Associations Between Venous Thromboembolism and...
![download Associations Between Venous Thromboembolism and …psychrights.org/Research/Digest/NLPs/BloodClots/Venous... · Thromboembolism and Antipsychotics ... case reports.[13-15] Since available](https://fdocuments.in/public/t1/desktop/images/details/download-thumbnail.png)
If you can't read please download the document
Transcript of Associations Between Venous Thromboembolism and...
-
ORIGINAL RESEARCH ARTICLEDrug SOfely 2008; 31 (8); 68&-694
01145916/08/
-
686
published between 1953 and 1984, several suspect-ed cases of VTE were reported with first-generationantipsychotics.[3] The possibility of an associationbetween treatment with antipsychotic drugs andVTE has received renewed attention during recentyearsp-121One of these studies, a case-control studypublished in 2000, found a significantly increasedrisk of venous thrombosis during treatment withfirst-generation antipsychotics.[61 However, it wasnot possible to reliably evaluate the association be-tween second-generation antipsychotics and throm-bosis as only a limited number of patients takingthese drugs were included in the study. In a recentlypublished retrospective cohort study among nursinghome residents, the rate of hospitalization for VTEwas significantly increased for users of the second-generation antipsychotic drugs (risperidone, olanza-pine, clozapine and quetiapine) but not for users offirst-generation antipsychotics.[101 While second-generation antipsychotic drugs are often used inpatients with dementia and dementia is associatedwith immobility, a risk factor for VTE, confoundingby indication is possible and may explain the as-sociations found. In another retrospective cohortstudy of patients aged ~65 years, no significantassociation between the use of antipsychotics andVTE was found'p2]With the exception of clozapine,there is, to date, no evidence of a link betweensecond-generation antipsychotics and VTE in pa-tients
-
Antipsychotics and Venous Thromboembolism
the UMC using the BCPNN method,ll5- 181This ana-lysis provides a statistical indicator, the IC, which isused to filter out combinations of particular drugsand suspected ADRs that are present in the databasemore frequently than would be expected on the basisof chance alone. An IC value can be calculated for aspecific drug-ADR combination. The IC is a loga-rithmic measure of association and is based on thenumber of case reports with a particular drug x (Cx),the number of case reports with a particular adversereaction (Cy), the number of reports with the specif-ic drug-ADR combination xy (Cxy) and the totalnumber of reports (C). The higher the Cx, Cy andCxy values are, the narrower becomes the credibilityinterval. The IC value can be viewed as the strengthof dependency between a drug and an adverse eventrelative to a background of all other adverse eventspontaneous reports. The credibility interval of theIC value provides a measure of the robustness of thevalue. An association between the drug and thereaction is considered statistically significant if thelower bound of the 95% credibility interval of the IC(IC025) is greater than zero. A subset of associationsupon clinical review are considered signals. TheBCPNN method has been described in detail pre-viously. [16-J8.20.23] The method has been thoroughlytested and evaluated[18.2*.25] and is effective in identi-fying early signals of possible ADRs, as evident bythe publication of important signals detected usingthe mcthodp6.27] Because of the incomplete natureof the dataset, the method is used for hypothesisgeneration rather than for hypothesis testing.
In the present study, the BCPNN method wasused with the WHO database to investigate whetherthere are more reports on VTE during treatment withantipsychotic drugs than would be expected on thebasis of chance alone based on general reporting inthis database. Additional analysis was performed toidentify possible risk factors. For this analysis, thefollowing antipsychotic drugs belonging to the ATCclassification group N05 were studied: the lOW-po-tency, first-generation antipsychotics chlorproma-zine, cyamemazine, melperone, levomepromazine,perazine and thioridazine; the high-potency, first-generation antipsychotics benperidol, bromperidol,clopenthixol, fluphenazine, flupenthixol, haloperi-dol, perphenazine, pimozide, tiotixene, trifluperidol,trifluoperazine and zuclopenthixol; and the second-
