Attitudes Toward Mental Health Dissertation
127
Michelle Rodriguez 12404089 PSY4001 THE UNIVERSITY OF NORTHAMPTON School of Social Sciences Attitudes Toward Mental Health Michelle Rodriguez April 2015 1
-
Upload
michelle-rodriguez -
Category
Documents
-
view
2.448 -
download
1
Transcript of Attitudes Toward Mental Health Dissertation

Michelle Rodriguez 12404089 PSY4001
THE UNIVERSITY OF NORTHAMPTON School of Social Sciences
Attitudes Toward Mental Health
Michelle Rodriguez
April 2015
Submitted in part-fulfilment of the requirements for the BSc Psychology degree as awarded by The University of Northampton.
DECLARATION1

Michelle Rodriguez 12404089 PSY4001
I, Michelle Rodriguez, declare that this dissertation has been composed by myself, and that the work presented herein is my own.
Where any work or material that is not entirely my own has been used, its source is clearly stated and acknowledged.
Word Count: 9575
Date
20/04/15
Signature
Michelle Rodriguez
ContentsPage number
2

Michelle Rodriguez 12404089 PSY4001
Title page ………………………………………………………………………………………..1Declaration………………………………………………………………………………….…..2Contents………………………………………………………………………………………....3–4Abstract………………………………………………………………………………………..….5Introduction…………………………………………………………………………………….6–16
An Overview of Attitudes Towards Mental Health……………….6–10Demographic Differences in Attitudes TowardsMental Health……………………………………………………………………..
….10Gender Differences in Attitudes Towards Mental Health and Empathy as an Explanation………………………………………………….11–12Measuring Attitudes Towards Mental Health……………………….12–13Attitudes Towards Depression and Schizophrenia………………13–16
Method…………………………………………………………………………………………...16–24
Design…………………………………………………………………………………..16–17
Participants………………………………………………………………………..….17
Materials………………………………………………………………………………17–18
Multidimensional Emotional Empathy Scale……………………..18–19Community Attitudes towards the Mentally Ill………………….19–20Social Distance Scale…………………………………………………………..21Procedure……………………………………………………………………….
….21–23
3

Michelle Rodriguez 12404089 PSY4001
Ethical Considerations…………………………………………………….….23–24Results……………………………………………………………………………………….….24–33
Gender Differences…………………………………………………………….25–26
Correlational Analysis………………………………………………………..26–29
Group Differences……………………………………………………………..29–30
ANOVA/ANCOVA…………………………………………………………………30–32
ANOVA for Non-Related Variables…………………………………….32–33Discussion…………………………………………………………………………………….34–40
Hypothesis One……………………………………………………………….…..34
Hypothesis Two…………………………………………………………………….34
Hypothesis Three………………………………………………………………….35
Hypothesis Four………………………………………………………….……..35–36
Further Discussion……………………………………………………….…….36–40References……………………………………………………………………………………41–48Appendices…………………………………………………………………………………..49–108
4

Michelle Rodriguez 12404089 PSY4001
Abstract
The following research is an online study looking at attitudes towards mental health and factors that affect these. To do so, 210 participants were gathered (37 males, and 173 females) using a random and self-selected sample. Participants’ empathy levels were assessed using the Multidimensional Emotional Empathy Scale; they were then presented with a vignette that had the diagnosis of either ‘depression’, ‘schizophrenia’, or no diagnosis and then they had to answer the Community Attitudes towards the Mentally Ill scale and a Social Distance Scale to assess their attitudes and social distance towards mental health.
5

Michelle Rodriguez 12404089 PSY4001
Findings supported the hypothesis that Females generally have significantly better attitudes than males, females have significantly higher levels of empathy than males and that people with higher levels of empathy had significantly better attitudes towards mental health overall. Contrary to hypothesis, participants had a significantly better attitude towards schizophrenia than towards depression, with participants in the depression condition having the worst attitudes towards mental health overall. Results are discussed in terms of previous research and implications for further research to be carried out are strongly advised with mention of practical applications of findings.
Introduction
An Overview of Attitudes Towards Mental Health
Historically, attitudes towards mental health have never been very positive, the label ‘mental illness’ has been stigmatised (Fink, 1992) and has been widely documented since as early as the 1950’s (Rabkin, 1974); people and the media tend to stigmatise mental illness, with Hollywood dramatizing the portrayal of mental distress for entertainment (Wahl & Lefkowits, 1989; Diefenbach & West, 2007), many people get the wrong idea about what mental illness is really like and because they are misinformed (Sarbin & Mancuso, 1970). Much of the negativism affecting
6

Michelle Rodriguez 12404089 PSY4001
the topic of mental health is believed to come from lack of knowledge of what mental illness really is; Angermeyer, Matschinger, & Corrigan (2004) have found that in a German participant population of 5025, increased familiarity with mental illness led to a weaker desire for social distance and they propose that if the public’s familiarity with mental illness is increased then stigma towards it will decrease which sounds promising when looking at their findings. However, other research has found the complete opposite of this. For example, Angermeyer & Matschinger (2005) found that those who have a different type of knowledge focusing on an increased tendency to endorse biological causes of schizophrenia also increased the desire for social distance from people with schizophrenia which contradicts the general theory that with more knowledge there will be less social distance and better attitudes. Similarly, research conducted by Nordt, Rössler, & Lauber (2006) and Jorm, Korten, Jacomb, Christensen, & Henderson (1999) found that mental health professionals actually held more negative views and stereotypes towards mental illness than the general population, and that 1 in 4 psychiatrists and psychologists considered a non-mentally-ill vignette as mentally ill. This shows that mental health professionals, although they have the most knowledge about mental health and mental illness, have the most negative attitudes towards it. This would not make sense to theorists considering that more research has found that with more knowledge, there is a better attitude towards mental health as will be discussed further on. Interestingly, no difference in attitudes towards mental illness has been shown in pre and post-trained mental health nurses (Malla & Shaw, 1987). Although it has to be acknowledged that the research conducted is less modern so it could be out of date for nurse training and it would be interesting to find out if the same is true of pre and post-trained mental health nurses in this day and age since the preferred approach to psychiatric illness have changed from century to century (Nolan, 2000). Another nurse sample from nursing homes has shown that staff showed moderately positive attitudes towards patients with dementia and had well-developed empathy overall and that the most
7

Michelle Rodriguez 12404089 PSY4001
positive attitudes towards patients lied in those staff with the highest empathy levels. However, increased burnout experience decreased empathy levels in nurses (Àstrom, Nilsson, Norberg, & Winblad, 1990) which suggest that mental health professionals who have more demanding roles when it comes to mental illness can lose empathy towards mental health issues as stress burnout increases which could be why Nordt, et al. (2006) found that mental health professionals hold a more negative attitude than the general public about mental illness.
It has been found that acceptance of and attitudes towards mental illness depends highly on age, Stuart & Arboleda-Flórez (2001) found that from a sample of 1657 people aged 15 and over, older people over the age of 60 hold more negative and skeptical views towards schizophrenia and the effectiveness of its treatment and that those with more knowledge instead of exposure, had less distancing attitudes. This goes back to the theory that with more knowledge, there comes more acceptance, yet old age seems to affect this in the sense that older people hold less positive attitudes towards mental health anyway which could be because of the increased stigma mental illness has received in the past decades (Fink, 1992). Even though mental health understanding and acceptance has moved forwards greatly in recent years (World Health Organisation, 2001), it does not take away from the stereotypes and attitudes people have already formed, especially if they grew up with them. Lauber, Nordt, Falcato, & Rössler (2000) also found, from a representative sample in the German, French, and Italian-speaking part of Switzerland, that age, education, and gender are some of the main things that affect public acceptance of the mentally ill and in a study with a sample of 89 adolescents, it was found that what mostly affected their attitudes towards mental illness was the mass media, personal experience with mental illness, and their parents, and that adolescents had a more negative attitude and greater social distance towards the mentally ill when proposed with relationships that suggested greater intimacy (Lopez,1991). These findings uphold that age is a very strong correlator with
8

Michelle Rodriguez 12404089 PSY4001
attitudes towards mental illness and it seems like both the older and younger generation are the ones who have less positive views about mental illness and that these attitudes are influenced by outside forces such as media, peers and the amount of exposure to mental illness experienced by people along with knowledge of it, most of all. Alas, from the research reviewed above, it seems like once someone has their opinion and attitude set, they are very hard to be changed which is why it is so important to implement intervention strategies targeting the younger population before they are exposed to too many mental health stigmas and develop a negative attitude towards mental illness.
Further evidence that the mass media plays an important part in the setting of mental health attitudes is a study conducted by Wahl & Lefkowits (1989) which has found that people who watch a movie depicting a mentally ill killer have significantly more negative attitudes towards mental illness than those who watch a movie with nothing to do about mental illness, regardless of having received information about mental illness beforehand or not and this supports the concern many people have of media depictions adding to the negative stigma of mental illness. What is even scarier is that they also found that corrective information alone may not be enough to counteract the stigmatising impact such films have on the general population. Similarly, Thornton & Wahl (1995) found more negative attitudes towards mental illness after participants read a news article depicting a crime with a mentally ill person involved; also, Granello, Pauley, & Carmichael (1999) found that 102 undergraduates who got information about mental health through the media reported more negative attitudes and similarly, Diefenbach & West (2007) found that media stereotypes affect the public’s attitudes towards mental health issues negatively and portrayals of mentally ill people tend to be violent, false, and negative with mentally ill characters being portrayed as 10 times more likely to be aggressive, and criminals, than non-mentally ill characters. This is a huge problem for the movement of better understanding of mental illness as movie and media depictions of
9

Michelle Rodriguez 12404089 PSY4001
the mentally ill are grossly overdramatized which causes a vast stigmatising view of mental health for the general public who are susceptible to such garbage, especially younger people such as children and teenagers. Wilson, Nairn, Coverdale, & Panapa (2000) found that in children’s TV, references of mental illness was found predominantly in cartoons and that commonly occurring terms such as ‘crazy’, ‘mad’, and ‘losing your mind’ were employed to denote the loss of control. Not surprisingly, the six consistently mentally ill characters were almost entirely devoid of admirable attributes; Wahl (2003) found similar results and he concludes that children are being socialised into stigmatising conceptions of mental illness from a young age. These studies were conducted on TV aimed at children under the age of 10. How are attitudes towards mental illness supposed to be changed for the better if children’s TV, which they grow up watching, and even 85% Disney animated films (Lawson & Fouts, 2004) depict mental illness as a bad thing and uses derogatory terms aimed at mental health casually to denote negative behaviours and actions; it reduces mental health to something to be made fun of and it is not right since studies mentioned previously/above have shown that media affects the way we shape our attitudes towards mental illness.
Demographic Differences in Attitudes Towards Mental Health
Culture wise, it has been found that regular contact with mentally ill patients is associated with better knowledge and better acceptance of mental illness in Hong Kong (Siu, et al., 2012) and sub-Saharan Africa, where having never cared for the mentally ill, being over the age of 50, the perception of the stereotypes that mentally ill people are dangerous, and perceived supernatural causation of mental illness increased social distance (Adewuya & Makanjuola, 2008) which is supported through research by Ukpong & Abasiubong (2010) which found that a Nigerian university teaching hospital population of 208 had strongly negative attitudes towards mental illness, and most of them thought the cause of
10

Michelle Rodriguez 12404089 PSY4001
mental illness to be witches or other supernatural causes. The above research suggests that the African population is very superstitious towards mental health and mental illness itself, no matter if they are educated on it. This means that there is evidence of culture differences when looking at attitudes towards mental health since the Hong Kong population mentioned above did not share any such supernatural beliefs about the causation of mental illness, and no other culture apart from the African culture so far from the research reviewed has been so superstitious about mental health. However, the fact that Nigeria and sub-Saharan countries in Africa are low-income countries could explain these supernatural stigmas since there are many witch-doctors around and education levels of mental health are low in the continent overall. It is believed that a greater understanding of mental disorders in the general public would lessen the stigma created towards mental health and encourage the usage of effective interventions available to them (Hugo, Boshoff, Traut, Zungu-Dirwayi, & Stein, 2003).
Gender Differences in Attitudes Towards Mental Health and Empathy as an Explanation
Overall, Males tend to show a more negative attitude when it comes to seeking mental health treatment (Gonzalez, Alegria, & Prihoda, 2005; Berger, Levant, McMillan, Kelleher, & Sellers, 2005) whilst females tend to show a more positive attitude towards it and this could be because negative attitudes associated with psychological openness contribute to men’s underutilisation of mental health services (Mackenzie, Gekoskia, & Knox, 2006; Ojeda & Bergstresser, 2008). It is well known that men are stereotyped into being the strong masculine beings (Broverman, Vogel, Broverman, Clarkson, & Rosenkrantz, 1972; Prentice & Carranza, 2002) and stigma towards mental illness makes men who have a mental illness to be perceived as weaker and less masculine which lowers the chance of them seeking help and can have a big impact on them, making men exhibit more depressive symptoms (Möller-Leimkühler, 2002; Mahalik,
11

