
Bacteriophage Therapy
6
Scientists and clinicians currently working in medical microbiology will have spent most of their working lives attempting to address the issue of antibiotic resistance. It is not a new phenomenon and yet it is an issue that seems to have reached a certain defining moment in time. This is partly because the level of bacterial resistance has reached alarming proportions, but also because the subject has attracted profound media attention and, at the same time, the pharmaceutical industry has backed away from research and development of new antibiotics. So, as the problem marches relentlessly onwards, we do not have the assurance that new drugs for the treatment of multiresistant infection lie just around the corner. The expectant public (and, consequently, politicians) are therefore looking for answers and there is clearly a need to explore alternative avenues to reduce our reliance on antibiotics. Here, I will focus on the possibilities offered by the use of bacteriophages to treat bacterial infections. It is outside the scope of this article to discuss the subject of antibiotic resistance in detail. We are all aware of the extent to which certain bacteria have acquired multiple resistance to antibiotics, and, while media attention has focused on methicillin-resistant Staphylococcus aureus (MRSA), it could be argued that the problems posed by Acinetobacter baumanii and Clostridium difficile are far more acute. It has been suggested that one of the reasons for the emergence of resistance in the West is inappropriate prescribing (partly driven by public demand). Steps are now being taken to address this but antibiotic resistance is a worldwide problem and while we may slow the spread the trend will not be reversed. In the past, the pharmaceutical industry has provided a constant stream of new classes of antibiotics to help stem the tide of resistance development. However, the US Food and Drug Administration (FDA) recently showed that of the nine antibacterial agents approved by it since 1998 only two had novel mechanisms of action. While ‘me too’ drugs have their value, the battle against antibiotic resistance can only make major strides with the discovery of new chemical classes of drugs. In its study, the FDA looked at the 15 largest pharmaceutical companies to see what products were currently in development. Of 303 new molecular entities currently undergoing research and development (R&D), only five were new antibacterials and none had novel mechanisms of action. Given the long lead-in times for new drugs we cannot expect any new antibiotics in the near future. The reasons for this loss of interest in antibiotic research are entirely understandable. The cost of bringing a new chemical entity to the market place has been estimated to be somewhere between $400 and $800 million, and the process takes about eight years, from phase I clinical trials to product launch. When a new antibiotic is launched, the medical profession quite rightly adopts a cautious approach and often keeps the drug in reserve. Coupled with the fact that, by definition, antibiotics cure the disease they are treating, the pharmaceutical industry has limited opportunities for recouping its R&D outlay before resistance almost inevitably occurs, or patents expire. Bacteriophage therapy A once and future solution? THE BIOMEDICAL SCIENTIST October 2005 1048 Fig 1. Bacteriophages exhibi t a variety of different morphologic al forms. A R T I C L E At a recent conference on infection control, hosted by microbiology expert Oxoid, Professor Geoff Hanlon described bacteriophages and explained the role they could play in treating bacterial infection. Professor Hanlon ’s talk prompted many questions from the audience and became the hot topic of the conference. Here, he expands on a fascinating subject. pp1048-1052 BMSOct05 16/9/05 10:55 AM Page 1
-
Upload
mario-fernandes -
Category
Documents
-
view
231 -
download
0
Transcript of Bacteriophage Therapy

8/3/2019 Bacteriophage Therapy
http://slidepdf.com/reader/full/bacteriophage-therapy 1/5
Scientists and clinicians currently
working in medical microbiology will
have spent most of their working lives
attempting to address the issue of
antibiotic resistance. It is not a new
phenomenon and yet it is an issue that
seems to have reached a certain defining
moment in time. This is partly because
the level of bacterial resistance has
reached alarming proportions, but also
because the subject has attracted
profound media attention and, at the
same time, the pharmaceutical industry
has backed away from research and
development of new antibiotics.So, as the problem marches relentlessly
onwards, we do not have the assurance thatnew drugs for the treatment of multiresistantinfection lie just around the corner. Theexpectant public (and, consequently,politicians) are therefore looking for answersand there is clearly a need to explorealternative avenues to reduce our reliance onantibiotics. Here, I will focus on thepossibilities offered by the use ofbacteriophages to treat bacterial infections.
