evidence-based par-enting programs nurse home visit
programs high-quality child care structured preschoolssuch as Head Start)
Evaluating Specific Characteristics ofScreening MeasuresAlthough experts agree that no single screening instrumentwill suffice to identify every developmental-behavioralproblem in every practice setting it is also true thatall screening tools are not constructed equal In 2008Drotar et al (10) provided guidelines to help pediatri-cians select which screening tools were best-suited totheir practices based on their populationrsquos risk level
Figure 2 Narrow-band parent-report social-emotional (SE) communication amp autism-specific screens Data not included for the M-CHAT Follow-up Interview (FI) which isrecommended for any failed M-CHAT Core standards are highlighted in yellow See textto explain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
452 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
For general developmental parent-report tools Drotaret al recommended the ASQ and Parentsrsquo Evaluation ofDevelopmental Status (PEDS) for general primary carepopulations and the ASQ specifically for high-risk popula-tions For ASD-specific screening tools the ModifiedChecklist for Autism in Toddlers (M-CHAT) was recom-mended for general primary care populations For furtherdetails and recommendations refer to httpwwwcmwforgContentPublicationsFund-Manuals2008FebPediatric-Developmental-ScreeningndashUnderstanding-and-Selecting-Screening-Instrumentsaspx
Since 2008 new tools have been developed (eg Pa-rentsrsquo Evaluation of Developmental StatusndashDevelopmental
Milestones [PEDSDM] Quantita-tive Checklist for Autism in Tod-dlers) and others have undergonerevisions (eg Ages amp Stages Ques-tionnaire Third Edition [ASQ-3])In 2009 an AAP periodic surveyin concert with the screening toolselection trends in national andstatewide implementation initiativescollectively suggested that the ASQPEDS and M-CHAT have emergedas the three most commonly selectedscreening instruments for childrenage 0 to 5 years in US primary caresettings (6)
For broad-band developmentalscreening tools from 2002 to2009 pediatriciansrsquo use of the ASQincreased from 73 to 224 anduse of the PEDS increased from24 to 159 (6) In 2011 a well-designed study indicated that theASQ (second edition) was signifi-cantly more accurate than the PEDSespecially for children over age 30months in the identification of de-velopmental delays in a primary caresetting (11) The strengths of theASQ include its accuracy (both over-all and across all age ranges) and itsability to be used as a developmentalpromotion tool When caregiversmark ldquonot yetrdquo to an item becausethey have never tried that particulardevelopmental task with their childthis is considered a ldquoteachable mo-mentrdquo where clinicians can promotea new developmental activity
Although multiple primary care studies suggest thatthe paper-based ASQ is feasible it does require gettingall items on the correct age-interval ASQ thoughtfullycompleted by caregivers (and then correctly scored) beforethe health supervision visit In contrast the strength ofthe PEDS is its feasibility as a previsit screen with its 2- to5-minute administration time fourth- to fifth-grade read-ing level and single questionnaire format for all ages
Interestingly the PEDS has been designed to detecta broader array of ldquoat-riskrdquo (not just ldquodelayedrdquo) childrenand can be used not only as a screening and surveillancemeasure but also as a scaffold to enhance parentndashprovidercommunication Compared with the ASQ a higher
Figure 3 Mental healthbehavior screening amp assessment measures (used mostly inschool age children) Commonly used ADHD tools were included per the editorrsquos requesthowever an exhaustive list of depression- anxiety- and substance abuse-specificscreening tools was not included Core standards are highlighted in yellow See text toexplain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 453
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
percentage of children who have concerning or positivescreens on the PEDS which casts a ldquobroad netrdquo willbe found ineligible for EIECSE services and a higherpercentage of children who have delays will be missed be-cause of a negative screening result (although this findingvaries by age)
Of note the accuracy and feasibility of the ASQ andPEDS theoretically improve with online modalities that au-tomatically correct for prematurity foster a more thought-ful at-homeprevisit implementation approach and scoreresults without interference from human error Also withits online modality the PEDS can be used in combinationwith the PEDSDM
For autism-specific screening tools research now indi-cates that the M-CHAT follow-up interview should be
administered routinely for any pos-itive or borderline M-CHAT resultdue to a high false-positive rate(w90 are not subsequently diag-nosed as having ASD) when usingthe M-CHAT at 18 and 24 monthsin a general primary care popula-tion (8)
The strength of the M-CHAT isits feasibility and that it is far less likelyto miss a case of autism comparedwith a clinicianrsquos unstructured surveil-lance (8) Any positive M-CHAT re-sult should lead to an EIECSEagency referral and ideally an earlyreturn office visit for further as-sessment Unfortunately a positiveM-CHATdoes not necessarily justifyan expensive comprehensive ASD-specific evaluation and EI plan in allcases Children who screen positiveon the M-CHAT plus Follow-up In-terview should be referred for anASD-specific EI plan and compre-hensive evaluation Although somechildren will not be diagnosed as hav-ing ASD ultimately over-referralsare not a major concern becausethose not diagnosed as having ASDgenerally have other developmentaldisorders predominantly languageimpairment or cognitive disabilities
Of note unstructured surveillance(eg caregiver concerns about ASDworrisome social-communicationdeficits or behavioral observations
or having a sibling who has ASD) still should be usedin combination with the interpretation of a screening tool(eg a number of ldquocriticalrdquo M-CHAT items failed) to de-termine the need for an ASD-specific comprehensive eval-uation and EI plan without need for the follow-upinterview
To develop a deeper understanding about thestrengths and weaknesses of various screening tools anunderstanding is needed about the basic precepts behindpsychometric and feasibility standards Core standards af-fect a screening toolrsquos application to a primary care setting(eg performance on a wide variety of populations screen-ing tool completion rates sustainability over time) Thequestion arises what is a core standard Throughout thisarticle a core standard is defined as an inflexible property
Figure 4 Broad-band (general) developmental practitioner-administered screening andassessment measures Core standards are highlighted in yellow See text to explainshading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
454 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

Practitioner-administered screens (Fig 4) which di-rectly elicit or make observations about the childrsquos skillsand behavior generally measure another component ofsurveillance making accurate and informed observa-tions about the child and parentndashchild interactionsScreens may be broad-band (general) (Figs 1 and 4)meaning they tap all or most developmental-behavioral do-mains (expressive speech and language receptive languagegross motor fine motor cognitiveproblem-solving self-help and adaptive skills social-emotionalbehavior) ornarrow-band (Fig 2) meaning domain- disorder- or dis-ability-specific Narrow-band screens may partially tap oneor more domains but are not designed to assess the widespectrum of development-behavioral conditions at variousages (Table 2) and therefore ideally should always beused in conjunction with a broad-band screen
Current RecommendationsThe American Academy of Pediatrics (AAP) currently rec-ommends universal postpartum mood disorder screeningin the first year after birth general developmental screen-ing at 9 18 and 30 (or 24) months autism-specificscreening at 18 and 24months social-emotional screening
whenever a general or autism-specific instrument is abnor-mal ldquokindergarten readinessrdquo screening at 4 years social-emotionalmental healthpsychosocial function screeningat every health supervision visit from ages 5 to 18 yearsand substance abusendashspecific screening at every healthsupervision visit throughout adolescence
