Bariatric Surgery
51
BARIATRIC SURGERY BARIATRIC SURGERY from a from a MEDICAL RISK MEDICAL RISK vs vs BENEFIT BENEFIT PERSPECTIVE PERSPECTIVE and
-
Upload
joaquim-c-freire -
Category
Documents
-
view
118 -
download
2
description
Técnicas de cirurgia bariátrica.
Transcript of Bariatric Surgery

BARIATRIC SURGERYBARIATRIC SURGERYfrom afrom a
MEDICAL RISK MEDICAL RISK vsvs BENEFITBENEFITPERSPECTIVEPERSPECTIVE
and
Measuring ObesityMeasuring Obesity
•• Determined by height and Determined by height and weightweight
•• Waist circumferenceWaist circumference•• Body Mass Index (BMI) = Body Mass Index (BMI) =
kg/mkg/m22
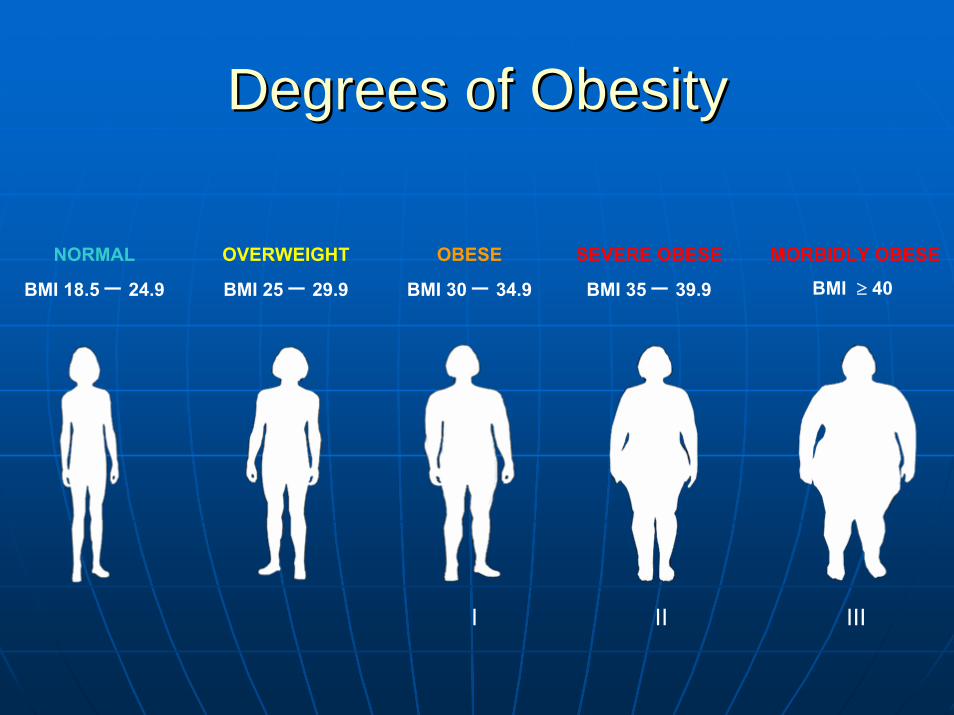
Degrees of Obesity Degrees of Obesity
NORMAL
BMI 18.5 – 24.9
OVERWEIGHT
BMI 25 – 29.9
OBESE
BMI 30 – 34.9
SEVERE OBESE
BMI 35 – 39.9
MORBIDLY OBESE
BMI ≥ 40
I II III
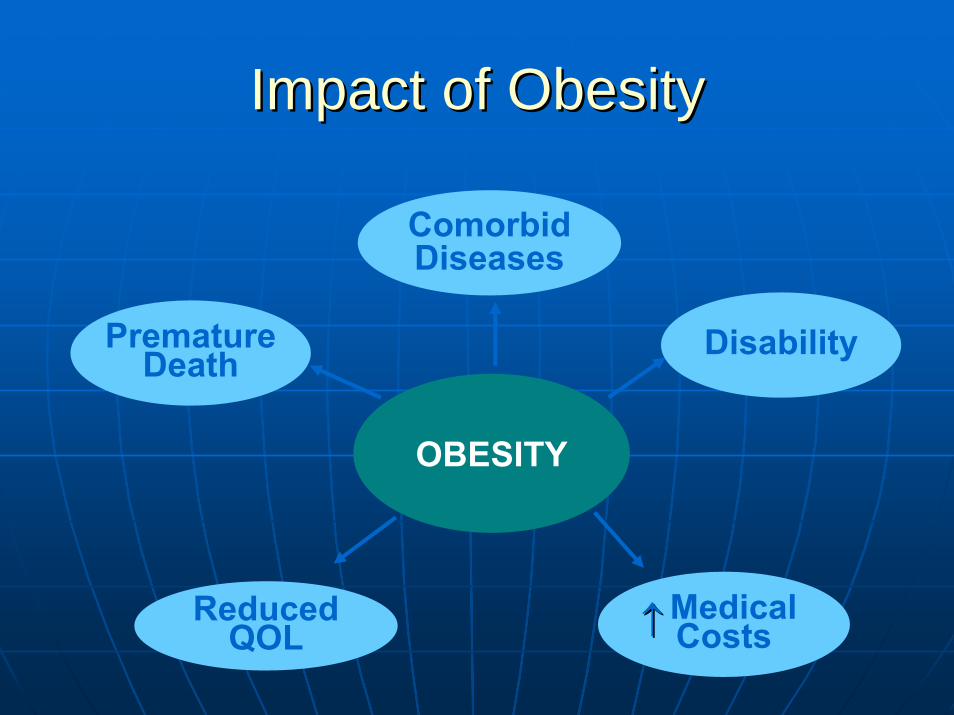
Impact of ObesityImpact of Obesity
MedicalCosts
OBESITY
PrematureDeath
Comorbid Diseases
Disability
Reduced QOL ↑↑