It is outside the scope of this article todiscuss the subject of antibiotic resistance indetail. We are all aware of the extent to
which certain bacteria have acquired multiple
resistance to antibiotics, and, while mediaattention has focused on methicillin-resistant Staphylococcus aureus (MRSA), it could beargued that the problems posedby Acinetobacter baumanii and Clostridium
difficile are far more acute.It has been suggested that one of the
reasons for the emergence of resistance inthe West is inappropriate prescribing (partly driven by public demand). Steps are now being taken to address this but antibioticresistance is a worldwide problem and while
we may slow the spread the trend will not bereversed.
In the past, the pharmaceutical industry
has provided a constant stream of new classes of antibiotics to help stem the tide ofresistance development. However, the USFood and Drug Administration (FDA)recently showed that of the nineantibacterial agents approved by it since1998 only two had novel mechanisms ofaction. While ‘me too’ drugs have their
value, the battle against antibiotic resistancecan only make major strides with thediscovery of new chemical classes of drugs.
In its study, the FDA looked at the 15 largestpharmaceutical companies to see whatproducts were currently in development. Of
303 new molecular entities currently undergoing research and development (R&D),only five were new antibacterials and none hadnovel mechanisms of action. Given the long
lead-in times for new drugs we cannot expectany new antibiotics in the near future.
The reasons for this loss of interest inantibiotic research are entirely understandable.The cost of bringing a new chemical entity tothe market place has been estimated to besomewhere between $400 and $800 million,and the process takes about eight years, fromphase I clinical trials to product launch. Whena new antibiotic is launched, the medicalprofession quite rightly adopts a cautiousapproach and often keeps the drug in reserve.Coupled with the fact that, by definition,antibiotics cure the disease they are treating,
the pharmaceutical industry has limitedopportunities for recouping its R&D outlay before resistance almost inevitably occurs, orpatents expire.
Bacteriophage therapy A once and future solution?
THE BIOMEDICAL SCIENTIST October 20051048
Fig 1. Bacteriophages exhibit a variety of different morphological forms.
A R TICLE
At a recent conference on infection control, hosted by microbiology expert
Oxoid, Professor Geoff Hanlon described bacteriophages and explained
the role they could play in treating bacterial infection. Professor Hanlon’s
talk prompted many questions from the audience and became the hot
topic of the conference. Here, he expands on a fascinating subject.
pp1048-1052 BMSOct05 16/9/05 10:55 AM Page 1
8/3/2019 Bacteriophage Therapy
http://slidepdf.com/reader/full/bacteriophage-therapy 2/5
No wonder then that companies are diverting
their resources to the development of products
for the long-term treatment of the burgeoning
elderly population, such as antihypertensives,
lipid-lowering drugs, antidepressants and anti-
dementia drugs. In order to bring industry back
onboard, changes are necessary at the highest
level, perhaps to provide tax incentives for
antibiotic research, to extend the patent life for
new antibiotics, or possibly to introduce fast-track drug approval procedures for new
antibacterial agents.
Alternatives to antibiotics Although much has been said about the end
of the antibiotic era, it is fairly certain that
these agents will be with us for some time to
come and will continue to be the frontline
approach for the treatment of bacterial
infections. However, we need to take the
pressure off them and reduce our reliance
on them as the only option available. To this
end, a variety of alternative strategies are
being explored and some, including
photodynamic disinfection, essential oil
therapy and treatment with bacteriophages,are showing promise. The remainder of this
article will examine the potential of
bacteriophage therapy as a possible adjunct
to antibiotic treatment of bacterial infections.
