
Azelnidipine exerts renoprotective effects by improvement of renal
8
Azelnidipine ameliorates Ang II-induced damage 3651 35. Han KH, Kang YS, Han SY et al. Spironolactone ameliorates renal in- jury and connective tissue growth factor expression in type II diabetic rats. Kidney Int 2006; 70: 111–120 36. Piecha G, Koleganova N, Gross ML et al. Regression of glomeru- losclerosis in subtotally nephrectomized rats: effects of monotherapy with losartan, spironolactone, and their combination. Am J Physiol Renal Physiol 2008; 295: F137–F144 37. Mokwe E, Ohmit SE, Nasser SA et al. Determinants of blood pres- sure response to quinapril in black and white hypertensive patients: the quinapril Titration Interval Management Evaluation trial. Hyper- tension 2004; 43: 1202–1207 38. Struthers A, Krum H, Williams GH. A comparison of the aldosterone- blocking agents eplerenone and spironolactone. Clin Cardiol 2008; 31: 153–158 Received for publication: 9.2.09; Accepted in revised form: 6.7.09 Nephrol Dial Transplant (2009) 24: 3651–3658 doi: 10.1093/ndt/gfp407 Advance Access publication 7 August 2009 Azelnidipine exerts renoprotective effects by improvement of renal microcirculation in angiotensin II infusion rats Sohachi Fujimoto, Minoru Satoh, Hajime Nagasu, Hideyuki Horike, Tamaki Sasaki and Naoki Kashihara Division of Nephrology, Department of Internal Medicine, Kawasaki Medical School, Kurashiki, Okayama, Japan Correspondence and offprint requests to: Minoru Satoh; E-mail: [email protected] Abstract Background. Hypoxia-induced tubulointerstitial injury caused by loss of peritubular capillary (PTC) blood flow may be associated with progressive renal disease. There- fore, the maintenance of blood flow in PTCs may protect against loss of renal function. A long-acting calcium chan- nel blocker, azelnidipine, has been shown to be useful in the treatment of progressive renal disease. However, its mech- anism of action remains unclear. The aim of the present study was to elucidate whether azelnidipine maintains PTC blood flow and to compare it to nifedipine in its ability to improve tubulointerstitial injury caused by angiotensin II (AII) infusion in rats. Methods. PTC blood flow was initially monitored using a pencil-lens interval microscope before and after intra- venous AII (30 ng/kg/min) infusion with or without azel- nidipine (10 µg/kg/min). Next, Wistar rats were treated with chronic infusion of AII (500 ng/kg/min) via an os- motic minipump with or without azelnidipine (3 mg/kg/day, orally) or nifedipine (60 mg/kg/day, orally) for 14 days, and tubulointerstitial damage (PTC loss, interstitial fibro- sis, tubular atrophy) was examined. Results. PTC blood flow was reduced after AII infusion but improved after a bolus injection of azelnidipine. Tubu- lointerstitial damage observed in chronically AII-treated kidneys was associated with hypoxic conditions, as indi- cated by the measurement of hypoxia biomarkers (intra- cellular hypoxyprobe-1 adducts). These tubulointerstitial injuries in AII-infused rats were more effectively reduced by azelnidipine than by nifedipine. The area showing hy- poxic conditions in the kidney was also more reduced with azelnidipine than nifedipine treatment. Conclusions. Azelnidipine may increase PTC blood flow and improve renal hypoxia and tubulointerstitial injury in- duced by AII infusion. Keywords: calcium channel blocker; hypoxia; peritubular capillary; tubulointerstitial injury Introduction Tubulointerstitial injury is an important risk factor for pro- gressive renal damage [1,2]. It is reported that ischaemia, i.e. a decrease in tissue oxygen concentration caused by loss of peritubular capillaries (PTCs) and a decrease in blood flow in PTCs, is extensively involved in the pathogenesis of tubulointerstitial injury [3–5]. Therefore, the maintenance of blood flow in PTCs and the resultant improvement of tissue hypoxia may prevent progression of renal damage. Calcium channel blockers (CCBs) are the most com- monly used antihypertensive agents. Their renoprotective effects have been demonstrated in many studies using ex- perimental models of renal damage, especially those of hypertensive renal damage [6–8]. Recent large-scale clini- cal studies, such as the Lipid-Lowering Treatment to Pre- vent Heart Attack Trial and international Nifedipine GITS study: Intervention as a Goal in Hypertension Treatment, have shown that long-acting dihydropyridine CCBs effec- tively suppress progression of renal damage [9,10]. Sev- eral hypotheses have been proposed for the mechanism of such renoprotective effects of CCBs; one of these proposed mechanisms is the improvement of renal haemodynamics C The Author 2009. Published by Oxford University Press [on behalf of ERA-EDTA]. All rights reserved. For Permissions, please e-mail: [email protected] Downloaded from https://academic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 December 2021
Transcript of Azelnidipine exerts renoprotective effects by improvement of renal
Azelnidipine ameliorates Ang II-induced damage 3651
35. Han KH, Kang YS, Han SY et al. Spironolactone ameliorates renal in-jury and connective tissue growth factor expression in type II diabeticrats. Kidney Int 2006; 70: 111–120
36. Piecha G, Koleganova N, Gross ML et al. Regression of glomeru-losclerosis in subtotally nephrectomized rats: effects of monotherapywith losartan, spironolactone, and their combination. Am J PhysiolRenal Physiol 2008; 295: F137–F144
37. Mokwe E, Ohmit SE, Nasser SA et al. Determinants of blood pres-sure response to quinapril in black and white hypertensive patients:the quinapril Titration Interval Management Evaluation trial. Hyper-tension 2004; 43: 1202–1207
38. Struthers A, Krum H, Williams GH. A comparison of the aldosterone-blocking agents eplerenone and spironolactone. Clin Cardiol 2008;31: 153–158
Received for publication: 9.2.09; Accepted in revised form: 6.7.09
Nephrol Dial Transplant (2009) 24: 3651–3658doi: 10.1093/ndt/gfp407Advance Access publication 7 August 2009
Azelnidipine exerts renoprotective effects by improvement of renalmicrocirculation in angiotensin II infusion rats
Sohachi Fujimoto, Minoru Satoh, Hajime Nagasu, Hideyuki Horike, Tamaki Sasaki and Naoki Kashihara
Division of Nephrology, Department of Internal Medicine, Kawasaki Medical School, Kurashiki, Okayama, Japan
Correspondence and offprint requests to: Minoru Satoh; E-mail: [email protected]
AbstractBackground. Hypoxia-induced tubulointerstitial injurycaused by loss of peritubular capillary (PTC) blood flowmay be associated with progressive renal disease. There-fore, the maintenance of blood flow in PTCs may protectagainst loss of renal function. A long-acting calcium chan-nel blocker, azelnidipine, has been shown to be useful in thetreatment of progressive renal disease. However, its mech-anism of action remains unclear. The aim of the presentstudy was to elucidate whether azelnidipine maintains PTCblood flow and to compare it to nifedipine in its ability toimprove tubulointerstitial injury caused by angiotensin II(AII) infusion in rats.Methods. PTC blood flow was initially monitored usinga pencil-lens interval microscope before and after intra-venous AII (30 ng/kg/min) infusion with or without azel-nidipine (10 µg/kg/min). Next, Wistar rats were treatedwith chronic infusion of AII (500 ng/kg/min) via an os-motic minipump with or without azelnidipine (3 mg/kg/day,orally) or nifedipine (60 mg/kg/day, orally) for 14 days,and tubulointerstitial damage (PTC loss, interstitial fibro-sis, tubular atrophy) was examined.Results. PTC blood flow was reduced after AII infusionbut improved after a bolus injection of azelnidipine. Tubu-lointerstitial damage observed in chronically AII-treatedkidneys was associated with hypoxic conditions, as indi-cated by the measurement of hypoxia biomarkers (intra-cellular hypoxyprobe-1 adducts). These tubulointerstitialinjuries in AII-infused rats were more effectively reducedby azelnidipine than by nifedipine. The area showing hy-poxic conditions in the kidney was also more reduced withazelnidipine than nifedipine treatment.
