Atls head trauma modified pdf
30
Committee on Trauma Presents ©ACS Head Trauma
-
Upload
yousuf-mahomed -
Category
Healthcare
-
view
600 -
download
4
Transcript of Atls head trauma modified pdf
Committee on Trauma Presents
©ACS
Head Trauma
Objectives
➢ Describe basic intracranial physiology. ➢ Recognize the importance of limiting
secondary brain injury. ➢ Perform a focused neurologic exam. ➢ Stabilize and arrange for definitive care.
©ACS
➢ Rigid, nonexpansile skull filled with brain, CSF, and blood
➢ CBF autoregulation ➢ Autoregulatory compensation
disrupted by brain injury ➢ Mass effect of intracranial hemorrhage
©ACS
Anatomy and physiology effects?
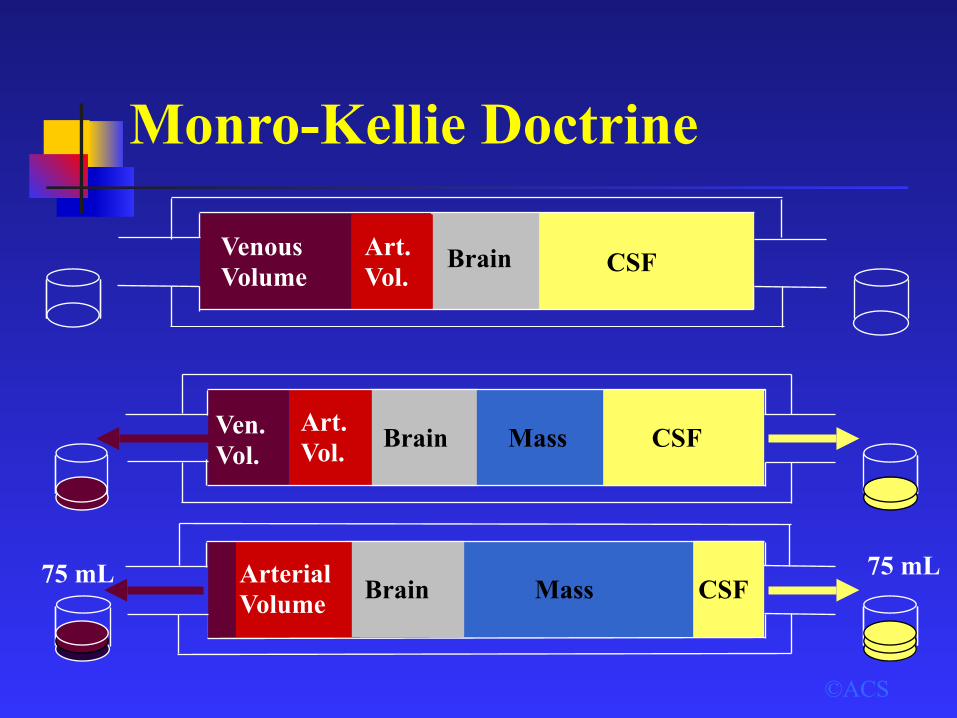
Monro-Kellie Doctrine
©ACS
Ven. Vol.
Art. Vol. Brain CSFMass
Arterial Volume Brain CSF75 mL Mass
75 mL
Venous Volume
Art. Vol.