Characteristics of bacteriophagesBacteriophages (phages) are viruses that only
kill bacteria. Indeed, they are highly specific
and each phage will only attack one species
or even a single strain of bacterium. They are
the most abundant life form on earth,
outnumbering bacteria by a factor of 10,
and have been isolated from many different
habitats. There are a variety of different
morphological types contained within 12
families and their genome may comprise
single- or double-stranded DNA (ss-DNA,
ds-DNA) or RNA (Fig 1). Of course, they have
co-evolved with bacteria over the last 3-4
billion years and so have developed similar
abilities to adapt to changing environments.
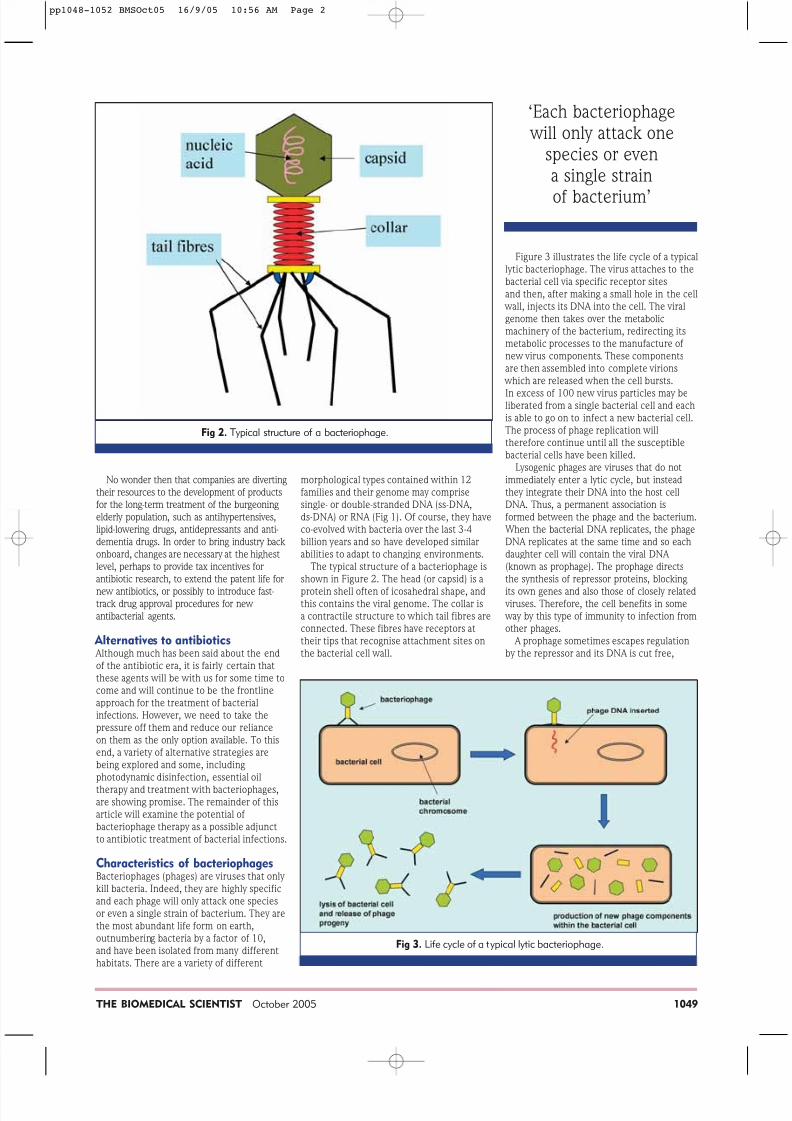
The typical structure of a bacteriophage is
shown in Figure 2. The head (or capsid) is a
protein shell often of icosahedral shape, andthis contains the viral genome. The collar is
a contractile structure to which tail fibres are
connected. These fibres have receptors at
their tips that recognise attachment sites on
the bacterial cell wall.
Figure 3 illustrates the life cycle of a typical
lytic bacteriophage. The virus attaches to the
bacterial cell via specific receptor sites
and then, after making a small hole in the cell
wall, injects its DNA into the cell. The viral
genome then takes over the metabolic
machinery of the bacterium, redirecting its
metabolic processes to the manufacture of
new virus components. These components
are then assembled into complete virions
which are released when the cell bursts.
