Aspects of maxillofacial trauma care with emphasis on dissertation.pdf · Aspects of maxillofacial...
156
Transcript of Aspects of maxillofacial trauma care with emphasis on dissertation.pdf · Aspects of maxillofacial...


Aspects of maxillofacial trauma care with emphasis on
closed treatment of mandibular condyle fractures in an
era of open reduction and internal fixation.
B. van den Bergh
Bergh, Bart vd.indd 1 23-10-15 16:34

Financial support for publication of this thesis was provided by:
ACTA, Dam Medical B.V., Dentsply Implants B.V., KNMT, KLS Martin Nederland B.V., NVMKA, Ortholab B.V., Spaarne Gasthuis wetenschapsbureau
ISBN: 978-90-6464-941-7
Cover: Serge A. Steenen
Lay-out: Ferdinand van Nispen, Citroenvlinder-dtp.nl, my-thesis.nl, Bilthoven, The Netherlands
Printed by:GVO drukkers & vormgevers B.V. | Ponsen & Looijen, Ede, The Netherlands
Bergh, Bart vd.indd 2 23-10-15 16:34

VRIJE UNIVERSITEIT
Aspects of maxillofacial trauma care
with emphasis on closed treatment of
mandibular condyle fractures in an era of
open reduction and internal fixation.
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aande Vrije Universiteit Amsterdam,
op gezag van de rector magnificusprof.dr. V. Subramaniam,
in het openbaar te verdedigenten overstaan van de promotiecommissie
van de Faculteit der Tandheelkundeop donderdag 28 januari 2016 om 13.45 uur
in de aula van de universiteit,De Boelelaan 1105
door
Bart van den Bergh
geboren te Amsterdam
Bergh, Bart vd.indd 3 23-10-15 16:34

promotoren: prof.dr. T. Forouzanfarprof.dr. D.B. Tuinzing
copromotor: dr. J.J. de Mol van Otterloo
Bergh, Bart vd.indd 4 23-10-15 16:34

promotiecommissie: prof.dr. A.G. Becking prof.dr. R.R.M. Bos prof.dr. R. Koole prof.dr. F. Lobbezoo prof.dr. J.P.R. van Merkesteyn
paranimfen: Koen van den Bergh Hylke Schouten
Faculteit der Tandheelkunde
Bergh, Bart vd.indd 5 23-10-15 16:34

Bergh, Bart vd.indd 6 23-10-15 16:34

Contents
Chapter 1 General introduction 9
Chapter 2 Aetiology and incidence of maxillofacial trauma in Amsterdam: A retrospective analysis of 579 patients.
21
Chapter 3 Treatment and complications of mandibular fractures: A 9-year analysis.
35
Chapter 4 Long-term results and complications after bilateral mandibular condyle fractures.
49
Chapter 5 Closed treatment of mandibular condyle fractures: comparing intermaxillary fixation with screws or arch bar. A randomised clinical trial.
63
Chapter 6 IMF screws or arch bars for closed treatment of mandibular condyle fractures: the quality of life-aspects.
81
Chapter 7 Post-operative radiographs after maxillofacial trauma: sense or nonsense?
99
Chapter 8 General discussion 113
Chapter 9 Summary 121
Dutch summary 129List of publications 137Dankwoord / Acknowledgements 141Curriculum vitae 147
Bergh, Bart vd.indd 7 23-10-15 16:34

Bergh, Bart vd.indd 8 23-10-15 16:34
Chapter 1:
General introduction
Bergh, Bart vd.indd 9 23-10-15 16:34

Chapter 1
10
General introduction
Maxillofacial fractures commonly occur as a result of various types of trauma.1 The reported diversity of their incidence and aetiology is due to a range of environmental, cultural and socio-economic factors.2-5 In developed countries, the main causes appear to be traffic accidents, assaults, falls and sports injuries 4,6-8, whereas in economically less advanced countries maxillofacial injuries are most often the result of interpersonal violence.4,9
Mandibular Fractures in GeneralWhere mandibular fractures are concerned, maxillofacial surgeons may encounter difficulty restoring the pre-traumatic occlusion to optimise the masticatory function.10,11 Over the years numerous authors have described different treatment modalities for managing these fractures.In the past, fractures of the mandibular body, ramus or angle, were generally treated by closed reduction (CR) and the application of intermaxillary fixation (IMF) for a certain period of time. Nowadays, except for condylar fractures, the majority of mandibular fractures are repositioned and immobilized by open reduction and internal fixation (ORIF) using screws and plates.12-14 Whilst there is existing worldwide consensus regarding the management of mandibular fractures, diversity in treatment options may result in treatment-related complications in 9%-36% of cases.15-22 To date, there is little consensus on how to treat condylar fractures. As this type of fractures can be managed surgically by ‘closed treatment’ or by ORIF 20,22,23, special attention is given to this subject.
Condylar FracturesAlthough condylar fractures are the most common type of mandibular fracture 8,24,25, the ‘best treatment’ is still a point of discussion. These fractures occur mainly as a result of direct or indirect blunt forces transmitted through the body of the mandible to the condyle.26 The relatively weak condylar neck fractures easily, thereby reducing the risk of base of skull fracture, dislocation into the cranial cavity and damage to the brain.27 Fractured condyles can be treated with closed treatment (CT) by the application of IMF over a certain time period without anatomically reducing the condyle.10,20 After releasing the rigid IMF, ‘functional therapy’ using elastic bands is applied to restore the pre-traumatic occlusion.
Bergh, Bart vd.indd 10 23-10-15 16:34

General introduction
11
1ORIF following anatomic reduction can be considered as an alternative treatment modality.28,29 Many studies, including a Cochrane review, have investigated and compared these two treatment modalities without reaching a consensus, leaving this issue controversial.20,30,31,74,75 In overview, these studies conclude that ORIF provides superior clinical outcomes (e.g. less malocclusion, improved mandibular movements i.e. laterotrusion, protrusion mouth opening, less chin deviations) compared to CT. Unfortunately, these studies often neglected possible side-eff ects of ORIF, such as the development of facial nerve weakness, sialocele or salivary fi stulae, metalwork failure and (post-operative) infections. Another possible aspect in favour of CT may be the decreased costs in comparison with ORIF. CT requires shorter operative time, consequently shorter general anaesthesia and theatre time, and no expensive hardware.75
CT of condylar fractures is in many countries preferred over ORIF, including the Netherlands. However, the diff erent methods of achieving IMF may be subject to discussion. Throughout history, ‘tooth-borne’ appliances such as arch bars, eyelets and interdental wiring have been the primary choice. More recently, ‘bone-borne’ IMF screws (IMFS) were introduced, providing many benefi ts to patients and surgeons.32-34 These screws are relatively cheap, quick and easy to place and remove, and reduce operation time. The risk of needlestick injuries is low as no wire fi xation is used.35 Furthermore, this method is benefi cial to the patient as trauma to the interdental papillae and buccal mucosa is avoided and oral hygiene is easy to maintain post-operatively.32-39
Publications regarding the usefulness of IMFS report a number of complications such as fracture of the screw on insertion, iatrogenic damage to teeth, loss or loosening of screws and post-operative malocclusion.33,34,38,40-44
Quality of LifeOver the last few decades, particularly in the fi eld of healthcare, quality of life (QOL)-aspects have been given increasingly more attention. Patients are better informed about the diff erent treatment modalities and their potential social and physical impacts on their daily lives because of the internet, television and newspapers.While QOL has gained popularity in general healthcare, few publications can be found regarding QOL in relation to maxillofacial surgery. Most studies describe QOL in relation to chronic diseases (e.g. temporomandibular dysfunction) 45- 47,
Bergh, Bart vd.indd 11 23-10-15 16:34

Chapter 1
12
cancers 48,49 and dento-alveolar surgery.50,51 To date, little can be found in international literature on QOL and maxillofacial trauma. One publication reported that lowered health-related QOL increased the risk of patients with facial trauma developing depression, regardless of the cause of trauma.52 Another publication found increased depressive symptoms associated with QOL in patients with mandible fractures.53 Only three studies have investigated subjective discomfort for condylar fractures. 54-56 However, some consider that these studies examined the QOL aspects superficially and that the results were contradictory.57 With regard to QOL and closed treatment of condylar fractures, Zachariades reports that the treatment-related use of arch bars is inconvenient to the patient and that they might have a negative impact on QOL.26 To overcome arch bars-related inconvenience, IMFS were developed to facilitate the application of IMF during surgery.
Bilateral Condylar FracturesAccording to some authors, the treatment of bilateral condylar fractures is associated with more complications than in unilateral cases.26,28 Bilateral shortening of the mandibular ramus combined with suprahyoid muscle traction may cause a downward and posterior rotation of the mandible resulting in an open-bite malocclusion.10,24,58,59
One study reports the need for secondary orthognathic corrective surgery in 10% of cases with bilateral condylar fractures that received closed treatment.60 As this complication rate is considered unacceptably high, this treatment is regarded to be inappropriate. Some authors are convinced that bilateral fractures of the condyles should be treated with ORIF on at least one side.26,28 Another author describes satisfactory results with bilateral ORIF.10 Although often limited information is given on the exact outcome of the different treatment regimens, the majority of publications are focussed on functional impairment following treatment, without including the influence of these impairments on patients’ daily function.
Diagnostic Dilemma in Maxillofacial Trauma- Radiographic follow upIn many clinics, it is routine practice to obtain radiographs post-operatively after treatment of maxillofacial fractures.61,62 Several reasons are put forth for performing standard post-operative radiographic analysis, but little
Bergh, Bart vd.indd 12 23-10-15 16:34

General introduction
13
1evidence exists to support this protocol.61-64 Several authors and associations (e.g. The Royal College of Radiologists, UK) have suggested that unnecessary radiation exposure increases the risk of cancer, causing 100-250 deaths yearly worldwide.65
Some researchers have demonstrated a signifi cant relationship between the use of diagnostic dental radiography and thyroid cancer, parotid gland cancer and intracerebral tumours.66-69 Others question this relationship as it is very diffi cult to prove this radiation-associated cancer risk.70,71 Although the relationship between maxillofacial radiographic analysis and increased risk of cancer remains debatable, according to the ‘as low as reasonably achievable’ (ALARA) principle, unnecessary radiography should be avoided.Post-operative assessment of the position of the condyles by radiological investigation can be defended after closed treatment (i.e. IMF). If the fracture was treated with ORIF, post-operative radiological analysis is considered to be questionable as satisfactory fracture reduction can be determined intraoperatively.72 Some authors state that for post-operative evaluation of maxillofacial fractures, clinical judgement alone is adequate and taking standard radiographs is unnecessary.61,63,64,73
Aim of the Study Search is on for the best treatment for fractured mandibular condyles. Although nowadays more and more surgeons tend to prefer an ORIF procedure, these types of fractures are still widely treated with CT. Of these, the arch bar method is mostly used and described in the literature. A recently developed alternative, using IMFS for obtaining maximal occlusion, has been described in case reports and retrospective analyses. Although the use of IMFS is considered promising in these reports, no prospective clinical trials are available to date in which arch bars are compared to IMFS for treating fractured mandibular condyles.
Objectives:• The aetiology, incidence, treatment and complications of maxillofacial
trauma in general and mandibular trauma in particular will be retrospectively analysed.
• As bilateral fractures of the mandibular condyle are associated with major management problems, long-term results and complications will
Bergh, Bart vd.indd 13 23-10-15 16:34

Chapter 1
14
be investigated. Due to this evaluation, another aim has evolved: the influence of post-operative complications on masticatory function and quality of life.
• To assess the advantages, disadvantages and the results of IMFS, this method will be compared prospectively to the use of arch bars for IMF in mandibular condyle fractures.
• The impact of arch bars and IMFS on quality of life will be investigated.• The standard use of post-operative radiographic imaging to evaluate
surgery is widely accepted. The necessity for this will be questioned and investigated.
Bergh, Bart vd.indd 14 23-10-15 16:34

General introduction
15
1References
1. Erdmann D, Price K, Reed S, Follmar KE, Levin LS, Marcus JR. A fi nancial analysis of operative facial fracture management. Plast Reconstr Surg 2008;121(4):1323-7.
2. Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(2):166-70.
3. Bakardjiev A, Pechalova P. Maxillofacial fractures in Southern Bulgaria - a retrospective study of 1706 cases. J Craniomaxillofac Surg 2007;35(3):147-50.
4. Lee JH, Cho BK, Park WJ. A 4-year retrospective study of facial fractures on Jeju, Korea. J Craniomaxillofac Surg 2010;38(3):192-6.
5. van Beek GJ, Merkx CA. Changes in the pattern of fractures of the maxillofacial skeleton. Int J Oral Maxillofac Surg 1999;28(6):424-8.
6. Ellis E,3rd, Moos KF, el-Attar A. Ten years of mandibular fractures: an analysis of 2,137 cases. Oral Surg Oral Med Oral Pathol 1985;59(2):120-9.
7. Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J Craniomaxillofac Surg 2003;31(1):51-61.
8. Motamedi MH. An assessment of maxillofacial fractures: a 5-year study of 237 patients. J Oral Maxillofac Surg 2003;61(1):61-4.
9. Aksoy E, Unlu E, Sensoz O. A retrospective study on epidemiology and treatment of maxillofacial fractures. J Craniofac Surg 2002;13(6):772-5.
10. Chen CT, Feng CH, Tsay PK, Lai JP, Chen YR. Functional outcomes following surgical treatment of bilateral mandibular condylar fractures. Int J Oral Maxillofac Surg 2011;40(1):38-44.
11. Seemann R, Perisanidis C, Schicho K, Wutzl A, Poeschl WP, Kohnke R, et al. Complication rates of operatively treated mandibular fractures--the mandibular neck. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109(6):815-9.
12. Iatrou I, Samaras C, Theologie-Lygidakis N. Miniplate osteosynthesis for fractures of the edentulous mandible: a clinical study 1989-96. J Craniomaxillofac Surg 1998;26(6):400-4.
13. Iatrou I, Theologie-Lygidakis N, Tzerbos F. Surgical protocols and outcome for the treatment of maxillofacial fractures in children: 9 years’ experience. J Craniomaxillofac Surg 2010;38(7):511-6.
14. Sauerbier S, Schon R, Otten JE, Schmelzeisen R, Gutwald R. The development of plate osteosynthesis for the treatment of fractures of the mandibular body - a literature review. J Craniomaxillofac Surg 2008;36(5):251-9.
15. Bell RB, Wilson DM. Is the use of arch bars or interdental wire fi xation necessary for successful outcomes in the open reduction and internal fi xation of mandibular angle fractures?. J Oral Maxillofac Surg 2008;66(10):2116-22.
16. Bormann KH, Wild S, Gellrich NC, Kokemuller H, Stuhmer C, Schmelzeisen R, et al. Five-year retrospective study of mandibular fractures in Freiburg, Germany: incidence, etiology, treatment, and complications. J Oral Maxillofac Surg 2009;67(6):1251-5.
17. Ellis E,3rd. Treatment methods for fractures of the mandibular angle. Int J Oral Maxillofac Surg 1999;28(4):243-52.
18. Fox AJ, Kellman RM. Mandibular angle fractures: two-miniplate fi xation and complications. Arch Facial Plast Surg 2003;5(6):464-9.
19. Jing J, Han Y, Song Y, Wan Y. Surgical treatment on displaced and dislocated sagittal fractures of the mandibular condyle. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111(6):693-9.
20. Park JM, Jang YW, Kim SG, Park YW, Rotaru H, Baciut G, et al. Comparative study of the prognosis of an extracorporeal reduction and a closed treatment in mandibular condyle head and/or neck fractures. J Oral Maxillofac Surg 2010;68(12):2986-93.
21. Seemann R, Schicho K, Wutzl A, Koinig G, Poeschl WP, Krennmair G, et al. Complication rates in the operative treatment of mandibular angle fractures: a 10-year retrospective. J Oral Maxillofac Surg 2010;68(3):647-50.
Bergh, Bart vd.indd 15 23-10-15 16:34

Chapter 1
16
22. Seemann R, Lauer G, Poeschl PW, Schicho K, Pirklbauer M, Russmuller G, et al. CROOMA, complication rates of operatively treated mandibular fractures, paramedian and body. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111(4):449-54.
23. Mueller RV, Czerwinski M, Lee C, Kellman RM. Condylar fracture repair: use of the endoscope to advance traditional treatment philosophy. Facial Plast Surg Clin North Am 2006;14(1):1-9.
24. Marker P, Nielsen A, Bastian HL. Fractures of the mandibular condyle. Part 2: results of treatment of 348 patients. Br J Oral Maxillofac Surg 2000;38(5):422-6.
25. van den Bergh B, van Es C, Forouzanfar T. Analysis of mandibular fractures. J Craniofac Surg 2011;22(5):1631-4.
26. Zachariades N, Mezitis M, Mourouzis C, Papadakis D, Spanou A. Fractures of the mandibular condyle: a review of 466 cases. Literature review, reflections on treatment and proposals. J Craniomaxillofac Surg 2006;34(7):421-32.
27. MacLennan WD. Fractures of the mandibular condylar process. Br J Oral Surg 1969;7(1):31-9.28. Gupta M, Iyer N, Das D, Nagaraj J. Analysis of different treatment protocols for fractures of condylar
process of mandible. J Oral Maxillofac Surg 2012;70(1):83-91.29. Throckmorton GS, Ellis E,3rd. Recovery of mandibular motion after closed and open treatment of
unilateral mandibular condylar process fractures. Int J Oral Maxillofac Surg 2000;29(6):421-7.30. Palmieri C, Ellis E,3rd, Throckmorton G. Mandibular motion after closed and open treatment
of unilateral mandibular condylar process fractures. J Oral Maxillofac Surg 1999;57(7):764,75; discussion 775-6.
31. Sharif MO, Fedorowicz Z, Drews P, Nasser M, Dorri M, Newton T, et al. Interventions for the treatment of fractures of the mandibular condyle. Cochrane Database Syst Rev 2010;(4):CD006538. doi(4):CD006538.
32. Gordon KF, Reed JM, Anand VK. Results of intraoral cortical bone screw fixation technique for mandibular fractures. Otolaryngol Head Neck Surg 1995;113(3):248-52.
33. Coburn DG, Kennedy DW, Hodder SC. Complications with intermaxillary fixation screws in the management of fractured mandibles. Br J Oral Maxillofac Surg 2002;40(3):241-3.
34. Roccia F, Tavolaccini A, Dell’Acqua A, Fasolis M. An audit of mandibular fractures treated by intermaxillary fixation using intraoral cortical bone screws. J Craniomaxillofac Surg 2005;33(4):251-4.
35. Laurentjoye M, Majoufre-Lefebvre C, Siberchicot F, Ricard AS. Result of maxillomandibular fixation using intraoral cortical bone screws for condylar fractures of the mandible. J Oral Maxillofac Surg 2009;67(4):767-70.
36. Arthur G, Berardo N. A simplified technique of maxillomandibular fixation. J Oral Maxillofac Surg 1989;47(11):1234.
37. Ho KS, Tan WK, Loh HS. Case reports: the use of intermaxillary screws to achieve intermaxillary fixation in the treatment of mandibular fractures. Ann Acad Med Singapore 2000;29(4):534-7.
38. Onishi K, Maruyama Y. Simple intermaxillary fixation for maxillomandibular osteosynthesis. J Craniofac Surg 1996;7(2):170-2.
39. Schneider AM, David LR, DeFranzo AJ, Marks MW, Molnar JA, Argenta LC. Use of specialized bone screws for intermaxillary fixation. Ann Plast Surg 2000;44(2):154-7.
40. Coletti DP, Salama A, Caccamese JF,Jr. Application of intermaxillary fixation screws in maxillofacial trauma. J Oral Maxillofac Surg 2007;65(9):1746-50.
41. Gerlach KL, Schwarz A. Bite forces in patients after treatment of mandibular angle fractures with miniplate osteosynthesis according to Champy. Int J Oral Maxillofac Surg 2002;31(4):345-8.
42. Hashemi HM, Parhiz A. Complications using intermaxillary fixation screws. J Oral Maxillofac Surg 2011;69(5):1411-4.
43. Jones DC. The intermaxillary screw: a dedicated bicortical bone screw for temporary intermaxillary fixation. Br J Oral Maxillofac Surg 1999;37(2):115-6.
44. Tate GS, Ellis E,3rd, Throckmorton G. Bite forces in patients treated for mandibular angle fractures: implications for fixation recommendations. J Oral Maxillofac Surg 1994;52(7):734-6.
Bergh, Bart vd.indd 16 23-10-15 16:34

General introduction
17
145. Schuurhuis JM, Dijkstra PU, Stegenga B, de Bont LG, Spijkervet FK. Groningen temporomandibular
total joint prosthesis: an 8-year longitudinal follow-up on function and pain. J Craniomaxillofac Surg 2012;40(8):815-20.
46. Karacayli U, Mumcu G, Cimilli H, Sisman N, Sur H, Gunaydin Y. The eff ects of chronic pain on oral health related quality of life in patients with anterior disc displacement with reduction. Community Dent Health 2011;28(3):211-5.
47. Wang L, Su YX, Liao GQ. Quality of life in osteoradionecrosis patients after mandible primary reconstruction with free fi bula fl ap. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108(2):162-8.
48. Harding SA, Hodder SC, Courtney DJ, Bryson PJ. Impact of perioperative hyperbaric oxygen therapy on the quality of life of maxillofacial patients who undergo surgery in irradiated fi elds. Int J Oral Maxillofac Surg 2008;37(7):617-24.
49. Rogers SK, Gomez CF, Carpenter P, Farley J, Holson D, Markowitz M, et al. Quality of life for children with life-limiting and life-threatening illnesses: description and evaluation of a regional, collaborative model for pediatric palliative care. Am J Hosp Palliat Care 2011;28(3):161-70.
50. Savin J, Ogden GR. Third molar surgery--a preliminary report on aspects aff ecting quality of life in the early postoperative period. Br J Oral Maxillofac Surg 1997;35(4):246-53.
51. Bradshaw S, Faulk J, Blakey GH, Phillips C, Phero JA, White RP,Jr. Quality of life outcomes after third molar removal in subjects with minor symptoms of pericoronitis. J Oral Maxillofac Surg 2012;70(11):2494-500.
52. Ukpong DI, Ugboko VI, Ndukwe KC, Gbolahan OO. Health-related quality of life in Nigerian patients with facial trauma and controls: a preliminary survey. Br J Oral Maxillofac Surg 2008;46(4):297-300.
53. Gironda MW, Der-Martirosian C, Belin TR, Black EE, Atchison KA. Predictors of depressive symptoms following mandibular fracture repair. J Oral Maxillofac Surg 2009;67(2):328-34.
54. Santler G, Karcher H, Ruda C, Kole E. Fractures of the condylar process: surgical versus nonsurgical treatment. J Oral Maxillofac Surg 1999;57(4):392,7; discussion 397-8.
55. Eckelt U, Schneider M, Erasmus F, Gerlach KL, Kuhlisch E, Loukota R, et al. Open versus closed treatment of fractures of the mandibular condylar process-a prospective randomized multi-centre study. J Craniomaxillofac Surg 2006;34(5):306-14.
56. Schneider M, Erasmus F, Gerlach KL, Kuhlisch E, Loukota RA, Rasse M, et al. Open reduction and internal fi xation versus closed treatment and mandibulomaxillary fi xation of fractures of the mandibular condylar process: a randomized, prospective, multicenter study with special evaluation of fracture level. J Oral Maxillofac Surg 2008;66(12):2537-44.
57. Kommers SC, van den Bergh B, Forouzanfar T. Quality of life after open versus closed treatment for mandibular condyle fractures: a review of literature. J Craniomaxillofac Surg 2013;41(8):e221-5.
58. Bhagol A, Singh V, Kumar I, Verma A. Prospective evaluation of a new classifi cation system for the management of mandibular subcondylar fractures. J Oral Maxillofac Surg 2011;69(4):1159-65.
59. Becking AG, Zijderveld SA, Tuinzing DB. Management of posttraumatic malocclusion caused by condylar process fractures. J Oral Maxillofac Surg 1998;56(12):1370,4; discussion 1374-5.
60. Newman L. A clinical evaluation of the long-term outcome of patients treated for bilateral fracture of the mandibular condyles. Br J Oral Maxillofac Surg 1998;36(3):176-9.
61. Durham JA, Paterson AW, Pierse D, Adams JR, Clark M, Hierons R, et al. Postoperative radiographs after open reduction and internal fi xation of the mandible: are they useful?. Br J Oral Maxillofac Surg 2006;44(4):279-82.
62. Ogden GR, Cowpe JG, Adi M. Are post-operative radiographs necessary in the management of simple fractures of the zygomatic complex?. Br J Oral Maxillofac Surg 1988;26(4):292-6.
63. Bali N, Lopes V. An audit of the eff ectiveness of postoperative radiographs--do they make a diff erence?. Br J Oral Maxillofac Surg 2004;42(4):331-4.
64. Childress CS, Newlands SD. Utilization of panoramic radiographs to evaluate short-term complications of mandibular fracture repair. Laryngoscope 1999;109(8):1269-72.
65. National Radiologic Protection Board - United Kingdom, London. Patient Dose Reduction in Diagnostic Radiology.<br /> 1990.
Bergh, Bart vd.indd 17 23-10-15 16:34

Chapter 1
18
66. Horn-Ross PL, Ljung BM, Morrow M. Environmental factors and the risk of salivary gland cancer. Epidemiology 1997;8(4):414-9.
67. Memon A, Godward S, Williams D, Siddique I, Al-Saleh K. Dental x-rays and the risk of thyroid cancer: a case-control study. Acta Oncol 2010;49(4):447-53.
68. Neuberger JS, Brownson RC, Morantz RA, Chin TD. Association of brain cancer with dental X-rays and occupation in Missouri. Cancer Detect Prev 1991;15(1):31-4.
69. Preston-Martin S, White SC. Brain and salivary gland tumors related to prior dental radiography: implications for current practice. J Am Dent Assoc 1990;120(2):151-8.
70. Rodvall Y, Ahlbom A, Pershagen G, Nylander M, Spannare B. Dental radiography after age 25 years, amalgam fillings and tumours of the central nervous system. Oral Oncol 1998;34(4):265-9.
71. Ron E. Cancer risks from medical radiation. Health Phys 2003;85(1):47-59.72. Jain MK, Alexander M. The need of postoperative radiographs in maxillofacial fractures--a
prospective multicentric study. Br J Oral Maxillofac Surg 2009;47(7):525-9.73. Chandramohan J, McLoughlin PM. Fractures of the mandible and zygomatic complex:
postoperative radiographs are not necessary. Br J Oral Maxillofac Surg 2007;45(1):90.74. Chrcanovic BR. Surgical versus non-surgical treatment of mandibular condylar fractures: a meta-
analysis. Int J Oral Maxillofac Surg 2015;44:158-79. 75. Al-Moraissi EA, Ellis E 3rd. Surgical treatment of adult mandibular condylar fractures provides
better outcomes than closed treatment: a systematic review and meta-analysis. J Oral Maxillofac Surg 2015;73:1482-493.
Bergh, Bart vd.indd 18 23-10-15 16:34

Bergh, Bart vd.indd 19 23-10-15 16:34

Bergh, Bart vd.indd 20 23-10-15 16:34

Chapter 2:
“Aetiology and incidence of maxillofacial trauma in
Amsterdam: A retrospective analysis of 579 patients.”
This is an edited version of the manuscript: B. van den Bergh, K.H. Karagozoglu, M.W. Heymans, T. Forouzanfar.
Aetiology and incidence of maxillofacial trauma in Amsterdam: A retrospective analysis of 579 patients.
Journal of Cranio-Maxillo-Facial Surgery 2012 Sep;40(6):e165-9.
Bergh, Bart vd.indd 21 23-10-15 16:34

Chapter 2
22
Abstract
Introduction: The incidence of maxillofacial fractures varies widely between different countries. The large irregularity in reported incidence and aetiology is due to a variety of contributing factors, including environmental, cultural and socioeconomic factors. This retrospective report presents a study investigating the aetiology and incidence of patients with maxillofacial fractures in Amsterdam over a period of 10 years (2000-2010).
Results: The study population consisted of 408 males and 171 females with a mean age of 35.9 (SD: ± 16.3) years. The age group 20-29 years accounted for the largest subgroup in both sexes. The most common cause of the fractures was traffic related, followed by interpersonal violence. In patients with alcohol consumption the injury was mostly the result of interpersonal violence. Mandibular and zygomatic bone fractures accounted for approximately 80% of all fractures. Solitary mandibular fractures were observed in 246 patients. The main fracture pattern of the mandible was the combination of mandibular body with mandibular condyle (66 patients (66/246); 26.8%), followed by the combination of bilateral condylar fracture and fracture of the symphysis (43 patients (43/246); 17.5%). In fractures of the upper 2/3 of the face, zygomatic bone fractures were most common.
Conclusion: This report provides important data for the injury prevention planning, as compared with previous studies. Injuries related to interpersonal violence are on the rise, whereas fractures caused by traffic accidents are decreasing.
Bergh, Bart vd.indd 22 23-10-15 16:34

