Baseline Assessment of HIV Service Provider Productivity and ......TECHNICAL REPORT Baseline...
56
MARCH 2011 This report was prepared by University Research Co., LLC (URC) for review by the United States Agency for International Development (USAID). It was authored by Alison Wittcoff (URC), Lauren Crigler (Initiatives Inc.), Peter Mbago (URC), Edward Moshi (URC), and Rebecca Furth (Initiatives Inc.). The assessment was funded by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) and carried out under the USAID Health Care Improvement Project, which is made possible by the generous support of the American people through USAID. Baseline Assessment of HIV Service Provider Productivity and Efficiency in Tanzania TECHNICAL REPORT
Transcript of Baseline Assessment of HIV Service Provider Productivity and ......TECHNICAL REPORT Baseline...

MARCH 2011
This report was prepared by University Research Co., LLC (URC) for review by the United States Agency for International Development (USAID). It was authored by Alison Wittcoff (URC), Lauren Crigler (Initiatives Inc.), Peter Mbago (URC), Edward Moshi (URC), and Rebecca Furth (Initiatives Inc.). The assessment was funded by the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) and carried out under the USAID Health Care Improvement Project, which is made possible by the generous support of the American people through USAID.
Baseline Assessment of HIV Service Provider Productivity and Efficiency in Tanzania
T E C H N I C A L R E P O R T


TECHNICAL REPORT
Baseline Assessment of HIV Service Provider Productivity and Efficiency in Tanzania
MARCH 2011
Alison Wittcoff, University Research Co., LLC Lauren Crigler, Initiatives Inc. Peter Mbago, University Research Co., LLC Edward Moshi, University Research Co., LLC Rebecca Furth, Initiatives Inc.
DISCLAIMER
The views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government.

Acknowledgements: : The authors would like to thank our partners in the antiretroviral therapy (ART)/prevention of mother-to-child transmission (PMTCT) improvement collaborative in Mtwara, Tanzania: the Clinton Health Access Initiative (CHAI), the Elizabeth Glaser Pediatric AIDS Foundation (EGPAF), PharmAccess, the Mtwara Regional Health Management Team and Council Health Management Teams, and Dr. I.A. Msonde, District Medical Officer. The authors would also like to thank Dr. Davis Rumisha, University Research Co., LLC (URC) Chief of Party in Tanzania, for his assistance in making this activity possible. We also offer special thanks to Godfrey Nyomby, Regional Health Secretary; Alloyce Baba of CHAI; Dr. Richard Mbale of EGPAF; and Ms. Juliana Nabwire of URC’s Uganda office for their participation in the assessment.
The USAID Health Care Improvement Project (HCI) is implemented by URC under the terms of Contract Numbers GHN-I-01-07-00003-00 (HCI Task Order 1) and GHN-I-03-07-00003-00 (HCI Task Order 3). The Tanzania HIV service provider productivity and efficiency baseline assessment was carried out under HCI Task Order 1, which is made possible by the generous support of the American people through USAID. Support for the HIV service provider assessment was provided by the U.S. President’s Emergency Plan for AIDS Relief.
URC’s subcontractors for the USAID Health Care Improvement Project include EnCompass LLC, Family Health International, Health Research, Inc., Initiatives Inc., Institute for Healthcare Improvement, Johns Hopkins University Center for Communication Programs, and Management Systems International. Initiatives is the lead organization for HCI’s health workforce development activities. For more information on the work of the USAID Health Care Improvement Project, please visit www.hciproject.org or contact [email protected].
Recommended citation: Wittcoff A, Crigler L, Mbago P, Moshi E, and Furth R. 2011. Baseline Assessment of HIV Service Provider Productivity and Efficiency in Tanzania. Technical Report. Published by the USAID Health Care Improvement Project. Chevy Chase, MD: University Research Co., LLC (URC).

Tanzania HIV Provider Productivity and Efficiency Assessment • i
TABLE OF CONTENTS LIST OF TABLES AND FIGURES ................................................................................................................................... i ABBREVIATIONS .............................................................................................................................................................. ii EXECUTIVE SUMMARY ................................................................................................................................................. iii I. BACKGROUND ...................................................................................................................................................... 1 A. Assessment Objectives ........................................................................................................................................... 2 II. METHODOLOGY ................................................................................................................................................... 2 A. Site Selection ............................................................................................................................................................. 2 B. Instruments ................................................................................................................................................................ 3 C. Data Collection ......................................................................................................................................................... 5 III. FINDINGS .................................................................................................................................................................. 5 A. Staffing and Human Resources Management ..................................................................................................... 5 B. Workload and Staff Absences ............................................................................................................................... 7 C. Productivity ................................................................................................................................................................ 8 D. Employee Engagement ........................................................................................................................................... 10 E. Client Flow ............................................................................................................................................................... 12 F. Performance Management.................................................................................................................................... 13 G. Performance Evaluation ........................................................................................................................................ 16 H. Human Resource Management Challenges ...................................................................................................... 18 IV. CONCLUSIONS AND RECOMMENDATIONS ........................................................................................... 19 V. NEXT STEPS ............................................................................................................................................................ 20 VI. REFERENCES ........................................................................................................................................................... 21 VII. APPENDIX: DATA COLLECTION TOOLS ................................................................................................... 21 Site Manager Interview ................................................................................................................................................. A-1 Health Worker Interview ............................................................................................................................................ B-1 Council Health Management Team Interview ........................................................................................................C-1 Regional Health Management Team Interview ...................................................................................................... D-1 Time Utilization Observation ..................................................................................................................................... E-1 Employee Engagement Questionnaire ....................................................................................................................... F-1 Client Flow Assessment Tool .................................................................................................................................... G-1
LIST OF TABLES AND FIGURES Table 1: Characteristics of the sites assessed ............................................................................................................. 2 Table 2: Sample sizes for data collection tools ........................................................................................................... 3 Table 3: Staffing levels at sites assessed ........................................................................................................................ 7
Figure 1: Vacancy rates in Mtwara ................................................................................................................................. 6 Figure 2: Productivity by task for providers delivering ART services in three sites in Mtwara (n=15) ........ 8 Figure 3: Percentage of ART service provider time spent on productive tasks in three Care and Treatment Centers (n=15) .............................................................................................................................................. 9 Figure 4: Productivity levels for health workers observed during one work day in three sites (n=15) ....... 9 Figure 5: Overall engagement score by type of provider (n=27) ......................................................................... 10 Figure 6: Overall average employee engagement score per site (n=27) ............................................................ 11 Figure 7: Average score per question on engagement questionnaire, all sites (n=27) ................................... 11 Figure 8: Average wait and contact time for each service, four sites (n=29) ................................................... 12 Figure 9: Average client wait and contact times per service, Site 1(n=16) ....................................................... 13 Figure 10: Areas in which health workers feel they need more training (n=19) ............................................. 14 Figure 11: Last supervision visit received (n=14) ..................................................................................................... 15 Figure 12: Level of staff motivation in facilities (n=15) ........................................................................................... 17

ii • Tanzania HIV Provider Productivity and Efficiency Assessment
ABBREVIATIONS AIDS Acquired immunodeficiency syndrome ART Antiretroviral therapy ARV Antiretroviral CD4 Cluster of differentiation 4 CHAI Clinton Health Access Initiative CHMT Council Health Management Team CO Clinical officer CTC Care and treatment center DACC District AIDS Control Coordinator EGPAF Elizabeth Glaser Pediatric AIDS Foundation FP Family planning HC Health center HCI USAID Health Care Improvement Project HIV Human immunodeficiency virus HMIS Health Management Information System HR Human resources MO Medical officer MOH Ministry of Health MOHSW Ministry of Health and Social Welfare NGO Non-governmental organization OPRAS Open performance review and appraisal system PMS Performance management system PMTCT Prevention of mother-to-child transmission PITC Provider-initiated counseling and testing QI Quality improvement RACC Regional AIDS Control Coordinator RHMT Regional Health Management Team STI Sexually transmitted infection TB Tuberculosis URC University Research Co., LLC USAID United States Agency for International Development VCT Voluntary counseling and testing WHO World Health Organization

Tanzania HIV Provider Productivity and Efficiency Assessment • iii
EXECUTIVE SUMMARY
Tanzania, like many other countries in Africa, is facing a severe shortage of qualified health professionals. Only 35% of positions in government health facilities have been filled, leaving Tanzania in the wake of burgeoning human resources for health crisis. According to the Annual Health Statistical Abstract from 2008, the national average population per medical officer was 64,000; 31,000 per assistant medical officer; and 7,000 per clinical officer. The shortage of health professionals has been exacerbated by the HIV/AIDS pandemic and other communicable diseases, such as malaria and tuberculosis.
In addition to the personnel crisis, according to studies conducted by both the Clinton Foundation and the Capacity Project, one of the most critical gaps in human resources in Tanzania is the need for improved performance management at the facility level. Over-loaded health workers, understaffed facilities, and weak or non-existent performance management systems negatively impact worker productivity and engagement. These issues become increasingly severe in rural and hard-to-reach areas and can create a serious barrier to improvement in the quality of antiretroviral therapy (ART) and prevention of mother-to-child transmission of HIV (PMTCT).
In an effort to improve the quality of HIV services delivered in Tanzania, the USAID Health Care Improvement Project (HCI) and the Ministry of Health and Social Welfare (MOHSW) began implementing a partner improvement collaborative in the Mtwara Region in June of 2009. The aim of the collaborative is to apply improvement methods to ART and PMTCT services in order to ensure the delivery of high quality care to clients.
In order to improve the efficiency of service delivery and strengthen health worker performance and engagement, the collaborative began to integrate human resources interventions into its work in 2010. Health worker engagement describes a health worker’s state of mind when he or she is not only satisfied with his or her job, but is also motivated to do the work, committed to doing it well, and feels valued for doing it. Health worker productivity and engagement are integral to improving efficiency, as they determine what tasks health workers perform and how engaged and motivated they are to perform at a high level.
In collaboration with the MOHSW, HCI designed a baseline assessment of HIV/AIDS service providers to gather information on productivity and engagement. The information gathered from the baseline assessment was used to develop a set of improved human resource practices that will be integrated into the ongoing ART/PMTCT collaborative. The baseline was conducted in six sites in Mtwara from June 30−July 6, 2010.
Key findings from the assessment include:
• Providers observed spent 36% of their total time on direct patient care and 19% on indirect patient care. Providers thus spent 55% of their time caring for patients, 8% of their time on meetings/ administration and 4% on cleaning/preparation. However, providers spent 11% of their time waiting for patients, 8% on breaks, 7% on social visits, and 7% in unexplained absences.
• In the six sites assessed, five of the six site managers said that staff absences occur on a regular basis ranging from 1-3 staff absences per week. All six site managers said that providers at their site have to work more than their scheduled hours.
• When providers were asked individually if they had written job descriptions that clearly defined their tasks and responsibilities, 73% said no (11/15) and 27% said yes (4/15). However, when data collectors asked to see the job descriptions for those who said yes, only 1 of those 4 could produce their job description.
• Engagement scores for recognition (2.2) and materials (3.3) scored very low, highlighting definite areas where improvements can be made.

