Assessment of Secondary Cleft Rhinoplasty Using Resorbable ... · Assessment of Secondary Cleft...
5
Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited. Assessment of Secondary Cleft Rhinoplasty Using Resorbable Plates at the Age of Primary School Arun K. Gosain, MD and Amir H. Fathi, MD Background: Secondary rhinoplasty after a cleft lip repair remains a significant challenge. We have developed a technique in which re- sorbable plates are used to support the cleft alar cartilage to minimize relapse. There are few guidelines by which one can objectively assess the outcome of cleft rhinoplasty over time. This study attempts to demonstrate a means by which the symmetry and form of the pro- posed rhinoplasty technique can be evaluated. Methods: Sixteen patients with unilateral cleft lip/palate repair had a secondary rhinoplasty performed at age 6 to 8 years, using a resorb- able plate (resorption time, 2Y3 years) placed between the nasal lining and cleft alar cartilage to simulate the shape of the noncleft cartilage. Photographs were taken preoperatively and postoperatively. Median follow-up was 9.6 T 2.8 months. Various angles and ratios were measured to demonstrate outcomes, comparing preoperative to post- operative measures, and symmetry between cleft and noncleft sides. Results: Postoperatively, the angle between the horizontal axis, drawn across the alar base and tangent to the alar rim on both sides, was significantly altered (P G 0.001); both sides were closer to 60 degrees (mean, 56.28 degrees), approximating the angle of the aesthetic norm. A measure of the angle between the horizontal axis and a line drawn from midpoint of axis to nasal tip was sig- nificantly closer to 90 degrees (P G 0.05). The shape of the affected nostril became more oval and symmetric relative to the unaf- fected side (P G 0.05). Angle between the horizontal axis and a line drawn through the widest point of each nostril was close to zero. (P G 0.001). The difference in nostril height between the cleft and noncleft sides was significantly decreased (P G 0.001). Conclusion: We have objectively evaluated the outcomes of our technique of secondary cleft rhinoplasty using resorbable plates for alar support. A careful geometric evaluation of preoperative and postoperative photographs can help determine the symmetry and overall quality of the result. These measures may help to evaluate long-term outcomes of cleft rhinoplasty over time. Key Words: Secondary cleft rhinoplasty, cleft nasal deformity, resorbable plates, photogrammetric analysis (J Craniofac Surg 2009;20: 1801Y1805) U nilateral cleft nasal deformity is a clinical term referring to a nose with residual deformity after primary unilateral lip and palate repair. 1 The complex three-dimensional nature of this anomaly involves skin, cartilage, vestibular lining, and skeletal platform. Cor- rection of this deformity remains a challenging problem for recon- structive surgeons. 2 Growth increases the complexity of secondary cleft nasal correction. The nose undergoes a late growth spurt during puberty and early adolescence, and surgical intervention has the potential to interfere with this growth. Therefore, appropriate timing of repair is of paramount importance. We believe that secondary cleft nasal correction is often indi- cated at the age of primary school (ages 6Y8 years). At this age, patients’social interactions increase significantly, and they begin to experience significant pressures from peers that form their self- image. Although final rhinoplasty may still be required after the completion of nasal growth, we feel that secondary correction at this age is warranted to as to optimize the child’s developing self-image. The optimal technique for providing support of the cleft alar cartilage at the age of primary school remains controversial. Millard 3 describes an alar lift to correct the unilateral cleft nasal deformity and recommends that this be done at the age of primary school and no earlier than age 5 years as the cartilage is felt to be too delicate to retain its position before this age. Whereas there has been an ongoing debate as to whether rhinoplasty performed before age 16 to 18 years causes long-term alteration in growth of the nose, Ortiz- Monasterio and Olmedo 4 have demonstrated that corrective rhinoplasty performed before puberty does not interfere with the long-term growth of the nose. However, other authors feel that definitive nasal surgery should be delayed as flattening of the alar cartilage will continue throughout adolescence, and the underlying maxillary deficiency cannot be corrected until skeletal growth is complete. 