Michelle Rodriguez 12404089 PSY4001
Burns, & Syzdek, 2007). The fact that men are more likely to put their health at risk just because they have negative views and attitudes towards mental illness is irresponsible and it is mostly because they care about how others will perceive them and about appearing masculine which does not seem to impact women as they have higher rates of help-seeking (Judd, Komiti, & Jackson, 2008; Leong & Zachar, 1999) and femininity influences the level of stigma tolerance in people (Ang, Lim, Tan, & Yau, 2004). The stigma towards mental illness makes it so that if someone has a mental health issue then they will be viewed as being weak-willed even though it is not their fault and they cannot help it. It has nothing to do with weakness and that is what the public needs to learn and understand so that neither gender suffers alone in silence. Because of this, one of the hypotheses to be tested for this study will be that females will generally have a more positive attitude towards mental health than males.
For the purpose of this study, attitudes towards depression and schizophrenia will be assessed as much of the current research focuses on mainly these two diagnoses; gender differences will be explored to find out if results from previous research can be reproduced in which males have a less positive attitude towards mental health than women. Since it has been found that empathy correlates to attitudes towards mental health and that more empathetic people have better attitudes towards mental health (Batson, Polycarpou, & Harmon-Jones, 1997; Elizur & Rosenheim, 1982), this will also be explored in this study and it will be theorised that females will have more empathy than males since much research has found this to be true (Eisenberg & Lennon, 1983; Rueckert, 2011; Toussainta & Webb, 2005), in addition, Rueckert & Naybar (2008) also found that there is a possible neural basis for gender differences in empathy. Empathy, for the purpose of this study, will be defined as ‘the vicarious affective response to another person's feelings’ (Hoffman, 1977).
12

Michelle Rodriguez 12404089 PSY4001
Measuring Attitudes Towards Mental Health
In order to conduct this study, the Community Attitudes towards the Mentally Ill scale was used to asses participants’ attitudes towards mental health. This scale was chosen as it has high validity and reliability and research mentioned in this literature review have used it themselves (Granello, et al., 1999; Thornton & Wahl, 1995; Ukpong & Abasiubong, 2010). Similarly, the Social Distance Scale was chosen as it has proved to be very reliable and valid in its use of assessing social distance with research looking at mental health (Adewuya & Makanjuola, 2008; Angermeyer & Matschinger, 2005; Angermeyer, et al., 2004; Nordt, et al., 2006; Stuart & Arboleda-Flórez, 2001). To measure empathy, the Multidimensional Emotional Empathy Scale was chosen above another empathy scale for its superior reliability. All of the scales mentioned will be discussed in depth in the materials section of the report (p. 17).
Attitudes Towards Depression and Schizophrenia
Depression and schizophrenia were the two chosen diagnoses to be presented to participants in this study because one is generally more well-known and mainstream than the other. More people will know about depression and what it is since it is one of the most talked about mental health issues, whereas less people will be familiar with what schizophrenia and its classification, etc. really is since it is talked about much less and it has many more myths around it than depression.
The term ‘depression’ is used to describe a range of moods, ranging from low spirits to more intense and severe moods that can and do interfere with everyday life. Symptoms often include irritableness or depressed mood such as feeling sad or empty, decreased interest or pleasure, a significant weight change, or change in appetite, not being able to sleep or sleeping too much, loss of energy, not wanting to do anything, feelings of guilt or worthlessness, diminished concentration and most severely,
13

Michelle Rodriguez 12404089 PSY4001
suicidality (American Psychiatric Association, 2013). Between 8% and 12% of the UK population experience depression in any given year (Singleton, Bumpstead, O’Brien, Lee, & Meltzer, 2001).
Schizophrenia is a psychotic disorder; ‘psychosis’ describes a loss of touch with reality and the psychotic symptoms of schizophrenia include delusions, hallucinations, disorganised speech, grossly disorganised or catatonic behaviour, and negative symptoms such as diminished emotional expression or a lack of drive or motivation (avolition) (APA, 2013). Schizophrenia is the most common form of psychotic disorder, affecting about 1% of the population over a lifetime (NICE, 2009).
Dietrich, Mergl, Freudenberg, Althaus, & Hegerl (2010) has found that campaigning in order to inform the general public about and create more awareness towards depression works in that it creates more positive attitudes towards causation and medication treatment. However, there was a decline in positive attitudes towards depression in the second year of the campaign which were done with lower intensity. This shows that there is a need for permanent and high intensity campaigning to raise awareness of depression. In addition to this, Schulze, Richter-Werling, Matschinger, & Angermeyer (2003) found that project weeks carried out with secondary school students where they met a young person with schizophrenia, showed a significant reduction of negative stereotypes and social distance which were still evident at the 1-month-follow-up. This suggests that young people are susceptible to changing their attitude towards mental illness through intervention plans such as antistigma projects which could be beneficial in improving the attitudes of the public towards mental health. Similarly, Altindag, Yanik, Ucok, Alptekin, & Ozkan (2006) found that antistigma programmes improved the attitudes of medical students towards schizophrenia, and also lowered their social distance which is further proof that intervention programmes do work but need to be kept up and offered on a regular basis as this sample’s attitude lowered at the 1-month-follow-up. The fact that antistigma interventions
14

Michelle Rodriguez 12404089 PSY4001
work on improving the attitudes people have towards both depression and schizophrenia means that more such programmes should be implemented to raise awareness of what each mental illness actually is and combat negative stereotypes as these affect people’s perceptions and attitudes towards mental illness. For example, nursing staff in somatic care reported more negative attitudes towards people with schizophrenia than nursing staff in mental health since they regard them to be more dangerous and unpredictable (Björkman, Angelman, & Jönsson, 2008). Similarly, Reavley & Jorm (2011) found that schizophrenia was most likely to be associated with dangerousness.
An explanation for this could be, as discussed earlier on, the media. It has an effect on the attitudes people have towards mental illness and specifically, selective media reporting of schizophrenic people reinforces the stereotypes of dangerousness and unpredictability which makes the public have more negative attitudes towards the diagnosis (Angermeyer & Matschinger, 1996). And not just that, but labelling also affect people’s attitudes towards mental illness. For example, Angermeyer & Matschinger (2003a) found that the labelling of schizophrenia has negative effects outweighing those of a positive nature for people with schizophrenia. The label endorses the stigma of dangerousness which has a strong negative effect on people’s attitudes towards schizophrenia and increases the preference for social distance. However, they also found that labelling has practically no effect on the public’s attitudes towards depression, interestingly. This raises the question of why does the label of schizophrenia affect people’s attitudes towards individuals with the diagnosis, but there is no effect from the label of depression. This could be because people are generally more aware of and accept depression more than they do schizophrenia since it is a more common diagnosis.
When looking at attitudes towards these two diagnoses, much of the literature available must be reviewed and a study by Ozmen, et al. (2004) has actually found attitudes towards depression to be very negative, with
15

Michelle Rodriguez 12404089 PSY4001
nearly half of participants perceiving people with depression as dangerous and more than half of participants stating that they would not marry someone with depression. Those who believed that depression was caused by a weakness of personality had more negative attitudes towards the illness. Similarly, it was found that people from Bali, Indonesia, a non-industrialise society, actually had a more positive attitude towards schizophrenia and a more negative attitude towards depression, interestingly (Kurihara, Kato, Sakamoto, Reverger, & Kitamura, 2000). These findings are interesting as not much research has found attitudes towards depression to be more negative than those towards schizophrenia as it generally tends to be the other way around (Angermeyer & Matschinger, 2003b). However, overall, it seems like people have the most negative attitudes towards schizophrenia when compared to depression (Eker, 1989). This is why, from reviewing all the literature above, the theory that generally, people will have better attitudes towards depression than schizophrenia, has been set for this study.
Also, a fourth hypothesis for this study is that people with higher levels of empathy will have better attitudes towards mental health overall since empathy has been found to correlate with attitudes towards mental illness. As most of the sample for this study was to be psychology students, their knowledge of mental health did not get measured although it would be interesting to see whether more research would demonstrate that people with more knowledge about the mental health have better attitudes or whether it is the opposite or whether it has no effect at all since much of the research states that knowledge generally does influence the attitudes people have towards mental illness; however, there is much contradicting research about the effect. Further research could benefit from measuring this.
Method
Design
16

Michelle Rodriguez 12404089 PSY4001
This was an online based study; a quantitative approach was used to assess the impact of using a vignette on attitudes towards mental health whilst controlling for participants’ natural empathy levels. A correlational experiment with an independent measures design was chosen as participants either selected an experimental group or the control group in order to explore whether empathy had any effect on the attitudes participants had towards a vignette diagnosed with depression, or schizophrenia, or a non-diagnosed control so it could be certain that it was the independent variable (IV) of the diagnoses that swayed the dependent variable (DV) of the attitudes of participants instead of it being just the description of the vignette. Each participant’s empathy level was a naturally-occurring IV.
Participants
In total, 262 participants took part in the online study; however, some responses were discarded due to being incomplete, therefore, out of the 262 responses collected, 210 were included in the analysis. In total there were 37 males and 173 females and each condition had 70 participants all over the age of 18. There were 8 males and 62 females in the schizophrenia condition, 15 males and 55 females in the depression condition, and 14 males and 56 females in the non-diagnosis condition. Some participants were recruited from the University of Northampton using a self-selected sample from the university’s student participant pool and others, worldwide from social media outlets such as Facebook and Tumblr. Participants all allocated themselves randomly to any of 6 conditions (see procedure, p. 21) depending on which online link they clicked. The use of a self-selected sample allowed for the provision of a data sample which included a diverse range of people as participants ranged from undergraduate university students to any other background as long as they were over 18 years old. The data collection process took place over a period of 40 days.
17

Michelle Rodriguez 12404089 PSY4001
Materials
The materials used in this study consisted of an information sheet (see appendix 1), a consent form (see appendix 2), a debrief sheet (see appendix 3), a vignette (see appendix 4), the Multidimensional Emotional Empathy Scale (MDEES) (see appendix 5), the Community Attitudes towards the Mentally Ill (CAMI) scale (see appendix 6), and the Social Distance Scale (SDS) (see appendix 7). These materials were all put together into an online survey platform website called SurveyMonkey to make it easier to gather participants/data. The vignette depicted an ‘a day in the life of’ paragraph since what is depicted could happen to anyone when having a particularly bad day, however, the vignette contained some symptoms that are usually seen as typical of depression and/or schizophrenia but did not fulfil any diagnostic criteria; the vignette was either headed by the diagnosis of depression, schizophrenia, or no diagnosis. The vignette depiction was the same for all 3 diagnoses since unlike previous research (Angermeyer & Matschinger, 2005; Jorm, et al., 1999; Nordt et al., 2006), the present study wanted to assess whether the labels of the diagnoses were the ones to have an impact on participants’ attitudes instead of the description of the vignette. The name chosen for the vignette and the pronouns used were all gender-neutral to make sure no gender bias affected the results. The vignette was created strictly for the purpose of this study.
Multidimensional Emotional Empathy Scale
The MDEES is a 30-item scale that was designed by Caruso & Mayer (1998) and it measures five related emotionally-relevant components of empathy including: emotional suffering; positive sharing; crying; emotional attention; and feeling for others, as well as a total scale score. To calculate empathy, the scale includes positively and negatively worded statements such as “I feel like crying when watching a sad movie” and “I
18

Michelle Rodriguez 12404089 PSY4001
don’t give others’ feelings much thought” to avoid response bias. The response format employed for this questionnaire was a 5-point Likert scale, ranging from 1 (Strongly Disagree), to 5 (Strongly Agree). Negatively worded statements were reverse scored before the total for each participant was calculated by adding up all the scores and dividing by 30. The 5 component sub-scales mentioned above were of no particular interest to this study since the scale was based upon an emotional view of empathy rather than on a multidimensional empathy model (Caruso & Mayer, 1998) so only the total scale score was calculated for each participant. A high score on this scale corresponded to high levels of empathy whereas a low score corresponded to low levels of empathy. Caruso & Mayer (1998) found the alpha reliabilities for all scale scores for the MDEES to be moderate to high with the total 30-item scale scores being 0.88 and overall, they found the scale to have internal consistency reliability as measured by coefficient alpha of 0.86 which means they were found to be reliable. There is another 28-item empathy scale available developed by Davis (1980) for a multidimensional approach, however, the researcher chose to use the MDEES instead seeing as none of Davis’ 4 sub-scales have an alpha coefficient higher than 0.79 which means that Caruso & Mayer’s MDEES is more reliable. The Cronbach’s alpha for the 30-item MDEES scale in this study was found to be 0.88.
Community Attitudes towards the Mentally Ill
The CAMI scale is a 40-item scale designed by Taylor & Dear (1981) which consists of 4 sub-scales with 10 items each that measure authoritarianism, benevolence, social restrictiveness, and community mental health ideology (CMHI) with new items to explicitly measure community attitudes toward the mentally ill instead of previous scales that have been primarily applied in a professional context. Each sub-scale contains statements that either support or oppose the underlying concept such as “One of the main causes of mental illness is a lack of self-discipline and will power” and “Mental illness is an illness like any other”
19