iv • Tanzania HIV Provider Productivity and Efficiency Assessment
• Lab staff and nurse/midwives were engaged, scoring 4.1 and 4.2, respectively. Scores for clinical officers, counselors, and other personnel (which included data clerks and volunteers) fell just below the engagement threshold, at 3.9. Nurse assistants and pharmacist/dispensers scored a bit lower, at 3.6 and 3.7, respectively, signaling they are somewhat disengaged.
• Patients on average waited a total of 76 minutes (1 hour 16 minutes) at care and treatment centers for an average of 30 minutes of contact time for all services combined. The greatest wait times occurred at consultation (19 minutes on average) and at the lab (38 minutes).
• While a large percentage of health workers had received training within the past year, 80% do not feel that they receive adequate training on a regular basis. Areas in which providers felt they were lacking training included PMTCT, CD4 tests, and use of antiretroviral medications.
• Although health workers are being supervised, they do not appear to be receiving feedback about their performance on a regular basis: 7% of providers said they receive feedback once a week, 13% once every two weeks, and 20% once a month. Half (47%) of providers responded ‘other’ when asked about frequency of feedback, which included the following: no feedback given, immediately on specific tasks, every two months, after supervision visits, and during performance evaluations. The other 13% did not respond to the question.
• Only 27% of the providers interviewed said they had ever received a performance evaluation.
In summary, the assessment identified several areas where human resource management systems can be improved to strengthen provider efficiency and productivity and improve the quality of HIV/AIDS service delivery. All health workers should be provided with written job descriptions that clearly align their tasks and goals. Without written job descriptions, it is impossible to implement strong performance management.
Recognition and reward systems can be improved to ensure that health workers get the acknowledgement and praise they deserve when they perform well. The process for performance evaluations needs to be communicated clearly with lower level facilities. Facility managers and providers should also learn how to set performance objectives. Promotion and career advancement opportunities are somewhat rare, which may affect worker motivation. The majority of employees are moderately engaged, regardless of the type of facility or the position they hold, but specific areas of engagement, such as recognition and materials, could be improved.
Productivity appears to vary throughout the day with providers being very productive in the morning when patients arrive and productivity levels decreasing dramatically in the afternoon when client loads are low. Client flow does not appear to be a problem, but is something that should continue to be monitored since client loads can vary dramatically by day.
Based on the results of the assessment, a set of human resource management interventions was developed into a change package that QI teams from 12 sites in Mtwara are now testing to improve engagement and efficiency at the facility level. Teams began with Improvement Objective 1 (clearly aligned tasks and goals), which will result in more clearly defined roles and responsibilities for all health workers delivering HIV services. QI teams share lessons learned and best practices during quarterly learning sessions. Upon completion of all seven improvement objectives, the key practices leading to better outcomes will be packaged for spread at the national level.

Tanzania HIV Provider Productivity and Efficiency Assessment • 1
I. BACKGROUND As in a number of other African countries, Tanzania is facing a severe shortage of qualified health professionals. Only 35% of positions in government health facilities have been filled, leaving Tanzania in the wake of a burgeoning human resources for health crisis (Bilame and Masui, 2010). According to the Annual Health Statistical Abstract from 2008, the national average of the population per medical officer was 64,000, 31,000 per assistant medical officer, and 7,000 per clinical officer. The shortage of personnel has been exacerbated by the HIV/AIDS pandemic and other communicable diseases, such as malaria and tuberculosis (TB).
In addition to the personnel crisis, according to studies conducted by the Clinton Foundation and the Capacity project, one of the most critical gaps in human resources (HR) in Tanzania points to the need for improved performance management at the facility level. Over-loaded health workers, understaffed facilities, and weak or non-existent performance systems can negatively impact worker productivity, and engagement, and contribute to a seeming lack of ownership and empowerment from workers regarding their jobs and responsibilities. These issues become increasingly severe in rural and hard to reach areas and can create a serious barrier to improvement in the quality of ART and PMTCT services.
In order to improve performance management and maximize health worker output, Tanzania introduced several systems to manage performance at both the institutional and individual level. To assist institutions in the planning, implementation, monitoring and reporting on performance, Performance Management Systems (PMS) were introduced by the MOHSW in 2003. However a study conducted by the Clinton Foundation found that the use of these systems and compliance to them was fairly low. In 2004, the Open Performance Review and Appraisal System (OPRAS) was introduced to enhance performance management as well as offering a mechanism for measuring performance. However, awareness and understanding of OPRAS was found to be low during the Clinton Foundation study. In addition, use of OPRAS was found to be inconsistent and not available at all facilities (Clinton Foundation, 2008).
A critical first step in confronting the scarcity, mal-distribution, and often disengaged health workforce is to reduce turnover and increase the productivity of staff already in place. There are many factors that influence how productive a worker is: research has shown there is a clear link between job satisfaction and intention to leave a post, and some studies demonstrate that efforts to improve job satisfaction are closely related to efforts to improve productivity, competence, and responsiveness of workers (Schoo and Dunbar, 2005). Financial benefits are an important factor, especially when salaries are very low, but they are not the only, nor the most important factor (Hongoro and Normand, 2006; Dussault and Fanceschini, 2006). Other important elements are organizational and professional support, supportive supervision and feedback, influence in decision-making regarding the medical practice and working life, career opportunities and professional development, the work environment, worker safety, and the availability of opportunities to develop skills and to grow (Dieleman and Harnmeijer, 2006).
In an effort to improve the quality of care of HIV services delivered in Tanzania, the USAID Health Care Improvement Project (HCI) and the Ministry of Health and Social Welfare (MOHSW) began implementing a partner improvement collaborative in Mtwara region in June of 2009 with the aim of ensuring high quality ART and PMTCT care is being delivered to clients. The collaborative is now looking to integrate HR interventions into its work in order to improve the quality of care by strengthening the efficiency of service delivery, strengthening health worker performance, improving health worker engagement, and increasing staff retention. Health worker productivity and engagement1
1 Engagement describes a health worker’s state of mind when he or she is not only satisfied with his/her job, but is motivated to do the work, committed to doing it well, and feels valued for doing it. Extensive research conducted in both in the United States and internationally has shown that if a person is “engaged” in his or her job, the productivity of the organization improves significantly, and he or she performs far better in client-facing roles.

2 • Tanzania HIV Provider Productivity and Efficiency Assessment
are integral to improving efficiency as they determine what tasks health workers perform and how engaged and motivated they are to perform at a high level.
A. Assessment Objectives In collaboration with the MOHSW, HCI designed the baseline assessment to gather information on productivity and engagement of HIV/AIDS service providers. The information gathered will be used to develop a set of HR improvements based on best practices that will be integrated into the ongoing ART/PMTCT collaborative. The assessment was designed to gather information on:
• Performance management and evaluation systems • The engagement of providers delivering ART or PMTCT services • The productivity of providers delivering ART or PMTCT services
• Provider perceptions of their current workload • Patient flow, wait times and time of contact with providers In addition to the objectives above, the assessment briefly looked at HR management systems, policies, and planning as well as HR issues present at regional, district and site levels to provide further context for the baseline.
II. METHODOLOGY
A. Site Selection HCI selected six ART sites in Mtwara for the baseline assessment. This purposive sample included sites from different levels of the health system in Tanzania (a hospital, health centers, and dispensaries). All of the sites chosen are currently participating in the ART/PMTCT partner collaborative. Table 1 lists the sites and their characteristics, including whether services were “vertical” (HIV only) or “integrated” (HIV included as part of a larger, integrated package of service delivery). Sites with staff classified as “mixed” had some staff that were dedicated to providing only HIV/AIDS services and others who provided both HIV/AIDS and other health services. It should be noted that all sites provided a variety of health services, but that those facilities that offered HIV/AIDS services in a separate room or building and with separate staff from the rest of the facility were classified as “vertical,” although they were not “stand-alone” sites in the classic sense.
Table 1: Characteristics of the sites assessed
Site Site Type Service Type
Staff Type Days/week ART/PMTCT
Service Offered
ART /PMTCT
Clinic Staff - Total
Numbers
Clients per Month (April 2010)
1 Government Hospital Integrated Mixed Daily 21 1031
2 Government Health Center Integrated All Integrated Daily 19 15
3 Government Health Center Integrated All Integrated Daily 4 201
4 Government Dispensary Integrated All Integrated Tuesdays 3 1
5 Government Dispensary Integrated All Integrated Tuesdays 3 30
6 Faith-based NGO Health Center Integrated Mixed Daily 6 80

Tanzania HIV Provider Productivity and Efficiency Assessment • 3
B. Instruments Seven data collection instruments were applied in the assessment: a site manager interview, a health worker interview, Council Health Management Team (CHMT) interview, Regional Health Management Team (RHMT) interview, a time utilization observation, an employee engagement questionnaire, and a client flow assessment tool. The data collection instruments are included in the appendix to this report. Table 2 shows the sample size for each data collection instrument per site. As illustrated in the chart below, Site 1 had a greater number of health worker interviews, employee engagement questionnaires, and client flow tools implemented than the other sites. This is because on the day of data collection, site 1 had a larger number of health workers present than other sites as well as a greater number of clients.
Table 2: Sample sizes for data collection tools
Instrument Number Applied per Site Total
Site 1
Site 2
Site 3
Site 4
Site 5
Site 6
Clinic/Site Manager Interview and Record Review 1 1 1 1 1 1 6
Health Worker Interview 7 2 3 2 0 1 15
Time Utilization Observation 6 5 4 0 0 0 15
Employee Engagement Questionnaire 13 3 4 3 2 2 27
Client Flow Assessment 16 7 4 0 2 0 29
CHMT Interview 5
RHMT Interview 2
1. Site manager interview Interviews were conducted with site managers at all six sites to gather information on services provided, structure of services, staffing structures, human resource management systems, and client load.
2. Health worker interview Interviews with individual health workers were conducted at five of the six sites to gather information on workload, job satisfaction, working conditions, supervision, opportunities for advancement, performance management, motivation, and training. The health workers interviewed included: medical officers, clinical officers, nurses, midwives, pharmacist, lab personnel, and a data clerk. No health worker interviews were conducted at site 5 because there were only two staff on duty (the site manager and another health worker) when the health worker became ill and went home. Fifteen health workers were interviewed at five sites: three lab personnel, two nurse assistants, five nurses/midwives, one pharmacist, and four other types of health workers.
3. RHMT and CHMT interviews Interviews with members of one CHMT and members of the RHMT were conducted to gather information on human resources policies, supervision systems, performance management and evaluation, promotions, incentives available to health workers, recruitment, and training. The interviews of the CHMT members were conducted individually but due to time constraints, a group interview was conducted with several RHMT members: the Regional Medical Officer, Regional Pharmacist, Regional Lab Technologist, and the Acting Regional Health Officer. In addition, an individual RHMT member interview was also conducted.