5,6 Therefore, many patients will require definitive cleft rhinoplasty after skeletal maturation is complete. 6 Cartilage grafts placed at primary school age may therefore become obsolete should completion rhinoplasty be required after completion of skeletal growth. In addition, harvest of septal cartilage at primary school age would preclude the possibility of reharvest of this donor site as a source of nonscarred graft at a later age. To address this issue, we have developed a technique in which resorbable plates are used to support the cleft alar cartilage during rhinoplasty performed at primary school age to minimize relapse. The aims of the current study were to (1) describe our technique for primary cleft rhinoplasty at primary school age using resorbable plates and (2) demonstrate a means by which the symmetry and form of the proposed rhinoplasty technique can be evaluated. METHODS A total of 16 patients, 10 boys and 6 girls with unilateral cleft lip and nasal deformity, were included in this study. All patients operated on by the senior author who underwent secondary cleft rhinoplasty at primary school age and had placement of resorbable ORIGINAL ARTICLE The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 1801 From the Department of Plastic Surgery, Case Western Reserve University School of Medicine, Cleveland, Ohio. Received February 6, 2009. Accepted for publication March 11, 2009. Address correspondence and reprint requests to Arun K. Gosain, MD, Department of Plastic Surgery, Case Western Reserve University, University Hospitals of Cleveland, MS 5044, 11100 Euclid Ave, Cleveland, OH 44106; E-mail: [email protected] This article did not require any sources of funding. The authors declare that they had no financial interests or commercial associations during the course of this study. Copyright * 2009 by Mutaz B. Habal, MD ISSN: 1049-2275 DOI: 10.1097/SCS.0b013e3181b5d4c0
Transcript of Assessment of Secondary Cleft Rhinoplasty Using Resorbable ... · Assessment of Secondary Cleft...

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Assessment of Secondary Cleft Rhinoplasty UsingResorbable Plates at the Age of Primary School
Arun K. Gosain, MD and Amir H. Fathi, MD
Background: Secondary rhinoplasty after a cleft lip repair remains asignificant challenge. We have developed a technique in which re-sorbable plates are used to support the cleft alar cartilage to minimizerelapse. There are few guidelines by which one can objectively assessthe outcome of cleft rhinoplasty over time. This study attempts todemonstrate a means by which the symmetry and form of the pro-posed rhinoplasty technique can be evaluated.Methods: Sixteen patients with unilateral cleft lip/palate repair had asecondary rhinoplasty performed at age 6 to 8 years, using a resorb-able plate (resorption time, 2Y3 years) placed between the nasal liningand cleft alar cartilage to simulate the shape of the noncleft cartilage.Photographs were taken preoperatively and postoperatively. Medianfollow-up was 9.6 T 2.8 months. Various angles and ratios weremeasured to demonstrate outcomes, comparing preoperative to post-operative measures, and symmetry between cleft and noncleft sides.Results: Postoperatively, the angle between the horizontal axis,drawn across the alar base and tangent to the alar rim on both sides,was significantly altered (P G 0.001); both sides were closer to60 degrees (mean, 56.28 degrees), approximating the angle ofthe aesthetic norm. A measure of the angle between the horizontalaxis and a line drawn from midpoint of axis to nasal tip was sig-nificantly closer to 90 degrees (P G 0.05). The shape of the affectednostril became more oval and symmetric relative to the unaf-fected side (P G 0.05). Angle between the horizontal axis and aline drawn through the widest point of each nostril was close to zero.(P G 0.001). The difference in nostril height between the cleft andnoncleft sides was significantly decreased (P G 0.001).Conclusion: We have objectively evaluated the outcomes of ourtechnique of secondary cleft rhinoplasty using resorbable plates foralar support. A careful geometric evaluation of preoperative andpostoperative photographs can help determine the symmetry andoverall quality of the result. These measures may help to evaluatelong-term outcomes of cleft rhinoplasty over time.