Brain CSF
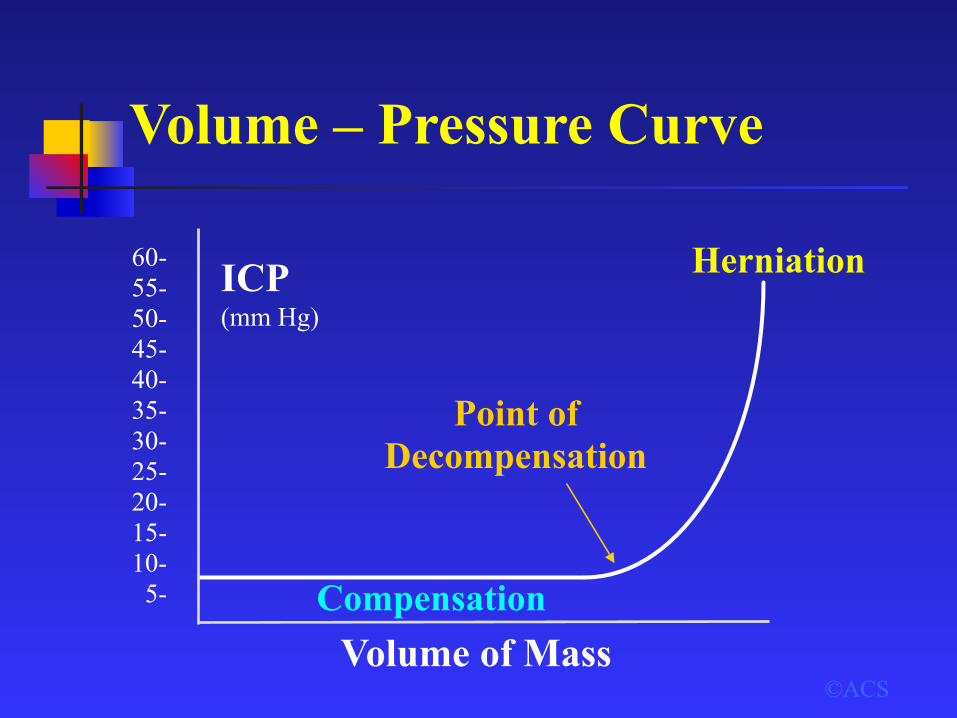
Volume – Pressure Curve
©ACSVolume of Mass
60- 55- 50- 45- 40- 35- 30- 25- 20- 15- 10- 5-
ICP (mm Hg)
Compensation
Herniation
Point of Decompensation
Intracranial Pressure (ICP)
➢ 10 mm Hg = Normal ➢ > 20 mm Hg = Abnormal ➢ > 40 mm Hg = Severe ➢ Many pathologic processes affect outcome ➢ Sustained ↑ ICP leads to ↓ brain function and
outcome
©ACS
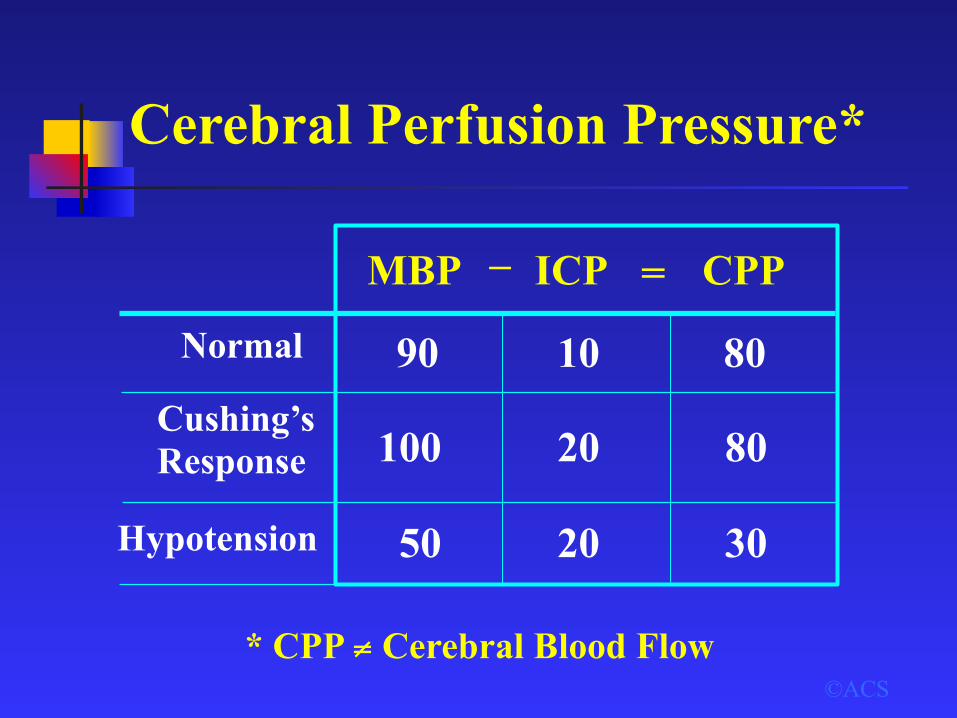
Cerebral Perfusion Pressure*
©ACS* CPP ≠ Cerebral Blood Flow
MBP ICP CPP
Normal
Cushing’s Response
Hypotension
– =
30
90
100
50
10 80
20
20
80
Autoregulation
➢ If autoregulation is intact, CBF is maintained with a mean BP of 50 to 160 mm Hg.