4 • Tanzania HIV Provider Productivity and Efficiency Assessment
4. Time utilization observation How service providers spend their time can have a major impact on service quality and client flow. Members of the data collection team directly observed providers for an entire day. Providers were observed every fifteen minutes to identify whether they were involved in productive or unproductive tasks. Data collection started at the clinic’s official opening hours and concluded when the clinic closed or the service provider left for the day. Data collectors observed a total of 15 health workers in three facilities. Data collection was not possible in site 6 because the data collection team was involved in a road accident and was unable to make it to the site on the 2nd day. The team was also unable to complete the time utilization tool at sites 4 and 5 where data were collected on only one day, as opposed to the two days spent at sites 1, 2 and 3.2
5. Employee engagement tool
The employee engagement tool was used to assess engagement levels of health workers. Employee engagement refers to elements of motivation, but goes beyond traditional definitions of motivation or satisfaction to include issues related to employee commitment to the organization and to performing high quality work to help the organization advance. Employee engagement may be defined as “a heightened emotional connection that an employee feels for his or her organization that influences him or her to exert greater discretionary effort to the work.”3
6. Client flow assessment tool
Studies have shown that employees that are more engaged tend to be more productive, more loyal and less likely to vacate their posts. Baseline data on engagement was collected using a confidential questionnaire of 16 statements relating to self-efficacy, performance, work relationships, and work climate. The questionnaire included statements related to the worker’s belief in the importance of his/her work and the organization; belief in his/her ability to succeed; relations with colleagues and supervisors; opportunities for professional advancement; support and recognition; and the perceived influence he/she has in decision making. Members of the data collection team reviewed the sixteen statements with the providers individually to ensure that they understood each statement before leaving providers to complete the tool privately. The tool requires providers to rate their response to each statement on a five-point scale from “strongly disagree” (1) to “strongly agree” (5). A total of 27 health workers representing all cadres at the six sites filled out the engagement tool.
To document information on how clients move from one service to another, how long they waited for services, and how much time they spend with providers, the data collection team administered a client flow tool. The team worked with clinic staff to initiate the tool at registration. Each client who presented at the clinic registration was asked what time he or she arrived at the clinic. The arrival time and the start and end time for registering the client were recorded on the form. The form went with the client to each point of service at the clinic. Each staff member was provided with a clock and instructed to record the start time and end time of the service provided. Services recorded included: registration, triage, clinical assessment, clinical care, counseling, laboratory, and pharmacy/dispensary. The form provided space for other types of services to be recorded as necessary. Data were collected for a total of 29 clients across the four sites where the client flow tool was applied. There was no information collected on client flow at sites 4 and 6 because there were no clients that arrived for HIV/AIDS services on the days the sites were assessed.
2 The scheduling of HIV service delivery days at site 4 and 5, combined with the schedules of other sites and time limitations of the data collection team, made it impossible to allocate a second day of data collection.
3Definition of engagement at http://www.management-issues.com/2007/3/8/opinion/employee-engagement-what-exactly-is-it.asp.

Tanzania HIV Provider Productivity and Efficiency Assessment • 5
C. Data Collection Two data collection teams each visited three sites from June 30- July 6, 2010. The teams included URC staff from headquarters, the Uganda office, and the Tanzania office, as well as members from partners participating in the improvement collaborative: EGPAF, Clinton Foundation, and the Regional Health Secretary from Mtwara. HCI’s headquarters team provided a one-day training to the data collectors on the tools, data collection methods, and methods to ensure data quality. Team members also had the opportunity to test out the tools and apply what they had learned in the training during the field test that took place prior to baseline data collection.
1. Ethical considerations All interviews and questionnaires were anonymous and confidential. Data collectors were trained to explain the purpose of each interview or questionnaire to the provider, and providers were given an option to opt out of the interview or survey. The client flow tool was explained to each client at registration, and their permission was sought to administer the tool. No data on individual clients or details of the medical service provided to them was recorded on the form. Data collectors were instructed not to interrupt clinical services or counseling sessions when documenting time utilization. All time in which a client was in a room with a clinician or counselor was recorded as direct client care.
2. Limitations The human resources assessment was only conducted at six HIV sites that are part of an ongoing HCI-supported partner improvement collaborative. Because of the small sample size, the findings and recommendations in this report should not be perceived as a solution or prescription for all HIV clinics in Tanzania. HCI hopes that the findings and recommendations in this report will engender further discussion and research on how to solve the human resource issues present in the Tanzanian health system and improve the efficiency, productivity, and quality of care delivered by HIV/AIDS service providers.
III. FINDINGS A. Staffing and Human Resources Management The Regional Health Management Team in Mtwara is responsible for the coordination, planning, and implementation of health services in the region. This also includes conducting supportive supervision, monitoring and evaluation of activities, and dissemination of policies and guidelines. The Council Health Management Teams support health activities in the district and are responsible for preparing the Comprehensive Health Plan, evaluating health activities, implementing national guidelines, and offering supportive supervision to lower level health facilities in their respective district.
1. Staffing The staffing of clinics can have a significant impact on provider productivity, efficiency and even engagement. If clinics have a shortage of clinicians, clients can back up at the clinician’s door; too many staff or staff members that do not have clear roles or responsibilities may result in idle time. Few support systems or no means of recognition can leave staff disengaged from their work and uninterested in making the effort needed to provide a high quality service. The RHMT, CHMT, and site manager interviews gathered data on service delivery, staffing levels and recognition and reward systems to provide a descriptive framework for understanding time utilization, human resource management systems, client flow, and engagement.
RHMT and CHMT members were asked how staffing levels were determined in their region/district. According to both RHMT and CHMT members, staffing levels are determined by the staff establishment directives set by the MOHSW for each health system level. The national staffing establishment

6 • Tanzania HIV Provider Productivity and Efficiency Assessment
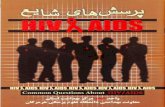
directives are determined by using a data system that helps identify deficits. In order to recruit/fill open positions, the CHMT members identify the vacancies in the district and communicate these needs to the District Executive Officer, who then sends the needs to the Prime Minister’s Office for Regional Administration for approval, which advertises the vacancies. The RHMT follows a similar process of identifying needs, sending them to the President’s Office for Public Service Management for approval, and then the jobs are posted. It should be noted that the process of identifying needs and sending them for approval only occurs once a year. Figure 1 below shows the current rates of vacancy for medical officers, clinical officers, and nurses/midwives, according to the CHMT members interviewed in Mtwara.
Figure 1: Vacancy rates in Mtwara
Results from the site manager interview show variability in the numbers and types of staff allocated to the sites and position vacancies. Table 3 shows the types and numbers of providers working at each site. Five of the six sites assessed had neither a pharmacist nor a pharmacy assistant on staff. Instead, nurses or midwives were allocated to dispense drugs. The majority of site managers as well as providers complained of understaffing. Vacancies compared with the perceived4
2. Recruitment process
staffing standards for sites ranged from three posts to 18 posts. The posts that were vacant included: counselors, pharmacists, nurse/midwives, lab staff, medical officers, and clinical officers. The issue of staffing shortages is likely to remain for the near future in the Mtwara Region due to limits on resources for contracting staff.
It is important for recruitment processes to be as fair and reasonable as possible, especially when there is a crisis in terms of having adequate human resources for health. The process should not be cumbersome or take an unreasonable amount of time or this will discourage people from applying. The process should also be as fair and transparent as possible so that everyone is given a fair chance. When asked how they were recruited, 53% of health workers interviewed said they applied for the position, were interviewed, and then received a job offer; 33% applied for the position and were accepted without an interview; and 13% were absorbed into the system or recommended for a position. Eighty percent (12/15) of health workers felt that the recruitment process was reasonable. The three providers who felt the process was unreasonable cited the fact that they had to work for a long period of time temporarily without a contract. This is an issue that was also cited by the CHMT.
4 Most managers were unaware of a designated staffing standard for their site. They based their assessment of staffing expectations on staffing levels defined by the site or program overseeing the site, but the rationale for the staffing levels was not clear.
68%
49%
68%
0%10%20%30%40%50%60%70%80%90%
100%
Medical Officer Clinical Officer Nurse/Midwife
Source: Tanzania MOHSW HMIS 2009

Tanzania HIV Provider Productivity and Efficiency Assessment • 7
Table 3: Staffing levels at sites assessed
Cadre Site 1:
Hospital
Site 2: Health Center
Site 3: Health Center
Site 4: Dispensary
Site 5: Dispensary
Site 6: Health Center
Total per
Cadre Medical Officers 1 - - - - - 1 Assistant Medical Officer 3 - 1 - - - 4
Clinical Officers 3 2 - - 1 - 6 Nurses/Midwives 4 2 1 1 - 25 10 Nurse Assistants - 4 1 1 - 16 7 Lab Staff 3 2 - 1 - 1 7 Counselors 3 37 - - 2 - 8 Pharmacist Assistant 1 - - - - - 1 Pharmacist - - - - - 3 Social Worker 3 Nursing Officer 2 - - - - - 2
B. Workload and Staff Absences Not only are many sites in Tanzania faced with a shortage of workers, there are also a high number of staff absences occurring on a regular basis. In the six sites assessed, five of the six site managers said that staff absences occur on a regular basis ranging from 1-3 staff absences per week. The reasons that site managers noted for absences8
Almost all (14/15) health workers interviewed said that absences of co-workers occurred on a regular basis at the facility. When asked why staff were absent, the following responses were received (more than one response was possible): vacation (7), sick leave (5), maternity leave (2), training (10), don’t know (1), banking services (2), staff work in other department (3), and day off after having worked night-shift (1). Health workers reported that the frequent staff absences led to staff having to work more hours: 93% (14/15) of staff said they have to work more than their schedule hours. Of those staff, 57% said this happened more than once a week; 14% said they work more than their scheduled hours once a week; 14% said twice a month; 7% said more than two times a month; and 7% said almost every day. Reasons noted for having to work extra hours included: high number of patients, administrative matters, coordination meetings, emergencies, and shortage of staff.
included: vacation (2), sick leave (2), maternity leave (1), training (4), and other (2). Frequent absences have an impact on the daily workload of clinic staff present. All six site managers said that providers at their site have to work more than their scheduled hours. Five of the six site managers said that staff members work more than their scheduled hours more than once a week. When asked why, all six site managers cited low number of staff as one of the reasons. Other reasons included a high number of patients and emergencies. However, in half of the sites assessed, site managers said that providers also work less than scheduled hours. The reasons noted for working fewer that scheduled hours included low number of patients and scarcity of drugs.
Providers were also asked if they ever worked less than their scheduled hours. Only 27% (4/15) of providers said they worked less than their scheduled hours. Reasons given included low number of patients, preparation for night duty, and evening classes. 5The nurses are also counselors. 6The nurse asst. also does counseling. 7 One of the counselors is a nurse. 8 More than one response was allowed.