Maxillofacial trauma in Amsterdam
23
2
Introduction
Facial fractures are the result of various types of trauma to the face, and may occur in isolation or combined with other injuries.1 Diagnosis and treatment of facial fractures remain a challenging problem that frequently requires a multidisciplinary approach.1,2 The incidence of maxillofacial fractures varies widely between diff erent countries.3 The main causes worldwide are traffi c accidents, assaults, falls and sport injuries.4-7 Studies performed in countries like Singapore, New Zealand, Denmark, Japan and the Middle East region have shown that motor vehicle crashes are the most common cause of maxillofacial fractures in those countries, whereas in less economically advanced countries like parts of sub-Saharan Africa and South Africa maxillofacial injuries are more often the result of interpersonal violence in the form of fi ghts, assaults and gunshots.6,8 The large irregularity in reported incidence and aetiology is due to a variety of contributing factors, including environmental, cultural and socioeconomic factors.3,6,9,10 Some studies describe a decrease in road traffi c accidents, and an increase in interpersonal violence due to alcohol abuse and growing aggression in the society.10-12
To our knowledge there is a lack in reports detailing the causes and incidence of maxillofacial trauma in The Netherlands. This retrospective report presents a study investigating the aetiology and incidence of patients with maxillofacial fractures in Amsterdam over a period of 10 years.
Materials and Methods
The hospital and outpatient records of 579 patients treated for maxillofacial trauma from January 2000 to January 2010, were reviewed and analysed retrospectively. The hospital database was used to identify the patients. Patients with all types of maxillofacial fractures that were treated surgically with closed reduction or ORIF were included. Patients with solitary dento-alveolar and nose fractures were excluded, as these patients were primarily managed by dentists and the department of ENT of our hospital respectively. Data collected included gender, age, cause of injury, type of maxillofacial trauma, alcohol consumption, drug (ab)use, treatment modality and complications.
Bergh, Bart vd.indd 23 23-10-15 16:34

Chapter 2
24
The maxillofacial fractures were subdivided into zygomatic fractures (fracture of the zygomatic body or zygomatic arch), mandibular fractures (fracture of the mandibular condyle, mandibular angle or mandibular body), blow-out fractures, Le Fort I/II/III fractures, the frontal bone fractures, panfacial fractures and polytrauma (combination of fractures).
StatisticsData was processed using the Statistical Package for Social Sciences (SPSS) version 15.0. For parametric data Student t-test and for non-parametrics Chi square tests were performed.
Results
Fracture type and aetiological cause according to genderThe study population consisted of 408 males and 171 females with a mean age of 35.9 (SD: ± 16.3) years. The youngest patient was 2 years and the oldest 88 years. There was no significant difference in average age between male and female patients. As shown in table 1a and 1b there were mainly mandibular and zygomatic bone fractures in both males and females accounting for approximately 80% of all fracture sites. No differences concerning type of fractures between male and female patients were noted.
Table 1a . Facial fractures according to age for male patients.
Age
Man
dibl
e
Zygo
mat
ic b
one
Le F
ort
Panf
acia
l
Poly
-tra
uma
Blow
-out
Fron
tal S
inus
Zygo
mat
ic a
rch
Tota
l
(%)
0-9 2 2 1 5 (1.2)10-19 31 9 2 3 1 2 48 (11.8)20-29 57 38 2 2 11 6 7 123 (30.1)30-39 40 34 2 2 4 1 8 91 (22.3)40-49 24 32 3 2 13 3 1 4 82 (20.1)50+ 16 34 2 2 3 1 1 59 (14.5)Total(%)
170(41.6)
149(36.5)
11(2.7)
8(2.0)
34(8.3)
6(1.5)
11(2.7)
19(4.7)
408
Bergh, Bart vd.indd 24 23-10-15 16:34

Maxillofacial trauma in Amsterdam
25
2
Table 1b . Facial fractures according to age for female patients.Ag
e
Man
dibl
e
Zygo
mat
ic b
one
Le F
ort
Panf
acia
l
Poly
-tra
uma
Blow
-out
Fron
tal S
inus
Zygo
mat
ic a
rch
Tota
l
(%)
0-9 3 1 4 (2.3)10-19 12 4 1 2 19 (11.1)20-29 26 13 2 1 1 2 45 (26.3)30-39 14 10 1 2 3 3 1 34 (19.9)40-49 9 17 1 27 (15.8)50+ 12 20 2 1 3 3 1 42 (24.6)Total(%)
76(44.4)
65(38.0)
4(2.3)
6(3.5)
9(5.3)
6(3.5)
2(1.2)
3(1.8)
171
In both groups traffi c accidents were the main cause of injury (table 2a and 2b), followed by interpersonal violence for the male cohort (27.7%) and falls for females (19.9%). Signifi cantly more males than females were treated for fractures caused by interpersonal violence and sports (p < 0.01). Dividing the traffi c accidents by mode of transport, bicycle and automobile accidents resulted in signifi cantly more injuries in female patients when compared to males (p < 0.01).
Table 2a. Cause of injury according to age for male patients.
Age
Fall
Inte
rper
sona
l vio
lenc
e
Pede
stria
n hi
t
Bicy
cle
acci
dent
Mot
orcy
cle
acci
dent
Auto
mob
ile A
ccid
ent
Spor
ts
Suic
ide
atte
mpt
Oth
ers
Miss
ing
fi le
Tota
l
(%)
0-9 1 1 1 1 4 (1.0)10-19 8 13 2 6 11 2 1 5 48 (11.8)20-29 15 39 13 14 8 17 1 3 13 123 (30.1)30-39 13 28 11 10 8 15 1 2 4 92 (22.5)40-49 10 23 12 5 3 7 1 9 11 81 (19.9)50+ 18 9 1 14 5 2 3 3 5 60 (14.7)Total(%)
64(15.7)
113(27.7)
4(1.0)
57(14.0)
45(11.0)
23(5.6)
43(10.5)
3(0.7)
17(4.2)
39(9.6)
408
Bergh, Bart vd.indd 25 23-10-15 16:34

Chapter 2
26
Table 2b. Cause of injury according to age for female patients.Ag
e
Fall
Inte
rper
sona
l vio
lenc
e
Pede
stria
n hi
t
Bicy
cle
acci
dent
Mot
orcy
cle
acci
dent
Auto
mob
ile a
ccid
ent
Spor
ts
Suic
ide
atte
mpt
Oth
ers
Miss
ing
file
Tota
l
(%)
0-9 4 1 5 (2.9)10-19 3 5 2 3 2 1 2 1 19 (11.1)20-29 3 7 18 3 3 1 1 9 45 (26.3)30-39 3 4 1 10 2 8 1 1 3 33 (19.3)40-49 6 2 9 3 3 1 2 1 27 (15.8)50+ 16 3 2 13 1 2 5 42 (24.6)Total(%)
35(20.5)
16(9.4)
3(1.8)
55(32.2)
11(6.4)
19(11.1)
5(2.9)
2(1.2)
5(2.9)
20(11.7)
171
Fracture and injury according to age classificationThe age group 20-29 years accounted for the largest subgroup in both sexes (30.1% of the males, 26.3% of the females). In the male patients between 20-49 years interpersonal violence and traffic accidents were equally divided and formed the main cause of the fractures, whereas in the female population traffic accidents were recorded significantly higher compared with the other causes in patients between 20-49 years (p < 0.05). In patients aged 50 years and older the injuries were mostly a result of traffic accidents and falls (table 2a and 2b).
Mandibular fracturesIn table 3 the mandibular fractures are listed according to the cause of injury. A total of 246 patients with solitary mandibular fractures were identified. The main fracture pattern was the combination of mandibular body with mandibular condyle (66 patients; 26.8%), followed by the combination of bilateral condylar fracture and fracture of the symphysis (43 patients; 17.5%). A list of causes is given for the group of angle fractures (20 patients; 8.1%), body fractures (36 patients; 14.6%) and a combination of angle and body fracture (32 patients; 13.0%) A group of 49 patients remained, containing types of fractures that occur less frequently (e.g. combined bilateral angle with a bilateral body fracture or a combination of a bilateral body and unilateral condyle fracture).
Bergh, Bart vd.indd 26 23-10-15 16:34

Maxillofacial trauma in Amsterdam
27
2
Table 3. Mandibular fractures according to cause of injury.Fr
actu
re si
te
Fall
Inte
rper
sona
l vio
lenc
e
Pede
stria
n hi
t
Bicy
cle
acci
dent
Mot
orcy
cle
acci
dent
Auto
mob
ile a
ccid
ent
Spor
t
Suic
ide
atte
mpt
Oth
ers
Miss
ing
Tota
l
(%)
B1 + C2 10 17 1 14 5 5 5 2 7 66 (26.8)B + C + C 12 2 20 4 5 43 (17.5)B 7 3 6 2 4 9 5 36 (14.6)A3 + B 3 18 1 2 4 1 3 32 (13.0)A 3 11 1 1 1 1 1 1 20 (8.1)
Other combinations 13 16 6 4 3 2 1 4 49 (19.9)
Total(%)
48(19.5)
67(27.2)
2(0.8)
49(19.9)
20(8.1)
14(5.7)
17(6.9)
1(0.4)
3(1.2)
25(10.2)
246
1 B: Body; 2 C: Condyle; 3 A: Angle;
The fractures were mainly caused by traffi c accidents (34.5%), with bicycle accidents being most common followed by interpersonal violence with 27.2 %. Interpersonal violence related trauma proved to be a signifi cant cause of injury in patients with isolated angle fractures and angle fractures combined with mandibular body fractures (p < 0.01). In patients with a combination of bilateral condylar fracture and fracture of the symphysis bicycle accidents were the most common cause (p < 0.01).
Fractures of the 2/3 upper face.In this study there were 333 patients with fractures of the 2/3 upper face. In table 4 these fractures are listed according to the cause of injury. Zygoma fractures were most common (64.3%), followed by panfacial fractures and midface fractures (Le Fort I/II/III and combined midfacial fractures). For all fractures of the upper 2/3 of the face, except isolated zygomatic arch fractures and panfacial trauma, traffi c accidents were the main cause of injury, followed by interpersonal violence. Isolated zygomatic arch fractures were mostly the result of interpersonal violence and sports related trauma. Panfacial trauma was most often the result of traffi c accidents, followed by falls.
Bergh, Bart vd.indd 27 23-10-15 16:34

Chapter 2
28
Table 4. Fractures of the upper 2/3 of the face according to cause of injury.Fr
actu
re si
te
Fall
Inte
rper
sona
l vi
olen
ce
Pede
stria
nhi
t
Bicy
cle
acci
dent
Mot
orcy
cle
acci
dent
Auto
mob
ileac
cide
nt
Spor
t
Suic
ide
atte
mpt
Oth
ers
Miss
ing
Tota
l
(%)
Zygomatic bone 36 38 3 47 25 17 23 9 16 214 (64.3)
Panfacial 8 3 2 9 5 2 1 3 2 2 37 (11.1)Midface 3 10 5 3 6 1 1 6 35 (9.9)Zygomatic arch 7 2 1 6 2 4 22 (6.6)
Frontal Sinus 2 2 2 1 1 2 3 13 (3.9)
Blow-out 2 2 2 3 3 12 (3.6)Total(%)
51(15.3)
62(18.6)
5(1.5)
63(18.9)
36(10.8)
28(8.4)
31(9.3)
4(1.2)
19(5.7)
34(10.2)
333
Alcohol consumptionConcerning alcohol consumption the data of 135 patients was missing. Of the remaining 444 patients 79 reported to have consumed alcohol prior to the injury (table 5).
Table 5. Cause of injury related to alcohol consumption.
Alcohol consumptionInjury cause Yes No TotalFall 12 65 77Interpersonal violence 33 83 116Pedestrian hit 1 4 5Bicycle accident 22 76 98Motorcycle accident 8 40 48Automobile accident 3 29 32Sports - 46 46Suicide - 4 4Other - 18 18Total(%)
79(17.8)
365(82.2)
444
Missing data: 135
Pearson Chi-square demonstrated signifi cant diff erences (p < 0.01) between women and men. The values of Phi, Cramer’s V and the Contingency coeffi cient were under 0.3, therefore the relationship is not coincidental, but it is also not very strong.
Bergh, Bart vd.indd 28 23-10-15 16:34

Maxillofacial trauma in Amsterdam
29
2
Facial injury was mostly the result of interpersonal violence as shown in fi gure 1. Compared to other causes this diff erence proved to be signifi cant (p < 0.05). There was no signifi cant diff erence in the cause of injury in patients who consumed alcohol or in those that did not.
Figure 1. Patients with alcohol consumption listed according to cause of injury.
Fall 15,2%Violence 41,8%Pedestrian hit 1,3%Bicycle accident 27,8%Motorcycle accident10,1%Car accident 3,8%
Fall
Violence
Pedestrian hit
Bicycle accident
Motorcycle accident
Car accident
Discussion
Maxillofacial fractures are one of the most common injuries and can be challenging to diagnose and treat.1,2,6,7 The cause of facial injuries depends on a variety of contributing factors, including environmental, cultural and socioeconomic factors.3,4,10,13 Several studies have reported that facial bone injuries are mostly the result of traffi c accidents and interpersonal violence.3,4,9-11,13-15
This study describes the epidemiology of 579 patients with facial injury. The male female ratio was 2.4:1. Mandibular and zygomatic bone fractures were the most common fractures, accounting for 80% of all fracture sites. The highest rate of incidence of fractures was caused by traffi c accidents, with bicycle accidents being the most common aetiology, followed by interpersonal violence especially in males. When comparing males to females, interpersonal violence related fractures proved to be signifi cantly higher in males. Like previous studies the age group of 20-29 years counted for the largest subgroup in both sexes.3,9,16 In all age groups traffi c accidents resulted in most fractures. These fi ndings are comparable to several other studies.3,9,13,16 Up to the age of 50, interpersonal violence was the second most common cause,
Bergh, Bart vd.indd 29 23-10-15 16:34

Chapter 2
30
whereas in patients above 50 years of age traffic accidents were followed by fall related fractures.In mandibular fractures the combination of mandibular body with mandibular condyle was the most common fracture pattern. Lee et al. demonstrated that interpersonal violence results mostly in mandibular fracture, especially fracture of the angle.12 In this study interpersonal violence related fractures consisted mainly of isolated angle fractures and angle fracture combined with mandibular condyle or body fracture. In patients with upper 2/3 face fractures, zygomatic bone fractures were most common, mainly caused by traffic accidents. Isolated zygomatic arch fractures were the result of interpersonal violence and sports. In patients with alcohol consumption facial injury was mostly the result of interpersonal violence. The results of the Iida study demonstrated that in elderly women the facial injuries are mostly caused by falls, which is in line with the present study.13
The decrease of road traffic accidents as a cause of facial fractures in the EU is the result of preventive measures, such as the obligatory wearing of crash helmets, the seat belt and the more aggressive enforcement of the law regarding driving under the influence of alcohol.10 Van Beek et al. showed in their longitudinal study that during a time period of 20 years traffic accident related facial fractures decreased whereas interpersonal violence related fractures increased. Comparing our study with the study of van Beek et al., the trend of decreasing traffic accident related facial injury and increased fractures caused by interpersonal violence can be noted. On the other hand, opposed to the Nijmegen-region investigated by Van Beek et al., the Amsterdam-region contains an extensive tramway network system. This aspect, in combination with the finding that cyclists are a substantial part of the transport-system in the Amsterdam-region, may be a good explanation for the high incidence of bicycle-related accidents as a cause of maxillofacial trauma in general and zygomatic bone fractures and uni-/bilateral condylar fractures in particular. The present study has several shortcomings. In Amsterdam there are 4 hospitals of which two are university hospitals. All hospitals treat patients with facial injury, however some hospitals have a higher workload. Most patients are treated in the two university hospitals. Therefore it is questionable if the results of our study can be extrapolated to the whole population of Amsterdam. Furthermore, like other retrospective studies this retrospective analysis may be subject to information bias. However, the results presented are in line with
Bergh, Bart vd.indd 30 23-10-15 16:34

Maxillofacial trauma in Amsterdam
31
2
other studies and the analysis of this report provides important data for the design of plans for injury prevention and concurs with previous studies that interpersonal violence related injuries are increasing whereas fractures caused by traffi c accidents are decreasing.
Conclusion
The results of this retrospective study provide important data for the design of future plans for injury prevention. Mandibular and zygomatic bone fractures remain the most frequent fractures. The trend of increasing interpersonal violence related injuries and decreasing traffi c related injuries continues. In Amsterdam bicycle accidents are a major cause of maxillofacial trauma.
Bergh, Bart vd.indd 31 23-10-15 16:34

Chapter 2
32
References
1. Erdmann D, Price K, Reed S, Follmar KE, Levin LS, Marcus JR. A financial analysis of operative facial fracture management. Plast Reconstr Surg 2008;121(4):1323-7.
2. Katzen JT, Jarrahy R, Eby JB, Mathiasen RA, Margulies DR, Shahinian HK. Craniofacial and skull base trauma. J Trauma 2003;54(5):1026-34.
3. Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(2):166-70.
4. Ellis E,3rd, Moos KF, el-Attar A. Ten years of mandibular fractures: an analysis of 2,137 cases. Oral Surg Oral Med Oral Pathol 1985;59(2):120-9.
5. Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J Craniomaxillofac Surg 2003;31(1):51-61.
6. Lee JH, Cho BK, Park WJ. A 4-year retrospective study of facial fractures on Jeju, Korea. J Craniomaxillofac Surg 2010;38(3):192-6.
7. Motamedi MH. An assessment of maxillofacial fractures: a 5-year study of 237 patients. J Oral Maxillofac Surg 2003;61(1):61-4.
8. Aksoy E, Unlu E, Sensoz O. A retrospective study on epidemiology and treatment of maxillofacial fractures. J Craniofac Surg 2002;13(6):772-5.
9. Bakardjiev A, Pechalova P. Maxillofacial fractures in Southern Bulgaria - a retrospective study of 1706 cases. J Craniomaxillofac Surg 2007;35(3):147-50.
10. van Beek GJ, Merkx CA. Changes in the pattern of fractures of the maxillofacial skeleton. Int J Oral Maxillofac Surg 1999;28(6):424-8.
11. de Matos FP, Arnez MF, Sverzut CE, Trivellato AE. A retrospective study of mandibular fracture in a 40-month period. Int J Oral Maxillofac Surg 2010;39(1):10-5.
12. Lee KH. Interpersonal violence and facial fractures. J Oral Maxillofac Surg 2009;67(9):1878-83.13. Iida S, Kogo M, Sugiura T, Mima T, Matsuya T. Retrospective analysis of 1502 patients with facial
fractures. Int J Oral Maxillofac Surg 2001;30(4):286-90.14. Dimitroulis G, Eyre J. A 7-year review of maxillofacial trauma in a central London hospital. Br Dent J
1991;170(8):300-2.15. Scherer M, Sullivan WG, Smith DJ,Jr, Phillips LG, Robson MC. An analysis of 1,423 facial fractures in
788 patients at an urban trauma center. J Trauma 1989;29(3):388-90.16. Adebayo ET, Ajike OS, Adekeye EO. Analysis of the pattern of maxillofacial fractures in Kaduna,
Nigeria. Br J Oral Maxillofac Surg 2003;41(6):396-400.
Bergh, Bart vd.indd 32 23-10-15 16:34

Bergh, Bart vd.indd 33 23-10-15 16:34

Bergh, Bart vd.indd 34 23-10-15 16:34

Chapter 3:
“Treatment and complications of mandibular fractures:
A 9-year analysis.”
This is an edited version of the manuscript: B. van den Bergh, M.W. Heymans, F. Duvekot, T. Forouzanfar. Treatment and complications of mandibular fractures: A 10-year analysis.
Journal of Cranio-Maxillo-Facial Surgery 2012 Jun;40(4):e108-11.
Bergh, Bart vd.indd 35 23-10-15 16:34

Chapter 3
36
Abstract
Introduction The surgical treatment and associated complications of patients with mandibular fractures in Amsterdam over a period of 9 years are analysed.
ResultsBetween January 2000 and January 2009 225 patients were surgically treated for a mandibular fracture (mean age of 32.6 (SD: ± 14.6) years). A total of 431 fracture sites were identified. Of 213 dentate patients 29 patients were treated primarily with intermaxillary fixation (IMF). IMF combined with osteosynthesis was performed in 99 patients. 79 patients received IMF only perioperatively to aid open reduction and internal fixation (ORIF). Of 12 edentulous patients, 3 patients were treated with Gunning splints. Nine patients were treated by manual reduction and internal fixation. A total of 1965 screws and 442 plates were used. Sixty (26.7%) patients presented with complications, including (transient) hyposensibility of the lip and chin (34 patients), malocclusion (15 patients), infected osteosynthesis material (6 patients) and temporomandibular dysfunction (5 patients). Four patients needed surgical retreatment for correction of a malocclusion.
Conclusion The results of this report are partly in line with other studies and provide important data for improving the management of the fractured mandible.
Bergh, Bart vd.indd 36 23-10-15 16:34

Mandibular fractures
37
3
Introduction
Mandibular fractures have caused signifi cant management challenges for maxillofacial surgeons for many years.1 Restoring a pretraumatic occlusion is the common aim for optimisation of masticatory function.2 Reduction of compression of sensory nerves can be accomplished. The fracture site, pattern and displacement associated with other factors such as post-injury malocclusion determines the surgical treatment and the decision for either closed reduction or open reduction with internal fi xation (ORIF).3-5
Diff erent treatment modalities for managing a mandibular fracture have been described by several authors. Although in the past fractures of the mandibular body, ramus or angle were treated through closed reduction and intermaxillary fi xation (IMF), currently the “gold standard” is to anatomically reduce and stabilize these fractures by open reduction and fi xation with osteosynthesis material.6-8 A fracture of the condyle can be treated with closed treatment with IMF1,4 or surgically by an open reduction through either a submandibular, preauricular, retroauricular, transparotid approach4,9 or transoral approach with or without endoscopic assistance.4,10 The diversity of treatment options results in a variety of treatment-related complications.9 The overall complication rate for all mandibular fractures is reported to be 9-36%.4,5,11-15 Post-operative complications are related to the type of fracture, angulation or displacement, presence of teeth in the fracture line, uni-/bilaterality, other additional fractures of the mandible/maxilla and the chosen surgical treatment.16 Common complications described are mandibular deviation/asymmetry, temporomandibular joint pain, malocclusion, (transient) facial nerve paresis, (transient) loss of sensibility, wound infection, osteosynthesis failure and pseudarthrosis.1,4,9,17-19 The need for a secondary operative intervention is rare but sometimes necessary, mainly to remove infected hardware or to correct a malocclusion.This study was performed to analyse the diagnosis, treatment and associated complications of mandibular fractures surgically treated in a Dutch population.
Bergh, Bart vd.indd 37 23-10-15 16:34

Chapter 3
38
Materials and methods
The hospital and outpatient records of 225 patients surgically treated for a mandibular bone fracture from January 2000 to January 2009, were reviewed and analysed retrospectively. The patients were identified using the hospital database. Patients with all types of mandibular fractures that were treated surgically with closed reduction or ORIF were included. Patients with isolated dento-alveolar fractures were excluded as these patients were primarily managed by dentists. Patients with panfacial trauma (mandibular trauma in combination with a Le Fort I/II/III fracture) were also excluded for the clarity of the data. Data collected included gender, age, cause of injury, pre- and post-operative radiographic analysis, type of mandibular trauma, treatment modality and complications.At presentation of the patient at our department or emergency ward the mandibular fracture was diagnosed by either dental panoramic tomographs and submentovertex radiographs or by a (conebeam) CT-scan.The mandibular fractures were subdivided into body- (including symphysis and parasymphysis), angle, condyle, and ramus fractures. Patients were treated according to our departments’ protocol as demonstrated in table 1a and 1b.
Table 1a: treatment protocol in dentate patients.
Location Treatment modality
Fixation Follow up Post-operative radiographic analysis
Condyle IMF1
ORIF
-
2 X 1.5 mm plates
Weekly during 6 weeks
Weekly during 6 weeks
Submentovertex + dental panoramic tomography or CBCT
Submentovertex + dental panoramic tomograph or CBCT
Body ORIF 2 X 2.0 mm plates
Weekly during 6 weeks
dental panoramic tomograph or CBCT
Angle / Ramus
IMF
ORIF
-
2 X 2.0 mm plates
Weekly during 6 weeks
Weekly during 6 weeks
dental panoramic tomograph or CBCT
dental panoramic tomograph or CBCT
Multiple fractures
IMF + ORIF Weekly during 6 weeks
Submentovertex + dental panoramic tomograph or CBCT
1 IMF is performed by arch bars with ligatures and guided elastics
Bergh, Bart vd.indd 38 23-10-15 16:34

Mandibular fractures
39
3
Table 1b: treatment protocol in edentulous patients.
Location Treatment modality
Fixation Follow up Post-operative radiographic analysis
Condyle (uni-/ bilateral)
IMF1 - Weekly during 6 weeks
Submentovertex + dental panoramic tomograph or CBCT
Body ORIF 2.7 mm and / or 2.0 mm plates
Weekly during 6 weeks
dental panoramic tomograph or CBCT
Angle / Ramus
ORIF 2.7 mm and / or 2.0 mm plates
Weekly during 6 weeks
dental panoramic tomograph or CBCT
Multiple fractures
IMF + ORIF Weekly during 6 weeks
Submentovertex + dental panoramic tomograph or CBCT
1 IMF is performed using patient’s dentures fi xed with perizygomatical and perimandibular wiring.
Post-operatively all patients received standard analgesics (diclofenac 50 mg three times daily with paracetamol 1000 mg four times daily or codeine 20 mg four times daily with paracetamol 1000 mg four times daily). Patients treated with osteosynthesis received prophylactic antibiotics for one week (either clindamycin 600mg three times daily or amoxicillin-clavulate 625mg three times daily). Patients were seen weekly during six weeks by a oral & maxillofacial surgeon, on review the patients were also seen by an oral hygienist.The osteosynthesis material was only removed in cases of persisting infection that did not respond to oral antibiotics (after 2-3 months after surgery). To prevent any possible growth restriction of the mandible in patients younger than 18 years of age the osteosynthesis material was removed 6-12 months after surgery.
StatisticsData were processed using the Statistical Package for Social Sciences (SPSS) version 15.0. For parametric data Student t-test and for non-parametric data Chi square tests were performed.
Bergh, Bart vd.indd 39 23-10-15 16:34

Chapter 3
40
Results
The study population consisted of 151 males and 74 females with a mean age of 32.6 (SD: ± 14.6) years (range 2-88 years). An overview of the mandibular fractures is given in table 2.
Table 2. Overview of the mandibular fractures.
Type of fracture No. %
Unilateral condyle 16 7.1
Unilateral body / angle / ramus fracture 56 24.9
Unilateral condyle fracture + body / ramus / angle fracture 67 29.8
Bilateral condyle fracture 2 0.8
Bilateral condyle fracture + ramus / angle / body fracture 42 18.7
Bilateral body / angle / ramus fracture 42 18.7
Total (%) 225 100%
Table 3 demonstrates the type of mandibular fracture according to cause. A total of 431 fracture lines were identified. There were mainly mandibular body and condyle fractures, counting for approximately 86% of all fracture sides. Traffic accidents (42.0%) were the main cause of the fractures followed by interpersonal violence (24.1%) and falls (19.2%).
Table 3. Mandibular fractures according to cause of injury.
Frac
ture
site
Fall
Inte
rper
sona
l vi
olen
ce
Traffi
cac
cide
nt
Spor
t
Oth
ers
Miss
ing
Tota
l
(%)
Body 39 51 81 14 3 12 200 (46.4)Condyle 34 24 87 6 3 17 171 (39.6)Angle 9 29 13 1 1 5 58 (13.5)Ramus 1 1 2 (0.5)Total(%)
83(19.2)
104(24.1)
181(42.0)
21(5.0)
8(1.9)
34(7.8)
431
Radiographic analysis Type of pre- and post-operative analyses was divided into dental panoramic tomography, submentovertex radiograph, (cone-beam) CT-scan and other
Bergh, Bart vd.indd 40 23-10-15 16:34