In excess of 100 new virus particles may beliberated from a single bacterial cell and each
is able to go on to infect a new bacterial cell.
The process of phage replication will
therefore continue until all the susceptible
bacterial cells have been killed.
Lysogenic phages are viruses that do not
immediately enter a lytic cycle, but instead
they integrate their DNA into the host cell
DNA. Thus, a permanent association is
formed between the phage and the bacterium.
When the bacterial DNA replicates, the phage
DNA replicates at the same time and so each
daughter cell will contain the viral DNA
(known as prophage). The prophage directs
the synthesis of repressor proteins, blocking
its own genes and also those of closely related viruses. Therefore, the cell benefits in some
way by this type of immunity to infection from
other phages.
A prophage sometimes escapes regulation
by the repressor and its DNA is cut free,
THE BIOMEDICAL SCIENTIST October 2005 1049
Fig 2. Typical structure of a bacteriophage.
Fig 3. Life cycle of a typical lytic bacteriophage.
‘Each bacteriophage will only attack one
species or evena single strain
of bacterium’
pp1048-1052 BMSOct05 16/9/05 10:56 AM Page 2

8/3/2019 Bacteriophage Therapy
http://slidepdf.com/reader/full/bacteriophage-therapy 3/5
allowing it to embark on a lytic cycle.However, mistakes are often made when theprophage DNA is cut free and bacterial genesmay be incorporated in the viral DNA andthen transferred to the next viral host cell.This process is known as transduction and isresponsible for the horizontal transference of
genes from one bacterial cell to another.Lysogenic phages are not useful for therapy and will not be considered further.
History of bacteriophagesThe concept of using phages in antibacterialtherapy is not new. In 1896 Ernest Hankinobserved that the Ganges and Jumna rivers inIndia seemed to possess antibacterialproperties, and he surmised that this mightin some way be responsible for the reducednumber of cases of gastrointestinal infection,particularly cholera, in those villages close tothe river.
It was not until 1915 that Frederick Twort,an English army officer, suggested that this
antibacterial activity might be due to a virus.Twort did not pursue his ideas and it was leftto Felix d’Herelle to continue this work. Henamed the viruses bacteriophages (bacteriaeaters) and quickly realised their potential forthe treatment of bacterial infections. In 1919he was working in Paris, treating patients with dysentery, and his first patient was a15-year-old boy. D’Herelle obtained thephages from contaminated stool samples andpurified them. To test that they were safe hetook a dose of the phage preparation himself.The following day, having suffered no illeffects, he gave the boy a single draft of thepreparation. The boy recovered rapidly andd’Herelle went on to treat other cases in the
ward.Needless to say, this generated
considerable interest, coming as it did adecade before the discovery of penicillin,and in an age when contracting a bacterialinfection was highly likely to lead to death. About this time, d’Herelle began working with Giorgi Eliava, who was from Tblisi inGeorgia in the then USSR. Eliava wasconvinced of the importance of phagetherapy and decided to set up a researchinstitute in his home country.
The Eliava Institute became, and remainstoday, a world centre for research intobacteriophage therapy. Unfortunately, Eliavafell foul of the authorities, was arrested and
executed in 1937 as an enemy of the people.There is a suggestion that his friendship withthe wife of the local KGB chief may have ledto his undoing.
Following his initial success, d’Herelle went on to study the potential of phagetherapy in a range of bacterial diseases andtreated patients with typhoid and paratyphoidfevers, cholera, wound infections and urinary tract infections. Other researchers becameinterested and pharmaceutical companiesstarted manufacturing bacteriophagepreparations. There was a huge expansion ofresearch papers in the area but unfortunately there were also many failures, which were
due mainly to the fact that those working inthe area had little or no understanding ofbasic phage biology.
In 1931 the Council on Pharmacy andChemistry of the American Medical Association published a damning report which cast doubt on the value of phagetherapy. It was at about this time thatantibiotics came to the fore and phagetherapy was quietly forgotten, at least in the West. However, phage therapy proliferated inthe USSR and other Eastern bloc countriessuch as Poland.