Conclusions. Azelnidipine may increase PTC blood flowand improve renal hypoxia and tubulointerstitial injury in-duced by AII infusion.
Keywords: calcium channel blocker; hypoxia; peritubular capillary;tubulointerstitial injury
Introduction
Tubulointerstitial injury is an important risk factor for pro-gressive renal damage [1,2]. It is reported that ischaemia,i.e. a decrease in tissue oxygen concentration caused by lossof peritubular capillaries (PTCs) and a decrease in bloodflow in PTCs, is extensively involved in the pathogenesis oftubulointerstitial injury [3–5]. Therefore, the maintenanceof blood flow in PTCs and the resultant improvement oftissue hypoxia may prevent progression of renal damage.
Calcium channel blockers (CCBs) are the most com-monly used antihypertensive agents. Their renoprotectiveeffects have been demonstrated in many studies using ex-perimental models of renal damage, especially those ofhypertensive renal damage [6–8]. Recent large-scale clini-cal studies, such as the Lipid-Lowering Treatment to Pre-vent Heart Attack Trial and international Nifedipine GITSstudy: Intervention as a Goal in Hypertension Treatment,have shown that long-acting dihydropyridine CCBs effec-tively suppress progression of renal damage [9,10]. Sev-eral hypotheses have been proposed for the mechanism ofsuch renoprotective effects of CCBs; one of these proposedmechanisms is the improvement of renal haemodynamics
C© The Author 2009. Published by Oxford University Press [on behalf of ERA-EDTA]. All rights reserved.For Permissions, please e-mail: [email protected]
Dow
nloaded from https://academ
ic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 D
ecember 2021

3652 S. Fujimoto et al.
by CCBs. CCBs are reported to not only decrease bloodpressure but also increase renal plasma flow (RPF) [11,12].
End-stage renal failure can result from various fac-tors, such as diabetic nephropathy and chronic glomeru-lonephritis. Previous reports have revealed that therenin–angiotensin (RA) axis is involved in the commonmechanism of progressive renal damage. Large-scale clin-ical studies have also suggested that RA inhibitors, such asangiotensin II (AII)-receptor antagonists, have renoprotec-tive effects that are independent of their antihypertensiveeffects [13]. AII exerts its constrictive effect more intenselyon efferent arterioles than on afferent arterioles, causing anincrease in intraglomerular pressure (glomerular hyperten-sion). It is reported that some dihydropyridine CCBs reduceAII-induced constriction of efferent arterioles and therebyreduce intraglomerular pressure [14,15]. On the other hand,there has been no report on the effect of CCBs on bloodflow in PTCs.
Azelnidipine is a long-acting dihydropyridine CCB de-veloped and marketed in Japan. The drug has been shown tohave not only a potent antihypertensive effect but also a car-dioprotective effect [16]. Its renoprotective effect has alsobeen demonstrated in several experimental models [17,18]and in patients with hypertension [19]. In the present study,we investigated the renoprotective effects of azelnidipinevia its improvement of renal haemodynamics. We demon-strated that azelnidipine exerts its renoprotective effect bynot only decreasing blood pressure but also increasing bloodflow in PTCs and improving tubulointerstitial hypoxia andinjury.
Subjects and methods
Acute effect of azelnidipine in AII-infused rat
Analysis of renal microcirculation. All experiments were performed withthe approval (No. 08–004) of the Ethics Review Committee for Ani-mal Experimentation of the Kawasaki Medical School (Kurashiki, Japan).Male Wistar rats (Charles river laboratories Japan, Inc., Kanagawa, Japan)weighing 200–250 g were used in this study. The rats were anaesthetizedwith isoflurane. Then a catheter was inserted and held in place in the leftjugular vein. A continuous infusion of saline (0.05 mL/min) was adminis-tered through the catheter. Another catheter was inserted and held in placein the left carotid artery for measurement of blood pressure. Monitoringof blood flow in PTCs and observation of glomeruli were performed usinga needle-probe Charge-Coupled Device Videomicroscope (CCDV), basedon reports by Yamamoto et al. [20–22]. This system (VMS-1210; NihonKohden, Tokyo, Japan) consisted of a needle-type probe, a camera bodywith a CCD sensor, a gradient index lens and an optical fibre guide forillumination. The needle-type probe (4.5 mm in diameter) contained 18optical fibres. The CCD had an image sensor with 680 × 480 pixels, andprovided digitized images and a video recorder (EVO-9850; Sony, Tokyo,Japan). The spatial resolution of this CCD system is 0.87 µm. PTC bloodflow was recorded with the CCDV placed in direct contact with the ex-posed surface of the kidney. Images of glomeruli were taken using theCCDV, whose tip was inserted into the kidney through a small incision(0.5–1 mm) made on the exposed surface of the kidney. Bleeding wasminimal during the procedure and usually discontinued within 10 min.The probe was moved gently to gain clear images of glomeruli. Sequentialimages of renal microvessels were captured with a freeze-frame modal-ity. The diameters of afferent and efferent arterioles were measured usingthe Image-J software (http://rsbweb.nih.gov/ij/), and the flow rate of redblood cells (RBCs) was analysed using blood velocity analysis software,Medex (JMC Co, Ltd., Kyoto, Japan). A vessel segment ∼15 µm in lengthwas scanned, and the mean RBC velocity was determined by averagingat least five measurements. The specific protocol was as follows. Firstly,blood flow in PTCs or glomeruli was recorded under continuous infu-
sion of saline. Then, the infusion was changed from saline to AII, whichwas then continuously infused (30 ng/kg/min) for 10 min, and blood flowin PTCs or glomeruli was recorded. Under continuous infusion of AII,azelnidipine (Sankyo Co., Ltd., Tokyo, Japan) at 10 µg/kg/min was ad-ministered through the jugular vein, and blood flow in PTCs or glomeruliwas recorded 10 min after azelnidipine administration. The dosage ofazelnidipine was determined to achieve enough blood pressure drops aspreviously described [23].