2008 Adis Data Information BV. All rights reserved.
687
generation antipsychotics amisulpride, aripiprazole,c1ozapine, olanzapine, remoxipride, risperidone,sertindole, sultopridc, quetiapine, ziprasidone andzotepine. We included clozapine in the analyses as apositive control since recurring, albeit preliminary,evidence supports an association with VTE. The ICwas calculated for the three antipsychotic groupsand for each particular compound separately. More-over, sex- and age-specific ICs were also calculated.As the risk for VTE in general is clearly increased inindividuals ~55 years of age,[28] study patients weredivided into two age groups;
-
688
clozapine and 379 concerned other antipsychoticdrugs. After scrutinizing these reports, 20 suspectedduplicate reports were found. These included tenpossible duplicate reports for clozapine, eight forolanzapine, one for zuclopenthixol and one for per-azine. All these were marked as duplicate reports inthe database. The remaining 734 patients were in-cluded in the case analysis.
Of all VTE reports, most concerned second-gen-eration antipsychotics (table I) and the second-gen-eration antipsychotics group had a positive IC025. Incontrast, the corresponding value was negative forboth the high-potency antipsychotics group and forthe low-potency, first-generation antipsychoticsgroup. Of the individual antipsychotics, olanzapinehad the highest IC025 values in addition to the posi-tive control clozapine. In addition, sertindole andzuclopenthixol had positive IC025 values; however,these associations were weaker, based on few cases(table I) and observed later (figure I). In addition,perazine had an IC025 value of 0.0 (table I). Whenusing the less specific definition VTE2, the IC val-ues for the associations between VTE2 and cloza-pine, olanzapine, sertindole and the second-genera-tion antipsychotics group were slightly lower thanfor VTEI but, with the exception of zuclopenthixol,were regarded as statistically significant.
IC values for the individual drugs olanzapine,sertindole, zuclopenthixol and clozapine related togender and age (information not always available)are presented in table II. A trend towards a higher ICvalue for olanzapine and clozapine in men comparedwith women was observed. Patient characteristics,doses and treatment durations in the VTEI cases arepresented in table III. Most patients were between20 and 50 years old. The median ages of the patientstreated with olanzapine, sertindole, and zu-clopenthixol were 45,37 and 52 years, respectively.In the VTE cases with known duration of therapywith these drugs, 60% (32/53) occurred within thefirst 3 months of treatment (table III). The corre-sponding figure for clozapine was 39% (94/242).The time intervals between the initiation of therapywith olanzapine and clozapine to occurrence of VTEare displayed in figure 2.
For cases where olanzapine, sertindole andzuclopenthixol were the suspected agents for VTE,concurrent medications with other drugs known to
2008 Adis Data Information BV. All rights reserved.
Haggel al.
increase the risk ofVTE were reported in eight cases(8%), three cases (50%) and zero cases (0%), re-spectively. The corresponding figure for clozapinewas 16 cases (4%). In 86% of the cases with concur-rent treatment with drugs known to increase the riskfor VTE, estrogen-containing medications were re-ported.
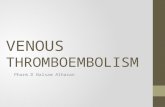
The associations became significant in 200 I,2002 and 2003 for sertindole, olanzapine andzuclopenthixol (figures lb, la and Ie), respectively.For comparison, the first time the IC025 value forclozapine and VTEI was above zero was in 1993,when 53 cases of the association were included andIC025 reached 0.07 (figure ld). A detailed analysis,including review of the individual cases, was under-taken and suggested a possible causal relationshipbetween use of these drugs and VTE.
Discussion
The reliability of data in the WHO database isdependent on the quality of the participating nation-al systems of spontaneous reporting of ADRs. Ingeneral, spontaneous ADR reporting is limited byfactors such as provision of incomplete informationand under-reporting.[29J Moreover, the reporting isinfluenced by several factors such as the extent ofuse of the drugs, the year of introduction to themarket, general knowledge of the adverse effects ofthe drug, public attention to specific problems andhealth professionals' attitudes to reporting of ADRs.Despite these limitations, assessing data from spon-taneous ADR reporting systems, including theWHO database, is an important and cost-effectiveway of detecting possible infrequent reactions,[18.19]although the method, by itself, cannot he used toestablish a conclusive causal relationship betweenan event and a drug.