Pulmonary DiseaseAbnormal FunctionObstructive Sleep ApneaHypoventilation Syndrome
Nonalcoholic FattyLiver Disease
SteatosisSteatohepatitisCirrhosis
Coronary Heart DiseaseDiabetesDyslipidemiaHypertension
Gynecologic AbnormalitiesAbnormal MensesInfertilityPolycystic Ovarian Syndrome
Osteoarthritis
Skin
Gall Bladder Disease
CancerBreast, Uterus, Cervix,Colon, Esophagus, Pancreas,Kidney, Prostate
PhlebitisVenous Stasis
Gout
Medical Complications of ObesityMedical Complications of ObesityIdiopathic Intracranial Hypertension
StrokeCataracts
Severe Pancreatitis
1. Obesity OnLine slide presentation. Accessed May 17, 2007. Accessible as slide #5 at http://www.obesityonline.org/slides/slide01.cfm?tk=33.
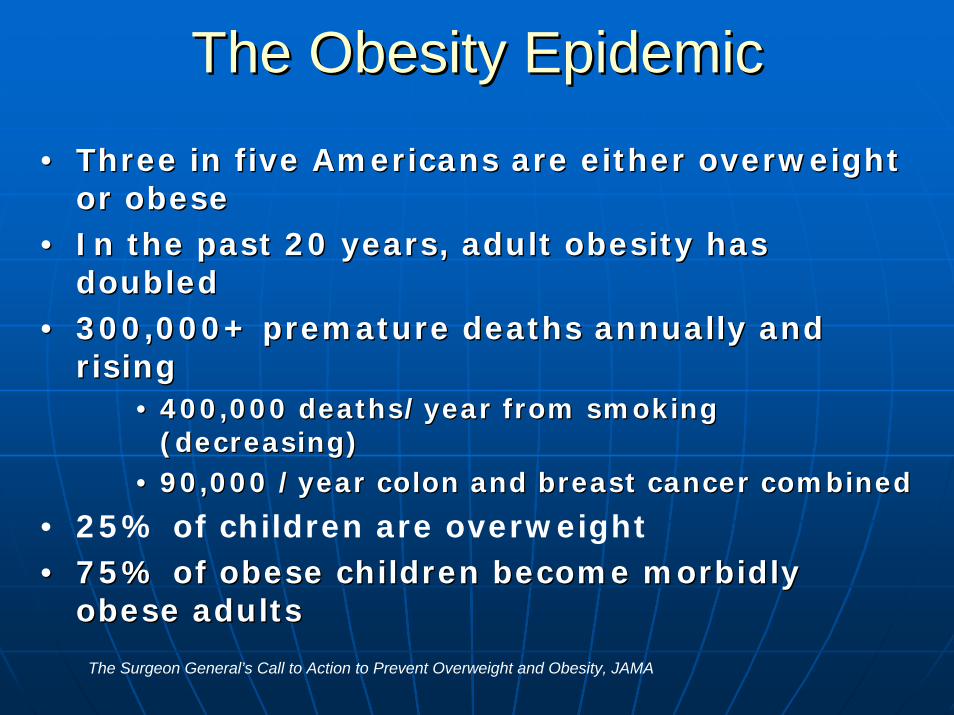
The Obesity EpidemicThe Obesity Epidemic
•• Three in five Americans are either overweight Three in five Americans are either overweight or obeseor obese
•• In the past 20 years, adult obesity has In the past 20 years, adult obesity has doubleddoubled
•• 300,000+ premature deaths annually and 300,000+ premature deaths annually and risingrising
•• 400,000 deaths/year from smoking 400,000 deaths/year from smoking (decreasing)(decreasing)
•• 90,000 /year colon and breast cancer combined90,000 /year colon and breast cancer combined
• 25% of children are overweight•• 75% of obese children become morbidly 75% of obese children become morbidly
obese adultsobese adults
The Surgeon General’s Call to Action to Prevent Overweight and Obesity, JAMA

1991 1995
2000
Obesity* Trends Among U.S. AdultsObesity* Trends Among U.S. Adults(*BMI ≥ 30, or ~ 30 lbs overweight for 5’4” person)
No Data <10% 10%-14% 15-19% ≥20%
Source: BRFSS, CDC.
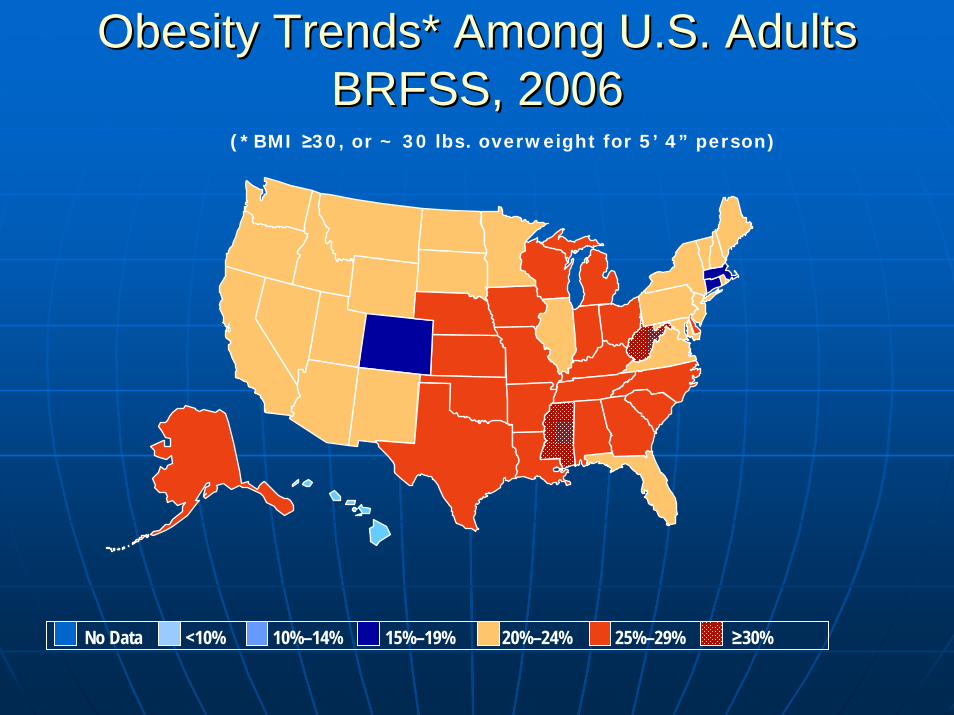
Obesity Trends* Among U.S. AdultsObesity Trends* Among U.S. AdultsBRFSS, 2006BRFSS, 2006
(*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

Lifestyle ChangesLifestyle Changes
•• Current weight loss programs use:Current weight loss programs use:•• DietDiet•• ExerciseExercise•• Behavior therapyBehavior therapy
•• Can be expected to achieve and Can be expected to achieve and maintainmaintain a weight loss of 5 a weight loss of 5 --10 lbs, 10 lbs, if continuedif continued
Source: Tsai AG, Wadden TA. Systematic Review: An Evaluation of Major Commercial Weight Loss Programs in the United States. Ann Intern Med. 2005;142(1):56-66.

