“ATTD Session: Needs and solutions in -...
104
The Jesse Z and Sara Lea Shafer Institute for Endocrinology and Diabetes National Center for Childhood Diabetes Schneider Children’s Medical Center of Israel Moshe Phillip MD “ATTD Session: Needs and solutions in Type 1 diabetes from youth to seniors: towards software prescriptions”
Transcript of “ATTD Session: Needs and solutions in -...

The Jesse Z and Sara Lea Shafer Institute for Endocrinology and Diabetes
National Center for Childhood Diabetes
Schneider Children’s Medical Center of Israel
Moshe Phillip MD
“ATTD Session: Needs and solutions in Type 1 diabetes from youth to seniors:
towards software prescriptions”

Institute Research Support: Abbott Diabetes, Andromeda Biotech, Animas, BMS , Eli Lilly, Ferring, Geffen
Medical, Medtronic Diabetes, MSD Merck, Novo Nordisk, Pfizer, Prolor , Sanofi, Bristol-Myers Squibb
Moshe Phillip
Medical Advisory Board Member: Astra Zeneca, Bristol-Myers Squibb, Merck & Co, Roche Diagnostics, Sanofi , Eli Lilly & Company, Medtronic Board Member: CGM3 Ltd, DreaMed-Diabetes LtdConsultant: Andromeda BiotechChairman: NG Solutions LtdSpeaker’s Bureau: Novo Nordisk, Pfizer, Sanofi, Medtronic Minimed
Revital Nimri
Speaker’s Bureau: Novo Nordisk, Pfizer, Sanofi
Shareholder: DreaMed Diabetes
Active Position: DreaMed Diabetes
Disclosure Information

In our session- we will:
• Define the need for clinical decision support systems
• Discuss clinical cases and how do we deal with the data that the new technologies provide
• Discuss several ways to overcome barriers in diabetes treatment and technology implementation
• Introduce the idea of software prescription to tailor the treatment of patients with different devices

Do you care for patients with:
A. Type 1 Diabetes
B. Type 2 Diabetes
C. Both
D. Other
Get To Know You

Do you take care of:
A. Pediatric patients
B. Adult patients
C. Both
D. Other
Get To Know You

Does your clinic is based in the:
A. Hospital
B. Primary care
A. Both
B. Other
Get To Know You
What is the percentage of your patients who use pump therapy ?
A. Up to 25%
B. 25-50%
C. 50-75%
D. More than 75%
Get To Know You

What is the percentage of your patients who use continuous glucose monitoring?
A. Up to 10%
B. 10-25%
C. 25-50%
D. More than 50%
Get To Know You

Do you download data from your patient’s devices (pump, sensor, glucometer)?
A. Yes, to all of my patients
B. Yes, to some of my patients
C. No, I don’t have the ability/manpower/time for that
D. No, I don’t think this is necessary
Get To Know You

Do you enable your patients to download and send to you the data from their devices (pump, sensor, glucometer) at home to you in between visits?
A. Yes, to all of my patients
B. Yes, to some of my patients
C. No, I don’t have the ability/manpower/time for that
D. No, I don’t think this is necessary
Get To Know You

The Goal !
Rate
of
pro
gre
ssio
n o
f re
tin
op
ath
y
(per
100 p
ati
en
t years
)
Rate
of
sev
ere
Hyp
og
lycem
ia
(per
100 p
ati
en
t years
)
Severe hypoglycemia 120
60
0
12
10
8
6
4
2
0
0 5.5 6 6.5 7 7.5 8 8.5 9 9.5 10 10.5
HbA1c (%)
Relative risk
of retinopathy
The Diabetes Control and Complications Trial Research Group, N Eng J Med; 329:977-986, 1993

Percent of patients achieving HbA1c ADA targets by age-group
Kellee M. Miller et al. Dia Care 2015;38:971-978

How Many Hit The Target?
Miller KM et al, Diabetes Care ;38:971-8, 2015Wong JC et al, Diabetes Care ;37:2702-9, 2014
USA Exchange registry 17,317 T1DM, 67 clinics

TEENs Study – Glycemic Control72% did not achieve targets
ADA, 2014;IDF,2015
ADA 2014;IDF 2015
Proposal to addresults from the TEENS study to
show in one slide « how many hit
the targets » from 8 to 25
reinforcingprevious slides