Our analyses found that in the WHO ADR data-base, VTE was reported more often in combinationwith second-generation antipsychotic drugs andwith the individual drugs olanzapine, sertindole,zuclopenthixol and clozapine than would he expec-ted based on general reporting patterns in thedataset. The disproportional reporting of the anti-psychotic drugs olanzapine, sertindole, zu-clopenthixol and VTE represent new ADR signalsthat should be investigated further. The observeddisproportional reporting may have several explana-
Drug Safely 2008; 31 (8)
-
Antipsychotics and Venous Thromboembolism 689
tions in addition to there being a causal associationbetween the drugs and the ADR. These includereporting bias, confounding by indication, otherconfounding factors, that the association may havearisen by chance, or a combination of these factors.Given the nature of spontaneous reporting data, it isnot possible to exclude different types of bias. Con-
founding factors such as the underlying disease,smoking, obesity, which may in turn be associatedwith the antipsychotic drug treatment or immobili-zation could all have contributed to disproportionalreporting.
For olanzapine and risperidone, an associationbetween the drug and VTE has recently been sug-
Table I. Cases of venous thromboembolism (specific definition; VTE1) during treatment with antipsychotic drugs reported to the WHOdatabase, with information component (Ie) values"
Drugs Total no. of
reports for drug
VTE1
no. of casereports
IC value lower 95%credibility interval ofthe IC value (IC02S)
-2.6
-1.0
0.9
0.5
-0.2
-2.5
-0.1
0.3
-1.5
-0.2
-0.6
-1.8
-1.1
-1.8
-0.3
0.0
-1.6
0.7
-0.5
-0.9
-1.2
-1.4
-0.8
-1.6
-0.7
-1.2
-3.1
-5.3
-1.6
-1.3
0.2
-1.0
-1.0
0.2
-0.8
1.0
1.0
-0.8
0.8
0.8
0.5
0.3
0.2
-0.6
-0.2
-0.2
-1.0
-2.4
-0.5
0.9
1.0
-0.6
-0.2
2
2
2
9
8
41
7
1
o6
1
10
46
88
14
4
6
4
7
12
620
5785
665
2103
300
567
4330
69598
132
219
284
1561
2438
9428
1549
596
847
1794
20
848
13419
19277High potency, first-generationantipsychotics
Benperidol
Bromperidol
Clopenthixol
Flupenthixol
Fluphenazine
Haloperidol
Perphenazine
Pimozide
Tiotixene
Trifluoperazine
Trifluperidol
Zuclopenthixol
Low-potency first-generationantipsychotics
Chlorpromazine
Cyamemazine
Levomepromazine
Melperone
Perazine
Thioridazine
Second-generationantipsychotics
Amisulpride 945 2 -1.0
Aripiprazole 597 4 0.3
Clozapine 36739 385 1.0
Olanzapine 11 480 99 0.7
Quetiapine 2 857 20 0.4
Remoxipride 319 1 -0.4
Risperidone 15064 91 0.2
Sertindole 316 6 1.4
Sultopride 65 1 0.6
Ziprasidone 1678 13 0.6
Zotepine 249 3 0.8
a The table show the number of case reports and IC values prior to exclusion of suspected duplicates.