Lifestyle ChangesLifestyle Changes
Tsai AG, Wadden TA. Systematic Review: An Evaluation of Major Commercial Weight Loss Programs in the United States. Ann Intern Med. 2005;142(1):56-66.
Evaluation of Major United States Commercial Weight Loss Programs
ProgramProgram Study DesignStudy Design Sample CharacteristicsSample Characteristics DurationDuration
Participants Participants (n)(n)
Mean Initial Mean Initial BMI or WeightBMI or Weight
Women Women (%)(%)
TOPSTOPS Multisite randomized trialMultisite randomized trial 234234 81.9 kg/m81.9 kg/m22 Not Not givengiven 12 weeks12 weeks
Health Management Health Management ResourcesResources
SingleSingle--site randomized trial of site randomized trial of diabetic patientsdiabetic patients 4040 104.7 kg (228 104.7 kg (228
lb)lb) 4848 12 weeks12 weeks
OPTIFASTOPTIFASTMultisite prospective case Multisite prospective case series of consecutive series of consecutive participantsparticipants
517517 38.1 kg/m38.1 kg/m22 7979 26 weeks26 weeks
Weight WatchersWeight Watchers Multisite randomized trialMultisite randomized trial 423423 33.7 kg/m33.7 kg/m22 8585 2 years2 years

Lifestyle ChangesLifestyle Changes
Tsai AG, Wadden TA. Systematic Review: An Evaluation of Major Commercial Weight Loss Programs in the United States. Ann Intern Med. 2005;142(1):56-66.
TreatmentTreatment Weight Change (%)Weight Change (%) Attrition Rate (%)Attrition Rate (%)
MaximumMaximum Long TermLong Term InitialInitial Long TermLong Term
TOPSTOPS
Behavior therapy, therapistBehavior therapy, therapist --2.3 at 12 weeks2.3 at 12 weeks --3.2 at 1 year3.2 at 1 year Not givenNot given 38 at 1 year38 at 1 year
Behavior therapy. TOPS leaderBehavior therapy. TOPS leader --1.0 at 12 weeks1.0 at 12 weeks 0.0 at 1 year0.0 at 1 year Not givenNot given 41 at 1 year41 at 1 year
Health Management ResourcesHealth Management Resources
Very low calorie diet using meal replacementsVery low calorie diet using meal replacements --15.3 at 12 weeks15.3 at 12 weeks --8.4 at 1 year8.4 at 1 year 00 7.5 at 1 year7.5 at 1 year
Very low calorie diet using meal replacements and usual Very low calorie diet using meal replacements and usual foodsfoods --14.1 at 12 weeks14.1 at 12 weeks --8.4 at 1 year8.4 at 1 year 2.52.5 7.5 at 1 year7.5 at 1 year
Weight WatchersWeight Watchers
Weight Watchers, groupWeight Watchers, group 5.3 at 26 weeks5.3 at 26 weeks 3.2 at 2 years3.2 at 2 years 18 at 1 year18 at 1 year 27 at 2 years27 at 2 years
SelfSelf--help with 2 visits and a dietitianhelp with 2 visits and a dietitian 1.5 at 26 weeks1.5 at 26 weeks 0 at 2 years0 at 2 years 18 at 1 year18 at 1 year 27 at 2 years27 at 2 years
Group counseling and a 12Group counseling and a 12--week veryweek very--lowlow--calorie dietcalorie diet --21.8 at 26 weeks21.8 at 26 weeks --9.0 at 1.5 years9.0 at 1.5 years 4545 57 at 1.5 years57 at 1.5 years
Nutrition therapy, TOPS leaderNutrition therapy, TOPS leader --0.1 at 12 weeks0.1 at 12 weeks 1.0 at 1 year1.0 at 1 year Not givenNot given 55 at 1 year55 at 1 year
Usual TOPS programUsual TOPS program 0.4 at 12 weeks0.4 at 12 weeks 1.6 at 1 year1.6 at 1 year Not givenNot given 67 at 1 year67 at 1 year
OPTIFASTOPTIFAST

1991 NIH1991 NIH--RecommendationsRecommendations
•• BMI > 40 are potential candidates for BMI > 40 are potential candidates for surgerysurgery
•• BMI 35BMI 35--40 if they have 40 if they have ““high risk co high risk co morbid conditionsmorbid conditions””•• HypertensionHypertension•• Sleep apneaSleep apnea•• Severe DMSevere DM

OBESITYOBESITY--RELATED MEDICAL PROBLEMS RELATED MEDICAL PROBLEMS RESPONSE TO WEIGHT LOSSRESPONSE TO WEIGHT LOSS
PROBLEMPROBLEM N / %N / % RESOLVEDRESOLVED IMPROVED IMPROVED UNCHANGEDUNCHANGED
HypertensionHypertension 106 (54%)106 (54%) 5555 4545 66ArthritisArthritis 50 (26%)50 (26%) 2222 2525 33HyperlipidemiaHyperlipidemia 35 (18%)35 (18%) 2424 77 44Asthma Asthma 25 (12%)25 (12%) 1414 1010 11DiabetesDiabetes 21 (11%)21 (11%) 1414 7 7 00Angina/CHFAngina/CHF 20 (10%) 11 9 20 (10%) 11 9 00Venous StasisVenous Stasis 7 (4%)7 (4%) 55 22 00Sleep ApneaSleep Apnea 6 (3%) 6 (3%) 66 00 00
TOTALTOTAL 270270 151151 105105 1414
Brolin RE. Results of Obesity Surgery. Brolin RE. Results of Obesity Surgery. GastroenterolGastroenterol ClinClin NA, 1987NA, 1987