The failure of phage therapy in those early days was almost inevitable and was the result
of high expectations on the part of the publicand poor knowledge of the science behindphage replication. Indeed, it was thought atone time that only a single type ofbacteriophage attacked all bacterial cells.The exquisite specificity of phages was notappreciated, nor the difference between lyticand lysogenic viruses. The methods used toprepare the phages were crude and oftenpatients were dosed with products containingno viable phage but large amounts ofendotoxin. Patients were also poorly diagnosed and this led to treatment withinappropriate phage products.
This situation has, of course, changed and we now know a great deal about the biology
of bacteriophages, which have beeninstrumental in improving our understandingof molecular genetics and basic cell biology.Methods for their isolation and purificationare highly refined and preparations can now meet the exacting standards required ofpharmaceutical products. These facts,together with our current knowledge ofeffective clinical trials design, means that weare well placed to revisit some past work andevaluate the true potential of phage therapy.
While the West began its love affair withantibiotics the USSR embraced phagetherapy, which became part of normalhealthcare. The Eliava Institute grew tobecome a research establishment and a major
manufacturer of phage products. At its peak,it employed 1200 people and tons of phageproducts were manufactured daily andexported throughout the USSR, being usedboth for therapy and prophylaxis. A majoruser of phage products was the military, which routinely included these preparationsin first aid kits.
Therefore, there is a wealth of expertise inthe former USSR on the application ofbacteriophages in the treatment of bacterialinfections. However, much of the work hasbeen published in rather obscure journals,often written in Georgian or Ukrainian, andhence is rather inaccessible. In addition, the
quality of the scientific work would not meetthe rigorous standards applied in the West,particularly in areas such as clinical trials.
Bacteriophage preparationsThe Eliava Institute currently produces arange of phage preparations in a variety ofpharmaceutical forms. They can beadministered topically, orally, rectally, by inhalation or by injection. The purified phagemay be a single clone active against onebacterial species or a mixture of phages thatcan be used against a broad range ofpathogens.
An example of a monoclonal preparation is
a single staphylococcal bacteriophage activeagainst 80–95% S. aureus strains, includingMRSA. This product can be used for localand generalised infections, sepsis in thenewborn, osteomyelitis, pneumonia etc. A phage mixture that can be used for thetreatment and prophylaxis of purulent wound infections is a preparation calledPyophage. This contains bacteriophagesactive against staphylococci, streptococci, Pseudomonas aeruginosa, Proteus speciesand Escherichia coli . This is used in surgery (both pre- and post-operatively), burn wounds, osteomyelitis, skin infections andeye and ear infections. For the treatment ofgastrointestinal infections there is an
11-component mixture active against sixdifferent Salmonella species, and a 17-component cocktail effective against a broadrange of intestinal pathogens.
The advantages afforded by bacteriophage over conventional antibiotictreatment are as follows:• They kill only harmful pathogens and the
normal gut microflora are not affected.• They are effective against antibiotic-
resistant bacteria. As they act in acompletely different way to antibiotics,the presence of resistance determinantsis irrelevant.
• The pharmacokinetics of therapy is quitedifferent from that of antibiotics.
After administration, the number ofbacteriophages increases and continues todo so until all the susceptible bacteria aredead. Often there is no need to give arepeat dose.
• Clinical experience suggests there arefew side effects or allergic reactions. We have grown up surrounded by bacteriophages and so we do not reactto them.
•They are cheap and easy to produce. As bacteriophages are abundant in theenvironment, it is a relatively simple task to obtain and purify new ones whennecessary.