Mandibular fractures
41
3
(e.g. occipitomental radiograph, cephalometric radiograph, posteroanterior radiograph). In total 471 preoperative radiographical analyses were performed (table 4). Post-operatively 330 radiographs were taken. For some patients a CT-scan of the skull was performed, mainly for neurological reasons.
Table 4. Radiographical analyses done pre- and post-operatively.
pre-operatively post-operativelydental panoramic tomograph 169 165submentovertex radiograph 158 132(cone-beam)CT-scanOther
6777
627
Total 471 330
Treatment modalities and operation duration213 patients were dentate, 12 patients edentulous. A total of 1965 screws (5 – 12 mm) and 442 plates (1.5 – 2.7 mm) were used. Nine patients were treated with reconstruction plates (2.7 mm). In two patients 1.5 mm plates were used for fi xation of a fractured condyle extraorally.Of the 213 dentate patients 29 patients were treated primarily with IMF. IMF combined with osteosynthesis was performed in 97 patients (2.0 mm plates). In 2 patients 2.7 mm reconstruction plates were used. In 79 patients IMF was performed only peroperatively to aid open reduction and internal fi xation. In 6 patients ORIF (2.0 and 2.7 mm) was performed manually without using IMF. 5 patients were treated with 2.7 mm plates for a comminuted body or angle fracture. These plates were applied transorally.Twelve edentulous patients were treated for a fractured mandible (table 5), mainly caused by a fall (7 patients). In 3 edentulous patients Gunning splints were used as IMF, in 9 patients the fractures were manually reduced. 6 patients were treated with 2.0 mm, 4 patients with 2.7 mm plates.
Table 5. Type of fractures in edentulous patients.
No.Unilateral body fractureUnilateral angle fractureUnilateral condyle fracture + body fractureBilateral body fracture
1117
Bilateral condyle fracture + body fracture 1Bilateral condyle fracture + bilateral body fracture 1Total 12
Bergh, Bart vd.indd 41 23-10-15 16:34
Chapter 3
42
Of 127 patients with a uni- or bilateral condyle fracture 2 dentate patients were treated extraorally by a preauricular approach. These patients had severely dislocated bilateral condylar fractures.The mean operation time was 102.2 (± 28.0) minutes. The operation time correlated significantly with the number of fractures (p < 0.01; Pearson’s R 0.7).
ComplicationsOf 225 patients, 34 (15.1%) patients complained of reduced sensitivity of the lip- and chin-region of the fractured side. After 6 months none of the patients complained of permanent hypaesthesia, dysaesthesia or anaesthesia. Objective analyses were not performed.During follow up 15 (6.7%) patients visited the outpatient clinic with a malocclusion of whom 11 malocclusions were corrected by traction through guided elastics. Two (0.9%) patients were retreated surgically within 4 weeks post-operatively, one patient with a fractured mandibular body and another patient with a combined condyle fracture and a mandibular body. These patients underwent a revision of the reduction and fixation procedure. Two other patients who developed a malocclusion were surgically retreated 6 months after initial surgery. One patient had a fractured mandibular angle and developed a lateral open bite on the affected side. This was surgically corrected by a unilateral sagittal split osteotomy. The fourth patient had bilateral condylar fractures and a body fracture and developed an anterior open bite. This patient underwent a bilateral sagittal split osteotomy. Both malocclusions were successfully treated. The long-term results of the occlusions of all patients are unknown as the follow up was stopped six months after surgery according to our departments’ protocol.Six patients presented with infected osteosynthesis. In three of these patients the osteosynthesis was removed. The remaining patients were successfully treated with oral antibiotics. Five patients developed temporomandibular dysfunction during the follow up. These patients were successfully treated with physical therapy.
Bergh, Bart vd.indd 42 23-10-15 16:34

Mandibular fractures
43
3
Discussion
As plate osteosynthesis has become the “gold standard” in the treatment of facial fractures, all mandibular body, angle and ramus fractures were fi xed with plates.3,23,24 A total of 442 plates were used. Zachariades et al. stated that early mobilization is the key in treating condylar fractures.16 Whilst rigid internal fi xation provides stabilization and allows early mobilization, closed treatment is the treatment of choice in our institute. However, in some cases open reduction is recommended, especially in severely displaced and dislocated fractures with loss of ramus height. Despite the fact that some patients of the studied population presented with severely dislocated condyle fracture only two patients were treated with an open reduction. There were no diff erences in treatment results or complications between patients with severely dislocated condyle and patients with some dislocation. Furthermore no diff erences in treatment results or complications were identifi ed between closed treatment and open reduction through a preauricular approach. The treatment results were not measured objectively and because of the small number of patients with a solitary or bilateral condyle fractures it is not possible to make fi rm conclusions from these results.Although in general a high risk of developing an open bite after a bilateral condyle fracture is assumed, no literature relating to this topic is available. Silvenoinnen described two major complications following (uni- or bilateral) condyle fracture.25 In patients with persistent malocclusion, ramus height was signifi cantly reduced, irrespective of the degree or direction of angulation between the fragments. Deviation of the jaw on mouth opening without occlusal disturbances occurred in patients with dislocated condyles. In our study two patients were surgically retreated for an open bite. One of these patients had a bilateral condyle fracture with a body fracture and developed an anterior open bite. No statistical signifi cance could be observed, mainly because of the small number of patients.For several reasons radiographs are taken routinely after treatment of maxillofacial trauma, including surgical treatment evaluation, detection of defects after surgery before the patient is discharged, registration of the osteosynthesis material for removal in the future, for teaching and medico-legal reasons.26,27 For the treatment of 225 patients 471 pre-surgical and 330 post-operative radiographs were taken. It is questionable whether all these
Bergh, Bart vd.indd 43 23-10-15 16:34

Chapter 3
44
radiographic investigations were necessary. Studies have shown that for post-operative evaluation of maxillofacial fractures clinical judgement alone is adequate and taking radiographs is unnecessary.26,27 However, this issue has to be investigated further and will not be discussed further as it is out of the scope of this study.Sixty patients (26.7%) presented with minor or major complications, including altered sensation of the lip and chin, malocclusion, infected osteosynthesis and temporomandibular dysfunction. This proved to be in line with the existing literature.5,28 Four patients needed surgical retreatment for correction of a post-treatment malocclusion. In three patients infected osteosynthesis metalwork was removed. The present study has several shortcomings. In Amsterdam there are 4 hospitals of which two are university hospitals. All these hospitals treat patients with facial injury, however the numbers treated are not equally divided between the hospitals. Most patients are treated in the two university hospitals. Therefore it is questionable if the results of our study can be extrapolated to the whole population of Amsterdam. Like other retrospective studies this retrospective analysis may lead to information bias. The results presented are partly in line with other studies and the analysis of this report provides important data for improving the management of the fractured mandible. Further research must be done into the incidence and prevalence of malocclusion after a bilateral condyle fracture.
Conclusion
The present study gives an overview of 225 patients surgically treated for a fractured mandible. 60 patients (26.7%) presented with minor or major complications. This proved to be in line with the existing literature. In general a high risk of developing an anterior open bite after a bilateral condyle fracture is assumed although no literature related to this topic is available. Further research needs to be performed on the prevalence of an open bite and related clinical problems needing surgical correction. The necessity to take standard post-operative radiographs for evaluation of maxillofacial fractures should be investigated.
Bergh, Bart vd.indd 44 23-10-15 16:34

Mandibular fractures
45
3
References1. Chen CT, Feng CH, Tsay PK, Lai JP, Chen YR. Functional outcomes following surgical treatment of
bilateral mandibular condylar fractures. Int J Oral Maxillofac Surg 2011;40(1):38-44.2. Seemann R, Perisanidis C, Schicho K, Wutzl A, Poeschl WP, Kohnke R, et al. Complication rates of
operatively treated mandibular fractures--the mandibular neck. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109(6):815-9.
3. de Matos FP, Arnez MF, Sverzut CE, Trivellato AE. A retrospective study of mandibular fracture in a 40-month period. Int J Oral Maxillofac Surg 2010;39(1):10-5.
4. Park JM, Jang YW, Kim SG, Park YW, Rotaru H, Baciut G, et al. Comparative study of the prognosis of an extracorporeal reduction and a closed treatment in mandibular condyle head and/or neck fractures. J Oral Maxillofac Surg 2010;68(12):2986-93.
5. Seemann R, Schicho K, Wutzl A, Koinig G, Poeschl WP, Krennmair G, et al. Complication rates in the operative treatment of mandibular angle fractures: a 10-year retrospective. J Oral Maxillofac Surg 2010;68(3):647-50.
6. Iatrou I, Samaras C, Theologie-Lygidakis N. Miniplate osteosynthesis for fractures of the edentulous mandible: a clinical study 1989-96. J Craniomaxillofac Surg 1998;26(6):400-4.
7. Iatrou I, Theologie-Lygidakis N, Tzerbos F. Surgical protocols and outcome for the treatment of maxillofacial fractures in children: 9 years’ experience. J Craniomaxillofac Surg 2010;38(7):511-6.
8. Sauerbier S, Schon R, Otten JE, Schmelzeisen R, Gutwald R. The development of plate osteosynthesis for the treatment of fractures of the mandibular body - a literature review. J Craniomaxillofac Surg 2008;36(5):251-9.
9. Seemann R, Lauer G, Poeschl PW, Schicho K, Pirklbauer M, Russmuller G, et al. CROOMA, complication rates of operatively treated mandibular fractures, paramedian and body. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111(4):449-54.
10. Mueller RV, Czerwinski M, Lee C, Kellman RM. Condylar fracture repair: use of the endoscope to advance traditional treatment philosophy. Facial Plast Surg Clin North Am 2006;14(1):1-9.
11. Bell RB, Wilson DM. Is the use of arch bars or interdental wire fi xation necessary for successful outcomes in the open reduction and internal fi xation of mandibular angle fractures?. J Oral Maxillofac Surg 2008;66(10):2116-22.
12. Bormann KH, Wild S, Gellrich NC, Kokemuller H, Stuhmer C, Schmelzeisen R, et al. Five-year retrospective study of mandibular fractures in Freiburg, Germany: incidence, etiology, treatment, and complications. J Oral Maxillofac Surg 2009;67(6):1251-5.
13. Ellis E,3rd. Treatment methods for fractures of the mandibular angle. Int J Oral Maxillofac Surg 1999;28(4):243-52.
14. Fox AJ, Kellman RM. Mandibular angle fractures: two-miniplate fi xation and complications. Arch Facial Plast Surg 2003;5(6):464-9.
15. Jing J, Han Y, Song Y, Wan Y. Surgical treatment on displaced and dislocated sagittal fractures of the mandibular condyle. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111(6):693-9.
16. Zachariades N, Mezitis M, Mourouzis C, Papadakis D, Spanou A. Fractures of the mandibular condyle: a review of 466 cases. Literature review, refl ections on treatment and proposals. J Craniomaxillofac Surg 2006;34(7):421-32.
17. Burm JS, Hansen JE. The use of microplates for internal fi xation of mandibular fractures. Plast Reconstr Surg 2010;125(5):1485-92.
18. Ellis E,3rd. Complications of mandibular condyle fractures. Int J Oral Maxillofac Surg 1998;27(4):255-7.
19. Marker P, Nielsen A, Bastian HL. Fractures of the mandibular condyle. Part 2: results of treatment of 348 patients. Br J Oral Maxillofac Surg 2000;38(5):422-6.
20. Chuong R, Donoff RB, Guralnick WC. A retrospective analysis of 327 mandibular fractures. J Oral Maxillofac Surg 1983;41(5):305-9.
21. Olson RA, Fonseca RJ, Zeitler DL, Osbon DB. Fractures of the mandible: a review of 580 cases. J Oral Maxillofac Surg 1982;40(1):23-8.
Bergh, Bart vd.indd 45 23-10-15 16:34

Chapter 3
46
22. Stacey DH, Doyle JF, Mount DL, Snyder MC, Gutowski KA. Management of mandible fractures. Plast Reconstr Surg 2006;117(3):48e-60e.
23. Alkan A, Celebi N, Ozden B, Bas B, Inal S. Biomechanical comparison of different plating techniques in repair of mandibular angle fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104(6):752-6.
24. Ellis E,3rd, Moos KF, el-Attar A. Ten years of mandibular fractures: an analysis of 2,137 cases. Oral Surg Oral Med Oral Pathol 1985;59(2):120-9.
25. Silvennoinen U, Iizuka T, Oikarinen K, Lindqvist C. Analysis of possible factors leading to problems after nonsurgical treatment of condylar fractures. J Oral Maxillofac Surg 1994;52(8):793-9.
26. Durham JA, Paterson AW, Pierse D, Adams JR, Clark M, Hierons R, et al. Postoperative radiographs after open reduction and internal fixation of the mandible: are they useful?. Br J Oral Maxillofac Surg 2006;44(4):279-82.
27. Jain MK, Alexander M. The need of postoperative radiographs in maxillofacial fractures--a prospective multicentric study. Br J Oral Maxillofac Surg 2009;47(7):525-9.
28. Serena-Gomez E, Passeri LA. Complications of mandible fractures related to substance abuse. J Oral Maxillofac Surg 2008;66(10):2028-34.
Bergh, Bart vd.indd 46 23-10-15 16:34

Bergh, Bart vd.indd 47 23-10-15 16:34

Bergh, Bart vd.indd 48 23-10-15 16:34

Chapter 4:
“Long-term results and complications after bilateral
mandibular condyle fractures.”
This is an edited version of the manuscript: T. Forouzanfar, F. Lobbezoo, M. Overgaauw, A. de Groot, S. Kommers, M. van Selms, B. van den Bergh.
Long-term results and complications after bilateral mandibular condyle fractures. British Journal of Oral and Maxillofacial Surgery 2013 Oct;51(7):634-8.
Bergh, Bart vd.indd 49 23-10-15 16:34

Chapter 4
50
Abstract
Introduction: The purpose of this study was to investigate the long-term results of closed treatment of bilateral condylar fractures and to study the influence of possible functional impairment on intensity of pain and associated disability.
Results: We studied 71 patients (mean (SD) age 33 (14) years) with bilateral condylar fractures treated with closed treatment. Traffic accidents (n = 42, 59%) and falls (n = 20, 28%) were the main cause of the fractures. Forty-one patients (58%) were re-examined after about 90 months (mean 86, range 3–193). Five of the 41 (12%) had a post-treatment malocclusion, but did not experience any pain in the temporomandibular joint according to the Research Diagnostic Criteria for Temporomandibular Disorders. There was a significant negative relation between the presence of pain and the duration of follow up (p = 0.02). Increasing age was significantly related to reduction in the intensity of pain (p = 0.03). Of the remaining 30 patients who were not followed up, 2 had had bilateral sagittal split osteotomy and 1 a Le Fort I osteotomy. One patient had had orthodontic correction for a malocclusion. Including the five malocclusion patients, at least 9 of the total of 71 (13%) developed a malocclusion after closed treatment. Functional impairment had no influence on the intensity of pain or pain-related disability in the patients with malocclusion after closed treatment for bilateral condylar fractures.
Conclusion: This report may be of value in the debate about whether open or closed treatment is better for bilateral mandibular condylar fractures.
Bergh, Bart vd.indd 50 23-10-15 16:34

Bilateral condyle fractures
51
4
Introduction
A fractured condyle is a common fracture of the mandible, and can be treated with closed treatment and intermaxillary fi xation (IMF) or by open reduction and internal fi xation (ORIF).1-7 Although many studies have investigated the best treatment, the issue remains controversial.5,6 Both types of treatments have complications, including deviation of the chin and facial asymmetry 1,6,8,9, reduced mandibular mobility 5,10, dysfunction of the temporomandibular joint (TMJ) 11,13, ankylosis 5, chronic pain 14, and malocclusion.4,8,11,12
It has been claimed that these complications are more severe after bilateral condylar fractures.12,13 Marker et al. found malocclusion in about 5% of 49 bilateral condylar fractures.4 The combination of bilateral shortening of the ramus8,14 and traction of the suprahyoid musculature is prone to downward mandibular rotation and therefore the development of malocclusion.15 Newman found that 5/52 (10%) patients needed corrective orthognathic surgery after closed treatment for bilateral fracture of the condyles.16 Newman thinks that this complication rate is unacceptably high and is therefore opposed to closed reduction of these types of fractures.Some authors have been convinced that bilateral fractures of the condyles should be treated with ORIF on at least one side 12,13, and Chen et al. found satisfactory functional outcomes when ORIF was used bilaterally for condylar fractures.14 There is a lack of information about the outcomes of the diff erent treatments of these fractures. Reported studies have drawn attention to functional impairments after treatment, often without an investigation into the infl uence of these impairments on patients’ daily function. The purpose of the current study was twofold: fi rstly, to investigate the long-term results of closed treatment of bilateral condylar fractures, and secondly, to study the infl uence of possible functional impairment on the characteristic intensity of pain and pain-related disability assessed by clinical measurements.
Bergh, Bart vd.indd 51 23-10-15 16:34

Chapter 4
52
Patients and methods
We retrospectively reviewed the records of all patients who presented with bilateral condylar fractures between January 1995 and September 2011. Patients with panfacial trauma were excluded. Under general anaesthesia, arch wires were applied for intermaxillary fixation (rigid and guiding elastics) for 6 weeks according to our department’s protocol. (Para)symphyseal fractures were treated with ORIF using 2.0 mm osteosynthesis plates. Data collected included sex, age, length of time between trauma and review (months), cause of the fracture, presence of (para)symphyseal fracture, and dislocation or displacement of the condylar fracture (present or not). All patients were invited to attend for review and the rationale for the study was explained to them. After given informed consent, they had a thorough physical examination using the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD).17 If patients declined to attend, the reason of refusal was ascertained, and they were asked to complete a digital RDC/TMD axis II questionnaire.
Physical examinationA functional examination of the masticatory system was made using the protocol of the RDC/TMD17 by one of the authors (FL, a dentist who specialises in TMD and orofacial pain). The occlusion was noted, and the type of malocclusion (anterior open bite or crossbite) was recorded. The active and passive mouth opening, presence of deviation of the mandible at maximal mouth opening (MMO), and protrusion and laterotrusion were measured (including the possible intensity and site of pain). MMO of less than 40 mm was considered restricted, a modification to the restricted mouth opening regarded by RDC/TMD (MMO < 35 mm). The masseter muscle, temporal muscle, medial and lateral pterygoid muscle, and the TMJ were palpated bilaterally. In total, 12 sites were palpated on both sides; 8 extraoral and 2 intraoral muscle sites, and 2 in the TMJ. Finally, static and dynamic pain tests were done, and directly after each test, patients were asked if they experienced any sensitivity or pain in the investigated area. They were asked to point to the site of the pain and to indicate if they were familiar with the feeling (“familiar pain”).
Bergh, Bart vd.indd 52 23-10-15 16:34

Bilateral condyle fractures
53
4
Digital questionnairePatients were asked to fi ll out a digital RDC/TMD axis II questionnaire 17, which included the 7-item graded classifi cation of chronic pain based on its characteristic intensity and pain-related disability. The aim of the questions was to quantify the patients’ chronic facial pain and its impact on their activities on 11-point visual analogue scales. The classifi cation placed respondents into 1 of 5 hierarchical grades: free of pain (grade 0), little disability or intensity (grade 1); little disability but intense pain (grade 2); seriously disabling and moderately limiting, (grade 3); and seriously disabling and severely limiting (grade 4). We have subdivided the scores into “characteristic pain intensity” (mean of three pain-related questions multiplied by 10) and “disability score” (mean of three disability-related questions multiplied by 10).
Statistical analysisDescriptive statistics were computed for age, gender, cause of trauma, duration of follow up, occlusion, sounds in the TMJ, deviation of the mandible at MMO, and dislocated condylar fracture. To facilitate interpretation, bilateral measures (such as sounds in the TMJ) were combined into single variables. For palpation, the 4-point ordinal scale was divided into “no pain” and compared with “any pain” (the presence of pain regardless of intensity) categories. Similarly, joint sounds were divided into “sounds” and “no sounds”. For continuous measures (for example, the mandibular range of movement), mean (SD) and range were calculated, while for dichotomous measures, the number of positive ratings was calculated. Single regression analyses were used to identify possible factors associated with the presence of pain (logistic regression) or with characteristic intensity of pain and disability scores (linear regression). The linearity of the eff ect of ordinal variables was checked by analysis of dummy variables. When the regression coeffi cients of the dummy variables consistently increased (or decreased), they were regarded as linear. The odds ratios (ORs) and their 95% confi dence intervals (CIs) are reported for the predictive variables in the regression analyses. Data were processed with the help of the Statistical Package for the Social Sciences (SPSS version 19.0, Chicago, IL, USA). Probabilities of less than 0.05 were accepted as signifi cant.
Bergh, Bart vd.indd 53 23-10-15 16:34

Chapter 4
54
ResultsSeventy-one patients (36 men and 35 women, mean (SD) age 33 (14) years) were eligible for inclusion in this study. The causes of injury are shown in tables 1 and 2. Fourteen patients had “solitary” condylar fractures and 57 had an associated (para)symphyseal fracture that was anatomically reduced and plated to stabilise the occlusion.
Table 1. Cause of trauma for the participants and non-participants. Data are number and percentages.
Follow up (N=41)
No follow up (N=30)
Combined
No. % No. % No. %
Fall 9 22 11 37 20 28
Interpersonal violence 2 5 2 7 4 6
Traffic accident (pedestrian / bicycle / motor / car) 27 66 15 50 42 59
Sports-related trauma 2 5 1 3 3 4
Missing 1 2 1 3 2 3
Total (%) 41 100 30 100 71 100
Table 2. Causes of trauma by sex. Data are numbers and percentages.
♀ % ♂ % ♀+♂ %
Fall 7 20 13 36 20 28
Interpersonal violence 1 3 3 8 4 6
Traffic accident – pedestrian 0 0 1 3 1 1
Traffic accident – bicycle 23 66 10 28 33 47
Traffic accident - motor 1 3 5 14 6 8
Traffic accident – car 0 0 2 6 2 3
Sports-related trauma 1 3 0 0 1 1
Otherwise specified (e.g. work-related) 2 5 0 0 2 3
Missing 0 0 2 5 2 3
Total % 35 100% 36 100% 71 100%
The details of patients’ participation in the follow up are shown in table 3. Forty-one patients (58%) therefore participated in the study. The follow up period was approximately 90 months (mean 86, range 3–193).
Bergh, Bart vd.indd 54 23-10-15 16:34

Bilateral condyle fractures
55
4
Table 3. Participation in the follow up (n=71).
No. %
Did not attend outpatient clinic, but completed questionnaire 3 4
Agreed to participate, but did not attend 3 4
Refused to participate 1 1
Failed to obtain contact (telephone, email, letter, or through GP) 23 33
Attended outpatient clinic 41 58
Total (%) 71 100%
Of the 41 patients, no patients were seen with a crossbite, but 5 presented with an anterior open bite. The follow up periods for these 5 patients were respectively 3, 16, 99, 132, and 146 months (table 4).
Table 4. Results of functional examination of the mastication system. Data are mean (SD) or number (No., %).
Variable Measurement
Mean (SD) maximum mouth opening (mm) ( n=41) 49 (SD 9)
Patients with no malocclusion (n=36) 49 (SD 9)
Patients with malocclusion (n=5) 51 (SD 10)
No. with deviated mandible at maximum mouth opening 8 (20)
No. with pain 19 (46)
No. with limited range of mandibular movement (40mm or less) 7 (17)
No. with sounds in the temporomandibular joint 11 (27)
Of the 30 patients who did not attend for follow up, we found that 2 had had bilateral sagittal split osteotomy and 1 a Le Fort I osteotomy. One patient was treated orthodontically. Therefore at least 9 patients (9/71, 13%) had developed a malocclusion.With regard to the classifi cation of pain taken from the RDC/TMD, no patients with malocclusion had any temporomandibular pain during the previous 6 months (grade 0). Of those who did not have a malocclusion, 32 had no complaints regarding the TMD. Five patients were diagnosed with little intensity or disability (grade 1). One patient experienced intense pain but little disability (grade 2), and 1 patient had moderately limiting but seriously disabling pain (grade 3). No patients experienced severely limiting and
Bergh, Bart vd.indd 55 23-10-15 16:34

Chapter 4
56
seriously disabling pain (grade 4). The regression analyses showed a (negative) significant relation between the presence of pain and the duration of follow up (p = 0.02, table 5). After dividing the classification into intensity of pain and disability score, increasing age was significantly related to decreasing intensity of pain (p = 0.03, tables 6a and 6b). A (negative) trend was noticed between the cause of the trauma and the disability score (p = 0.08). We found no other significant relations or trends.
Table 5. Logistic regression analysis of the factor used to predict pain.
Prognostic factor p-value odds ratio 95% CI
Age (years) 0.94 0.99 0.95 – 1.05
Sex 0.21 2.48 0.60 – 10.27
Cause of injury 0.25 1.24 0.86 – 1.77
Duration of follow up 0.02 0.98 0.97 – 0.99
Occlusion 0.74 1.53 0.13 – 18.76
Sounds in the temporomandibular joint 0.18 2.93 0.61 – 14.23
Mandibular deviation at MMO 0.07 8.273 0.88 – 78.01
Dislocated condylar fracture 0.40 0.36 0.03 – 3.92
CI, confidence interval; MMO: maximum mouth opening
Table 6a. Linear regression analysis for prediction of intensity of pain.
Prognostic factor p-value odds ratio 95% CI
Age (years) 0.03 -0.54 -1.01 to -0.05
Sex 0.64 2.99 -9.93 to 15.90
Cause of injury 0.28 1.78 -1.51 to 5.06
Duration of follow up 0.72 0.24 -0.11 to 0.16
Occlusion 0.52 -9.41 -38.97 to 20.15
Sounds in the temporomandibular joint 0.28 -7.47 -21.30 to 6.35
Mandibular deviation at MMO 0.23 -9.71 -26.05 to 6.63
Dislocated condylar fracture 0.37 -5..87 -19.31 to 7.57
CI, confidence interval; MMO: maximum mouth opening
Bergh, Bart vd.indd 56 23-10-15 16:34

Bilateral condyle fractures
57
4
Table 6b. Linear regression analysis for prediction of disability score.
Prognostic factor p-value odds ratio 95% CI
Age (years) 0.70 -0.09 -0.56 to 0.38
Sex 0.91 0.67 -11.18 to 12.52
Cause of injury 0.08 2.61 -0.32 to 5.53
Duration of follow up 0.57 -0.04 -0.16 to 0.09
Occlusion 0.66 -5.98 -33.21 to 21.24
Sounds in the temporomandibular joint 0.33 -6.14 -19.03 to 6.75
Mandibular deviation at MMO 0.48 -5.37 -20.60 to 9.87
Dislocated condylar fracture 0.66 4.38 -15.86 to 24.63
CI, confi dence interval; MMO: maximum mouth opening
Discussion
We assumed that the pre-existing occlusion was normal if there were no anatomical features to suggest otherwise (such as mamelons) and attempted to confi rm this with previous photographs if available. Few reports have dealt with pain after bilateral condylar fractures, and this study of 71 patients is, to the best of our knowledge, the largest of its kind. Interestingly there is a greater proportion of bilateral condylar fractures in female patients than in other reports, although we do not know why.4,7,12 In this study 66% of the trauma in female patients were caused by bicycle accidents, compared to 28% of the trauma in male patients. This remarkable observation is in concordance with a previous epidemiology study of maxillofacial trauma in Amsterdam.25
Palmieri et al. compared mandibular movement after either open treatment or closed treatment for unilateral condylar fractures.5 Initially the MMO was signifi cantly greater after closed treatment than open, but in the long term there were no signifi cant diff erences. Chen et al. assessed the functional outcomes of bilateral fractured condyles treated by ORIF and found a signifi cantly higher incidence of limited mouth opening, particularly after bilateral condylar fractures, compared with combined condylar/subcondylar and subcondylar/subcondylar fractures.14 Marker et al. investigated 39 patients with bilateral condylar fractures, and 21% of them experienced pain in the TMJ or the muscles, 15% had reduced MMO, 8% developed malocclusion,
Bergh, Bart vd.indd 57 23-10-15 16:34

