ASSESSMENT OF VISUAL ACUITY IN INFANCY AND EARLY CHILDHOOD
9
Click here to load reader
-
Upload
janette-atkinson -
Category
Documents
-
view
216 -
download
1
Transcript of ASSESSMENT OF VISUAL ACUITY IN INFANCY AND EARLY CHILDHOOD

S Y M P O S I U M E A R L Y V I S U A L D E V E L O P M E N T March 1982, Solna, Sweden
Acta Ophthalmol (Copenh). Suppl157: 18-26
Department of Experimental Psychology (Head: N . J . Mackintosh), University of Cambridge, England
ASSESSMENT OF VISUAL ACUITY IN INFANCY AND EARLY CHILDHOOD
BY
JANETTE ATKINSON and OLIVER BRADDICK
The forced-choice preferential looking method (FPL) shows the development of acuity during the first year of life, and is applicable to clinical assessment. A tracking test using a narrow strip of grating yields a more sensitive measure for the later part of this age range, however. The development of acuity is dominated by neural rather than optical or accommodative factors. By age 3 years resolution acuity is very close to adult performance, but at 5 years ‘crowding’ effects may still impair performance on practical acuity tasks more than for the adult.
Key word!: visual acuity - preferential looking - visual development in infancy - crowding effect.
Methods of assessing vision in infants and young children have greatly developed in recent years, with techniques, originally devised for research work, being applied to clinical problems. One of the best established techniques is forced choice preferential looking (FPL) pioneered by Davida Teller (Teller et al. 1974; Teller 1979) and used in our laboratory (Atkinson et al. 1977; Atkinson & Braddick 1981; Atkinson et al. 1982) and a number of others (for example, Banks & Salapatek 1978; Gwiazda et al. 1978; Allen 1978). In this method the infant is presented on each trial with a patterned screen on one side and a blank screen of matched average luminance on the other (see Fig. 1). On successive presentations the side on which the pattern is presented is randomly changed; if the infant consistently looks at the patterned side this is evidence that he or she can detect the pattern. The judgement of which side the infant is attending is made as a forced choice by an
18

Fig. 1. Preferential looking testing of acuity. The infant shown is a one year old and is being tested to
check the visual effectiveness of a refractive correction.
observer who does not know on which side the pattern is presented, so the percentage correct of the observer’s judgements can be used as an index of the infant’s detection. The commonest application of the method has been with graded series of striped patterns to assess infant acuity, although it can also be used to investigate contrast sensitivity and colour discrimination.
The optimal age range for the use of this method is between 1 and 6 months, when infants will readily attend to the stimulus patterns over sufficient repetitions to obtain a reliable measure of threshold. An important point for clinical use of the method is that it can be used to test each eye separately (Atkinson et al. 1982) although somewhat more care is needed in handling and observing the child than for binocular testing. Many children remain testable by FPL at 9 or 12 months or even older, but over this age range infants become rapidly bored with the test stimuli and are too active to watch them passively for long. When the method is applied to these older infants, approximate estimates of acuity may often have to be made from shorter sequences of presentations than our full staircase procedurg. In some cases of mental retardation, FPL may provide a valuable means of visual assessment well outside the usual age range.
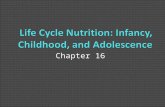
Fig. 2 presents FPL acuity data obtained in our laboratory in a number of studies at different ages, with acuity at ages 3-4 obtained by a different behavioural
19

method (Atkinson et al. 1981a) for comparison. Comparable data on the development of acuity in infancy have been described by Dobson & Teller (1978) and Held (1979). Acuity develops very rapidly over the first few months of life, but at 6 months is still clearly less than adult norms. By 3-4 years acuity is 6/6 or better with grating targets and thus approximates of that adult. Because of the difficulties of accurate testing in the age range 1-3 years it is not yet possible to state at what age adult acuity is approached, but in any case it is clear that this approach is gradual and asymptotic. It should be noted that over the early months, quite marked individual variations in acuity are found (Atkinson et id. 1982; Allen 1978).
0 05 1 2 3 4 adult age years
Fig. 2. Mean acuity measurements at different ages from studies in our laboratory. Different studies at given age differ in parameters such as screen size and separation: thus the highest acuity found at a given age presumably represents performance as revealed by conditions closest to optimal. Solid circles are data from preferential looking tests; the star is from the tracking test on a Gaussian-modulated grating (see Figs. 4 and 5 ) ; triangles are from grating orientation
discrimination in an alley-running task.
20