Key Words: Secondary cleft rhinoplasty, cleft nasal deformity,resorbable plates, photogrammetric analysis
(J Craniofac Surg 2009;20: 1801Y1805)
Unilateral cleft nasal deformity is a clinical term referring to a nosewith residual deformity after primary unilateral lip and palate
repair.1 The complex three-dimensional nature of this anomalyinvolves skin, cartilage, vestibular lining, and skeletal platform. Cor-rection of this deformity remains a challenging problem for recon-structive surgeons.2 Growth increases the complexity of secondarycleft nasal correction. The nose undergoes a late growth spurt duringpuberty and early adolescence, and surgical intervention has thepotential to interfere with this growth. Therefore, appropriate timingof repair is of paramount importance.
We believe that secondary cleft nasal correction is often indi-cated at the age of primary school (ages 6Y8 years). At this age,patients’ social interactions increase significantly, and they begin toexperience significant pressures from peers that form their self-image. Although final rhinoplasty may still be required after thecompletion of nasal growth, we feel that secondary correction at thisage is warranted to as to optimize the child’s developing self-image.
The optimal technique for providing support of the cleft alarcartilage at the age of primary school remains controversial. Millard3
describes an alar lift to correct the unilateral cleft nasal deformityand recommends that this be done at the age of primary school andno earlier than age 5 years as the cartilage is felt to be too delicateto retain its position before this age. Whereas there has been anongoing debate as to whether rhinoplasty performed before age 16 to18 years causes long-term alteration in growth of the nose, Ortiz-Monasterio and Olmedo4 have demonstrated that correctiverhinoplasty performed before puberty does not interfere with thelong-term growth of the nose. However, other authors feel thatdefinitive nasal surgery should be delayed as flattening of the alarcartilage will continue throughout adolescence, and the underlyingmaxillary deficiency cannot be corrected until skeletal growth iscomplete.5,6 Therefore, many patients will require definitive cleftrhinoplasty after skeletal maturation is complete.6 Cartilage graftsplaced at primary school age may therefore become obsolete shouldcompletion rhinoplasty be required after completion of skeletalgrowth. In addition, harvest of septal cartilage at primary school agewould preclude the possibility of reharvest of this donor site as asource of nonscarred graft at a later age. To address this issue, we havedeveloped a technique in which resorbable plates are used to supportthe cleft alar cartilage during rhinoplasty performed at primary schoolage to minimize relapse. The aims of the current study were to (1)describe our technique for primary cleft rhinoplasty at primary schoolage using resorbable plates and (2) demonstrate a means by which thesymmetry and form of the proposed rhinoplasty technique can beevaluated.
METHODSA total of 16 patients, 10 boys and 6 girls with unilateral cleft
lip and nasal deformity, were included in this study. All patientsoperated on by the senior author who underwent secondary cleftrhinoplasty at primary school age and had placement of resorbable
ORIGINAL ARTICLE
The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 1801
From the Department of Plastic Surgery, Case Western Reserve UniversitySchool of Medicine, Cleveland, Ohio.Received February 6, 2009.Accepted for publication March 11, 2009.Address correspondence and reprint requests to Arun K. Gosain, MD,
Department of Plastic Surgery, CaseWesternReserveUniversity,UniversityHospitals of Cleveland, MS 5044, 11100 Euclid Ave, Cleveland,OH 44106; E-mail: [email protected]
This article did not require any sources of funding.The authors declare that they had no financial interests or commercial
associations during the course of this study.Copyright * 2009 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/SCS.0b013e3181b5d4c0

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
plates to support the affected alar cartilage were included in thestudy group. Mean age was 6 years, raging from 4 to 8 years.Patients were regularly monitored for a mean follow-up period of9.6 T 2.8 months (mean T SEM), with the range of 20 days to2 years postoperatively. A control group consisting of 16 childrenwith no cleft lip or nasal deformity aged 6 to 8 years was alsostudied to confirm that the measurement technique demonstratednasal symmetry in control subjects.