➢ Moderate or severe brain injury: Autoregulation often impaired
➢ Brain more vulnerable to episodes of hypotension → secondary brain injury
©ACS
Mild Brain Injury
©ACS
➢ GCS Score = 14–15 ➢ History ➢ Exclude systemic
injuries ➢ Neurologic exam
➢ X-rays as indicated ➢ Alcohol / drug
screens as indicated ➢ Liberal use of head
CT
Observe or discharge based on findings
Moderate Brain Injury
©ACS
➢ GCS Score = 9–13 ➢ Initial evaluation
same as for mild injury
➢ CT scan for all
➢ Admit and observe • Frequent neurologic exams • Repeat CT scan
➢ Deterioration: Manage as severe head injury

Severe Brain Injury
➢ GCS Score = 3–8 ➢ Evaluate and resuscitate ➢ Intubate for airway protection ➢ Focused neurologic exam ➢ Frequent reevaluation ➢ Identify associated injuries
©ACS
Classifications of Brain Injury
©ACS
By Morphology: Brain
Focal
Diffuse
• Epidural (extradural) • Subdural • Intracerebral
• Concussion • Multiple contusions • Hypoxic / ischemic injury
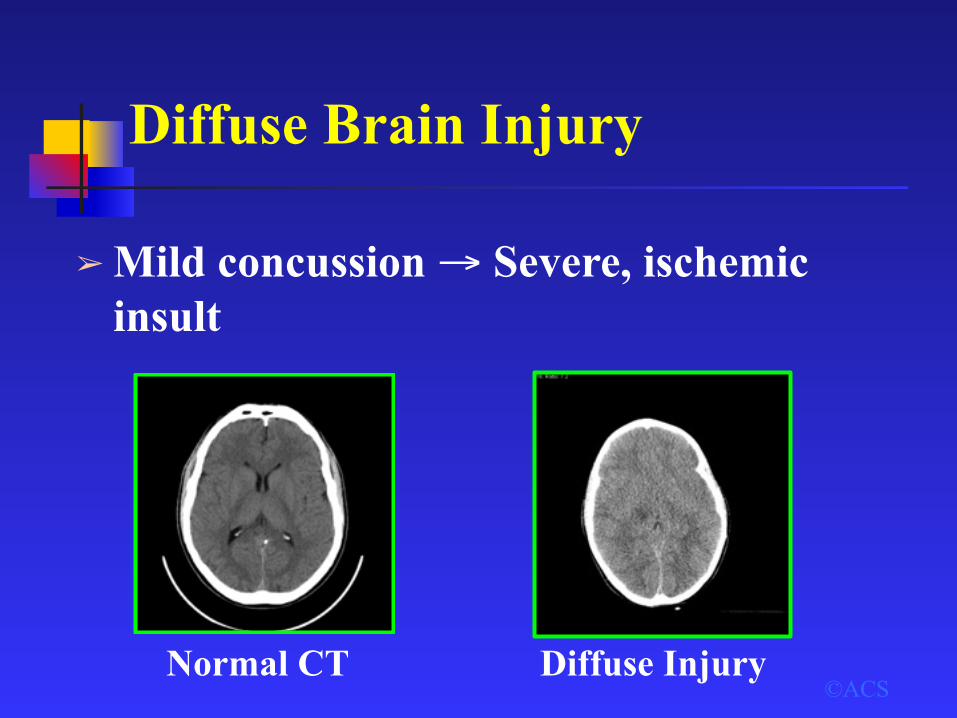
Diffuse Brain Injury
➢ Mild concussion → Severe, ischemic insult
©ACSNormal CT Diffuse Injury
Contusion / Hematoma
➢ Coup / contracoup injuries ➢ Most common: Frontal / temporal lobes ➢ CT changes usually progressive ➢ Most conscious patients: No operation
©ACS