2008 Adis Dolo Information BV. All rights reserved. Drug Safety 2008; 31 (8)
-
690 Hiigg et al.
a3
2
o
-1
b
4
3
-3Olanzapine
-2 -'-T-------,..----r---.----.-------r----,.--.----1997 1998 1999 2000 2001 2002 2003 2004
Sertindole-4.L,------,-----,-----,----,.---,.---,.------r-
1997 1998 1999 2000 2001 2002 2003 2004
Zuclopenthixol
1980 1983 1986 1989 1992 1995 1998 2001 2004
d
4
3
2
o-1
-2
-3--4 Clozapine
197519781981 198419871990199319961999 2002
c4
2
-2
-4
~ 0
Year Year
Fig. 1. Change in the information component (IC) ploned cumulatively over time for the association between: (a) olanzapine and venousthromboembolism (VTE)1; (b) sertindole and VTE1; (c) zuclopenthixol; and VTE1 (d) clozapine and VTE1. The IC values are planed atquarterly intervals with the lower and higher bounds of the 95% credibility intervals shown.
gested in a population of nursing home residents>65 years of age,lIO] That study population may bevery different from younger populations usingsecond-generation antipsychotics with regard to thepresence of VTE risk factors. This, and confoundingby indication, may be an alternative explanation forthe associations found in that study.llD] To date, nostudy has been published investigating these as-sociations in individuals 55 years). Thus, young patients may also be at riskfor this possible ADR. Regarding risperidone, wefound no corresponding disproportional reporting in
the WHO database. However, because of the natureof the spontaneous reporting system, a negativefinding does not necessarily prove that there is noexcess risk for VTE during treatment with risper-idone, but only that relatively infrequent reportingoccurs. For sertindole and zuclopenthixol, no datahave been published supporting or challenging anassociation between these drugs and VTE.
As expected, the IC values were slightly higherusing a more specific definition of VTE (VTE I)compared with a wider definition where other ADRsmight be included (VTE2). Few additional caseswere identified when the less specific definition ofVTE was used, which suggests that if VTE is ob-served and reported it is often diagnosed as VTEI.
Approximately half of the VTE cases reportedduring the use of antipsychotics concerned cloza-pine. This association has been highlighted in case
2008 Adis Data Information BV. All rights reserved. Drug Safety 2008: 31 (8)
-
Antipsychotics and Venous Thromboembolism
reports,l31 ADR monitoring system reports[5] andretrospective autopsy data.[~8J A substantial numberof the clozapine reports in this study predated therecent publications reporting these associations,making reporting bias due to an increased awarenessless likely as an explanation. Since patients treatedwith clozapine are intensively monitored for agranu-locytosis, the possibility that the association be-[ween clozapine and VTE may be a result of anintense monitoring of other medical disorders can-not be excluded. However, the IC for VTE shouldnot be affected in such cases, as the reporting of a))suspected ADRs would be expected to increase.Another possible, or at least theoretical, explanationis that patients taking c10zapine might be more oftenco-prescribed drugs that are known to cause VTEthan other antipsychotics. However, are-evaluationof these reports showed that in only 4% of the casessuch exposure was present. Associations betweenolanzapine, sertindole, zuclopenthixol and VTEwere based on relatively fewer cases than clozapine.
691
In approximately one-sixth of these cases, olanza-pine was the suspected drug. Exposure to concomi-tantly used drugs that are known to cause VTE wasdocumented in only 8% of the olanzapine reports. Ina few case reports, an association between olanza-pine and VTE has been suggested. I13 .3D) However, asthe relationship in the database was statistically sig-nificant before these case reports were published,reporting bias is an unlikely explanation for thepositive IC value for olanzapine with VTE.
Associations between sertindole and zu-clopenthixol and VTE were based on only six andten reports, respectively. Possibly confoundingdrugs were present in three of the six reports wheresertindole was the suspected agent, making a causalassociation between sertindole and VTE less likely.IC and IC025 values for sertindole have remained atstable high levels since 200 1. In 1998, sertindolewas withdrawn [rom the market because of suspect-ed cardiac ADRs. The suspension was lifted in2001, but wider use of the drug has only occurred
IC
Table II. Cases of venous thromboembolism (specitic definition; VTE1) during treatment with clozapine, olanzapine, sertindole andzuclopenthixoJ, with information component (IC), in relation to sex and age"
Drug Total no. of _VT_E_1 _reports tor drug no. of case
reports
Clozapine 36739 385 1.0
Males 21122 180 1.4
Females 14 052 202 1.1
0-55 Y 27871 152 0.8
>55 Y 5 660 69 1.3Olanzapine 11480 99 0.7
Males 5 664 50 1.4
Females 5 181 46 0.4
Age 0-55 y 7184 68 0.6
Age >55 y 2499 18 0.5
Sertindole 316 6 1.4
Males 153 0 -0.6
Females 156 6 1.8
Age 0-55 y 233 4 1.0
Age >55 y 58 2 1.2
Zuclopenthixol 848 10 1.0
Males 484 6 1.5
Females 333 4 0.6
Age 0-55 y 609 6 0.6
Age >55 y 161 4 1.5a The table shows number of case reports and IC values prior to exclusion ot suspected duplicates.