In addition according to the AAP an appropriatescreen should be administered whenever a clinicianrsquos sur-veillance determines ldquoriskrdquo All of these screening recom-mendations have heightened the need for clinicians toimplement office-based and community-based systemsthat are simultaneously effective and efficient especiallyfor those for whom research suggests interventions aremost effective the 257 million children in the UnitedStates who are age lt5 years (projected population in2012 per httpwwwchildstatsgov)
Incorporating Periodic Screening Into OngoingSurveillanceFigure 5 provides a collaborative model for screening andsurveillance in a medical home setting and is a combina-tion of the 2006 developmental 2007 autism spec-trum disorders (ASDs) and 2010 mental health AAP
Table 2 Prevalence of Developmental-Behavioral Conditions in Childrena
Any developmental disability 150 (3ndash17 y in 2006ndash2008)Condition Prevalence ( most studies conducted in the United States)Common conditions (Dagger1)1 Social-emotionalbehavioral disorders bull 21 (children and adolescents who meet criteria for a mental
health disorder with at least minimal impairment in 1999)bull 95ndash142 (ldquoserious emotional disturbancerdquo 0ndash5 y in2006)
2 Speech and language impairment bull 135 (expressive speech delays 18ndash23 mo in 1996ndash2000)bull 175 (expressive speech delays 30ndash36 mo in 1996ndash2000)bull 74 (language impairment kindergarten in 1997)
3 Attention-deficithyperactivity disorder bull 76 (3ndash17 y in 2006ndash2008)bull 41 (4ndash8 y in 2006ndash2008)
4 Learning disability bull 72 (3ndash17 y in 2006ndash2008)5 Developmental coordination disorder bull 6 (5ndash11 y in 2000) 17 (7ndash8 y in 2009)6 Intellectual disabilitymental retardation bull 12 (3ndash10 y in 1991)
bull 067 (3ndash17 y in 2006ndash2008)7 ASDs bull 066 (8 y and 3ndash10 y in 1998)
bull 11b (3ndash17 y in 2006ndash2008)Less common conditions (lt 1)8 Cerebral palsy bull 024 (3ndash10 y in 1991)9 Hearing impairmentc bull 038 (3ndash17 y in 2006ndash2008)10 Vision impairmentd bull 013 (3ndash17 y in 2006ndash2008)
ASDfrac14autism spectrum disorderaPlease note that all of these developmental-behavioral conditions have high rates of comorbiditybIn 2007 the ASD point prevalence was 110 per 10000 (11) Diagnosis of ASD was defined by 1) a physician or other health-care provider who said thatthe child had ASD and 2) that the child currently had the condition Nearly 40 of those ever diagnosed with ASD did not currently have the condition at thetime of a random-digit-dial telephone National Survey of Childrenrsquos Health (sample size frac14 78037)cDefined by the Centers for Disease Control and Prevention as moderate hearing loss (40 dB) or worse unaided in the better eardDefined by the Centers for Disease Control and Prevention as 2070 visual acuity or worse with correction in the better eye
growth and development developmental-behavioral screening measures
450 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
algorithms (8) When a psychometrically sound screen rai-ses concerns the algorithm emphasizes system-widereferral care coordination and a secondary screening orassessment which in a primary care setting is best ac-complished with the help of an EIECSE agency andan early return (pound1 month) office visit
In this algorithm pediatric clinicians are encouragedto refer automatically when their clinical impressionconfidently detects a developmental delay or if the childpossesses a biological or environmental condition associatedwith a sufficiently high probability of a delay developmental-behavioral promotion has been formally incorporated as acomponent of surveillance to make the process safer more
effective and parent-centered plusgreater detail has been providedabout the decisions and actionsteps that should reliably occur af-ter a screening test is administered(ie postscreening surveillance) (8)
ldquoStructured surveillancerdquo meansthat the process and decision-makingare enhanced with periodic screeningby using evidence-based measures(8) ldquoUnstructured surveillancerdquomeans that the process and decision-making are reliant on subjective im-pressions or casual observations (8)In a systematic review a pediatricclinicianrsquos unstructured surveillancewhen compared with a validatedscreening tool or a diagnostic inter-view has good specificity (the propor-tion of children correctly identifiedas not having a developmental-behavioral problem) ranging from69 to 100 but poor sensitivity(the proportion of children correctlyidentified as having a developmental-behavioral problem) ranging from14 to 54 (9)
When pediatric health-care pro-viders detect a problem they usuallyare correct however they struggleto identify the majority of delaysmost likely because they over-relyon psychometrically unsound mile-stone checklists with vague referralcriteria (1)(2)(8) As a result thelarge majority of children who haveevolving developmental-behavioralproblems can be deprived of the ben-
efits of EI ECSE or other evidence-based communityservices before kindergarten entrance
Periodic screening (ie structured surveillance) has beenproven repeatedly to enhance a clinicianrsquos ability todetect refer and monitor children who have evolvingdevelopmental-behavioral problems (1)(2)(3)(4)(5)(8)
Limitations of Screening in Primary CareAlthough standardized screening improves the quality ofcare at health supervision visits increases parental satisfac-tion leads to substantial cost savings for society and pos-itively affects the lives of children and families via the
Figure 1 Broad-band (general) developmental parent-report screening measures Corestandards are highlighted in yellow See text to explain shading and see Table 3 forabbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 451
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
benefits of EI and ECSE clinicians should be aware thatscreening has its limitations No single instrument willsuffice to identify every developmental-behavioral prob-lem and match the needs of every population or practicesetting The population screened and the method of im-plementation affect the psychometric properties ofa screening measure Screens can be falsely negative(ie they can yield negative or borderline results butthe child could be promptly deemed eligible for EIECSE services) or falsely positive (ie the screening testis positive or concerning but the child is subsequentlydeemed EIECSE ineligible) However a clinicianrsquos
longitudinal surveillance can beused to better interpret the typicalor borderline results of a screeningtest
For example when a pediatri-cian confidently suspects a delayand simultaneously a screen suchas the Ages and Stages Question-naire (ASQ) is found to be typicalor borderline 92 of pediatrician-referred children (blind to ASQ re-sults) promptly receive some formof EI services (40 are found to beEI-eligible 52 are placed on anEI-monitoring list) (1) Howeverthere is no evidence to support theconcept that unstructured surveil-lance should be used to overridethe concerning results of a psycho-metrically sound screen and negatethe need for a community-basedreferral (8) Children who failscreening tests and subsequentlyare not promptly found to have adevelopmental-behavioral diagno-sis (false-positives) nonethelesstend to have numerous psychoso-cial risk factors and exhibit perfor-mance well below average in thebetter predictors of school suc-cess pre-academics languageand intelligence (7) Indeed chil-dren found to have false-positivescreening results are a high-riskgroup in need of closer monitoringrepeat screenings at subsequentvisits and other community re-sources (eg evidence-based par-enting programs nurse home visit
programs high-quality child care structured preschoolssuch as Head Start)
Evaluating Specific Characteristics ofScreening MeasuresAlthough experts agree that no single screening instrumentwill suffice to identify every developmental-behavioralproblem in every practice setting it is also true thatall screening tools are not constructed equal In 2008Drotar et al (10) provided guidelines to help pediatri-cians select which screening tools were best-suited totheir practices based on their populationrsquos risk level
Figure 2 Narrow-band parent-report social-emotional (SE) communication amp autism-specific screens Data not included for the M-CHAT Follow-up Interview (FI) which isrecommended for any failed M-CHAT Core standards are highlighted in yellow See textto explain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
452 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