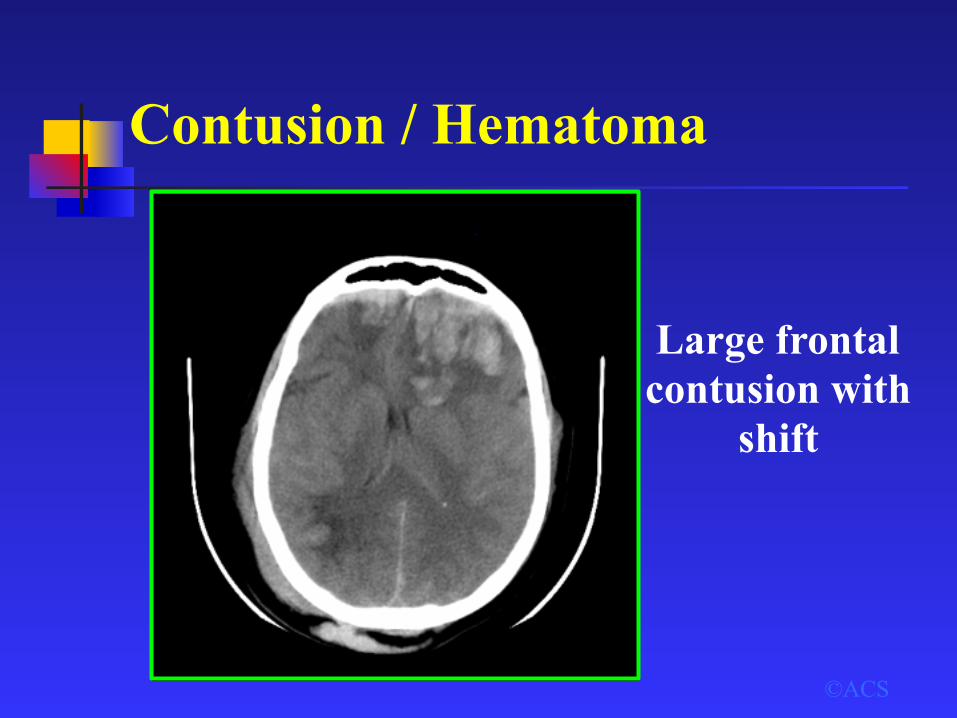
Contusion / Hematoma
©ACS
Large frontal contusion with
shift

Epidural Hematoma
➢ Associated with skull fracture ➢ Classic: Middle meningeal artery tear ➢ Lenticular / biconvex ➢ Lucid interval ➢ Can be rapidly fatal ➢ Early evacuation essential
©ACS
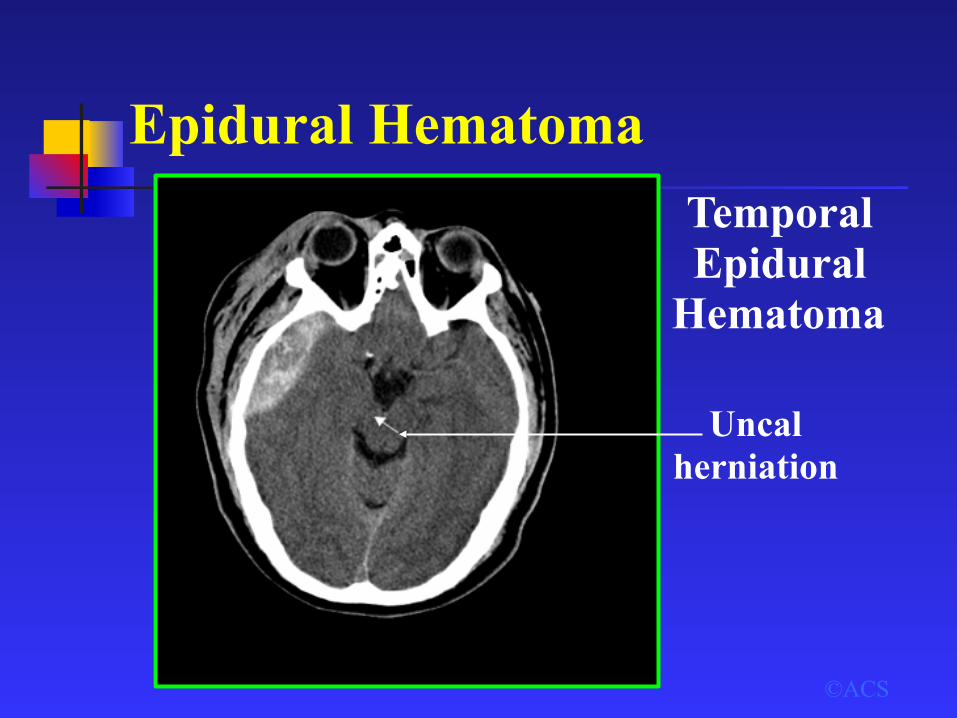
Epidural Hematoma
Uncal herniation
Temporal Epidural
Hematoma
©ACS
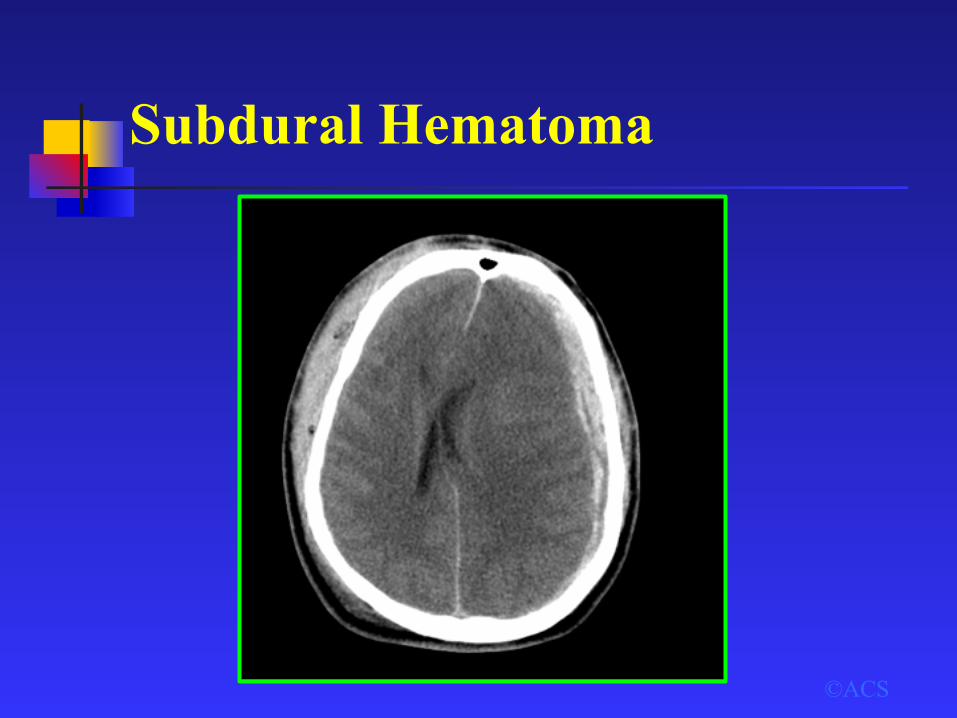
Subdural Hematoma
➢ Venous tear / brain laceration ➢ Covers cerebral surface ➢ Morbidity / mortality due to underlying
brain injury ➢ Rapid surgical evacuation
recommended, especially if > 5 mm shift of midline
©ACS
Subdural Hematoma
©ACS
Priorities
➢ ABCDE
©ACS
➢ Minimize secondary brain injury• Administer O2 • Maintain blood pressure
(systolic > 90 mm Hg)

Focused Neurologic Exam?
➢ GCS Score
©ACS
Consult neurosurgeon early
➢ Pupils➢ Lateralizing signs

Indications for CT Scan?
©ACS
All patients with suspicion of brain
injury
Medical Management
➢ Controlled ventilation
©ACS
➢ Intravenous fluids• Euvolemia • Isotonic
• Goal: Paco2 at 35 mm Hg
Medical Management
©ACS
➢ Mannitol• Use with signs of tentorial herniation • Dose: 1.0 g / kg IV bolus • Consult with neurosurgeon first
Medical Management