Surgical TechniqueAll patients in the study group had primary repair of the cleft
nasal deformity at the time of primary lip repair. The secondaryrhinoplasty is performed between 4 and 8 years of age to minimizepsychosocial pressure.
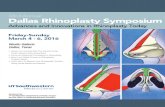
Using a transcolumellar stair-step incision, an open rhino-plasty technique is used to approach the alar cartilages (Fig. 1, topleft). Many patients have restriction of vestibular lining that con-tributes to alar stenosis and diminished airflow through the affectednostril. This is addressed with a Z-plasty, using the constricted alarweb as a guide for placing the central axis of the BZ[ (Fig. 1, topright). Bilateral infracartilaginous extensions provide access to thecaudal border of the lower lateral cartilage. Both alar cartilages aredissected free on the cutaneous surface. The alar cartilage on the af-fected side is completely freed from the overlying skin envelope andunderlying vestibular skin, providing complete mobilization of theaffected alar cartilage (Fig. 1, bottom left). Thereafter, the adja-cent fibrous soft tissue is completely removed, and the cartilage istrimmed using the unaffected side as the reference guide. A mal-leable metal template is then fashioned as a mirror image of theunaffected alar cartilage, and the resorbable plate is then fashionedto simulate the template; the resorbable plate is cut identical to thetemplate and allowed to passively assume the shape of the template
in the hot water bath. The plate is then placed beneath the affectedalar cartilage and sutured to the cartilage with 5-0 Prolene suture(Ethicon, Somerville, NJ) and actively positioned to support andrender it symmetric to the unaffected side (Fig. 1, bottom right).Symmetry of the alar dome in height and width is crucial in thepositioning of alar cartilage-resorbable plate complex. The plate issandwiched between vestibular mucosa and alar cartilage, therebypreventing collapse of the alar cartilage. As previously mentioned, incases in which there is stenosis of the vestibular lining, Z-plasty
FIGURE 1. Technique for secondary cleft rhinoplasty doneat primary school age using resorbable plates, performed ina 6-year-old boy after right unilateral cleft lip and nosecorrection done at infancy. See Surgical Technique for detailedexplanation.
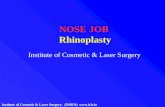
FIGURE 2. Secondary rhinoplasty is completed by trimmingredundant skin from the alar rim (left, blue line), followed bysupport with a silastic nasal splint used for at least 3 monthspostoperatively (right).
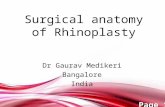
FIGURE 3. Six-year-old boy for whom surgical techniquehas been demonstrated is shown preoperatively (above)and 1 year postoperatively (below) after secondary cleftrhinoplasty and revision cheiloplasty.
Gosain and Fathi The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009
1802 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
release of the vestibular mucosa is critical to retaining the augmentedconfiguration of the alar cartilage. At conclusion of the procedure,the nasal skin is redraped to its normal anatomic position. The softtriangle is assessed, and any redundant skin on the affected side istrimmed to restore symmetry to the alar rim. The skin to be excisedis demonstrated by the blue dotted line in Figure 2, left. We use aPorex nasal stent (Porex Surgical, Newton, GA) sized to match theunaffected nostril to help retain shape of the lining and repositionedalar rim (Fig. 2, right). The stent is not sutured in place but is heldin place with tape across the external wings. The family is instructedas to how to remove the stent for cleaning, and it is recommendedthat the stent be worn continuously for the first 3 months, and its use
continued for up to 6 months should the patient tolerate it. Stent usein the latter 3 months can be decreased to nighttime only if thepatient prefers not to wear it during the day. Photographs of 2patients who have completed this regimen are shown (Figs. 3 and 4).
Photogrammetric MeasurementsAccuracy and reliability of the photogrammetry of the face
(indirect anthropometry) is well described by Farkas.7 It is an-thropometry adapted for quantification of surface features fromstandard photographs. We used the same principles in our study.