Michelle Rodriguez 12404089 PSY4001
for authoritarianism; so if participants agreed with the first statement which is pro-authoritarianism, they would have scored higher on the authoritarianism sub-scale and so on. Authoritarianism reflects a view of the mentally ill as an inferior class requiring coercive handling; benevolence shows a sympathetic view of the mentally ill based on humanistic and religious principles; social restrictiveness reflects viewing the mentally ill as a threat to society; CMHI judge mental health facility locations more desirably. Participants had to indicate how strongly they agreed or disagreed with each statement using a 5-point Likert scale ranging from SA (Strongly Agree) to SD (Strongly Disagree). Their response was transformed into a numerical score between 1 and 5 depending on which statements supported or opposed the nature of each sub-scale component; for the supporting statements, SA was given a 5 and SD a 1 and this was reversed for opposing statements. Statements were sequenced in 10 sets of 4 items and they were ordered by scale within each set so as to avoid response bias. Mean scores were calculated for each sub-scale per participant and depending on which statements they agreed more with for each of the 4 sub-scales, participants either exhibited a less or more sympathetic attitude towards mental illness. The alpha coefficient for each sub-scale was higher than 0.75, with the highest being 0.88 which shows high internal validity (Taylor & Dear, 1981). However, a disadvantage of having so many items in a questionnaire is that participants tend to show boredom/fatigue effects which led some to skip the CAMI scale completely which meant that their data had to be discarded. In order to minimise this, some participants completed the CAMI scale first and then the SDS and others completed them the other way around in order to counterbalance order effects. Nevertheless, Morrison (2011) has findings consistent with those of Taylor & Dear’s which means the reliability of the scale is high. This study’s Cronbach’s alpha for the CAMI scale was found to surprisingly be 0.21 which is much lower than what previous research has found, this could be interpreted as being down to the length of the scale and participants not answering the scale properly.
20

Michelle Rodriguez 12404089 PSY4001
Social Distance Scale
The SDS is a 7-item scale originally designed to be used to measure prejudice towards ethnicity and religion by Bogardus (1933) but has since been successfully and validly used in much research to measure attitudes towards mental health (Nordt, et al., 2006). Originally, to calculate social distance, participants would be given a number of races, religions, and occupations and they would tick ‘yes’ or ‘no’ for each of the statements and the scale would be scored by adding up the number of races, etc. ticked for the negatively worded items and dividing by 3 to obtain the participant’s social distance quotient; however, since the study was looking at mental health, the researcher changed the scoring instructions slightly as they saw fit. Participants read the description of the vignette with one of the diagnoses and used that information to answer either ‘yes’ or ‘no’ using a dichotomous scale, for each statement; for example, the scale contains positively and negatively worded statements such as, “Would marry” and “Would have live outside my neighbourhood”. Responses were transformed into a numerical score between 1 and 2 for ‘yes’ and ‘no’ respectively and negatively worded statements were reverse scored. Scores were added up and the mean was taken; the higher the score, the greater the participant’s social distance. The minimum score was 1 for a low/no social distance level and the maximum score was 2 for a high social distance level. Buchegger-Traxler & Sirsch (2012) found that the Cronbach’s Alpha of the SDS was 0.77 when it comes to the reliability of social distance being a risk factor for teenagers but it shows that the scale has good reliability. This study’s Cronbach’s alpha for the SDS was found to be somewhat lower at 0.61.
Procedure
21

Michelle Rodriguez 12404089 PSY4001
The study was carried out online using the online survey platform called SurveyMonkey as this method was much easier and faster for higher data gathering in as little time as possible (Wright, 2005). As participation was not restricted to only individuals that the researcher could physically reach, people in other parts in the world could participate. Participants also had the ability to complete the study in their own time in a place they felt comfortable and without the researcher being present so they were more likely to complete the study properly. The study consisted of the researcher creating 6 different surveys on the SurveyMonkey website: 2 per condition. This was for counterbalancing purposes; for example, one survey for all of the 3 conditions had the CAMI scale before the SDS and for the second survey, the order was reversed. The MDEES was always put first, before either of the other scales, to avoid social desirability bias.
Participants were gathered either through social media or through the university’s student participant pool. Those who were gathered using social media were done so by the researcher posting all 6 online study links on Facebook groups and Tumblr along with a short message asking anyone who would be inclined to take part in order to help with the researcher’s Psychology dissertation on the topic of mental health, to complete and click on only one of the 6 links provided and to share or reblog the post on their Facebook wall or Tumblr page. Participants gathered through the university’s student participant pool just had to sign up to one of the 6 studies to take part; restrictions were applied to make sure that each participant could only sign up and complete one study. An equal number of participants in each condition was ensured as the links would close once a certain number of responses was reached and the researcher checked responses to filter out those which were not completed; once this was done, the link reopened. This was repeated as necessary so that all responses had completed the surveys fully. Once participants clicked on any link, the first page they were taken to was an information sheet informing them of the nature of the study, etc. followed
22

Michelle Rodriguez 12404089 PSY4001
by a consent form which they had to tick to continue with the study. The MDEES proceeded and then participants either read the ‘a day in the life of’ a gender-neutral vignette diagnosed with depression, schizophrenia, or not diagnosed and answered the SDS or CAMI scale depending on which link they clicked on. The last page was the debrief sheet which informed participants of the complete research aims and gave contact information for a helpful hotline should they feel the need to talk to someone. Throughout the survey, participants could move back and forth through the pages at their leisure if they wished to change their answers, or close their browser window if they wished to withdraw their data at any point up until they clicked the submit button at the end of the survey. There was no time limit on how fast participants needed to complete the study and once participants from the student participant pool completed the study, they were awarded a credit.
Ethical Considerations
Ethical approval was sought (see appendix 8) and all British Psychological Society ethical guidelines were adhered to and full ethical approval was granted by them and the Psychology Division Ethics Panel of the University of Northampton with several major corrections (see appendix 9). Amendments were made according to the corrections suggested, prior to data collection.
All online links for the study contained an information sheet as the first page which informed participants of the nature of the study, for example, how long it would take and why it was being carried out, along with withdrawal details and the contact information of the researcher and their supervisor in case participants wanted to enquire about the study. Following the information sheet, a consent form was provided on the second page of the online study. Informed consent was obtained through participants’ ticking of several boxes on the form which meant that they were over 18 years old, understood the aims of the study and that it was
23

Michelle Rodriguez 12404089 PSY4001
completely voluntary and anonymous, as well as knowing the deadline date for their withdrawal which was a week after participation; they were also asked to indicate their gender. In order to ensure complete anonymity, the SurveyMonkey website offered the option of disabling the tracking of IP addresses which the researcher did. Participants were given a unique number to identify them in case they wished to withdraw.
No deception was used in the study and participants were shown a debrief sheet once they completed the study but before they submitted their data, as the last page of the online survey. The debrief sheet informed participants of the research aims more clearly than in the information sheet as there was more than one condition they could be put into, therefore, in-depth knowledge of the study aims such as knowing the researcher was investigating whether people have better attitudes towards depression or schizophrenia, could have impelled participants to develop demand characteristics and not answer the questionnaires honestly. As the topic of mental health and the nature of the questions included in the questionnaires could be potentially distressing for some people, the university’s Nightline hotline number was provided in the debrief sheet so that participants could talk to someone for support if they felt the need to or found participating distressing. If participants were not from the university then they could not call the hotline but the contact information of the researcher and their supervisor were provided in any case so participants from other areas could get in touch. No other hotline number was provided since the researcher believed that the participation in the research would not be distressing enough to warrant further aid.
Results
The assumption for a t-test of data being normally distributed (Dancey & Reidy, 2011) was checked and the descriptive summary for overall scores for each variable is presented in table 1 below.
24

Michelle Rodriguez 12404089 PSY4001
Table 1. Descriptive Statistics of groups with 95% Confidence Intervals
Variable Mean SD 95% CILower Upper
Empathy 3.80 .45 .39 .51Authoritarianis
m2.02 .50 .44 .56
Benevolence 4.24 .51 .42 .59Social
Restrictiveness1.96 .51 .45 .57
CMHI 3.90 .55 .49 .60Social Distance 1.32 .24 .22 .26
Note. SD = Standard Deviation. CI = Confidence Interval. Number of participants = 210
Gender Differences
The low number of males compared to females could have affected the data so in order to test whether males and females could be treated as equals, an independent samples t-test running Levene's Test of Equality of Variances was used on the data. Table 2 below shows the descriptive summary of each variable split into males and females and the t-test results for both genders.
Table 2. Gender Differences between variables and t-test of Equality of Means for both genders
25

Michelle Rodriguez 12404089 PSY4001
VariableMale Female Joint
Mean SD95% CI
Mean SD95% CI
t df p d95% CI
Lower Upper Lower Upper Lower Upper
Empathy 3.60 .59 .41 .75 3.84 .40 .35 .45 -2.41 42 .021 .48 -.45 -.04
Authoritarianism
2.16 .53 .38 .66 1.99 .49 .43 .56 2.00 208 .047 .33 .002 .36
Benevolence
4.05 .63 .42 .80 4.29 .47 .40 .56 -2.62 208 .009 -.43 -.42 -.06
Social Restrictive
ness2.12 .53 .39 .68 1.92 .50 .43 .57 2.21 208 .028 .39 .02 .038
CMHI 3.76 .49 .39 .57 3.93 .55 .49 .62 -1.64 208 .103 -.33 -.36 .03
Social Distance
1.37 .24 .17 .30 1.31 .24 .21 .26 1.48 208 .140 .25 -.02 .15
Note. SD = Standard Deviation. CI = Confidence Interval. df = degrees of freedom. p = significance. d = Cohen’s d. Number of males = 37. Number of females = 173. Bonferroni correction = 0.05/6 α = 0.008
Empathy scores were slightly higher for female participants than for male participants. Interestingly, all variable scores were slightly higher for females apart from social restrictiveness, in which case, males scored marginally higher than females. However, these results could be partly due to the small amount of males compared to females as there were only 37 male participants to the much greater 173 female participants. There was a significant difference in variance between males and females in empathy (t(42) = -2.41, p = .021, d = .48) however, since there was such a small number of males included in the study the groups were treated homogenously. The effect size was small/medium as a .50 is considered a medium effect size (Cohen, 1988). Table 2 above also shows that authoritarianism, social restrictiveness, CMHI, and social distance all had small effect sizes and benevolence had a small to medium effect size.
Correlational Analysis
Correlational analyses were used to explore the relationship between empathy and for the following sets of variables: authoritarianism, benevolence, social restrictiveness, CMHI, and social distance; and also to
26

Michelle Rodriguez 12404089 PSY4001
explore whether there was a relationship between gender and empathy and all aforementioned variables. Table 3 and 4 below illustrate this.
Table 3. Correlations of Empathy with Other Variables
Variable Pearson’s r p 95% CILower Upper
Authoritarianism -.11 .10 -.24 .02Benevolence .26 <.001 .14 .39
Social Restrictiveness -.18 .01 -.30 -.05CMHI .14 .04 -.02 .28
Social Distance -.06 .41 -.20 .08Note. p = significance. CI = Confidence Interval .10 = small, .30 = medium, .50 = large effect size (Cohen, 1988). Number of participants = 210
Table 3 indicates no significant relationship between empathy and social distance and empathy and authoritarianism along with a negative small effect size. However, the correlation indicates a weak negative relationship between empathy and social restrictiveness which was classed as significant, this shows that the more empathetic and pro-CMHI participants had a more positive view towards mental health; there was also a weak positive relationship between empathy and CMHI and empathy and benevolence which were both classed as significant which means that the less empathetic participants who scored higher on the social restrictiveness scale had a more negative view towards mental health.
Table 4. Correlations of Empathy by Gender with Other Variables
Variable Gender Pearson’s r p Z-score
27

Michelle Rodriguez 12404089 PSY4001
MinimumMaximu
mAuthoritarianis
mMale -.15 .38 -1.83 2.92
Female -.07 .38 -2.02 3.93
Benevolence Male .32 .06 -2.96 1.52Female .20 .01 -5.70 1.51
Social Restrictiveness
Male -.18 .28 -1.72 2.95Female -.14 .06 -1.85 4.59
CMHI Male .40 .02 -1.76 2.31Female .04 .56 -3.48 1.94
Social DistanceMale -.08 .63 -1.55 2.63
Female -.02 .75 -1.30 2.93Note. p = significance. male = 37, female =173.
Table 4 above shows that for males, empathy levels only had a significantly moderate positive relationship with CMHI (r = .40, N = 37, p < .05, two tails) scores which shows that males have a more positive attitude towards mental health facility locations. Whilst for females, empathy levels only had a significantly weak positive relationship with benevolence (r = .20, N = 173, p < .01, two tails) scores which means that females have a more sympathetic view towards mental illness, however, this significance could have been due to the small number of male participants as males showed a moderate effect size with benevolence. All other variables for either gender did not have a significant relationship with empathy scores although males tended to have larger effect sizes than females.
A multiple regression analysis was not used as there were only 2 statistically significant correlations connected to gender and this was not the main hypothesis the study was looking for, plus there were not enough males to truly gauge if gender accounts for attitudes towards mental health as the Levene’s test showed that the variances of the male and female groups were homogenous.
28

Michelle Rodriguez 12404089 PSY4001
Group Differences
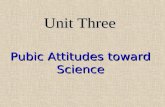
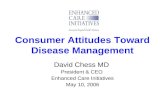
Graph 1 shows the mean scores of the 4 CAMI sub-scales with error bars.
Participants generally scored low for authoritarianism and social restrictiveness which is a positive sign as those sub-scales are associated with negative attitudes towards mental illness, whereas benevolence and CMHI are associated with positive attitudes towards mental illness and participants across all groups scored much higher on those sub-scales. Overall, there was not much variance of mean scores between all groups; however, the schizophrenia group scored the lowest on both authoritarianism and social constrictiveness and the highest on both benevolence and CMHI which indicates that they seemed to be the group
29