For general developmental parent-report tools Drotaret al recommended the ASQ and Parentsrsquo Evaluation ofDevelopmental Status (PEDS) for general primary carepopulations and the ASQ specifically for high-risk popula-tions For ASD-specific screening tools the ModifiedChecklist for Autism in Toddlers (M-CHAT) was recom-mended for general primary care populations For furtherdetails and recommendations refer to httpwwwcmwforgContentPublicationsFund-Manuals2008FebPediatric-Developmental-ScreeningndashUnderstanding-and-Selecting-Screening-Instrumentsaspx
Since 2008 new tools have been developed (eg Pa-rentsrsquo Evaluation of Developmental StatusndashDevelopmental
Milestones [PEDSDM] Quantita-tive Checklist for Autism in Tod-dlers) and others have undergonerevisions (eg Ages amp Stages Ques-tionnaire Third Edition [ASQ-3])In 2009 an AAP periodic surveyin concert with the screening toolselection trends in national andstatewide implementation initiativescollectively suggested that the ASQPEDS and M-CHAT have emergedas the three most commonly selectedscreening instruments for childrenage 0 to 5 years in US primary caresettings (6)
For broad-band developmentalscreening tools from 2002 to2009 pediatriciansrsquo use of the ASQincreased from 73 to 224 anduse of the PEDS increased from24 to 159 (6) In 2011 a well-designed study indicated that theASQ (second edition) was signifi-cantly more accurate than the PEDSespecially for children over age 30months in the identification of de-velopmental delays in a primary caresetting (11) The strengths of theASQ include its accuracy (both over-all and across all age ranges) and itsability to be used as a developmentalpromotion tool When caregiversmark ldquonot yetrdquo to an item becausethey have never tried that particulardevelopmental task with their childthis is considered a ldquoteachable mo-mentrdquo where clinicians can promotea new developmental activity
Although multiple primary care studies suggest thatthe paper-based ASQ is feasible it does require gettingall items on the correct age-interval ASQ thoughtfullycompleted by caregivers (and then correctly scored) beforethe health supervision visit In contrast the strength ofthe PEDS is its feasibility as a previsit screen with its 2- to5-minute administration time fourth- to fifth-grade read-ing level and single questionnaire format for all ages
Interestingly the PEDS has been designed to detecta broader array of ldquoat-riskrdquo (not just ldquodelayedrdquo) childrenand can be used not only as a screening and surveillancemeasure but also as a scaffold to enhance parentndashprovidercommunication Compared with the ASQ a higher
Figure 3 Mental healthbehavior screening amp assessment measures (used mostly inschool age children) Commonly used ADHD tools were included per the editorrsquos requesthowever an exhaustive list of depression- anxiety- and substance abuse-specificscreening tools was not included Core standards are highlighted in yellow See text toexplain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 453
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
percentage of children who have concerning or positivescreens on the PEDS which casts a ldquobroad netrdquo willbe found ineligible for EIECSE services and a higherpercentage of children who have delays will be missed be-cause of a negative screening result (although this findingvaries by age)
Of note the accuracy and feasibility of the ASQ andPEDS theoretically improve with online modalities that au-tomatically correct for prematurity foster a more thought-ful at-homeprevisit implementation approach and scoreresults without interference from human error Also withits online modality the PEDS can be used in combinationwith the PEDSDM
For autism-specific screening tools research now indi-cates that the M-CHAT follow-up interview should be
administered routinely for any pos-itive or borderline M-CHAT resultdue to a high false-positive rate(w90 are not subsequently diag-nosed as having ASD) when usingthe M-CHAT at 18 and 24 monthsin a general primary care popula-tion (8)
The strength of the M-CHAT isits feasibility and that it is far less likelyto miss a case of autism comparedwith a clinicianrsquos unstructured surveil-lance (8) Any positive M-CHAT re-sult should lead to an EIECSEagency referral and ideally an earlyreturn office visit for further as-sessment Unfortunately a positiveM-CHATdoes not necessarily justifyan expensive comprehensive ASD-specific evaluation and EI plan in allcases Children who screen positiveon the M-CHAT plus Follow-up In-terview should be referred for anASD-specific EI plan and compre-hensive evaluation Although somechildren will not be diagnosed as hav-ing ASD ultimately over-referralsare not a major concern becausethose not diagnosed as having ASDgenerally have other developmentaldisorders predominantly languageimpairment or cognitive disabilities
Of note unstructured surveillance(eg caregiver concerns about ASDworrisome social-communicationdeficits or behavioral observations
or having a sibling who has ASD) still should be usedin combination with the interpretation of a screening tool(eg a number of ldquocriticalrdquo M-CHAT items failed) to de-termine the need for an ASD-specific comprehensive eval-uation and EI plan without need for the follow-upinterview
To develop a deeper understanding about thestrengths and weaknesses of various screening tools anunderstanding is needed about the basic precepts behindpsychometric and feasibility standards Core standards af-fect a screening toolrsquos application to a primary care setting(eg performance on a wide variety of populations screen-ing tool completion rates sustainability over time) Thequestion arises what is a core standard Throughout thisarticle a core standard is defined as an inflexible property
Figure 4 Broad-band (general) developmental practitioner-administered screening andassessment measures Core standards are highlighted in yellow See text to explainshading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
454 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

algorithms (8) When a psychometrically sound screen rai-ses concerns the algorithm emphasizes system-widereferral care coordination and a secondary screening orassessment which in a primary care setting is best ac-complished with the help of an EIECSE agency andan early return (pound1 month) office visit
In this algorithm pediatric clinicians are encouragedto refer automatically when their clinical impressionconfidently detects a developmental delay or if the childpossesses a biological or environmental condition associatedwith a sufficiently high probability of a delay developmental-behavioral promotion has been formally incorporated as acomponent of surveillance to make the process safer more
effective and parent-centered plusgreater detail has been providedabout the decisions and actionsteps that should reliably occur af-ter a screening test is administered(ie postscreening surveillance) (8)
ldquoStructured surveillancerdquo meansthat the process and decision-makingare enhanced with periodic screeningby using evidence-based measures(8) ldquoUnstructured surveillancerdquomeans that the process and decision-making are reliant on subjective im-pressions or casual observations (8)In a systematic review a pediatricclinicianrsquos unstructured surveillancewhen compared with a validatedscreening tool or a diagnostic inter-view has good specificity (the propor-tion of children correctly identifiedas not having a developmental-behavioral problem) ranging from69 to 100 but poor sensitivity(the proportion of children correctlyidentified as having a developmental-behavioral problem) ranging from14 to 54 (9)
When pediatric health-care pro-viders detect a problem they usuallyare correct however they struggleto identify the majority of delaysmost likely because they over-relyon psychometrically unsound mile-stone checklists with vague referralcriteria (1)(2)(8) As a result thelarge majority of children who haveevolving developmental-behavioralproblems can be deprived of the ben-
efits of EI ECSE or other evidence-based communityservices before kindergarten entrance
Periodic screening (ie structured surveillance) has beenproven repeatedly to enhance a clinicianrsquos ability todetect refer and monitor children who have evolvingdevelopmental-behavioral problems (1)(2)(3)(4)(5)(8)
Limitations of Screening in Primary CareAlthough standardized screening improves the quality ofcare at health supervision visits increases parental satisfac-tion leads to substantial cost savings for society and pos-itively affects the lives of children and families via the