‘Patients have travelled from the West to Tblisi in Georgia in order to obtain
phage therapy not available elsewhere'
1050 THE BIOMEDICAL SCIENTIST October 2005
pp1048-1052 BMSOct05 16/9/05 10:57 AM Page 3

8/3/2019 Bacteriophage Therapy
http://slidepdf.com/reader/full/bacteriophage-therapy 4/5
Clinical studies
During the Second World War, phages wereused by the troops of the USSR for the
treatment of wound infections, particularly
gangrene. Studies showed that the mortality
in phage-treated soldiers was less than 20%,
whereas those in the control groups had
mortality rates in excess of 50%.
A major trial was conducted in the 1960s
on the prophylactic use of phages against
dysentery in children in Georgia. A town was
divided in two along the main street and
children on one side were given phages while
those on the other were given a placebo. A
total of 30,769 children between the ages of
6 months and seven years were included in
the trial: 17,044 were given Shigella phage
orally once every seven days, while 13,725received placebo in place of the phage. Both
groups were visited once a week and faecal
samples from those children with
gastrointestinal disorders were examined
microbiologically. The trial lasted for 109
days. Outcome was based on clinical
diagnosis and it was found that the incidence
of dysentery was 3.8 times higher in the
placebo group than in the phage treated
group.
Phage therapy was also used widely in
Poland and a large amount of clinical data was
summarised recently. Over a period of time
during the 1980s a total of 550 patients
(aged from one week to 86 years) were
treated at 10 different hospitals. Of thesepatients, 518 had previously been treated
unsuccessfully with antibiotics. Their
conditions ranged from wound infections,
respiratory tract infections, peritonitis and
bacteraemia, and the pathogens included
staphylococci, Klebsiella spp., Pseudomonas
spp., E. coli and Salmonella spp.
The phages were obtained from a culture
collection of bacteriophages and treatment
involved 10 mL suspension by mouth, half an
hour before meals (after gastric acid
neutralisation), or topically using phage-
soaked dressings. The success rate, defined
by complete recovery and negative cultures,
was reported as 75–100% (94% overall)
depending upon the pathogen.
A clinical study was published comparing
the effect of bacteriophages and antibiotics
in the treatment of salmonella infections.
Using both symptomatic and microbiological
criteria, the phage-treated group generally
responded more quickly than the antibioticgroup and the infections resolved more
quickly (Table 1). Unfortunately, although
this provides interesting information on the
potential of phage therapy, the trial was not
well designed and vital information was
lacking.
There have been examples of patients
from the West travelling to Tblisi in order to
obtain phage therapy not available
elsewhere. One celebrated example was
Fred Bledsoe from the USA who contracted
an MRSA infection in his foot after stepping
on a nail. Despite 10 weeks’ intravenous
antibiotic treatment, he was told the
condition was incurable and amputation of
the leg was scheduled. Relatives heard of the work being conducted in Georgia and they
arranged for him to travel to the Eliava
Institute for treatment. For two weeks he
was given phage solutions and powders on
the infected wounds and tests after three
weeks revealed the bacteria had been
eradicated and the wounds healed. He has
now completely recovered.
A number of scientists in the West have
been impressed by the results from the
former USSR but were aware that anecdotal
evidence and poorly conducted experiments
would not convince the regulatory
authorities to allow its use here. Thus, it
was necessary to begin to assemble a
substantial body of hard scientific evidence
proving the value of this form of therapy.
In the early 1980s, Smith and Huggins
conducted a series of studies on the
bacteriophage treatment of animals
artificially infected with a pathogenic strain
of E. coli . When a group of mice wereinjected intramuscularly with a dose of
106 colony forming units of the bacterial
pathogen they all died. However, concurrent
treatment with 104 phage specifically lytic
against this strain of E. coli resulted in
survival of all the animals. Interestingly, the
phages used in the experiment were
selective for the K1 capsule antigen on the
bacterial host; thus, any resistant bacterial
strains that emerged had no capsule and
were therefore much less virulent.
A parallel study compared the efficacy of
phages in this system with a range of
antibiotics. The only one that gave
comparable results was streptomycin, and
that required multiple dosing. Tetracycline,ampicillin, chloramphenicol and
trimethoprim/sulphafurazole all gave inferior
results. Further studies on diarrhoeal disease
in calves reinforced these laboratory studies.