I I
/
, , ,
/
0
/
l o I
I / * I .
I ' $ I I I ,* *
* * b
* left eye * right eye
0 binocular
0 5 1 2 3
Fig. 3 . age years
4
Results of acuity tests on an infant who had bilateral cataracts removed at 1-2 weeks of age. All data were obtained by preferential looking except the point for age 3 years, which was obtained by testing with Sheridan-Gardiner optotypes. The dashed line is taken from the
normal data of Fig. 2 for comparison.
Fig. 3 shows an example of the clinical application of FPL. This patient had bilateral congenital cataracts removed from one eye at 1 week of age and from the second eye at 2 weeks of age, and the acuity of each eye separately followed by FPL though the first year. The child is now 3 years old, and the final point on the graph represents his 6/24 acuity determined at 3 m with single optotypes (Sheridan- Gardiner). The FPL measures reflect a development of acuity which follows a similar course to normal development but is lower age-for-age : this difference may be due in part to difficulties in maintaining a clear aperture for vision and perhaps also to the difficulty of exact refractive correction.
21

In recent work we have been looking for a method that may be better adapted than PL to the visual behaviour of infants over 6 months. Existing tests which require infants to track a moving object, such as the Catford Drum (Catford & Oliver 1973) and the STYCAR Balls (Sheridan 1976) seem to be successful in eliciting visual attention in infants aged 6-18 months. However, the spots of varying size used in such tests are not appropriate for testing acuity (Atkinson et al. 198Ib). A more appropriate target is a narrow band of grating whose contrast is smoothly reduced on either side by a Gaussian function so that its edges merge with a background of equal mean luminance, as illustrated in Fig. 4. This pattern (as for a grating) is invisible against the background for a child whose acuity is too low to resolve the stripes, but, like a spot, when it is visible it forms a localized target that can be tracked. In our test the infant’s attention is initially drawn to the centre of the screen by a high contrast flashing bar with a synchronized accompanying sound. This bar is replaced by the test target which moves off either to the left or right. An observer has to judge direction of the infant’s tracking eye movement. As in the FPL method, the observer’s judgement is forced-choice without knowledge of the side to which the stimulus moves. Acuity may be tested by using a range of different
Fig. 4 . Stimulus used in a tracking test. The spatial frequency of the grating can be varied to assess acuity. The contrast of the grating is modulated by a Gaussian function whose space constant is 4 times the grating period. A grating whose spatial frequency exceeds the acuity limit becomes invisible against the background (this may not be true in this example due to
non-linearities in the reproduction process).
22

acuity in tracking task c/degree
-
age 27-36 weeks
PL acuity c/degree
Fig. 5. Comparison of acuity measures on 11 individual infants using the tracking stimulus of Fig. 4 (ordinate) and preferential looking (abcissa). The diagonal line represents equal assessment
of acuity by the 2 measures.
stripe widths. Fig. 5 shows the acuity of a group of 6-9 month olds as measured by this tracking test, compared with the acuity of the same infants assessed by FPL. In almost every case, the tracking test provides the higher estimate of acuity. We conclude that at this age behaviour elicited in the tracking test more closely reflects the limits of the infant’s visual performance than does FPL, although it must be pointed out that, because each presentation is longer, the tracking test is also somewhat more laborious. We are currently experimenting with various adapta- tions of this tracking procedure to see whether they can be used to assess acuity in infants aged 9-18 months, an age range where clinical information is often required but which is very difficult to test with existing techniques.
The rapid initial development of acuity in the first 6 months of life (see Fig. 2) raises the question of whether this development is due to improvement in the optical quality of the image on the infant’s fundus, or to maturation of the neural pathways signalling visual pattern information to the brain. We have used a
23

photographic method (Howland & Howland 1974) to examine the accuracy of accommodation in young infants (Braddick et al. 1979). Between birth and 6 months infants show a considerable improvement in accommodation, especially for targets at distances of over 1 m. However, our calculations show that the errors of accommodation for infants under 6 months are by no means great enough to account for the relatively low acuity of these infants in PL testing. The same conclusion has been reached from dynamic retinoscopic studies of infant accommodation (Banks 1980). It seems, therefore, that the acuity of the young infant is primarily limited by neural rather than optical factors, and that the early improvement in acuity reflects development of the nervous system.
The improvement in accommodation over the same period may be a conse- quence rather than a cause of this, since accurate control of accommodation requires good neural information transmission to signal errors of defocus.
Acuity, as discussed so far, is the simple detection of fine spatial detail, as exemplified by resolution of a grating. Fig. 2 shows that this function is effectively mature by age 3% years, if not earlier. However, such a measure of acuity may be an incomplete indicator of visual function. It is clinically well known that some patients, for instance many amblyopes, show much poorer acuity for recognition of letters in an array such as a Snellen chart than for an isolated letter or for grating target. This phenomenon is known as ‘crowding’ (Hilton & Stanley 1972). We have recently investigated the acuity of normal 5 year olds for single optotypes and for
o c c o c o
0,Co =OC
Fig. 6. Stimulus arrangements used to test ‘crowding’ effects on acuity in 5-year-olds and adults. In the circular array (below) only the central symbol has to be identified. With both arrange- ments the children’s acuity was impaired, relative to single symbols, more than that of the adults, although this ‘crowding’ effect was more marked with the circular than with the linear array. A choice between C and 0 symbols was used, rather than the conventional Landolt C‘s,
to avoid orientation confusions to which young children are prone.
24