Chapter 4
58
and 3% had deviation on MMO.4 Gupta et al. compared closed treatment and ORIF for both unilateral (n = 22) and bilateral (n = 6) condylar fractures. Initially they found less passive pain, less pain on movement, less swelling, increased MMO, better recovery of mandibular movements, and greater masticatory efficiency in the ORIF group. However, after a period of 12 weeks there were no differences.13 Park et al. found no differences in post-operative complications after ORIF and closed treatment for fractures of the mandibular condyle.6 Three patients required surgical correction and one orthodontic treatment, although it is not clear whether the decisions were made on clinical grounds or at the patients’ request. The remaining 5 patients with malocclusion had no treatment and no ongoing issues with the TMD issues (pain grade 0). The MMO in patients with malocclusion was comparable (51.2 mm) with that of patients who had no malocclusion (48.5 mm). Regression analyses of the different variables showed a significant (negative) relation between the presence of pain and duration of follow up (p = 0.02), and a significant relation between decreasing intensity of pain with increasing age (p = 0.03). This may suggest that sensations of pain can diminish or even disappear over time, which could be of great importance when counselling new patients. Twenty-six patients (30 who did not participate in the follow up minus 4 who had surgical or orthodontic correction) were not seen at follow up. As these 26 patients are therefore without complaints or may have presented elsewhere, at least 13% of patients (9 of 71) developed malocclusion.14,18 In the discussion about treating mandibular condylar fractures with ORIF or with closed treatment, the treatment-related and corrective surgical complications should be taken into account. Published complications related to ORIF are: temporary or permanent paresis of branches of the facial nerve, wound infection, transient salivary fistula, failure of osteosynthesis, pseudarthrosis, functional occlusal disturbance or malocclusion, and the need for revisional surgery.19–21 Major complications such as palsy of the facial nerve and the need for revision are rare in the hands of sufficiently skilled surgeons, independently of the approach.21,22 However, a malocclusion that developed after closed treatment can be corrected secondarily by orthognatic surgery. In 2007 Kim et al. reviewed the incidence of orthognathic-related complications in 301 patients. A total of 34 perioperative complications (4% unfavourable osteotomies, 2% excessive bleeding, 1% fractures of instruments, 2% soft tissue injuries, 1% exposure of nerve, and 1% injuries to teeth), and 300 post-
Bergh, Bart vd.indd 58 23-10-15 16:34

Bilateral condyle fractures
59
4
operative complications (65% temporary sensory disturbances, 21% transient respiratory diffi culties, 9% neck pain or discomfort, 4% open bites, and 1% wound infections) occurred.23 The authors concluded that despite the great variety of severe complications reported, their incidence seems to be low. Orthognathic surgery therefore seems to be safe, a conclusion that is also affi rmed by Morris et al.24 The low recall rate is normal for a follow up study in trauma. From a statistical point of view it is questionable whether the clinical assessments of a study group of 41 patients can be extrapolated to an entire group of 71 patients treated. Although there is the potential for selection bias, the study showed two distinctly signifi cant relations (pain and duration of follow up, and age and intensity of pain). We think therefore that the results of this report may be of value in the debate about whether open or closed treatment is best for (bilateral) fractures of the mandibular condyle and the need to treat malocclusion that develops after trauma, as not all malocclusions lead to functional problems.
Bergh, Bart vd.indd 59 23-10-15 16:34
Chapter 4
60
References
1. Bormann KH, Wild S, Gellrich NC, Kokemuller H, Stuhmer C, Schmelzeisen Ret al. Five-year retrospective study of mandibular fractures in Freiburg, Germany: incidence, etiology, treatment, and complications. J Oral Maxillofac Surg 2009;6:1251-1255.
2. de Matos FP, Arnez MF, Sverzut CE, Trivellato AE. A retrospective study of mandibular fracture in a 40-month period. Int J Oral Maxillofac Surg 2010;1:10-15.
3. Loukota RA, Eckelt U, De Bont L, Rasse M. Subclassification of fractures of the condylar process of the mandible. Br J Oral Maxillofac Surg 2005;1:72-73.
4. Marker P, Nielsen A, Bastian HL. Fractures of the mandibular condyle. Part 2: results of treatment of 348 patients. Br J Oral Maxillofac Surg 2000;5:422-426.
5. Palmieri C, Ellis E, III, Throckmorton G. Mandibular motion after closed and open treatment of unilateral mandibular condylar process fractures. J Oral Maxillofac Surg 1999;7:764-775.
6. Park JM, Jang YW, Kim SG, Park YW, Rotaru H, Baciut Get al. Comparative study of the prognosis of an extracorporeal reduction and a closed treatment in mandibular condyle head and/or neck fractures. J Oral Maxillofac Surg 2010;12:2986-2993.
7. Sharif MO, Fedorowicz Z, Drews P, Nasser M, Dorri M, Newton Tet al. Interventions for the treatment of fractures of the mandibular condyle. Cochrane Database Syst Rev 2010;4:CD006538.
8. Bhagol A, Singh V, Kumar I, Verma A. Prospective evaluation of a new classification system for the management of mandibular subcondylar fractures. J Oral Maxillofac Surg 2011;4:1159-1165.
9. Yang WG, Chen CT, Tsay PK, Chen YR. Functional results of unilateral mandibular condylar process fractures after open and closed treatment. J Trauma 2002;3:498-503.
10. Niezen ET, Bos RR, de Bont LG, Stegenga B, Dijkstra PU. Complaints related to mandibular function impairment after closed treatment of fractures of the mandibular condyle. Int J Oral Maxillofac Surg 2010;7:660-665.
11. Silvennoinen U, Raustia AM, Lindqvist C, Oikarinen K. Occlusal and temporomandibular joint disorders in patients with unilateral condylar fracture. A prospective one-year study. Int J Oral Maxillofac Surg 1998;4:280-285.
12. Zachariades N, Mezitis M, Mourouzis C, Papadakis D, Spanou A. Fractures of the mandibular condyle: a review of 466 cases. Literature review, reflections on treatment and proposals. J Craniomaxillofac Surg 2006;7:421-432.
13. Gupta M, Iyer N, Das D, Nagaraj J. Analysis of Different Treatment Protocols for Fractures of Condylar Process of Mandible. J Oral Maxillofac Surg 2011.
14. Chen CT, Feng CH, Tsay PK, Lai JP, Chen YR. Functional outcomes following surgical treatment of bilateral mandibular condylar fractures. Int J Oral Maxillofac Surg 2011;1:38-44.
15. Becking AG, Zijderveld SA, Tuinzing DB. Management of posttraumatic malocclusion caused by condylar process fractures. J Oral Maxillofac Surg 1998;12:1370-1374.
16. Newman L. A clinical evaluation of the long-term outcome of patients treated for bilateral fracture of the mandibular condyles. Br J Oral Maxillofac Surg 1998;3:176-179.
17. Lobbezoo F, van Selms MK, John MT, Huggins K, Ohrbach R, Visscher CMet al. Use of the Research Diagnostic Criteria for Temporomandibular Disorders for multinational research: translation efforts and reliability assessments in The Netherlands. J Orofac Pain 2005;4:301-308.
18. Smets LM, Van Damme PA, Stoelinga PJ. Non-surgical treatment of condylar fractures in adults: a retrospective analysis. J Craniomaxillofac Surg 2003;3:162-167.
19. Downie JJ, Devlin MF, Carton AT, Hislop WS. Prospective study of morbidity associated with open reduction and internal fixation of the fractured condyle by the transparotid approach. Br J Oral Maxillofac Surg 2009;5:370-373.
20. Vesnaver A, Ahcan U, Rozman J. Evaluation of surgical treatment in mandibular condyle fractures. J Craniomaxillofac Surg 2011.
21. Meyer C, Zink S, Chatelain B, Wilk A. Clinical experience with osteosynthesis of subcondylar fractures of the mandible using TCP plates. J Craniomaxillofac Surg 2008;5:260-268.
Bergh, Bart vd.indd 60 23-10-15 16:34

Bilateral condyle fractures
61
4
22. Ellis E, III, McFadden D, Simon P, Throckmorton G. Surgical complications with open treatment of mandibular condylar process fractures. J Oral Maxillofac Surg 2000;9:950-958.
23. Kim SG, Park SS. Incidence of complications and problems related to orthognathic surgery. J Oral Maxillofac Surg 2007;12:2438-2444.
24. Morris DE, Lo LJ, Margulis A. Pitfalls in orthognathic surgery: avoidance and management of complications. Clin Plast Surg 2007;3:e17-e29.
25. B. van den Bergh, K.H. Karagozoglu, M.W. Heymans, T. Forouzanfar. Aetiology and incidence of maxillofacial trauma in Amsterdam: A retrospective analysis of 579 patients. Journal of Cranio-Maxillo-Facial Surgery 2012 Sep;40(6):e165-9.
Bergh, Bart vd.indd 61 23-10-15 16:34

Bergh, Bart vd.indd 62 23-10-15 16:35

Chapter 5:
“Closed treatment of mandibular condyle fractures: comparing
intermaxillary fi xation with screws or arch bar. A randomised
clinical trial.”
This is an edited version of the manuscript: B. van den Bergh, J. Blankestijn, T. van der Ploeg, D.B. Tuinzing, T. Forouzanfar. Conservative treatment of a mandibular condyle fracture:
comparing intermaxillary fi xation with screws or arch bar. A randomised clinical trial. Journal of Cranio-Maxillo-Facial Surgery 2015 Jun;43(5):671-6.
Bergh, Bart vd.indd 63 23-10-15 16:35

Chapter 5
64
Abstract
Introduction: A mandibular condyle fracture can be treated with closed treatment by intermaxillary fixation (IMF) or with open reduction and internal fixation (ORIF). Many IMF-modalities can be chosen, including IMF screws (IMFS). This prospective multicentre randomised clinical trial compared the use of IMFS with the use of arch bars in closed treatment of mandibular condyle fractures.
Results: The study population consisted of 50 patients (mean age: 31.8 years). Twenty-four (48%) patients were allocated in the IMFS group. Twenty-six (52%) patients were assigned to the arch bars group. In total 188 IMF screws were used (5–12 screws per patient, mean 7.83 screws per patient). All pain scores were lower in the IMFS group. Three patients developed a malocclusion (IFMS-group: one patient, arch bars-group: two patients). Mean surgical time was significantly shorter in the IMFS group (59 vs. 126 min; p <0.001). There were no needlestick injuries (0%) in the IMFS group and eight (30.7%) in the arch bars group (p = 0.003). One IMF screw fractured on insertion (0.53%), one (0.53%) screw was inserted into a root. Six (3.2%) screws loosened spontaneously in four patients. Mucosal disturbances were seen in 22 patients, equally divided over both groups.
Conclusion: Considering the advantages and the disadvantages of IMFS, and observing the results of this study, the authors conclude that IMFS provide a superior method for IMF. IMFS are safer for the patients and surgeons.
Bergh, Bart vd.indd 64 23-10-15 16:35

Screws or arch bars?
65
5
Introduction
A mandibular condyle fracture is one of the most common fractures of the mandible15,16,26, and is mostly caused by falls, interpersonal violence and traffi c-accidents.15,26 This kind of fracture can be treated with closed treatment by intermaxillary fi xation (IMF) or with open reduction and internal fi xation (ORIF). Although many studies have searched for the best and most suitable treatment, the issue remains controversial.19,20,24, 30,31 In both types of treatment complications occur, such as deviation of the chin and/or facial asymmetry.3,20,28; reduced mandibular motility17,19; dysfunction of the temporomandibular joint10,25; ankylosis10; chronic pain4; and malocclusion2,7,15,25,29. When closed treatment of a condylar fracture is preferred over ORIF, many modalities for obtaining IMF can be considered (e.g. arch bars, eyelets, interdental wiring or orthodontic braces). Whereas the use of arch bars is generally the treatment of choice, the use of interdentally placed screws (IMFS) is gaining popularity and is increasing.The use of these screws provides many benefi ts to both patients and surgeons.5,9,11,22 Compared with arch bars, IMFS are quick and easy to place, have relatively low costs, are ideal for use when teeth have been heavily restored and give reduced trauma to dental papillae and the oral mucosa. Furthermore, gingival health is easier to maintain and IMFS are easily and painlessly removed.1,5,9,11,12,14,18,22,23 Related to this there is reduced risk of needlestick injury to the surgeon as the need for placing interdental wiring is absent14, while operation time is considerably reduced compared with IMF techniques with arch bars.21-23,27 Several case reports and some retrospective studies support the usefulness of the IMFS technique.6,8,13,18 Complications relating to IMFS may occur. Potential surgical complications include the fracture of the screw on insertion, iatrogenic damage to dental roots, causing bony sequestra around the area of screw placement and loss of teeth.5,11,22 Post-operative complications include infection associated with screws, loss or loosening of screws, screws covered by oral mucosa, post-operative malocclusion and paraesthesia due to injury to the mental or inferior alveolar nerve.5,6,11,14,22
In 2011 a clinical trial was published in which the use of IMFS in maxillofacial trauma was compared with Erich arch bars.21 West et al. recently described a randomised clinical trial of 20 patients who were all treated for a mandibular fracture, but excluded patients with a condylar fracture.27 There is still a lack of
Bergh, Bart vd.indd 65 23-10-15 16:35

Chapter 5
66
prospective randomised clinical trials concerning the use of IMFS in oral and maxillofacial trauma, especially in closed treatment of mandibular condylar fractures.The purpose of the present study is to compare the use of IMFS-screws with arch bars in closed treatment of mandibular condylar fractures. In particular pain, the occlusal results, surgical duration, oral hygiene, mouth opening and intra- and post-operative complications/adverse side effects will be analysed.
Material and methods
A prospective multi-centre randomised clinical trial was conducted between May 2010 and July 2014. Patients were eligible when aged between 18 and 65 years, who had given signed informed consent and required treatment of a fractured mandibular condyle (with or without concomitant mandibular fractures). The study protocol was approved by the Ethics Committee of the VU University Medical Center Amsterdam and Medical Centre Alkmaar (reg. no. NL28831.029.09; 2009/311).Exclusion criteria included: inability to give informed consent, known chronic pain syndrome, mental retardation or psychiatric abnormalities, concomitant maxillary or other facial fractures and known malignant disease. All patients provided signed informed consent before surgical treatment.
Study protocolAfter giving consent, patients were randomised by an assignment scheme that was generated from a table of random numbers. This table was developed, using a computer program designed for randomisation purposes. The randomised and sealed envelopes were opened by the surgeon the moment the patient was brought under general anaesthesia. Randomisation was to either IMFS study group or arch bars control group. Trial participants were blinded to group allocation until the end of the operation.
ProcedureThe Food and Drug Administration-approved screws (Dual-Top™ G2 Screw, Jeil Medical, Seoul, Korea) were placed in the interproximal or edentulous spaces at the mucogingival junction. The screw insertion site was based on clinical
Bergh, Bart vd.indd 66 23-10-15 16:35
Screws or arch bars?
67
5
and radiographic information. Screws were placed in locations that provided appropriate vectors to re-establish the pretraumatic occlusion and at an appropriate distance from root prominences. The intention was to orient the long axis of the screws at 90 degrees to the roots of the adjacent teeth. IMF was established by stainless steel wires through/around the placed screws in the maxilla and mandible. The arch bar was fi xed by stainless steel wires around teeth from the incisors to the second molar (if available). IMF was established by fi xing the mandible against the maxilla with stainless steel wires around the cleats of the arch bars. If fi xation of the body of the mandible was necessary, 2.0-mm plates were used. The length of these plates and screws depended on the line of fracture. The plates were placed according to the Champy-principle.
Follow upThe post-operative follow up was the same as described in the treatment protocol for mandibular fractures as used in our department, i.e. every week post-operatively for 6 weeks. After 6 weeks the screws or arch bars were removed in an outpatient clinical setting without the use of analgesic medication or local anaesthesia. Loosened screws during the follow up period would have been replaced in an alternative location under local anaesthesia if necessary. Dropout was observed and reasons for dropout were registered.
Outcome measuresThe primary outcome measure was pain assessment. All patients were asked to rate their level of pain, three times daily (at 9am, 3pm and 9pm) for 7 days on a 100-mm visual analogue scale (VAS). This scale was anchored by two extremes of pain: ‘no pain’ on the left and ‘the worst possible pain’ on the right end. At day 7 patients were asked to mark their average pain of the fi rst week on a VAS scale with the same extremes. On day 3 and on day 7 patients were asked if the pain had changed in comparison with the fi rst two days (7-point scale: ‘maximally worse’, ‘a lot worse’, ‘mildly worse’, ‘equally painful’, ‘mildly improved’, ‘a lot improved’ and ‘maximally improved’). Six weeks post-operatively, when the IMFS or arch bars were removed, patients were asked to rate their pain immediately after and fi ve min after removal on a 100-mm VAS.Secondary outcome measures were the dental occlusion (rated as: pretraumatic occlusion, suboptimal occlusion or malocclusion); surgical treatment time (in min); oral hygiene (using a Likert scale: good, moderate, or poor oral
Bergh, Bart vd.indd 67 23-10-15 16:35

Chapter 5
68
hygiene); intraoperative complications/adverse side effects (e.g. needlestick injuries, screw-fracture on insertion, iatrogenic damage causing loss of teeth or bony sequestra around the area of screw placement, and/or damage to dental roots); post-operative complications/adverse side effects (e.g. infection associated with IMFS, loss of bone screws, screws covered by oral mucosa and/or paraesthesia due to injury to the mental or inferior alveolar nerve).
Statistical analysisPower analysisA power analysis was performed with α = 0.05 and β = 0.1. The authors assumed the VAS-score to change 2 points on the 10 point scale (δ = 2) and also assumed a deviation would be equal to 2 (σ = 2). These assumptions lead to a sample size of 22 per group: n = 2σ²/(m2-m1)² × f (α,β) = 2*4/4 × 10.5 = 21 per group (n = population; σ = common standard deviation; m1 = mean of population 1; m2 = mean of population 2; α = desired level of statistical significance; β = desired power; * = multiplication sign). Therefore n = 22. Descriptive statistics (numbers, percentages, mean and standard deviation) were computed for sex, age, cause of trauma and total IMFS. Differences with respect to the groups were tested (for example, VAS-scores) using a Mann–Whitney U test. Dichotomous measures (for example, occlusion) and ordinal measures (for example, oral hygiene) with respect to the groups were tested using chi-square tests. For the analysis the IBM Statistical Package SPSS version 22.0.0 was used. P-values less than 0.05 were considered as significant.
Results
After giving informed consent, in total 50 patients were included: 30 (60%) male patients and 20 (40%) female patients (mean age: 31.8 yrs; SD 13.9 yrs; range 18-64 yrs). Of these patients, 40 (80%) were treated in de VU University Medical Center Amsterdam, and 10 (20%) in the Medical Centre Alkmaar. Seven (14%) patients were treated for a solitary condylar fracture, 34 (68%) patients had a concomitant mandibular fracture, two (4%) patients were treated for bilateral condylar fractures, and seven (14%) patients had bilateral condylar fractures combined with another mandibular fracture (table 1). Twenty-four (48%)
Bergh, Bart vd.indd 68 23-10-15 16:35

Screws or arch bars?
69
5
patients were allocated to the study group (IMFS). In total, 188 IMF screws were used (5–12 screws per patient; mean 7.83 screws per patient). Twenty-six (52%) patients were assigned to the control group (arch bars).
Table 1. Overview of type of fractures.
Type of fracture No. %
Solitary condylar fractures 7 14
Condylar fracture with concomitant mandibular fracture 34 68
Bilateral condylar fractures 2 4
Bilateral condylar fractures with concomitant mandibular fracture 7 14
Total % 50 100
Clinical admittance periods for patients treated with IMFS did not diff er signifi cantly from patients treated with arch bars (p = 0.718; mean 2.14 vs. 2.48 days). For three patients the follow up results were not available (three of 50 patients: 6% dropout). These three patients were treated with arch bars (three of 26 patients: 11.5%; p = 0.086). Two patients did not attend the outpatient clinic and removed their arch bars themselves (information obtained through their GP or dentist). The third patient had the arch bars removed after four weeks (instead of 6 weeks protocol), as this patient had to be imprisoned and the presence of metal-containing materials was prohibited for safety-reasons. This patient had a pretraumatic occlusion and further functional therapy was considered unnecessary.The randomisation procedure was checked by comparing the groups for relevant variables. The groups did not diff er signifi cantly when observing sex, age, smoking habit, presence of diastemata, presence of hematoma in the fl oor of the mouth, loss of or altered sensitivity of the lower lip, presence of deviation of the mandible, post-traumatic maximal mouth opening, cause of trauma, impact, nature and side of impact, type of fracture and side of condylar fracture (all p-values >0.05, table 2).
Bergh, Bart vd.indd 69 23-10-15 16:35

Chapter 5
70
Table 2. Comparison of IMF screws group and arch bars group.
Characteristic p-value
Sex 0.729
Age 0.247
Smoking habit 0.052
Presence of diastema 0.786
Presence of hematoma in floor of mouth 0.312
Loss of or altered sensitivity lower lip 0.086
Presence of deviation of the mandible 0.446
Post-traumatic maximal mouth opening (MMO) 0.167
Cause of trauma 0.683
Nature of impact 1.000
Side of impact 0.670
Type of fracture 0.972
Side of condylar fracture 0.700
PainAll pain scores measured in the first week, were lower in the IMFS group in comparison to the arch bars group, and they were significantly lower on day 1 (at 9pm), day 2 (at 9am and 3pm), day 3 (at 9am, 3pm and 9pm) and day 5 (at 9pm; table 3). A trend was observed at time point 9pm on day 2 (p = 0.075). The recorded average pain of the last 7 days was significantly lower in the IMFS group (p = 0.048, mean 25.35 mm) compared with arch bars (mean 36.86 mm; table 3). No significant difference was observed between the study groups for the pain changes in comparison with the first two days, asked on day 3 and 7 (p = 0.161 and p = 0.381 respectively). Pain, measured directly after removing the IMFS (mean 20.79 mm) or arch bars (mean 33.32 mm) and five min later (mean 7.21 mm vs. 18.59 mm), was significantly lower in the IMFS group (p = 0.025 and p = 0.004 respectively).
Bergh, Bart vd.indd 70 23-10-15 16:35

Screws or arch bars?
71
5
Table 3. Pain-analysis of IMF screws group and arch bars group.
Day Pain score IMF screwsMean (SD and
range)
Arch barsMean (SD and
range)
p-value
1 VAS-score 9AM (in mm) 30.70 (22.3; 2–90) 38.42 (23.7; 0–98) 0.193
VAS-score 3PM (in mm) 29.78 (16.1; 3–64) 39.42 (19.8; 6–90) 0.111
VAS-score 9PM (in mm) 30.57 (18.4; 2–72) 42.42 (18.7; 5–77) 0.039*
2 VAS-score 9AM (in mm) 24.22 (15.2; 1–56) 40.57 (21.7; 3–88) 0.012*
VAS-score 3PM (in mm) 26.78 (15.9; 2–55) 40.76 (21.1; 5–77) 0.022*
VAS-score 9PM (in mm) 31.09 (23.9; 1–90) 40.95 (21.3; 7–84) 0.075^
3 VAS-score 9AM (in mm) 21.65 (16.4; 1–67) 37.19 (25.8; 6–98) 0.035*
VAS-score 3PM (in mm) 20.13 (15.7; 1–51) 37.71 (23.5; 4–91) 0.006*
VAS-score 9PM (in mm) 24.48 (20.4; 1–81) 37.14 (20.4; 4–83) 0.027*
4 VAS-score 9AM (in mm) 25.00 (19.8; 3–74) 30.48 (24.3; 1–93) 0.480
VAS-score 3PM (in mm) 21.13 (15.3; 4–57) 29.71 (20.5; 1–82) 0.192
VAS-score 9PM (in mm) 21.91 (17.8; 3–71) 28.71 (19.6; 2–84) 0.188
5 VAS-score 9AM (in mm) 18.48 (19.8; 2–62) 30.43 (23.9; 3–88) 0.034*
VAS-score 3PM (in mm) 18.35 (18.1; 1–62) 25.67 (18.8; 2–56) 0.240
VAS-score 9PM (in mm) 20.35 (19.7; 0–77) 26.38; (19.7; 1–57) 0.341
6 VAS-score 9AM (in mm) 16.57 (15.3; 2–50) 27.48 (25.3; 0–93) 0.244
VAS-score 3PM (in mm) 16.43 (15.2; 0–58) 25.48 (19.3; 0–68) 0.158
VAS-score 9PM (in mm) 16.09 (15.3; 2–50) 22.33 (19.7; 0–70) 0.510
Pain at day 3 compared to day 0 ––– ––– 0.161
Pain at day 7 compared to day 0 ––– ––– 0.381
Average pain of last week (VAS-score, in mm)
25.35 (18.6; 1–71) 36.86 (20.6; 3–85) 0.048*
Pain directly after removal of IMF screws or arch bars (mm)
20.79 (18.5; 1–74) 33.32 (23.5; 0–84) 0.025*
Pain 5 min after removal of IMF screws or arch bars (mm)
7.21 (11.6; 0–49) 18.59 (19.9; 0–65) 0.004*
*signifi cant p <0.05; ^trend. IMF: intermaxillary fi xation; VAS: visual analogue scale.
Occlusal resultsAt 6 weeks, after removal of the IMF screws or arch bars, three patients had developed a malocclusion/suboptimal occlusion. An anterior open bite was noticed in one (4.2%) patient who was treated with IMFS for a bilateral condylar fracture with concomitant mandibular fracture. In the arch bars group, two patients (7.7%; p = 0.576) developed a suboptimal occlusion: the fi rst patient was treated for a bilateral condylar fracture and developed a minimal anterior
Bergh, Bart vd.indd 71 23-10-15 16:35

Chapter 5
72
open bite. The second patient was treated for a solitary condylar fracture and developed a minor open bite in the premolar region.
Surgical procedureThe (mean) time needed to place IMFS was 17 min (range 5–30), significantly shorter than applying arch bars (mean time: 69 min; range: 35–132; p < 0.001). The mean surgical times for the IMFS group and arch bars group were mean 59 min (range 14–104) and 126 min (range 54–220; p < 0.001) respectively.
Oral hygieneOral hygiene did not differ in both groups in the six-week post-operative period (table 4).
Table 4. Analysis of oral hygiene in IMF screws group and arch bars group.
Week Oral hygiene IMF screws (No.)
Arch bars (No.)
p-value
1 Poor oral hygiene 5 9
Moderate oral hygiene 8 6
Good oral hygiene 10 7
Missing 1 4 0.223
2 Poor oral hygiene 3 4
Moderate oral hygiene 6 6
Good oral hygiene 13 11
Missing 2 5 0.615
3 Poor oral hygiene 3 3
Moderate oral hygiene 4 6
Good oral hygiene 15 14
Missing 2 3 0.678
4 Poor oral hygiene 2 2
Moderate oral hygiene 5 6
Good oral hygiene 16 11
Missing 1 7 0.464
5 Poor oral hygiene 1 2
Moderate oral hygiene 5 6
Good oral hygiene 16 11
Missing 2 7 0.149
6 Poor oral hygiene 1 3
Moderate oral hygiene 2 6
Good oral hygiene 16 11
Missing 5 6 0.450
Bergh, Bart vd.indd 72 23-10-15 16:35