Age Age vsvs Incidence of Incidence of Medical ProblemsMedical Problems
AGEAGE PATIENTS PATIENTS N / % WITH N / % WITH MEDICAL PROBLEMSMEDICAL PROBLEMS
<< 35 Yrs.35 Yrs. 7878 32 (41%)32 (41%)36 36 –– 44 Yrs.44 Yrs. 6969 52 (75%)52 (75%)45 45 –– 65 Yrs.65 Yrs. 4848 46 (96%)46 (96%)
TOTALTOTAL 195195 130 (67%)130 (67%)
Brolin RE. Results of Obesity Surgery. Brolin RE. Results of Obesity Surgery. GastroenterolGastroenterol ClinClin NA, 1987NA, 1987
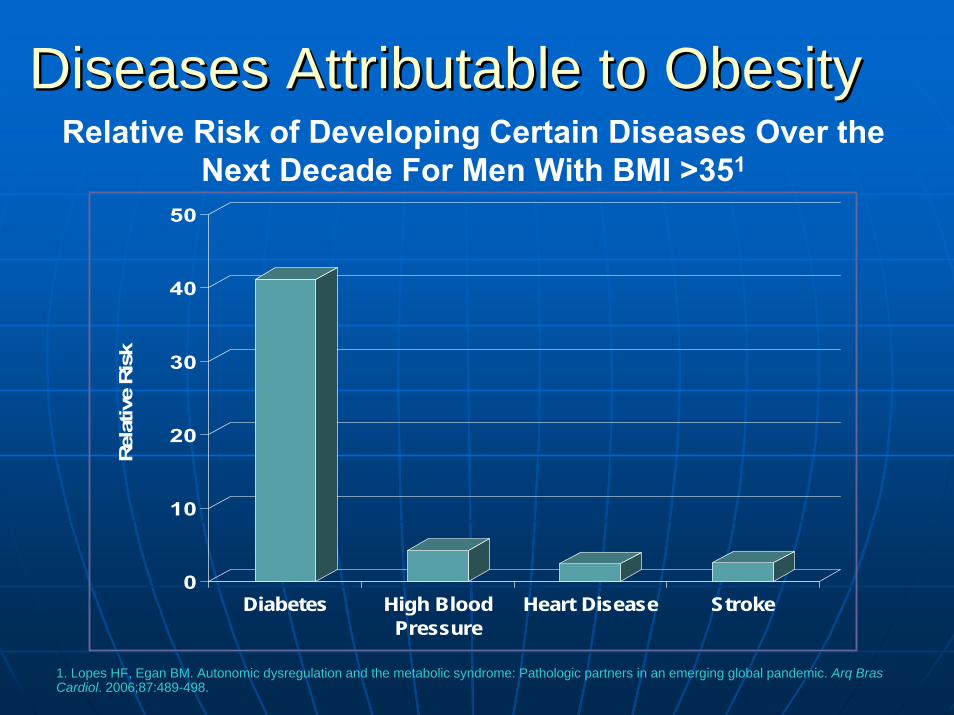
Diseases Attributable to ObesityDiseases Attributable to ObesityRelative Risk of Developing Certain Diseases Over the
Next Decade For Men With BMI >351
0
10
20
30
40
50
Rel
ativ
e Ris
k
Diabetes High BloodPressure
Heart Disease Stroke
1. Lopes HF, Egan BM. Autonomic dysregulation and the metabolic syndrome: Pathologic partners in an emerging global pandemic. Arq Bras Cardiol. 2006;87:489-498.

Relationship Between BMI and Relationship Between BMI and Cardiovascular Disease MortalityCardiovascular Disease Mortality
Cardiovascular
1. Abete P, Cacciatore F, Ferrara N, et al. Body mass index and preinfarction angina in elderly patients with acute myocardial infarction. Am J Clin Nutr. 2003;78:796–801.
In-Hospital Mortality Stratified by BMI1(in patients 65 years or older with pre-infaction angina)
0%
10%
20%
30%
40%
19.0 to 21.9 22.0 to 24.9 25.0 to 26.9 ≥27.0
Body Mass Index
Pere
cent
age
of P
atie
nts Death Death and Cardiogenic Shock

Early mortality among Medicare Early mortality among Medicare Beneficiaries undergoing bariatric Beneficiaries undergoing bariatric
surgical procedures. surgical procedures. FlumFlum DR, et al. JAMA 2005; 294:1903DR, et al. JAMA 2005; 294:1903--19081908
16,155 Patients, 199716,155 Patients, 1997--20022002
CharlsonCharlson ComorbidityComorbidity IndexIndexcalculated for each patientcalculated for each patient
81% had gastric bypass (open)81% had gastric bypass (open)
UPIN used to identify surgeonsUPIN used to identify surgeons
Mean follow up Mean follow up –– 3.4 years3.4 years

BARIATRIC SURGERY in BARIATRIC SURGERY in MEDICARE PATIENTSMEDICARE PATIENTS
3030--DAY GENDER RELATED MORTALITYDAY GENDER RELATED MORTALITYAGEAGE MALESMALES FEMALESFEMALES
**25 25 –– 45 2.1 45 2.1 –– 3.2% 0.8 3.2% 0.8 –– 1.1%1.1%
55 55 –– 6464 2.1%2.1% 2.0%2.0%
*65 *65 –– 7474 5.8% 2.6%5.8% 2.6%
>> 7575 19.6%19.6% 18.8%18.8%
*p < 0.001*p < 0.001
FlumFlum DR, et al. JAMA 2005; 294:1903DR, et al. JAMA 2005; 294:1903--19081908

BARIATRIC SURGERY in BARIATRIC SURGERY in MEDICARE PATIENTS MEDICARE PATIENTS
MORTALITYMORTALITYAGEAGE 1 MONTH1 MONTH 3 MONTHS3 MONTHS 12 MONTHS12 MONTHS
<< 6565 11--2%2% 1.5 1.5 –– 2.7%2.7% 2 2 –– 5.2%5.2%
65 65 –– 7474 3.4%3.4% 4.6%4.6% 7.8%7.8%
>> 7575 19.1%19.1% 30.9%30.9% 44.1%44.1%
Flum DR, et al. JAMA 2005; 294:1903-1908