Michelle Rodriguez 12404089 PSY4001
that had the most positive attitude towards mental illness. The depression group managed the opposite, scoring the highest on both authoritarianism and social constrictiveness, and the lowest on both benevolence and CMHI which means they were the group with the most negative attitude towards mental illness. Interestingly, the control non-diagnosis group scored in the middle for all scales.
ANOVA/ANCOVA
A One way Between Measures ANOVA was carried out to investigate whether empathy and group scores were significant or not. The ANOVA indicated that there was not a significant difference between groups (F(2, 207) = 2.93, p = .055, ηp2 = .028). Table 5 below shows the mean and standard deviation with 95% confidence intervals for the ANOVA.
Table 5. Descriptive Statistics for Group ANOVA Controlling for Empathy
Group Mean SD n 95% CILower Upper
Depression 3.69 .48 70 3.59 3.80Non-
Diagnosis3.86 .48 70 3.76 3.97
Schizophrenia
3.84 .37 70 3.74 3.95
Note. SD = Standard Deviation. n = number of participants. CI = Confidence Interval
Since the significance score for the ANOVA test was extremely close to the arbitrary dichotomous cut off point of .05, the Tukey HSD post hoc test was conducted to make sure that random allocation was effective. The post hoc test showed that there were no significant differences between depression and non-diagnosis (p = .07, 95%CI[-.34, .01], d = -.35), nor between schizophrenia and depression (p = .13, 95%CI[-.03, .32], d =
30

Michelle Rodriguez 12404089 PSY4001
-.35), nor between non-diagnosis and schizophrenia (p = .96, 95%CI[-.16, .20], d = .05).
The assumptions for the ANCOVA test of normal distribution, homogeneity of variances, linearity of regression, homogeneity of regression slopes, and independence of error terms (Dancey & Reidy, 2011) were checked and it was found that only benevolence and social restrictiveness were related to empathy, therefore, the ANCOVA test was carried out for those and as some assumptions were violated such as the linearity of regression, and authoritarianism, CMHI, and social distance were not related to empathy, it was decided to drop the covariate from the model and run a one-way ANOVA instead for these 3 variables. A factorial ANOVA was not carried out instead as this would mean that the data would have to be split and sample size would decrease which would increase the degree of sampling error (Dancey & Reidy, 2011).
Two separate ANCOVA analyses were carried out to test the empathy effects on benevolence and social restrictiveness.
The predicted main effect of empathy shows that empathy had a significant effect on benevolence (F(1, 206) = 13.44, p = .001, ηp2 = .061). This indicates that participants who scored higher on empathy also scored significantly higher on benevolence. The groups do not differ on benevolence, once the effects of empathy are partialled out (F(2, 206) = 1.24, p = .29, ηp2 = .012).
The predicted main effect of empathy shows that empathy had a significant effect on social restrictiveness (F(1, 206) = 6.00, p = .02, ηp2 = .028). This indicates that participants who scored higher on empathy, scored significantly lower on social restrictiveness. The groups do not differ on social restrictiveness, once the effects of empathy are partialled out (F(2, 206) = 2.16, p = .12, ηp2 = .021).
31

Michelle Rodriguez 12404089 PSY4001
ANOVA for Non-Related Variables
Table 6 below shows the mean, standard deviation, and 95% confidence intervals for each group per scale.
Table 6. Descriptive Statistics for Interaction Between Scales and Groups
Scale Group Mean SD 95% CILower Upper
Authoritarianism
Depression 2.09 .49 1.97 2.21Non-
diagnosis2.08 .53 1.95 2.20
Schizophrenia
1.88 .45 1.78 1.99
CMHIDepression 3.75 .52 3.63 3.87
Non-diagnosis
3.96 .64 3.81 4.11
Schizophrenia
3.98 .44 3.88 4.09
Social DistanceDepression 1.29 .23 1.24 1.35
Non-diagnosis
1.30 .23 1.24 1.35
Schizophrenia
1.37 .24 1.31 1.43
Note. SD = Standard Deviation. CI = Confidence Interval
It shows that authoritarianism scores were highest for the depression condition and lowest for the schizophrenia condition and that CMHI and social distance scores were highest for the schizophrenia condition and lowest for the depression condition.
A One way Between Measures ANOVA was carried out to investigate whether authoritarianism and group scores were significant or not. The ANOVA indicated that there was a significant difference between two or
32

Michelle Rodriguez 12404089 PSY4001
more groups (F(2, 207) = 3.88, p = .02, ηp2 = .04). A Tukey HSD post hoc test confirmed that the differences between the depression and schizophrenia conditions were unlikely to have arisen by sampling error (p = .04, 95%CI[.01, .41], d = .45). There was no significant difference between depression and non-diagnosis (p = .99, 95%CI[-.18, .21], d = .02), nor between non-diagnosis and schizophrenia (p = .05, 95%CI[-.002, .39], d = .41).
A One way Between Measures ANOVA was carried out to investigate whether CMHI and group scores were significant or not. The ANOVA indicated that there was a significant difference between two or more groups (F(2, 207) = 3.91, p = .02, ηp2 = .04). A Tukey HSD post hoc test confirmed that the differences between the depression and schizophrenia conditions were unlikely to have arisen by sampling error (p = .03, 95%CI[-.45, -.02], d = -.48). There was no significant difference between depression and non-diagnosis (p = .06, 95%CI[-.42, .01], d = -.36) although it must be identified that this was very close to the cut-off point (.05) and there is a moderate effect size. There was no significant difference found between non-diagnosis and schizophrenia either (p = .96, 95%CI[-.24, .19], d = -.04).
A One way Between Measures ANOVA was carried out to investigate whether social distance and group scores were significant or not. The ANOVA indicated that there was not a significant difference between groups (F(2, 207) = 2.27, p = .11, ηp2 = .02).
Discussion
33

Michelle Rodriguez 12404089 PSY4001
Hypothesis One
Women scored higher than males on all scales apart from the authoritarianism, social restrictiveness, and social distance scales and from this it can be deduced that women do have a better attitude towards mental illness than men since these results were found to be statistically significant apart from the CMHI and social distance scales – even though all effect sizes were small to medium – which means that the null hypothesis of the theory that females would generally have a better attitude towards mental health overall can be rejected. This means that findings do support those of Gonzalez, et al. (2005) and Berger, et al. (2005) in which men tend to show a more negative attitude towards mental health. The non-significant findings from the CMHI and social distance scales could be due to a small male sample size more than anything; the risk of type 1 error is very small since only two out of six scale results were found to be non-significant (Stangor, 2014), however, more research must be carried out with a larger male sample to properly explore gender differences in attitudes towards mental health.
Hypothesis Two
Females generally scored higher on the empathy scale than males and this was to a significant level which means that the hypothesis that females will have more empathy than males is accepted and supports findings of previous research mentioned in the introduction (Eisenberg & Lennon, 1983; Rueckert, 2011; Rueckert & Naybar, 2008; Toussainta & Webb, 2005).
Hypothesis Three
34

Michelle Rodriguez 12404089 PSY4001
Contrary to the hypothesis that attitudes towards depression would generally be more positive than attitudes towards schizophrenia, it was found that participants in the schizophrenia condition had the best attitudes towards mental health whereas participants in the depression condition actually had the worst attitudes towards mental health overall; this was deduced from the findings of a significant difference on authoritarianism and CMHI scores between the schizophrenia and depression conditions. This does not support the findings of vast research in which people have generally better attitudes towards depression than schizophrenia (Angermeyer & Matschinger, 2003a; Angermeyer & Matschinger, 2003b; Eker, 1989). However, it does support the findings of Ozmen, et al. (2004) and Kurihara, et al. (2000) which showed that attitudes towards mental health are not as straightforward as they seem since schizophrenia is a diagnosis that comes with the stigma of dangerousness and unpredictableness whereas depression is generally viewed as vulnerability which would lead many to predict that people would favour depression over schizophrenia but for some reason, these studies have found the opposite. This study’s findings, along with those of Ozmen, et al. (2004) and Kurihara, et al. (2000), are the start of a new and intriguing perspective towards the vast unpredictableness of attitudes towards mental health which challenges the way these diagnoses are predicted to be perceived when compared to one another. This opens up a path for the need of further study into the way the general public reacts to and how they perceive depression and schizophrenia.
Hypothesis Four
There were no significant differences of empathy between the depression, schizophrenia, and non-diagnosis conditions, however, Empathy had a significant positive correlation with benevolence and CMHI scores and a significant negative correlation with social restrictiveness which means that participants with higher empathy levels also scored higher on the benevolence and CMHI scales but lower on the social restrictiveness scale;
35

Michelle Rodriguez 12404089 PSY4001
this means that participants who had more empathy also had a more positive attitude towards mental health. These findings support the hypothesis that people with higher levels of empathy will have better attitudes towards mental health overall. And this is in agreement with the research mentioned in the introduction by Àstrom, et al. (1990), Batson, et al. (1997) and Elizur & Rosenheim (1982) as they all also found that empathy correlated positively with better attitudes towards mental health.
Further Discussion
Even though the linearity of regression assumption was not met for the ANCOVA test, the scatterplots comparing all three conditions and their scores for benevolence and social restrictiveness against empathy scores (see appendices 10 and 12 respectively) show that the depression and schizophrenia conditions do follow a correlational pattern since as empathy scores increase, so do benevolence scores whereas social restrictiveness scores decrease as empathy scores increase which shows that participants do tend to have a better attitude towards mental health, the more empathetic they are.
Participants in the depression condition seemed to naturally be less empathetic than participants in the non-diagnosis and schizophrenia conditions, this could be due to sampling error even though allocation of participants was random so the chance that sampling error occurred is very low. Another explanation for the lack of empathy for participants in the depression condition is that no matter what vignette or description of an unknown person participants are given, the fact that they have no ties to this person and already probably have their own opinions and attitudes towards mental health formed means that they will not change their minds about how they view mental health and depression particularly. This is interesting and gives grounds for conducting more research into attitudes towards mental health to find out whether people view depression in a less favourable light because they get so much exposure
36

Michelle Rodriguez 12404089 PSY4001
to it from the media and those around them or if there are other factors affecting this. For example, from the results of this study, it appears that empathy has an impact on some areas of attitudes towards mental illness but not others as discussed previously and Rueckert & Naybar (2008) found that there is a neural basis for gender differences in empathy which could play a big role in why women are found to be more empathetic than men in general and future research could look at these neurological differences to tie in to what was discussed above about whether empathy could be changed through a number of methods.
The study did not look at age, ethnicity, occupation, level of education, or socio-economic background as variables when researching attitudes towards mental health since most of the participants were undergraduate students. However, since previous research has found that these all play an important role in shaping people’s attitudes towards mental health (Adewuya & Makanjuola, 2008; Lauber, et al., 2000; Lopez, 1991; Stuart & Arboleda-Flórez, 2001; Ukpong & Abasiubong, 2010); it is suggested that future research takes these factors into account as asks participants their age, ethnicity, occupation, level of education, and socio-economic background as well as their level of experience and/or knowledge of mental illness since previous research has found differing results, with some finding that people with better knowledge of mental illness show more positive attitudes towards mental health (Angermeyer, et al., 2004; Siu, et al., 2012), and others finding that knowledge plays a negative part on people’s and professional’s attitudes towards mental health (Angermeyer & Matschinger, 2005; Jorm, et al., 1999; Nordt et al., 2006), and there has even been a study where it was found that that knowledge played no real part in attitudes people have towards mental health (Malla & Shaw, 1987). So as can be seen, the knowledge factor should be investigated more as scholars have yet to come to an agreement about what part, if any, knowledge plays upon the formation of attitudes towards mental health. Of course, it could be consequential that maybe it all depends on empathy levels and whether people know a person with
37

Michelle Rodriguez 12404089 PSY4001
mental health issues personally and whether they are close to them or not, etc. The next step is researching how we can impact empathy and whether it is possible to change it with intervention plans, empathy exercises, and so on as many aspects of people’s lives can influence the attitudes they hold towards mental illness which is why it would be interesting to see to what extent this is true and for which aspects which is why more research must be conducted to better understand the relationships of many difference factors affecting attitudes towards mental health.
However, the fact that this study used a self-selected sample and was online and not restricted to just university students means that the sample gathered was more representative of the general population so it is very likely that various people part of different age and socio-economic groups, for example, took part in the research although it would have been interesting to gather data about such things as discussed above. Participants had the ability to complete the study in their own time and in a place they felt comfortable, without the researcher or anyone being present since it was an online study which lowers any procedural bias. However, most participants gathered using the student participant pool had to take part in student research in order to receive credits as a requirement of their course which can be a disadvantage as they could potentially be more likely to quickly fill in the questionnaires without really reading the questions properly so that they get it over with quickly and are awarded their credits since mandatory participation seems to have some unintended side effects (Bullen, 2007) but since not all of the participants were recruited that way, this should not have affected the results significantly.
There is potential for practical applications of the results from this study to be used in a positive and helpful manner. For example, since this study has found that empathy levels significantly correlate with better attitudes towards mental health, these findings could be implemented in
38