Screws or arch bars?
73
5
Intra-operative complicationsEight needlestick injuries occurred, all in the arch bars group (eight out of 26 patients; 30.7%). No needlestick injuries were observed in the IMFS group (0%; p = 0.003). One IMF screw fractured on insertion (0.53%), distally in the right side of the mandible (fi g. 1a and b). One (0.53%) screw was inserted in a root (fi g. 2). During a follow up period of three years, this premolar remained asymptomatic and sensible to pulp-testing, and did not need endodontic treatment. Placement of screws did not lead to loss of teeth or bony sequestra around the area of screw placement.
Fig. 1 A) An orthopantomogram is presented of a patient treated with IMF screws for a bilateral condylar fracture. A remnant of a fractured screw can be observed in the apical region of element 46.
Fig. 1 B) Occlusal view of the same remnant of the fractured screw.
Bergh, Bart vd.indd 73 23-10-15 16:35
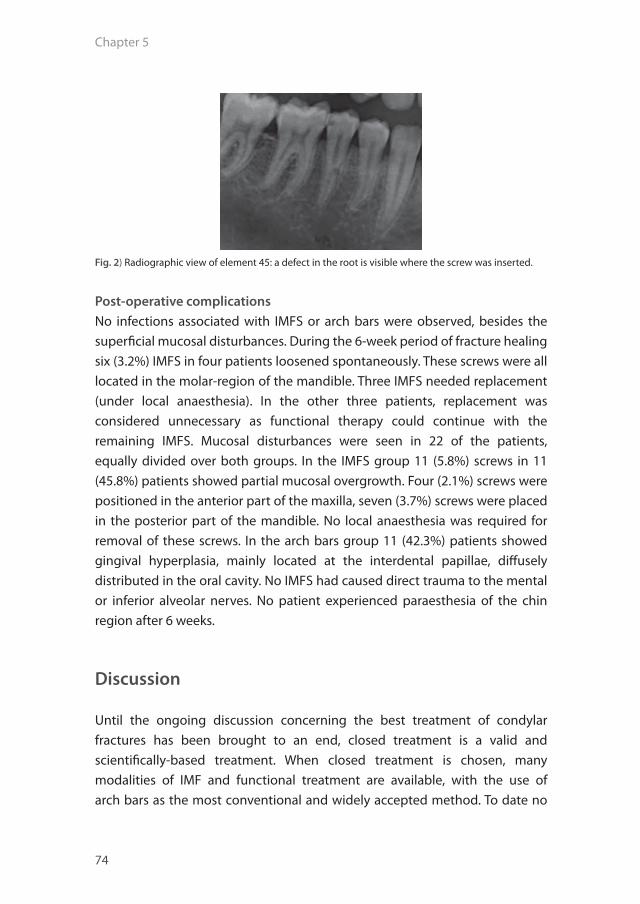
Chapter 5
74
Fig. 2) Radiographic view of element 45: a defect in the root is visible where the screw was inserted.
Post-operative complicationsNo infections associated with IMFS or arch bars were observed, besides the superficial mucosal disturbances. During the 6-week period of fracture healing six (3.2%) IMFS in four patients loosened spontaneously. These screws were all located in the molar-region of the mandible. Three IMFS needed replacement (under local anaesthesia). In the other three patients, replacement was considered unnecessary as functional therapy could continue with the remaining IMFS. Mucosal disturbances were seen in 22 of the patients, equally divided over both groups. In the IMFS group 11 (5.8%) screws in 11 (45.8%) patients showed partial mucosal overgrowth. Four (2.1%) screws were positioned in the anterior part of the maxilla, seven (3.7%) screws were placed in the posterior part of the mandible. No local anaesthesia was required for removal of these screws. In the arch bars group 11 (42.3%) patients showed gingival hyperplasia, mainly located at the interdental papillae, diffusely distributed in the oral cavity. No IMFS had caused direct trauma to the mental or inferior alveolar nerves. No patient experienced paraesthesia of the chin region after 6 weeks.
Discussion
Until the ongoing discussion concerning the best treatment of condylar fractures has been brought to an end, closed treatment is a valid and scientifically-based treatment. When closed treatment is chosen, many modalities of IMF and functional treatment are available, with the use of arch bars as the most conventional and widely accepted method. To date no
Bergh, Bart vd.indd 74 23-10-15 16:35
Screws or arch bars?
75
5
randomised clinical trials have been published in which IMFS and arch bars are compared for the closed treatment of condylar fractures.Rai et al. (2011) reported on the treatment of minimally displaced favourable fractures of both the mandible and maxilla with IMFS (n = 60) or arch bars (n = 30). This research already disclosed the many advantages of IMFS: easy and quick to use, and better oral hygiene maintenance. However, for long-term IMF (5–6 weeks), these authors prefer the use of arch bars, without mentioning the reason of this statement.West et al. (2014) recently published a prospective study involving 20 patients with uncomplicated favourable mandibular fractures in which condylar fractures were excluded. In this study ORIF (n = 11) was compared with closed reduction (n = 9), in both groups IMFS were used. These authors concluded in favour of ORIF because of signifi cant screw failure and patient noncompliance. This supports the opinion of West et al. that IMFS are not reliable to provide suffi cient stability up to 5–6 weeks.In our study, the results, comprising the perioperative elements (e.g. time of surgery, time of application, needlestick injuries) and post-operative elements (e.g. pain, occlusion), were mostly in favour of IMFS.All pain-scores (including the average pain over the week and pain when removing IMF-fi xing) were lower in the IMFS group compared with the arch bars group. Lower pain scores with the use of IMFS, especially in the initial 3 days in which the impact of trauma and surgery itself causes much inconvenience and stress, may lead to a reduction of these latter aspects. Remarkably, when patients were asked on day 3 and 7 about pain changes in comparison with the fi rst two days, they did not rate the pain as signifi cantly diff erent. An explanation for this contradictory phenomenon could be that patients fi nd it diffi cult to recall their pain scores 3 and 7 days afterwards. The investigation of pain scores hasn’t been described in available literature, therefore these results are unique.With regard to occlusion, the use of IMFS leads to the same favourable occlusal results as arch bars. Three patients developed a suboptimal occlusion: one patient was treated with IMFS, and two patients were treated with arch bars. Two of these three patients were treated for a bilateral condylar fracture, one from each group. In total, nine patients were treated for bilateral condylar fractures, therefore 22% of this subgroup resulted in the development of an open bite. This is higher than the percentages available in the literature 7, although the sample size was relatively small.
Bergh, Bart vd.indd 75 23-10-15 16:35

Chapter 5
76
Concerning the surgical treatment time, the use of IMFS leads to a shorter duration of surgery (in average 67 min shorter, p <0.001). Application of IMFS was 52 min shorter than applying arch bars (p <0.001). This is in accordance with other studies.21,27 Although not investigated in this trial, the shorter duration of surgery will probably lead to lower costs. West et al. (2014) estimated total cost savings of $661 per patient with the use of IMFS. Regardless of the costs, one can discuss the negative effect or increased risks of longer general anaesthetic to the patients’ health. At this point, opposed to general anaesthesia, it is worth mentioning that IMFS are easily applied under local anaesthetic. The authors assume that this could lead to a decreased use of general anaesthesia and theatre time, and therefore lower costs.From the surgeons’ point of view the use of IMFS is significantly safer. In this trial eight (30.7%) needlestick injuries were observed, all accidents occurred during the application of arch bars (p = 0.003). Rai et al. reported an incidence of glove perforation of 36.66%.Concerning the risk of damaging teeth due to the use of IMFS, West et al. (2014) reported 14% of the IMFS were penetrating roots, but concluded that no discernible root defects were noted. In relation to this subject, Rai et al. (2011) report teeth damage in 5.81% of the patients. Endodontic treatment was not indicated as all injured teeth remained asymptomatic and sensible on pulp tests. In our study one (0.53%) root was affected caused by the insertion of an IMFS, again no further treatment was indicated. This is a small percentage compared with available retrospective studies and case reports.11,22
Considering screw failures, one screw fracture was observed out of 188 screws (0.53%). This low incidence is in accordance with other studies (0–4%)6,21,22 Six (3.2%) screws loosened spontaneously during the follow up period of six weeks. This is remarkably lower when compared with international literature, in which percentage rates of between 10.4% and 24% are reported.11,21,27 For this reason the authors disagree with the conclusion of Rai et al. and West et al. that long term IMF with IMFS is not reliable. West et al. calculated that a posterior jaw location is a significant factor in failure of screws. This factor is confirmed by the results observed in our study, in which all six loosened screws were initially placed in the molar region of the mandible.Concerning oral mucosal damage this was observed in 22 patients, equally distributed over both groups. In the arch bars group 11 patients presented with gingival hyperplasia of the interdental papillae. In the IMFS group
Bergh, Bart vd.indd 76 23-10-15 16:35

Screws or arch bars?
77
5
partial mucosal overgrowth of 11 (5.9%) screws in 11 patients was seen. Rai et al. reported a total of 92 (38.3%) screws partially or totally covered with mucosa out of 240 screws. The authors attributed this high percentage to the placement of the IMFS in alveolar mucosa rather than in attached mucosa. Placement apically in the alveolar mucosa was mandatory as the investigated population had high levels of periodontal disease activity and concomitant alveolar bone loss. The results in the present study show equal amounts of mucosal disturbances in both groups.With regard to compliance, three patients dropped out: two patients were lost to follow up, and one patient could not fulfi l the 6 weeks follow up period. These three patients were all treated with arch bars, and statistically a trend could be observed (p = 0.086). The arch bars cannot be blamed for this higher dropout percentage as trauma patients in general are known for a higher rate of noncompliance.West et al. advise not to use IMFS in noncompliant patients. In their study seven (out of 22) screws failed because patients removed the screws, and three patients cut their wires themselves. In our study no evidence could be found regarding noncompliance to care, although it was notable that three screws failed in one patient and needed replacement.Although not investigated, it is expected that the use of IMFS will lead to a higher quality of life and lower costs. These latter assumptions, however, need to be investigated in future studies.
Conclusion
Considering the advantages and the disadvantages of IMFS, and observing the results of this study, the authors conclude that IMFS are a superior method to apply IMF. IMFS lead to less pain, the same occlusal results, a shorter operation time, better opportunities for treatment under local anaesthesia and fewer needlestick injuries. IMFS are safer for patients and surgeons.
Bergh, Bart vd.indd 77 23-10-15 16:35

Chapter 5
78
References
1. Arthur G, Berardo N. A simplified technique of maxillomandibular fixation. J Oral Maxillofac Surg 1989;47(11):1234.
2. Bhagol A, Singh V, Kumar I, Verma A. Prospective evaluation of a new classification system for the management of mandibular subcondylar fractures. J Oral Maxillofac Surg 2011;69(4):1159-65.
3. Bormann KH, Wild S, Gellrich NC, Kokemuller H, Stuhmer C, Schmelzeisen R, et al. Five-year retrospective study of mandibular fractures in Freiburg, Germany: incidence, etiology, treatment, and complications. J Oral Maxillofac Surg 2009;67(6):1251-5.
4. Chen CT, Feng CH, Tsay PK, Lai JP, Chen YR. Functional outcomes following surgical treatment of bilateral mandibular condylar fractures. Int J Oral Maxillofac Surg 2011;40(1):38-44.
5. Coburn DG, Kennedy DW, Hodder SC. Complications with intermaxillary fixation screws in the management of fractured mandibles. Br J Oral Maxillofac Surg 2002;40(3):241-3.
6. Coletti DP, Salama A, Caccamese JF,Jr. Application of intermaxillary fixation screws in maxillofacial trauma. J Oral Maxillofac Surg 2007;65(9):1746-50.
7. Forouzanfar T, Lobbezoo F, Overgaauw M, de Groot A, Kommers S, van Selms M, et al. Long-term results and complications after treatment of bilateral fractures of the mandibular condyle. Br J Oral Maxillofac Surg 2013;51(7):634-8.
8. Gerlach KL, Schwarz A. Bite forces in patients after treatment of mandibular angle fractures with miniplate osteosynthesis according to Champy. Int J Oral Maxillofac Surg 2002;31(4):345-8.
9. Gordon KF, Reed JM, Anand VK. Results of intraoral cortical bone screw fixation technique for mandibular fractures. Otolaryngol Head Neck Surg 1995;113(3):248-52.
10. Gupta M, Iyer N, Das D, Nagaraj J. Analysis of different treatment protocols for fractures of condylar process of mandible. J Oral Maxillofac Surg 2012;70(1):83-91.
11. Hashemi HM, Parhiz A. Complications using intermaxillary fixation screws. J Oral Maxillofac Surg 2011;69(5):1411-4.
12. Ho KS, Tan WK, Loh HS. Case reports: the use of intermaxillary screws to achieve intermaxillary fixation in the treatment of mandibular fractures. Ann Acad Med Singapore 2000;29(4):534-7.
13. Jones DC. The intermaxillary screw: a dedicated bicortical bone screw for temporary intermaxillary fixation. Br J Oral Maxillofac Surg 1999;37(2):115-6.
14. Laurentjoye M, Majoufre-Lefebvre C, Siberchicot F, Ricard AS. Result of maxillomandibular fixation using intraoral cortical bone screws for condylar fractures of the mandible. J Oral Maxillofac Surg 2009;67(4):767-70.
15. Marker P, Nielsen A, Bastian HL. Fractures of the mandibular condyle. Part 2: results of treatment of 348 patients. Br J Oral Maxillofac Surg 2000;38(5):422-6.
16. Motamedi MH. An assessment of maxillofacial fractures: a 5-year study of 237 patients. J Oral Maxillofac Surg 2003;61(1):61-4.
17. Niezen ET, Bos RR, de Bont LG, Stegenga B, Dijkstra PU. Complaints related to mandibular function impairment after closed treatment of fractures of the mandibular condyle. Int J Oral Maxillofac Surg 2010;39(7):660-5.
18. Onishi K, Maruyama Y. Simple intermaxillary fixation for maxillomandibular osteosynthesis. J Craniofac Surg 1996;7(2):170-2.
19. Palmieri C, Ellis E,3rd, Throckmorton G. Mandibular motion after closed and open treatment of unilateral mandibular condylar process fractures. J Oral Maxillofac Surg 1999;57(7):764,75; discussion 775-6.
20. Park JM, Jang YW, Kim SG, Park YW, Rotaru H, Baciut G, et al. Comparative study of the prognosis of an extracorporeal reduction and a closed treatment in mandibular condyle head and/or neck fractures. J Oral Maxillofac Surg 2010;68(12):2986-93.
21. Rai A, Datarkar A, Borle RM. Are maxillomandibular fixation screws a better option than Erich arch bars in achieving maxillomandibular fixation? A randomized clinical study. J Oral Maxillofac Surg 2011;69(12):3015-8.
Bergh, Bart vd.indd 78 23-10-15 16:35
Screws or arch bars?
79
5
22. Roccia F, Tavolaccini A, Dell’Acqua A, Fasolis M. An audit of mandibular fractures treated by intermaxillary fi xation using intraoral cortical bone screws. J Craniomaxillofac Surg 2005;33(4):251-4.
23. Schneider AM, David LR, DeFranzo AJ, Marks MW, Molnar JA, Argenta LC. Use of specialized bone screws for intermaxillary fi xation. Ann Plast Surg 2000;44(2):154-7.
24. Sharif MO, Fedorowicz Z, Drews P, Nasser M, Dorri M, Newton T, et al. Interventions for the treatment of fractures of the mandibular condyle. Cochrane Database Syst Rev 2010;(4):CD006538. doi(4):CD006538.
25. Silvennoinen U, Raustia AM, Lindqvist C, Oikarinen K. Occlusal and temporomandibular joint disorders in patients with unilateral condylar fracture. A prospective one-year study. Int J Oral Maxillofac Surg 1998;27(4):280-5.
26. van den Bergh B, Heymans MW, Duvekot F, Forouzanfar T. Treatment and complications of mandibular fractures: a 10-year analysis. J Craniomaxillofac Surg 2012;40(4):e108-11.
27. West GH, Griggs JA, Chandran R, Precheur HV, Buchanan W, Caloss R. Treatment outcomes with the use of maxillomandibular fi xation screws in the management of mandible fractures. J Oral Maxillofac Surg 2014;72(1):112-20.
28. Yang WG, Chen CT, Tsay PK, Chen YR. Functional results of unilateral mandibular condylar process fractures after open and closed treatment. J Trauma 2002;52(3):498-503.
29. Zachariades N, Mezitis M, Mourouzis C, Papadakis D, Spanou A. Fractures of the mandibular condyle: a review of 466 cases. Literature review, refl ections on treatment and proposals. J Craniomaxillofac Surg 2006;34(7):421-32.
30. Chrcanovic BR. Surgical versus non-surgical treatment of mandibular condylar fractures: a meta-analysis. Int J Oral Maxillofac Surg 2015;44:158-79.
31. Al-Moraissi EA, Ellis E 3rd. Surgical treatment of adult mandibular condylar fracturesprovides better outcomes than closed treatment: a systematic review and meta-analysis. J Oral Maxillofac Surg 2015;73:1482-493.
Bergh, Bart vd.indd 79 23-10-15 16:35
Bergh, Bart vd.indd 80 23-10-15 16:35

Chapter 6:
“IMF screws or arch bars for closed treatment of mandibular condyle fractures: the quality of
life-aspects.”
This is an edited version of the manuscript: B. van den Bergh, J.J. de Mol van Otterloo, T. van der Ploeg, D.B. Tuinzing, T. Forouzanfar. IMF-screws or arch bars as conservative treatment
for mandibular condyle fractures: the quality of life-aspects. Journal of Cranio-Maxillo-Facial Surgery 2015 Sep;43(7): 1004-9.
Bergh, Bart vd.indd 81 23-10-15 16:35

Chapter 6
82
Abstract
Introduction: Arch bars as treatment for a fractured mandibular condyle are inconvenient to patients and lead to lowered quality of life (QOL). To overcome arch bars-related inconvenience, IMF screws (IMFS) were developed. The purpose of the present study is to investigate and compare QOL for patients treated for a fractured mandibular condyle with either IMFS or arch bars.
Results: In total 50 patients were included: 30 (60%) male patients and 20 (40%) female patients (mean age: 31.8 yrs, SD 13.9 yrs, range 18-64 yrs). Twenty-four (48%) patients were allocated in the IMFS-group. Twenty-six (52%) patients were assigned to the arch bars-control group. Significant results were observed in the subscales social isolation, possibility to eat and vary diet, influence on sleep and satisfaction with the given treatment, all in favour of IMFS.
Conclusion: In conclusion, using IMFS as a method for closed treatment of condylar fractures leads to a higher QOL during the six-week period of fracture healing. In comparison to arch bars, patients treated with IMFS experienced less social isolation, experience less problems with eating and express the feeling they are able to continue their normal diet. Furthermore it seems that the use of IMFS has a lower negative impact on social and financial aspects of the patient.
Bergh, Bart vd.indd 82 23-10-15 16:35

Quality of life
83
6
Introduction
Over the last decades, particularly in the fi eld of healthcare, quality of life (QOL)-aspects have been given increasingly more attention. Patients are better informed about the diff erent treatment modalities and their potential social and physical impacts on their daily lives because of the internet, television and newspapers.While QOL has gained popularity in general healthcare, few publications can be found regarding QOL in relation to maxillofacial surgery. Most studies describe QOL in relation to chronic diseases 5,11,15, oncology 4,7 and dento-alveolar surgery.1,9 To date little can be found on QOL and maxillofacial trauma. One publication reported that in patients with facial trauma lowered health-related QOL increased the risk of developing depression, regardless of the cause of trauma.3 Another publication found increased depressive symptoms associated with QOL in patients with mandibular fractures.13 Only three studies have investigated subjective discomfort for condylar fractures.2,8,10 However, Kommers et al. consider that these studies examined the QOL aspects superfi cially and that the results were contradictory.6
Zachariades reports that the treatment-related use of arch bars is inconvenient to the patient and that they might have a negative impact on QOL.16 To overcome arch bars-related inconvenience, IMF screws (IMFS) were developed to facilitate the application of intermaxillary fi xation during surgery. Recently Van den Bergh compared IMF screws to arch-bars for application of IMF in mandibular condyle fractures. Both methods have their treatment-related complications (table 1). Of note the use IMF screws led to less pain, shorter duration of surgery, and favourable occlusal results compared to the use of arch bars. Therefore IMF screws are concluded to be a superior treatment-method compared to the use of arch bars.14
Table 1. Overview of (treatment-related) complications.
Type of complication Arch bars IMF screws
Needlestick injuries 8 0
Fracture of an IMF screw on insertion n.a. 1
IMF screws inserted in a root n.a. 1
Mucosal disturbances 11 11
Bergh, Bart vd.indd 83 23-10-15 16:35

Chapter 6
84
The purpose of the present study is to investigate and compare QOL for patients treated for a fractured mandibular condyle with either IMFS or arch bars.
Material and Methods
This research trial was conducted between May 2010 and July 2014, and is part of an earlier submitted prospective multi-centre randomised clinical trial in which the use of IMFS was compared to the use of arch bars in the treatment of mandibular condylar fractures.14 In this study the IMFS were concluded as a superior method to apply IMF compared to arch bars.Patients were eligible when aged between 18 and 65 years, when given signed informed consent and needed treatment for a fractured mandibular condyle (with or without concomitant mandibular fractures). The study protocol was approved by the Ethics Committee of the VU University Medical Center Amsterdam and Medical Centre Alkmaar (reg. nr. NL28831.029.09; 2009/311).Exclusion criteria included: inability to give informed consent, known chronic pain syndrome, mental retardation or psychiatric abnormalities, concomitant maxillary or other facial fractures and known malignant disease. All patients provided signed informed consent before surgical treatment.
Study protocolAfter giving consent patients were randomised by an assignment scheme that was generated from a table of random numbers. This table was developed, using a computer program developed for randomisation purposes. Randomisation was to either the IMFS study group or arch bars control group. Trial participants were blinded to group allocation until the end of the operation.
ProcedureThe IMFS were placed in the interproximal or edentulous spaces at the muco-gingival junction. Screw insertion site was based on clinical and radiographic information. IMF was established by stainless steel wires through/around the placed screws in maxilla and mandible. The arch bars were fixed by stainless steel wires around teeth from the cusp to the second molar (if available). IMF was established by fixating the mandible against the maxilla with stainless
Bergh, Bart vd.indd 84 23-10-15 16:35

Quality of life
85
6
steel wires around the cleats of the arch bars. If fi xation of the body of the mandible was necessary, 2.0 mm plates were used.
Follow upThe post-operative follow up was similar to the treatment protocol for mandibular fractures as used in our department, i.e. every week post-operatively during 6 weeks. At post-operative week 1, 3 and 6, when visiting the outpatient clinic, patients were asked to fi ll out a questionnaire concerning the QOL. Evaluation was done by self-report using a validated Dutch questionnaire regarding daily activities, based on the English questionnaire designed by Savin and Ogden.9 The following subscales were obtained: social isolation, isolation from work, possibility to eat and vary diet, possibility to speak, infl uence on sleep, facial appearance and satisfaction with the given treatment (fi gure 1). The questionnaire contains closed questions (to be answered with dichotomous ‘yes’ or ‘no’), open questions (that can be answered with a continuous answer, for example: “for how many days...?”) and open questions (that can be answered nominally on the 4-step Likert scale: ‘not at all / a little / quite a lot / very much’).
Statistical analysisDichotomous measures per week (e.g. answers on closed questions) with respect to the groups were tested using Chi-square tests. Continuous and ordinal measures per week (for example, ‘for how many days did you stop working?’ or ‘did you continue your normal diet?’) with respect to the groups were tested using a Mann-Whitney U-test. Ordinal and continuous variables were presented as mean and standard deviation, whereas dichotomous variables were presented as percentages.For the analysis the IBM Statistical Package SPSS version 22.0.0 was used. P-values less than 0.05 were considered as signifi cant.
Bergh, Bart vd.indd 85 23-10-15 16:35

Chapter 6
86
Figure 1. Quality of life – questionnaireSocially isolated1a. Did you continue your normal daily activities? Yes / No1b. Did you continue your daily sports activities and hobbies? Yes / No
Give the reason for social isolation1c. Pain and/or swelling Yes / No1d. Appearance Yes / No1e. Bad mood Yes / No1f. discomfort (flu-like) Yes / No
Isolation of work2a. Did you ask for sick leave or did you temporarily stopped working? Yes / No2b. If you did stop working, for how many days? ……… 2c. Did your operation influence your work? Yes / No2d. Did someone accompany you? Yes / No2e. This person cancelled his or her job to accompany you? Yes / No
Ability to eat and vary diet3a. Did you continue your normal diet? not at all / a little /
quite a lot / very much3b. Did you notice difference in your ability to taste/taste perception? not at all / a little /
quite a lot / very much3c. If you experienced problems with eating, for how many days ? ………
Ability to speak4a. Did you notice difference in your voice? not at all / a little /
quite a lot / very much4b. Did you notice any difference in your ability to speak? not at all / a little /
quite a lot / very much4c. When you speak to others, do they understand you? not at all / a little /
quite a lot / very much4d. In case you noticed any differences, for how many days did you notice this? …….
Influence on sleep5a. Did you experience problems falling asleep? not at all / a little /
quite a lot / very much5b. Did you experience interruptions during your sleep? not at all / a little /
quite a lot / very much5c. Was your sleep refreshing? not at all / a little /
quite a lot / very much5d. When your sleep was affected, for how many days? ……..5e. Did you experience a dazed feeling/sensitation? Yes / No
Appearance6a. Did you experience any change in appearance? not at all / a little /
quite a lot / very much6b. Did you expect this appearance? not at all / a little /
quite a lot / very much6c. How many days did the change in appearance last? ……
Satisfaction with the given treatment7a. Are you satisfied with your treatment? Yes / No7b. Would you recommend this treatment to someone else? Yes / No7c. Would you undergo the same treatment again? Yes / No7d. Do you think the problem that needed treatment, is solved? Yes / No
Bergh, Bart vd.indd 86 23-10-15 16:35

Quality of life
87
6
Results
In total 50 patients were included: 30 (60%) male patients and 20 (40%) female patients (mean age: 31.8 yrs, SD 13.9 yrs, range 18-64 yrs). Seven (14%) patients were treated for a solitary condyle fracture, 34 (68%) patients had a concomitant mandibular fracture, 2 (4%) patients were treated for a bilateral condyle fracture and 7 (14%) patients had a bilateral condyle fracture combined with another mandibular fracture. Twenty-four (48%) patients were allocated in the study group (IMFS). Twenty-six (52%) patients were assigned to the control group (arch bars). For 3 patients the follow up results were not available (3 of 50 patients: 6% dropout). These 3 patients were treated with arch bars (3 of 26 patients: 11.5%, p=0.086).The randomisation procedure was checked by comparing the groups for relevant variables. Both groups did not diff er signifi cantly when observing gender, age, smoking habit, presence of diastemata, presence of hematoma in the fl oor of the mouth, loss of or altered sensitivity of the lower lip, presence of deviation of the mandible, posttraumatic maximal mouth opening, cause of trauma, impact, nature and side of impact, type of fracture and side of condylar fracture (all p-values >0.05).The outcomes of the comparison of QOL per week for dichotomous variables are outlined in table 2. In week 1 96% of the IMFS-patients would recommend their treatment to someone else versus 61% of the arch bars-patients (question 7b, p = 0.004). A trend was observed at question 2e: 36% of the arch bars-patients were accompanied by someone who took time off from work for their visit to the outpatient clinic against 13% of the IMFS-patient (p = 0.069).In week 3 again question 7b appeared signifi cant: 100% of the IMFS patients would recommend the treatment against 65% of the arch bars-patients (p = 0.002).
Bergh, Bart vd.indd 87 23-10-15 16:35

Chapter 6
88
In week 6 questions 1a, 5e and 7b showed significant differences. Of the IMFS-patients 91% had the feeling they could continue their normal daily activities versus 59% of the arch bars-patients (question 1a, p = 0.012). A dazed feeling/sensitation was experienced by 41% of the arch bars-patients and 9% of the IMFS-patients (p = 0.012). Question 7b showed significant differences, conform week 1 and 3 (p = 0.007). The differences for both groups at question 1b and 1c were almost significant (respectively p = 0.095 and p = 0.088).For continuous and ordinal variables, the outcomes are outlined in tables 3a (week 1), 3b (week 3) and 3c (week 6). An overview of the p-values is given in table 3d. In week 1 question 3a (“Did you continue your normal diet?”) a mean value of 0.6 was observed for the IMFS-group (SD 0.9) against a mean value of 0.1 observed for the arch bars-group (SD 0.3, p = 0.013). IMFS-patients experienced significantly less problems falling asleep (mean 0.9, SD 0.7) in comparison with arch bars-patients (mean 1.4, SD 0.8, p = 0.028). A trend was observed at question 3c (IMFS: mean 3.8, SD 3.1 versus arch bars: mean 5.5, SD 2.2, p = 0.080).
Bergh, Bart vd.indd 88 23-10-15 16:35