BARIATRIC SURGERYBARIATRIC SURGERYin MEDICARE PATIENTSin MEDICARE PATIENTS
EFFECT of SURGEON EFFECT of SURGEON EXPERIENCEEXPERIENCE
3030--day mortality 1.6x higher for surgeons with day mortality 1.6x higher for surgeons with less than median number of casesless than median number of cases
9% 9% vsvs 1% mortality with lowest volume quartile 1% mortality with lowest volume quartile vsvs highest volume quartile in patients highest volume quartile in patients >> 65 years 65 years
FlumFlum DR, et al. JAMA 2005; 294:1903DR, et al. JAMA 2005; 294:1903--19081908
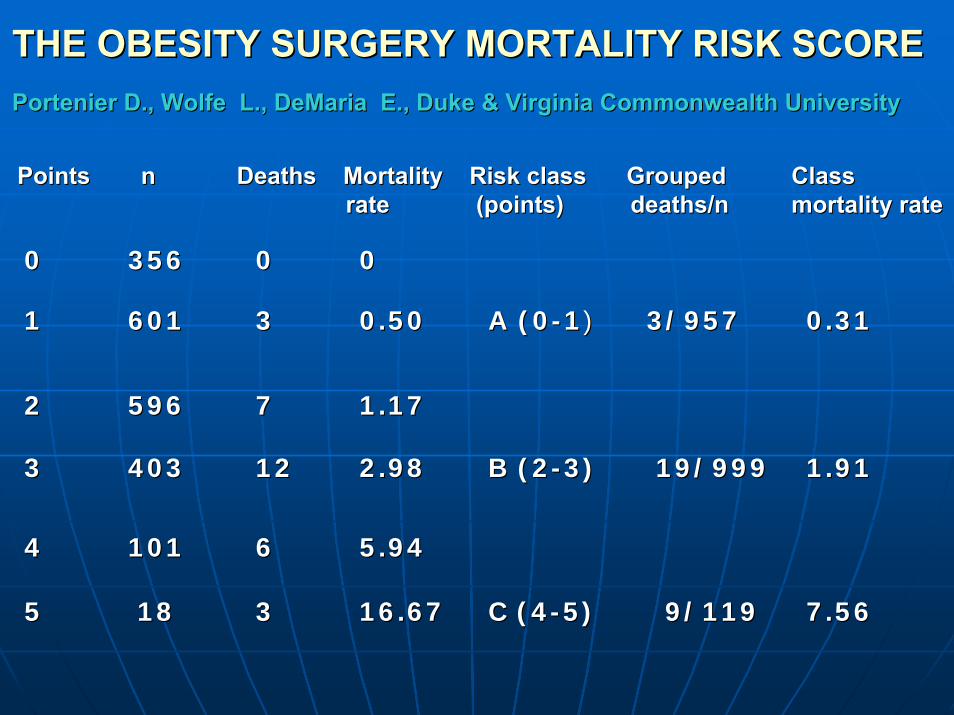
THE OBESITY SURGERY MORTALITY RISK SCORETHE OBESITY SURGERY MORTALITY RISK SCOREPortenierPortenier D., Wolfe L., DeMaria E., Duke & Virginia Commonwealth UniverD., Wolfe L., DeMaria E., Duke & Virginia Commonwealth Universitysity
PointsPoints n n Deaths Mortality Risk class Grouped Deaths Mortality Risk class Grouped ClassClassrate (points) deaths/n rate (points) deaths/n mortality ratemortality rate
00 356356 00 00
11 601601 33 0.500.50 A (0A (0--11)) 3/957 3/957 0.310.31
22 596596 77 1.171.17
33 403403 1212 2.982.98 B (2B (2--3)3) 19/99919/999 1.911.91
44 101101 66 5.945.94
55 1818 33 16.6716.67 C (4C (4--5)5) 9/1199/119 7.567.56

Table VIII. Table VIII. Hospital mortality rates following Hospital mortality rates following common operations in U.S. hospitals July 2006common operations in U.S. hospitals July 2006
AorticAortic Esophageal Hip Esophageal Hip PancreatectomyPancreatectomyaneurysm CABG Craniotomy resection replacementaneurysm CABG Craniotomy resection replacement
# # Hospital 2,485 1,026 1,600Hospital 2,485 1,026 1,600 1,7171,717 3,445 1,3023,445 1,302PerformingPerformingOperationsOperations
National Average 3.9 3.5 10.7National Average 3.9 3.5 10.7 9.1 0.39.1 0.3 8.38.3Mortality Rate (%)Mortality Rate (%)
Average Hospital 30 491 12 5Average Hospital 30 491 12 5 24 824 8Caseloads MedianCaseloads Median
____________________________________________________________________________________________________________________________
CABG, coronary artery bypass grafting.CABG, coronary artery bypass grafting.Adapted from Adapted from DimickDimick JB, Welch HG, JB, Welch HG, BirkmeyerBirkmeyer JD. Surgical mortality as an indicator of hospital quality. JD. Surgical mortality as an indicator of hospital quality. JAMA 2004; 292JAMA 2004; 292--847847--51.51.

RISK OF NOT HAVING RISK OF NOT HAVING BARIATRIC SURGERYBARIATRIC SURGERY
A Washington state group reviewed over A Washington state group reviewed over 66,000 obese patients including 3328 who 66,000 obese patients including 3328 who had bariatric surgery.had bariatric surgery.
Surgical mortality was 1.9% and strongly Surgical mortality was 1.9% and strongly correlated with surgical inexperience.correlated with surgical inexperience.
Risk of death was 33% lower in surgically Risk of death was 33% lower in surgically treated patients.treated patients.
FlumFlum DR, Dellinger EP. J Amer College of DR, Dellinger EP. J Amer College of SurgSurg, 2004, 2004

RISK OF NOT HAVING RISK OF NOT HAVING BARIATRIC SURGERYBARIATRIC SURGERY
A Canadian group reviewed nearly 7000 A Canadian group reviewed nearly 7000 patients hospitalized with severe obesity patients hospitalized with severe obesity over a 15 year period including 1035 who over a 15 year period including 1035 who had bariatric operations.had bariatric operations.
The mortality rate in the surgical group was The mortality rate in the surgical group was 0.68% vs. 6.17% in non surgical patients; 0.68% vs. 6.17% in non surgical patients; a relative risk reduction of 80%!a relative risk reduction of 80%!
Christou, N et al. Annals of Surgery, 2004.Christou, N et al. Annals of Surgery, 2004.