Diabetes Related Adverse Events are Still Frequent
Changes in diabetes-related
complications in the U.S.
Richard M. Bergenstal Dia Care 2015;38:1615-1621
Incidence rate of severe hypoglycaemia in
the U.S., N=225 patients, age 9-15 years
Inci
den
ce r
ate
of
seve
re h
ypo
glyc
em
ia
(pe
r 10
0 p
atie
nt-
year
s)
50
40
30
20
10
0
37.6
9.6
46.1*
14.4
34.4
11.1
31.8*
4.5
All NPH Basal-bolus
injection
Pump therapy
†
‡
‡ ‡†
*pump therapy vs. NPH, P = 0.04;Severe hypoglycaemia resulting in seizure ⁄ coma:
† pump therapy vs. NPH, P = 0.004; ‡ pump therapy vs. basal-bolus injection therapy, P = 0.05
Katz ML, et al. Diabet Med; 29:926-32, 2012

Current Type 1 Diabetes Comprehensive Technological Treatment
Managing diabetes is complex
Daily ActivitiesMeasure Glucose
Doctor Visit
Infuse Insulin How to set the patient’s insulin treatment profile?
How much insulin to deliver?How to interpret my diabetes data?

Current Type 1 Diabetes Comprehensive Technological Treatment
Insulin Delivery Devices
Insulin Analogues
Glucose Measurement Devices
Patients
Physician
Educator Nurse
Dietitian
Social Worker
Psychologist
Diabetes management platforms

Data Interpretation is Complex

Key Challenges
Patients Physicians
• Need expertise to deduct from the data (the patient’s glucose levels, insulin injections, meals, physical activity and more) how to optimize the insulin treatment profile
• Swamped with information, data from CGM, SMBG, pump… that makes it difficult to retrieve a more efficient treatment strategy
• Even for experts, it takes a lot of time to perform this optimization
• Worldwide shortage of Diabetologists/ Endocrinologists
• Lack of knowledge / ability to perform the insulin decision cycle
• Swamped with information, data from CGM, SMBG, pump…
• Poor accessibility to expert physician for optimize the insulin treatment profile (both in developed and developing countries)
• NO treatment tools for diabetes self management and optimizing insulin treatment profile between clinic visits

GlookoDexcom CLARITYTM
Tidepool's platformDiasend
Diabetes Management Software
Ambulatory Glucose Profile
app connects personal health data to electronic medical records
Case presentations- The challenges

Case 1 (Adolescent who use pump and sensor)
BE, 12.6 years old boy,
• 42 Kg, 153 cm, Tanner 3
• T1D 1 since the age of 4.5 years
• CSII since T1D onset, CGM use since last year
• Active in sport, treated with Ritalin (methylphenidate) 10 mg
• HbA1c 6 % (42 mmol/mol Hb)

Case 1 (Adolescent who use pump and sensor)
mg/dl mmol/l
Average 131 7.3
Median 123 6.8
SD 49 2.7
% Time with in range 70-180 mg/dl (3.9-10 mmol/l) 80
% Time > 180 mg/dl (10 mmol/l) 16
% Time < 70 mg/dl (3.9 mmol/l) 4
SunSatFriThuWedTueMon
Glucose Level
Time
22.2
19.4
16.8
13.9
11.1
8.3
5.6
2.8
0
mmol/l

Total Daily Insulin Dose: 0.8 u/Kg/day
80% of insulin dose given as basal
C:I 1:15, CF 1:50
Target glucose levels 120 mg/dl
Case 1 (Adolescent who use pump and sensor)
Basal Insulin RateBasal/Bolus Ratio per Day
Insulin units
alert limit for high BG alert limit for low BG Median Average

Case 1: Question
What action would be most appropriate?
A. Increase insulin basal rate at first part of the night
B. Change basal/bolus ratio
C. Increase insulin basal rate at second part of the night
D. Reduce evening basal rate

Case 1: Answer
What action would be most appropriate?
A. Increase insulin basal rate at first part of the night
B. Change basal/bolus ratio
C. Increase insulin basal rate at second part of the night
D. Reduce evening basal rate

Over the Weekend MD-Logic Study ITT Results [60h]
P*ControlMD-LogicN=22 (Average ± STD)
N.S116.2 ± 35.7122.6 ± 38.6Total Insulin Dose [Units]
N.S9.4 ± 3.310.1 ± 4.0Total Night Insulin Dose [Units]
0.00162.3 ± 21.355.5 ± 21.1Total Basal Insulin [Units]
0.01253.8± 22.467.0 ± 24.4Total Bolus Dose [Units]
0
20
40
60
80
0
20
40
60
80
0
20
40
60
80P=N.S P=0.007 P=0.006
% Within 70-180 mg/dl % > 180 mg/dl% < 60 mg/dl
68.4 57.5
24.6 37.5
0.80.9
0
30
60
90
120
150
180
P=0.006
144
159.5
Glucose Levels [mg/dl]
SAP MD-Logic
• ITT analysis, (N=22). • Median (IQR)
% o
f Ti
me
Basal-Bolus Makes the Difference