2008 Adis Data Information 6V. All rights reserved.
0.9
1.2
0.9
0.7
1.0
0.5
1.0
0.0
0.3
-0.1
0.3
-3.5
0.6
-0.3
-0.5
0.2
0.4
-0.7
-0.5
0.2
Drug Safety 2006; 31 (8)
-
692 Hiigge! al.
Table III. Characteristics of cases of venous thromboembolism (specific definition; VTE1) during treatment with antipsychotic drugsreported to the WHO database after excluding suspected duplicates
Pt and treatment details _D.:..:ru..:::g ---,- ---,- _
clozapine olanzapine zuclopenthixol sertindole
2/6 (33%)
4/5 (80%)
6 (0/6/0)
37 (32-65)
20 (4-20)1
3/9 (33%)
25/44 (57%)
25/91 (26%)
94/242 (39%)
375 (176/196/3) 91 (45/43/3) 9 (6/3/0)
40 (20--89)a 45 (20--87)b 52 (33-64)
350 (12-2000) 10 (3-100)d 150 (100--200)8, IV or1M in four sUbjects;25 mg PO in one subject
4/5 (80%)Duration of drug treatment(proportion ~3 months)
Percentage of monotherapy 201/375 (54%)
Number of pts (m/f/unknown)
Median age, y (range)
Median dose, mgld (range)
a Information available in 361 cases.
b Information available in 78 cases.
c Information available in 199 cases.
d Information available in 40 cases.
e Depot formulation.
Information available in 3 cases.
f = females; 1M = intramuscular administration ; IV = intravenous administration; m = males; PO = oral administration; pI = patient.
O-'----..L......JL...L---'-..L......J~-_r-'--'----'-..L......JL...L--"--
Clozapine Olanzapine
Duration of treatment (mo)
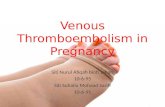
Fig. 2. Time from start of therapy to occurrence of venous thrombo-embolism 1 for the reports where clozapine and olanzapine wereimplicated as suspected drugs (data available in 64.5% of the clo-zapine reports and 48.3% of the olanzapine reports).
high-potency drugs. Separate analyses for each drugwere not undertaken in that study. The reason for thediscrepancy between our data and the results fromthe case-control study is unclear but may well reflectthe differences in data sources used and the method-ologies employed.
The median doses in the VTE cases were slightlyhigher than the defined daily dose (DDD) for c1oza-pine (300 mg) and equal to the DDD for olanzapine(10 mg), indicating that the reaction was not depen-dent on excessive doses of these drugs. Due to the
D 0.00-1.00D 1.01-2.00.2.01-3.00
D 3.01-4.00D 4.01-5.00.5.00-6.00
>6.00
10
60
~ 50oCo~ 40'0Q)
g> 30CQ)
~ 208:
very recently. We have not found any previousreports suggesting that sertindole has been asso-ciated with VTE. The association betweenzuc1openthixol and VTE was statistically significantonly when the specific VTE definition (VTE1) wasused. When using the less specific VTE definition(VTE2), the association was not statistically signif-icant. Furthermore, no previous reports suggestingthat zuc1openthixol is associated with VTE havebeen identified in the literature. These findingsmight thus be coincidental, but further investiga-tions are nevertheless warranted. A trend towardshigher IC values for olanzapine and c10zapine inmen compared with women was observed, sug-gesting a more disproportional reporting in men.However, it is possible that some VTE events inwomen using antipsychotic drugs may have beenattributed to the concomitant use of estrogens. Thus,it remains an open question as to whether there is atrue gender difference in risk.