8 • Tanzania HIV Provider Productivity and Efficiency Assessment
C. Productivity Providers need to maintain a high level of productivity throughout the day in order to effectively address the demand for HIV services. To assess the productivity of health workers in HIV clinics during a regular work day, 15 health workers in three different sites were observed every 15 minutes for one full work day. Productive time included time spent in direct contact with patients as well as indirect patient care–preparation, review and updating of charts; consultation with other providers; management tasks such as meetings and routine maintenance; and off-site activities such as trainings and outreach. Activities classified as unproductive time included time spent waiting for patients, breaks, social visits and conversation, personal errands, and absences not related to client care or service delivery. It is important to note that each health worker was only observed during one day. Patient load varies on different days of the week at the HIV Clinics, thus findings on other days might be quite different.
Based on the direct observations of health providers in three facilities, the assessment found that providers spent 36% of their total time on direct patient care and 19% on indirect patient care. Providers thus spent 55% of their time caring for patients. However, providers also spent 11% of their time waiting for patients and 7% of their time was recorded as unexplained absences. Figure 2 provides a breakdown of productivity for all staff observed.
Figure 2: Productivity by task for providers delivering ART services in three sites in Mtwara (n=15)
Productivity levels were found to vary by providers; the average time spent doing productive tasks for medical officers was 74%, clinical officers 86%, nurse/midwives 74%, lab technicians 72%, pharmacy personnel 39%, and other employees such as data clerks was 61%. Figure 3 provides a breakdown of productivity levels by cadre.
36%
19%
0%8%
0% 4%11% 8% 7% 7%
0%
67%
33%
0%10%20%30%40%50%60%70%80%90%
100%
Productive time
Unproductive time

Tanzania HIV Provider Productivity and Efficiency Assessment • 9
Figure 3: Percentage of ART service provider time spent on productive tasks in three Care and Treatment Centers (n=15)
It is important to note that during the morning, patient loads are very high, but in the afternoon, patient loads tended to decrease at most sites leaving providers with no patients to see. This leads to most providers being extremely busy in the morning with the work tailing off later in the afternoon. Figure 4 below shows the percentage of staff engaged in productive activities by time of day.
Figure 4: Productivity levels for health workers observed during one work day in three sites (n=15)
74%
86%
74%
63%
72%
39%
61%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
8:00 9:00 10:00 11:00 12:00 1:00 2:00 3:00 3:30
% o
f pro
duct
ive
activ
ity
Time of day

10 • Tanzania HIV Provider Productivity and Efficiency Assessment
D. Employee Engagement Employee engagement measures how workers feel about their job and the environment in which they work. Research has shown that health workers that are “engaged” (scoring 4.0-5.0 on the questionnaire) in their work have a higher level of productivity, are more loyal to their organizations, tend to perform better, and are absent less often. Employees who are “disengaged” (scoring 3-3.9) are less productive than engaged employees, are less loyal to their organization, and are not having their needs met. Finally, those providers that are “actively disengaged” (scoring 1-2.9) have low levels of productivity, have high rates of absenteeism, feel compelled to spread their disillusionment to other colleagues, and are not loyal to their organization. To ensure high rates of efficiency and productivity, providers need to be engaged in their work.
Results from the employee engagement questionnaire, which was applied at all six sites with 27 health care providers, were analyzed by type of provider, site, and question. When overall average scores on the employee engagement questionnaire were analyzed by provider, there was little variation in scores (see Figure 5). Lab staff and nurses/midwives were engaged, scoring 4.1 and 4.2, respectively. Scores for clinical officers, counselors, and other personnel (which included data clerks and volunteers) fell just below the engagement threshold, at 3.9. Nurse assistants and pharmacist/dispensers scored a bit lower, at 3.6 and 3.7, respectively, signaling they are somewhat disengaged.
Figure 5: Overall engagement score by type of provider (n=27)
The engagement questionnaires were also analyzed by site. There was little variation in scores between sites with average scores ranging from 4.1 (engaged) to 3.6 (disengaged) as can be seen in Figure 6.
3.9
4.2
3.6
4.1
3.73.9 3.9
1
1.5
2
2.5
3
3.5
4
4.5
5
Scor
e ou
t of 5
Engaged
Actively Disengaged
Disengaged

Tanzania HIV Provider Productivity and Efficiency Assessment • 11
Figure 6: Overall average employee engagement score per site (n=27)
The analysis of employee engagement by question reveals more detail on specific areas where engagement is low. Figure 7 below shows that recognition (2.2) and materials (3.3) scored lowest, highlighting areas where improvements can be made. Other areas scored quite high, such as belief in their job being important (4.8), clarity of expectations (4.5), and respect (4.5), signaling areas of achievement.
Figure 7: Average score per question on engagement questionnaire, all sites (n=27)
4.13.9
4.1
3.6
3.8 3.9
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Site 1 Site 2 Site 3 Site 4 Site 5 Site 6
Scor
e ou
t of 5
4.84.5 4.5
3.3
4.3
3.9 3.94.0
3.6
4.0 3.8
2.2
4.2 4.14.4 4.3
1
1.5
2
2.5
3
3.5
4
4.5
5
Scor
e ou
t of 5

12 • Tanzania HIV Provider Productivity and Efficiency Assessment
E. Client Flow Client flow is a key measure to understanding the effectiveness and efficiency of services being delivered in sites. If services are being delivered efficiently and providers have high levels of productivity, clients should have fairly low wait times and have adequate contact time with providers to receive good quality care. The client flow tool was used in four different facilities to track a total of 29 clients. It is important to note that on the day assessment teams implemented the client flow tool, patient loads were not especially high. However, client loads can vary by day so it is possible that if the assessment teams implemented this tool on another day, client loads may have been higher and results may have varied.
Patients on average waited a total of 76 minutes (1 hour 16 minutes) for an average of 32 minutes of provider contact time for all services combined. The greatest wait times occurred at consultation (19 minutes on average) and at the lab (38 minutes). Figure 8 shows where clients observed at the HIV clinics in the four sites spent their time on average and how much time they spent waiting at each stage of their visit. At most stages of the process—registration, triage, consultation, clinical assessment, and counseling—patients are not forced to wait for exceedingly long periods of time to receive care.
Figure 8: Average wait and contact time for each service, four sites (n=29)
Figure 9 below provides a snapshot of how client flow worked at one Care and Treatment Center based on a total of 16 clients. Waiting times were quite reasonable at the center, with clients waiting on average 39 minutes for 12 minutes of contact time. However, clients were waiting disproportionately long times at the lab (51 minutes for 5 minutes of contact time), signaling an area where client flow could be improved.
157
19
83
38
4
76
1 3
147 4
105 5
32
0.0
20.0
40.0
60.0
80.0
MIN
UTE
S
Average Wait Time Average Contact

Tanzania HIV Provider Productivity and Efficiency Assessment • 13
Figure 9: Average client wait and contact times per service, Site 1 (n=16)
F. Performance Management 1. Job descriptions As mentioned in the beginning of this report, one of the major deficiencies of the human resource system in Tanzania cited in earlier studies is performance management at the facility level. Written job descriptions with clearly aligned goals and tasks are a cornerstone to ensuring the existence of strong performance management. Job descriptions are essential because they allow providers to know what specific tasks they are responsible for, and they provide a basis/standard against which providers can be given feedback about performance and evaluated.
The baseline assessment found that most providers at the facility level are lacking job descriptions. Only one site manager out of six interviewed said that employees at their facility had a written job description that clearly defined roles and tasks. Of the five CHMT members interviewed, only two said that all providers in their district had written job descriptions. When providers were asked individually if they had written job descriptions that clearly defined their tasks and responsibilities, 73% said no (11/15) and 27% said yes (4/15). However, when data collectors asked to see the job descriptions for those who said yes, only one of those four could produce their job description.
However, at higher levels of the system, for example RHMT members, job descriptions do exist. According to the group interview, all RHMT members have job descriptions (which they were able to produce). Yet, the RHMT members said that the majority of providers do not have written job descriptions even though it is the responsibility of the RHMT to provide those descriptions.
2. Training For health providers to offer high quality care, it is important that they have the necessary skills and training to perform their assigned duties. Continuous training of health providers is essential to ensure that skills of providers are up-to-date and that they are trained on any new procedures, guidelines, etc.
1
10
18
84
51
20
39
1 25
83 5 3
12
0
15
30
45
60
75
Registration Triage Consultation Clinical Assessment
Counseling Lab Dispensing Other TOTAL
16 16 1 6 15 6 5 0 16
100% 6% 38% 94% 38% 31% 0%
MIN
UTE
S
Wait Time
Contact Time

14 • Tanzania HIV Provider Productivity and Efficiency Assessment
that are implemented in the site. RHMT guidelines specify that providers should be trained on a yearly basis. When asked how often trainings were actually conducted, RHMT members said it varied based on the specialty of the provider. The guidelines for the CHMT specified that health workers in the district receive continuous training on a quarterly basis. When asked how often trainings actually take place, all five CHMT members interviewed said trainings took place on a quarterly basis. However, when site managers were asked how often providers in their facility received training, the responses were varied. One site manager said providers received training on a yearly basis, another said quarterly, two site managers responded that there was no regular interval for trainings to be conducted, and another site manager said trainings occur twice a year. When providers were asked if they had received training within the past 12 months, 80% (12/15) of the health workers said yes. Although the frequencies for trainings seem to vary, it is clear that most providers are receiving some type of training annually.
The process for selecting providers to receive training appears to vary. The RHMT and CHMT both noted that various actors can be responsible for selecting providers to be trained including: RHMT, CHMT, supervisor, facility in-charge, medical officer in-charge, matron, and the NGO conducting the training. According to the site manager interviews, the majority responded that the CHMT is in charge of selecting providers for trainings (5/6); one manager did not know how providers were chosen for trainings. When health workers were asked who is responsible for choosing providers for trainings, 20% (3/15) said they didn’t know, 27% (4/15) said the CHMT is responsible , 20% (3/15) said the District AIDS Control Coordinator, 27% (4/15) said it depended on the training, and 7% (1/15) said the District Medical Officer was responsible.
When health workers were asked who selects providers for trainings, 20% said they didn’t know, 27% said the CHMT, 20% said the District AIDS Control Coordinator, 27% said it is based on the training, and 6% said the District Medical Officer. While a large percentage of health workers had received training within the past year, 80% did not feel that they received adequate training on a regular basis. As shown in Figure 10, the top areas in which providers felt they were lacking included CD4 tests, ART, PMTCT, TB/HIV co-infection management, and management of sexually transmitted infections. It should be noted that the areas with higher number of responses all have to do with HIV/AIDS care. In order for providers to offer a high quality of care, it is essential that they receive ongoing training to ensure they have the skills, knowledge and capacity required.
Figure 10: Areas in which health workers feel they need more training (n=19)*
11%
16% 16%
5%
11%
5% 5%
11%
5% 5% 5% 5%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
PMTCT CD4 tests ARVs VCT STI Malaria FP TB/HIV QI Database Mgmt
Pediatric AIDS
Refresher on CTC services
*Health workers could have more than one response

