Barbara DiPietro Director of Policy Thursday, February 12, 2015 EVOLVING OPPORTUNITIES IN MEDICAID...
42
Barbara DiPietro Director of Policy Thursday, February 12, 2015 EVOLVING OPPORTUNITIES IN MEDICAID TO FINANCE AND DELIVER CARE FOR HOMELESS PATIENTS
Transcript of Barbara DiPietro Director of Policy Thursday, February 12, 2015 EVOLVING OPPORTUNITIES IN MEDICAID...

Barbara DiPietroDirector of Policy
Thursday, February 12, 2015
EVOLVING OPPORTUNITIES IN MEDICAID TO FINANCE AND
DELIVER CARE FOR HOMELESS PATIENTS

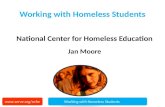
Note: Medicaid includes CHIP and other public Coverage.Sources: HRSA, 2013 National Homeless Data, Table 4: Selected Patient Characteristics; Health Resources and Services Administration, 2013 National Health Center Data; and U.S. Census Bureau, Current Population Survey Data, 2013.
THE HOMELESS POPULATION HAD SIGNIFICANTLY HIGHER UNINSURED RATES COMPARED TO OTHER GROUPS PRE-ACA
Health Insurance Coverage for Health Care for the Homeless Patients Compared to Other Groups, 2013:

• High rates of chronic and acute disease, often coupled with significant behavioral health conditions
• Need for intensive case management and care coordination• Frequent use of emergency departments and inpatient
hospitalizations→ Both “appropriate” and “avoidable”→ Staff- and resource-intensive→ Solutions typically outside hospital control
• High hospital re-admission rates and longer lengths of stay, poorer outcomes
• Few safe and appropriate discharge options• Difficulty fulfilling follow-up care plans/referrals/community care
POOR HEALTH & HIGH SERVICE NEEDS

1. Eligibility, outreach and enrollment2. Access to services3. Delivery of care4. Medicaid’s impact to administration and finance
• Opportunities to maximize moving forward• Challenges to address
• Highly dependent on state decisions, local capacity & partnerships
AREAS OF GREATEST CHANGE

• Outreach conducted through a broad range of venues
→ To include hospital EDs
• Clients generally eager to enroll and access services
• Nearly all homeless clients eligible for Medicaid at sites in expansion states
• Individuals needed substantial assistance to (re)enroll
• Clients unsure how to use new benefit and access health services
OUTREACH AND ENROLLMENT EXPERIENCES

Source: data reported by National Health Care for the Homeless study sites, 2014.

• Improved access to care• Broader benefits
→ Improved ability to work and regain housing→ Less stress and worry over medical bills→ Greater ability to access disability documentation
• Feeling empowered to manage health and participate in care decisions
• Those in non-expansion state continued to face gaps in care and experience poor health outcomes
IMPACTS OF COVERAGE GAINS FOR HOMELESS CLIENTS

• Wider treatment options are available→ Less reliance on inconsistent, ad hoc pro bono arrangements
• Increases in third-party payments help stability
• New revenue facilitates long-term strategic & operational improvements
• Better ability to increase and/or shift staff
• Other funding sources (beyond Medicaid) remain vital
IMPACTS OF COVERAGE GAINS FOR PROVIDERS (TO INCLUDE HOSPITALS)

• Support services, trusting relationships, and care coordination are key
• Important to incorporate social determinants of health (e.g., housing, poverty, hunger, etc.) into health care models
• Most individuals are staying with providers who have experience serving this population (or where they have relationships, such as specific hospitals)
• Broader system changes need to address the poor health and significant needs of this population
• Homeless provider sites have good internal data-sharing, but face gaps sharing data with external providers (hospitals specifically!)
ACCESS TO AND DELIVERY OF CARE FOR THE HOMELESS POPULATION

• Auto-enrollment into plans and providers
• Narrow or changing provider networks (includes changing hospital affiliations/partnerships)
• Prior authorizations and changing drug formularies (delays access)
• Credentialing of providers
• Lack of experience among managed care plans in serving this population (hospitals can help facilitate discussions/initiatives)
EMERGING CHALLENGES WITH MANAGED CARE

• Clients willing to enroll, happy to have benefits, and more engaged in outreach
• Consumers are spreading the word, leading to additional people initiating enrollment
• Able to access services at the point of enrollment (especially if presumptive eligibility status granted)
• Seeing visible improvements in outward appearance, increased trust, looking better, have more hope
LOOKING AHEAD: ENROLLMENT WORKER PERSPECTIVES ON
OPPORTUNITIES