Figure 1 Broad-band (general) developmental parent-report screening measures Corestandards are highlighted in yellow See text to explain shading and see Table 3 forabbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 451
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
benefits of EI and ECSE clinicians should be aware thatscreening has its limitations No single instrument willsuffice to identify every developmental-behavioral prob-lem and match the needs of every population or practicesetting The population screened and the method of im-plementation affect the psychometric properties ofa screening measure Screens can be falsely negative(ie they can yield negative or borderline results butthe child could be promptly deemed eligible for EIECSE services) or falsely positive (ie the screening testis positive or concerning but the child is subsequentlydeemed EIECSE ineligible) However a clinicianrsquos
longitudinal surveillance can beused to better interpret the typicalor borderline results of a screeningtest
For example when a pediatri-cian confidently suspects a delayand simultaneously a screen suchas the Ages and Stages Question-naire (ASQ) is found to be typicalor borderline 92 of pediatrician-referred children (blind to ASQ re-sults) promptly receive some formof EI services (40 are found to beEI-eligible 52 are placed on anEI-monitoring list) (1) Howeverthere is no evidence to support theconcept that unstructured surveil-lance should be used to overridethe concerning results of a psycho-metrically sound screen and negatethe need for a community-basedreferral (8) Children who failscreening tests and subsequentlyare not promptly found to have adevelopmental-behavioral diagno-sis (false-positives) nonethelesstend to have numerous psychoso-cial risk factors and exhibit perfor-mance well below average in thebetter predictors of school suc-cess pre-academics languageand intelligence (7) Indeed chil-dren found to have false-positivescreening results are a high-riskgroup in need of closer monitoringrepeat screenings at subsequentvisits and other community re-sources (eg evidence-based par-enting programs nurse home visit
programs high-quality child care structured preschoolssuch as Head Start)
Evaluating Specific Characteristics ofScreening MeasuresAlthough experts agree that no single screening instrumentwill suffice to identify every developmental-behavioralproblem in every practice setting it is also true thatall screening tools are not constructed equal In 2008Drotar et al (10) provided guidelines to help pediatri-cians select which screening tools were best-suited totheir practices based on their populationrsquos risk level
Figure 2 Narrow-band parent-report social-emotional (SE) communication amp autism-specific screens Data not included for the M-CHAT Follow-up Interview (FI) which isrecommended for any failed M-CHAT Core standards are highlighted in yellow See textto explain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
452 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
For general developmental parent-report tools Drotaret al recommended the ASQ and Parentsrsquo Evaluation ofDevelopmental Status (PEDS) for general primary carepopulations and the ASQ specifically for high-risk popula-tions For ASD-specific screening tools the ModifiedChecklist for Autism in Toddlers (M-CHAT) was recom-mended for general primary care populations For furtherdetails and recommendations refer to httpwwwcmwforgContentPublicationsFund-Manuals2008FebPediatric-Developmental-ScreeningndashUnderstanding-and-Selecting-Screening-Instrumentsaspx
Since 2008 new tools have been developed (eg Pa-rentsrsquo Evaluation of Developmental StatusndashDevelopmental
Milestones [PEDSDM] Quantita-tive Checklist for Autism in Tod-dlers) and others have undergonerevisions (eg Ages amp Stages Ques-tionnaire Third Edition [ASQ-3])In 2009 an AAP periodic surveyin concert with the screening toolselection trends in national andstatewide implementation initiativescollectively suggested that the ASQPEDS and M-CHAT have emergedas the three most commonly selectedscreening instruments for childrenage 0 to 5 years in US primary caresettings (6)
For broad-band developmentalscreening tools from 2002 to2009 pediatriciansrsquo use of the ASQincreased from 73 to 224 anduse of the PEDS increased from24 to 159 (6) In 2011 a well-designed study indicated that theASQ (second edition) was signifi-cantly more accurate than the PEDSespecially for children over age 30months in the identification of de-velopmental delays in a primary caresetting (11) The strengths of theASQ include its accuracy (both over-all and across all age ranges) and itsability to be used as a developmentalpromotion tool When caregiversmark ldquonot yetrdquo to an item becausethey have never tried that particulardevelopmental task with their childthis is considered a ldquoteachable mo-mentrdquo where clinicians can promotea new developmental activity
Although multiple primary care studies suggest thatthe paper-based ASQ is feasible it does require gettingall items on the correct age-interval ASQ thoughtfullycompleted by caregivers (and then correctly scored) beforethe health supervision visit In contrast the strength ofthe PEDS is its feasibility as a previsit screen with its 2- to5-minute administration time fourth- to fifth-grade read-ing level and single questionnaire format for all ages
Interestingly the PEDS has been designed to detecta broader array of ldquoat-riskrdquo (not just ldquodelayedrdquo) childrenand can be used not only as a screening and surveillancemeasure but also as a scaffold to enhance parentndashprovidercommunication Compared with the ASQ a higher
Figure 3 Mental healthbehavior screening amp assessment measures (used mostly inschool age children) Commonly used ADHD tools were included per the editorrsquos requesthowever an exhaustive list of depression- anxiety- and substance abuse-specificscreening tools was not included Core standards are highlighted in yellow See text toexplain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 453
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
percentage of children who have concerning or positivescreens on the PEDS which casts a ldquobroad netrdquo willbe found ineligible for EIECSE services and a higherpercentage of children who have delays will be missed be-cause of a negative screening result (although this findingvaries by age)
Of note the accuracy and feasibility of the ASQ andPEDS theoretically improve with online modalities that au-tomatically correct for prematurity foster a more thought-ful at-homeprevisit implementation approach and scoreresults without interference from human error Also withits online modality the PEDS can be used in combinationwith the PEDSDM
For autism-specific screening tools research now indi-cates that the M-CHAT follow-up interview should be
administered routinely for any pos-itive or borderline M-CHAT resultdue to a high false-positive rate(w90 are not subsequently diag-nosed as having ASD) when usingthe M-CHAT at 18 and 24 monthsin a general primary care popula-tion (8)
The strength of the M-CHAT isits feasibility and that it is far less likelyto miss a case of autism comparedwith a clinicianrsquos unstructured surveil-lance (8) Any positive M-CHAT re-sult should lead to an EIECSEagency referral and ideally an earlyreturn office visit for further as-sessment Unfortunately a positiveM-CHATdoes not necessarily justifyan expensive comprehensive ASD-specific evaluation and EI plan in allcases Children who screen positiveon the M-CHAT plus Follow-up In-terview should be referred for anASD-specific EI plan and compre-hensive evaluation Although somechildren will not be diagnosed as hav-ing ASD ultimately over-referralsare not a major concern becausethose not diagnosed as having ASDgenerally have other developmentaldisorders predominantly languageimpairment or cognitive disabilities
Of note unstructured surveillance(eg caregiver concerns about ASDworrisome social-communicationdeficits or behavioral observations
or having a sibling who has ASD) still should be usedin combination with the interpretation of a screening tool(eg a number of ldquocriticalrdquo M-CHAT items failed) to de-termine the need for an ASD-specific comprehensive eval-uation and EI plan without need for the follow-upinterview
To develop a deeper understanding about thestrengths and weaknesses of various screening tools anunderstanding is needed about the basic precepts behindpsychometric and feasibility standards Core standards af-fect a screening toolrsquos application to a primary care setting(eg performance on a wide variety of populations screen-ing tool completion rates sustainability over time) Thequestion arises what is a core standard Throughout thisarticle a core standard is defined as an inflexible property