Quality of life
89
6
Tabl
e 2.
Com
paris
on o
f qua
lity
of li
fe-a
spec
ts fo
r dic
hoto
mou
s var
iabl
es (I
MFS
vs.
arch
bar
s per
wee
k).
wee
k 1
wee
k 3
wee
k 6
perc
enta
ges
p-va
lue
perc
enta
ges
p-va
lue
perc
enta
ges
p-va
lue
Soci
ally
isol
ated
:1a
. Did
you
con
tinue
you
r nor
mal
dai
ly a
ctiv
ities
?1b
. Did
you
con
tinue
you
r dai
ly sp
orts
act
iviti
es a
nd h
obbi
es?
39%
vs.
26%
13%
vs.
9%0.
345
0.63
678
% v
s. 57
%26
% v
s. 35
%0.
116
0.52
291
% v
s. 59
%57
% v
s. 32
%0.
012*
0.09
5^
Giv
e th
e re
ason
for s
ocia
l iso
latio
n:1c
. Pai
n an
d/or
swel
ling
1d. A
ppea
ranc
e 1e
. Bad
moo
d1f
. disc
omfo
rt (fl
u-li
ke)
61%
vs.
78%
35%
vs.
26%
17%
vs.
26%
13%
vs.
17%
0.20
00.
522
0.47
50.
681
17%
vs.
23%
26%
vs.
9%13
% v
s. 9%
9% v
s. 9%
0.65
50.
136
0.63
70.
963
9% v
s. 29
%17
% v
s. 5%
4% v
s. 14
%0%
vs.
1%
0.08
8^0.
187
0.25
20.
290
Isol
atio
n of
wor
k:2a
. Did
you
ask
for s
ick
leav
e or
did
you
tem
pora
rily
stop
ped
wor
king
? 2c
. Did
you
r ope
ratio
n in
fl uen
ce y
our w
ork?
2d. D
id so
meo
ne a
ccom
pany
you
?2e
. Thi
s per
son
canc
elle
d hi
s or h
er jo
b to
acc
ompa
ny y
ou?
78%
vs.
91%
70%
vs.
87%
78%
vs.
65%
13%
vs.
36%
0.21
80.
153
0.32
6 0
.069
^
83%
vs.
70%
74%
vs.
83%
52%
vs.
55%
4% v
s. 9%
0.30
00.
475
0.87
30.
524
61%
vs.
55%
52%
vs.
59%
35%
vs.
33%
0% v
s. 2%
0.66
80.
641
0.91
90.
130
Slee
ping
beh
avio
ur:
5e. D
id y
ou e
xper
ienc
e a
daze
d fe
elin
g/se
nsita
tion?
65%
vs.
68%
0.83
344
% v
s. 52
%0.
555
9% v
s. 41
% 0
.012
*
Satis
fact
ion
with
the
give
n tr
eatm
ent:
7a. A
re y
ou sa
tisfi e
d w
ith y
our t
reat
men
t?7b
. Wou
ld y
ou re
com
men
d th
is tr
eatm
ent t
o so
meo
ne e
lse?
7c. W
ould
you
und
ergo
the
sam
e tr
eatm
ent a
gain
?7d
. Do
you
thin
k th
e pr
oble
m th
at n
eede
d tr
eatm
ent,
is so
lved
?
100%
vs.
96%
96%
vs.
61%
64%
vs.
61%
96%
vs.
87%
0.31
2 0
.004
*0.
848
0.31
7
100%
vs.
100%
100%
vs.
65%
65%
vs.
61%
91%
vs.
91%
1.00
0 0
.002
*0.
760
1.00
0
100%
vs.
100%
100%
vs.
73%
87%
vs.
68%
100%
vs.
96%
1.00
00.
007*
0.13
00.
301
Chi-s
quar
e te
st p
erfo
rmed
, per
cent
ages
of p
atie
nts t
hat a
nsw
ered
‘yes
’ (IM
FS v
s. ar
ch b
ars,
p-va
lue)
, * =
sign
ifi ca
nt (p
-val
ue <
0.0
5), ^
= tr
end
(0.0
5 <
p-va
lue
< 0.
10)
Bergh, Bart vd.indd 89 23-10-15 16:35

Chapter 6
90
Table 3a. Comparison of quality of life-aspect of IMF screws group and arch bars group, for continuous and ordinal variables (week 1).
Number Question IMF screwsMean (SD
and range)
Arch barsMean (SD and
range)
p-value
2b If you did stop working, for how many days? 5.0 (3.0, 0-7) 5.0 (2.5, 0-7) 0.542
3a Did you continue your normal diet? 0.6 (0.9, 0-3) 0.1 (0.3, 0-1) 0.013*
3b Did you notice difference in your ability to taste/taste perception?
0.7 (0.8, 0-3) 1.0 (1.3, 0-3) 0.592
3c If you experienced problems with eating, for how many days ?
3.8 (3.1, 0-7) 5.5 (2.2, 0-7) 0.080^
4a Did you notice difference in your voice? 1.0 (0.9, 0-3) 1.2 (1.2, 0-3) 0.697
4b Did you notice any difference in your ability to speak?
2.2 (0.8, 1-3) 1.8 (1.0, 0-3) 0.235
4c When you speak to others, do they understand you?
1.9 (0.7, 1-3) 2.0 (0.8, 0-3) 0.591
4d In case you noticed any differences, for how many days did you notice this?
4.8 (3.0, 0-7) 4.5 (2.8, 0-7) 0.455
5a Did you experience problems falling asleep? 0.9 (0.7, 0-2) 1.4 (0.8, 0-3) 0.028*
5b Did you experience interruptions during your sleep?
1.0 (0.9, 0-3) 1.3 (0.9, 0-3) 0.234
5c Was your sleep refreshing? 1.7 (0.8, 0-3) 1.4 (0.9, 0-3) 0.270
5d When your sleep was affected, for how many days?
3.0 (3.1, 0-7) 4.1 (2.9, 0-7) 0.246
6a Did you experience any change in appearance? 1.4 (0.9, 0-3) 1.7 (1.0, 0-3) 0.343
6b Did you expect this appearance? 1.4 (0.6, 0-2) 1.5 (1.1, 0-3) 0.718
6c How many days did the change in appearance last?
4.4 (2.9, 0-7) 4.6 (2.6, 0-7) 0.860
Mann-Whitney U test performed, * = significant (p-value < 0.05), ^ = trend (0.05 < p-value < 0.10)
Bergh, Bart vd.indd 90 23-10-15 16:35
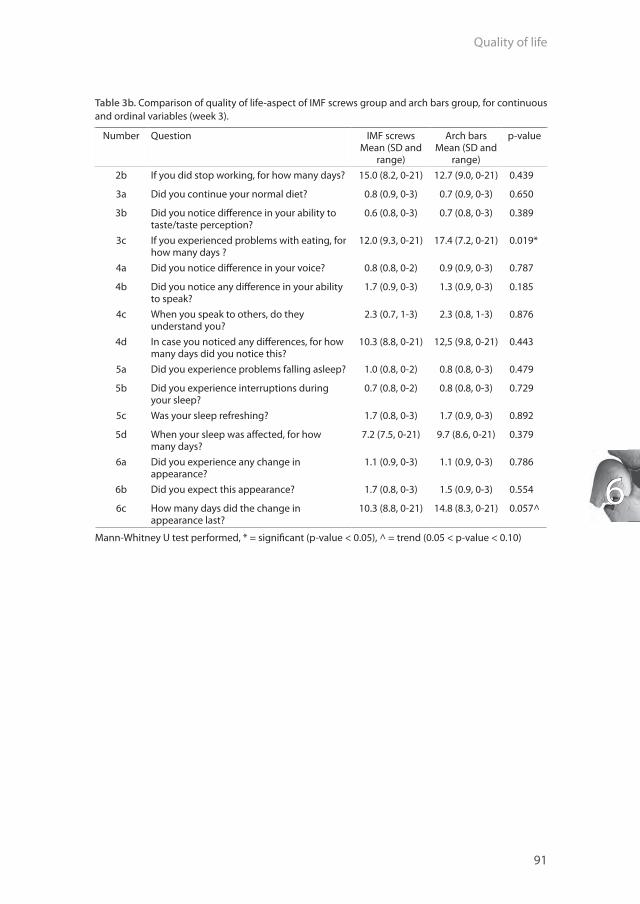
Quality of life
91
6
Table 3b. Comparison of quality of life-aspect of IMF screws group and arch bars group, for continuous and ordinal variables (week 3).
Number Question IMF screwsMean (SD and
range)
Arch barsMean (SD and
range)
p-value
2b If you did stop working, for how many days? 15.0 (8.2, 0-21) 12.7 (9.0, 0-21) 0.439
3a Did you continue your normal diet? 0.8 (0.9, 0-3) 0.7 (0.9, 0-3) 0.650
3b Did you notice diff erence in your ability to taste/taste perception?
0.6 (0.8, 0-3) 0.7 (0.8, 0-3) 0.389
3c If you experienced problems with eating, for how many days ?
12.0 (9.3, 0-21) 17.4 (7.2, 0-21) 0.019*
4a Did you notice diff erence in your voice? 0.8 (0.8, 0-2) 0.9 (0.9, 0-3) 0.787
4b Did you notice any diff erence in your ability to speak?
1.7 (0.9, 0-3) 1.3 (0.9, 0-3) 0.185
4c When you speak to others, do they understand you?
2.3 (0.7, 1-3) 2.3 (0.8, 1-3) 0.876
4d In case you noticed any diff erences, for how many days did you notice this?
10.3 (8.8, 0-21) 12,5 (9.8, 0-21) 0.443
5a Did you experience problems falling asleep? 1.0 (0.8, 0-2) 0.8 (0.8, 0-3) 0.479
5b Did you experience interruptions during your sleep?
0.7 (0.8, 0-2) 0.8 (0.8, 0-3) 0.729
5c Was your sleep refreshing? 1.7 (0.8, 0-3) 1.7 (0.9, 0-3) 0.892
5d When your sleep was aff ected, for how many days?
7.2 (7.5, 0-21) 9.7 (8.6, 0-21) 0.379
6a Did you experience any change in appearance?
1.1 (0.9, 0-3) 1.1 (0.9, 0-3) 0.786
6b Did you expect this appearance? 1.7 (0.8, 0-3) 1.5 (0.9, 0-3) 0.554
6c How many days did the change in appearance last?
10.3 (8.8, 0-21) 14.8 (8.3, 0-21) 0.057^
Mann-Whitney U test performed, * = signifi cant (p-value < 0.05), ^ = trend (0.05 < p-value < 0.10)
Bergh, Bart vd.indd 91 23-10-15 16:35

Chapter 6
92
Table 3c. Comparison of quality of life-aspect of IMF screws group and arch bars group, for continuous and ordinal variables (week 6).
Number Question IMF screwsMean (SD and
range)
Arch barsMean (SD and
range)
p-value
2b If you did stop working, for how many days?
20.4 (15.6, 0-42) 19.7 (16.9, 0-42) 0.908
3a Did you continue your normal diet? 1.3 (1.0, 0-3) 0.6 (0.7, 0-2) 0.013*
3b Did you notice difference in your ability to taste/taste perception?
0.6 (0.8, 0-3) 0.8 (0.9, 0-3) 0.548
3c If you experienced problems with eating, for how many days ?
16.8 (16.0, 0-42) 29.0 (18.5, 0-42) 0.036*
4a Did you notice difference in your voice? 0.5 (0.7, 0-3) 0.6 (0.7, 0-2) 0.608
4b Did you notice any difference in your ability to speak?
0.8 (0.9, 0-3) 0.9 (0.9, 0-3) 0.865
4c When you speak to others, do they understand you?
2.6 (0.5, 2-3) 2.7 (0.5, 2-3) 0.262
4d In case you noticed any differences, for how many days did you notice this?
15.0 (14.7, 0-42) 19.7 (16.6, 0-42) 0.382
5a Did you experience problems falling asleep?
0.6 (0.7, 0-2) 0.5 (0.7, 0-2) 0.516
5b Did you experience interruptions during your sleep?
0.4 (0.6, 0-2) 0.5 (0.7, 0-2) 0.813
5c Was your sleep refreshing? 1.9 (0.9, 0-3) 2.1 (0.8, 0-3) 0.462
5d When your sleep was affected, for how many days?
6.1 (9.4, 0-42) 13.1 (16.2, 0-42) 0.344
6a Did you experience any change in appearance?
0.9 (0.7, 0-3) 0.9 (0.8, 0-3) 0.735
6b Did you expect this appearance? 1.7 (0.9, 0-3) 1.8 (0.8, 1-3) 0.595
6c How many days did the change in appearance last?
17.2 (17.4, 0-42) 20.2 (17.7, 0-42) 0.692
Mann-Whitney U test performed, * = significant (p-value < 0.05), ^ = trend (0.05 < p-value < 0.10)
Bergh, Bart vd.indd 92 23-10-15 16:35
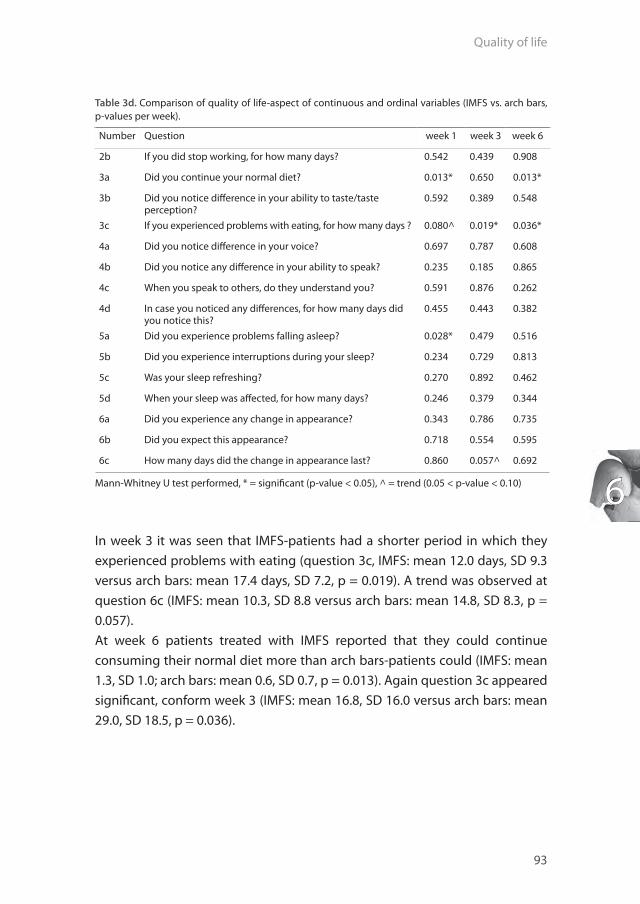
Quality of life
93
6
Table 3d. Comparison of quality of life-aspect of continuous and ordinal variables (IMFS vs. arch bars, p-values per week).
Number Question week 1 week 3 week 6
2b If you did stop working, for how many days? 0.542 0.439 0.908
3a Did you continue your normal diet? 0.013* 0.650 0.013*
3b Did you notice diff erence in your ability to taste/taste perception?
0.592 0.389 0.548
3c If you experienced problems with eating, for how many days ? 0.080^ 0.019* 0.036*
4a Did you notice diff erence in your voice? 0.697 0.787 0.608
4b Did you notice any diff erence in your ability to speak? 0.235 0.185 0.865
4c When you speak to others, do they understand you? 0.591 0.876 0.262
4d In case you noticed any diff erences, for how many days did you notice this?
0.455 0.443 0.382
5a Did you experience problems falling asleep? 0.028* 0.479 0.516
5b Did you experience interruptions during your sleep? 0.234 0.729 0.813
5c Was your sleep refreshing? 0.270 0.892 0.462
5d When your sleep was aff ected, for how many days? 0.246 0.379 0.344
6a Did you experience any change in appearance? 0.343 0.786 0.735
6b Did you expect this appearance? 0.718 0.554 0.595
6c How many days did the change in appearance last? 0.860 0.057^ 0.692
Mann-Whitney U test performed, * = signifi cant (p-value < 0.05), ^ = trend (0.05 < p-value < 0.10)
In week 3 it was seen that IMFS-patients had a shorter period in which they experienced problems with eating (question 3c, IMFS: mean 12.0 days, SD 9.3 versus arch bars: mean 17.4 days, SD 7.2, p = 0.019). A trend was observed at question 6c (IMFS: mean 10.3, SD 8.8 versus arch bars: mean 14.8, SD 8.3, p = 0.057).At week 6 patients treated with IMFS reported that they could continue consuming their normal diet more than arch bars-patients could (IMFS: mean 1.3, SD 1.0; arch bars: mean 0.6, SD 0.7, p = 0.013). Again question 3c appeared signifi cant, conform week 3 (IMFS: mean 16.8, SD 16.0 versus arch bars: mean 29.0, SD 18.5, p = 0.036).
Bergh, Bart vd.indd 93 23-10-15 16:35

Chapter 6
94
Discussion
To the authors’ knowledge the present study is the first investigating QOL for closed treatment of condylar fractures, based on a QOL-questionnaire. Therefore all results are unique, for both IMFS and arch bars.When looking at table 2 it can be noticed that IMFS-patients have the feeling that they can continue their normal daily activities more often than arch bars-patients can (question 1a). In all weeks these percentages are in favour of IMFS-patients, but it appears only to be significant in week 6 (p = 0.012). With regard to question 1b it is seen that a trend was observed in week 6: IMFS-patients tend to continue their daily sports activities and hobbies more when compared to arch bars-patients (p = 0.095). The same trend-phenomenon was found at question 1c in week 6: arch bars-patients give pain and/or swelling as the reason for this isolation (29% compared to 9% of the IMFS-patients, p = 0.088). Questions 1a, 1b and 1c show that IMFS-patients feel less socially isolated when compared to patients treated with arch bars.All patients, treated with either IMFS or arch bars, tend to ask for sick leave or stopped working temporarily, especially in the first week (78% and 91% respectively). At week 6 these percentages are gradually lowered to 61% and 55% respectively, but this did not lead to a significant difference. The same observations were made at question 2c. Of all patients treated with IMFS, 78% were accompanied by someone when visiting the outpatient clinic one week post-operatively, but only 13% of these persons cancelled their job to support the patient. In the control group, 65% of the arch bars patients were accompanied by someone, and a rather high 36% took time off work to accompany the patient. This difference showed a trend (p = 0.069). These findings would imply that treatment with IMFS leads to a lower social and financial impact on the environment of the patient.IMFS-patients have the feeling that they can continue normal diet for the whole six-week period of fracture healing. In week 1 and 6 this differed significantly from arch bars-patients (p = 0.013 and p = 0.013). These results were confirmed by the findings as observed for question 3c: arch bars-patients experience problems with eating for a longer period when compared to IMFS-patients. These differences showed a trend at week 1 (p = 0.080), but were significant in week 3 (p = 0.019) and week 6 (p = 0.036). Although an instruction was given to maintain a strict soft diet, patients treated with IMFS express the feeling that
Bergh, Bart vd.indd 94 23-10-15 16:35

Quality of life
95
6
they were able to continue a normal diet and experience less problems with eating.In the subscale ‘possibility to speak’ no diff erences were observed between both groups (questions 4a-4d). Apparently, IMFS and arch bars aff ected voice and patients’ ability to speak, equally. Furthermore all patients had the feeling that others could understand them when speaking to them.In the fi rst week, arch bars aff ected patients’ falling asleep more when compared to IMFS (p = 0.028). Both groups did not experience diff erences in sleep interruption, and in both groups patients felt that their sleep was refreshing. As most patients did not experience problems with sleeping, question 5d did not apply and no diff erences were observed. In week 6 arch bars-patients more often experienced a dazed feeling/sensitation compared to IMFS-patients (p = 0.012). The authors fi nd it diffi cult to explain this fi nding.No signifi cant diff erences between both groups were seen with regard to appearance (question 6a, 6b and 6c). For all weeks, the mean number of days that patients experienced a change in appearance was higher in the arch bars-group, but these diff erences were not signifi cant.In general, all patients are satisfi ed with the given treatment (question 7a), but IMFS-patients would recommend their treatment to someone else more often than arch bars-patients would. The percentages were signifi cantly higher in all weeks (week 1: p = 0.004; week 3: p = 0.002; week 6: p = 0.007). All patients were of the opinion that the problem that needed treatment, was solved.
Conclusion
In conclusion, using IMFS as a method for closed treatment of condylar fractures leads to a higher QOL during the six-week period of fracture healing. In comparison to arch bars, patients treated with IMFS experienced less social isolation and less problems with eating. Patients treated with IMFS express the feeling they are able to continue their normal diet. Furthermore it seems that the use of IMFS has a lower negative impact on social and fi nancial aspects of the patient.
Bergh, Bart vd.indd 95 23-10-15 16:35

Chapter 6
96
References
1. Bradshaw S, Faulk J, Blakey GH, Phillips C, Phero JA, White RP,Jr. Quality of life outcomes after third molar removal in subjects with minor symptoms of pericoronitis. J Oral Maxillofac Surg 2012;70(11):2494-500.
2. Eckelt U, Schneider M, Erasmus F, Gerlach KL, Kuhlisch E, Loukota R, et al. Open versus closed treatment of fractures of the mandibular condylar process-a prospective randomized multi-centre study. J Craniomaxillofac Surg 2006;34(5):306-14.
3. Gironda MW, Der-Martirosian C, Belin TR, Black EE, Atchison KA. Predictors of depressive symptoms following mandibular fracture repair. J Oral Maxillofac Surg 2009;67(2):328-34.
4. Harding SA, Hodder SC, Courtney DJ, Bryson PJ. Impact of perioperative hyperbaric oxygen therapy on the quality of life of maxillofacial patients who undergo surgery in irradiated fields. Int J Oral Maxillofac Surg 2008;37(7):617-24.
5. Karacayli U, Mumcu G, Cimilli H, Sisman N, Sur H, Gunaydin Y. The effects of chronic pain on oral health related quality of life in patients with anterior disc displacement with reduction. Community Dent Health 2011;28(3):211-5.
6. Kommers SC, van den Bergh B, Forouzanfar T. Quality of life after open versus closed treatment for mandibular condyle fractures: a review of literature. J Craniomaxillofac Surg 2013;41(8):e221-5.
7. Rogers SK, Gomez CF, Carpenter P, Farley J, Holson D, Markowitz M, et al. Quality of life for children with life-limiting and life-threatening illnesses: description and evaluation of a regional, collaborative model for pediatric palliative care. Am J Hosp Palliat Care 2011;28(3):161-70.
8. Santler G, Karcher H, Ruda C, Kole E. Fractures of the condylar process: surgical versus nonsurgical treatment. J Oral Maxillofac Surg 1999;57(4):392,7; discussion 397-8.
9. Savin J, Ogden GR. Third molar surgery--a preliminary report on aspects affecting quality of life in the early postoperative period. Br J Oral Maxillofac Surg 1997;35(4):246-53.
10. Schneider M, Erasmus F, Gerlach KL, Kuhlisch E, Loukota RA, Rasse M, et al. Open reduction and internal fixation versus closed treatment and mandibulomaxillary fixation of fractures of the mandibular condylar process: a randomized, prospective, multicenter study with special evaluation of fracture level. J Oral Maxillofac Surg 2008;66(12):2537-44.
11. Schuurhuis JM, Dijkstra PU, Stegenga B, de Bont LG, Spijkervet FK. Groningen temporomandibular total joint prosthesis: an 8-year longitudinal follow-up on function and pain. J Craniomaxillofac Surg 2012;40(8):815-20.
12. Stegenga B, de Bont LG, de Leeuw R, Boering G. Assessment of mandibular function impairment associated with temporomandibular joint osteoarthrosis and internal derangement. J Orofac Pain 1993;7(2):183-95.
13. Ukpong DI, Ugboko VI, Ndukwe KC, Gbolahan OO. Health-related quality of life in Nigerian patients with facial trauma and controls: a preliminary survey. Br J Oral Maxillofac Surg 2008;46(4):297-300.
14. Van den Bergh B, Blankestijn J, van der Ploeg T, Tuinzing DB, Forouzanfar T. Conservative treatment of a mandibular condyle fracture: comparing intermaxillary fixation with screws or arch bar. A randomised clinical trial. currently under review 2015.
15. Wang L, Su YX, Liao GQ. Quality of life in osteoradionecrosis patients after mandible primary reconstruction with free fibula flap. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108(2):162-8.
16. Zachariades N, Mezitis M, Mourouzis C, Papadakis D, Spanou A. Fractures of the mandibular condyle: a review of 466 cases. Literature review, reflections on treatment and proposals. J Craniomaxillofac Surg 2006;34(7):421-32.
Bergh, Bart vd.indd 96 23-10-15 16:35

Bergh, Bart vd.indd 97 23-10-15 16:35

Bergh, Bart vd.indd 98 23-10-15 16:35
Chapter 7:
“Post-operative radiographs after maxillofacial trauma:
sense or nonsense?”
This is an edited version of the manuscript: B. van den Bergh, Y. Goey, T. Forouzanfar. Post-operative radiographs after maxillofacial trauma: sense or nonsense?
International Journal of Oral and Maxillofacial Surgery 2011 Dec;40(12): 1373-6.
Bergh, Bart vd.indd 99 23-10-15 16:35

Chapter 7
100
Abstract
Introduction:The purpose of the present study was to investigate the necessity of routine post-operative radiographic analysis in patients with maxillofacial trauma.
Results: Between January 2000 to January 2010 a total of 579 patients were treated surgically for 646 maxillofacial fractures including complex maxillofacial trauma. The incidence of surgical retreatments based on post-operative radiographs after maxillofacial trauma was investigated. In total 16 patients needed surgical retreatment. The decision to revise based on the post-operative imaging alone was for one patient (0.2%). The available data in the literature concerning post-operative radiography in maxillofacial trauma was reviewed. Six useful studies concerning post-operative radiography in maxillofacial trauma were available for review. When combining these studies, in total 1377 patients underwent surgery for correction of a maxillofacial fracture. Nine patients returned to the operating theatre for correction of the initial procedure after trauma (0.7%).
Conclusion: Our results are in line with the available literature. Performing routine post-operative radiographs is not necessary after surgical treatment of maxillofacial trauma. Avoiding performing routine post-operative radiographs will lead to a reduction in exposure of patients to ionising radiation, a reduction of costs and probably a more efficient discharge.
Bergh, Bart vd.indd 100 23-10-15 16:35

Postoperative radiographs
101
7
Introduction
Post-operative radiographs following surgical treatment in maxillofacial fractures are taken routinely.5,12 Several reasons are used to justify this analysis, including surgical treatment evaluation, detection of defects after surgery before the patient is discharged, registration of the osteosynthesis material for possible removal in future and for teaching and juridical reasons.5,7 There is however minimal evidence for this justifi cation.1,3,5
The Royal College of Radiologists suggested that unnecessary radiation from diagnostic radiology causes 100-250 deaths from cancer every year worldwide.10 Although it is stated that the risk from radiography is low, Memon et al. found a signifi cant association between dental x-ray exposure and the risk of thyroid cancer.8 In this study however radiation exposure dose or other previous radiographic examination (CT or other medical x-ray investigations) were not investigated. Other authors stated that there is a possible association between the use of diagnostic radiography and the development of tumours in brain and parotid gland.6,11,13 In contrast, Rodvall et al. did not found clear evidence associating radiographs with brain tumours.15 Ron commented on this topic stating that it is diffi cult to study the radiation-associated cancer risk, because the doses of radiation for diagnostic examination are low and epidemiologic methods are not easily applicable.16 In conclusion, the relation of maxillofacial radiographic imaging and elevated cancer risk is still debatable. Nevertheless according to the ALARA-principle unnecessary radiography should be avoided.The management of facial fractures has changed in recent years from closed reduction and fi xation to mainly open reduction with fi xation. The benefi t of post-operative radiographic quality analysis is therefore questionable as fracture lines can be inspected directly during surgery and therefore post-operative radiographs will not supply more information.7 Another questionable aspect of taking post-operative radiographs is described by Durham et al.5 They demonstrated that only 57% of the radiographs were reviewed by a member of the staff , which indicates that 43% of all patients were discharged from hospital stay without reviewing the radiographic analysis. In our institutes’ protocol, post-operative radiographs are reviewed prior to a patient’s discharge.Former studies stated that for post-operative evaluation of maxillofacial fractures clinical judgement alone is adequate and taking radiographs is
Bergh, Bart vd.indd 101 23-10-15 16:35

Chapter 7
102
unnecessary.1-3,5 When considering these aspects, the question remains if the amount of radiation the patient is exposed to, the extra expenses and the possible delay of discharge can be justified against the advantages of taking such radiographs? Further, it is not clear if post-operative radiographs influence the decision to return the patient to the operating theatre for a second correction after initial treatment.2
To attribute to the clarification of this important subject we investigated the incidence of surgical retreatments in our institute.
Materials and methods
All patients presented at our hospital from January 2000 to January 2010 with maxillofacial trauma were identified. The inclusion criteria were: patients of both sexes with all types of maxillofacial fractures that were treated surgically by open and closed reduction. Patients with dento-alveolar and nose fractures were excluded. The hospital and outpatient records were reviewed and analysed retrospectively. Data collected included gender, age at presentation, type of maxillofacial trauma, type and amount of post-operative analysis taken, open or closed reduction, surgical retreatment and cause of retreatment. Removal of the osteosynthesis material and correction of scars was not considered as retreatment of the fracture.The maxillofacial fractures were subdivided into zygomatic fractures (zygomatic body or fracture of the zygomatic arch), mandibular fractures (mandibular condyle, mandibular angle, body, symphyseal/parasymphyseal fractures), blow-out fractures, Le Fort I/II/III fractures and fracture of the frontal sinus. Type of post-operative analysis included dental panoramic tomography, submentovertex radiograph, occipitomental radiograph, Towne’s view, cephalometric radiograph, posteroanterior radiograph and (cone-beam) CT-scan. These analyses were performed post-operatively prior to discharge.Also, to conduct a review on the existing literature, a search in the U.S. National Library of Medicine Database (PubMed) was carried out to identify English written articles concerning post-operative radiography in maxillofacial trauma. All studies assessing the necessity for taking post-operative radiographs in maxillofacial trauma were included.
Bergh, Bart vd.indd 102 23-10-15 16:35