Overcorrection of Hypoglycemia
Case 1: Answer
Bolus
Basal
Temporary Basal
Basal (u/h ) Bolus (units )
Basal (u/h )
Basal (u/h )Basal (u/h )
Basal (u/h )
Basal (u/h )
Basal (u/h )
Bolus (units )
Bolus (units )
Bolus (units )
Bolus (units )
Bolus (units )
Bolus (units )

Approach to Retrospective Analysis of CGM-Profile
Check for common limitations for optimal CGM use by patients and diabetes teams alike:
– Avoid calibration issues
– Determining meaningful alarm settings
– Place of insertion
– Sensor adhesive issues
– Contineous use vs. intermitent : before clinic visits, changing insulin
treatment, changing lifestyle etc.
– Adjust expectations

1..
Prerequisite for pattern analysis of CGM-profiles:
– Representative data
– Data duration capture (how many days of data have been provided?)
– Varification
– Review patient history (typical daily routin): insulin regiment, time & amount of
meals, exersise ...
– Pump occlusion, sick days, menestural period, holidays , exeptional events....
Approach to Retrospective Analysis of CGM-Profile

Is the Data Representative ?
E.I, 12 years old boy, 42 Kg
▪ T1D since 4.5 years ▪ Treatment with CSII ▪ Total Daily Insulin Dose - 0.5 u/Kg/day▪ History of poor glycemic control 8-9.9 %
A1C 12% , 108 mmol/mol Hb
Insulin Delivery Data
GlucosmeterData

How Much Retrospective Data to Analyse?
A minimum duration of 12 days of CGM data is needed to infer glycemic variation Neylon OM et al, Journal of Diabetes Science and Technology 2014, Vol. 8(2) 273 –276
A minimum of 14 days of CGM data provides identification of individual glucose patterns Dunn TC, Crouther N. Assessment of the variance of the ambulatory glucose profile over 3 to 20 days of continuous glucose monitoring. Abstract 1054, presented at EASD 2010.

1..
Prerequisite for pattern analysis of CGM-profiles:
– Evaluating diabetes treatment adherence – need for pateint education
• Time of pre-meal bolus
• Use of Bolus Calculator
• Meals with no bolus, no correction boluses, blinded boluses ....
• Amount, type and frequency of food
• Over-treatment of hypoglycemia or hyperglycemia
• Insulin stucking
• Rate of infusion set changing
Approach to Retrospective Analysis of CGM-Profile

Need for Patient Education
A. In all young patients, meal bolus should be injected after meal
B. 15-20 min before the meal, if pre-meal blood glucose was within target or above
C. 60 min after meal, if meal preceded treatment of hypoglycemia
D. With the meal, if pre-meal blood glucose was within target
Approach to Retrospective Analysis of CGM-Profile
When is the ideal time for meal bolus?

• Randomized three-period open-label crossover intervention study
• 10 Patients with type 1 diabetes on CSII
• Insulin administration 0, -15 or -30 minutes
Dosing 15-20 min before meal is optimalCobry et al.; Scaramuzza et al; DT&T 2010

Need for Life Style ModificationWhen is the ideal time for meal bolus?
1..
2..
Then meaningful in-depth analysis of glucose regulation of CGM-profiles may be conducted.
Review patterns:
– Glucose stability
– Glucose levels
– Daily glucose patterns
Approach to Retrospective Analysis of CGM-Profile