We found no association between VTE and eitherlow-potency or high-potency first-generation anti-psychotics as a group. In contrast, an association forfirst-generation antipsychotics is supported by onelarge case-control study ,[6] which found a relativerisk of 7.1 (95% CI 2.3, 22.0) for current anti-psychotic use compared with no antipsychotic use.Low-potency first-generation antipsychotic drugswere more strongly associated with VTE than were
2008 Adis Data Information 8V. All rights reserved. Drug Safety 2008; 31 (8)
-
Antipsychotics and Venous Thromboembolism
limited number of cases, no solid analysis can bemade about the prescribed doses for sertindole andzuclopenthixol. In 60% of the VTE cases the eventoccurred within the first 3 months of treatment in thecases associated with olanzapine, sertindole andzuclopenthixol. The corresponding figure was 39%in the cases associated with clozapine. Similar find-ings have been reported previously.[5l However, itshould be taken into account that in the majority ofour reports, the treatment duration was unknown.Therefore, the results should be interpreted cau-tiously. Moreover, any association between a drugand an ADR is more obvious shortly after institutionof treatment and thus more likely to be reported.
The mechanisms underlying the relationship be-tween antipsychotic drugs and VTE are basicallyunknown but some plausible mechanisms have beensuggested, such as antipsychotic-induced sedation,obesity, hyperleptinemia, presence of antiphospho-lipid antibodies and enhanced platelet aggrega-tionYJ The use of clozapine has been shown toincrease platelet adhesion and aggregationYIJ Clo-zapine and olanzapine also have a particular propen-sity to induce metabolic abnormalities such as obesi-ty and hyperleptinemia.[J] Moreover, antipsychoticdrugs might predispose patients to venous thrombo-sis because of their sedative effects leading to im-mobilization and thereby venous stasis and bloodpooling in the lower extremities. Significant seda-tion is a common ADR for many second-generationantipsychotics, particularly clozapine. l32] Increasedadrenaline (epinephrine) secretion in patients havingacute psychotic excitation has also been suggestedas a possible factor enhancing blood coagulation,l33Jalthough no experimental data supporting this hypo-thesis have been published. Moreover, the frequen-cy of smoking among patients with schizophrenia isincreased compared with the general popula-tion.[34.35l However, some studiesl36l suggest thatsmoking is associated with a very small increasedrisk for VTE only, and others do not generallyaccept smoking as an important risk factor forVTE.[3738] Nevertheless, disease-related factors can-not explain why positive associations were observedfor c1ozapine, olanzapine, sertindole and zu-clopenthixol only, and not for all other antipsychot-ics or for antipsychotics in general. In the previouslymentioned large case-control study,[6l psychiatric
2008 Adis Data Information BV. All rights reserved.
693
conditions such as schizophrenia, other psychoses,affective and anxiety disorders and insomnia werenot independently associated with VTE.
Conclusions
The results of the present study show that VTEwas more often reported with the antipsychoticdrugs olanzapine, sertindole and zuclopenthixolthan with other drugs in the WHO database and aresuggestive of a causal relationship between thesedrugs and VTE in patients aged ~20 years. How-ever, one should bear in mind that results generatedfrom disproportionality analysis of spontaneousADR databases cannot be used to establish causali-ty. Therefore, further investigations are needed toexplain this signal and studies using alternativemethodologies are required to determine whetherantipsychotics actually cause VTE, to identify thefrequency of this possible adverse reaction, to ex-plore the mechanism and to identify possible riskfactors. Until such data are available, cliniciansshould be aware of VTE as a possible adverse reac-tion associated with use of antipsychotic agents. Inpatients experiencing VTE during treatment with anantipsychotic agent, it seems reasonable to reassessthe risks and benefits of continued therapy with thedrug.