Chronic effect of azelnidipine in AII-infused rat
Experimental animal models. Male Wistar rats (Charles river laborato-ries Japan Inc.) weighing 210–230 g were used. An osmotic minipump(Alzet model 2001; Alza Pharmaceuticals, Palo Alto, CA, USA) wasplaced under the skin of the rats, and either AII (500 ng/kg/min, n = 18)or saline (Cont, n = 6) was administered for 14 days. The rats that receivedAII were further divided into three groups based on whether they receivedno treatment (AII, n = 6), daily oral azelnidipine at 3 mg/kg/day (AII +Azl, n = 6) or nifedipine at 60 mg/kg/day (AII + Nif, n = 6). The dosageof azelnidipine was determined by referring to previous reports [24].The dosage of nifedipine was determined by preliminary experiment toachieve same blood pressure with azelnidipine treatment. Twenty-four-hour urine collection was performed 14 days after the completion of theadministration of either AII or saline. On the same day, rats were sacri-ficed under ether anaesthesia, and blood samples and both kidneys werecollected. Before the sacrifice, whole-kidney renal blood flow (RBF) wasmeasured using a V-shaped (size 0.5 V) non-cannulating flow probe con-nected to an ultrasonic transit-time flowmeter (Transonic Systems, Inc.,Ithaca, NY, USA). In this technique, the left renal artery was dissectedaway from the perinephritic fat, and a flow probe (ø 1 mm) was placedaround the renal artery near the hilum of the kidney. The probe was con-nected via a flowmeter to a computer, and RBF was recorded. After theanimals were sacrificed, portions of the removed kidneys were immersedand fixed in 4% paraformaldehyde and then embedded in paraffin, whileother portions were frozen-fixed using Tissue Tec.
Physiological and biochemical measurements. Body weight and bloodpressure were measured just before sacrifice. Blood pressure was mea-sured in pre-warmed rats by the tail-cuff method (BP-98A; Softron Co.,Ltd, Tokyo, Japan). To collect urine samples, rats were placed in metaboliccages for 24 h and were provided tap water but no food. After the final24-h fasting in metabolic cages, blood samples were obtained from ratsvia an 18-gauge needle inserted into the left ventricle after the rats werekilled. Kidney was removed and the kidney weight was measured. Theblood urea nitrogen (BUN) level was measured using urease UV. Serumand urinary creatinine levels were also measured using enzymatic meth-ods, and the urinary protein excretion (UPE) level was measured by anenzyme immunoassay.
Histopathological examination of kidneys. Paraffin-embedded sectionsof kidneys (approximately 4-µm thick) were deparaffinized and stainedby Masson staining. From these sections, the percentage of the area withtubulointerstitial injuries (infiltration of inflammatory cells, tubular di-latation/atrophy, interstitial fibrosis and tubular cast formation) was scored(grade 0 = no area of damage, grade 1 ≤ 10%, grade 2 = 10–25%, grade3 = 25–50%, grade 4 = 50–75% and grade 5 = 75–100%). The gradeswere assessed by examining 10 fields in six samples from each animal[25]. For the detection of tubulointerstitial damage, immunohistochemicalstaining for vimentin was performed. Frozen tissue sections were incu-bated in methanol with 3% hydrogen peroxide to block endogenous perox-idase activity and then incubated with a mouse anti-vimentin monoclonalantibody (Sigma-Aldrich Japan K.K., Tokyo, Japan) diluted 1:100 at 4◦Covernight. For negative controls, a mouse IgG1 (Santa Cruz Biotechnology,Inc., Santa Cruz, CA, USA) was used at equivalent concentrations. Theprimary antibody was detected using the Histofine Simple Stain MAX-PO (MULTI) kit (Nichirei Co, Tokyo, Japan) and 3,3′-diaminobenzidine(Sigma-Aldrich Japan K.K.). The percent area of vimentin positive ar-eas in the renal cortex, excluding the glomeruli and small arteries, wasmeasured using the Image-J software.
Examination of PTC volume. PTCs were detected by staining forRECA-1, a vascular endothelial marker for rats. Frozen sections of kidneys(∼4 µm thick) were fixed with acetone, to which an anti-RECA-1 mon-oclonal antibody (Cosmo Bio, Tokyo, Japan) diluted 1:50 was applied
Dow
nloaded from https://academ
ic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 D
ecember 2021

Azelnidipine ameliorates Ang II-induced damage 3653
Fig. 1. Effect of azelnidipine on changes to PTC microcirculation in-duced by acute AII infusion. Typical images of PTC haemodynamics atbaseline (A), after AII (30 ng/kg/min) infusion (B) and after azelnidipine(10 µg/kg/min) administration (C) recorded using a CCD videomicro-scope. Scale bar = 50 µm. (D) Systolic blood pressure changes. (E) RBCvelocity in PTCs. n = 6 in each group. ∗P < 0.05 versus baseline; †P <
0.05 versus AII infusion.
and incubated at 4◦C overnight. Histofine Simple Stain MAX-PO wasthen dropped onto the sections, which were then incubated for 30 minand thereafter colour was developed with 0.02% 3,3′-diaminobenzidine(Sigma-Aldrich Japan K.K.). The percent area of PTCs in the renal cortex,excluding the glomeruli, was measured using the Image-J software.
Detection of tissue ischaemia. Renal tissue ischaemia was detected usingpimonidazole (hypoxyprobe-1; CHEMICON International, Inc., Temec-ula, CA, USA). Briefly, pimonidazole hydrochloride (60 mg/kg) wasadministered through the caudal vein 2 h before euthanasia, and paraffin-embedded sections of the kidneys were prepared. The sections were de-paraffinized, and anti-pimonidazole monoclonal antibody diluted 1:100was applied and incubated at 4◦C overnight. Histofine Simple StainMAX-PO was then dropped onto the sections, which were then incu-bated for 30 min and thereafter colour was developed with 0.02% 3,3′-diaminobenzidine. The percentage of areas that stained positive for pi-monidazole in the renal cortex, excluding the glomeruli, was measuredusing the Image-J software.
Statistical analysis
All results were expressed as mean ± standard error. Statistical data pro-cessing was performed using the StatView software (StatView SE+ Graph-ics Version 4.0, Abacus Concepts, SAS Institute, Inc., Cary, NC, USA).Differences between the groups were analysed by the two-tailed unpairedStudent’s t-test, Welch’s t-test or Mann–Whitney’s U-test. The values ofP < 0.05 were considered significant.