Patterns Presented at Different Software

Patterns Presented at Different Software

Patterns Presented at Different Software
(

Patterns Presented at Different Software

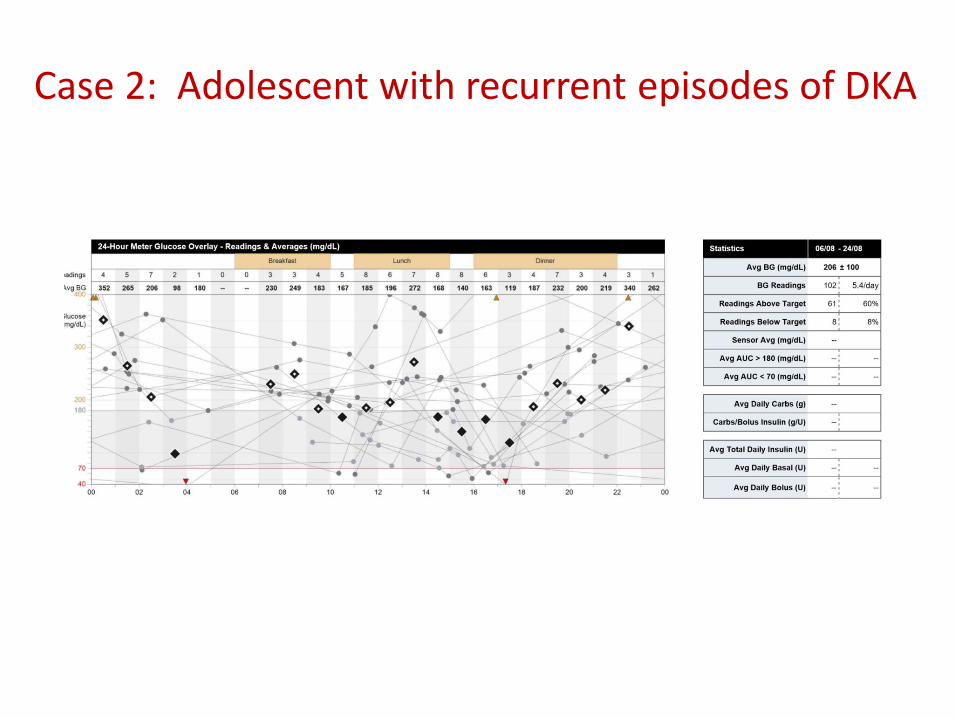
Case 2: Adolescent with recurrent episodes of DKA
P.D, 16 years old boy
• T1D at the age of 9 years
• Poor glycemic control, A1c 9-14%
• Previously treated at two different hospitals
– Treated with pump therapy and sensor, due to recurrent events of DKA, therapy was switched to Levemir twice a day and Lispro (1:15 and 1:40) but…..
• In the recent year was hospitalized 7 times due to DKA
• P.D expressed his will to switch again to pump therapy
Case 2: Adolescent with recurrent episodes of DKA
Case 2: Question
What would you do?
A. Keep therapy with MDI & Increase lunch C:I
B. Keep therapy with MDI & Increase basal insulin (Levamir) at evening
C. In order to have a more compliant patient change to pump therapy
D. Hospitalized for re-education and evaluation

Coefficient of Variance 100 × SD/MEAN= CV%100 ×100/206 = 50%
CV < 33% stable glucose level
CV > 50% instable glucose level
CV 33-50% intermediate stability
Case 2: Adolescent with recurrent episodes of DKA

Case 2: Answer
What would you do?
A. Keep therapy with MDI & Increase lunch C:I
B. Keep therapy with MDI & Increase basal insulin (Levamir) at evening
C. In order to have a more compliant patient change to pump therapy
D. Hospitalized for re-education and evaluation

Variability, 100 × 83/ 201 = 40%Lantus injection given by the parents in the morningNo DKA at the last 2 years
Case 2: (Adolescent who use MDI and Intermittent Sensor)
Median Average
mg/dl mmol/l
Average 201 11.2
Median 192 10.7
SD 83 4.6
Median & IQR (25-75%)

Case 3: Adolescent who use pump therapy & SMBG
AS, 12.5 years old boy
• T1D since the age of 8 years
• 55Kg, 155cm
• Pump therapy in the last 3 years
• A1c = 9% CV = 29%

Case 3: Adolescent who use pump therapy & SMBG
Total Daily Dose: 1u/kg/dayBasal Rate range 0.8-1 unit/hC:I 1:15 day, 1:25 nightCF 1:50 day, 1:100 night
calculated:Basal Rate range 0.9-1.1 unit/hC:I 1:8 day, 1:10 nightCF 1:30 day, 1:60 night
Average glucose measurements 5/dayAverage 8-10 boluses/day

Case 3: Question
What would you do?
A. Decrease C: I ratio for all 3 meals
B. Decrease C:I ratio and CF
C. Increase nighttime basal and decrease C:I ratio
D. Re-calculate pump settings

Case 3: Answer
What would you do?
A. Decrease C: I ratio for all 3 meals
B. Decrease C:I ratio and CF
C. Increase nighttime basal and decrease C:I ratio
D. Re-calculate pump settings

A1C=7.6 %
Case 3: Answer
Basal Rate range 0.9-1.3 unit/hC:I 1:7 day, 1:10 nightCF 1:40 day, 1:60 night

Case 5: (Child who use MDI and sensor)
A.M 8 years old girl,
• 21 Kg, 118 cm
• T1D since 2 years of age
• Well Controlled A1c: 6.6-7.5%
• 8 units Lantus at the evening and 2-4 units
Humalog for 3 main meals
• Sensor use for the last 2 years