Figure 4 Broad-band (general) developmental practitioner-administered screening andassessment measures Core standards are highlighted in yellow See text to explainshading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
454 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

benefits of EI and ECSE clinicians should be aware thatscreening has its limitations No single instrument willsuffice to identify every developmental-behavioral prob-lem and match the needs of every population or practicesetting The population screened and the method of im-plementation affect the psychometric properties ofa screening measure Screens can be falsely negative(ie they can yield negative or borderline results butthe child could be promptly deemed eligible for EIECSE services) or falsely positive (ie the screening testis positive or concerning but the child is subsequentlydeemed EIECSE ineligible) However a clinicianrsquos
longitudinal surveillance can beused to better interpret the typicalor borderline results of a screeningtest
For example when a pediatri-cian confidently suspects a delayand simultaneously a screen suchas the Ages and Stages Question-naire (ASQ) is found to be typicalor borderline 92 of pediatrician-referred children (blind to ASQ re-sults) promptly receive some formof EI services (40 are found to beEI-eligible 52 are placed on anEI-monitoring list) (1) Howeverthere is no evidence to support theconcept that unstructured surveil-lance should be used to overridethe concerning results of a psycho-metrically sound screen and negatethe need for a community-basedreferral (8) Children who failscreening tests and subsequentlyare not promptly found to have adevelopmental-behavioral diagno-sis (false-positives) nonethelesstend to have numerous psychoso-cial risk factors and exhibit perfor-mance well below average in thebetter predictors of school suc-cess pre-academics languageand intelligence (7) Indeed chil-dren found to have false-positivescreening results are a high-riskgroup in need of closer monitoringrepeat screenings at subsequentvisits and other community re-sources (eg evidence-based par-enting programs nurse home visit
programs high-quality child care structured preschoolssuch as Head Start)
Evaluating Specific Characteristics ofScreening MeasuresAlthough experts agree that no single screening instrumentwill suffice to identify every developmental-behavioralproblem in every practice setting it is also true thatall screening tools are not constructed equal In 2008Drotar et al (10) provided guidelines to help pediatri-cians select which screening tools were best-suited totheir practices based on their populationrsquos risk level
Figure 2 Narrow-band parent-report social-emotional (SE) communication amp autism-specific screens Data not included for the M-CHAT Follow-up Interview (FI) which isrecommended for any failed M-CHAT Core standards are highlighted in yellow See textto explain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
452 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
For general developmental parent-report tools Drotaret al recommended the ASQ and Parentsrsquo Evaluation ofDevelopmental Status (PEDS) for general primary carepopulations and the ASQ specifically for high-risk popula-tions For ASD-specific screening tools the ModifiedChecklist for Autism in Toddlers (M-CHAT) was recom-mended for general primary care populations For furtherdetails and recommendations refer to httpwwwcmwforgContentPublicationsFund-Manuals2008FebPediatric-Developmental-ScreeningndashUnderstanding-and-Selecting-Screening-Instrumentsaspx
Since 2008 new tools have been developed (eg Pa-rentsrsquo Evaluation of Developmental StatusndashDevelopmental
Milestones [PEDSDM] Quantita-tive Checklist for Autism in Tod-dlers) and others have undergonerevisions (eg Ages amp Stages Ques-tionnaire Third Edition [ASQ-3])In 2009 an AAP periodic surveyin concert with the screening toolselection trends in national andstatewide implementation initiativescollectively suggested that the ASQPEDS and M-CHAT have emergedas the three most commonly selectedscreening instruments for childrenage 0 to 5 years in US primary caresettings (6)
For broad-band developmentalscreening tools from 2002 to2009 pediatriciansrsquo use of the ASQincreased from 73 to 224 anduse of the PEDS increased from24 to 159 (6) In 2011 a well-designed study indicated that theASQ (second edition) was signifi-cantly more accurate than the PEDSespecially for children over age 30months in the identification of de-velopmental delays in a primary caresetting (11) The strengths of theASQ include its accuracy (both over-all and across all age ranges) and itsability to be used as a developmentalpromotion tool When caregiversmark ldquonot yetrdquo to an item becausethey have never tried that particulardevelopmental task with their childthis is considered a ldquoteachable mo-mentrdquo where clinicians can promotea new developmental activity
Although multiple primary care studies suggest thatthe paper-based ASQ is feasible it does require gettingall items on the correct age-interval ASQ thoughtfullycompleted by caregivers (and then correctly scored) beforethe health supervision visit In contrast the strength ofthe PEDS is its feasibility as a previsit screen with its 2- to5-minute administration time fourth- to fifth-grade read-ing level and single questionnaire format for all ages
Interestingly the PEDS has been designed to detecta broader array of ldquoat-riskrdquo (not just ldquodelayedrdquo) childrenand can be used not only as a screening and surveillancemeasure but also as a scaffold to enhance parentndashprovidercommunication Compared with the ASQ a higher
Figure 3 Mental healthbehavior screening amp assessment measures (used mostly inschool age children) Commonly used ADHD tools were included per the editorrsquos requesthowever an exhaustive list of depression- anxiety- and substance abuse-specificscreening tools was not included Core standards are highlighted in yellow See text toexplain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 453
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
percentage of children who have concerning or positivescreens on the PEDS which casts a ldquobroad netrdquo willbe found ineligible for EIECSE services and a higherpercentage of children who have delays will be missed be-cause of a negative screening result (although this findingvaries by age)
Of note the accuracy and feasibility of the ASQ andPEDS theoretically improve with online modalities that au-tomatically correct for prematurity foster a more thought-ful at-homeprevisit implementation approach and scoreresults without interference from human error Also withits online modality the PEDS can be used in combinationwith the PEDSDM
For autism-specific screening tools research now indi-cates that the M-CHAT follow-up interview should be
administered routinely for any pos-itive or borderline M-CHAT resultdue to a high false-positive rate(w90 are not subsequently diag-nosed as having ASD) when usingthe M-CHAT at 18 and 24 monthsin a general primary care popula-tion (8)
The strength of the M-CHAT isits feasibility and that it is far less likelyto miss a case of autism comparedwith a clinicianrsquos unstructured surveil-lance (8) Any positive M-CHAT re-sult should lead to an EIECSEagency referral and ideally an earlyreturn office visit for further as-sessment Unfortunately a positiveM-CHATdoes not necessarily justifyan expensive comprehensive ASD-specific evaluation and EI plan in allcases Children who screen positiveon the M-CHAT plus Follow-up In-terview should be referred for anASD-specific EI plan and compre-hensive evaluation Although somechildren will not be diagnosed as hav-ing ASD ultimately over-referralsare not a major concern becausethose not diagnosed as having ASDgenerally have other developmentaldisorders predominantly languageimpairment or cognitive disabilities
Of note unstructured surveillance(eg caregiver concerns about ASDworrisome social-communicationdeficits or behavioral observations
or having a sibling who has ASD) still should be usedin combination with the interpretation of a screening tool(eg a number of ldquocriticalrdquo M-CHAT items failed) to de-termine the need for an ASD-specific comprehensive eval-uation and EI plan without need for the follow-upinterview