More recently, Soothill carried out a
series of experiments using bacteriophages
to prevent graft rejection in burn wounds.
A guinea-pig model was used in which a
wound was artificially infected with either
P. aeruginosa or Acinetobacter baumanii .
He showed that appropriate phage treatment
would prevent graft rejection even when as
few as 100 phages were used against an
inoculum of 108 bacteria.
Issues to be consideredIf a population of bacterial cells is infected
with a dose of a single clone of
bacteriophage then it is very likely that some
cells within that population will be resistant
to the phage. This resistance can arise as a
result of alteration in the phage surface
receptor site, inhibition of phage DNA
penetration, modified restriction
endonucleases resulting in degradation of
phage DNA, or inhibition of viral
intracellular development. Thus, it is
essential to use promiscuous phages with a
broad host range, or, alternatively, employ
mixtures to cover all likely variants within a
population. If a resistant strain of bacteria
should evolve then it is relatively easy toisolate further lytic phages from the
environment. Unfortunately, this approach is
not likely to find favour with regulatory
authorities.
The use of highly characterised
bacteriophages from a culture collection
obviously has its advantages, as the
spectrum of activity and virulence will be
well defined. Moreover, administration of a
bacteriophage with defined characteristics
should avoid the inadvertent use of
lysogenic phages or those with transducing
potential, particularly if they have the ability
to transfer virulence genes.
THE BIOMEDICAL SCIENTIST October 2005 1051
Table 1. Comparison of the results of phage treatmentand antibiotc treatment.
TREATMENT NO OF PARAMETERS DAYS OF TREATMENT
PATIENTS OF RECOVERY 2 3 4 5-8 12 >13
Salmonella 130 Improvement
phage of general status 30 40 30 20 10 –
Normalisation
of stool 31 54 33 8 4 –
Elimination
of pathogen 15 46 41 20 4 –
Antibiot ics only 50 Improvement
of general status – – 10 10 16 14
Normalisation
of stool – 2 8 10 18 12
Elimination
of pathogen – – – 10 20 20
‘Knowledge of phasebiology underpins anunderstanding of theirmode of action in vivo’
pp1048-1052 BMSOct05 16/9/05 10:58 AM Page 4

8/3/2019 Bacteriophage Therapy
http://slidepdf.com/reader/full/bacteriophage-therapy 5/5
1052 THE BIOMEDICAL SCIENTIST October 2005
More information is required on theinteraction of phages with the immunesystem. There is no specific evidence thatthey generate an immune response but work is required to confirm the effect ofmultiple dosing. Similarly, clearance by non-specific defences is not well understood,
although Merrill and co-workers haveisolated bacteriophage with the property of prolonged circulation in the body.
At present there are at least 16companies worldwide devoted tobacteriophage technology with a view toexploiting phage therapy in the near future.There are still issues of patentability toaddress, together with the difficulties ofovercoming regulatory hurdles.
In summary Bacteriophages are viruses capable ofkilling bacteria, including strains that areresistant to multiple antibiotics, in a highly specific manner. Abundance in the
environment makes it a relatively simpletask to isolate phages against any givenpathogen and these can be characterisedusing a series of known protocols. Thetimescale and costs for the developmentof a new phage for therapy will be a fractionof those for a new antibiotic.
There is an extensive clinical provenancefor the use of bacteriophages in thetreatment of bacterial infections. They havebeen used for the past 80 years in Easternbloc countries, with many favourable reportsof clinical benefits and few incidents ofadverse reactions.
This is accompanied by a scientificrationale to their clinical use where
knowledge of phage biology underpins anunderstanding of their mode of action in
vivo. This is in comparison to alternativetherapies such as homeopathy andacupuncture where, even if we feel they areof significant clinical benefit, their use ishard to rationalise on a scientific basis.