Acknowledgements
We thank the national centres that contribute data to theWHO international drug monitoring programme. The opin-ions and conclusions in this article are. however. not necessa-rily those of the various national centres or of the WHO. Theresearch was funded by the Swedish Research Council andthe WHO Collaborating Centre without other external fund-ing. The corresponding author had full access to all the data inthe study and had final responsibility for the decision tosubmit for publication. The authors have no contlicts ofinterest directly relevant to the content of this study.
Referencesl. Melkersson K. Dahl ML. Adverse metabolic effects associated
with atypical antipsychotics: literature review and clinicalimplications. Drugs 2004: 64: 701-23
2. Newcomer JW. Metabolic risk during antipsychotic treatment.Clin Ther 2004: 26: 1936-46
3. Htigg S. Spigset O. Antipsychotic-induced venous thromboem-bolism: a review of the evidence. CNS Drugs 2002: 16: 765-76
4. Walker AM. Lanza LL. Arellano F. et al. Mortality in currentand fonner users of clozapine. Epidemiology 1997: 8: 671-7
5. Hligg S. Spigset O. Soderstrom TG. Association of venousthromboembolism and clozapine. Lancet :WOO: 355: 1155-6
Drug Safety 2008; 31 (8)
-
694
6. Zomberg GL. Jick H. Antipsychotic drug use and risk of tirst-time idiopathic venous thromboembolism: a case-controlstudy. Lancet :WOO: 356: 1219-23
7. Thomassen R. Vandenbroucke1P. Rosendaal FR. Antipsychoticmedication and venous thrombosis. Br J Psychiatry 200 1: 179:63-6
8. Parkin L. Skegg DC. Herbison GP. et al. Psychotropic drugs andfatal pulmonary embolism. Pharmacoepidemiol Drug Saf2003: 12: 647-52
9. Farah RE. Makhoul NM. Farah RE. et al. Fatal venous thrombo-embolism associated with antipsychotic therapy. Ann Pharma-cother 2004: 38: 1435-8
10. Liperoti R. Pedone C. Lapane KL. et al. Venous thromboembo-lism among elderly patients treated with atypical and conven-tional antipsychotic agents. Arch Intern Med 2005: 165:2677-82
II. Hamanaka S. Kamijo Y. Nagai T. et al. Massive pulmonarythromboembolism demonstrated at necropsy in Japane e psy-chiatric patients treated with neuroleptics including atypicalantipsychotics. Cire J 2004: 68: 850-2
12. Ray JG. Mamdani MM. Yeo EL. Antipsychotic and antidepres-sant drug use in the elderly and the risk of venous thromboem-bolism. Thromb HaclIlosl 2002; 88: 205-9
13. Waage 1M. Gedde-Dahl A. Pulmonary embolism possibly asso-ciated with olanzapine treatment [Ieller]. BMJ2003: 327: 1384
14. del Conde I. Goldhaber SZ. Pulmonary embolism associatedwith olanzapine [Ieller]. Thromb Haemost 2006: 96: 690-1
15. Kamijo Y. Soma K. Nagai T. et al. Acute massive pulmonarythromboembolism associated with risperidone and conven-tional phenothiazines. Circ J 2003: 67: 46-8
16. Bate A, Lindquist M. Edwards JR. et al. A Bayesian neuralnetwork method for adverse drug reaction signal generation.Eur J Clin Pharmacol 1998: 54: 315-321
17. Bate A, Lindquist M. Orre R. et al. Data-mining analyses ofpharmacovigilance signals in relation to relevant comparisondrugs. Eur J Clin Pharmacol 2002: 58: 483-490
18. Lindquist M. Stahl M. Bate A. et al. A retrospective evaluationof a data mining approach to aid finding new adverse drugreaction signals in the WHO international database. Drug Saf2000: 23: 533-42
19. Edwards IR. Olsson S. WHO programme: global monitoring.In: Mann RD. Andrews EB. editors. Pharmacovigilance.London: John Wiley & Sons: 2002: 169-182
20. Orre R. Lansner A. Bayesian neural networks with confidenceestimations applied to data mining, Comput Stat Data Anal2000: 34: 473-493
21. Edwards IR. Biriell C. Harmonisation in pharmacovigilance.Drug Saf 1994; 10: 93-102
22. WHO Collaborating Centre for Drug Statistics Methodology[online]. Available from URL: hIlP://www.whocc.no/[Ac-cessed 2005 May 15]
23. Noren GN, Bate A. Orre R. et al. Extending the methods used toscreen the WHO drug safety database towards analysis of