Results
Evaluation of renal microcirculation in rats receivingacute AII-infusion
The effects of azelnidipine on AII-induced altered renal mi-crocirculation were evaluated by measuring systolic bloodpressure (SBP), blood flow in PTCs and the diameters ofafferent and efferent arterioles. A marked increase in SBPwas observed after AII administration (139 ± 5 mmHgpost-AII versus 101 ± 4 mmHg at baseline; P < 0.05;Figure 1D), and this increase was significantly reduced by
Fig. 2. Effects of azelnidipine on glomerular microcirculation changesinduced by acute AII infusion. Typical images of glomerular haemody-namics at baseline (A) recorded using a CCD videomicroscope. Glo,glomerulus; A, afferent artery; E, efferent artery. Scale bar = 50 µm.(B) RBC velocity in PTCs at baseline, after AII (30 ng/kg/min) infusionand after azelnidipine (10 µg/kg/min) administration. (C) Afferent arteri-olar diameter. (D) Efferent arteriolar diameter. n = 6 in each group. ∗P <
0.05 versus baseline; †P < 0.05 versus AII infusion.
azelnidipine administration (118 ± 7 mmHg; P < 0.05versus post-AII; Figure 1D). Figure 1A shows images ofbasal blood flow in PTCs taken using a CCDV (see supple-mental movie 1). A decrease in the diameter of PTCs wasobserved following AII administration (Figure 1B and sup-plemental movie 2), which was then partially reversed byazelnidipine administration (Figure 1C and supplementalmovie 3). The flow rate of RBCs in PTCs was significantlyreduced by AII administration (55.2 ± 10.8%; P < 0.05versus baseline; Figure 1E). The AII-induced decrease inRBC flow rate was improved by azelnidipine (81.2 ± 4.7%;P < 0.05 versus post-AII; Figure 1E). Figure 2A shows im-ages of basal blood flow in a glomerulus obtained using aCCDV (see supplemental movie 4). The flow rate of RBCsin glomeruli was also decreased by AII infusion (50.2 ±11.8%; P < 0.05 versus baseline; Figure 2 B) and improvedby azelnidipine (76.1 ± 9.2%; P < 0.05 versus post-AII;Figure 2B). AII also induced constriction of afferent andefferent arterioles of glomeruli (75.1 ± 6.3% with P <0.05 versus baseline and 66.9 ± 1.2% with P < 0.05 versusbaseline, respectively; Figure 2C and D). In addition, azel-nidipine dilated not only afferent but also efferent arterioles(110.3 ± 4.1%, P < 0.05 versus post-AII and 89.2 ± 1.7%,P < 0.05 versus AII, respectively; Figure 2C and D).
Functional data and morphological evaluation in ratsreceiving chronic AII infusion
Physiological parameters 14 days after the subcutaneousadministration of AII are shown in Table 1. An in-crease in the mean blood pressure was observed in rats
Dow
nloaded from https://academ
ic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 D
ecember 2021

3654 S. Fujimoto et al.
Table 1. Biological parameters of chronic angiotensin II-infused rats
Control (N = 6) AII (N = 6) AII+ Azl (N = 6) AII+ Nif (N = 6)
BW (g) 334 ± 4 318 ± 6 313 ± 8 310 ± 6KW (g) 1.40 ± 0.09 1.66 ± 0.04a 1.60 ± 0.08a 1.65 ± 0.10a
MBP (mmHg) 89.2 ± 4.9 159.4 ± 11.3a 116.1 ± 3.5a,b 110.4 ± 6.4a,b
BUN (mg/dL) 16.3 ± 0.9 31.8 ± 1.5a 18.3 ± 0.8b 25.8 ± 1.0a,b,c
UPE (mg/day) 1.2 ± 0.6 42.0 ± 6.1a 7.0 ± 1.7a,b 11.4 ± 5.3a,b,c
CCr (mL/min/100 g BW) 1.40 ± 0.10 0.77 ± 0.09a 1.23 ± 0.10b 0.93 ± 0.13a,c
RBF (mL/min/g KW) 5.0 ± 0.3 4.1 ± 0.2a 4.8 ± 0.2b 4.9 ± 0.3 b
Data are expressed as mean ± SEM.AII, angiotensin II; Azl, azelnidipine; Nif, nifedipine; BW, body weight; KW, kidney weight; MBP, mean blood pressure; BUN, blood urea nitrogen;UPE, urinary protein excretion; CCr, creatinine clearance; RBF, renal blood flow.aP < 0.05 versus control.bP < 0.05 versus AII.cP < 0.05 versus Azl.
receiving subcutaneous administration of AII (159.4 ±11.3 mmHg, P < 0.05 versus control). The blood pressurein rats treated with azelnidipine or nifedipine decreasedsignificantly compared with those that received AII alone(116.1 ± 3.5 or 110.4 ± 6.4 mmHg, respectively, P <0.05 versus AII). No significant differences were found inbody weight among the four groups. The kidney weightwas increased by chronic AII infusion, but there was nodifference among the group. Excretion of urinary proteinwas significantly increased in rats that received AII and wassuppressed in those treated with azelnidipine or nifedipine(42.0 ± 6.1 in AII versus 7.0 ± 1.7 in AII plus azelnidipine,11.4 ± 5.3 mg/day in AII plus nifedipine, P < 0.05). Theurinary protein excretion was much lowered by treatmentwith azelnidipine than by treatment with nifedipine. BUNwas markedly increased by AII administration, which wasimproved by azelnidipine or nifedipine treatment (31.8 ±1.5 in AII versus 18.3 ± 0.8 in AII plus azelnidipine, or25.8 ± 1.0 mg/dL in AII plus nifedipine, P < 0.05). BUNwas also considerably lower in rats treated with azelnidipinethan in those treated with nifedipine. Creatinine clearancewas markedly reduced by AII administration and improvedby azelnidipine treatment (0.77 ± 0.09 in AII versus 1.23 ±0.10 mL/min/100 g BW in AII plus azelnidipine, P < 0.05),but not by nifedipine treatment (0.93 ± 0.13 mL/min/100g BW). RBF was reduced by AII administration (5.0 ± 0.3mL/min/g kidney weight, P < 0.05 versus control). RBFwas increased in both the azelnidipine treatment group andthe nifedipine treatment group, but no statistically signif-icant differences were observed in whole-kidney RBF be-tween two groups.
To investigate whether azelnidipine treatment can im-prove AII-induced renal damage, we evaluated damage torenal cortical tissue by Masson staining. While the ratsthat did not receive AII (control group) showed almost notubulointerstitial injuries (data not shown), some of the ratsthat received AII showed various types of tissue damage,such as tubular dilatation/atrophy and perivascular fibrosis(Figure 3A). The formation of these tubulointersti-tial injuries was suppressed by azelnidipine treatment(Figure 3B). When the tubulointerstitial injuries werescored and semiquantitatively evaluated, it was also foundthat azelnidipine treatment significantly reduced AII-induced tubulointerstitial injuries (1.57 ± 0.18 in AII versus
Fig. 3. Effects of azelnidipine or nifedipine on interstitial injury associatedwith chronic AII infusion. Light micrographs of rat renal cortex from ratsthat received chronic AII (500 ng/kg/min) infusion alone (A), with azel-nidipine (3 mg/kg/day) treatment (B) or with nifedipine (60 mg/kg/day)treatment (C). Masson staining; scale bar = 100 µm. (D) Semiquantita-tive interstitial injury in the renal cortex. n = 6 in each group. ∗P < 0.05versus control rats; †P < 0.05 versus AII-infused rats; ‡P < 0.05 versusnifedipine treated, AII-infused rats.
0.55 ± 0.22 in AII + azelnidipine, P < 0.05; Figure 3D).Nifedipine treatment also prevented AII-induced interstitialinjury, but less than azelnidipine treatment (1.03 ± 0.15 inAII + nifedipine, P < 0.05 versus AII + azelnidipine;Figure 3C and D). Meanwhile, few glomerular lesions suchas glomerular sclerosis were found in all groups of rats.