Case 5: Question
What would you do?
A. Increase dose of evening Lantus
B. Increase breakfast dose
C. Change time of Lantus injection to morning
D. Change breakfast insulin analog to regular insulin

meal time
Case 5: (Child who use MDI and sensor)

Case 5: Question
What would you do now?
A. Increase dose of evening Lantus
B. Increase breakfast dose
C. Change time of Lantus injection to morning
D. Change breakfast insulin analog to regular insulin

Case 5: Answer

Example – Fear of Nocturnal Hypoglycemia
F.S, 24 years old man
• T1D since age 6 years
• Treated with Tregludec insulin and Humalog
• Glycemic control 8-8.4%
• Hypoglycemia unawareness

Example – Fear of Nocturnal Hypoglycemia
F.S, 24 years old man
• T1D since age 6 years
• Treated with 640G pump with predicted low glucose suspend
• Glycemic control 7-7.4%

Preliminary Results – SmartGuard Study
Number of Hypoglycemic Events
Presented at ATTD Viena, 2015Accepted DC

Day Time Control After Overnight Closed-Loop ControlExamples – from the 6 weeks study
Night/MD-Logic Day/SAP Therapy Night/MD-Logic Day/SAP Therapy
Patient I :Male, 15 y, A1c 9.4% (79 mmol/l) Patient II: Female, 21 y, A1c 7% (53mmol/l)
SAP MD-AID
Median [IQR]

MD-Logic Pooled AnalysisOf 4 nights 1 and 6 weeks 2 Overnight Studies
1 Nimri R et al, Pediatric Diabetes2014 ;15: 91-92 Nimri R et al, Diabetes Care 2014;37:3025-32
N=848 N=807
Mean Overnight Glucose Levels [mg/dl]
Histogram of Mean Overnight Glucose Levels, PP
71 (33,75) % 45 (25,64) %
MD-Logic SAP

NEW ERA OF PERSONALIZED TREATMENT OF DIABETES USING DECISION SUPPORT TOOLS
“There are too few of the diabetes doctor specialists called endocrinologists”
• There are 29.1 million people with diabetes …of which 21 million are diagnosed (An estimated 8.1 million people live with diabetes but do not know it.)1
• As of 2011, there are 4,841 practicing endocrinologists in adult medicine and 1,016 in pediatric medicine 2
• An increase in the prevalence of diabetes mellitus further expands the demand for endocrinologists and HCPs 2,3
A Shortage of Diabetes Doctors in the US
1 CDC, National Diabetes Statistics Report, 20142 Vigersky RA et al, JCEM, 99:3122-121, 20143 HIS, The Complexity of Physicians Supply and Demand: Projections from 2014-2015, 2016 Update, April 5th 2016

A Shortage of Diabetes HCPs in the EU

Density of Physicians (total number per 1000 Population)
WHO, Global Health Observatory data, accessed Feb 2017, http://www.who.int/gho/health_workforce/physicians_density/en/

Managing Diabetes is Complex

The Majority of Patients with Diabetes Are Not in Control
• Treated by expert HCPs• Multidisciplinary team approach • Diabetes data is downloaded and is the basis for decisions and guidelines• Good accessibility
• Treated by trained physicians • Long periods between visits• Multidisciplinary team?
• Poorly controlled • Diabetes data download – not available and expertise
doesn’t exists

Clinical Decision Support definition
https://www.healthit.gov/policy-researchers-implementers/clinical-decision-support-cds
“Clinical Decision Support (CDS) System provides clinicians, staff, patients
or other individuals with knowledge and person-specific information,
intelligently filtered or presented at appropriate times, to enhance health
and health care. CDS encompasses a variety of tools to enhance decision-
making in the clinical workflow”

The Patient’s Visit to the Clinic
Download data
Review the data from different devices (sometimes using different diabetes management platforms)
“Detective Work” and recommendations

More Than 1,100 APPS Available for Patients With Diabetes and Their Caregiver
The Best Diabetes iPhone &
Android Apps of the Year

Apps & Diabetes
• Help counting calories and weight management
• Allow to upload glucose readings directly from the meter. Create a record of numbers so
the information is available to patients at all times. View statistics breakdown in graph
form. Share the information with the doctor.
• Large library of low-fat, low-sugar recipes.
• Help to interact with fellow patients so patients can talk, share tips, and learn together