To develop a deeper understanding about thestrengths and weaknesses of various screening tools anunderstanding is needed about the basic precepts behindpsychometric and feasibility standards Core standards af-fect a screening toolrsquos application to a primary care setting(eg performance on a wide variety of populations screen-ing tool completion rates sustainability over time) Thequestion arises what is a core standard Throughout thisarticle a core standard is defined as an inflexible property
Figure 4 Broad-band (general) developmental practitioner-administered screening andassessment measures Core standards are highlighted in yellow See text to explainshading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
454 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
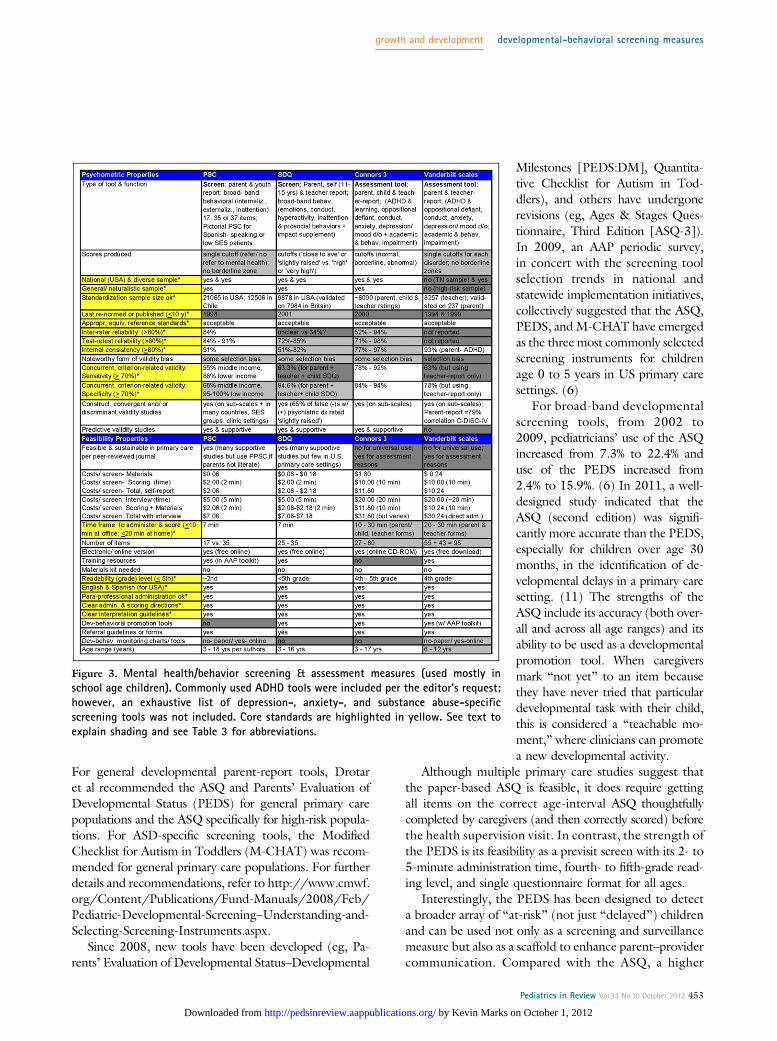
For general developmental parent-report tools Drotaret al recommended the ASQ and Parentsrsquo Evaluation ofDevelopmental Status (PEDS) for general primary carepopulations and the ASQ specifically for high-risk popula-tions For ASD-specific screening tools the ModifiedChecklist for Autism in Toddlers (M-CHAT) was recom-mended for general primary care populations For furtherdetails and recommendations refer to httpwwwcmwforgContentPublicationsFund-Manuals2008FebPediatric-Developmental-ScreeningndashUnderstanding-and-Selecting-Screening-Instrumentsaspx
Since 2008 new tools have been developed (eg Pa-rentsrsquo Evaluation of Developmental StatusndashDevelopmental
Milestones [PEDSDM] Quantita-tive Checklist for Autism in Tod-dlers) and others have undergonerevisions (eg Ages amp Stages Ques-tionnaire Third Edition [ASQ-3])In 2009 an AAP periodic surveyin concert with the screening toolselection trends in national andstatewide implementation initiativescollectively suggested that the ASQPEDS and M-CHAT have emergedas the three most commonly selectedscreening instruments for childrenage 0 to 5 years in US primary caresettings (6)
For broad-band developmentalscreening tools from 2002 to2009 pediatriciansrsquo use of the ASQincreased from 73 to 224 anduse of the PEDS increased from24 to 159 (6) In 2011 a well-designed study indicated that theASQ (second edition) was signifi-cantly more accurate than the PEDSespecially for children over age 30months in the identification of de-velopmental delays in a primary caresetting (11) The strengths of theASQ include its accuracy (both over-all and across all age ranges) and itsability to be used as a developmentalpromotion tool When caregiversmark ldquonot yetrdquo to an item becausethey have never tried that particulardevelopmental task with their childthis is considered a ldquoteachable mo-mentrdquo where clinicians can promotea new developmental activity
Although multiple primary care studies suggest thatthe paper-based ASQ is feasible it does require gettingall items on the correct age-interval ASQ thoughtfullycompleted by caregivers (and then correctly scored) beforethe health supervision visit In contrast the strength ofthe PEDS is its feasibility as a previsit screen with its 2- to5-minute administration time fourth- to fifth-grade read-ing level and single questionnaire format for all ages
Interestingly the PEDS has been designed to detecta broader array of ldquoat-riskrdquo (not just ldquodelayedrdquo) childrenand can be used not only as a screening and surveillancemeasure but also as a scaffold to enhance parentndashprovidercommunication Compared with the ASQ a higher
Figure 3 Mental healthbehavior screening amp assessment measures (used mostly inschool age children) Commonly used ADHD tools were included per the editorrsquos requesthowever an exhaustive list of depression- anxiety- and substance abuse-specificscreening tools was not included Core standards are highlighted in yellow See text toexplain shading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 453
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
percentage of children who have concerning or positivescreens on the PEDS which casts a ldquobroad netrdquo willbe found ineligible for EIECSE services and a higherpercentage of children who have delays will be missed be-cause of a negative screening result (although this findingvaries by age)
Of note the accuracy and feasibility of the ASQ andPEDS theoretically improve with online modalities that au-tomatically correct for prematurity foster a more thought-ful at-homeprevisit implementation approach and scoreresults without interference from human error Also withits online modality the PEDS can be used in combinationwith the PEDSDM
For autism-specific screening tools research now indi-cates that the M-CHAT follow-up interview should be
administered routinely for any pos-itive or borderline M-CHAT resultdue to a high false-positive rate(w90 are not subsequently diag-nosed as having ASD) when usingthe M-CHAT at 18 and 24 monthsin a general primary care popula-tion (8)
The strength of the M-CHAT isits feasibility and that it is far less likelyto miss a case of autism comparedwith a clinicianrsquos unstructured surveil-lance (8) Any positive M-CHAT re-sult should lead to an EIECSEagency referral and ideally an earlyreturn office visit for further as-sessment Unfortunately a positiveM-CHATdoes not necessarily justifyan expensive comprehensive ASD-specific evaluation and EI plan in allcases Children who screen positiveon the M-CHAT plus Follow-up In-terview should be referred for anASD-specific EI plan and compre-hensive evaluation Although somechildren will not be diagnosed as hav-ing ASD ultimately over-referralsare not a major concern becausethose not diagnosed as having ASDgenerally have other developmentaldisorders predominantly languageimpairment or cognitive disabilities
Of note unstructured surveillance(eg caregiver concerns about ASDworrisome social-communicationdeficits or behavioral observations
or having a sibling who has ASD) still should be usedin combination with the interpretation of a screening tool(eg a number of ldquocriticalrdquo M-CHAT items failed) to de-termine the need for an ASD-specific comprehensive eval-uation and EI plan without need for the follow-upinterview
To develop a deeper understanding about thestrengths and weaknesses of various screening tools anunderstanding is needed about the basic precepts behindpsychometric and feasibility standards Core standards af-fect a screening toolrsquos application to a primary care setting(eg performance on a wide variety of populations screen-ing tool completion rates sustainability over time) Thequestion arises what is a core standard Throughout thisarticle a core standard is defined as an inflexible property
Figure 4 Broad-band (general) developmental practitioner-administered screening andassessment measures Core standards are highlighted in yellow See text to explainshading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
454 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
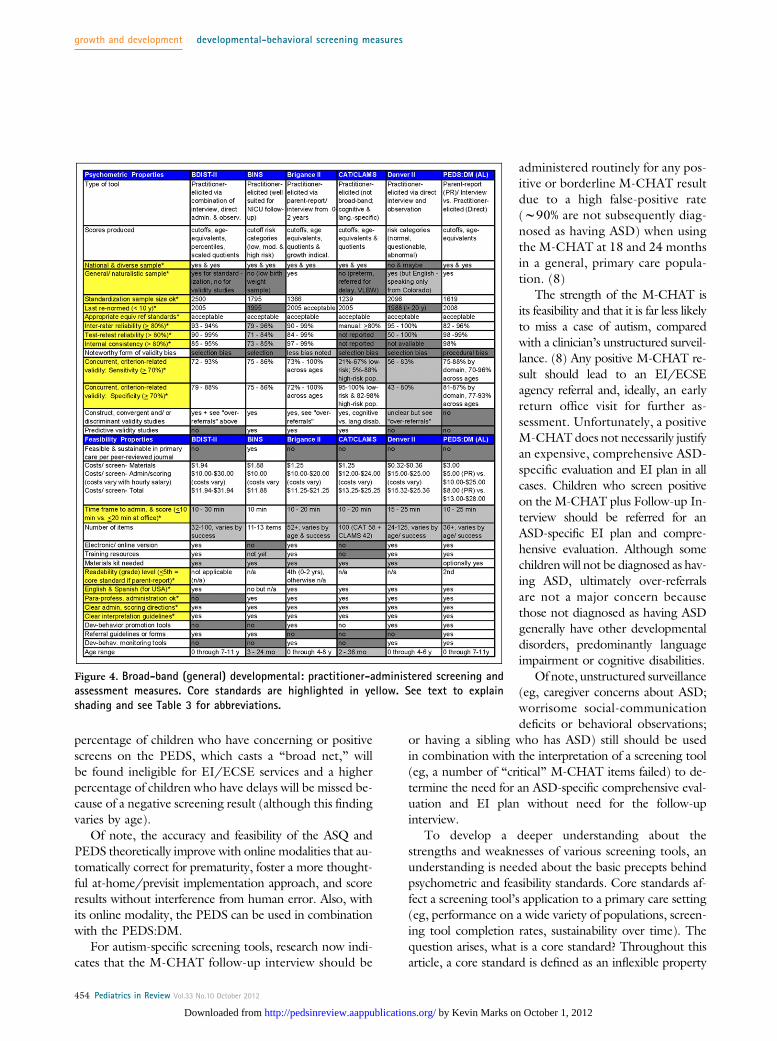
percentage of children who have concerning or positivescreens on the PEDS which casts a ldquobroad netrdquo willbe found ineligible for EIECSE services and a higherpercentage of children who have delays will be missed be-cause of a negative screening result (although this findingvaries by age)
Of note the accuracy and feasibility of the ASQ andPEDS theoretically improve with online modalities that au-tomatically correct for prematurity foster a more thought-ful at-homeprevisit implementation approach and scoreresults without interference from human error Also withits online modality the PEDS can be used in combinationwith the PEDSDM
For autism-specific screening tools research now indi-cates that the M-CHAT follow-up interview should be
administered routinely for any pos-itive or borderline M-CHAT resultdue to a high false-positive rate(w90 are not subsequently diag-nosed as having ASD) when usingthe M-CHAT at 18 and 24 monthsin a general primary care popula-tion (8)
The strength of the M-CHAT isits feasibility and that it is far less likelyto miss a case of autism comparedwith a clinicianrsquos unstructured surveil-lance (8) Any positive M-CHAT re-sult should lead to an EIECSEagency referral and ideally an earlyreturn office visit for further as-sessment Unfortunately a positiveM-CHATdoes not necessarily justifyan expensive comprehensive ASD-specific evaluation and EI plan in allcases Children who screen positiveon the M-CHAT plus Follow-up In-terview should be referred for anASD-specific EI plan and compre-hensive evaluation Although somechildren will not be diagnosed as hav-ing ASD ultimately over-referralsare not a major concern becausethose not diagnosed as having ASDgenerally have other developmentaldisorders predominantly languageimpairment or cognitive disabilities