Postoperative radiographs
103
7
Results
A total of 579 patients were surgically treated for 646 maxillofacial fractures. An overview of the types of fracture is shown in table 1. Pre-operatively 1263 radiographic analyses were performed, whereas 1097 radiographs were following surgical treatment.
Table 1. Maxillofacial fractures treated surgically.
Type of fracture No.Fracture of the mandible 270Fracture of the zygomatic body 243Fracture of the zygomatic arch 23Le Fort I 19Le Fort II 14Le Fort III 7Panfacial fracture 37Fracture of the frontal sinus 18Blow-out fracture 15Total 646
As seen in table 2 in total 16 patients (2.8%) needed a revision surgery. Three patients were retreated during hospital stay (0.5%). In one patient the zygomatic bone was still clinically displaced after initial treatment for a complex panfacial trauma. The second patient was treated for a solitary zygomatic body fracture. After open reduction with fi xation the clinical analysis demonstrated a displaced body. A retreatment was therefore needed. The third patient presented with a depressed zygomatic arch fracture. After closed reduction the radiographic analysis demonstrated a suboptimally performed reduction. The patient underwent surgical retreatment. For these three patients the post-operative radiographs confi rmed the clinically observed malpositions.Four patients (0.7%) were retreated surgically within two weeks after discharge. All patients were treated as a result of clinical signs. Three of these 4 patients had a fracture of the mandible and during visits at the outpatient clinic malocclusion was noted. One patient was treated for a fracture of the zygomatic bone by closed reduction. One week after discharge he presented with clinical signs of a displaced zygomatic complex. A retreatment was necessary. Retrospectively the post-operative radiographs taken prior to discharge showed no malposition or an indication for retreatment.
Bergh, Bart vd.indd 103 23-10-15 16:35

Chapter 7
104
Another 4 patients (0.7%) were retreated surgically between 2 and 4 weeks after discharge. Three patients needed a secondary correction of the orbital floor after having a fracture of the zygomatic complex. The orbital floor was initially not treated during the reduction of the zygomatic bone, as these patients initially and peri-operatively did not show clinical signs that could justify a primary orbital bone exploration and reconstruction. Post-operative radiographs were simple plain views (submentovertex radiographs and occipitomental radiographs) and on these views no malposition was detectable. The fourth patient was retreated for a developed malocclusion after a complex panfacial trauma. When viewing the post-operative CT-scan of this patient the reduction of this panfacial trauma can be judged as unsatisfactory.Five patients (0.9%) were retreated more than four weeks after discharge. One patient underwent a unilateral sagittal split osteotomy for correction of a malocclusion after a mandibular fracture. Retrospectively no indication of incorrect reduction could be detected on the post-operative views of this patient. Three patients underwent a secondary correction of the orbital floor (two blow-out fractures and one fracture of the zygomatic body). These patients initially had no clinical signs but developed enophthalmia and/or diplopia later on. A suboptimal reconstruction of the orbital floor could be detected on the post-operative CT-scan of one patient. On the post-operative views of the other two patients no malposition was visible. The fifth patient was retreated for a malpositioned frontal sinus wall after a fracture of the frontal sinus. Retrospectively the post-operative view of this patient showed no indication that something was potentially incorrect. These five retreatments were based on clinical findings only. The radiographic analyses were used to confirm the clinical findings.
Bergh, Bart vd.indd 104 23-10-15 16:35
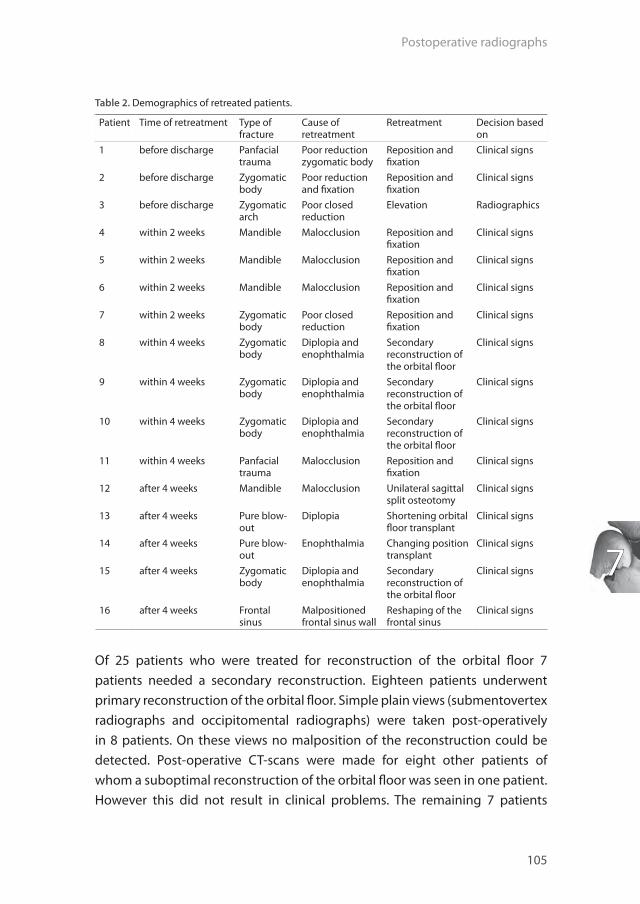
Postoperative radiographs
105
7
Table 2. Demographics of retreated patients.
Patient Time of retreatment Type of fracture
Cause of retreatment
Retreatment Decision based on
1 before discharge Panfacial trauma
Poor reduction zygomatic body
Reposition and fi xation
Clinical signs
2 before discharge Zygomatic body
Poor reduction and fi xation
Reposition and fi xation
Clinical signs
3 before discharge Zygomatic arch
Poor closed reduction
Elevation Radiographics
4 within 2 weeks Mandible Malocclusion Reposition and fi xation
Clinical signs
5 within 2 weeks Mandible Malocclusion Reposition and fi xation
Clinical signs
6 within 2 weeks Mandible Malocclusion Reposition and fi xation
Clinical signs
7 within 2 weeks Zygomatic body
Poor closed reduction
Reposition and fi xation
Clinical signs
8 within 4 weeks Zygomatic body
Diplopia and enophthalmia
Secondary reconstruction of the orbital fl oor
Clinical signs
9 within 4 weeks Zygomatic body
Diplopia and enophthalmia
Secondary reconstruction of the orbital fl oor
Clinical signs
10 within 4 weeks Zygomatic body
Diplopia and enophthalmia
Secondary reconstruction of the orbital fl oor
Clinical signs
11 within 4 weeks Panfacial trauma
Malocclusion Reposition and fi xation
Clinical signs
12 after 4 weeks Mandible Malocclusion Unilateral sagittal split osteotomy
Clinical signs
13 after 4 weeks Pure blow-out
Diplopia Shortening orbital fl oor transplant
Clinical signs
14 after 4 weeks Pure blow-out
Enophthalmia Changing position transplant
Clinical signs
15 after 4 weeks Zygomatic body
Diplopia and enophthalmia
Secondary reconstruction of the orbital fl oor
Clinical signs
16 after 4 weeks Frontal sinus
Malpositioned frontal sinus wall
Reshaping of the frontal sinus
Clinical signs
Of 25 patients who were treated for reconstruction of the orbital fl oor 7 patients needed a secondary reconstruction. Eighteen patients underwent primary reconstruction of the orbital fl oor. Simple plain views (submentovertex radiographs and occipitomental radiographs) were taken post-operatively in 8 patients. On these views no malposition of the reconstruction could be detected. Post-operative CT-scans were made for eight other patients of whom a suboptimal reconstruction of the orbital fl oor was seen in one patient. However this did not result in clinical problems. The remaining 7 patients
Bergh, Bart vd.indd 105 23-10-15 16:35

Chapter 7
106
showed a satisfactory result of the reconstruction. Of 2 patients data are missing for analysis.The search strategy on existing literature concerning post-operative radiographic imaging, resulted in 6 useful studies.1,2,4,5,7,12 Three studies were prospective 4,5,7, two were retrospective 2,12 and one was combined prospective / retrospective 1. One study conducted a multi-centre trial.7 In these studies different ‘populations’ were analysed. One study researched solitary mandible fractures5, two studies solitary zygomatic bone fractures4,12 and one study investigated both solitary mandible and solitary zygomatic bone fractures2. All types of maxillofacial fractures were analysed by two studies.1,7 All studies excluded complex craniofacial trauma. The post-operative follow up ranged from immediately post-operatively to three months post-operatively. In total 1377 patients (range 30-431) underwent surgery for correction of a maxillofacial fracture (table 3). Nine patients returned to the operating theatre for correction of the initial procedure after trauma (0.7%). In all patients the decision to revise was based solely on the clinical findings. The authors of these 6 studies concluded that clinical judgement alone is sufficient for the post-operative evaluation of maxillofacial fractures.
Table 3. Studies concerning post-operative imaging.
Author Year Type of study Type of fracture No. of patients
Retreatments
Durham et al. 2006 prospective mandible 100 0
Jain et al. 2009 prospective all types of fractures 431 2
Crighton et al. 2006 prospective zygoma 30 0
Bali et al. 2004 prospective / retrospective
all types of fractures 257 3
Chandramohan 2007 retrospective mandible + zygoma 376 3
Ogden et al. 1988 retrospective zygoma 183 1
Total 1377 9
Bergh, Bart vd.indd 106 23-10-15 16:35

Postoperative radiographs
107
7
Discussion
The purposes of the present study were to investigate the necessity of post-operative radiographic analysis in patients with maxillofacial trauma and compare these results with existing literature. Therefore a retrospective analysis was performed concerning all maxillofacial trauma surgically treated over the last ten years in our institute. In total 579 patients were treated for 646 fractures whereas in 16 patients (2.8%) a secondary treatment was needed as the initial treatment did not result in satisfactory reduction and fi xation. The decision for surgical revision was mainly based on clinical fi ndings (15 patients, 94%), confi rmed by radiographical analyses. For one patient (6%) the decision for retreatment was based on radiographical fi ndings only. This patient was treated immediately after the initial reduction as radiographic analysis demonstrated a suboptimally elevated zygomatic arch. Our results are in line with the available literature. However compared to the above mentioned studies our results show a relatively high number of retreatments which can probably be explained by the prolonged follow up compared to the other studies. Another explanation may be the inclusion of complex craniofacial trauma.Several authors postulated arguments to perform post-operative radiographs, including surgical treatment evaluation and detection of defects after surgery before the patient is discharged.5,7 As the treatment of facial fractures has changed in recent years from closed reduction with fi xation to mainly open reduction with fi xation the benefi t of post-operative radiographic analysis is questionable.1 Fracture lines can be inspected directly during surgery and therefore post-operative radiographs will not supply more information. In multiple facial injuries (e.g. panfacial trauma) it can sometimes be diffi cult to visualize every bone fragment during open reduction. In these cases the surgeon may consider taking post-operative radiographs.Further, post-operative radiographs are advised to prevent juridical complications. However according to Jain et al. if observation of the fracture lines during surgery and results of clinical fi ndings are documented well there is adequate evidence for a correct treatment and therefore post-operative radiography is unnecessary.7 As juridical aspects are out of the scope of the authors’ expertise this subject will not be discussed further.
Bergh, Bart vd.indd 107 23-10-15 16:35

Chapter 7
108
Another reason used to justify standard post-operative imaging is registration of used osteosynthesis material for possible removal in the future. To the authors’ opinion this can be performed on indication when the decision is made to remove the osteosynthesis.Our data did not demonstrate that avoiding routine post-operative radiographs will lead to a more efficient discharge. In our institute most patients surgically treated in the afternoon stay overnight. This is dictated by our institutes’ protocol and influenced by clinic-related factors (e.g. logistics, paramedical capacity). As a result of this process patients are not being discharged until the next morning after taking post-operative radiographs. Our institute is a university hospital and the department of oral and maxillofacial surgery has not only healthcare - , but also educational obligations. For educational purposes pre- and post-operative radiographs are indispensable. Interpretation of radiographs is stated to improve during the first years of practice.9,14 No information exists whether performing or interpreting radiographs in maxillofacial trauma will add to the learning curve of registrars of oral and maxillofacial surgery. Nevertheless to the authors’ opinion it is justified to take routine radiographs in a teaching hospital for this educational purpose. The consequence of this opinion is that radiographs are performed when a patient is submitted in a teaching hospital and not when submitted to a non-teaching hospital. This is a controversial and ethical matter. On the other hand in everyday practice this is already the case.The present retrospective study contains data of all maxillofacial trauma including complex maxillofacial trauma and has the largest population of all studies published. Like other retrospective studies our analysis may lead to information bias. Despite this shortcoming, the results presented are in line with other studies and the analysis of this report provides important data to support the elimination of standard post-operative radiographs as proposed by previous authors. In our opinion the merit of performing 1097 post-operative radiographs to identify 1 patient needing a secondary treatment after the initial reduction based on radiographic analysis alone, is questionable. Intra-operative analysis of the reduction and fixation, followed by immediate post-operative clinical assessment are better indicators to evaluate the adequacy of the treatment. Post-operative imaging should be reserved for patients with signs and symptoms suggestive of unfavourable post-operative outcome or complications.4 Furthermore taking post-operative radiographs
Bergh, Bart vd.indd 108 23-10-15 16:35

Postoperative radiographs
109
7
may be considered in multiple facial injuries and for educational purposes in a teaching hospital. Nevertheless avoiding performing routine post-operative radiographs will lead to a reduction in exposure of patients to ionising radiation. Further benefi ts of avoiding routine post-operative radiographs include cost savings and probably more effi cient discharge.
Bergh, Bart vd.indd 109 23-10-15 16:35

Chapter 7
110
References
1. Bali N, Lopes V. An audit of the effectiveness of postoperative radiographs--do they make a difference? Br J Oral Maxillofac Surg 2004: 42: 331-4.
2. Chandramohan J, McLoughlin PM. Fractures of the mandible and zygomatic complex: postoperative radiographs are not necessary. Br J Oral Maxillofac Surg 2007: 45: 90.
3. Childress CS, Newlands SD. Utilization of panoramic radiographs to evaluate short-term complications of mandibular fracture repair. Laryngoscope 1999: 109: 1269-72.
4. Crighton LA, Koppel DA. The value of postoperative radiographs in the management of zygomatic fractures: prospective study. Br J Oral Maxillofac Surg 2007: 45: 51-3.
5. Durham JA, Paterson AW, Pierse D, Adams JR, Clark M, Hierons R, Edwards K. Postoperative radiographs after open reduction and internal fixation of the mandible: are they useful? Br J Oral Maxillofac Surg 2006: 44: 279-82.
6. Horn-Ross PL, Ljung BM, Morrow M. Environmental factors and the risk of salivary gland cancer. Epidemiology 1997: 8: 414-9.
7. Jain MK, Alexander M. The need of postoperative radiographs in maxillofacial fractures--a prospective multicentric study. Br J Oral Maxillofac Surg 2009: 47: 525-9.
8. Memon A, Godward S, Williams D, Siddique I, Al-Saleh K. Dental x-rays and the risk of thyroid cancer: a case-control study. Acta Oncol 2010: 49: 447-53.
9. Miglioretti DL, Gard CC, Carney PA, Onega TL, Buist DS, Seckles EA, Kerlikowske K, Rosenberg RD, Yankaskas BC, Geller BM, Elmore JG. When radiologists perform best: the learning curve in screening mammogram interpretation 1. Radiology 2009: 253: 632-40.
10. National Radiologic Protection Board. Patient dose reduction in diagnostic radiology. 1990 11. Neuberger JS, Brownson RC, Morantz RA, Chin TD. Association of brain cancer with dental X-rays
and occupation in Missouri. Cancer Detect Prev 1991: 15: 31-4. 12. Ogden GR, Cowpe JG, Adi M. Are post-operative radiographs necessary in the management of
simple fractures of the zygomatic complex? Br J Oral Maxillofac Surg 1988: 26: 292-6. 13. Preston-Martin S, White SC. Brain and salivary gland tumors related to prior dental radiography:
implications for current practice. J Am Dent Assoc 1990: 120: 151-8. 14. Ripsweden J, Mir-Akbari H, Brolin EB, Brismar T, Nilsson T, Rasmussen E, Ruck A, Svensson A, Werner
C, Winter R, Cederlund K. Is training essential for interpreting cardiac computed tomography? 4. Acta Radiol 2009: 50: 194-200.
15. Rodvall Y, Ahlbom A, Pershagen G, Nylander M, Spannare B. Dental radiography after age 25 years, amalgam fillings and tumours of the central nervous system. Oral Oncol 1998: 34: 265-9.
16. Ron E. Cancer risks from medical radiation. Health Phys 2003: 85: 47-59.
Bergh, Bart vd.indd 110 23-10-15 16:35

Bergh, Bart vd.indd 111 23-10-15 16:35
Bergh, Bart vd.indd 112 23-10-15 16:35

Chapter 8:
General discussion
Bergh, Bart vd.indd 113 23-10-15 16:35

Chapter 8
114
General discussion
The aim of this thesis was to investigate the aetiology, incidence and complications of maxillofacial trauma in general and mandibular fractures in particular. Another objective was to investigate the long-term results and complications of bilateral fractures of the mandibular condyle, and whether post-operative complications would influence masticatory function and quality of life. Furthermore this thesis aimed to assess the advantages, disadvantages and the results of IMFS in the closed treatment of mandibular condylar fractures, and the impact of these IMF screws on quality of life. Finally, the necessity for the standard use of post-operative radiographic imaging to evaluate surgery is questioned and investigated.
A total of 579 patients were surgically treated for maxillofacial trauma in a 10-year period in the VU University Medical Center, one of 2 university hospitals, out of 4 hospitals in Amsterdam. Mandibular and zygomatic bone fractures were the most common fractures of both men and women, accounting for approximately 80% of all fractures. As reported in previous studies, the majority of the patients belonged to the age group of 20–29 years age group. The most common cause of fractures was traffic accidents (bicycle accidents being the most frequent), followed by interpersonal violence, particularly in males. Interpersonal violence-related fractures proved to be significantly more frequent in men compared to women. The results of this study are mostly in line with other international studies that were conducted in developed countries, but differ on one noteworthy aspect: a higher incidence of bicycle-related accidents. The Amsterdam-region contains an extensive tramway network system. This aspect, in combination with the finding that cyclists are a substantial part of the transport-system in the Amsterdam-region, may be a good explanation for the high incidence of bicycle-related accidents as a cause of maxillofacial trauma in general, and zygomatic bone fractures and uni-/bilateral condylar fractures in particular.
The long-term outcome of closed treatment of bilateral fractured condyles was investigated. In total 71 patients were identified from the hospital database, all surgically treated between 1995 and 2011. Of them, 41 attended the outpatient clinic for review and a thorough physical examination. A rather
Bergh, Bart vd.indd 114 23-10-15 16:35

General discussion
115
8
high malocclusion rate of 13% was observed after closed treatment of bilateral condylar fracture, but all these patients were without functional problems and without pain. Regression analyses showed a signifi cant (negative) relation between the presence of pain and duration of follow up, and a signifi cant relation between decreasing intensity of pain with increasing age. This may suggest that if sensations of pain exist, these can diminish or even disappear over time, which could be of great importance when counselling new patients. More important, the results of this investigation show rather good long-term functional results of closed treatment of bilateral condylar fractures with IMF. This is confl icting with several studies that argue in favour of ORIF for these type of fractures.4,5,6
A prospective multi-centre randomised clinical trial was conducted in which the use of IMFS was compared to the use of arch bars in closed treatment of mandibular condyle fractures. In total 50 patients were included. The results are mostly in favour of IMFS. When compared to arch bars, IMFS lead to shorter application time (on average 52 minutes shorter, p < 0.001), shorter surgical treatment time (on average 67 minutes shorter, p < 0.001), less needlestick injuries (p = 0.003), lower pain scores, and the same favourable occlusal results. As not many IMFS-related complications were encountered, using IMFS leads to predictable results. In conclusion, considering the results, advantages and the disadvantages of IMFS, IMFS are a superior method for IMF fracture management compared to arch bars. IMFS are safer for patients and surgeons. Also the impact of IMFS and arch bars on QOL was investigated. Patients treated with IMFS experience less social isolation, have fewer problems with eating, and express the feeling that they were able to continue a normal diet. Also, it seems that the use of IMFS has a lower negative impact on social and fi nancial aspects of the patient.
The favourable results of using IMFS are not only important for the individual patient, but could also have a major impact on Dutch society. Firstly it will improve quality of maxillofacial trauma care, secondly it will lead to a large cost reduction. In the VU University Medical Center Amsterdam, in a 9-year period, a total of 83 unilateral and 42 bilateral condyle fractures were treated with closed treatment. On average this would lead to approximately 9 unilateral and 5 bilateral condylar fractures per year. We expect these epidemiology-numbers
Bergh, Bart vd.indd 115 23-10-15 16:35

Chapter 8
116
to be 50% of all maxillofacial trauma treated in Amsterdam (approximately 800.000 inhabitants). Extrapolating these locally based epidemiology data to a national level (The Netherlands: 16.923.151 inhabitants1), every year approximately 380 unilateral and 212 bilateral condylar fractures are expected to be diagnosed and treated with closed treatment (i.e. IMF).Treating condylar fractures with IMFS compared to arch bars, would then lead to a reduction of 30.784 minutes of applying IMF and 39.664 minutes of total surgery time on a national basis. Using IMFS will thus lead to shorter periods of general anaesthesia and therefore reduced risks to patients, to reduced theatre time requirements, and lower costs. West et al. estimated total cost savings of $661 (approximately €500) per patient with the use of IMFS.2 Calculating with these cost savings, this would lead to a total cost savings on the national maxillofacial surgery budget of approximately €296.000 yearly. Apart from the observation that shorter general anaesthesia and shorter surgery times can be obtained, IMFS have the advantage of avoiding general anaesthesia with the application of IMFS under local anaesthesia. This may lead to a further decreasing theatre time requirement, less inconvenience for patients as admittance to the clinical ward is unnecessary, and a further decrease of costs.
As discussed in Chapter 5, using IMFS leads to lower pain scores, especially in the initial three days post-operatively. Not investigated in this thesis, but as lower pain scores are expected, consequently the use of analgesics (paracetamol, NSAID’s, opiates) will decrease as well. Apart from the beneficial effects this aspect will have on patients’ individual health (e.g. less NSAID’s-related gastritis, and less side-effects, e.g. drug-induced allergy), this again may be cost saving to hospital’s and general health’s financial budget.
With regard to QOL it can be concluded that IMFS lead to more subjective comfort in the six-weeks period of fracture healing. Patients treated with IMFS feel less socially isolated, have the feeling that they can continue normal diet and experience less problems falling asleep in the first post-operative week. On the whole patients treated with IMFS have a higher QOL compared to the use of arch bars. Although not investigated, this latter aspect may lead to a lower incidence of anxiety, depression or Posttraumatic Stress Disorder (PTSD), as this may develop after being exposed to one or more traumatic events.3,7
Bergh, Bart vd.indd 116 23-10-15 16:35

General discussion
117
8
Recently Kaukola et al. evaluated QOL of patients treated surgically for mandibular fractures (with the exception of condylar fractures and IMF).8 The authors found QOL to be signifi cantly reduced immediately after surgery. The usage of IMFS may therefore be benefi cial in this early post-operative period, as QOL has been shown to be better.
In conclusion, treating mandibular condyle fractures with IMFS leads to many benefi ts for the individual patient, both surgically and psychologically. The fi ndings of this thesis are also relevant for the Dutch society in a period where costs reductions are made throughout general health care, and quality of maxillofacial trauma care is improved.
The investigation of the necessity of post-operative radiographic analysis in patients with maxillofacial trauma, led to the conclusion that routine post-operative radiography is not necessary after surgical treatment of maxillofacial trauma. These results are in line with the available literature. Intra-operative analysis of the reduction and the immediate post-operative clinical symptoms are better indicators to evaluate the adequacy of treatment. Therefore post-operative imaging should be reserved for patients with signs and symptoms suggesting unsatisfactory post-surgical outcome or complications.4 Furthermore taking post-operative radiographs may be considered in multiple facial injuries and for educational purposes in a teaching hospital. Nevertheless avoiding performing routine post-operative radiographs will lead to a reduction in exposure of patients to ionising radiation.
Future Perspectives
The investigated incidences and prevalences could be of value in actualizing treatment protocols, this should be further evaluated. These results may also be important for future preventive strategies (e.g. obligatory helmet wearing during cycling?).As observed, treatment of condylar fractures with IMFS still leads to some disadvantages, such as the development of suboptimal occlusion, screw failure upon insertion and mucosal disturbances. Ideally, more research should be conducted to identify factors that contribute to the small chance of developing
Bergh, Bart vd.indd 117 23-10-15 16:35

Chapter 8
118
suboptimal occlusions. Another aim of future research lies in the design of IMFS. Presumably, the design of IMFS could be further improved, leading to less screw-related problems such as fracture and/or mucosal disturbances. The use of IMFS for maxillofacial trauma is relatively new. Therefore many aspects of their use could be subject to future research: application of IMFS under local anaesthesia; ideal number and placement location of IMFS; can IMFS be used perioperatively only and do they lead to the same advantages; the role of IMFS in orthognathic surgery or other fields in maxillofacial surgery.As discussed in the General Discussion section, cost reduction may be an associated factor for using IMFS. Further research should be performed to investigate the cost reductions more profoundly.Finally, quality of life-related issues in the treatment of maxillofacial trauma patients should be further explored and be taken into account in future treatment protocols.
Bergh, Bart vd.indd 118 23-10-15 16:35

General discussion
119
8
References
1. website Centraal Bureau voor Statistiek: http://www.cbs.nl/nl-NL/menu/cijfers/default.htm (period of measurement: may 2015)
2. West GH, Griggs JA, Chandran R, Precheur HV, Buchanan W, Caloss R. Treatment outcomes with the use of maxillomandibular fi xation screws in the management of mandible fractures. J Oral Maxillofac Surg 2014;72(1):112-20.
3. American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. pp. 271–280.
4. Zachariades N, Mezitis M, Mourouzis C, Papadakis D, Spanou A. Fractures of the mandibular condyle: a review of 466 cases. Literature review, refl ections on treatment and proposals. J Craniomaxillofac Surg 2006;7:421-432.
5. Gupta M, Iyer N, Das D, Nagaraj J. Analysis of Diff erent Treatment Protocols for Fractures of Condylar Process of Mandible. J Oral Maxillofac Surg 2011.
6. Chen CT, Feng CH, Tsay PK, Lai JP, Chen YR. Functional outcomes following surgical treatment of bilateral mandibular condylar fractures. Int J Oral Maxillofac Surg 2011;1:38-44.
7. Roccia F, Dell’Acqua A, Angelini G, Berrone S. The association between depression and anxiety disorders following facial trauma – a comparative study. J Craniofac Surg 2005;16:355-360.
8. Kaukola L, Snäll J, Lindqvist Ch, Roine R, Sintonen H, Törnwall J, Thorén H. Health-related quality of life after surgical treatment of mandibular fracture. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119:402-407.
Bergh, Bart vd.indd 119 23-10-15 16:35