We also evaluated renal cortical tissue damage by vi-mentin staining. There were few vimentin-positive areasexcept in the glomeruli and small arteries of the controlrats (data not shown). The vimentin-positive area was en-hanced by chronic AII infusion (Figure 4A). However,azelnidipine treatment limited the enhancement of AII-induced tubular damage in the renal cortex (Figure 4B). The
Dow
nloaded from https://academ
ic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 D
ecember 2021
Azelnidipine ameliorates Ang II-induced damage 3655
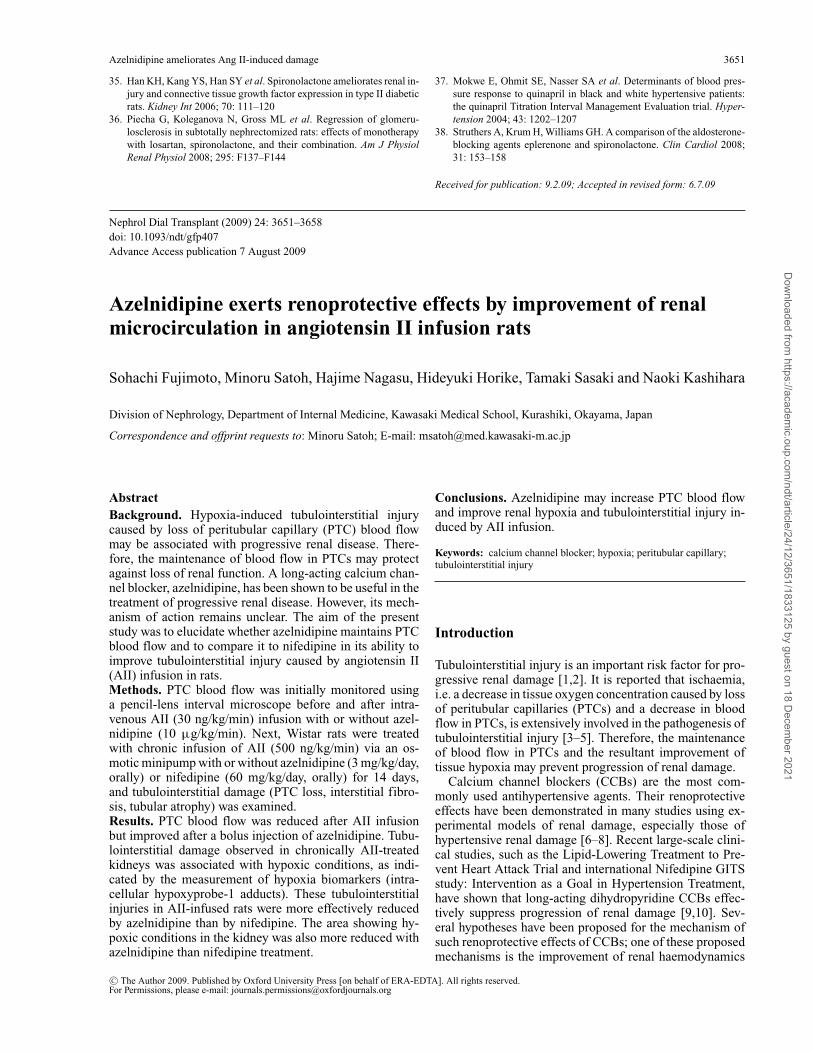
Fig. 4. Effects of azelnidipine or nifedipine on tubular damage inducedby chronic AII infusion. Tubular vimentin was used as a marker of tubulardamage. Immunohistochemical micrographs of renal cortex stained withanti-vimentin antibody from rats that received chronic AII (500 ng/kg/min)infusion alone (A), with azelnidipine (3 mg/kg/day) treatment (B) or withnifedipine (60 mg/kg/day) treatment (C). Scale bar = 100 µm. (D) Quan-titation of vimentin-positive area in the renal cortex. n = 6 in each group.∗P < 0.05 versus control rats; †P < 0.05 versus AII-infused rats,‡P < 0.05 versus nifedipine treated, AII-infused rats.
vimentin-positive area was markedly increased in rats thatreceived AII rather than saline (control group) (9.3 ± 0.3%versus 1.8 ± 0.4%, P < 0.05; Figure 4D) and was signifi-cantly reduced in rats treated with azelnidipine (3.0 ± 0.3%,P < 0.05 versus AII; Figure 4D). Nifedipine treatment alsodecreased AII-induced tubular damage (Figure 4C), but thiseffect was smaller than that with azelnidipine treatment(4.5 ± 0.6%, P < 0.05 versus AII + azelnidipine;Figure 4D).
Evaluation of renal hypoxia by pimonidazole proteinadducts
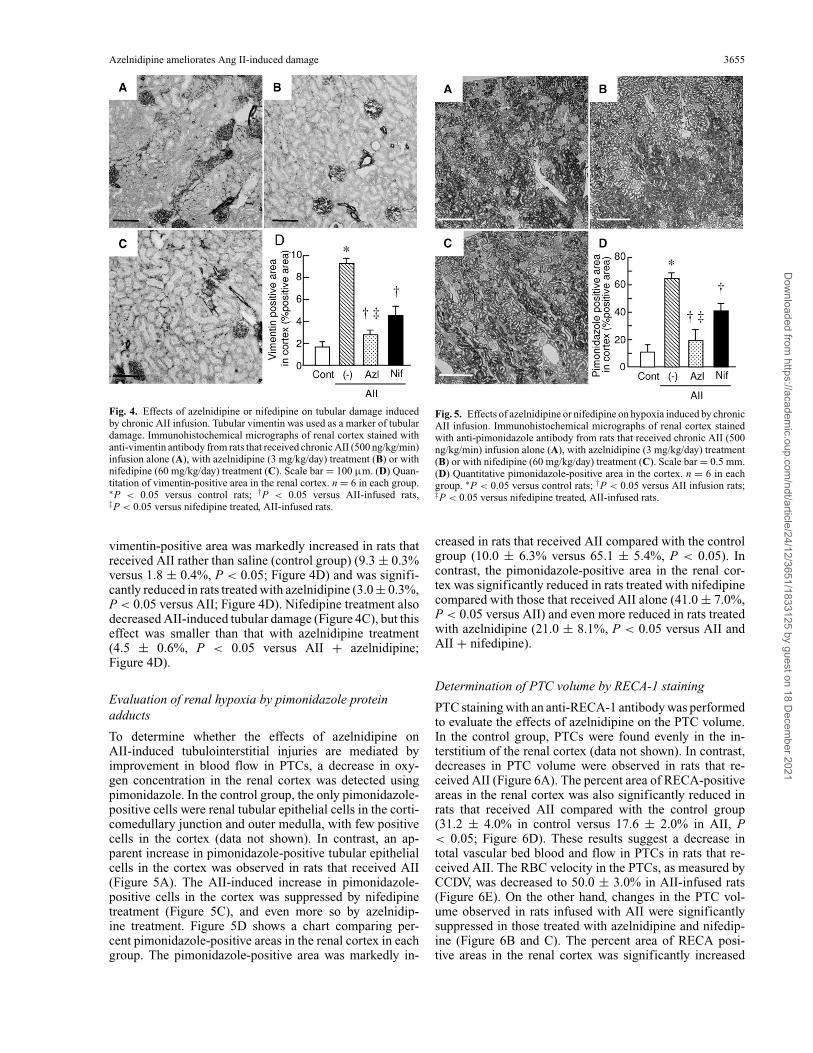
To determine whether the effects of azelnidipine onAII-induced tubulointerstitial injuries are mediated byimprovement in blood flow in PTCs, a decrease in oxy-gen concentration in the renal cortex was detected usingpimonidazole. In the control group, the only pimonidazole-positive cells were renal tubular epithelial cells in the corti-comedullary junction and outer medulla, with few positivecells in the cortex (data not shown). In contrast, an ap-parent increase in pimonidazole-positive tubular epithelialcells in the cortex was observed in rats that received AII(Figure 5A). The AII-induced increase in pimonidazole-positive cells in the cortex was suppressed by nifedipinetreatment (Figure 5C), and even more so by azelnidip-ine treatment. Figure 5D shows a chart comparing per-cent pimonidazole-positive areas in the renal cortex in eachgroup. The pimonidazole-positive area was markedly in-
Fig. 5. Effects of azelnidipine or nifedipine on hypoxia induced by chronicAII infusion. Immunohistochemical micrographs of renal cortex stainedwith anti-pimonidazole antibody from rats that received chronic AII (500ng/kg/min) infusion alone (A), with azelnidipine (3 mg/kg/day) treatment(B) or with nifedipine (60 mg/kg/day) treatment (C). Scale bar = 0.5 mm.(D) Quantitative pimonidazole-positive area in the cortex. n = 6 in eachgroup. ∗P < 0.05 versus control rats; †P < 0.05 versus AII infusion rats;‡P < 0.05 versus nifedipine treated, AII-infused rats.