2008 Adis Data Information BV. All rights reserved.
Hiigg et al.
complex associations and improved accuracy for rare events.Stat Med 2006: 25: 3740-57
24. van Puijenbroek EP. Bate A. Leufkens HG. et al. A comparisonof measures of disproponionality for signal detection in spon-taneous reporting systems for adverse drug reactions.Pharmacoepidemiol Drug Saf 2002: II: 3-10
25. Lindquist M. Edwards IR. Bale A. et al. From association toalen: a revised approach to international signal analysis.Pharmacoepidemiol Drug Saf 1999: 8: S 15-25
26. Sanz EJ. De-las-Cuevas C. Kiuru A. et al. Paroxetine in preg-nant women: SSRI and neonatal withdrawal syndrome. Lancet2005: 365: 482-7
27. Coulter OM. Bate A. MeyboOlll RH. et al. Antipsychotic drugsand heart muscle disorder in international pharmacovigilance:data mining study. BMJ 2001: 322: 1207-9
28. Anderson Jr FA, Wheeler HB. Goldberg RJ. et al. The preva-lence of risk factors for venous thromboembolism amonghospital patients. Arch Intern Med 1992: 152: 1660-4
29. ten Ham M. WHO's role in international ADR monitoring. PostMark Surveillance 1992: 5: 223-30
30. Hagg S. Tatting P. Spigs~t O. Olanzapine and venous thrombo-embolism. lnt Clin Psychopharmacol 2003: 18: 299-300
31. Axelsson S. Hagg S. Eriksson AC. et al. In vitro effects ofantipsychotics on human platelet adhesion and aggregationand plasma coagulation. Clin Exp Phanllacol Physiol 2007:34: 775-80
32. Wagstaff AJ. Bryson HM. Clozapine: a review of its pharmaco-logical propenies and therapeutic use in patients with schizo-phrenia who are unresponsive to or intolerant of classicalantipsychotic agents. CNS Drugs 1995: 4: 370-400
33. Lazarus A. Physical restraints. thromboembolism. and death in2 patients. J Clin Psychiatry 200 1: 62: 207-8
34. Hughes JR. Hatsukami OK. Mitchell JE. et al. Prevalence ofsmoking among psychiatric outpatients. Am J Psychiatry1986: 143: 993-7
35. Beratis S, Katrivanou A. Gourzis P. Factors affecting smokingin schizophrenia. Compr Psychiatry 2001: 42: 393-402
36. Goldhaber SZ. Grodstein F. Stampfer MJ. et al. A prospectivestudy of risk factors for pulmonary embolism in women.JAMA 1997: 277: 642-5
37. Danilenko-Dixon DR. Heit JA. Silverstein MD. et aJ. Riskfactors for deep vein thrombosis and pulmonary embolismduring pregnancy or post partum: a population-based. case-control study. Am J Obstet Gynecol 200 I: 184: 104-] 0
38. Rosendaal FR. Risk factors for venous thrombotic disease.Thromb Haemost 1999: 82: 610-9
Correspondence: Dr Staffan Hiigg, Division of Clinical Phar-macology, Link6ping University Hospital, 5-581 85Linkoping, Sweden.E-mail: staffan.haggimv.liu.se
Drug Safety 2008: 31 (8)