Tanzania HIV Provider Productivity and Efficiency Assessment • 15
3. Supervision and feedback Supervision is an integral piece of improving human resource management systems and worker productivity. Supportive supervision can also help an employee to feel more engaged by knowing there is someone who can help resolve any issues they may be facing in their work and who can provide constructive feedback on their performance. As mentioned above, both the RHMT and CHMTs are responsible for conducting supervision visits. Management team members interviewed have guidelines regarding supervision visits which they were able to produce for the data collectors. According to the guidelines for both the CHMT and RHMT, supervision visits should be conducted on a monthly basis. When asked how often supervision visits were actually conducted, the RHMT responded quarterly while all five CHMT members interviewed said visits were conducted monthly.
Site managers were also asked about supervision at their facility. According to site managers, providers are supervised by more than one individual. When asked who supervises clinical staff, site managers had the following responses: Clinical Officer in-charge (2/6), RHMT/CHMT (4/6), and the District or Regional Aids Control Coordinator (1/6). More than one response was possible for the question. The frequency of supervision visits seems to vary by site, with site managers noting the following frequencies: monthly basis (1/6), quarterly (2/6), daily (2/6), and every two months (1/6). While the frequency may be varied, it appears that the process for supervision has been somewhat standardized. Four out of six site managers said that supervisors use a supervision checklist.
Health workers were also questioned about supervision. Most (93%) of the providers interviewed reported that they do have a supervisor. Many providers have more than one supervisor because they are supervised internally by someone at the facility and externally by the CHMT or RHMT. According to health worker interviews, an array of cadres and management level officials can take on the role of supervisor including: the facility manager, medical officer, clinical officer, nurse/midwife, lab technician, District AIDS Coordinator, matron, CHMT/RHMT, and district nursing officer. Providers interviewed said that during supervision visits, records are examined, work is observed, feedback is given, problems encountered are discussed, and administrative updates are given. Although health workers are being supervised, they do not appear to be receiving feedback about their performance on a regular basis: 7% of providers said they receive feedback once a week, 13% once every two weeks, 20% once a month, and 13% did not respond to the question. About half (47%) of providers responded ‘other,’ which included the following: no feedback given, immediately on specific tasks, every two months, after supervision visits, and during a performance evaluation.
As noted above, according to RHMT and CHMT guidelines, providers should be receiving monthly supervision visits. However, in Figure 11 below, it is apparent that not all providers are receiving monthly visits. When asked the last time they received a supervision visit, 29% of providers said within the last seven days, 29% within the last month, 29% within the last three months, and 14% said they don’t receive supervision visits.
Figure 11: Last supervision visit received (n=14)
14%
29%
29%
29%
0% 5% 10% 15% 20% 25% 30% 35%
No supervision visit
Within the last 3 months
Within the last month
Within the last 7 days

16 • Tanzania HIV Provider Productivity and Efficiency Assessment
G. Performance Evaluation Performance evaluation can offer a means of assessing and appraising the performance of health workers and allowing the provider to know how his performance rates overall. It also offers an opportunity for providers to learn the things that they are doing well and the areas where they need improvement. It can provide a basis for receiving incentives or a promotion. Although a process does exist for conducting appraisals— the RHMT and CHMT members interviewed responded affirmatively when asked whether a process is in place to assess and appraise health workers—it does not seem to be well understood. According to the RHMT, the district is responsible for conducting the appraisals using the Open Performance Review and Appraisal System (OPRAS). However, the RHMT is responsible for overseeing the OPRAS process at all levels in the region. RHMT members are also appraised by the Regional Medical Officer through OPRAS.
Responses about the role of the CHMT in the appraisal process were varied. Two CHMT members said the district human resource officer is responsible for the appraisal; one member said the CHMT was not responsible; and two other CHMT members said that every CHMT member participates in the process in his/her area of expertise. When asked how often performance evaluations are given, the RHMT said once a year, and four of the five CHMT members interviewed said yearly while the fifth CHMT member said no set time-frame exists. When asked how providers felt about performance evaluations, the RHMT said they don’t really understand how OPRAS works but that those who perform feel positively about the process and those that don’t perform feel negative. Three of the five CHMT members interviewed responded that providers feel positive about the process and the other two said providers were neutral about the process.
When site managers were asked if a process for appraising health workers exists, only half (3/6) said yes. During the interviews, one site manager told data collectors that OPRAS is not in place, while another said staff do not know how to set their objectives and fill out the OPRAS form. Of the three site managers that said an appraisal process existed, two said performance evaluations are given yearly, and the third said that no evaluations had been conducted yet. These same site managers were also asked what performance evaluations are based on. All three site managers were unclear on this and gave the following responses: don’t know, done by CHMT, and registers are inspected. Only 27% of the providers interviewed said they had ever received a performance evaluation. Of those that did receive an evaluation, 100% found the process to be fair.
While there is a process in place for appraising the performance of health workers, it does not seem that all levels have been made aware of this process. Additionally, those who are aware of its existence do not seem to clearly understand the process or what evaluations should be based on.
1. Incentives Incentives can offer a way to reward and recognize providers for performing well. They can also help to motivate workers and even help generate a healthy sense of competition among providers if distributed in a fair and transparent manner. RHMT members noted that providers received the following non-financial incentives: verbal recognition, time off, referral for a bank loan, and transportation to town for banking needs. Financial incentives noted by the RHMT include: extra duty allowance, a financial reward for best performance given to health worker for the year, performance based incentive (pay for performance by facility), increased salary upon promotion, and a subsistence allowance. CHMT members interviewed noted the following non-financial incentives are received by providers: verbal recognition, written recognition, time off, clothes, and house-building materials. Financial incentives noted include: general bonus, performance-based incentives, hardship payment, and overtime pay.
When site managers were asked if providers received any financial or non-financial incentives, only four out of six said yes. This is interesting to note because both of the higher levels (RHMT and CHMT) noted that both financial and non-financial incentives were available for health workers in their

Tanzania HIV Provider Productivity and Efficiency Assessment • 17
region/district. Of the four site managers that said incentives were available, the following incentives were noted: verbal recognition (3/4), best health worker awarded on Labor Day (1/4), performance-based incentive given yearly (1/4), and a financial incentive from NGO (CHAI) when CD4s are received from facility (1/4). One site manager mentioned that he had heard about Pay for Performance, an MOH initiative to reward facilities based on performance, but was not aware of the process and how standards were measured. In addition, one site manager said that the facility does not understand how to set objectives. Of the four site managers that said their providers receive some kind of incentive, three felt that the incentives motivated staff to perform well because they raised recognition of what staff members are doing well and encouraged other providers to work harder.
While the CHMT and RHMT noted that both financial and non-financial incentives were available to providers in their region/district, it appears that not all facilities have the means or resources to give out incentives. Only 27% of health workers said they receive non-financial incentives, including verbal recognition. Results of the employee engagement questionnaire, which were discussed above, substantiate this finding and show that recognition systems are ineffective. Providers rated recognition the lowest of all engagement elements at only 2.2 out of 5, indicating that few staff had received recognition from a supervisor in the last seven days.
A quarter (27%) of providers interviewed said they receive financial incentives which included team-based incentives, performance-based incentives, general incentives, and rural/hardship incentives. However, respondents said that these incentives are not given out on a regular basis.
2. Motivation During the health worker interviews, providers were asked if they feel highly motivated to work at their facility. Figure 12 shows the results regarding motivation. The majority of providers (67%) said they felt highly motivated to do their work. Reasons given included: patient appreciation of services, liking the work, opportunities for learning and growing, recognition, incentives, and good relations with colleagues. A third (33%) of providers said they did not feel highly motivated to work at their facility. Reasons given included: work environment, workload, poor living conditions, no incentives, staff shortage, lack of performance evaluation, and problems with transportation for referrals.
Figure 12: Level of staff motivation in facilities (n=15)
Providers were also asked to note the important factors they thought influenced motivation of health workers. Responses were as follows: living and working conditions 20%, incentives 24%, supportive supervision 22%, professional growth/advancement 22%, and ability to influence decision making 11%. As discussed earlier in this report, factors such as professional advancement and ability to influence decision making are among some of the key drivers that influence employee engagement.
33%
67%
Not Highly Motivated
Highly Motivated

18 • Tanzania HIV Provider Productivity and Efficiency Assessment
3. Promotions Offering employees opportunities for professional advancement and growth is important in keeping providers engaged and motivated if the process is fair and transparent. In addition, opportunities for advancement give providers a goal that they can strive towards. Promotions for health workers are possible according to the RHMT and four out of the five CHMT members. Five out of six site managers also said that promotions were possible for providers at their facility. The RHMT and four out of five CHMT members also noted that guidelines regarding promotions exist. When asked how often promotions occur, the RHMT said yearly, two CHMT members said yearly, and two other CHMT members said between three and five years.
When site managers were asked about the process of promotions, the following responses were received: staff members are supposed to be promoted after three years but it’s not done on a regular basis (2/5); staff must obtain professional development before promotion (2/5); and the CHMT recommends those for promotion (1/5). According to the RHMT and CHMT, a number of different actors can make the decision to promote health workers, including: the supervisor, CHMT, human resource office, head of the clinical department, and district and regional employment committees. About half of all health workers interviewed (53%) said that they have opportunities for promotion in their position. The employee engagement questionnaire substantiated this finding: providers scored the availability of professional advancement opportunities at only 4.0 out of 5. While promotions are possible, they do not seem to occur on a frequent or regular basis.
4. Retention Having a high turnover rate can negatively impact facilities and the quality of care they are delivering. Frequent turnover can mean a shortage of staff in facilities that are already understaffed, negatively impact the workload of other providers in the facility, and be costly as new employees need to be trained and acclimated to the processes and working style of that particular facility. In general, both the RHMT and four of the five CHMT members interviewed felt that retention is not a problem in their district. Only two out of six site managers believe that retention is a problem for the HIV clinic. Even though retention does not appear to be a major issue in Mtwara, it is still important to note the reasons that health workers may leave their posts. The RHMT and CHMT noted the following reasons that health workers may leave: remote area, lack of supervision, lack of incentives, bad relations with supervisor, poor living conditions, new positions in parallel programs, further studies, and delay in employment after probationary period. Site managers also noted that a delay in employment after the probationary period causes health workers to leave.
H. Human Resource Management Challenges At the end of the RHMT group interview and the CHMT individual interviews, respondents were asked to note any other HR management challenges. The RHMT members noted the following issues: RHMT members have to work through the human resource office to get things done, promotions are not timely, payment for extra work is not always paid, hardship allowances are not always paid, accommodations for health workers, timeliness of the process of payment to new recruits, working environment, and the RHMT/CHMT should be trained in techniques for retaining health personnel.
CHMTs noted the following HR challenges: staff should be employed in a timely manner, accommodation and meal allowances should be given as early as possible, vacancies should be announced publicly, lack of qualified personnel, staff shortage, the need for planning how to retain health workers, and government should comply with requests for additional health personnel.
Site managers were also asked to share any HR challenges they felt should be noted. Their responses included: shortage of staff, low salaries, lack of training, reduced efficiency in HIV/AIDS services due to integration of services, and personal rights are not known by staff.