creased in rats that received AII compared with the controlgroup (10.0 ± 6.3% versus 65.1 ± 5.4%, P < 0.05). Incontrast, the pimonidazole-positive area in the renal cor-tex was significantly reduced in rats treated with nifedipinecompared with those that received AII alone (41.0 ± 7.0%,P < 0.05 versus AII) and even more reduced in rats treatedwith azelnidipine (21.0 ± 8.1%, P < 0.05 versus AII andAII + nifedipine).
Determination of PTC volume by RECA-1 staining
PTC staining with an anti-RECA-1 antibody was performedto evaluate the effects of azelnidipine on the PTC volume.In the control group, PTCs were found evenly in the in-terstitium of the renal cortex (data not shown). In contrast,decreases in PTC volume were observed in rats that re-ceived AII (Figure 6A). The percent area of RECA-positiveareas in the renal cortex was also significantly reduced inrats that received AII compared with the control group(31.2 ± 4.0% in control versus 17.6 ± 2.0% in AII, P< 0.05; Figure 6D). These results suggest a decrease intotal vascular bed blood and flow in PTCs in rats that re-ceived AII. The RBC velocity in the PTCs, as measured byCCDV, was decreased to 50.0 ± 3.0% in AII-infused rats(Figure 6E). On the other hand, changes in the PTC vol-ume observed in rats infused with AII were significantlysuppressed in those treated with azelnidipine and nifedip-ine (Figure 6B and C). The percent area of RECA posi-tive areas in the renal cortex was significantly increased
Dow
nloaded from https://academ
ic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 D
ecember 2021

3656 S. Fujimoto et al.
Fig. 6. Effects of azelnidipine or nifedipine on the reduction of PTC vol-ume induced by chronic AII infusion. Immunohistochemical micrographsof PTCs in the renal cortex stained with anti-RECA-1 antibody in ratsthat received chronic AII (500 ng/kg/min) infusion alone (A), with azel-nidipine (3 mg/kg/day) treatment (B) or with nifedipine (60 mg/kg/day)treatment (C). Scale bar = 100 µm. (D) Quantitative volume of PTCsin the renal cortex. n = 6 in each group. ∗P < 0.05 versus control rats;†P < 0.05 versus AII-infused rats. (E) RBC velocity in PTCs. n = 6 ineach group. ∗P < 0.05 versus baseline; †P < 0.05 versus AII infusion,‡P < 0.05 versus nifedipine treated, AII-infused rats.
in rats treated with azelnidipine or nifedipine comparedwith those that received AII alone (28.5 ± 4.2% or 24.1 ±4.5%, respectively, P < 0.05 versus AII; Figure 6D). TheRBC velocity in the PTCs was also increased to 63.3 ±3.0% with nifedipine, and even more increased with azel-nidipine (88.4 ± 7.0%; P < 0.05 versus AII + nifedipine,Figure 6E).
Discussion
We directly monitored the haemodynamics of PTCs andglomeruli in the superficial layer of the renal cortex usinga CCDV. This approach enables monitoring of haemody-namics under physiological conditions and can be used toevaluate changes in microcirculation in glomeruli and PTCs[20–22]. The present study revealed that (1) AII constricts
both afferent and efferent arterioles and thereby reducesdownstream blood flow in PTCs, and (2) azelnidipine par-tially suppresses AII-induced constriction of afferent andefferent arterioles and thereby increases blood flow inPTCs. It has already been reported that AII constricts notonly efferent but also afferent arterioles and reduces RBF ina dose-dependent manner [20]. However, there have beenno reports, to our knowledge, of changes in blood flowin PTCs as monitored directly on visualized images. Themethod used in the present study has enabled direct, in vivomonitoring of blood flow in PTCs and revealed a decreasein blood flow in PTCs following AII administration.
AII is known to be involved in the pathogenesis of renalimpairments through various effects. High-dose, chronicadministration of AII induces severe tubulointerstitial in-juries in rats; however, the degree of glomerular injuries isknown to be milder than that of tubulointerstitial injuries[26,27]. Moreover, AII has been shown to induce mor-phological changes in tubulointerstitial cells [26,27] andinfiltration of inflammatory cells [26]. The results of thepresent study suggest that AII induces tubulointerstitial in-juries by decreasing blood flow in PTCs. Animal models ofrenal damage induced by chronic administration of AII alsoexhibited tubulointerstitial injuries and the spread of tissuehypoxia in the cortex, as shown by pimonidazole staining.These results suggest that AII reduces blood flow in PTCsand thereby causes a decrease in blood flow and tissuehypoxia in the renal cortex, resulting in tubulointerstitialinjuries.
Oizumi et al. have reported an increase in RPF in sponta-neously hypertensive rats (SHRs) treated with azelnidipineat 3 mg/kg/day for 15 weeks [28]. Similarly, Yagil et al.compared changes in RPF induced by intravenous admin-istration of azelnidipine with those induced by nicardipine,with blood pressure controlled at comparable levels, and re-ported a significant increase in RPF induced by azelnidipine[17]. In this study, azelnidipine also increased glomerularfiltration rate (GFR), but the degree of increase in GFR waslower than that of increase in RPF. In a study by Kanazawaet al. using 5/6 nephrectomized SHR, azelnidipine wascomparable to angiotensin-converting enzyme inhibitors inexerting an inhibitory effect on urinary protein excretion[18]. The results from these reports suggest that azelnidip-ine dilates both afferent and efferent arterioles. Dihydropy-ridine CCBs generally block only the L-type calcium chan-nel, which is present in afferent arterioles but not in efferentarterioles. It has thus been believed that dihydropyridineCCBs dilate only afferent arterioles. Because nifedipineacts exclusively on L-type calcium channels, it may pre-dominantly dilate afferent arterioles and cause glomerularhypertension [29]. However, it has recently been reportedthat some long-acting dihydropyridine CCBs also dilate ef-ferent arterioles [30]. Azelnidipine is a new CCB and thusits dilating effect on afferent and efferent arterioles has notbeen established to date. It has been reported that azelni-dipine provides renal sympathoinhibitory effects [23,31].Activation of renal sympathetic nerves decrease RBF andincrease preglomerular and postglomerular resistance [32].Thus, the vasodilatory action of azelnidipine in afferent andefferent arterioles may be mediated at least in part by theinhibition of the sympathetic nervous system.