the same figures in arrays. Fig. 6 shows examples of the test stimuli used. As would be expected from the data of Fig. 2, these children showed adult acuity for the single optotypes. However, their acuity for the ‘crowded’ stimuli was only 58% of the adults’ in the case of the circular array. It is clear then that ‘crowding’ is not a phenomenon restricted to amblyopes, but that it indicates a respect in which 5 year olds fall short of mature visual information processing despite their adult-like acuity for simple targets. It is possible that younger children and infants show still greater crowding effects. It remains a challenge for future research to test this. In any case, i t is clear that the development of grating acuity is a valuable basic indicator, but by no means a complete account of the maturation of pattern vision.
Acknowledgments
This work was supported by the Medical Research Council of Great Britain. We gratefully acknowledge the assistance of Elizabeth Pimm-Smith, Carol Evans, and Gill Harding, and the collaboration of Mr. P. G. Watson, Consultant Ophthalmic Surgeon, Addenbrooke’s Hospital, in the study of clinical cases such as that described by Fig. 3.
References
Allen J L (1978): The development of visual acuity in human infants during the early postnatal weeks. Unpublished Ph.D. thesis, University of Washington.
Atkinson J. Braddick 0 & Moar K (1977): Development of contrast sensitivity over the first 3 months of life in the human infant. Vision Res 17: 1037- 1044.
Atkinson J & Braddick 0 (1981): Acuity, contrast sensitivity and accommodation in infancy. I n : Aslin R, Alberts J R & Petersen M R (eds). Development of Perception, Vol2: 245-277. Academic Press, New York.
.4tkinson J, French J & Braddick 0 (1981a): Contrast sensitivity function of pre-school children. Br J Ophthalmol65: 525-529.
Atkinson J, Braddick 0, Pimm-Smith E, Ayling L & Sawyer R (1981b): Does the Catford Drum give an accurate assessment of acuity? Br J Ophthalmol65: 652-656.
Atkinson J, Braddick 0 & Pimm-Smith E (1982): ‘Preferential looking’ for monocular and binocular acuity testing in infants. Br J Ophthalmol66: 264-268.
Banks M S (1980): The development of visual accommodation during early infancy. Child Dev 5 1 : 646-666.
Banks M S & Salapatek P (1978): Acuity and contrast sensitivity in I-, 2-, and 3-month-old human infants. Invest Ophthalmol Vis Sci 17: 361-365.
Braddick 0 J, Atkinson J, French J & Howland H C (1979): A photorefractive study of infant accommodation. Vision Res 19: 1319- 1330.
Catford G V & Oliver A (1973): Development of visual acuity. Arch Dis Child 48: 47-50. Dobson V & Teller D Y (1978): Visual acuity in human infants: A review and comparison of
behavioural and electrophysiological studies. Vision Res 18: 1469- 1483. Held R (1979): Development ofvisual resolution. Can J Psycho1 33: 213-221. Held R, Gwiazda J, Brill S & Mohindra I (1978): Infant visual acuity and its meridional
variation. Vision Res 18: 1557- 1564.
25

Hilton A F & Stanley J C (1972): Pitfalls in testing children’s vision by the Sheridan Gardiner
Howland H C & Howland B (1974): Photorefraction: a technique for study of refractive state
Sheridan M D (1976): Manual for the STYCAR Vision Tests. NFER Publishing Company
Teller D Y (1979): The forced-choice preferential looking procedures: a psychophysical
Teller D Y, Morse R, Borton R & Regal D (1974): Visual acuity for vertical and diagonal
single optotype method. Br J Ophthalmol56: 135- 139.
at a distance. J Opt SOC Am 64: 240-249.
Ltd., London.
technique for use with human infants. Infant Behav Dev 2: 135- 153.
gratings in human infants. Vision Res 14: 1433- 1439.
Author4 address:
Department of Experimental Psychology, University of Cambridge, Downing Street, Cambridge CB2 3EB, England.
26