Michelle Rodriguez 12404089 PSY4001
educational settings through intervention programmes in which people are taught to be more empathetic with activities so that they can practice being more empathetic which has real potential to help those involved to develop more positive attitudes towards mental health; this could be particularly helpful for young people who are still developing their views towards everything including mental illness and are more susceptible to intervention programmes. This application is in concurrence with previous research mentioned in the introduction in which interventions to make people, especially young people, aware of mental illness through programmes to educate them and improve their attitudes towards mental health have been shown to work (Altindag, et al., 2006; Dietrich, et al., 2010; Schulze, et al., 2003). However, the implementation must be ongoing in order for it to reach its full potential. Of course, more research into this area should be conducted to find out the ideal target population and using a much bigger sample. Another interesting idea would be to check empathy and attitude scores of participants every week or every month to see how these change over time and these could also be used to gauge how much the intervention plan is working.
Overall, the current research into attitudes towards mental health is vast yet there are many key findings that contradict each other such as whether knowledge makes for better or worse attitudes towards mental illness and whether people have better attitudes towards depression or schizophrenia. This makes for many gaps in research which is why there was a need for the carrying out of this study and even further research in order to be able to come to a more all-round and holistic conclusion on the subject which will take time but these research are the stepping stones which open the door for future knowledge.
39

Michelle Rodriguez 12404089 PSY4001
ReferencesAdewuya, A., & Makanjuola, R. (2008). Social distance towards people with
mental illness in southwestern Nigeria. Aust N Z J Psychiatry, 389-395.
Altindag, A., Yanik, M., Ucok, A., Alptekin, K., & Ozkan, M. (2006). Effects of an antistigma program on medical students’ attitudes towards people with schizophrenia. Psychiatry and Clinical Neurosciences, 283–288.
40

Michelle Rodriguez 12404089 PSY4001
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5 ed.). Arlington, VA: American Psychiatric Publishing.
Ang, R. P., Lim, K. M., Tan, A. G., & Yau, T. Y. (2004). Effects of gender and sex role orientation on help-seeking attitudes. Current Psychology, 23(3), 203-214.
Angermeyer, M. C., & Matschinger, H. (1996). The effect of violent attacks by schizophrenic persons on the attitude of the public towards the mentally ill. Social Science & Medicine, 1721–1728.
Angermeyer, M. C., & Matschinger, H. (2003a). The stigma of mental illness: effects of labelling on public attitudes towards people with mental disorder. Acta Psychiatrica Scandinavica, 304–309.
Angermeyer, M. C., & Matschinger, H. (2003b). Public beliefs about schizophrenia and depression: similarities and differences. Social Psychiatry and Psychiatric Epidemiology, 526-534.
Angermeyer, M. C., & Matschinger, H. (2005). Causal beliefs and attitudes to people with schizophrenia. The British Journal of Psychiatry, 331-334.
Angermeyer, M. C., Matschinger, H., & Corrigan, P. W. (2004). Familiarity with mental illness and social distance from people with schizophrenia and major depression: testing a model using data from a representative population survey. Schizophrenia Research, 175–182.
Àstrom, S., Nilsson, M., Norberg, A., & Winblad, B. (1990). Empathy, experience of burnout and attitudes towards demented patients among nursing staff in geriatric care. Journal of Advanced Nursing, 1236–1244.
Batson, D., Polycarpou, P., & Harmon-Jones, E. (1997). Empathy and attitudes: Can feeling for a member of a stigmatized group improve
41

Michelle Rodriguez 12404089 PSY4001
feelings toward the group? Journal of Personality and Social Psychology, 72(1), 105-118.
Berger, J. M., Levant, R., McMillan, K. K., Kelleher, W., & Sellers, A. (2005). Impact of Gender Role Conflict, Traditional Masculinity Ideology, Alexithymia, and Age on Men's Attitudes Toward Psychological Help Seeking. Psychology of Men & Masculinity, 6(1), 73-78.
Björkman, T., Angelman, T., & Jönsson, M. (2008). Attitudes towards people with mental illness: a cross-sectional study among nursing staff in psychiatric and somatic care. Scandinavian Journal of Caring Sciences, 170–177.
Bogardus, E. S. (1933). A Social Distance Scale. Sociology and Social Research, 265-271.
Broverman, I. K., Vogel, S. R., Broverman, D. M., Clarkson, F. E., & Rosenkrantz, P. S. (1972). Sex‐Role Stereotypes: A Current Appraisal. Journal of Social issues, 22(2), 59-78.
Buchegger-Traxler, A., & Sirsch, U. (2012). The impact of risk and protective factors on mental health and well-being - Austrian adolescents and migrant adolescents from war-affected countries. Italian Journal of Public Health.
Bullen, M. (2007). Participation and critical thinking in online university distance education. International Journal of E-Learning & Distance Education, 13(2), 1-32.
Caruso, D. R., & Mayer, J. D. (1998). A Measure of Emotional Empathy for Adolescents and Adults. Unpublished Manuscript.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. New Jersey: Lawrence Erlbaum.
Dancey, C. P., & Reidy, J. (2011). Statistics Without Maths for Psychology. Essex: Pearson Education Limited.
42

Michelle Rodriguez 12404089 PSY4001
Davis, M. H. (1980). A Multidimensional Approach to Individual Differences in Empathy. 85.
Diefenbach, D. L., & West, M. D. (2007). Television and attitudes toward mental health issues: Cultivation analysis and the third-person effect. Journal of Community Psychology, 181–195.
Dietrich, S., Mergl, R., Freudenberg, P., Althaus, D., & Hegerl, U. (2010). Impact of a campaign on the public's attitudes towards depression. Health Education Research, 135-150.
Eisenberg, N., & Lennon, R. (1983). Sex differences in empathy and related capacities. Psychological Bulletin, 100-131.
Eker, D. (1989). Attitudes toward mental illness: Recognition, desired social distance, expected burden and negative influence on mental health among Turkish freshmen. Social Psychiatry and Psychiatric Epidemiology, 146-150.
Elizur, A., & Rosenheim, E. (1982). Empathy and attitudes among medical students: the effects of group experience. Academic Medicine, 57(9), 675-683.
Fink, P. J. (1992). Stigma and Mental Illness. Washington: American Psychiatric Press.
Gonzalez, J. M., Alegria, M., & Prihoda, T. J. (2005). How do attitudes toward mental health treatment vary by age, gender, and ethnicity/race in young adults? Journal of Community Psychology, 611–629.
Granello, D. H., Pauley, P. S., & Carmichael, A. (1999). Relationship of the Media to Attitudes Toward People With Mental Illness. The Journal of Humanistic Counseling, Education and Development, 39, 98–110.
Hoffman, M. L. (1977). Sex differences in empathy and related behaviors. Psychological bulletin, 712-722.
43

Michelle Rodriguez 12404089 PSY4001
Hugo, C. J., Boshoff, D. E., Traut, A., Zungu-Dirwayi, N., & Stein, D. J. (2003). Community attitudes toward and knowledge of mental illness in South Africa. Social Psychiatry and Psychiatric Epidemiology , 715-719.
Jorm, A. F., Korten, A. E., Jacomb, P. A., Christensen, H., & Henderson, S. (1999). Attitudes towards people with a mental disorder: a survey of the Australian public and health professionals. Australian and New Zealand Journal of Psychiatry, 77-83.
Judd, F., Komiti, A., & Jackson, H. (2008). How does being female assist help-seeking for mental health problems? Australasian Psychiatry, 42(1), 24-29.
Kurihara, T., Kato, M., Sakamoto, S., Reverger, R., & Kitamura, T. (2000). Public attitudes towards the mentally ill: A cross-cultural study between Bali and Tokyo. Psychiatry and Clinical Neurosciences, 547–552.
Lauber, C., Nordt, C., Falcato, L., & Rössler, W. (2000). Public acceptance of restrictions on mentally ill people. Acta Psychiatrica Scandinavica, 26-32.
Lawson, A., & Fouts, G. (2004). Mental illness in Disney animated films. Canadian journal of psychiatry, 49(5), 310-314.
Leong, F. T., & Zachar, P. (1999). Gender and opinions about mental illness as predictors of attitudes toward seeking professional psychological help. British Journal of Guidance and Counselling, 27(1), 123-132.
Lopez, L. R. (1991). Adolescents' attitudes toward mental illness and perceived sources of their attitudes: An examination of pilot data. Archives of Psychiatric Nursing, 271–280.
Mackenzie, C. S., Gekoskia, W. L., & Knox. (2006). Age, gender, and the underutilization of mental health services: The influence of help-
44

Michelle Rodriguez 12404089 PSY4001
seeking attitudes. Aging & Mental Health, 574-582.
Mahalik, J. R., Burns, S. M., & Syzdek, M. (2007). Masculinity and perceived normative health behaviors as predictors of men's health behaviors. Social Science & Medicine, 2201–2209.
Malla, A., & Shaw, T. (1987). Attitudes towards mental illness: the influence of education and experience. Int J Soc Psychiatry, 33-41.
Möller-Leimkühler, A. M. (2002). Barriers to help-seeking by men: a review of sociocultural and clinical literature with particular reference to depression. Journal of Affective Disorders, 1–9.
Morrison, R. (2011). Nursing Students’ Attitudes toward People with Mental Illness: Do they change after instruction and clinical exposure?
NICE. (2009). Core Interventions In The Treatment And Management Of Schizophrenia In Primary And Secondary Care. Retrieved from http://www.nice.org.uk/guidance/cg82
Nolan, P. (2000). A History of Mental Health Nursing. Cheltenham: Nelson Thornes.
Nordt, C., Rössler, W., & Lauber, C. (2006). Attitudes of Mental Health Professionals Toward People With Schizophrenia and Major Depression. Schizophrenia Bulletin, 709-714.
Ojeda, V. D., & Bergstresser, S. M. (2008). Gender, race-ethnicity, and psychosocial barriers to mental health care: An examination of perceptions and attitudes among adults reporting unmet need. Journal of Health and Social Behavior, 49(3), 317-334.
Ozmen, E., Ogel, K., Aker, T., Sagduyu, A., Tamar, D., & Boratav, C. (2004). Public attitudes to depression in urban Turkey. Social Psychiatry and Psychiatric Epidemiology, 1010-1016.
45

Michelle Rodriguez 12404089 PSY4001
Prentice, D. A., & Carranza, E. (2002). What women and men should be, shouldn’t be, are allowed to be, and don’t have to be: The contents of prescriptive gender stereotypes. Psychology of Women Quarterly, 26(4), 269-281.
Rabkin, J. (1974). Public attitudes toward mental illness. Schizophrenia Bulletin, 1(10), 9-33.
Reavley, N. J., & Jorm, A. F. (2011). Stigmatizing Attitudes towards People with Mental Disorders: Findings from an Australian National Survey of Mental Health Literacy and Stigma. Australian & New Zealand Journal of Psychiatry, 1086-1093.
Rueckert, L. (2011). Gender differences in empathy. . Psychology of empathy, 221-234.
Rueckert, L., & Naybar, N. (2008). Gender differences in empathy: The role of the right hemisphere. Brain and cognition, 162-167.
Sarbin, T. R., & Mancuso, J. C. (1970). Failure of a moral enterprise: Attitude of the public toward mental illness. Journal of Consulting and Clinical Psychology, 35(2), 159-173.
Schulze, B., Richter-Werling, M., Matschinger, H., & Angermeyer, C. (2003). Crazy? So what! Effects of a school project on students' attitudes towards people with schizophrenia. Acta Psychiatrica Scandinavica, 142–150.
Singleton, N., Bumpstead, R., O’Brien, M., Lee, A., & Meltzer, H. (2001). Psychiatric Morbidity Among Adults Living In Private Households 2000. London: The Stationery Office.
Siu, B., Chow, K., Lam, L., Chan, W., Tang, V., & Chui, W. (2012). A Questionnaire Survey on Attitudes and Understanding towards Mental Disorders. East Asian Arch Psychiatry, 18-24.
Stangor, C. (2014). Research Methods for the Behavioral Sciences. Boston: Cengage Learning.
46

Michelle Rodriguez 12404089 PSY4001
Stuart, H., & Arboleda-Flórez, J. (2001). Community Attitudes Toward People With Schizophrenia. Can J Psychiatry, 245–252.
Taylor, S. M., & Dear, M. J. (1981). Scaling Community Attitudes Toward the Mentally Ill. Schizophrenia Bulletin, 225-240.
Thornton, J. A., & Wahl, O. F. (1995). Impact of a newspaper article on attitudes toward mental illness. Journal of Community Psychology, 17-25.
Toussainta, L., & Webb, J. R. (2005). Gender Differences in the Relationship Between Empathy and Forgiveness. The Journal of Social Psychology, 673-685.
Ukpong, D. I., & Abasiubong, F. (2010). Stigmatising attitudes towards the mentally ill: A survey in a Nigerian university teaching hospital. Scholars Academic Journal of Pharmacy, 58-60.
Wahl, O. (2003). Depictions of mental illnesses in children's media. Journal of Mental Health, 12(3), 249-258.
Wahl, O. F., & Lefkowits, J. Y. (1989). Impact of a television film on attitudes toward mental illness. American Journal of Community Psychology, 521-528.
Wilson, C., Nairn, R., Coverdale, J., & Panapa, A. (2000). How mental illness is portrayed in children's television. The British Journal of Psychiatry, 440-443.
World Health Organisation. (2001). The World health report: 2001: Mental health: new understanding, new hope.
Wright, K. B. (2005). Researching Internet-Based Populations: Advantages and Disadvantages of Online Survey Research, Online Questionnaire Authoring Software Packages, and Web Survey Services. Journal of Computer-Mediated Communication, 10, 00.
47