Tanzania HIV Provider Productivity and Efficiency Assessment • 19
1. Provider suggestions for improving the workplace At the end of the health worker interviews, providers were asked if they had any suggestions about how their job or working conditions could be improved. The following suggestions were the responses noted most by health workers: more staff, transportation to District Hospital for referrals, incentives, recognition, regular staff meetings, lab equipment, regular trainings/refresher courses, improve working environment, and educate the community about their relationship with health workers.
IV. CONCLUSIONS AND RECOMMENDATIONS The baseline assessment identified several areas where human resource management systems can be improved to strengthen provider efficiency and productivity and improve the quality of HIV/AIDS service delivery.
Written job descriptions: Job descriptions are integral to instituting a strong performance management cycle. They provide a basis for providing feedback, setting performance objectives, and even measuring performance. Without written job descriptions, it is impossible to implement strong performance management. Job descriptions and tasks assignments need to take into account provider perceptions of workload manageability—not only how many patients they are able to see, but how many they are able to provide with a quality service within the time available.
• Recommendation: Written job descriptions should be developed for all health workers to ensure they have clearly aligned tasks and goals. Efforts should also be made to increase health worker awareness of service delivery standards to ensure that, to the greatest extent possible, providers focus not only on throughput and output but also on delivering high quality services.
Performance evaluation: The performance evaluation process OPRAS, introduced by the MOHSW in 2004, is not well understood by site managers and providers. Providers and site managers need to understand the purpose of the evaluations, how performance should be measured, and how to set performance objectives.
• Recommendation: The process for performance evaluation needs to be communicated clearly with lower level facilities. Both supervisors and providers need to understand the process, the purpose of the performance evaluations, and what they should be based on.
• Recommendation: Performance evaluations should be conducted with providers on an annual basis and should offer an opportunity for performance objectives for the upcoming year to be set.
Recognition, rewards, and incentives: Recognition and reward systems can be improved to ensure that health workers get the acknowledgement and praise they deserve when they perform well. If the process is clear, transparent and well understood, incentives can help motivate individuals working in the facilities improve their performance and improve health outcomes for clients. Promotion and career advancement opportunities are somewhat rare, which may affect worker motivation.
• Recommendation: The process for receiving incentives needs to be clarified for health workers and might partially be based on performance. Provider need to be made aware of how their performance will be measured and how incentives are distributed.
Engagement: The majority of employees are moderately engaged, regardless of the type of center or the position they hold, but specific areas of engagement, such as recognition and materials, could be improved.
• Recommendation: To raise levels of engagement, sites should review the employee engagement results and pick two areas where scores were low to improve upon. This should be a joint exercise with both supervisors and staff so that providers feel empowered about being able to

20 • Tanzania HIV Provider Productivity and Efficiency Assessment
make a difference in their work environment. Ideas to improve areas where scores are low, such as recognition, should be tested and implemented. The employee engagement questionnaire should then be re-applied to determine if changes have improved engagement and identify new areas to work on.
Productivity: Productivity appears to vary by day with providers being very productive in the morning when patients arrive, and productivity levels decreasing dramatically in the afternoon when client loads are low. Client flow does not appear to be a huge problem, but is something that should continue to be monitored since client loads can vary dramatically by day. At the same time, several service providers were observed idly waiting for clients, while others were witnessed skipping lunch to attend to client needs.
• Recommendation: Sites should consider conducting task analysis of staff duties to help them assess which staff members are overburdened and where opportunities for task shifting exist.
Continuous training: Health care workers need to have the necessary skills and training to perform their assigned duties. Most of the providers interviewed felt that they had not received adequate training in key clinical areas.
• Recommendation: The CHMT and the sites themselves should ensure that providers are receiving continuous training every six months on areas/topics related to HIV/AIDS care. Site managers should hold a staff meeting to find out areas in which health workers feel they need to build their capacity. In addition, job aids on certain procedures and processes should be posted in facilities to offer health workers an easy reference.
Site staffing levels: Sites commonly experience staffing shortages due to staff absences for trainings, meetings, and leave. Most health workers view increasing the number of staff as the main solution for addressing client flow, efficiency, and engagement issues.
• Recommendation: Sites should consider developing strategies for improving daily staffing plans and creating staffing contingency plans to ensure that all tasks are covered and clients can be served even when some staff members are absent. For example, task shifting might occur on a periodic basis to cover select services when a specific staff member is absent: a nurse could be trained to take on selected clinical tasks when the clinical officer is pulled away or is not present but would resume her routine tasks when the clinical officer is present.
• Recommendation: Efforts should be made to increase provider’s awareness of staffing constraints and galvanize their interest and skills in developing creative solutions to addressing issues at the clinic level.
V. NEXT STEPS Based on the results of the assessment, a set of human resource management interventions was developed into a change package that QI teams from 12 sites in Mtwara are now testing to improve engagement and efficiency at the facility level. The goal of the collaborative is to improve the quality of ART/PMTCT while simultaneously working on improving HR issues at target sites.
Teams began with Improvement Objective 1 (clearly aligned tasks and goals), which will result in more clearly defined roles and responsibilities for all health workers delivering HIV services. QI teams will share lessons learned and best practices during quarterly learning sessions. Upon completion of all seven improvement objectives, the key practices leading to better outcomes will be packaged for national scale-up.

Tanzania HIV Provider Productivity and Efficiency Assessment • 21
VI. REFERENCES Bilame O, Masui L. 2010. Human Resources for Health Context Analysis: Tanzania. April 2010.
Clinton Foundation. 2008. Report on OPRAS baseline study. October 2008.
Dieleman M, Harnmeijer JW. 2006. Improving health worker performance: in search of promising practices. Geneva: World Health Organization. Available at: http://www.kit.nl/net/KIT_Publicaties_output/ShowFile2.aspx?e=1174.
Dussault G, Franceschini MC. 2006. Not enough there, too many here: understanding geographical imbalances in the distribution of the health workforce. Hum Resour Health 4:12-12.
Hongoro C, Normand C. 2006. “Health Workers: Building and Motivating the Workforce.” In Disease Control Priorities in Developing Countries, ed. Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, Jha P, Mills A, Musgrove P. New York: Oxford University Press: 1309-1322.
Schoo A, Stagnitti K, Mercer C, Dunbar J. 2005. A conceptual model for recruitment and retention: Allied health workforce enhancement in Western Victoria, Australia. Australia Rural Health Education Network, Deakin, A.C.T. Rural and Remote Health, 5 (477):1-18.
VII. APPENDIX: DATA COLLECTION TOOLS Site Manager Interview
Health Worker Interview
Council Health Management Team Interview
Regional Health Management Team Interview
Time Utilization Observation
Employee Engagement Questionnaire
Client Flow Assessment Tool

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Site Management Interview A-1
Site Manager Interview The USAID Health Care Improvement Project is conducting a baseline assessment of human resource systems and the productivity and engagement of health workers delivering ART services in the Mtwara Region. Your responses will remain anonymous and confidential. May I proceed with the interview?
1. Do all employees working at this facility have a written job description that clearly defines roles and tasks for their position? Yes No
1a. If yes, can you show me a job description? ______ (mark with an X if job description seen)
1b. Briefly describe how job descriptions are developed and disseminated____________ ____________________________________________________________________ ____________________________________________________________________
1c. Are job descriptions updated regularly? Yes No
(If no, go to question #3)
2. If yes, how often are job descriptions updated?
a. Every six months b. Annually c. Bi-annually d. Other: please specify______________________________________________
3. Do staff ever work more than their scheduled hours? Yes No (If no, go to question #5)
4. If yes, what is the reason(s) staff work more than their scheduled hours? (circle all that apply) a. High number of patients b. Coordination meetings c. Administrative matters d. Other: please specify ________________________________________
5. How often do staff work more than their scheduled hours? a. Once a month b. Once a week c. More than once a week d. Other: please specify_______________________________________
6. Do staff ever work less than their scheduled hours?
Yes No (If no, go to question #8)

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Site Management Interview A-2
7. What are the reasons staff may work less than their scheduled hours? a. Low number of patients b. They worked more than their scheduled hours on another day c. Other: Please specify__________________
8. Are staff at the HIV Clinic frequently absent due to training, scheduled leave or other reasons? Yes No (If no, go to question #11)
9. If yes, on average how many staff absences occur per week? Number _____________
10. Which of the following reason(s) accounts for the majority of staff absences?
a. Vacation leave ______ b. Sick leave ______ c. Maternity leave ______ d. Training ______ e. Other ______ ___________________
11. What is the process for recruiting/filling open positions for health workers a. Vacancies are posted and interviews conducted by site manager b. New staff are assigned to the facility by the CHMT or RHMT c. Other: please specify______________________________________
12. How often are new staff recruited or requested? a. Quarterly b. Yearly c. Biannually d. Other: please specify_________________________________________________
13. How often are staff at this facility reassigned to other facilities? a. Yearly b. Every two years c. Every three years d. Every four years e. Other: please specify_________________________________________________
14. Are new staff given an orientation when they begin work at the facility? Yes No (If no, go to question #16)
15. If yes, please briefly describe the orientation for new employees

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Site Management Interview A-3
16. How often do health workers in your facility receive training? a. Monthly b. Quarterly c. Yearly d. Other: please specify___________________________________________________
17. How are staff members chosen for trainings?
18. How do you assess the training needs for staff members at your facility?
19. How are staff at this facility supervised?
20. Who supervises clinical staff? (circle all that apply) a. Facility Manager b. Medical Officer c. Clinical Officer d. Nurse/Midwife e. RHMT/CHMT f. Other: specify___________________________________________________________
21. How often are staff supervised?
1. Weekly ______ 2. Monthly ______ 3. Quarterly ______ 4. Other: _____________________________
22. Do supervisors use a supervision checklist or form? Yes No
(If no, go to question #23)
22a. If yes, ask to see form_______ (mark with an X if seen) .
23. Aside from salary, do health workers in your district receive any other financial or non-financial incentives? Yes No
(If no, go to question #27)

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Site Management Interview A-4
(If yes, describe and circle all appropriate) Non-financial
a. Verbal recognition b. Written recognition c. Time off d. Other: please specify_____________________________________________
Financial e. General Bonus f. Salary increase g. Hardship payment h. Other: please specify_____________________________________________ i. Performance based incentive (If yes, go to question #24)
24. How often can staff receive performance-based incentives? a. Once a month b. Once every six months c. Once a year d. Other: please specify_________________________________________________________
25. Do you think these incentives motivate staff to perform well? Yes No
26. Why do you feel this way? Briefly explain
27. Is there a process to assess and appraise health workers? Yes No (If no go to question #30) 27a. If yes, can we see an example of a performance evaluation form? _______ (mark with X if form was seen)
28. If yes, how often are performance evaluations given? a. Once a year
b. Once every two years c. No set time-frame for evaluations exists d. Other: please specify ________________________________________________________

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Site Management Interview A-5
29. What are performance evaluations of health workers based on? a. Job descriptions b. Performance goals of health facility c. Health outcome indicators d. Performance objectives e. Other: please specify________________________________________________________
30. Are there any opportunities for staff promotion at this site? Yes No
31. If yes, please describe:
32. Is retention of health workers a problem for the HIV clinic? Yes No
33. If yes, what are some of the reasons retention is a problem? a. Remote area b. Leave for position in the private sector c. Lack of supervision d. Burnout e. Migration to another country f. Lack of professional advancement opportunities g. Other: please specify______________________________________________________
34. Are there any other human resources management challenges at this site you feel should be noted?
Record Review Ask to see the National HIV Care Monthly Report to gather information on the total numbers of clients seen for the months of March, April and May 2010.
Service March April May HIV ART
HIV Non-ART