Life-size frontal, lateral, and basilar views were obtained forall patients in preoperative and postoperative visits. Basilar viewswere obtained by tilting the patient’s head back to bring the dome tothe level of eyebrows, above the canthi. These views were used toidentify the craniofacial landmarks.8,9 Photograph requisition con-ditions were meticulously evaluated in each visit, to maintain theconsistency.
The photogrammetric analysis performed for each patient isdemonstrated in Figure 5 (left). Two main axes were used as the basisof our measurements: (1) horizontal axis (H): line drawn as a tangentacross the nostril floor bilaterally and (2) vertical axis (V): linedrawn perpendicular to horizontal axis passing through the middleof the columellar base. The following angles and ratios weremeasured for each patient on preoperative and postoperative basilarview photographs, making measurements both on the affected andthe unaffected sides:(1) Alar rim angle (ar): the angle between the horizontal axis and a
line drawn tangent to the alar rim. The ideal angle is identicalbetween the affected and the unaffected sides.
(2) Columellar axis angle (ca): the angle between the horizontalaxis (H) and a line drawn through the columellar axis. Thecolumellar axis (ca) was defined as a line connecting thepronasale to the subnasale. The ideal angle is 90 degrees.
(3) Nostril width angle (nw): the angle between the horizontal axisand a line drawn through the widest point of each nostril. Theideal angle is 0 degrees.
(4) Nostril height difference (nd): the height difference (in milli-meters) between the apex of the affected and unaffectednostrils. The ideal difference in nostril height is 0 mm.
(5) Nostril shape: nostril height (L) and width (W) were measuredTon both sides and divided by the correction factor previouslydescribed. The ideal measure would be equivalence in nostrilshape between the affected and unaffected sides of the nose.
Photographs analyzed were taken preoperatively and at least6 months postoperatively. Measurements made 1 year postoperatively
FIGURE 4. A 7-year-old boy in whom photogrammetricmeasurements are demonstrated is shown preoperatively(above) and 1 year postoperatively (below) after secondarycleft rhinoplasty and revision cheiloplasty.
FIGURE 5. Photogrammetric measurements are illustrated in the boy shown in Figure 4 taken preoperatively (left) and1 year postoperatively (right). Measurements are described in Photogrammetric Measurements.
The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 Cleft Rhinoplasty at Primary School Age
* 2009 Mutaz B. Habal, MD 1803

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
on the illustrative patient demonstrate marked improvement in nasalsymmetry (Fig. 5, right).
Method ErrorsThe method errors were assessed for intraobserver variance,
photograph consistency, and reliability. To minimize intraobservervariance, alar rim angle on the affected side was measured twice,2 weeks apart by the same observer on all samples. The measure-ments were analyzed by correlation analysis. A correction factor wasused to eliminate magnification error and subtle variation betweenpreoperative and postoperative photographs. Statistical analysis ofpreoperative and postoperative tip height measurements indicated nosignificant changes. Therefore, the ratio of preoperative nasal tipheight to postoperative nasal tip height was used as the correctionfactor.
In addition to photometric measurements, a panel of 5 peopleevaluated the preoperative and postoperative photographs. This panelconsisted of a board-certified plastic surgeon, 2 plastic surgery re-search fellows, a plastic surgery resident, and a layperson. Thepanelists rated the postoperative photographs relative to achievedsymmetry on a scale of 1 to 10, 10 being the level of symmetry in anormal nose.
To further validate these measures, basilar views were ob-tained from 16 randomly selected control subjects aged 4 to 8 years.The control subjects had no lip and/or nose deformity and had notundergone nasal surgery. Similar measures were made on thesesubjects to evaluate whether the measures described couldadequately assess symmetry (Table 1).
Statistical AnalysisA 2-tailed paired t test was performed to compare preoper-
ative and postoperative measurements after normalization with thecorrection factor. P G 0.05 was considered statistically significant.