• Changing enrollment systems and new requirements create confusion for frontline workers
• Need for phone numbers and email addresses are barriers to client engagement and communication
• Loss of Year 2 funding and added hours of training create shortages in enrollment workforce
• Potential for coverage losses at redetermination
LOOKING AHEAD:ENROLLMENT WORKER PERSPECTIVES ON
CHALLENGES

• Better access to comprehensive care→ Preventive services
→ Specialty care
• Increased availability of medications→ Medications for asthma, Hepatitis C, arthritis, diabetes
→ Wider choices of medications available to prescribe
• Patients have greater control over their health
• Potential for improved health outcomes over the long-term
LOOKING AHEAD:CLINICAL PERSPECTIVES ON OPPORTUNITIES

• Lack of housing is still the biggest clinical problem• Lack of reimbursement for key services
→ Case management, outreach, dental
• Changing formularies and need for prior authorizations in managed care plans create delays in access
• Changing networks disconnect providers and clients from familiar relationships
• Lack of access to integrated data systems inhibits care transitions• Providers still learning how to navigate the insurance landscape
LOOKING AHEAD:CLINICAL PERSPECTIVES ON CHALLENGES

• Increased revenue allows growth in infrastructure and staff positions
• Better data availability will yield better understanding of population/individual health needs and costs of care
• Potential to establish risk-stratified reimbursement based on specific population & appropriate outcomes
• Opportunity to build a system of integrated services (network) needed to effectively impact health of homeless populations
LOOKING AHEAD:ADMINISTRATOR PERSPECTIVES ON
OPPORTUNITIES

• Ongoing need for grant-based funding• Managed care requires multiple provider contracts, significant
investment in infrastructure, and increased compliance requirements
• Data is fragmented and remains in silos• Increased demand for services stretches provider capacity and
creates recruitment and retention issues• Initial cost of care will likely be high as clients access needed care,
but eventually costs will come down
LOOKING AHEAD:ADMINISTRATOR PERSPECTIVES ON
CHALLENGES

• Barbara DiPietro, Director of Policy, National HCH Council
[email protected] or @barbaradipietro
• Kaiser Family Foundation: Early Impacts of the Medicaid Expansion for the Homeless Population (November 2014)
Available at: http://kff.org/uninsured/issue-brief/early-impacts-of-the-medicaid-expansion-for-the-homeless-population/
Webinar: http://kff.org/medicaid/event/web-briefing-early-impacts-of-the-medicaid-expansion-for-the-homeless-population/
• Other Medicaid and health-reform materials: http://www.nhchc.org/policy-advocacy/reform/nhchc-health-reform-materials/
CONTACT & RESOURCES

FINANCING OPPORTUNITIES AND CHALLENGES: IMPROVING CARE FOR PATIENTS EXPERIENCING HOMELESSNESS
Carol Wilkins

We know what is needed
Housing is a social determinant of health Rx= make housing available as quickly as
possible Offer people with complex health and social problems
the support they need to get and keep housing Multi-disciplinary services for health, behavioral
health, and support for housing stability Frequent, face to face contact to engage people, build
trust and motivate change Focus the most expensive housing and services
on people who really need these interventions Use data and assessment tools to prioritize based on
vulnerability and/or cost and potential for savings

More than 30% of individuals in homeless shelters nationwide in 2013 over age 50
32% increase in number of homeless persons between 51-61 between 2007 and 2013
Growing number of older homeless adults

$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
Low
est
Deci
le
Seco
nd D
eci
le
Th
ird D
eci
le
Fo
urt
h D
eci
le
Fift
h D
eci
le
Six
th D
eci
le
Seve
nth
De
cile
Eig
hth
De
cile
Nin
th D
eci
le
Hig
hest
Deci
le
Probation
Sheriff mental healthjail
Sheriff medical jail
Sheriff general jail
LAHSA homelessservices
GR HousingVouchers
General Relief
Food Stamps
Paramedics
Public Health
Mental Health
Private hospitals-ER
Health Srv - ER
Health Srvoutpatient clinic
Private hospitals-inpatient
Health Srv hospital-inpatient
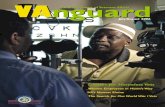
Source: 2,907 homeless GR recipients in LA County with Department of Health Services ER or inpatient records.
Reported in:
Monthly costs of $6,529 Annual cost: $78,348
10% of Highest-Cost Homeless People Were Extremely Expensive
Average Monthly Costs in All Months by Decile for Homeless GR Recipients
Hospitals: $3,452 per month annual cost: $41,424
More with jail medical & mental health.
Crisis Indicator: Triage Tool for Identifying Homeless Adults in Crisis. Economic Roundtable. 2011.
Where We Sleep: Costs when Homeless and Housed in Los Angeles. Economic Roundtable. 2009.
EconomicRoundtable