Of note unstructured surveillance(eg caregiver concerns about ASDworrisome social-communicationdeficits or behavioral observations
or having a sibling who has ASD) still should be usedin combination with the interpretation of a screening tool(eg a number of ldquocriticalrdquo M-CHAT items failed) to de-termine the need for an ASD-specific comprehensive eval-uation and EI plan without need for the follow-upinterview
To develop a deeper understanding about thestrengths and weaknesses of various screening tools anunderstanding is needed about the basic precepts behindpsychometric and feasibility standards Core standards af-fect a screening toolrsquos application to a primary care setting(eg performance on a wide variety of populations screen-ing tool completion rates sustainability over time) Thequestion arises what is a core standard Throughout thisarticle a core standard is defined as an inflexible property
Figure 4 Broad-band (general) developmental practitioner-administered screening andassessment measures Core standards are highlighted in yellow See text to explainshading and see Table 3 for abbreviations
growth and development developmental-behavioral screening measures
454 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

that is critically important for the effective and feasible per-formance of a screening measure on a primary care popu-lation but is not necessarily dependent on the individualneeds of a medical home
Core standards provide a frame of reference to assurethat relevant technical information is provided with thehope that practitioners thereby will make wiser more
informed decisions when selectingimplementing and interpretingscreening tools To learn more aboutwhat technical properties make ascreening tool psychometricallysound go to httppedsinreviewaappublicationsorgcontent3310448supplDC1 and to learnwhat properties make a screening toolfeasible go to httppedsinreviewaappublicationsorgcontent3310448supplDC2
Application of Psychometricand Feasibility Standards toPrimary CareThe AAP strongly endorses the useof properly standardized reliable(Dagger80) well-validated and accurate(sensitivity and specificity Dagger70)screening instruments for the earlyidentification of developmental-be-havioral problems However highlyaccurate practitioner-administeredinstruments often possess undesir-able feasibility characteristics forbusy primary care settings Practi-tioners should look hard at howpractical any given instrument theyare considering will be in the officesetting Suboptimal feasibility lowersscreening tool completion ratesLower completion rates logicallyhinder early detection rates becauseearly detection is more apt to relyon subjective unstructured surveil-lance instead of psychometricallysound screens
For the early detection of a broadrange of developmental delays be-fore kindergarten entrance parent-report tools such as the ASQ-3PEDS and the PEDSDM are good
examples of effective and feasible screening tools that arewell-suited to a wide array of primary care settings how-ever the use of yesno checklists such as the DenverPrescreening Developmental Questionnaire II is notrecommended For the early detection of a broadrange of social-emotionalmental health problemsthe Ages amp Stages Questionnaire Social-Emotional for
Figure 5 Algorithm for developmental-behavioral surveillance and screening (0 to 5years) in a medical home setting Permission to print this adapted figure was obtainedfrom Sage Publishing Kevin Marks MD 2012
growth and development developmental-behavioral screening measures
Pediatrics in Review Vol33 No10 October 2012 455
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

children age 3 months to 5 years and the Pediatric Symp-tom Checklist (PSC) for children age 6 to 18 years aregood examples of effective and feasible tools
For autism-specific screening the M-CHAT is currentlya commonly selected tool However whenever theM-CHAT is positive (failed) it is important to administerits follow-up interview to filter out which children aretruly in need of an ASD-specific comprehensive evaluationand EI plan
When selecting instruments be aware that medicalhome differences often exist in patient sociodemographiccharacteristics patient access patient flow and volume of-fice staff resources state EIECSE eligibility criteria andthe availability of early childhood community resourcesFor all these reasons different practices may require a dif-ferent combination of tools to optimize their early detec-tion and referral rates Table 3 provides a list of commonlyused tools along with their abbreviations and Web links
Objectively Comparing Measures for PrimaryCare SettingsAlthough all screens have their individual strengths andweaknesses Figs 1ndash4 (which are by no means an exhaus-tive list of measures) allow practitioners to compare someof the more commonly selected measures objectively Askyourself 1) Which measures meet the majority of techni-cal standards (white boxes) and best fit the needs of mypractice 2) Which measures do not meet the majority oftechnical standards (dark gray boxes) 3) Which measuresvariably or questionably meet many of these technicalstandards (light gray boxes) The authors of this articledo not have any conflicts of interest and have extrapolateddata directly from user manuals official Web sites andpublished peer-reviewed articles
Of note reported psychometric properties typicallywere determined in a combination of at-home day carepreschool and less frequently primary care settings by
Table 3 Abbreviations and Web Links for Commonly Used Measures
A Broad-band developmental parent-report screening measures1 ASQ-3 [ Ages amp Stages Questionnaire Third Edition httpwwwpbrookescom2 IDI [ Infant Development Inventory httpwwwchilddevrevcomindexhtmlCDR-PQ [ Childhood Development ReviewndashParent Questionnaire httpwwwchilddevrevcomindexhtmlCDI [ Child Development Inventory httpwwwchilddevrevcomindexhtml
3 PEDS [ Parentsrsquo Evaluation of Developmental Status httpwwwpedstestcom4 PEDSDM [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones httpwwwpedstestcom5 PDQ-II [ Prescreening Developmental Questionnaire II httpwwwdenveriicomPDQhtml
B Broad-band developmental practitioner-administered screening or assessment measures1 BDIST-II [ Battelle Developmental Inventory Screening TestndashII httpwwwriversidepublishingcom2 BINS [ Bayley Infant Neurodevelopmental Screener httpwwwpsychcorpcoukproductaspxn[1316ampskey[20703 Brigance Screens II httpwwwcurriculumassociates4 Capute Scales CATCLAMS [ Cognitive Adaptive TestClinical Linguistic Auditory Milestone Scales httpproducts
brookespublishingcomThe-Capute-Scales-P360aspx5 Denver II httpwwwdenveriicomDenverIIhtml6 PEDSDM (AL) [ Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones (Assessment Level) http
wwwpedstestcomC Narrow-band social-emotional- communication- and autism-specific screening measures1 ASQSE [ Ages amp Stages Questionnaire Social-Emotional httpwwwpbrookescom2 BITSEA [ Brief Infant Toddler Social Emotional Assessment httppearsonassesscom3 Greenspan SEGC[ Greenspan Social-Emotional Growth Chart httpwwwpearsonassessmentscomcgi-binMsmGo
exegrab_id[0amppage_id[8765ampquery[Greenspanamphiword[Greenspan204 CSBS DP ITC [ Communication and Symbolic Behavior Scales Developmental Profile InfantToddler Checklist http
wwwpbrookescom5 M-CHAT [ Modified Checklist for Autism in Toddlers (and its M-CHAT follow-up interview) httpwww2gsuedu
wpsydlrDiana_L_Robins_PhDhtmlD Mental health screening and assessment measures (for school-age children)1 PSC [ Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_homehtmPPSC [ Pictorial Pediatric Symptom Checklist httpwww2massgeneralorgallpsychpscpsc_formshtm
2 SDQ [ Strengths and Difficulties Questionnaire httpwwwsdqinfocom3 Conners 3[ Conners Rating Scalendash3rd edition (which can be used in children age 3ndash17 y) httpportalwpspublishcom
portalpage_pageid[53112710amp_dad[portalamp_schema[PORTAL4 Vanderbilt Assessment Scales httppedsmcvanderbilteducdcchilddevelopcenterhtm
growth and development developmental-behavioral screening measures
456 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