➢ Other medications
©ACS
• Anticonvulsants • Sedation • Paralytics
Surgical Management
©ACS
Scalp Injuries➢ Possible site of major blood loss ➢ Direct pressure to control bleeding ➢ Occasional temporary closure
Surgical Management
©ACS
Intracranial Mass Lesion➢ May be life-threatening if expanding
rapidly ➢ Immediate neurosurgical consult ➢ Hyperventilation / Mannitol ➢ Damage control craniotomy: Transfer
to neurosurgeon (rural / austere areas)
©ACS
?
Summary: What should I do?
➢ Maintain mean BP > 90 mm Hg ➢ Maintain Paco2 near / at 35 mm Hg ➢ Use isotonic solution for euvolemia ➢ Frequent neurologic exams ➢ Liberal use of CT scans ➢ Early neurosurgical consult
©ACS

Summary: What should I not do?
➢ Allow patient to become hypotensive ➢ Over-aggressively hyperventilate ➢ Use hypotonic IV fluids ➢ Use long-acting paralytics ➢ Paralyze before performing complete exam ➢ Depend on clinical exam alone
©ACS













![2006 - Head and Neck Trauma · terminology, such as those provided by the Advanced Trauma Life Support (ATLS) system and the GCS. A modified GCS should be used for paediatric patients.[3]](https://static.fdocuments.in/doc/165x107/5f8f75c37f78495d7300a25a/2006-head-and-neck-trauma-terminology-such-as-those-provided-by-the-advanced.jpg)