It is important to learn from mistakesmade in the past. Early phage therapy wasdogged by the combination of highexpectations and poor performance. If it isto become a useful adjunct to antibiotictherapy for bacterial infections then its usemust be introduced in a careful and rational way, supported by a firm underpinning ofgood science. ■
Geoff Hanlon is professor of
pharmaceutical microbiology in the
School of Pharmacy and Biomolecular
Sciences at the University of Brighton.
This article is based on a talk given
at the Oxoid Infection Control Seminar,
held in Stratford upon Avon in May.
Time to renew yourHPC registration
When do biomedical scientists
need to renew their registration?
Biomedical scientists renew theirregistration every two years; theirregistration period runs from the1 December to 30 November.
How will biomedical scientists
know when to renew?
The HPC has written to every biomedical scientist on the register
to let them know that they need torenew their registration. They should have received a renewalform in September.
What payment options do
registrants have?
The renewal fee is £120 (less if anindividual has recently registeredand is receiving the reduced rate)for two years. Registrants can pay by cheque or by postal/money order, in which case the amount must bepaid in full. Registrants can spreadthe cost of registration over thetwo-year registration cycle by paying
by Direct Debit.The HPC will deduct £30 (less ifreceiving the reduced rate) over thetwo-year registration cycle.Notification of the Direct Debitinstalment dates will have beenincluded in the letter accompanyingthe renewal form.
If biomedical scientists already
have a Direct Debit in place, do
they need to do anything else?
Yes, it is vital that they read all theinformation provided by the HPC.Even if a registrant has an existingDirect Debit they must still sign the
professional declaration and returnit to the HPC before the end ofNovember in order to remain on theregister.
What if people cannot remember
how they usually pay?
The HPC will have indicated on therenewal form if the registrant has a
current Direct Debit in place. If they do and have not changed their bankingdetails, they are only required to signthe declaration.
What happens if people do not
receive their renewal form?
A renewal notice has been sent toeveryone on the register; however,if they have moved and forgotten tonotify the HPC, or they think their form
may have been mislaid, they shouldcontact the UK RegistrationDepartment, either by phone (08453004 472 [lo-call, if calling from withinthe UK]) or by email ([email protected]), and the HPC will issuethem with a duplicate copy of therenewal form. Alternatively, go onlineand complete the online request format www.hpc-uk.org.
How will people know if they have
renewed successfully?
The register will be updated as soon asrenewal and payment have beenprocessed, and the date displayed next
to a registrant's name on the onlineregister will be updated to show 1December 2005 – 30 November 2007.
Will biomedical scientists receive
a certificate?
Yes, and it will be valid for two years.In addition to a certificate, registrants will receive a credit card-sized card on which will be a unique number. This isdesigned to combat identity fraud.Registrants should keep the card in asafe place, as the HPC will require it tobe used in the future.
Is CPD linked to re-registration?
No. The Council has taken the decisionto suspend CPD requirements for a year. CPD will be linked to re-registration from August 2006, and thefirst audit will take place in August2008. This means that althoughbiomedical scientists will have torecord their CPD from next year, theirfirst audit will be in November 2009.
Biomedical scientists are about to renew their registration with the Health
Professions Council (HPC). Here, UK Registration Manager Claire Harkin
provides an update on how the process will work.
Member Gets Member 2006 – offer ends on 31 October
pp1048-1052 BMSOct05 16/9/05 10:59 AM Page 5


![Bacteriophage [Compatibility Mode] (2)](https://static.fdocuments.in/doc/165x107/577cd7461a28ab9e789e8922/bacteriophage-compatibility-mode-2.jpg)











![BACTERIOPHAGE-RESISTANT AND BACTERIOPHAGE-SENSITIVE ...halsmith/phagemutantsubmitted_2.pdf · BACTERIOPHAGE-RESISTANT AND BACTERIOPHAGE-SENSITIVE BACTERIA IN A CHEMOSTAT ... [22],](https://static.fdocuments.in/doc/165x107/5b3839687f8b9a5a518d2ce1/bacteriophage-resistant-and-bacteriophage-sensitive-halsmithphagemutantsubmitted2pdf.jpg)