using paper-based and more recently online screeningmodalities Some forms of bias are present with varying de-grees of severity within the validation studies for all of thesemeasures but noteworthy issues are highlighted for eachinstrument Under feasibility costs have been calculateduniformly (the same for each tool) by using a paper-and-pen modifiable model from Dobrez et al (13) A costof $60 per hour was used to account for the combinationof practitioner and clinic staff wages Clinic costs will varybased on implementation procedures staff salaries thepercentage of caregivers with literacy problems andthe percentage of positive or concerning screens inonersquos practice
Note To view the references for this article and to viewlarger versions of the figures visit the October issue athttppedsinreviewaappublicationsorg and click onthe ldquoUnderstanding Developmental-Behavioral Screen-ing Measuresrdquo article
Summary
bull Although development and behavior are morecomplex than most anthropomorphic functions thatare measured in clinical practice they are quantifiableeven when applied to a busy primary care setting
bull Informal approaches to eliciting concerns ormeasuring milestones such as yesno checklistsextrapolated from lengthier measures surelycontribute to low detection rates of developmental-behavioral problems discerned by primary care providers
bull The periodic use of screening tools that better adhereto core psychometric and feasibility standards (egAges amp Stages Questionnaire Third Edition [ASQ-3]Parentsrsquo Evaluation of Developmental Status [PEDS]
andor Parentsrsquo Evaluation of Developmental StatusndashDevelopmental Milestones [PEDSDM] Ages amp StagesQuestionnaire Social-Emotional Pediatric SymptomChecklist) helps practitioners to optimize their earlyidentification rates for children who havedevelopmental-behavioral problems which leads to moreeffectively and efficiently enrolling greater numbers inearly intervention (EI) early childhood special education(ECSE) and other beneficial community services
bull Nevertheless to achieve a screening toolrsquos reportedreliability and accuracy it is essential that the tool beadministered and interpreted thoughtfully asdescribed in its userrsquos manual or official Web site
bull Careful attention to proper implementation andinterpretation also leads to a more collaborativeconversation between parents and practitioners
bull When screening results are concerning properimplementation and same-day interpretation ensurethat referrals occur in a 1) safe 2) equitable 3)effective 4) timely 5) parent- and patient-centeredand 6) efficient manner fulfilling the six quality aimsof the Institute of Medicine
bull If a practice has failed to implement the periodic use ofevidence-based screening measures successfully thenthe clinicians should strongly consider selecting somebroad-band developmental social-emotionalbehavioraland autism-specific screening tools for the practice
PIR QuizThis quiz is available online at httpwwwpedsinreviewaappublicationsorg NOTE Since January 2012 learners cantake Pediatrics in Review quizzes and claim credit online only No paper answer form will be printed in the journal
New Minimum Performance Level RequirementsPer the 2010 revision of the American Medical Association (AMA) Physicianrsquos Recognition Award (PRA) and creditsystem a minimum performance level must be established on enduring material and journal-based CME activities thatare certified for AMA PRA Category 1 CreditTM In order to successfully complete 2012 Pediatrics in Review articles forAMA PRA Category 1 CreditTM learners must demonstrate a minimum performance level of 60 or higher on thisassessment which measures achievement of the educational purpose andor objectives of this activity
Starting with the 2012 issues of Pediatrics in Review AMA PRA Category 1 CreditTM may be claimed only if 60 ormore of the questions are answered correctly If you score less than 60 on the assessment you will be givenadditional opportunities to answer questions until an overall 60 or greater score is achieved
1 A 17-year-old mother has concerns about her 3-year-old boyrsquos repeated temper tantrums and his frequentlyignoring her verbal communication She is feeling increasingly frustrated As a primary care provider which ofthe following is the most appropriate next step
A Administer a narrow-band ADHD screenB Administer and interpret a general developmental and social-emotional screen
Pediatrics in Review Vol33 No10 October 2012 457
growth and development developmental-behavioral screening measures
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

C Refer to a developmental-behavioral specialistD Refer to a teenage mother self-help group for counselingE Schedule a follow-up visit in 6 months and evaluate if symptoms persist
2 A 2-year-old otherwise healthy girl has not yet started to say ldquomamardquo and ldquodadardquo Her motor development appearsnormal Mother states that she does not appear to interact normally with her older siblings Which of the followingstatements is the most accurate regarding developmental and social-emotional screening in this situation
A False-positive result will unnecessarily increase parental anxietyB Normal screening results should reassure the parents that intervention will not be neededC Periodic screening identifies at-risk children for early intervention but in this clinical scenario an
automatic referral to an EI agency is justifiableD Screening is not valid in children age lt5 yearsE Screening should only be performed by a developmental-behavioral specialist
3 A mother is concerned about her 9-month-old boy developing autism like her neighborrsquos child Which of thefollowing is the most appropriate age to routinely administer an autism-specific screening tool
A 9 months and 15 monthsB 18 months and 2 yearsC 30 months and 3 yearsD 42 months and 4 yearsE 54 months and 5 years
4 Which of the following statements is most correct regarding developmental-behavioral screening measures
A Children who fail screening tests but subsequently are found not to have a developmental-behavioralproblem later perform as well academically as their peers
B Cliniciansrsquo subjective impressions are more accurate in identifying children having developmental-behavioral problem (sensitivity) than excluding those who do not (specificity)
C Majority of developmental delays are correctly identified by clinicians on routine examinations duringhealth supervision visits
D Periodic developmental-behavioral screening has been proven to enhance a clinicianrsquos ability to detectchildren who have evolving developmental-behavioral problems
E There is no evidence that early identification and intervention of developmental-behavioral problemsbefore kindergarten entrance improves subsequent academic performance
5 The mother of a 5-year-old boy replies to your inquiry about developmental or behavioral concerns ldquoWell hersquosa brat sometimes but I think thatrsquos pretty normal for this agerdquo To detect a wide spectrum of developmental-behavioral conditions accurately over time the American Academy of Pediatrics recommends
A Administering a social-emotional screening instrument only as needed if further history suggests that he isat risk for a previously undetected behavioral disorder
B Automatically referring the child and family to a mental health specialistC Automatically referring the child to assess eligibility for Early Childhood Special Education (ECSE)
Individual with Disability Education Act (IDEA) servicesD Routinely administering a screening test for maternal depressionE Routinely administering a social-emotional screening instrument
HealthyChildrenorg Parent Resources From the AAP
The reader is likely to find material to share with parents that is relevant to this article by visiting these links
bull httpwwwhealthychildrenorgEnglishfamily-lifehealth-managementpediatric-specialistsPagesWhat-
is-a-Developmental-Behavioral-Pediatricianaspx
bull httpwwwhealthychildrenorgEnglishages-stagestoddlerPagesAssessing-Developmental-Delaysaspx
growth and development developmental-behavioral screening measures
458 Pediatrics in Review Vol33 No10 October 2012
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from
DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from

DOI 101542pir33-10-448201233448Pediatrics in Review
Kevin P Marks and Angela C LaRosaUnderstanding Developmental-Behavioral Screening Measures
ServicesUpdated Information amp
httppedsinreviewaappublicationsorgcontent3310448including high resolution figures can be found at
Permissions amp Licensing
sitemiscPermissionsxhtmltables) or in its entirety can be found online at Information about reproducing this article in parts (figures
ReprintssitemiscreprintsxhtmlInformation about ordering reprints can be found online
by Kevin Marks on October 1 2012httppedsinreviewaappublicationsorgDownloaded from


