Apps & Diabetes
• Scan a barcode to get the nutrition data on the food patients buy?
• Access to a library of videos that can help patients learn more about diabetes - friendly
diets and how to make healthy lifestyle choices
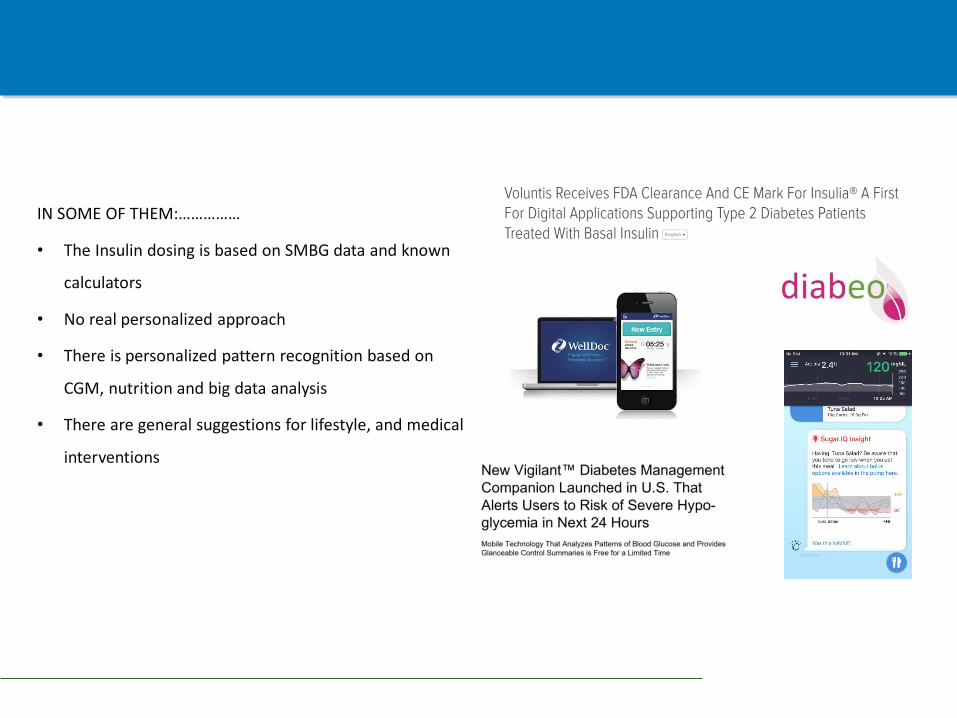
Existing Decision Support Systems
IN SOME OF THEM:……………
• The Insulin dosing is based on SMBG data and known
calculators
• No real personalized approach
• There is personalized pattern recognition based on
CGM, nutrition and big data analysis
• There are general suggestions for lifestyle, and medical
interventions

The Voice of HCPs Treating Diabetes
Associated psychosocial exploration data of the expectations of HCPs’ by Professor Katharine Barnard, un-published data
• Focus groups in three countries
• 26 healthcare professionals including:
• Endocrinologists
• Diabetologists
• Diabetes specialist nurses
• Diabetes educators
• Responded to self developed questionnaire

Expectations of HCPs from Decision Support System
Associated psychosocial exploration data of the expectations of HCPs’ by Professor Katharine Barnard, un-published data
• Easy to use and save time
• Personalized to individual patients
• As good as a HCP that does it on a
regular basis
• Provide specific advices
• Reliable and trustworthy

What should Decision Support System for HCPs include?
Associated psychosocial exploration data of the expectations of HCPs’ by Professor Katharine Barnard, un-published data
Pump settings
Systemic Analysis of the data
Carbohydrate Ratio, Correction Factor and Basal
Plan
• Reduce errors• Decision-making more
consistent within/across a clinical team
Specific pattern recognition Facilitating a discussion with the patient about behaviors impacting blood glucose

Introducing The “Digital” Clinic
Download data in the clinic or at home
Unified Platform for Diabetes Management
A digital detective that provides with recommendations

DreaMed ADVISORPro
• Decision support tool that enhances
the decision-making skills that HCPs
use every day
• Cloud-based technology, so its
support and guidance are accessible
from anywhere
• Evolves by continuous learning and
reporting
• Flexible to meet the needs of a
diverse group of patients

• Specific Behavioral analytics
• Rapid acting delivery compliance
• Reasons for hypoglycemia / hyperglycemia patterns
• Other tips for proper care
• Insulin dosing optimization
• Basal Plan
• Bolus sensitivity & bolus carbohydrate ratio (as CF/CR or in other sliding scale)
• Glucose target recommendation
DreaMed ADVISORPro Simplifies the Complexity of Diabetes Data

DreaMed’s Concept in Technology Development
ALL
MD-Logic Concept

How Similar Is the Algorithm Output to What I Would Recommend?