Michelle Rodriguez 12404089 PSY4001
Appendices
1. Information Sheet
48

Michelle Rodriguez 12404089 PSY4001
Information Sheet
This study is being carried out for a dissertation as part of a BSc Psychology degree at the University of Northampton.
You will need to be over 18 years old and may withdraw your data and it will be destroyed and not used in the research at any point during the course of the study up until a week after you have participated. All data gathered will be kept strictly confidential and only the researcher and their supervisor may look at it. Your data will be stored securely in the researcher’s laptop; all paper documentation will be kept under lock and key and these will only be used for the purpose of the study.
This study is looking at attitudes towards mental health, to do so I will need you to firstly fill out a questionnaire about empathy and then read the description of a person’s day and use that information to fill out two more questionnaires about your attitudes. The study should not take morethan 30 minutes to complete and there are no known risks involved to youor any other person by participating.
You may obtain a summary of results after the study has ended and data has been analysed if you wish; just contact me at [email protected] my supervisor’s contact details are [email protected]
The research adheres to the BPS Code of Ethics and Conduct and the study has been approved by the Psychology Division Ethics Panel.
2. Consent Form
49

Michelle Rodriguez 12404089 PSY4001
Consent Form
By ticking these boxes you are agreeing to partake in the following study and consenting for the data gathered to be used by the researcher in theirPsychology dissertation.
You are over 18 years old
You have read the informationsheet, understand the nature ofthe study, and wish to take part
You understand that participationis completely voluntary
You understand that up until aweek after your participation,you may withdraw your data atany moment if you wish and bydoing so any data gathered willbe destroyed and not used in theresearch
You understand that all informationgathered is strictly anonymous andconfidential – no identifyinginformation will be asked of you.You will be given a uniqueIdentification number in case youwish to contact the researcher
3. Debrief Sheet
50

Michelle Rodriguez 12404089 PSY4001
Debrief
Thank you for taking part in this study about attitudes towards mental health. Data gathered will be used to examine whether people with greater empathy have better attitudes towards mental health and particularly, whether people have a better attitude towards depression over schizophrenia, or the other way around. Finally, the gender differences of these will be explored. If you have any further queries or concerns about this research, you may contact me at
4. Vignette
A Day in the Life of Sam
Sam has been diagnosed with Major Depression Disorder (or ‘Schizophrenia’ or ‘has no mental health issues’ depending on which diagnosis participants read)
Sam’s day hasn’t been going very well, he/she feels sad for no apparent reason; all he/she wants is to be alone and as soon as Sam got home fromwork, he/she started crying uncontrollably. Sam doesn’t want to be this way but he/she doesn’t know what to do about it. All of Sam’s co-workers commented on his/her change of mood today and his/her boss warned Sam about controlling him/herself in the workplace. Sam now feels like
5. Multidimensional Emotional Empathy Scale
Multi-Dimensional Emotional Empathy Scale
51

Michelle Rodriguez 12404089 PSY4001
The following 30 questions are designed to measure your emotional empathy level, please answer as truthfully and quickly as you can. The scale used ranges from 1 to 5, 1 being ‘Strongly Disagree’, and 5 being ‘Strongly Agree’.
1. I feel like crying when watching a sad movie.
1 2 3 4 5
2. Certain pieces of music can really move me.
1 2 3 4 5
3. Seeing a hurt animal by the side of the road is very upsetting.
1 2 3 4 5
4. R - I don't give others' feelings much thought.
1 2 3 4 5
5. It makes me happy when I see people being nice to each other.
1 2 3 4 5
6. The suffering of others deeply disturbs me.
1 2 3 4 5
7. I always try to tune in to the feelings of those around me.
1 2 3 4 5
8. I get very upset when I see a young child who is being treated meanly.
1 2 3 4 5
9. R - Too much is made of the suffering of pets or animals.
1 2 3 4 5
10. If someone is upset I get upset, too.
1 2 3 4 5
11. When I'm with other people who are laughing I join in.
52

Michelle Rodriguez 12404089 PSY4001
1 2 3 4 5
12. It makes me mad to see someone treated unjustly.
1 2 3 4 5
13. R - I rarely take notice when people treat each other warmly.
1 2 3 4 5
14. I feel happy when I see people laughing and enjoying themselves.
1 2 3 4 5
15. It's easy for me to get carried away by other people's emotions.
1 2 3 4 5
16. R - My feelings are my own and don't reflect how others feel.
1 2 3 4 5
17. If a crowd gets excited about something so do I.
1 2 3 4 5
18. I feel good when I help someone out or do something nice for someone.
1 2 3 4 5
19. I feel deeply for others.
1 2 3 4 5
20. R - I don't cry easily.
1 2 3 4 5
21. I feel other people's pain.
1 2 3 4 5
22. Seeing other people smile makes me smile.
1 2 3 4 5
23. Being around happy people makes me feel happy, too.
53

Michelle Rodriguez 12404089 PSY4001
1 2 3 4 5
24. TV or news stories about injured or sick children greatly upset me.
1 2 3 4 5
25. I cry at sad parts of the books I read.
1 2 3 4 5
26. Being around people who are depressed brings my mood down.
1 2 3 4 5
27. R - I find it annoying when people cry in public.
1 2 3 4 5
28. It hurts to see another person in pain.
1 2 3 4 5
29. I get a warm feeling for someone if I see them helping another person.
1 2 3 4 5
30. I feel other people's joy.
1 2 3 4 5
Note: R indicates a reverse-scored item. To score the scale, change the scoring on the reverse-scored items (1=5, 2=4, 3=3, 4=2, 5=1). Add all the scores for the Total score and divide by 30. Add the following items together for each scale, and divide by the number of items: Suffering ( 3, 5, 6, 8, 12, 18, 24, 28); Positive Sharing (14, 22, 23, 29, 30); Responsive Crying (1, 20, 25); Emotional Attention (4, 9, 13, 27); Feel for Others (10, 15, 16, 21); Emotional Contagion (11, 17). Take the mean of these sub-scales to compute a General Empathy scale.6. Community Attitudes towards the Mentally Ill (CAMI) scale
COMMUNITY ATTITUDES TOWARDS THE MENTALLY ILL
The following 40 statements express various opinions about mental illness and the mentally ill. The mentally ill refers to people needing treatment for mental disorders but who are capable of independent living outside a hospital. Please choose the response which most accurately describes your reaction to each statement (SA= Strongly Agree; A= Agree; N=
54

Michelle Rodriguez 12404089 PSY4001
Neither Agree Nor Disagree; D= Disagree; SD= Strongly Disagree). It's your first reaction which is important. Don't be concerned if some statements seem similar to ones you have previously answered. Please be sure to answer all statements.
1. As soon as a person shows signs of mental disturbance, he should be hospitalized.
SA A N D SD
2. More tax money should be spent on the care and treatment of the mentally ill.
SA A N D SD
3. The mentally ill should be isolated from the rest of the community.
SA A N D SD
4. The best therapy for many mental patients is to be part of a normal community.
SA A N D SD
5. Mental illness is an illness like any other.
SA A N D SD
6. The mentally ill are a burden on society.
SA A N D SD
7. The mentally ill are far less of a danger than most people suppose.
SA A N D SD
8. Locating mental health facilities in a residential area downgrades the neighbourhood.
SA A N D SD
9. There is something about the mentally ill that makes it easy to tell them from other people.
SA A N D SD
10. The mentally ill have for too long been the subject of ridicule.
SA A N D SD
55

Michelle Rodriguez 12404089 PSY4001
11. A woman would be foolish to marry a man who has suffered from mental illness, even though he seems fully recovered.
SA A N D SD
12. As far as possible mental health services should be provided through community-based facilities.
SA A N D SD
13. Less emphasis should be placed on protecting the public from the mentally ill.
SA A N D SD
14. Increased spending on mental health services is a waste of tax money.
SA A N D SD
15. No one has the right to exclude the mentally ill from their neighbourhood.
SA A N D SD
16. Having mental patients living within residential neighbourhoods might be good therapy, but the risks to residents are too great.
SA A N D SD
17. Mental patients need the same kind of control and discipline as a young child.
SA A N D SD
18. We need to adopt a far more tolerant attitude toward the mentally ill in our society.
SA A N D SD
19. I would not want to live next door to someone who has been mentally ill.
SA A N D SD
20. Residents should accept the location of mental health facilities in their neighbourhood to serve the needs of the local community.
SA A N D SD
56

Michelle Rodriguez 12404089 PSY4001
21. The mentally ill should not be treated as outcasts of society.
SA A N D SD
22. There are sufficient existing services for the mentally ill.
SA A N D SD
23. Mental patients should be encouraged to assume the responsibilities of normal life.
SA A N D SD
24. Local residents have good reason to resist the location of mental health services in their neighbourhood.
SA A N D SD
25. The best way to handle the mentally ill is to keep them behind locked doors.
SA A N D SD
26. Our mental hospitals seem more like prisons than like places where the mentally ill can be cared for.
SA A N D SD
27. Anyone with a history of mental problems should be excluded from taking public office.
SA A N D SD
28. Locating mental health services in residential neighbourhoods does not endanger local residents.
SA A N D SD
29. Mental hospitals are an outdated means of treating the mentally ill.
SA A N D SD
30. The mentally ill do not deserve our sympathy.
SA A N D SD
31. The mentally ill should not be denied their individual rights.
57

Michelle Rodriguez 12404089 PSY4001
SA A N D SD
32. Mental health facilities should be kept out of residential neighbourhoods.
SA A N D SD
33. One of the main causes of mental illness is a lack of self-discipline and will power.
SA A N D SD
34. We have the responsibility to provide the best possible care for the mentally ill.
SA A N D SD
35. The mentally ill should not be given any responsibility.
SA A N D SD
36. Residents have nothing to fear from people coming into their neighbourhood to obtain mental health services.
SA A N D SD
37. Virtually anyone can become mentally ill.
SA A N D SD
38. It is best to avoid anyone who has mental problems.
SA A N D SD
39. Most women who were once patients in a mental hospital can be trusted as baby sitters.
SA A N D SD
40. It is frightening to think of people with mental problems living in residential neighbourhoods.
SA A N D SD
58

Michelle Rodriguez 12404089 PSY4001
Key to items ScoringSA A N D SD
AuthoritarianismPro: 1, 9, 17, 25, 33 5 4 3 2 1
Con: 5, 13, 21, 29, vvvvvvvvv37
1 2 3 4 5
BenevolencePro: 2, 10, 18, 26, 34 5 4 3 2 1
Con: 6, 14, 22, 30, 38 1 2 3 4 5
Social Restrictiveness
Pro: 3, 11, 19, 27, 35 5 4 3 2 1
Con: 7, 15, 23, 31, 39 1 2 3 4 5
Community Mental Health Ideology
Pro: 4, 12, 20, 28, 36 5 4 3 2 1
Con: 8, 16, 24, 32, 40 1 2 3 4 5
7. Social Distance Scale (SDS)
Social Distance Scale
Please answer the following questions, ticking Yes or No for each, considering the description of the person you just read.
1. Would marry Yes No
2. Would have as regular friends Yes No
3. Would work beside in an office Yes No
4. Would have several families in my neighbourhood Yes No
5. Would have merely as speaking acquaintances Yes No
6. Would have live outside my neighbourhood Yes No
7. Would have live outside my country Yes No
59

Michelle Rodriguez 12404089 PSY4001
Item ScoringYes No
1, 2, 3, 4 1 25, 6, 7 2 1
8. Ethics Application Form
Before completing this ethics application you are strongly advised to consult the guidelines and documentation on ethics applications.
You must meet and discuss ethical considerations relating to your study with your supervisor before submitting your application to them.
You will find a full list of Ethics Committee deadlines and meeting dates on NILE. You must submit your ethics application by the deadline for your application to be considered within that time period. Please familiarise yourself with the date of the final deadline and do not leave discussions with supervisors until the last minute.
60
Psychology Ethics Application Form

Michelle Rodriguez 12404089 PSY4001
RISK ASSESSMENT
Does the Study Involve any of the following? YES NO
1 The study involves participants who are under the age of 16
2 The study involves participants who are particularly vulnerable or unable to give informed consent or in a dependent position (e.g. vulnerable children, people with learning difficulties, over-researched groups or people in care facilities).
3a Participants will be taking part in the study without their consent or knowledge at the time and no deception of any sort will be used (this might for example be the covert observation of people in non-public places).
3b The study involves a level of deception
4 There is a risk that the nature of the research topic might lead to disclosures from the participant concerning their own involvement in illegal activities or other activities that represent a risk to themselves or others (e.g. sexual activity, drug use or professional misconduct).
5 The study has a significant risk of inducing psychological stress or anxiety, lead to humiliation, cause harm or any negative consequences beyond the risks encountered in the participants normal lives
6 Drugs, placebos or other non-food substances will be administered as part of this study and/or invasive, intrusive or potentially harmful procedures of any kind will be used
If you have ticked Yes to Q1 or 2 of the risk assessment please indicate who you are doing research with in Question 7 and 8. If you have ticked NO to Q 1 or 2 please leave Q 7 and 8 blank.
61
Please read through the following checklists and tick the most appropriate answer. To “check” a box double click on the box and select “checked” in the Default Value section.