Housing First + Supports = a better use of health care resources
Fewer hospitalizations, emergency room visits, stays in detox, residential treatment, or nursing homes
Savings in other systems – ambulance, shelters and jails
People are more likely to get recommended care if they are in housing
Substance use declines even if not a condition of housing
Reduced mortality
Savings Better care and outcomes

Reducing the avoidable costs of homelessness Seattle: median per person costs for services
used by chronically homeless people with severe alcohol problems $4,066 per month when homeless $1,492 after 6 months in housing $958 after 12 months in housing
Chicago: homeless hospital patients randomly assigned to housing and case management $6,307 average annual savings per person compared
to usual care. Lower costs for: Hospitalizations ($6,786) Emergency room visits ($704) Residential substance use treatment ($897) Nursing home days ($895)

How can Medicaid and other resources in health care system pay for effective care – including the SUPPORT that helps people get and keep housing?
How can we pay for the care homeless patients need?

Medicaid’s role in supportive housing for chronically homeless peopleHHS Office of the Assistant Secretary for Planning and Evaluation (ASPE) Medicaid and Permanent Supportive Housing for Chronically Homeless Individuals: Emerging Practices from the Field (2014)A Primer on Using Medicaid for People Experiencing Chronic Homelessness and Tenants in Permanent Supportive Housing (2014)Literature Synthesis and Environmental Scan (2011)Four papers published by HHS/ASPE in 2012

Major changes in financing for services Expansion of Medicaid eligibility – in some
states - to include nearly all homeless people States make policy decisions about Medicaid
benefit design and implementation Increasing role of Medicaid managed care Changes in health care finance and delivery
systems impacts for both chronically homeless people
and health care providers who serve them

Medicaid and solutions to homelessness Medicaid is a partnership between state and
federal government with shared costs States make choices about benefit design,
optional benefits and waiver requests Medicaid services can help people get and
keep housing Some Medicaid services can be provided in
supportive housing Other Medicaid services can help meet the
needs of people who are homeless or supportive housing tenants

Medicaid managed care
Enrollment in Medicaid managed care is rising People newly eligible for Medicaid Seniors and people with disabilities (SSI) Needs and risks for groups newly enrolled in
health plans are very different from children and their parents
Plan and provider selection Many homeless people are auto-assigned if they
do not choose a plan and provider Big implications for clinics and health care
providers that serve homeless people – and for partnerships to link services to housing

A mix of payment mechanisms for service providers Shifting from paying for volume to paying from
value Fee for service
Usually for encounters or minutes of service Sometimes for a bundle of services (per episode,
day, or month) Capitation
Per member per month payment for a defined set of services
Sometimes with financial incentives for controlling utilization & costs (shared risk / savings) and quality
Grants and contracts for programs May pay for costs not covered by Medicaid
reimbursement

Medicaid for services in supportive housing – collaborations with hospitals and health plans Capitation creates incentives for hospitals and
health plans to coordinate care and pay for services that reduce avoidable costs But uncertainty about how spending for new types
of services will be reflected in future rate-setting Medicaid managed care plans in some states
are paying for services in supportive housing Care coordination delivered face to face by trusted
service providers Diversionary services to reduce avoidable
hospitalizations by providing community support Case management services linked to housing
assistance for homeless plan members Some hospitals paying for medical respite /
recuperative care and intensive case management for frequent users

Medicaid for services in supportive housing – current practices Most often Medicaid is covering mental health
services connected to supportive housing To be eligible, a person must have a serious mental
illness Some Federally Qualified Health Centers (FQHC)
also provide services in supportive housing Payment for visits with doctors (including
psychiatrist), mid-level practitioners (NP, PA), LCSW Integrated primary care and behavioral health
services Often partnerships use both Medicaid payment
models Funding from federal, state, county, local sources
is needed to cover what Medicaid doesn’t pay for

FQHC services linked to housing Satellite clinics in supportive housing buildings Clinic located close to supportive / affordable
housing Home visits to people living in scattered site
housing Collaborations with mental health service
providers to create interdisciplinary teams linked to housing
Health Care for the Homeless programs can continue to serve homeless people after they move into supportive housing