RESULTSThe Pearson correlation test illustrated a highly significant
intraobserver correlation for repeated measurements (r = 0.9779,P G 0001). Having validated the reliability of the data, preoperativeand postoperative measures were compared (Table 2). Durationfrom surgery to the postoperative photograph analyzed was 9.6 T2.8 months (mean T SEM), with a maximum duration to post-operative photograph of 38 months. Comparable measures in age-matched controls are provided in Table 1. No significant differenceswere noted between sides in the parameters measured in these age-matched controls (P 9 0.05).
Analysis of the data indicates that there was a statisticallysignificant improvement in nasal symmetry postoperatively. The mean
alar rim angle went from 46.1 degrees preoperatively to 56.3 degreespostoperatively (P G 0.001); the mean alar rim angle in age-matchedcontrols was 58.9 to 60.6 degrees, validating the ideal measure of60 degrees. The mean columellar axis angle went from 80.6 degreespreoperatively to 86.3 degrees postoperatively (P G 0.05); the meancolumellar axis angle in age-matched controls was 89 degrees,validating the ideal measure of 90 degrees. The mean nostril widthangle went from 7.1 degrees preoperatively to 3.3 degrees post-operatively (P G 0.001); the mean nostril width angle in age-matchedcontrols was 0.8 degrees, validating the ideal measure of 0 degrees,or parallel to the horizontal axis. Nostril shape measurement wentfrom a mean of 0.8 to 1.2 on the affected side (P G 0.05), ap-proximating the mean of the unaffected nostril of 1.1; the nostrilshape on the affected side showed no significant change postoper-atively, retaining the oval shape of the control nostrils (mean nostrilshape of 1.6Y1.7). The mean nostril height difference went from3.8 mm preoperatively to 1.4 mm postoperatively (P G 0.001); themean nostril height difference in age-matched controls was 0.8 mm,validating the ideal of no difference in nostril height between sides.
The panel’s comparative and clinical assessment of preoper-ative and postoperative photographs revealed that the surgery ren-dered more symmetric and appealing noses. Overall outcomes scorewent from 3.7 T 0.4 (mean T SEM) preoperatively to 6.4 T 0.2postoperatively.
DISCUSSIONThere are 3 primary goals of the secondary rhinoplasty
performed at primary school age: (1) to minimize or eliminate stig-mata of the cleft nasal deformity, (2) to maintain or restore patencyof the nasal airway when compromised by alar webbing or externalvalve collapse, and (3) to minimize interference with nasal growthand to avoid harvest of critical nasal tissues that will becomeobsolete with nasal growthVspecifically to maintain septal cartilagedonor sites for final rhinoplasty after skeletal maturity if needed. Aclear understanding of the pathologic anatomy of the deformity isessential to achieve satisfactory aesthetic and functional outcomes.Moreover, it must be distinguished from the primary nasal deformityof the unrepaired anomalies. Table 3 summarizes some commonfeatures of the unilateral cleft nasal deformity as described byBardach and Cutting.10,6
First successful utilization of biodegradable plates in oraland maxillofacial surgery field was reported in animal studies, andlater on, in humans, they were modified for fixation purposes inorthognathic surgeries.11,12
TABLE 2. Descriptive and Statistical Analysis ofAnthropometric Changes (Mean T SEM)
PreoperativeMeasurement
PostoperativeMeasurement P
Alar rim angle: affected side 46.1 T 2.9 56.3 T 2.4 G0.001Alar rim angle: unaffected side 46.5 T 2.7 56.3 T 2.3 G0.001Columellar axis angle 80.6 T 1.8 86.3 T 0.9 G0.05Nostril width angle 7.1 T 0.8 3.3 T 0.3 G0.001Nostril shape: affected side 0.8 T 0.1 1.2 T 0.2 G0.05Nostril shape: unaffected side 1.0 T 0.1 1.1 T 0.1 90.05Nostril height difference, mm 3.8 T 0.5 1.4 T 0.3 G0.001
See Photogrammetric Measurements for explanation of measurementsused for each calculation. Statistical analyses compare preoperative topostoperative measures.