The EXPERTS Survey Study
• Design: Data analysis of existing patient's sensor and insulin pump data without any
intervention
3 Physicians per site 10-15 anonymous patient data 1 ADVISORPro

The EXPERTS Survey Study – Analysis Plan
Basal, CR and CF plan were compared at every hour:
Basal Plan (pump Format)
19:0007:0000:00Time of Day
0.810.5Value [u/h]
Basal Plan (Decision Points Format)
23222120191817161514131211109876543210Hour
0.80.80.80.80.81111111111110.50.50.50.50.50.50.5Value [u/h]
Decision Point

The EXPERTS Survey Study – Interim Results
Patient Characteristics
(N=8)Mean(SD)
4/4Gender [F/M]
15.1 (3.7)Age [yr]
56.2(16.2)Weight [kg]
158.5(12.9)Height [cm}
8.0(0.5)HbA1c [%]
6.5(2.6)Years with Diabetes [yr]
Physician Characteristics
• 3 Physicians from Hannover
• 2 Physicians from Slovenia
In this interim analysis we have 192
decision points (equal to 24 times 8
patients)

In what percentage of cases will 2 physicians from the same center agree on the changes in basal rate?
a. 80%b. 60%c. 40%d. 20%

The EXPERTS Survey Study – Interim Results
There are differences
between physicians
advice on the same
data set
Agreed on
changes to basal
No change of basal vs
more basal
No change of basal vs
less basal
Do not agree on how to
change basal

The EXPERTS Survey Study – Interim Results
The difference
between ADVISORPro
and physicians is
similar to the
differences among
the physicians
themselves Agreed on
changes to basal
No change of basal vs
more basal
No change of basal vs
less basal
Do not agree on how to
change basal

The EXPERTS Survey Study – Interim Results
Agreed on
changes to basal
No change of CR vs less
insulin through
CR
No change of CR vs
more insulin
through CR
Do not agree on how to
change basal

The EXPERTS Survey Study – Interim Results
Agreed on
changes to basal
No change of CF vs less
insulin through
CF
No change of CF vs
more insulin
through CF
Do not agree on how to
change basal

Salvador Dali 1930
A Paint By Salvador Dali
What do you see?
A. Old Couple
B. Holy Grail
C. Two Musicians
D. Beautiful Lady

How do we know that the algorithm is as good as expert HCPs (to compliment their efforts)?

The MD-Logic Advise4U Pilot Study
• Design: An open label, parallel (two-arm), randomized controlled prospective study
Every Three weeks new recommendations on pump settings and / or verbal recommendations were issued to the patients
N=34
Run in Period3 weeks
The MD-Logic Advise4U Pilot Study
• We hypothesize that the use of DreaMed’s ADVISORPro will achieve similar glycemic
control to that achieved by medical guided recommendations
Endpoint:
• Primary: Non-inferiority in time within 70-180 mg/dl
• Safety: Non inferiority in time below 70 mg/dl