Effects of Bariatric Surgery on mortality in Effects of Bariatric Surgery on mortality in Swedish Obese Subjects.Swedish Obese Subjects.
SjostromSjostrom L, L, NarbroNarbro K, K, SjostromSjostrom CD, et al. NEJM 2007; 357:741CD, et al. NEJM 2007; 357:741--752752
4,0474,047 Obese PatientsObese Patients
2,010 had bariatric surgery2,010 had bariatric surgery
2,037 had 2,037 had nonsurgicalnonsurgical treatmenttreatment
Matched by age, gender, BMIMatched by age, gender, BMI
Mean 10.9 Year Follow UpMean 10.9 Year Follow Up

SWEDISH OBESE SUBJECTSSWEDISH OBESE SUBJECTSSjSjööstrströömm, et al, NEJM, 2007, et al, NEJM, 2007
WEIGHT LOSS RESULTS (10 YR)WEIGHT LOSS RESULTS (10 YR)
NO SURGERYNO SURGERY ++2% change2% change
SURGERYSURGERYGastric Banding (376)Gastric Banding (376) 1414++14%14%VBG (1369)VBG (1369) 1616++11%11%RNY Gastric Bypass(265)RNY Gastric Bypass(265) 2525++11%11%

SWEDISH OBESE SUBJECTSSWEDISH OBESE SUBJECTSSjSjööstrströömm, et al, NEJM, 2007, et al, NEJM, 2007
OVERALL MORTALITY (16 yr)OVERALL MORTALITY (16 yr)
NO SURGERYNO SURGERY (6.3%)(6.3%)SURGERYSURGERY (5.0%)(5.0%)
unadjusted hazard ration = 0.76, p = 0.04unadjusted hazard ration = 0.76, p = 0.04
*adjusted hazard ratio = 0.71, p = 0.01*adjusted hazard ratio = 0.71, p = 0.01
*for age, gender, *for age, gender, cvcv risk factorsrisk factors

LONGLONG--TERM MORTALITY after TERM MORTALITY after GASTRIC BYPASS SURGERY. GASTRIC BYPASS SURGERY.
Adams TD, Adams TD, GressGress RE, Smith SC, et al. RE, Smith SC, et al. NEJM 2007; 57:753NEJM 2007; 57:753--761761
7,925 had RNY gastric bypass7,925 had RNY gastric bypass
*7,925 had no treatment*7,925 had no treatment
Matched by age, gender, BMIMatched by age, gender, BMI
Mean 7.9 year Mean 7.9 year followupfollowup
*Drivers license applications*Drivers license applications

GASTRIC BYPASS MORTALITYGASTRIC BYPASS MORTALITYAdams TD, et al. NEJM, 2007Adams TD, et al. NEJM, 2007
Decreased by 40% in RYGB groupDecreased by 40% in RYGB groupvsvs no surgeryno surgery
37.6 37.6 vsvs 57.1 deaths per 10,000 57.1 deaths per 10,000 person years p<0.001 person years p<0.001
*ALL CAUSE MORTALITY*ALL CAUSE MORTALITY
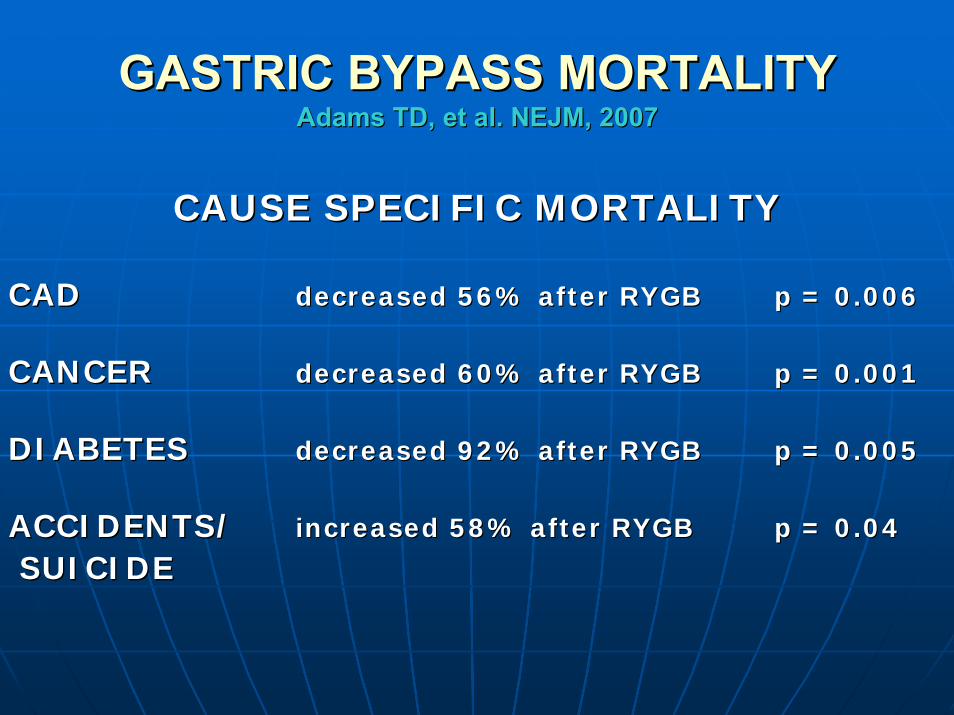
GASTRIC BYPASS MORTALITYGASTRIC BYPASS MORTALITYAdams TD, et al. NEJM, 2007Adams TD, et al. NEJM, 2007
CAUSE SPECIFIC MORTALITYCAUSE SPECIFIC MORTALITY
CADCAD decreased 56% after RYGBdecreased 56% after RYGB p = 0.006p = 0.006
CANCERCANCER decreased 60% after RYGBdecreased 60% after RYGB p = 0.001p = 0.001
DIABETESDIABETES decreased 92% after RYGBdecreased 92% after RYGB p = 0.005p = 0.005
ACCIDENTS/ACCIDENTS/ increased 58% after RYGBincreased 58% after RYGB p = 0.04p = 0.04
SUICIDESUICIDE