TABLE 1. Descriptive and Statistical Analysis of NormalNoses (Mean T SEM)
Measurement (Mean T SEM)
Alar Rim angle (right) 58.9 T 0.8Alar Rim angle (left) 60.6 T 0.8Columellar Axis angle 89 T 0.4Nostril Width angle 0.8 T 0.3Nostril Shape (right) 1.7 T 0.1Nostril Shape (left) 1.6 T 0.1Nostril Height difference (mm) 0.8 T 0.2
See text (BPhotogrammetric Measurements[) for explanation of measure-ments used for each calculation. BSEM[ = Standard Error of the Mean.
Gosain and Fathi The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009
1804 * 2009 Mutaz B. Habal, MD

Copyright @ 2009 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Biodegradable plates have been made of lactic and glycolicacid polymers that degrade by diffusion-controlled hydration, theproducts of which are taken up by macrophages and finallyeliminated through the Krebs cycle. Recently, these polymers havebeen blended with trimethylene carbonate to increase their flexi-bility. Further bioengineering using highly orientated fibers in thelongitudinal axis of the polyester has allowed the development of abiocompatible, bioresorbable material suitable for use in cranio-maxillofacial surgery.13,14 We have extended the use of these platesfrom support of the craniomaxillofacial skeleton to support of thealar cartilages when secondary cleft rhinoplasty is done at the age ofprimary school (ages 6Y8 years). Wong et al15 first described the useof resorbable plates for support of the alar cartilages in primary cleftnasal repair performed during the first year of life. The present studyis the first to report on the outcome of resorbable plates forsecondary cleft nasoplasty. We feel this to be an excellent appli-cation of these biomaterials in soft tissue nasal surgery because itallows for cartilage support without harvesting native tissues thatmight be required for final cleft nasoplasty upon completion ofskeletal growth. In the current study, we have used 0.75 Inion plates(Stryker, Kalamazoo, MI), with resorption time of 2 to 3 years. Theplates were softened in a water bath, then contoured and cut to thedesired shape and size according to the unaffected alar cartilage.
In summary, the current study has used the following approachto correction of the cleft nasal surgery in the growing child:1. Primary cleft nasal surgery is done during the first year of life, at
time of the cleft lip repair.2. Secondary cleft nasal surgery is done at the time of early grade
school (6Y8 years old) should there be relapse after primarysurgery. This is an age in which children are exposed to a broadersocial network and optimizing aesthetic appearance is paramount,although some children may still require a final rhinoplasty afterskeletal growth is complete. When rhinoplasty is performed atthe age of primary school, we feel it is important to minimizethe harvest of septal cartilage so as not to impair further cartilage
growth and to leave unscarred cartilage for the final rhinoplasty.We use resorbable plates to support the alar cartilage, selectingplates with a resorption time of 2 to 3 years. We have found thistechnique to provide adequate support to restore a normal nostrilshape, as confirmed by photogrammetric measurements. In addi-tion, we use a silastic nasal stent (Porex Surgical) to providefurther support to the alar contour for 3 months postoperatively.We also avoid nasal osteotomies so as to avoid potential distur-bance in skeletal growth, reserving osteotomies for the final rhi-nolasty if indicated.
3. Final cleft nasal surgery, if needed, is performed after com-pletion of nasal growth (age 16 years). By following the pro-tocol outlined, virgin septal cartilage remains for final grafting,and one does not need to dissect out obsolete pieces of cartilagegraft that no longer fit the size of the adult nose. Nasal osteo-tomies, if required, are reserved until this age.
The present study introduces a novel application of resorbableplates to support the affected alar cartilage during secondary cleftrhinoplasty performed at the age of primary school. Furthermore, wepresent a protocol for objective assessment of postoperative out-comes of cleft nasal surgery using standardized photographs takenpreoperatively and postoperatively. Using this analytic technique, wehave demonstrated that the operated noses return to normal as com-pared with the unaffected side in the unilateral cleft nasal deformity,as well as relative to a normal cohort of age-matched controls.