Michelle Rodriguez 12404089 PSY4001
If you ticked Yes to Q1 or 2 please complete the following: Yes No
7 Does your project involve work with animals?
8 Do participants fall into any of the following special groups?
If they do, please refer to the university and BPS ethical guidelines and outline how you will deal with this on page 2.
N.B. Any research involving the NHS MUST gain appropriate LREC ethical clearance
Note that you may also need to obtain satisfactory Criminal Records Bureau (CRB) clearance
Schoolchildren(under 18 years of age)
People with learning or communication difficulties
Patients
People in custody
People engaged in illegal activities (e.g. drug-taking)
OTHER INFORMATION RELATING TO RISK
Will the study place the researcher at any risk greater than that encountered in his/her daily life? (e.g. interviewing alone or in dangerous circumstances, or data collection outside the UK).
Yes No
62

Michelle Rodriguez 12404089 PSY4001
Supervisors – please note that by meeting and advising your students about ethical concerns and considerations as well as checking the ethics documents this will aid a smooth process through the ethics application process. By supporting your students you, as a supervisor, are indicating that you are familiar with the University of Northampton and the BPS guidelines for ethical practices in psychological research and approve this project
DIVISION OF PSYCHOLOGY DISSERTATION ETHICS FORM
Tick one box: Undergraduate project Postgraduate project
Title of project:
Attitudes Towards Mental Health
Name of researcher(s):
Michelle Rodriguez
Researchers Email:
Name of supervisor:
Lesley-Ann Smith
Yes No N/A
1 Will you describe the main research procedure to participants in advance, so that they are informed what to expect?
2 Will you tell participants that their participation is voluntary?
63

Michelle Rodriguez 12404089 PSY4001
3 Will you obtain written consent from participants? (please include the consent form with your ethics submission)
4 If the research is observational, will you ask participants for their consent to being observed?
5 Will you tell participants that they may withdraw from the research at any time without needing to provide a reason?
6 With questionnaires/interviews, will you give participants the option of omitting questions they do not want to answer?
7 Will you tell participants that their data will be treated with full confidentiality and that, if published, it should not be identifiable as theirs?
8 Will you debrief participants at the end of their participation (i.e. give them a brief explanation of the study)?
If you have ticked NO to any question from 1- 8 you must provide a full explanation for the ethics panel for your decision within the following sections of the ethics application
Please provide full details of your project below
(if insufficient detail is provided and the precise nature of the study is unclear then the Ethics panel will not be able to approve the project and your form will be returned)
NB. The Psychology Division does NOT permit the use of NILE to send out unsolicited requests for participants or to distribute questionnaires
SECTION 1: AIMS, OBJECTIVES AND NATURE OF STUDY
Provide the academic/scientific justification of the study as well as detailing and explaining the principal research question, objectives and hypotheses to be tested. This should be in no more than 500 words and include at least 2 references.
Attitudes towards mental health have never been very positive, people tend to stigmatise mental illness. Much of this is believed to come from actual knowledge of what mental illness is; Angermeyer, Matschinger, & Corrigan (2004) has found that incresead familiarity with mental illness led to a weaker desire for social distance. However, other research has found that mental health professionals held more negative stereotypes towards mental illness than the general population (Nordt, Rössler, & Lauber, 2006) which contradicts the notion that with more knowledge comes more acceptance and a better attitude. For this reason, it is important to carry out more research concerning this topic to see if people who have experienced or had contact with mental illness are generally more understanding or if this makes no difference towards their attitude. Therefore, a
64

Michelle Rodriguez 12404089 PSY4001
hypothesis that will be tested is that people with more knowledge about mental health will have better attitudes towards it than those who do not. For this research, attitudes towards Schizophrenia and Depression will be assesed as much of the research focuses on mainly those two diagnoses. Gender differences will also be explored as it has been found that males generally reported a more negative attitude towards mental illness than females (Gonzalez, Alegria, & Prihoda, 2005) therefore, another hypothesis to be tested will be that females will generally have a more positive attitude towards mental health than males. A third hypothesis for this research is that people with higher levels of empathy will have better attitudes towards mental health as research by Àstrom, Nilsson, Norberg, & Winblad (1990) has found evidence for this.
SECTION 2. STUDY DESIGN/METHODOLOGY, DATA COLLECTION & ANALYSIS
Provide a brief outline of the step-by-step procedure of your proposed study in lay language, in no more than 500 words where possible. Extensive research protocols that have been prepared for funding bodies or similar organisations are likely to be of too technical a nature, or will provide more information than is necessary for ethical review/approval. Please ensure you focus on using non-technical lay language throughout, outlining clearly and simply the methodology to be used in your study.
Participants will be approached, whether through a student poll or online through social media to complete an empathy scale questionnaire, then be randomly allocated to read a description of a day in the life of a person either diagnosed with Depression, Schizophrenia, or not diagnosed and deemed normal and complete a further two questionnaires assessing their attitudes towards mental health. The Multi-Dimensional Empathy Scale will be used to analyse participants’ empathy as it was hypothesised that people with more empathy will have more positive attitudes towards mental health and much research has supported the use of a multi-dimensional approach to empathy using this scale and the reliability for all scale scores was found to be moderate to high which makes this a good scale (Caruso & Mayer, 1998). An identic description of ‘a day in the life of’ a made up individual with either a diagnosis or not will be given to each participant to read after completing the empathy scale, they will then use the information in the description to answer a Social Distance Scale and a Community Attitudes towards Mental Illness (CAMI) Scale which will measure their
65

Michelle Rodriguez 12404089 PSY4001
attitudes. The Social Distance Scale was originally created to measure prejudice towards ethnicity and religion but has since been successfully and validly used in much research to measure attitudes towards mental health which is why it has been chosen for this study (Nordt, Rössler, & Lauber, 2006). The CAMI scale was designed specifically to measure attitudes towards mental illness and has been found to be valid (Taylor & Dear, 1981). The administration of the attitudes scales will be randomised and participants will be randomly allocated to the diagnoses.
MEASURES TO BE USED – Confirm that any measures (such as tests/questionnaires) employed in the research study, but not developed specifically for the study, will be used in accordance with any copyright or licensing conditions that apply.
YES NA
SECTION 3 PARTICIPANTS
3.1 Projected number of participants
80+
3.2 Selection Criteria
Opportunity sample
3.3 Recruitment
Please provide information of where you intend to recruit participants from
Some participants will be recruited around Park campus of The University of Northampton; others will be recruited online through social media (Facebook, etc.)
66

Michelle Rodriguez 12404089 PSY4001
Where will the research take place?
Mainly online, so wherever the participants are at the time, for example, in a classroom located at Park campus
SECTION 4. ETHICAL CONSIDERATIONS
4.1 INFORMED CONSENT
Describe the process you will use to ensure your participants are freely giving fully informed consent to participate. This will always include the provision of an information sheet and will normally require a consent form unless it is a purely self-completion questionnaire based study or there is a justification for not doing so (this must be clearly stated). Templates for Information Sheets and consent forms are available [give NILE site]
An information sheet will be given to participants to read; it will have information explaining what the study is about, following that, they will read a consent form which will inform them of their rights as a participant and that they do not have to take part in the study if they do not wish to do so, they will give informed consent by ticking boxes, for example, they would tick the box next to ‘you are over 18 years old’, showing that they understand and wish to be a participant.
4.2 RIGHT OF WITHDRAWAL
Participants should be able to withdraw from the research process at any time and also should be able to withdraw their data if it is identifiable as theirs and should be told when this will no longer be possible (e.g. once it has been included in the final report). Please describe the exact arrangements for withdrawal from participation and withdrawal of data depending on your study design.
Participants will be informed that participation is fully voluntary and that they have the right to withdraw any data they wish at any time and by doing so, all data gathered will be destroyed and not used in the research up until a week after they have partaken in the study.
67

Michelle Rodriguez 12404089 PSY4001
SECTION 5. DATA PROTECTION, CONFIDENTIALITY, DATA AND RECORDS MANAGEMENT, DISSEMINATION
5.1. Confirm that all processing of personal information related to the study will be in full compliance with the Data Protection Act 1998 including the Data Protection Principles.
YES NO
5.2. What steps will be taken to ensure the confidentiality of personal information? Give details of procedures to maintain the anonymity of data and of physical and technical security measures. Please note: to make data truly anonymous all information that could potentially identify a participant needs to be removed in addition to names. NB: Personally identifiable data held on mobile devices must be encrypted
Participants will be given an identification number that has no association with their person and they won’t need to sign anything so no names will be taken; no personal information will be asked of them.
5.3. Who will have access to personal information relating to this study? Confirm that any necessary wider disclosures of personal information (for instance to colleagues beyond the study team, translators, transcribers, auditors etc) have been properly explained to study participants.
No one else but the researcher and the research supervisor may have access to personal information relating to this study.
5.4. Data management responsibilities after the study.
State how long study information (including research data, consent forms and administrative records) will be retained for: Up until the dissertation grade is obtained.
State in what format(s) the information will be retained (for example, as physical and/or electronic copies): Electronic copies of filled questionnaires will be retained to make data handling easier. All paperwork will be kept securely under lock and key.
NB: Any personally identifiable data that is held on any mobile device should be encrypted. This includes data stored on USB keys, laptop/netbooks, desktop computers, smart phones, workgroup servers and relevant emails
Section 6: Other Ethical Issues
68

Michelle Rodriguez 12404089 PSY4001
Please consider what other ethical issues there are that have not already been addressed elsewhere in the form. Please note that all research projects have some ethical considerations, even if this only relates to how confidentiality will be maintained. DO NOT LEAVE THIS SECTION BLANK
Some options you may consider: dealing with potential distress, fatigue of participant in experimental design, use of direct quotes in qualitative designs.
Participants may become fatigued by a long questionnaire; there is slight potential that some participants may find the topic of mental health distressing. This will be dealt with by giving participants the number to Nightline, the university’s counselling service, on the debrief form so they can talk to someone if they feel upset.
Student checklist Yes No N/A
Have you checked the ethics form and materials for typos and spelling?
Have you included a copy of all of the materials (e.g. recruitment advertisement and participant information sheet, consent form, questionnaires (as they will appear to the participant), interview schedule) with your ethics submission?
Are you conducting this research during a university placement?
Does this research involve any kind of external organisation (e.g. a school, business, charity etc.)?
Does the external organisation require that you have a CRB check (or equivalent for overseas students)?
I am familiar with the University of Northampton and the BPS guidelines for ethical practices in
69

Michelle Rodriguez 12404089 PSY4001
psychological research (and have discussed them with my supervisor)
Signed (student): Michelle Rodriguez Date: 25/11/14
APPENDICES MUST BE ATTACHED HERE
Please include all your supporting documents here (with the exception of letters of consent from external organisations if required)
You should include:
Information Sheet
Information Sheet
This study is looking at attitudes towards mental health, to do so I will need you to firstly fill out a questionnaire about empathy and then read the description of a person’s day and use that information to fill out two more questionnaires about your attitudes. The study should not take morethan 30 minutes to complete and there are no known risks involved to you
Consent form
70

Michelle Rodriguez 12404089 PSY4001
Consent Form
By ticking these boxes you are agreeing to partake in the following study and consenting for the data gathered to be used by the researcher in theirPsychology dissertation.
You are over 18 years old
You have read the informationsheet, understand the nature ofthe study, and wish to take part
You understand that participationis completely voluntary
You understand that up until aweek after your participation,you may withdraw your data atany moment if you wish and bydoing so any data gathered willbe destroyed and not used in theresearch
You understand that all informationgathered is strictly anonymous andconfidential – no identifyinginformation will be asked of you.You will be given a uniqueIdentification number in case youwish to contact the researcher
Interview schedule/ questionnaires (as presented to participants)/ experimental images/ videos/ instructions
Multi-Dimensional Emotional Empathy Scale
The following 30 questions are designed to measure your emotional empathy level, please answer as truthfully and quickly as you can. The scale used ranges from 1 to 5, 1 being ‘Strongly Disagree’, and 5 being ‘Strongly Agree’.
71

Michelle Rodriguez 12404089 PSY4001
1. I feel like crying when watching a sad movie.
1 2 3 4 5
2. Certain pieces of music can really move me.
1 2 3 4 5
3. Seeing a hurt animal by the side of the road is very upsetting.
1 2 3 4 5
4. I don't give others' feelings much thought.
1 2 3 4 5
5. It makes me happy when I see people being nice to each other.
1 2 3 4 5
6. The suffering of others deeply disturbs me.
1 2 3 4 5
7. I always try to tune in to the feelings of those around me.
1 2 3 4 5
8. I get very upset when I see a young child who is being treated meanly.
1 2 3 4 5
9. Too much is made of the suffering of pets or animals.
1 2 3 4 5
10. If someone is upset I get upset, too.
1 2 3 4 5
11. When I'm with other people who are laughing I join in.
1 2 3 4 5
12. It makes me mad to see someone treated unjustly.
1 2 3 4 5
72

Michelle Rodriguez 12404089 PSY4001
13. I rarely take notice when people treat each other warmly.
1 2 3 4 5
14. I feel happy when I see people laughing and enjoying themselves.
1 2 3 4 5
15. It's easy for me to get carried away by other people's emotions.
1 2 3 4 5
16. My feelings are my own and don't reflect how others feel.
1 2 3 4 5
17. If a crowd gets excited about something so do I.
1 2 3 4 5
18. I feel good when I help someone out or do something nice for someone.
1 2 3 4 5
19. I feel deeply for others.
1 2 3 4 5
20. I don't cry easily.
1 2 3 4 5
21. I feel other people's pain.
1 2 3 4 5
22. Seeing other people smile makes me smile.
1 2 3 4 5
23. Being around happy people makes me feel happy, too.
1 2 3 4 5
24. TV or news stories about injured or sick children greatly upset me.
1 2 3 4 5
73