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Health Worker Interview B-1
Health Worker Interview The USAID Health Care Improvement Project is conducting a baseline assessment of human resource systems and the productivity and engagement of health workers delivering ART services in the Mtwara Region. Your responses will remain anonymous and confidential. May I proceed with the interview? Provider type: 1. Medical Officer ____ 2. Clinical Officer_____ 3. Nurse/ Midwife____ 4. Nurse's Assistant ____ 5.Lab _____ 6. Pharmacist/Dispenser ____ 7. Counselor___ 8. Other _____
Gender: Male____ Female_____
1. What is your role at this HIV Clinic?
2. How long have you been working at this facility? Years_________/Months_____________
3. Do you have a written job description that clearly defines your tasks and responsibilities?
Yes No 3a. If yes, can you show me a copy (mark only when you see the job description)? Yes No
4. Has anyone discussed your job description with you? Yes No If yes, who discussed with you? a. Supervisor b. Facility manager c. MO/CO d. Coworker
e. other
5. How were you recruited as a health worker? (please describe the process and timeline)
6. Did you feel that the recruitment process was reasonable?
Yes No
7. If no, please briefly explain why not:

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Health Worker Interview B-2
8. Have you participated in any training in the past 12 months? Yes No (If no, go to question #10)
9. If yes, please note the theme(s) of the training(s) you attended: Theme of training (circle all that apply)
Duration of training
9a)STI 9b) OI 9c) VCT 9d) PMTCT 9e) ART 9f) Other 1: specify 9g)Other 2: specify
10. Do you know how health workers are selected to attend trainings? (Prompt: By whom? On what basis?)
11. Do you feel that you receive adequate training on a regular basis? Yes No (If yes, go to question #13)
12. If not, in which areas are you lacking?
13. Do absences of your co-workers occur on a regular basis at this facility? Yes No (If no, go to question #15)
14. Which of the following reason(s) accounts for the majority of staff absences? (check all that apply)
a. Vacation ______ b. Sick leave ______ c. Maternity leave ______ d. Training ______ e. Don’t know ______ f. Other (specify) ______ ___________________

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Health Worker Interview B-3
15. Do you ever work more than your scheduled hours?
Yes No
(If no, go to question #18)
16. If yes, what are the reasons? a. High number of patients
b. Coordination meetings c. Administrative matters d. Other: please specify ________________________________________
17. How often do you have to work more than your scheduled hours? a. Once a month b. Once a week c. More than once a week d. Other: please specify______________________________________
18. Do you ever work less than your scheduled hours? Yes No (If no, go to question #20)
19. If yes, what are the reasons? a. Low number of patients
b. Worked more than scheduled hours on another day c. Other: Please specify__________________
20. Do you have a supervisor? Yes No (If no, go to question #24)
21. If yes, who is your supervisor? (circle all that apply)
a. Facility manager b. Medical Officer c. Clinical Officer d. Nurse/Midwife e. Other: specify____________________
22. What happens when you are supervised? (circle all that apply) a. Records are examined b. Work observed c. Feedback given d. Discuss problems encountered e. Administrative updates given f. Other: please specify___________________________________________
23. How often do you receive feedback from your supervisor on your performance? a. Once a week b. Once every two weeks c. Once every three weeks d. Once a month e. Other: please specify____________________________________________

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Health Worker Interview B-4
24. When was the last time you received a supervision visit?
a. Within the past 7 days b. Within the last month c. Within the last 3 months d. I don’t remember e. I never receive supervision visits
25. If you have been working at this facility for at least one year, have you ever received a
performance evaluation? Yes No
(If no, go to question #29)
26. If yes, did you feel that you were evaluated fairly? Yes No
27. Please briefly explain why or why not:
28. Do you have opportunities for promotion in your position? Yes No (If no, go to question #31)
29. If yes, how were you informed about these opportunities?
30. Do you receive any non-financial incentives for working at this facility?
Yes No (If no, go to question #33)
31. If yes, please briefly describe the non-financial incentive:
a. Verbal recognition b. Written recognition c. Free health care/medicines d. Other: please specify_________________________________________________
32. Do you receive any financial incentives in addition to your regular salary?
Yes No` (If no, go to question #39)

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: Health Worker Interview B-5
33. If yes, please explain Describe incentive: 34a. Team-based incentive? Yes/No 34b. Individual? Yes/No 34c. Performance-based? Yes/No 34d. Rural/Hardship? Yes/No 34e. General (for everyone)? Yes/No 34f. How often are incentives given? Quarterly
Every six months Yearly Other (please specify)
34. Do you feel highly motivated to do your work at this facility? Yes No
35. Please explain why you feel this way
36. What are some important factors that you think influence health worker motivation? (read options and circle all that apply)
a. Living and working conditions b. Incentives d. Supportive supervision e. Possibility for professional advancement/growth f. Ability to influence decision-making g. Other: please specify______________________________________________________
37. Do you have any suggestions about how your job or working conditions could be improved?

Site Name: ____________________________ Date: ____________________ ID __________ dd/mm/yyyy
Tanzania HR Baseline Assessment: CHMT Interview C-1
CHMT Interview
Interviewer name: ____________________________________ The USAID Health Care Improvement Project is conducting a baseline assessment of human resource systems and the productivity and engagement of health workers delivering ART services in the Mtwara Region. Your responses will remain anonymous and confidential. May I proceed with the interview? 1. What is the role of the CHMT?
2. How are staffing levels determined in your district?
3. What is the process for recruiting/filling open positions for health workers?
4. How often are new staff recruited/requested?
a. Quarterly b. Yearly c. When a need is identified d. Other: specify__________________________________________________________ 5. What is the level of vacancy in your district for the following cadres: (percentages if possible)
a. Medical Officers_______ b. Clinical Officers_______ c. Nurses/Midwives_______ d. Lab______ e. Counselors_______ f. Other: please specify____________________________________________________ 6. What do you think are some of the main reasons that health workers leave their posts? (circle all
that apply) a. Remote area b. Leave for position in the private sector c. Lack of supervision d. Burnout e. Migration to another country f. Lack of professional advancement opportunities g. Other: please specify______________________________________________________

Site Name: ____________________________ Date: ____________________ ID __________ dd/mm/yyyy
Tanzania HR Baseline Assessment: CHMT Interview C-2
7. Do all health workers in your district have a written job description that clearly defines roles and tasks for that position?
Yes No
a. If yes, can you show me your job description? ________ (mark with an X if job description seen)
b. Briefly describe how job descriptions are developed and disseminated______________________________________________________________ _________________________________________________________________________
c. Are job descriptions updated regularly? Yes No
8. If yes, how often are job descriptions updated?
a. Every six months b. Annually c. Bi-annually d. Other:
specify_______________________________________________________________ 9. Are there guidelines and/or a plan in place that determines how often health workers in your district
receive continuous training? (ask to see the plan or guidelines) Yes No
a. If yes, not the frequency of trainings according to plan_____________________
10. How often are trainings actually conducted in your district? a. Monthly b. Quarterly c. Every six months d. Yearly e. Other: please specify____________________________________
11. Who determines which health workers should participate in trainings?
a. Medical officer b. Supervisor c. RHMT/CHMT d. Facility manager e. Other: please specify____________________________________________________
12. Is staff turnover a problem in your district?
Yes No
13. If yes, please briefly describe

Site Name: ____________________________ Date: ____________________ ID __________ dd/mm/yyyy
Tanzania HR Baseline Assessment: CHMT Interview C-3
14. Are there guidelines that determine how often health workers can be/should be reassigned to different facilities? Yes No
15. If yes, how often are staff reassigned? a. Yearly b. Every two years c. Every three years d. Other: please specify____________________________________________________
16. Do you conduct supervision visits in your district? Yes No 17. Are there supervision guidelines? (Ask to see them) Yes No
a. If yes, note the frequency of supervision according to plan__________________
18. How often are supervision visits usually conducted?
a. Monthly b. Quarterly c. Yearly d. Other: please specify_____________________________________________
19. Is there a process to assess and appraise health workers? (Ask to see form)
Yes No
a. If yes , please briefly describe the CHMT role in the process
20. Aside from salary, do health workers in your district receive any other financial or non-financial
incentives? Yes No
(If yes, describe and circle all appropriate) Non-financial
a. Verbal recognition b. Written recognition c. Time off d. Other: please specify_____________________________________________
Financial e. General Bonus f. Performance-based incentive g. Salary increase h. Hardship payment i. Other: please specify_____________________________________________

Site Name: ____________________________ Date: ____________________ ID __________ dd/mm/yyyy
Tanzania HR Baseline Assessment: CHMT Interview C-4
21. How do health workers feel about the performance evaluation process?
a. Positive b. Neutral c. Negative d. Other: please specify_______________________________________________
22. Are promotions possible for health workers?
Yes No
a. If yes, are there guidelines regarding promotion? Yes No
b. How often do promotions occur? i. Monthly ii. Quarterly iii. Yearly iv. Other: please specify_______________________
23. Who makes the decision to promote health workers?
a. Supervisor b. Facility Manager c. CHMT d. RHMT e. Other: please specify______________________________________________
24. Are health workers aware of how promotions occur? Yes No 25. Are there are any other HR issues which you think should be noted?

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: RHMT Interview D-1
RHMT Interview The USAID Health Care Improvement Project is conducting a baseline assessment of human resource systems and the productivity and engagement of health workers delivering ART services in the Mtwara Region. Your responses will remain anonymous and confidential. May I proceed with the interview? 1. What is the role of the RHMT?
2. How are staffing levels determined in your region?
3. What is the process for recruiting/filling open positions for health workers?
4. How often are new staff recruited/requested?
a. Quarterly b. Yearly c. When a need is identified d. Other: specify__________________________________________________________ 5. What is the level of vacancy in your region for the following cadres: (percentages if possible)
a. Medical Officers_______ b. Clinical Officers_______ c. Nurses/Midwives_______ d. Lab______ e. Counselors_______ f. Other: please specify____________________________________________________ 6. What do you think are some of the main reasons that health workers leave their posts? (circle all
that apply) a. Remote area b. Leave for position in the private sector c. Lack of supervision d. Burnout e. Migration to another country f. Lack of professional advancement opportunities g. Other: please specify______________________________________________________

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: RHMT Interview D-2
7. Do all health workers in your region have a written job description that clearly defines roles and
tasks for that position? Yes No (If no, go to question #9)
7a. If yes, can you show me your job description? ________ (mark with an X if job description seen) 7b. Briefly describe how job descriptions are developed and disseminated _________________________________________________________________
_________________________________________________________________
7c. Are job descriptions updated regularly? Yes No (If no, go to question #9)
8. If yes, how often are job descriptions updated?
a. Every six months b. Annually c. Bi-annually d. Other: specify _______________________________________________________
9. Are there guidelines and/or a plan in place that determines how often health workers in your region
receive continuous training? (ask to see the plan or guidelines) Yes No
9a. If yes, note the frequency of trainings according to plan_____________________
10. How often are trainings actually conducted in your region? a. Monthly b. Quarterly c. Every six months d. Yearly e. Other: please specify____________________________________
11. Who determines which health workers should participate in trainings? (circle all that apply)
a. Medical officer b. Supervisor c. RHMT/CHMT d. Facility manager e. Other: please specify____________________________________________________
12. Is staff turnover a problem in your region? Yes No
(If no, go to question #14) 13. If yes, please briefly describe