REFERENCES1. Farkas LG, Hajnis K, Posnick JC. Anthropometric and anthroposcopic
findings of the nasal and facial region in cleft patients before and afterprimary lip and palate repair. Cleft Palate Craniofac J 1993;30:1Y12
2. Shih CW, Sykes JM. Correction of the cleft-lip nasal deformity.Facial Plast Surg 2002;18:253Y262
3. Millard RD. Earlier correction of the unilateral cleft lip nose. PlastReconstr Surg 1982;70:64Y73
4. Ortiz-Monasterio F, Olmedo A. Corrective rhinoplasty before puberty:a long-term follow-up. Plast Reconstr Surg 1981;68:381Y391
5. Broadbent TR, Woolf RM. Cleft lip nasal deformity. Ann Plast Surg1984;12:216Y234
6. Guyuron B. MOC-PS(SM) CME article: late cleft lip nasal deformity.Plast Reconstr Surg 2008;121(4 suppl):1Y11
7. Farkas LG. Anthropometry of the Head and Face. 2nd ed. New York,NY: Raven Press, 1994:79Y100
8. Liou EJ, Subramanian M, Chen PK. Progressive changes of columellalength and nasal growth after nasoalveolar molding in bilateral cleftpatients: a 3-year follow-up study. Plast Reconstr Surg 2007;119:642Y648
9. Liou EJ, Subramanian M, Chen PK, et al. The progressive changes ofnasal symmetry and growth after nasoalveolar molding: a three-yearfollow-up study. Plast Reconstr Surg 2004;114:858Y864
10. Bardach J, Cutting C. Anatomy of unilateral and bilateral cleft lip andnose. In: Bardach J, Morris HL, eds. Multidisciplinary Management ofCleft Lip and Palate. Philadelphia, PA: Saunders, 1990:154Y158
11. Laughlin RM, Block MS, Wilk R, et al. Resorbable plates for thefixation of mandibular fractures: a prospective study. J Oral MaxillofacSurg 2007;65:89Y96
12. Wood GD. Inion biodegradable plates: the first century. Br J OralMaxillofac Surg 2006;44:38Y41
13. Tormala P, PellinenM, Pohionen T. Totally biodegradable self-reinforcedrods and screws for internal fixation of bone fractures. Acta OrthopScand 1988;59(part 5)suppl 227:17
14. Cordewener FW, Bos RR, Rozema FR, et al. Poly(L-lactide) implants forrepair of human orbital floor defects: clinical and magnetic resonanceimaging evaluation of long-term results. J Oral Maxillofac Surg1996;54:9Y14
15. Wong GB, Burvin R, Mulliken JB. Resorbable internal splint: an adjunctto primary correction of unilateral cleft lip-nasal deformity. PlastReconstr Surg 2002;110:385Y391
TABLE 3. Features of Unilateral Cleft Nasal Deformity
1 The columella is shorter on the cleft side.2 The base of the columella is deviated to the noncleft side.3 The lateral crus of the lower lateral cartilage is longer on the
cleft side.4 The nasal tip is displaced in both the frontal and the horizontal
planes.5 The nasal tip is asymmetric.6 The ala is flattened, resulting in horizontal orientation of the
nostril.7 The nostrils are asymmetric.8 The entire nostril is retropositioned because of the deficiency
in the underlying frame.9 The base of the ala is displaced laterally and/or posteriorly and
sometimes inferiorly.10 The nasal floor is caudal on the cleft side.11 A nasolabial fistula could be present.12 The septum and anterior nasal spine are shifted toward the
noncleft vestibule.13 The nasal septum is deviated, resulting in a varying degree of
nasal obstruction.14 The inferior turbinate on the cleft side is hypertrophic.15 The maxilla is hypoplastic on the cleft side.16 The premaxilla and the maxillary segments are displaced.
The Journal of Craniofacial Surgery & Volume 20, Supplement 2, September 2009 Cleft Rhinoplasty at Primary School Age
* 2009 Mutaz B. Habal, MD 1805