Michelle Rodriguez 12404089 PSY4001
25. I cry at sad parts of the books I read.
1 2 3 4 5
26. Being around people who are depressed brings my mood down.
1 2 3 4 5
27. I find it annoying when people cry in public.
1 2 3 4 5
28. It hurts to see another person in pain.
1 2 3 4 5
29. I get a warm feeling for someone if I see them helping another person.
1 2 3 4 5
30. I feel other people's joy.
1 2 3 4 5
A Day in the Life of Sam
Sam has been diagnosed with Major Depression Disorder (or ‘Schizophrenia’ or ‘hasn’t been diagnosed and is considered normal’ depending on which diagnosis participants read)
Sam’s day hasn’t been going very well, he/she feels sad for no apparent reason; all he/she wants is to be alone and as soon as Sam got home fromwork, he/she started crying uncontrollably. Sam doesn’t want to be this way but he/she doesn’t know what to do about it. All of Sam’s co-workers commented on his/her change of mood today and his/her boss warned Sam about controlling him/herself in the workplace. Sam now feels like
COMMUNITY ATTITUDES TOWARDS THE MENTALLY ILL
74

Michelle Rodriguez 12404089 PSY4001
The following 40 statements express various opinions about mental illness and the mentally ill. The mentally ill refers to people needing treatment for mental disorders but who are capable of independent living outside a hospital. Please choose the response which most accurately describes your reaction to each statement (SA= Strongly Agree; A= Agree; N= Neither Agree Nor Disagree; D= Disagree; SD= Strongly Disagree). It's your first reaction which is important. Don't be concerned if some statements seem similar to ones you have previously answered. Please be sure to answer all statements.
1. As soon as a person shows signs of mental disturbance, he should be hospitalized.
SA A N D SD
2. More tax money should be spent on the care and treatment of the mentally ill.
SA A N D SD
3. The mentally ill should be isolated from the rest of the community.
SA A N D SD
4. The best therapy for many mental patients is to be part of a normal community.
SA A N D SD
5. Mental illness is an illness like any other.
SA A N D SD
75

Michelle Rodriguez 12404089 PSY4001
6. The mentally ill are a burden on society.
SA A N D SD
7. The mentally ill are far less of a danger than most people suppose.
SA A N D SD
8. Locating mental health facilities in a residential area downgrades the neighbourhood.
SA A N D SD
9. There is something about the mentally ill that makes it easy to tell them from normal people.
SA A N D SD
10. The mentally ill have for too long been the subject of ridicule.
SA A N D SD
11. A woman would be foolish to marry a man who has suffered from mental illness, even though he seems fully recovered.
SA A N D SD
12. As far as possible mental health services should be provided through community-based facilities.
76

Michelle Rodriguez 12404089 PSY4001
SA A N D SD
13. Less emphasis should be placed on protecting the public from the mentally ill.
SA A N D SD
14. Increased spending on mental health services is a waste of tax dollars.
SA A N D SD
15. No one has the right to exclude the mentally ill from their neighbourhood.
SA A N D SD
16. Having mental patients living within residential neighbourhoods might be good therapy, but the risks to residents are too great.
SA A N D SD
17. Mental patients need the same kind of control and discipline as a young child.
SA A N D SD
18. We need to adopt a far more tolerant attitude toward the mentally ill in our society.
SA A N D SD
77

Michelle Rodriguez 12404089 PSY4001
19. I would not want to live next door to someone who has been mentally ill.
SA A N D SD
20. Residents should accept the location of mental health facilities in their neighbourhood to serve the needs of the local community.
SA A N D SD
21. The mentally ill should not be treated as outcasts of society.
SA A N D SD
22. There are sufficient existing services for the mentally ill.
SA A N D SD
23. Mental patients should be encouraged to assume the responsibilities of normal life.
SA A N D SD
24. Local residents have good reason to resist the location of mental health services in their neighbourhood.
SA A N D SD
25. The best way to handle the mentally ill is to keep them behind locked doors.
78

Michelle Rodriguez 12404089 PSY4001
SA A N D SD
26. Our mental hospitals seem more like prisons than like places where the mentally ill can be cared for.
SA A N D SD
27. Anyone with a history of mental problems should be excluded from taking public office.
SA A N D SD
28. Locating mental health services in residential neighbourhoods does not endanger local residents.
SA A N D SD
29. Mental hospitals are an outdated means of treating the mentally ill.
SA A N D SD
30. The mentally ill do not deserve our sympathy.
SA A N D SD
31. The mentally ill should not be denied their individual rights.
SA A N D SD
79

Michelle Rodriguez 12404089 PSY4001
32. Mental health facilities should be kept out of residential neighbourhoods.
SA A N D SD
33. One of the main causes of mental illness is a lack of self-discipline and will power.
SA A N D SD
34. We have the responsibility to provide the best possible care for the mentally ill.
SA A N D SD
35. The mentally ill should not be given any responsibility.
SA A N D SD
36. Residents have nothing to fear from people coming into their neighbourhood to obtain mental health services.
SA A N D SD
37. Virtually anyone can become mentally ill.
SA A N D SD
38. It is best to avoid anyone who has mental problems.
80

Michelle Rodriguez 12404089 PSY4001
SA A N D SD
39. Most women who were once patients in a mental hospital can be trusted as baby sitters.
SA A N D SD
40. It is frightening to think of people with mental problems living in residential neighbourhoods.
SA A N D SD
Social Distance Scale
Please answer the following questions, ticking Yes or No for each, considering the description of the person you just read.
1. Would marry Yes
2. Would have as regular friends Yes
3. Would work beside in an office Yes
4. Would have several families in my neighbourhood Yes
5. Would have merely as speaking acquaintances Yes
Debrief (if required)
81

Michelle Rodriguez 12404089 PSY4001
Debrief
Thank you for taking part in this study about attitudes towards mental health. Data gathered will be used to examine whether people with greater empathy have better attitudes towards mental health and particularly, whether people have a better attitude towards depression over schizophrenia, or the other way around. Finally, the gender differences of these will be explored. If you have any further queries or concerns about this research, you may contact me at
Any other necessary documents
9. Cover Letter – Major Corrections
82

Michelle Rodriguez 12404089 PSY4001
Division of Psychology
Dr Roz Collings
Chair of Psychology Ethics Committee
University of Northampton
Boughton Green Road
Northampton
NN2 7AL
10th December 2014
cc: Lesley-Ann Smith
REF: Michelle Rodriguez
Dear Colleagues
Attitudes towards mental health.
Your research proposal has been considered by the Division of Psychology Ethics Review Committee and they are satisfied that the research proposal accord with the relevant ethical guidelines.
Your Ethics application has been approved with major corrections and comments have been supplied by the reviewer. You are required to meet with your supervisor before commencing any research to address the major corrections needed to begin your study. Please note that you may also be required to resubmit a part of your ethics (e.g. information sheet;
83

Michelle Rodriguez 12404089 PSY4001
this will be stated in the reviewer’s comments). Please resubmit the section requested via [email protected]
If you wish to make any additional modifications to the research project, you must speak to your supervisor about it. If your supervisor thinks that the modifications are at all important you must inform the committee in writing before proceeding. Please also inform the committee as soon as possible if participants experience any unanticipated harm as a result of taking part in your research.
Good luck with your research.
Chair Psychology Ethics Committee.
84

Michelle Rodriguez 12404089 PSY4001
85
REVIEWERS COMMENTS:
Approval major amendments (due to lack of information on the information sheet):
1. Supervisor needs to approve the online version of the questionnaire before being launched and the student should discuss which social media sites the link will be distributed to2. On the CAMI questionnaire there is a question that refers to dollars (consider changing to pounds?)3. Supervisor should ensure they approve the 'day in the life of' blurb for an individual with a diagnosis of schizophrenia4. Rather than using the word 'normal' for the third condition, perhaps just keep to 'non-diagnosis' or no mental health issues?5. How will participants be randomly allocated to conditions?6. The information sheet needs much more information and should include:- withdrawal details- confidentiality information- how data will be stored and used- why doing the research (i.e., for BSc Psychology degree at the UoN/dissertation)- contact details for the student and the supervisor- can the participants obtain a summary of results?- will the research adhere to the Data Protection Act or BPS Code of Ethics and Conduct?- add that the research study has been approved by the Psychology Division Ethics Panel- add that Ps are over 18

Michelle Rodriguez 12404089 PSY4001
10. Scatterplot showing benevolence scores against empathy scores for all conditions
11. SPSS Output for Linear Regression results showing effect of empathy on benevolence
86

Michelle Rodriguez 12404089 PSY4001
Model Summary
Group Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
Depression 1 .352a .124 .111 .47020
Non-Diagnosis 1 .144a .021 .006 .57739
Schizophrenia 1 .273a .075 .061 .41527
a. Predictors: (Constant), Empathy Scores
ANOVAa
Group Model
Sum of
Squares df Mean Square F Sig.
Depression 1 Regression 2.120 1 2.120 9.590 .003b
Residual 15.034 68 .221
Total 17.154 69
Non-Diagnosis 1 Regression .483 1 .483 1.449 .233b
Residual 22.670 68 .333
Total 23.153 69
Schizophrenia 1 Regression .947 1 .947 5.491 .022b
Residual 11.727 68 .172
Total 12.674 69
a. Dependent Variable: Benevolence_Scores
b. Predictors: (Constant), Empathy Scores
Coefficientsa
Group Model
Unstandardized
Coefficients
Standardized
Coefficients
t Sig.B Std. Error Beta
Depression 1 (Constant) 2.800 .440 6.359 .000
Empathy Scores .366 .118 .352 3.097 .003
Non-Diagnosis 1 (Constant) 3.581 .565 6.343 .000
Empathy Scores .175 .145 .144 1.204 .233
Schizophrenia 1 (Constant) 3.104 .524 5.930 .000
Empathy Scores .318 .136 .273 2.343 .022
a. Dependent Variable: Benevolence_Scores
12. Scatterplot showing social restrictiveness scores against empathy scores for all conditions
87

Michelle Rodriguez 12404089 PSY4001
13. SPSS Output for Linear Regression results showing effect of empathy on social restrictiveness
88

Michelle Rodriguez 12404089 PSY4001
14. Histograms showing distribution of authoritarian scores for all conditions
89
Model Summary
Group Model R R Square
Adjusted R
Square
Std. Error of the
Estimate
Depression 1 .263a .069 .055 .52772
Non-Diagnosis 1 .049a .002 -.012 .53507
Schizophrenia 1 .204a .042 .028 .42658
a. Predictors: (Constant), Empathy Scores
ANOVAa
Group Model
Sum of
Squares df Mean Square F Sig.
Depression 1 Regression 1.406 1 1.406 5.047 .028b
Residual 18.937 68 .278
Total 20.343 69
Non-Diagnosis 1 Regression .047 1 .047 .163 .687b
Residual 19.468 68 .286
Total 19.515 69
Schizophrenia 1 Regression .540 1 .540 2.967 .090b
Residual 12.374 68 .182
Total 12.914 69
a. Dependent Variable: Social_Restrictiveness_Scores
b. Predictors: (Constant), Empathy Scores
Coefficientsa
Group Model
Unstandardized
Coefficients
Standardize
d
Coefficients
t Sig.B Std. Error Beta
Depression 1 (Constant) 3.130 .494 6.333 .000
Empathy
Scores-.298 .133 -.263 -2.247 .028
Non-
Diagnosis
1 (Constant) 2.201 .523 4.207 .000
Empathy
Scores-.054 .134 -.049 -.404 .687
Schizophreni
a
1 (Constant) 2.768 .538 5.147 .000
Empathy
Scores-.240 .139 -.204 -1.723 .090
a. Dependent Variable: Social_Restrictiveness_Scores

Michelle Rodriguez 12404089 PSY4001
90

Michelle Rodriguez 12404089 PSY4001
91

Michelle Rodriguez 12404089 PSY4001
15. Histograms showing distribution of benevolence scores for all conditions
92

Michelle Rodriguez 12404089 PSY4001
93

Michelle Rodriguez 12404089 PSY4001
94

Michelle Rodriguez 12404089 PSY4001
16. Histograms showing distribution of social restrictiveness scores for all conditions
95

Michelle Rodriguez 12404089 PSY4001
96

Michelle Rodriguez 12404089 PSY4001
97

Michelle Rodriguez 12404089 PSY4001
17. Histograms showing distribution of CMHI scores for all conditions
98

Michelle Rodriguez 12404089 PSY4001
99

Michelle Rodriguez 12404089 PSY4001
100

Michelle Rodriguez 12404089 PSY4001
18. Histograms showing distributions of social distance scores for all conditions
101

Michelle Rodriguez 12404089 PSY4001
102

Michelle Rodriguez 12404089 PSY4001
103

Michelle Rodriguez 12404089 PSY4001
19. Histograms showing distributions of empathy scores for all conditions
104

Michelle Rodriguez 12404089 PSY4001
105

Michelle Rodriguez 12404089 PSY4001
106

Michelle Rodriguez 12404089 PSY4001
107