RANDOMIZED CONTROLLED TRIAL OF RANDOMIZED CONTROLLED TRIAL OF MEDICAL vs. SURGICAL THERAPYMEDICAL vs. SURGICAL THERAPY
Australian study in which the Australian study in which the LAP BANDLAP BANDwas compared with diet/exercise in was compared with diet/exercise in patients with BMI 30patients with BMI 30--35 kg/m35 kg/m2.2.
After 1 year weight loss diabetes, After 1 year weight loss diabetes, hypertension and sleep apnea were hypertension and sleep apnea were significantly improved in LAP BAND significantly improved in LAP BAND patients vs. minimal/no change in patients vs. minimal/no change in remaining patientsremaining patients

ADJUSTABLE GASTRIC BANDING ADJUSTABLE GASTRIC BANDING and CONVENTIONAL THERAPY for and CONVENTIONAL THERAPY for
TYPE 2 DIABETESTYPE 2 DIABETESA randomized controlled trial. Dixon JB, et al JAMA, 2008.A randomized controlled trial. Dixon JB, et al JAMA, 2008.
60 patients (BMI 3060 patients (BMI 30--40) randomized to 40) randomized to diet/exercise diet/exercise vsvs Lap Band 92% 2 yr. follow upLap Band 92% 2 yr. follow up
Remission of DMRemission of DM 73% with Lap Band73% with Lap Band13% with diet13% with diet
Weight lossWeight loss 21% with Lap Band21% with Lap Band2% with diet2% with diet
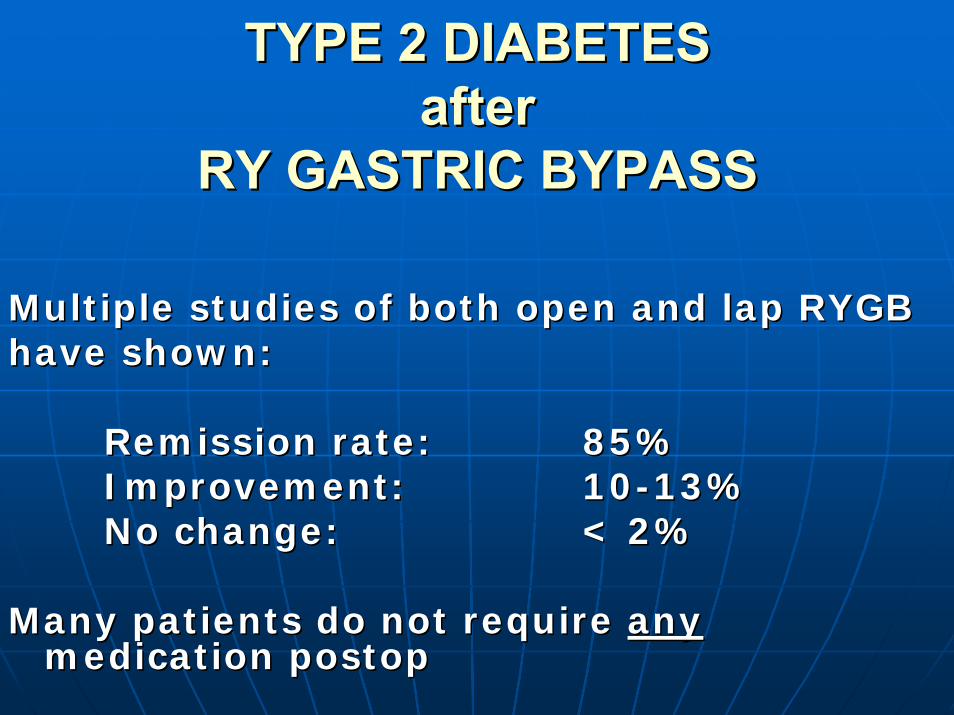
TYPE 2 DIABETES TYPE 2 DIABETES after after
RY GASTRIC BYPASSRY GASTRIC BYPASS
Multiple studies of both open and lap RYGBMultiple studies of both open and lap RYGBhave shown:have shown:
Remission rate:Remission rate: 85%85%Improvement:Improvement: 1010--13%13%No change:No change: < 2%< 2%
Many patients do not require Many patients do not require anyanymedication medication postoppostop
The gastric bypass operation reduces The gastric bypass operation reduces the progression and mortality of NIDDMthe progression and mortality of NIDDM. . MacDonald KG, Jr., et al. J MacDonald KG, Jr., et al. J GastrointestGastrointest Surgery, 1997Surgery, 1997
Retrospective comparison of 232 morbidly obese patients who Retrospective comparison of 232 morbidly obese patients who presented as surgery candidates over a 5 year period. presented as surgery candidates over a 5 year period.
66--9 year follow up.9 year follow up.154 had RY gastric bypass154 had RY gastric bypass78 had medical treatment78 had medical treatment
Comparable age, gender, weight and prevalence of Comparable age, gender, weight and prevalence of hypertensionhypertension
Mortality 28% (22/78) in NonMortality 28% (22/78) in Non--Op GroupOp Group4.5% death rate per year of follow up 4.5% death rate per year of follow up
vs.vs.9% (14/154) in Surgical Group 9% (14/154) in Surgical Group
1.0% death rate per year of follow up1.0% death rate per year of follow up

BMI should be a VITAL BMI should be a VITAL SIGNSIGN
and recorded with other vital and recorded with other vital signs at physician office visitssigns at physician office visitsin acknowledgement of the in acknowledgement of the significant health risks significant health risks associated with obesity.associated with obesity.

Is there another procedure Is there another procedure or intervention or intervention
that can improve that can improve overall health to a greateroverall health to a greaterextent than weight lossextent than weight losssurgery?surgery?
HOW TO RECOGNIZE A HIGHLY HOW TO RECOGNIZE A HIGHLY QUALIFIED BARIATRIC SURGEONQUALIFIED BARIATRIC SURGEON
Number of years in the field.Number of years in the field.Number of bariatric operations performed.Number of bariatric operations performed.Board Certified!Board Certified!Fellow in the American College of Fellow in the American College of Surgeons, F.A.C.S.Surgeons, F.A.C.S.Regular member of the American Society Regular member of the American Society for Bariatric Surgery.for Bariatric Surgery.Center of Excellence.Center of Excellence.