The MD-Logic Advise4U Pilot Study
Inclusion Criteria:
• Documented T1D for at least 1 year prior to study enrolment
• Age ≥ 10 years and up to 25 years
• HBA1c ≤ 11%
• Insulin pump therapy for at least 4 months
• BMI SDS – below the 97th percentile
The MD-Logic Advise4U Pilot Study – Interim Results
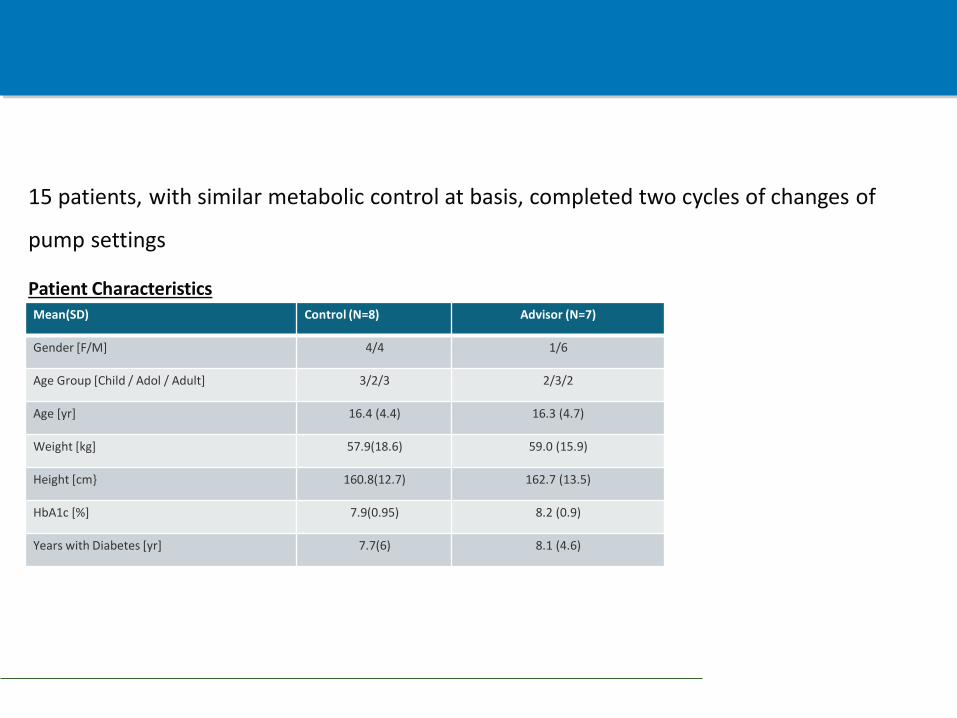
15 patients, with similar metabolic control at basis, completed two cycles of changes of
pump settings
Patient CharacteristicsAdvisor (N=7)Control (N=8)Mean(SD)
1/64/4Gender [F/M]
2/3/23/2/3Age Group [Child / Adol / Adult]
16.3 (4.7)16.4 (4.4)Age [yr]
59.0 (15.9)57.9(18.6)Weight [kg]
162.7 (13.5)160.8(12.7)Height [cm}
8.2 (0.9)7.9(0.95)HbA1c [%]
8.1 (4.6)7.7(6)Years with Diabetes [yr]

The MD-Logic Advise4U Pilot Study – Interim Results
Glucose Control After 6 Weeks of Intervention
Control (N=8) Advisor (N=7)
52% 50%42% 49%
7%2%
Time Below 70mg/dl Time Within 70-180 mg/dl Time Above 180 mg/dl

Example 1: Advisor is sensitive to basal/bolus ratio
• Basal Insulin is meant to offset glucose and ketones production
• Physicians often use the “basal” to treat high glucose levels due to bolus
insulin omission
• High basal ratio (of TDD) is associated with increased risk of hypoglycemia
The MD-Logic Advise4U Pilot Study – Interim Results

Basal Insulin Delivery - Analysis
Advisor (N=7)Control (N=8)Mean values
53%50%Basal Ratio (of TDD) at baseline
-1.81.8Change in Total Daily Basal between Baseline and 6 weeks [Units]
1.57-0.125Change in Number of Basal Periods between Baseline and 6 weeks [Units]
51%54%Basal Ratio (of TDD) at 6 weeks
The MD-Logic Advise4U Pilot Study – Interim Results
More info at Dr. Nimri’s Presentation, Friday(Feb 17th), 17:50-18:00, Maillot Hall

Personalized and Specific

Time
00:00
03:00
07:00
10:00
14:00
18:00
Basal value [U/h]-current
1.3
1.15
1.2
1.25
1.3
1.4
Time
00:00
06:00
09:00
12:00
17:00
22:00
CR value [gram/U]-current
6.6
5.7
6
5.4
7
7
Time
00:00
06:00
CF value [mg/dl/U]-current
55
42 IQR
Median
Before Visit
Basal value [U/h]-suggested
1.3
1.15
1.2
1.25
1.3
1.4
CR value [gram/U]-suggested
6.7
5.7
6
4.8
6.8
6.7
CF value [mg/dl/U]-suggested
40
40 IQR
Median
After Visit
Your patient tends to override the amount of insulin recommended by the bolus wizard.
Take Home Messages
• Decision support systems represent a new evolution in the treatment of patients with
diabetes and are HERE TO STAY.
• Next generation of DSS turns pure information into specific and personalized
actionable recommendations
• Interim results show that DSS can be in agreement with expert physicians in similar
way to their agreement with each other
• Interim results show that DSS can be as good as expert Diabetologists in controlling
glucose levels

Where Are We Heading ?

Acknowledgment
Dr. Revital Nimri
Dr. Alon Farfel
Prof Shlomit Shalitin
Dr Ariel Tenenboim
Dr Tal Oron
Dr Judith Nir
Dr Rachel Belo
Alona Hamu
Orna Hermon
Prof Thomas Danne
Prof Olga Kordonouri
Dr Torben Biester
Prof Tadej Battelino
Dr Natasa Bratina
Eran Atlas
Ido Muller
Aviel Fogel
Noam Greenboim
Yaron Matiash
Nitzan Goldfeder
Tomer Segall
Dan Erez