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: RHMT Interview D-3
14. Are there guidelines that determine how often health workers can be/should be reassigned to
different facilities? Yes No (If no, go to question #16)
15. If yes, how often are staff reassigned? a. Yearly b. Every two years c. Every three years d. Other: please specify____________________________________________________
16. Do you conduct supervision visits in your region? Yes No 17. Are there supervision guidelines? (Ask to see them) Yes No
17a. If yes, note the frequency of supervision according to plan__________________
18. How often are supervision visits usually conducted?
a. Monthly b. Quarterly c. Yearly d. Other: please specify_____________________________________________
19. Is there a process to assess and appraise health workers? (Ask to see form)
Yes No
(If no, go to question #21)
19a. If yes, please briefly describe the RHMT role in the process
20. How often are performance evaluations given? a. Once a year b. Once every two years c. No set time-frame for evaluations exists d. Other: please specify_______________________________________________

ID ______ Date________________ Interviewer name: _____________ Site #:______ dd/mm/yyyy
Tanzania HR Baseline Assessment: RHMT Interview D-4
21. Aside from salary, do health workers in your region receive any other financial or non-financial incentives? Yes No
(If yes, describe and circle all appropriate) Non-financial
a. Verbal recognition b. Written recognition c. Time off d. Other: please specify_____________________________________________
Financial e. General Bonus f. Performance based incentive g. Salary increase h. Hardship payment i. Other: please specify_____________________________________________
22. How do health workers feel about the performance evaluation process?
a. Positive b. Neutral c. Negative d. Other: please specify_______________________________________________
23. Are promotions possible for health workers?
Yes No (If no, go to question #26)
23a. If yes, are there guidelines regarding promotion? Yes No
23b. How often do promotions occur? i. Monthly ii. Quarterly iii. Yearly iv. Other: please specify_______________________
24. Who makes the decision to promote health workers?
a. Supervisor b. Facility Manager c. CHMT d. RHMT e. Other: please specify______________________________________________
25. Are health workers aware of how promotions occur? Yes No 26. Are there are any other HR issues which you think should be noted?

ID: _______
Tanzania HR Baseline Assessment: Time Utilization Observation Form E-1
Time Utilization Observation Form Health Worker: A
Evaluator Name: ____________________________________ Site : __________________________________________ Cadre: ___________________________________ Date: ____________________________________ (dd/mm/yyyy)
Dire
ct p
atie
nt
care
Indi
rect
Car
e
Out
reac
h
Mee
tings
/ A
dmin
istra
tion
Trai
ning
Cle
anin
g/
prep
arat
ion,
pe
rson
al h
ygie
ne
Wai
ting
for
patie
nts
Bre
aks
Soc
ial v
isits
Une
xpla
ined
A
bsen
ce
Oth
er
Mis
sed
Obs
erva
tion
Hour Min 8 10
25 40 55
9 10 25 40 55
10 10 25 40 55
11 10 25 40 55
12 10 25 40 55
13 10 25 40 55
14 10 25 40 55
15 10 25 40 55
16 10 25 40 55
17 10 25 40 55

ID: _______
Tanzania HR Baseline Assessment: Time Utilization Observation Form E-2
Time Utilization Observation Form Health Worker: B
Evaluator Name: ____________________________________ Site : __________________________________________ Cadre: ___________________________________ Date: ____________________________________ (dd/mm/yyyy)
Dire
ct p
atie
nt
care
Indi
rect
Car
e
Out
reac
h
Mee
tings
/ A
dmin
istra
tion
Trai
ning
Cle
anin
g/
prep
arat
ion,
pe
rson
al h
ygie
ne
Wai
ting
for
patie
nts
Bre
aks
Soc
ial v
isits
Une
xpla
ined
A
bsen
ce
Oth
er
Mis
sed
Obs
erva
tion
Hour Min 8 10
25 40 55
9 10 25 40 55
10 10 25 40 55
11 10 25 40 55
12 10 25 40 55
13 10 25 40 55
14 10 25 40 55
15 10 25 40 55
16 10 25 40 55
17 10 25 40 55

ID: _______
Tanzania HR Baseline Assessment: Time Utilization Observation Form E-3
Time Utilization Observation Form
Health Worker: C Evaluator Name: ____________________________________
Site : __________________________________________ Cadre: ___________________________________ Date: ____________________________________ (dd/mm/yyyy)
Dire
ct p
atie
nt
care
Indi
rect
Car
e
Out
reac
h
Mee
tings
/ A
dmin
istra
tion
Trai
ning
Cle
anin
g/
prep
arat
ion,
pe
rson
al h
ygie
ne
Wai
ting
for
patie
nts
Bre
aks
Soc
ial v
isits
Une
xpla
ined
A
bsen
ce
Oth
er
Mis
sed
Obs
erva
tion
Hour Min 8 10
25 40 55
9 10 25 40 55
10 10 25 40 55
11 10 25 40 55
12 10 25 40 55
13 10 25 40 55
14 10 25 40 55
15 10 25 40 55
16 10 25 40 55
17 10 25 40 55

Site Name: ______________________________ Date: ____________________ ID:_______ Jina la kituo:_____________________________ Tarehe:________________ Utambulisho:_______________
Tanzania HR Baseline Assessment: Employee Engagement Questionnaire F-1
Questionnaire on Employee Engagement
Dodoso kuhusu sababu za ukaaji kazini mfanyakazi
Site Name: _____________________________ Date:_____________________
Jina la Kituo:____________________________ Tarehe:____________________
Provider type: (please check all that apply) CO_____ MO_____ Nurse/Midwife_____ Nurse’s Assistant______
(Weka alama ya vema katika jibu kuhusu) Mganga msaidizi_______ Mganga_________ Nesi/Mkunga______ Nesi msaidizi______
Lab personnel__ Dispenser/Pharmacist_____ Counselor______ Other __ Specify ___________________________
Mfanyakazi wa maabara_____ Mtoa Dawa/Mfamasia______ Mshauri nasaha________ Kada nginyine____ Taja
Instructions for the health worker:
Maelezo kwa mtoa huduma
Please complete this survey by selecting one response for each statement that communicates how much you disagree or you agree with the statement. Please respond honestly thinking about how you feel today about each item.
Tafadhali jaza dodoso kwa kuchagua jibu moja kwa kila sentensi kuhudu kukubali au kukataa. Tafadhali jibu kwa makini unachofikiria kuhusu kila jambo
Choose only one response for each question Chagua jibu moja tu kwa kila swali

Site Name: ______________________________ Date: ____________________ ID:_______ Jina la kituo:_____________________________ Tarehe:________________ Utambulisho:_______________
Tanzania HR Baseline Assessment: Employee Engagement Questionnaire F-2
1. Strongly
Disagree Sikubaliani kabisa
2. Disagree Sikubaliani
3.Neutral Nipo kati. Nakubaliana/Sikubaliani
4. Agree Nakubaliana
5. Strongly Agree Nakubaliana kabisa
1.
I believe that what I do as a health worker is important Ninaamini kuwa ninachokifanya kama mfanyakazi wa afya ni muhimu
1 2 3 4 5
2. I know what is expected of me at work Ninafahamu majukumu yangu kazini 1 2 3 4 5
3. I feel respected at work Ninaheshimika kazini 1 2 3 4 5
4. I have the materials I need to do my job right Nina vitendea kazi nahitaji kufanya kazi kwa ufanisi 1 2 3 4 5
5.
My supervisor or someone at work cares about me as a person Mkuu wangu au mfanyakazi mwenzangu ananithamini mimi kama mtu
1 2 3 4 5
6.
When I face problems at work, I am able to solve them with the help of others. Nikiwa na tatizo kazini, naweza kutatua kwa msaada wa watu wengine
1 2 3 4 5
7.
I have a close friend at work with whom I can share my ideas or problems. Nina rafiki wa karibu kazini, ninayeweza kumshirikisha mawazo au matatizo yangu
1 2 3 4 5
8. At work my opinions seem to count. Mawazo yangu kazini yanatiliwa manani 1 2 3 4 5
9.
My supervisor or someone at work gives me feedback on my work. Mkuu wangu au mfanyakazi mwenzangu ananipa mrejesho wa nyuma kuhusu kazi yangu
1 2 3 4 5

Site Name: ______________________________ Date: ____________________ ID:_______ Jina la kituo:_____________________________ Tarehe:________________ Utambulisho:_______________
Tanzania HR Baseline Assessment: Employee Engagement Questionnaire F-3
1. Strongly
Disagree Sikubaliani kabisa
2. Disagree Sikubaliani
3.Neutral Nipo kati. Nakubaliana/Sikubaliani
4. Agree Nakubaliana
5. Strongly Agree Nakubaliana kabisa
10. I have enough opportunities at my job to grow and develop. Nina nafasi kubwa ya kujiendeleza kazini 1 2 3 4 5
11. There is someone at work that encourages my development. Nina mtu kazini anayenitia moyo kwenye maendeleo yangu 1 2 3 4 5
12.
In the last 7 days I have received recognition or praise for doing good work. Katika kipindi cha siku 7 zilizopita nimetambuliwa au kupongezwa kwa kufanya kazi vizuri
1 2 3 4 5
13.
I believe that I am evaluated based on the quality of my work. Ninaamini kwamba tathimini ninayofanyiwa inatokana na ubora wa kazi ninayofanya
1 2 3 4 5
14.
My colleagues openly listen to my ideas and opinions Wafanyakazi wenzangu wapo wazi kusikia mawazo na ushauri wangu
1 2 3 4 5
15.
I can make meaningful decision about how I do my job. Naweza kufanya maamuzi ya maana/busara kuhusu jinsi ninavyofanya kazi yangu
1 2 3 4 5
16. I am proud to work at this health facility. Ninafurahia kufanya kazi katika kituo hiki cha afya. 1 2 3 4 5

Site: ______________________________ ID: _______
Tanzania HR Baseline Assessment: Client Flow Assessment Tool G-1
Client Flow Assessment Tool
Date : ________ dd/mm/yyyy
Arrival Time: _______:________ 24 hr hour min
Visit Type:
1. Initial Visit __________
2. Pre-ARV __________
3. ARV Initiation __________
4. ARV Follow-up visit ________
5. Refill __________
Cadre Staff
Initials
Time service started
Time service completed
Waiting time (in minutes)
Contact time
(in minutes) Registration ________ ________ _______ _______ _______ _______ Triage ________ ________ _______ _______ _______ _______ Consultation ________ ________ _______ _______ _______ _______ Clinical Assessment ________ ________ _______ _______ _______ _______ Counseling ________ ________ _______ _______ _______ _______
Lab ________ ________ _______ _______ _______ _______
Dispensing ________ ________ _______ _______ _______ _______
PMTCT ________ ________ _______ _______ _______ _______
Other ________ ________ ________ _______ _______ _______
_________________ ________ ________ ________ _______ _______ _______


USAID HEALTH CARE IMPROVEMENT PROJECTUniversity Research Co., LLC
5404 Wisconsin Ave., Suite 800Chevy Chase, MD 20815
Tel: (301) 654-8338Fax: (301) 941-8427www.hciproject.org