BARIATRIC SURGERY CENTERS BARIATRIC SURGERY CENTERS of EXCELLENCEof EXCELLENCE
Lengthy 2 stage application process Lengthy 2 stage application process followed by site visit.followed by site visit.
Both the individual surgeons and the Both the individual surgeons and the hospital must pass review to receive hospital must pass review to receive designation.designation.

BARIATRIC SURGERY CENTERS BARIATRIC SURGERY CENTERS of EXCELLENCEof EXCELLENCE
Surgeon QualificationsSurgeon QualificationsABS CertificationABS CertificationRegular membership in ASBSRegular membership in ASBSAt least 125 bariatric operations At least 125 bariatric operations
performedperformedCME in bariatric surgeryCME in bariatric surgery
Office staff/facilities focused on bariatric Office staff/facilities focused on bariatric surgery.surgery.

BARIATRIC SURGERY CENTERS BARIATRIC SURGERY CENTERS of EXCELLENCEof EXCELLENCE
Hospital requirements include:Hospital requirements include:Specific credentialing for bariatric surgerySpecific credentialing for bariatric surgeryRegular administrative and educational seminars Regular administrative and educational seminars forfor
nurses and staffnurses and staffLatest technology in OR and XLatest technology in OR and X--ray departmentray departmentTransportation, bedroom and bathroom facilities Transportation, bedroom and bathroom facilities that canthat can
accommodate the morbidly obeseaccommodate the morbidly obese

CENTERS OF CENTERS OF EXCELLENCEEXCELLENCE
Status can be verified on the website of the Status can be verified on the website of the Surgical Review Corporation,Surgical Review Corporation,
www.surgicalreview.orgwww.surgicalreview.org
ProceduresProceduresG
astri
c B
ypas
s
LAP
-BA
ND

Advantages of LaparoscopyAdvantages of Laparoscopy
•• Fewer wound complications Fewer wound complications •• Less herniasLess hernias•• Less pain and faster recoveryLess pain and faster recovery•• Surgeon has better view of the Surgeon has better view of the
anatomy anatomy

Open Surgical ApproachOpen Surgical Approach

Laparoscopic ApproachLaparoscopic Approach

RouxRoux--enen--Y Gastric BypassY Gastric Bypass
•• Restrictive and Restrictive and MalabsorptiveMalabsorptive
•• Most frequently Most frequently performed performed bariatric bariatric procedure in the procedure in the USUS
•• First done in 1967First done in 1967•• Laparoscopically Laparoscopically
since 1993since 1993 ASBS

Gastric BypassGastric BypassAdvantagesAdvantages
Rapid initial weight Rapid initial weight losslossMinimally invasive Minimally invasive approach is possibleapproach is possibleHigher Success rate Higher Success rate than LAPthan LAP--BAND BAND System or VBGSystem or VBGHigher total average Higher total average weight loss reported weight loss reported than with LAPthan with LAP--BAND BAND System or VBGSystem or VBG
DisadvantagesDisadvantagesCutting and stapling of Cutting and stapling of stomach and bowel is stomach and bowel is requiredrequiredMore operative More operative complications than complications than with LAPwith LAP--BAND BAND SystemSystemMalabsorption Malabsorption reportedreportedNonadjustable Nonadjustable Higher mortality rate Higher mortality rate than LAPthan LAP--BAND BAND System or VBG System or VBG proceduresprocedures

Laparoscopic Adjustable Gastric Laparoscopic Adjustable Gastric BandingBanding
•• RestrictiveRestrictive•• Good results in Good results in
Europe and AustraliaEurope and Australia•• FDA approved 6/01FDA approved 6/01•• US results inferior to US results inferior to
European, but European, but improvingimproving

The LAPThe LAP--BAND SystemBAND SystemAdvantagesAdvantages
Least invasive approachLeast invasive approachNo stomach stapling or No stomach stapling or cutting, or intestinal cutting, or intestinal reroutingreroutingAdjustableAdjustableReversibleReversibleLowest operative Lowest operative complication ratecomplication rateLowest mortality rateLowest mortality rateLow malnutrition riskLow malnutrition risk
DisadvantagesDisadvantagesSlower initial weight Slower initial weight loss than gastric loss than gastric bypassbypassLess weight loss Less weight loss than gastric bypassthan gastric bypassHigher Failure than Higher Failure than Gastric bypassGastric bypassRegular followRegular follow--up up critical for optimal critical for optimal resultsresultsRequires a medical Requires a medical implantimplant

Nutritional ConsiderationsNutritional Considerations•• Post operatively, your stomach is approximately Post operatively, your stomach is approximately
the size of an eggthe size of an egg•• Rules to follow after surgery:Rules to follow after surgery:
•• Do not eat if you are not hungry, however you must Do not eat if you are not hungry, however you must continue to drink no calorie liquids throughout the day.continue to drink no calorie liquids throughout the day.
•• Do not eat and drink at the same time. Wait to drink Do not eat and drink at the same time. Wait to drink liquids 45 liquids 45 ––60 minutes after eating.60 minutes after eating.
•• Stop eating when you are full to avoid overeating.Stop eating when you are full to avoid overeating.•• Eat slowly and chew foods thoroughly. At least 20 Eat slowly and chew foods thoroughly. At least 20
chews per bite.chews per bite.•• Drink only no or low calorie liquids. Drink only no or low calorie liquids. •• Drink enough fluids during the day (at least 48 ounces). Drink enough fluids during the day (at least 48 ounces).
•• Take your daily vitamin, calcium and protein Take your daily vitamin, calcium and protein supplements.supplements.
•• Bake, broil, boil, or steam foods instead of frying Bake, broil, boil, or steam foods instead of frying to cut down on empty calories.to cut down on empty calories.

BariatricBariatric Operations Performed at Operations Performed at UMCPUMCP
Total numberTotal number 835 Operations835 OperationsMortalityMortality 5 (0.5%)5 (0.5%)Major complicationsMajor complications 45 (5.4%)45 (5.4%)Minor complicationsMinor complications 11 (1.3%)11 (1.3%)ALOSALOS 3.1 days3.1 days