Challenges and gaps
Costs for some members of inter-disciplinary teams are not reimbursed in FQHC rates set under federal and state policies Nurses do not provide billable encounters Case management costs may not be included in rates
Productivity concerns Fewer visits per day when working outside of clinics
States may limit reimbursement for same-day visits Managed care:
Difficult to get reimbursed if people enrolled in and assigned to other primary care providers
PMPM rates not adjusted to reflect acuity / complexity of needs Provider networks may not facilitate continuity of care
Some FQHCs have not adapted service delivery approach to meet needs of people experiencing chronic homelessness May have limited capacity for serving people with serious
mental health or substance use disorders

Financing for mental health services Optional Medicaid benefits can cover mental
health services Eligibility often limited to people with serious
mental illness Services delivered in a range of community settings With supervision by clinicians, services can be
delivered by teams with peers, workers with other skills and training Rehabilitative services Targeted case management Home and community-based services
Effective service strategies support recovery by doing “whatever it takes” Flexible funding from grants, states, or local
government pays for services not covered by Medicaid

Community Support Teams and ACT covered by Medicaid in some states Teams are mobile and interdisciplinary
Assertive engagement, individualized and flexible approach
Frequent home visits, face-to-face contact in range of settings
Small caseloads For persons with serious mental illness who meet
additional criteria: Recent and/or multiple hospitalizations, ED visits,
contacts with law enforcement Inability to participate or remain engaged in less
intensive services; inability to sustain involvement in needed services
Inability to meet basic survival needs, homeless Co-occurring mental illness and substance use
disorder Lack of support systems

Challenges and gaps
Fragmented and inconsistent approaches to covering services for medical, mental health, and substance use disorders In most states Medicaid benefits cover limited array of
services to address substance use – only in approved settings, making it hard to deliver integrated services for co-occurring disorders
Covered mental health services and goals usually must be related to diagnosis, symptoms and impairments related to mental illness – not (directly) related to substance use problems or other health needs
Provider requirements often not designed for mobile, team-based models of service or shared electronic records
These are state policy decisions – not federal requirements

Challenges and gaps (continued) Federal rules make distinction between
“rehabilitative” and “habilitative” services Some skills people need to get and keep housing
may not be covered As people recover, they may lose eligibility for
ongoing support from intensive mental health service models Other less intensive services may not be mobile
with capacity to do “whatever it takes” It can be hard to return to more intensive services
during a crisis that could lead to losing housing Responsibility for mental health services may shift
to managed care plans Changes may disrupt trusting relationships

What’s working?
Outreach teams assess homeless people who are not engaged in the mental health system and can determine eligibility for services
States and counties understand mobile, team models and provide training for Medicaid reimbursement with focus on services in supportive housing and other settings outside of clinics
Partnerships use flexible funding to create integrated teams linking behavioral health and primary care services
Mental health providers help consumers navigate managed care enrollment, provider selection, access to care
Medicaid managed care plans contract with behavioral health providers for risk assessment and care management

Some counties with public hospitals are investing in supportive housing as health care Housing for most vulnerable and high cost
homeless people reduces avoidable hospital costs and improves health Evidence of savings justifies health system investment
Hennepin Health funds housing navigators Facilitate housing referrals for patients with high costs
and/or health conditions impacted by homelessness Los Angeles DHS Housing for Health program
County health department pays nonprofit partners for case management and housing-related services
Linked to housing developed with city funding and vouchers administered by housing authorities
Public-private partnership funds Flexible Housing Subsidy Pool
Permanent and interim / respite housing options

Medicaid for services in supportive housing – more options for state policy Home and community-based services
(HCBS) for people with disabilities Medicaid can pay for housing locators and
other housing-related services and supports Health homes – an optional Medicaid
benefit For people with multiple chronic health
conditions and/or serious mental illness Whole-person, comprehensive and
individualized case management More than a medical home

What changes are needed to finance what works? Payment mechanisms and rules create incentives
(and remove obstacles) for teams that integrate care for health, mental health and substance use needs
Medicaid coverage for services in settings outside treatment programs to address harmful substance use, and motivate people to make changes to reduce risks
Payments to health plans and providers are adjusted to reflect risk and complexity of consumer needs Taking social determinants of health into consideration Allowing reinvestment of savings to pay for services that
help reduce avoidable costs For vulnerable people with complex needs, services to
support housing stability are recognized as essential part of health care and care coordination Cost are incorporated into rate-setting