Dow
nloaded from https://academ
ic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 D
ecember 2021

Azelnidipine ameliorates Ang II-induced damage 3657
Azelnidipine suppressed AII-induced tubulointerstitialinjuries and reduced tissue hypoxia in the renal cortex. Therenoprotective effect of CCBs is mediated by their improv-ing effect on the glomerular microcirculation, as well asby their antihypertensive effect [27]; however, no reportshave so far demonstrated that CCBs exert their renopro-tective effects by increasing blood flow in PTCs. Kondoet al. reported that azelnidipine attenuates AII-induced per-itubular ischaemia, which may be involved in its beneficialeffects on renal injury [33]. In the previous report, azelni-dipine, unlike other dihydropyridine CCBs, was shown toslightly decrease heart rate in clinical settings [34]. More-over, azelnidipine decreased urinary protein excretion inpatients with hypertension much more than did amlodipine[19]. These effects may result from its anti-sympathetic andanti-inflammatory effects. Given the present finding thatazelnidipine increases blood flow in PTCs, as confirmedusing a CCDV, this agent may improve tubulointerstitial is-chaemia by correcting interstitial blood flow altered by AII.
PTCs diverging from glomerular efferent arterioles forma vascular network in the renal cortex. Thus, blood flow inPTCs is closely linked with changes in glomerular bloodflow. Furthermore, damage in PTCs is not only involved inthe pathogenesis of tubulointerstitial injuries but is also animportant prognostic factor for renal function [1–3]. Main-tenance of blood flow in PTCs is thus essential for pre-vention of progressive renal damage. In the present study,a decrease in the PTC volume induced by chronic admin-istration of AII was observed in the regions of interstitialinjuries, and the lumens of PTCs were also narrowed fol-lowing AII administration. These findings were consistentwith the findings of PTCs obtained using a CCDV. Takentogether, the decrease in the area of PTCs was assumed to bea result of the narrowing of their lumens due to a decreasein blood flow. In addition, rats treated with azelnidipineretained normal lumens, as also confirmed using a CCDV.We thus speculated that azelnidipine maintains blood flowin PTCs by improving microcirculation.
Our observations using a CCDV were limited to the outerlayer of the kidney. In the kidney, renal glomerular arteri-oles are morphologically heterogeneous, and the responsesof intracellular calcium concentration to AII differ amongcell types [35,36]. AII controls the vascular tone of pre- andpost-glomerular arterioles, and thereby controls glomeru-lar filtration. In the outer cortex, AII-induced smaller in-tracellular calcium concentration increases in thin efferentarterioles than in afferent arterioles. In the inner cortex,two subpopulations of juxtamedullary efferent arterioles,muscular ones that terminate as vasa rectae and thin onesthat terminate as PTCs, have been described. They displayfunctional heterogeneity with regard to the AII response.The response to AII was lower in thin than in the muscularefferent arterioles but did not differ from that obtained withcorresponding afferent arterioles. The glomeruli and PTCsobserved using a CCDV were almost in the outer cortex,so the data from the CCDV do not reflect the PTCs of thewhole kidney.
The RBF reduced by AII administration was increasedby both azelnidipine treatment and nifedipine treatment tothe same degree. However, the PTC volume and RBC ve-locity in the PTCs were higher in the azelnidipine group
than in the nifedipine group. These data indicate that azel-nidipine treatment improved cortical blood flow especially.The data from pimonidazole staining showing that azelni-dipine reduced the cortical hypoxic area in the AII-infusedkidney also support this conclusion. The blood flow nearthe cortex is supplied through efferent arteries of the cor-tical glomeruli. Azelnidipine may improve cortical bloodflow by dilating these arteries, thereby increasing the PTCblood supply.
Our RBF values in healthy control animals were slightlylower than normal (∼7.0 mL/min). RBF in the rat variesgreatly depending on the anaesthetic used and the plane ofanaesthesia. Hypothermia is also a common cause of lowerthan expected flow measurements. In our experiment, RBFwas measured just before sacrifice. So, we did not maintainthe body temperature with a heat pad, which may haveresulted in the lower RBF values than expected.
Tubular hypoxia and hypoxia-induced tubular damagemay be improved by an increase in the number of PTCs.However, it is difficult to precisely measure the PTC num-ber. The PTC volume that we measured by RECA staining isdependent on tubular blood flow. This measurement of PTCvolume does not reflect the exact number of PTCs. Insteadof measuring PTC number, we checked VEGF mRNA ex-pression, an indicator of angiogenesis. The VEGF mRNAexpression was increased by AII infusion and decreased byazelnidipine or nifedipine treatment, and the VEGF expres-sion was much higher in the nifedipine group than the azel-nidipine group (supplemental data). Therefore, the increasein PTC volume and RBC velocity in PTCs by azelnidipinewas not induced by increased angiogenesis.
In conclusion, we have demonstrated that azelnidipinemaintains blood flow in PTCs by suppressing AII-inducedconstriction of afferent and efferent arterioles and therebysuppresses tubulointerstitial injuries caused by ischaemia.Currently, CCBs are widely used for the treatment of hy-pertension. The present study suggests that azelnidipineimproves not only glomerular blood flow but also renalinterstitial microcirculation.
Acknowledgements. This work was supported by the KAKENHI(19590969 and 19590968). We thank Mrs Sawako Tsujita for theanimal care.
Conflict of interest statement. None declared.
Supplementary data
Supplementary data are available online at http://ndt.oxfordjournals.org.
References
1. Klahr S, Schreiner G, Ichikawa I. The progression of renal disease. NEngl J Med 1988; 318: 1657–1666
2. Nath KA. Tubulointerstitial changes as a major determinant in theprogression of renal damage. Am J Kidney Dis 1992; 20: 1–17
3. Bohle A, Mackensen-Haen S, Wehrmann M. Significance of post-glomerular capillaries in the pathogenesis of chronic renal failure.Kidney Blood Press Res 1996; 19: 191–195
Dow
nloaded from https://academ
ic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 D
ecember 2021

3658 S. Fujimoto et al.
4. Ohashi R, Kitamura H, Yamanaka N. Peritubular capillary injury dur-ing the progression of experimental glomerulonephritis in rats. J AmSoc Nephrol 2000; 11: 47–56
5. Nangaku M. Chronic hypoxia and tubulointerstitial injury: a finalcommon pathway to end-stage renal failure. J Am Soc Nephrol 2006;17: 17–25
6. Dworkin LD, Benstein JA, Parker M et al. Calcium antagonists andconverting enzyme inhibitors reduce renal injury by different mecha-nisms. Kidney Int 1993; 43: 808–814
7. Wenzel UO, Troschau G, Schoeppe W et al. Adverse effect of thecalcium channel blocker nitrendipine on nephrosclerosis in rats withrenovascular hypertension. Hypertension 1992; 20: 233–241
8. Ma G, Allen TJ, Cooper ME et al. Calcium channel blockers, ei-ther amlodipine or mibefradil, ameliorate renal injury in experimentaldiabetes. Kidney Int 2004; 66: 1090–1098
9. Salvetti A, Ghiadoni L. Guidelines for antihypertensive treatment: anupdate after the ALLHAT study. J Am Soc Nephrol 2004; 15(Suppl1): S51–S54
10. Brown MJ, Palmer CR, Castaigne A et al. Morbidity and mortalityin patients randomised to double-blind treatment with a long-actingcalcium-channel blocker or diuretic in the International NifedipineGITS study: Intervention as a Goal in Hypertension Treatment (IN-SIGHT). Lancet 2000; 356: 366–372
11. Yokoyama S, Kaburagi T. Clinical effects of intravenous nifedipineon renal function. J Cardiovasc Pharmacol 1983; 5: 67–71
12. Bell AJ, Lindner A. Effects of verapamil and nifedipine on renalfunction and hemodynamics in the dog. Ren Physiol 1984; 7: 329–343
13. Brenner BM, Cooper ME, de Zeeuw D et al. Effects of losartan onrenal and cardiovascular outcomes in patients with type 2 diabetes andnephropathy. N Engl J Med 2001; 345: 861–869
14. Carmines PK, Navar LG. Disparate effects of Ca channel blockadeon afferent and efferent arteriolar responses to ANG II. Am J Physiol1989; 256: F1015–F1020
15. Honda M, Hayashi K, Matsuda H et al. Divergent natriuretic action ofcalcium channel antagonists in mongrel dogs: renal haemodynamicsas a determinant of natriuresis. Clin Sci (Lond) 2001; 101: 421–427
16. Nishiya D, Enomoto S, Omura T et al. The long-acting Ca2+-channelblocker azelnidipine prevents left ventricular remodeling after myocar-dial infarction. J Pharmacol Sci 2007; 103: 391–397
17. Yagil Y, Miyamoto M, Frasier L et al. Effects of CS-905, a noveldihydropyridine calcium channel blocker, on arterial pressure, renalexcretory function, and inner medullary blood flow in the rat. Am JHypertens 1994; 7: 637–646
18. Kanazawa M, Kohzuki M, Yoshida K et al. Combination therapywith an angiotensin-converting enzyme (ACE) inhibitor and a cal-cium antagonist: beyond the renoprotective effects of ACE inhibitormonotherapy in a spontaneous hypertensive rat with renal ablation.Hypertens Res 2002; 25: 447–453
19. Nakamura T, Sugaya T, Kawagoe Y et al. Azelnidipine reduces uri-nary protein excretion and urinary liver-type fatty acid binding proteinin patients with hypertensive chronic kidney disease. Am J Med Sci2007; 333: 321–326
20. Yamamoto T, Hayashi K, Matsuda H et al. In vivo visualization ofangiotensin II- and tubuloglomerular feedback-mediated renal vaso-constriction. Kidney Int 2001; 60: 364–369
21. Yamamoto T, Tada T, Brodsky SV et al. Intravital videomicroscopy ofperitubular capillaries in renal ischemia. Am J Physiol Renal Physiol2002; 282: F1150–F1155
22. Yamamoto T, Tomura Y, Tanaka H et al. In vivo visualization ofcharacteristics of renal microcirculation in hypertensive and diabeticrats. Am J Physiol Renal Physiol 2001; 281: F571–F577
23. Shokoji T, Fujisawa Y, Kiyomoto H et al. Effects of a new calciumchannel blocker, azelnidipine, on systemic hemodynamics and renalsympathetic nerve activity in spontaneously hypertensive rats. Hyper-tens Res 2005; 28: 1017–1023
24. Oizumi K, Nishino H, Miyake S et al. Hemodynamic changes fol-lowing long-term administration of CS-905, a novel dihydropyri-dine calcium blocker, in conscious SHR. Jpn J Pharmacol 1990; 54:1–6
25. Namikoshi T, Tomita N, Satoh M et al. Olmesartan ameliorates reno-vascular injury and oxidative stress in Zucker obese rats enhanced bydietary protein. Am J Hypertens 2007; 20: 1085–1091
26. Johnson RJ, Alpers CE, Yoshimura A et al. Renal injury from an-giotensin II-mediated hypertension. Hypertension 1992; 19: 464–474
27. Giachelli CM, Pichler R, Lombardi D et al. Osteopontin expressionin angiotensin II-induced tubulointerstitial nephritis. Kidney Int 1994;45: 515–524
28. Oizumi K, Nishino H, Miyamoto M et al. Beneficial renal ef-fects of CS-905, a novel dihydropyridine calcium blocker, in SHR.Jpn J Pharmacol 1989; 51: 501–508
29. Hayashi K, Wakino S, Sugano N et al. Ca2+ channel subtypes andpharmacology in the kidney. Circ Res 2007; 100: 342–353
30. Hayashi K, Ozawa Y, Fujiwara K et al. Role of actions of calcium an-tagonists on efferent arterioles—with special references to glomerularhypertension. Am J Nephrol 2003; 23: 229–244
31. Nakamoto M, Ohya Y, Sakima A et al. Azelnidipine attenuates car-diovascular and sympathetic responses to air-jet stress in geneticallyhypertensive rats. Hypertens Res 2007; 30: 359–366
32. Denton KM, Shweta A, Anderson WP. Preglomerular and post-glomerular resistance responses to different levels of sympatheticactivation by hypoxia. J Am Soc Nephrol 2002; 13: 27–34
33. Kondo N, Kiyomoto H, Yamamoto T et al. Effects of calcium channelblockade on angiotensin II-induced peritubular ischemia in rats. JPharmacol Exp Ther 2006; 316: 1047–1052
34. Fujisawa M, Yorikane R, Chiba S et al. Chronotropic effects of azelni-dipine, a slow- and long-acting dihydropyridine-type calcium channelblocker, in anesthetized dogs: a comparison with amlodipine. J Car-diovasc Pharmacol 2009; 53: 325–332
35. Helou CM, Marchetti J. Morphological heterogeneity of renalglomerular arterioles and distinct [Ca2+]i responses to ANG II. AmJ Physiol 1997; 273: F84–F96
36. Helou CM, Imbert-Teboul M, Doucet A et al. Angiotensin receptorsubtypes in thin and muscular juxtamedullary efferent arterioles of ratkidney. Am J Physiol Renal Physiol 2003; 285: F507–F514
Received for publication: 21.10.08; Accepted in revised form: 16.7.09
Dow
nloaded from https://academ
ic.oup.com/ndt/article/24/12/3651/1833125 by guest on 18 D
ecember 2021


