Bergh, Bart vd.indd 120 23-10-15 16:35

Chapter 9:
Summary
Bergh, Bart vd.indd 121 23-10-15 16:35

Chapter 9
122
Chapter 2: “ Aetiology and incidence of maxillofacial trauma in Amsterdam: A retrospective analysis of 579 patients.”
All patients treated in the VU University Medical Center (Amsterdam), for maxillofacial trauma, were identified retrospectively (period 2000-2010). A total of 579 patients were identified (408 men and 171 women), with a mean age of 35.9 ± 16.3 years. Mandibular and zygomatic bone fractures were the most common among both men and women, accounting for approximately 80% of all fractures. As reported in previous studies, majority of the patients belonged to the age group of 20–29 years among both sexes.The most common cause of fractures was traffic accidents (bicycle accidents being the most frequent), followed by interpersonal violence, particularly among men. The results of this study are mostly in line with other international studies that were conducted in developed countries, but differ on one noteworthy aspect: a higher incidence of bicycle-related accidents.
Chapter 3: “ Treatment and complications of mandibular fractures: A 9-year analysis.”
During the period 2000-2009, a total of 225 patients were treated for a uni- or multifocal mandibular fracture. The mean age of this population was slightly lower (32.6 ± 14.6 years) compared with the mean age of all maxillofacial trauma patients. A total of 431 fracture lines were identified. Similar to maxillofacial trauma in general, traffic-accidents were the main cause of mandibular fracture (42%), followed by interpersonal violence (24%) and falls (19%). A total of 1965 screws and 442 plates were used.Of the total population of 225 patients, 171 condylar fractures in 127 patients were observed. Of these 225 patients, 213 were dentate and 12 were edentulous. Eighty-two (36%) dentate patients presented with a unilateral condyle fracture with or without concomitant fracture of the mandible. These patients were all treated with IMF and osteosynthesis in case of an associated mandible fracture. Forty (18%) dentate patients were treated with IMF for a bilateral condyle fracture, with or without concomitant mandibular fracture. Two (2/225: 1%) patients were treated extraorally using a preauricular approach. Three edentulous patients were diagnosed with either a unilateral (n = 1) or bilateral (n = 2) condyle fracture.
Bergh, Bart vd.indd 122 23-10-15 16:35

Summary
123
9
Of all patients treated for mandibular trauma, 27% presented with complications. These included (transient) hyposensibility of the lip and chin, malocclusion, infected osteosynthesis material and temporomandibular dysfunction. Four (4/225: 1.8%) patients needed surgical correction of a post-treatment malocclusion.
Chapter 4: “ Long-term results and complications after bilateral mandibular condyle fractures.”
The long-term outcome of closed treatment of bilateral fractured condyles (with or without an associated mandible fracture) was investigated. Seventy-one patients were identifi ed from the hospital database, all surgically treated between 1995 and 2011. Of these 71 patients, 41 attended the outpatient clinic for review and a thorough physical examination using the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD). Five of them presented with an anterior open bite (AOB), but all were without functional problems and without pain (RDC/TMD grade 0). Of the 30 patients that were not available for clinical evaluation, it was found in the hospital and outpatient records that three patients needed orthognathic correction and one patient orthodontic correction for a post-treatment malocclusion. A rather high malocclusion rate (9/71: 13%) was observed after closed treatment of bilateral condylar fracture.Furthermore, in this investigation, regression analyses showed a signifi cant negative relation between the presence of pain and duration of follow up (p = 0.02), and between decreasing intensity of pain with increasing age (p = 0.03). This may suggest that if sensations of pain exist, these can diminish or even disappear over time, which could be of great importance when counselling new patients. Furthermore, these results may be of value when discussing what the best treatment is regarding (uni- or bilateral) condylar fractures. Finally, one might debate the need to treat all malocclusions that develop following treatment, as not all malocclusions lead to functional problems or pain.These long-term fi ndings and the rather high success rate of IMF, support closed treatment of uni- or bilateral condyle fractures with arch bars.
Bergh, Bart vd.indd 123 23-10-15 16:35

Chapter 9
124
Chapter 5: “ Closed treatment of mandibular condyle fractures: comparing intermaxillary fixation with screws or arch bar. A randomised clinical trial.”
The results of this prospective multi-centre randomised clinical trial are mostly in favour of IMFS in treating mandibular condyle fractures, in comparison with the use of arch bars. These results comprise perioperative as well as post-operative elements. The surgical treatment time with the use of IMFS led to a significantly shorter application time (on average 52 minutes shorter, p < 0.001) and consequently to a shorter duration of surgery (on average 67 minutes shorter, p < 0.001). From the surgeons’ point of view, the use of IMFS is significantly safer. In this trial 8 (30.7%) needlestick injuries were observed; all accidents occurred during the application of arch bars (p = 0.003). Not many complications with the use of IMFS occurred: one (0.53%) root was affected by the insertion of an IMFS. One out of 188 screws failed (breakage) during insertion (0.53%). Six (3.2%) screws loosened spontaneously during the follow up period of six weeks, three of which needed to be replaced to apply further functional therapy. Compared to existing literature the incidence of the encountered complications are relatively low. All pain-scores were lower in the IMFS group compared with the arch bars group, including the average pain over the week and pain when removing IMFS. With regard to occlusion, the use of IMFS leads to the same favourable occlusal results as arch bars. Three patients developed a suboptimal occlusion: one patient was treated with IMFS, and two patients were treated with arch bars. Oral mucosal damages were observed in 22 patients, 11 in each group. In the arch bars group, gingival hyperplasia of the interdental papillae was observed. In the IMFS group, partial mucosal overgrowth of screws was encountered. In overview, taking these results into account and considering the advantages and the disadvantages of IMFS, it is concluded that IMFS are a superior method for applying IMF. IMFS lead to less pain, the same occlusion results, shorter operation times, better opportunities for treatment under local anaesthesia and fewer needlestick injuries. In short, IMFS are safer for patients and surgeons.
Bergh, Bart vd.indd 124 23-10-15 16:35

Summary
125
9
Chapter 6: “ IMF screws or arch bars for closed treatment of mandibular condyle fractures: the quality of life-aspects.”
The results of this QOL investigation are mostly in favour of IMFS. Patients treated with IMFS experience less social isolation and fewer problems with eating. IMFS-patients express the feeling that they were able to continue a normal diet. Also, it seems that the use of IMFS has a lower negative impact on social and fi nancial aspects of the patient. This conclusion was based on the fact that 36% of persons accompanying arch bars-patients to a regular post-operative check-up cancelled their job commitments for this visit. No diff erences were observed in the ability to speak between each group.In today’s literature no QOL-data is available for any type of IMF application. Therefore these results are unique, and may act as a baseline measurement in future research.
Chapter 7: “ Post-operative radiographs after maxillofacial trauma: sense or nonsense?”
The purposes of the present study were to investigate the necessity of post-operative radiographic analysis in patients with maxillofacial trauma and compare these results with existing literature. A retrospective analysis was performed concerning all maxillofacial trauma surgically treated in the last ten years in our institute. In total 579 patients were treated for 646 fractures whereas in 16 patients (2.8%) a secondary treatment was needed as the initial treatment did not result in a satisfactory reduction and fi xation. The decision to retreatment was mainly based on clinical fi ndings (15 patients, 94%), confi rmed by radiographical analyses. For one patient (6%) the decision for retreatment was based on radiographical fi ndings alone. This patient was treated immediately after the initial reduction as radiographic analysis demonstrated a suboptimally elevated zygomatic arch. These results led to the conclusion that routine post-operative radiography is not necessary after surgical treatment of maxillofacial trauma.Our results are in line with the available literature. However compared to these available studies our results show a relatively high number of retreatments that can probably be explained by the prolonged follow up compared to the other studies. Another explanation may be the inclusion of complex craniofacial trauma.
Bergh, Bart vd.indd 125 23-10-15 16:35

Chapter 9
126
Intra-operative inspection of the reduction and the immediate post-operative clinical symptoms are better indicators to evaluate the adequacy of the treatment. Post-operative imaging should be reserved for patients with signs and symptoms suggestive of unsatisfactory surgical outcome or complications. Furthermore taking post-operative radiographs may be considered in multiple facial injuries and for educational purposes in a teaching hospital. Nevertheless avoiding performing routine post-operative radiographs will lead to a reduction in exposure of patients to ionising radiation. Further benefits of avoiding routine post-operative radiographs include cost savings and probably more efficient discharge.
Bergh, Bart vd.indd 126 23-10-15 16:35

Bergh, Bart vd.indd 127 23-10-15 16:35
Bergh, Bart vd.indd 128 23-10-15 16:35
Dutch summary
Bergh, Bart vd.indd 129 23-10-15 16:35

130
Hoofdstuk 2: “ Etiologie en incidentie van maxillofaciaal trauma in Amsterdam: een analyse van 579 patiënten.”
Alle patiënten die in het VU medisch centrum (Amsterdam) in narcose behandeld zijn voor aangezichtsfracturen, zijn retrospectief geïdentificeerd (periode 2000-2010). In totaal 579 patiënten zijn geïdentificeerd (408 mannen, 171 vrouwen), met een gemiddelde leeftijd van 35.9 ± 16.3 jaar. Mandibula- en zygoma-fracturen kwamen bij zowel mannen als vrouwen het meest voor, tezamen ongeveer 80% van alle fracturen innemend. Conform de resultaten uit eerdere onderzoeken, behoorde de meerderheid van de patiënten tot de 20-29 jaar leeftijdsgroep.De meeste fracturen zijn veroorzaakt door verkeersongevallen (fietsongevallen kwamen het meest frequent voor), gevolgd door geweld, met name bij mannen. Geweld-gerelateerde fracturen kwamen significant vaker voor bij mannen in vergelijking met vrouwen.De resultaten uit dit onderzoek komen overeen met eerdere internationale studies die zijn uitgevoerd in ontwikkelde landen, maar wijkt af op één aspect: de hogere incidentie van fiets-gerelateerde ongevallen.
Hoofdstuk 3: “ Behandeling en complicaties van mandibula-fracturen: een analyse van 9 jaar.”
Tijdens de periode 2000-2009 zijn in totaal 225 patiënten in narcose behandeld voor een uni- of multifocaal voorkomend mandibula-fractuur. De gemiddelde leeftijd van deze populatie was iets lager (32.6 ± 14.6 jaar) vergeleken met de gemiddelde leeftijd van de totale maxillofaciale trauma populatie.In totaal werden 431 fractuurlijnen geïdentificeerd. Conform de bevindingen bij de totale maxillofaciale trauma-populatie, waren verkeersongevallen de meest voorkomende oorzaak van het ontstaan van een mandibula-fractuur (42%), gevolgd door geweld (24%) en vallen (19%). In totaal werden 1965 schroeven en 442 platen gebruikt.166 collumfracturen in 127 patiënten werden gezien in de totale mandibula-populatie van 225 patiënten. 213 patiënten waren betand, en 12 waren onbetand/edentaat. 82 (36%) betande patiënten presenteerden zich met een unilaterale collumfractuur, mét of zonder een bijkomende fractuur van
Bergh, Bart vd.indd 130 23-10-15 16:35

Dutch summary
131
het corpus van de mandibula. Deze 82 patiënten zijn allen behandeld met IMF en gebruik van osteosynthesemateriaal in geval van een bijkomende corpus-fractuur. 40 (18%) betande patiënten werden behandeld met IMF voor een bilateraal voorkomende collumfractuur, met of zonder bijkomende mandibula-fractuur. Twee (2/225: 1%) patiënten zijn extraoraal behandeld gebruik makend van een pre-auriculaire benadering. Drie onbetande/edentate patiënten waren gediagnosticeerd met ofwel een unilateraal voorkomend (n = 1) ofwel een bilateraal voorkomend (n = 2) collumfractuur. Van alle patiënten die zijn behandeld voor een mandibula-fractuur, traden bij 27% complicaties op. Tot deze complicaties behoorden (passagère) hyposensibiliteit van de onderlip en kin-regio, malocclusie, geïnfecteerd osteosynthesemateriaal en temporomandibulaire dysfunctie. Vier (4/225: 1.8%) patiënten behoefden chirurgische herbehandeling in verband met een persisterende of ontwikkelde malocclusie.
Hoofdstuk 4: “ Lange termijn resultaten en complicaties na bilaterale mandibulaire collumfracturen.”
De lange termijn resultaten van gesloten behandeling van bilaterale collumfracturen (met of zonder bijkomende mandibula-fractuur) werd onderzocht. 71 patiënten werden geïdentifi ceerd uit het ziekenhuis-bestand, allen in narcose behandeld tussen 1995 en 2011. Van deze 71 patiënten bezochten 41 patiënten de polikliniek voor beoordeling en een uitgebreid lichamelijk onderzoek, gebruik makend van de Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD). Vijf van hen presenteerden zich met een anterieure open beet, maar waren allen zonder functionele klachten en zonder pijn (RDC/TMD graad 0). Van de 30 patiënten die niet beschikbaar waren voor beoordeling en lichamelijk onderzoek, bleek uit de klinische en poliklinische statussen dat ontstane malocclusie bij drie patiënten gecorrigeerd was door orthognatische chirurgie, en dat bij één patiënt orthodontische correctie nodig was. Een redelijk hoog percentage malocclusie (9/71: 13%) was daarom gezien na gesloten behandeling van bilaterale collumfracturen.Daarnaast bleek uit regressie analyses, dat er een signifi cant negatieve relatie bestaat tussen de aanwezigheid van pijn en de duur van ‘follow-up’ (p = 0.02), en tussen vermindering van pijn-intensiteit en toenemende leeftijd (p = 0.03).
Bergh, Bart vd.indd 131 23-10-15 16:35

132
Deze relatie zouden er op kunnen wijzen dat met de tijd bestaande pijn kan afnemen of zelfs verdwijnen. Dit kan van groot belang zijn bij uitleg aan nieuwe patiënten. Daarnaast kunnen deze resultaten van belang zijn in de discussie over de beste behandeling aangaande (uni- en bilaterale) collumfracturen. Als laatste kan men zich afvragen of het nodig is om alle ontstane malocclusies te behandelen, aangezien niet alle malocclusies leiden tot functionele klachten en/of pijn.Deze lange termijn resultaten ondersteunen gesloten behandeling van uni- of bilaterale collumfracturen met winterspalken.
Hoofdstuk 5: “ Gesloten behandeling van collumfracturen: IMF-schroeven vergeleken met winterspalken ten behoeve van intermaxillaire fixatie. Een gerandomiseerde klinische studie.”
De resultaten van dit prospectieve multicenter gerandomiseerde klinische onderzoek zijn overwegend in het voordeel van IMFS, bij de behandeling van collumfracturen, wanneer vergeleken met winterspalken. Deze resultaten behelzen zowel perioperatieve als postoperatieve elementen. Gebruik van IMFS leidde tot kortere applicatie (gemiddeld 52 minuten, p < 0.001) en dientengevolge een kortere operatieduur (gemiddeld 67 minuten, p < 0.001). Vanuit het perspectief van de MKA-chirurg gebruik van IMFS is significant veiliger. In dit onderzoek werden 8 (30.7%) prikaccidenten waargenomen, waarvan allen voorkwamen bij het aanbrengen van winterspalken (p = 0.003). Er werden weinig IMFS-gerelateerde complicaties waargenomen: 1 (0.53%) wortel raakte beschadiging door het indraaien van een IMFS. Eén schroef uit 188 schroeven faalde (breuk) tijdens het indraaien. Zes (3.2%) schroeven kwamen los tijdens de 6 weken helingsperiode, waarvan het bij 3 schroeven nodig was om terug te plaatsen om functionele therapie toe te passen. In vergelijking met bestaande literatuur is de incidentie van complicaties laag. De pijnscores waren allen lager in de IMFS-groep in vergelijking met de winterspalk-groep, inclusief de gemiddelde pijn van de eerste week en de pijnscore bij verwijderen van IMFS of winterspalken.
Bergh, Bart vd.indd 132 23-10-15 16:35

Dutch summary
133
Gebruik van IMFS leidt tot dezelfde goede occlusale resultaten als gebruik van winterspalken. Drie patiënten ontwikkelden een suboptimale occlusie: 1 patiënt was behandeld met IMFS, en 2 patiënten waren behandeld met winterspalken. Mucosale afwijkingen/beschadigingen werden waargenomen bij 22 patiënten, gelijk verdeeld over beide onderzoeksgroepen. In de winterspalk-groep was er gingiva-hyperplasie van de interdentale papillen. In de IMFS-groep werd partiële overgroei van mucosa gezien. Na het beoordelen van de onderzoeksresultaten, en de voordelen en de nadelen van gebruik van IMFS, kan geconcludeerd worden dat IMFS is een betere methode om IMF te bewerkstelling. In vergelijking met winterspalken, leidt gebruik van IMFS tot minder pijn, dezelfde occlusale resultaten, kortere operaties, betere mogelijkheden tot behandeling onder lokale verdoving en minder prikaccidenten. IMFS zijn veiliger voor patiënt en behandelaars.
Hoofdstuk 6: “ Gebruik van IMF-schroeven of winterspalken als gesloten behandeling voor mandibulaire collumfracturen: een kwaliteit van leven-analyse.”
De resultaten van dit kwaliteit-van-leven onderzoek zijn grotendeels in het voordeel van IMFS. Patiënten behandeld met IMFS ervaren minder sociale isolatie en minder problemen met eten. Patiënten behandeld met IMFS geven aan het idee te hebben een normaal dieet tot zich te kunnen nemen. Daarnaast lijken IMFS een lager negatief eff ect te hebben op de sociale en fi nanciële situatie van een patiënt. Deze conclusie is gebaseerd op het feit dat 36% van de personen die een patiënt vergezelde die behandeld was met winterspalken, hiervoor een baan afzegden.Er werd in beide groepen geen verschil in de mogelijkheid tot spreken gezien. In hedendaagse literatuur zijn geen gegevens bekend over kwaliteit-van-leven bij een of andere vorm van IMF. Deze resultaten zijn daarom uniek, en kunnen mogelijk dienen als uitgangspunt voor toekomstige onderzoeken.
Bergh, Bart vd.indd 133 23-10-15 16:35

134
Hoofdstuk 7: “ Postoperatieve beeldvorming na maxillofaciaal trauma: zinvol of zinloos?”
De doelstelling van het huidige onderzoek was om de noodzaak voor het maken van postoperatieve beeldvorming bij patiënten met aangezichtsfracturen, te beoordelen. Daarnaast was een doelstelling om deze resultaten te vergelijken met bestaande literatuur. Een retrospectieve analyse werd uitgevoerd waarin alle chirurgisch behandelde patiënten in het VU medisch centrum (Amsterdam) in de periode 2000-2010 werden beoordeeld. In totaal werden 579 patiënten met 646 fracturen geïdentificeerd, hiervan werden 16 (2.8%) patiënten opnieuw geopereerd omdat de initiële therapie niet tot een goede repositie en fixatie had geleid. De beslissing om opnieuw te opereren was voornamelijk gebaseerd op klinische bevindingen (15 patiënten, 94%), deze bevindingen werden bevestigd door radiografische analyses. Bij één (6%) patiënt bleek de beslissing om opnieuw te opereren gebaseerd op alléén de radiografische analyses. Deze patiënt werd tijdens dezelfde opname opnieuw behandeld omdat bij beeldvorming gebleken was dat de behandelde arcus zygomaticus-fractuur bij de eerste behandeling suboptimaal gereduceerd was.Deze resultaten leidden tot de conclusie dat routinematig postoperatieve radiografie niet nodig is na chirurgische behandeling van aangezichtsfracturen. Deze resultaten komen overeen met bestaande literatuur. Vergeleken met deze literatuur wordt een relatief hoog percentage van herbehandelingen gezien, hetgeen vermoedelijk kan worden verklaard door enerzijds de langere duur van follow-up en anderzijds door de inclusie van complexe craniofaciale fracturen.Peroperatieve analyse van de repositie en de direct postoperatieve klinische symptomen zijn betere indicatoren om de behandeling te evalueren. Postoperatieve beeldvorming zou behouden moeten blijven voor patiënten met klachten of klinisch waarneembare afwijkingen die kunnen passen bij complicaties. Daarnaast kan het nemen van postoperatieve beeldvorming overwogen worden bij patiënten met complexe aangezichtsfracturen en voor onderwijsdoeleinden. Het vermijden van routinematige postoperatieve beeldvorming zal leiden tot een reductie in ioniserende straling, kostenreductie en mogelijkerwijs een efficiëntere opnamebeleid.
Bergh, Bart vd.indd 134 23-10-15 16:35

Bergh, Bart vd.indd 135 23-10-15 16:35

Bergh, Bart vd.indd 136 23-10-15 16:35
List of publications
Bergh, Bart vd.indd 137 23-10-15 16:35

List of publications:
• IMF-screws or arch bars as conservative treatment for mandibular condyle fractures: the quality of life-aspects. Van den Bergh B, De Mol van Otterloo JJ, Van der Ploeg T, Tuinzing DB, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2015 Sep;43(7):1004-9
• Conservative treatment of a mandibular condyle fracture: Comparing intermaxillary fixation with screws or arch bar. A randomised clinical trial. Van den Bergh B, Blankestijn J, Van der Ploeg T, Tuinzing DB, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2015 Jun;43(5):671-6.
• Does the advent of modern implant systems and refinement of free flap techniques negate the effect of radiotherapy in patients with oral cancer undergoing dental implant-based oral rehabilitation? Hammond D, Dover MS, Parmar S, McMillan K, Van den Bergh B, Bayoumi S. Oral Surgery 2014 Dec.
• Dysocclusion after maxillofacial trauma: a 42-year analysis. Kommers SC, Van den Bergh B, Boffano P, Verweij KP, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2014 Oct;42(7):1083-6.
• A ten-year analysis of the traumatic maxillofacial and brain injury patient in Amsterdam: incidence and aetiology. Salentijn EG, Peerdeman SM, Boffano P, Van den Bergh B, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2014 Sep;42(6):705-10.
• The clinical and radiographical characteristics of zygomatic complex fractures: a comparison between the surgically and non-surgically treated patients. Salentijn EG, Boverhoff J, Heymans MW, Van den Bergh B, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2014 Jul;42(5):492-7.
• Quality of life after open versus closed treatment for mandibular condyle fractures: a review of literature. Kommers SC, Van den Bergh B, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2013 Dec;41(8):e221-5.
• Long-term results and complications after treatment of bilateral fractures of the mandibular condyle. Forouzanfar T, Lobbezoo F, Overgaauw M, de
Bergh, Bart vd.indd 138 23-10-15 16:35

139
List of publications
Groot A, Kommers S, van Selms M, Van den Bergh B. British Journal of Oral And Maxillofacial Surgery. 2013 Oct;51(7):634-8.
• A 10-year analysis of the “Amsterdam” protocol in the treatment of zygomatic complex fractures. Forouzanfar T, Salentijn E, Peng G, Van den Bergh B. Journal of Cranio-Maxillo-Facial Surgery. 2013 Oct;41(7):616-22.
• A ten-year analysis of midfacial fractures. Salentijn EG, Van den Bergh B, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2013 Oct;41(7):630-6.
• The epidemiological characteristics of zygomatic complex fractures: A comparison between the surgically and non-surgically treated patients. Salentijn EG, Boff ano P, Boverhoff J, Van den Bergh B, Forouzanfar T. National Journal of Maxillofacial Surgery. 2013 Jul;4(2):214-8.
• Clinical outcomes of surgical management of anterior bilateral mandibular fractures. Boff ano P, Gallesio C, Roccia F, Van den Bergh B, Forouzanfar T. Journal of Craniofacial Surgery. 2013 Jul;24(4):e387-90.
• Aetiology and incidence of maxillofacial trauma in Amsterdam: a retrospective analysis of 579 patients. Van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2012 Sep;40(6):e165-9.
• Is thromboembolism prophylaxis necessary for low and moderate risk patients in maxillofacial trauma? A retrospective analysis. Skorpil N, Van den Bergh B, Heymans MW, Forouzanfar T. International Journal of Oral and Maxillofacial Surgery. 2012 Aug;41(8):902-5.
• Treatment and complications of mandibular fractures: a 10-year analysis. Van den Bergh B, Heymans MW, Duvekot F, Forouzanfar T. Journal of Cranio-Maxillo-Facial Surgery. 2012 Jun;40(4):e108-11.
• Post-operative radiographs after maxillofacial trauma: Sense or nonsense? Van den Bergh B, Goey Y, Forouzanfar T. International Journal of Oral and Maxillofacial Surgery. 2011 Dec;40(12):1373-6.
• A 10 years analysis of mandibular fractures. Van den Bergh B, Van Es C, Forouzanfar T. Journal of Craniofacial Surgery. 2011 Sep; 22(5):1631-4.
Bergh, Bart vd.indd 139 23-10-15 16:35

Bergh, Bart vd.indd 140 23-10-15 16:35

Dankwoord / Acknowledgements
Dankwoord / Acknowledgements
Bergh, Bart vd.indd 141 23-10-15 16:35

142
Graag maak ik van deze mogelijkheid gebruik om iedereen te bedanken voor de hulp die zij op enigerlei wijze geboden hebben tijdens het uitvoeren van mijn onderzoek en het samenstellen van dit proefschrift. Veel dank ben ik hierbij verschuldigd aan de patiënten die bereid waren zich te laten onderwerpen aan mijn onderzoeken, en het vertrouwen dat zij hiermee in mij gesteld hebben.
Daarnaast wil ik enkele personen bij naam bedanken:
Prof.dr. T. Forouzanfar (promotor). Beste Tim, jij maakte mij enthousiast om te promoveren nog voordat ik met mijn opleiding begonnen was. Je had al direct enkele plannen en begeleidde me in het maken van de eerste stappen. In de beginperiode begeleidde je me en wekte je mijn interesse, later gaf je me de ruimte om mijn promotie zelf vorm te geven, waarvoor ik je bedank.
Prof.dr. D.B. Tuinzing (promotor). Beste Bram, jij raakte vooral betrokken bij het schrijven van de laatste artikelen en bij het daadwerkelijke afronden van mijn proefschrift. Eerder al toonde je veel interesse in mijn onderzoek, omdat het veel overeenkomsten vertoonde met jouw eerste onderzoek, dat ook trauma-gerelateerd was. Ik wil je hartelijk danken voor de goede feedback en niet-aflatende enthousiasme.
Dr. J.J. de Mol van Otterloo (co-promotor). Beste Just, ik ben je dankbaar voor je op- en aanmerkingen tijdens het samenstellen van de laatste 2 artikelen. Bijzonder vind ik het ook dat je niet alleen mijn co-promotor bent, maar dat wij in het dagelijkse werkzame leven ook directe collega’s zijn. Ik bewonder je om je hoge kennisniveau wanneer het gaat om orale pathologie, orale implantologie als orthognatische chirurgie. Ik vermoed dat je tot een uitstervend ras van allround MKA-chirurgen behoort. Ik vind het een eer dat jij mijn co-promotor bent.
Leden van de beoordelingscommissie. Prof.dr. A.G. Becking, prof.dr. R.R.M. Bos, prof.dr. R. Koole, prof.dr. F. Lobbezoo, prof.dr. J.P.R. van Merkesteyn, u allen ben ik veel dank verschuldigd voor het beoordelen van mijn thesis en voor de opbouwende feedback. Deze feedback heeft het geheel kwalitatief doen toenemen.
Bergh, Bart vd.indd 142 23-10-15 16:35

143
Dankwoord / Acknowledgements
Maatschap MKA Kennemerland. Beste Joppe, Eddy, Just, Jeroen, Hylke en (straks ook) Volken, de afgelopen tijd was een roerige. Ik heb me altijd gesteund gevoeld, en zonder jullie support zou in de afgelopen tijd veel onmogelijk zijn geweest. Ik wil jullie daarvoor hartelijk danken. In het bijzonder zou ik op deze plaats prof.dr. A.G. Becking willen danken: beste Eddy, niet alleen ben ik je veel dank verschuldigd voor de begeleiding van mijn eerste jaren als MKA-chirurg, maar ook voor de energie en doortastendheid waarmee je mijn thesis doorgenomen hebt. Hier heb ik zeer veel aan gehad. Ik voel me zeer vereerd dat jij zitting hebt in de beoordelingscommissie.Drs. H. Schouten. Beste Hylke, we leerden elkaar kennen toen jij als parttime stafl id van de afdeling MKA-chirurgie werkzaam was in het VUmc. Sinds mijn toetreden in de maatschap is onze band eigenlijk echt ontstaan. De voor jouw typerende humor gecombineerd met je relativeringsvermogen en professionaliteit, maakt dat het heel fi jn werken is met je. Ik ben blij dat je mijn paranimf bent.
Lieve Koen, vaak heb ik met je gesproken over de voortgang van mijn promotieonderzoek, en vaak heb je mij aangespoord om het proefschrift een keer af te maken. Zo gaf je me onder andere het advies om mezelf ergens een paar dagen op te sluiten. Gelukkig is dat laatste niet nodig geweest, en heeft het toch geleid tot een afronding. Ik prijs me gelukkig met zo’n broer.
Dank aan alle medeauteurs voor de hulp en steun die zij gegeven hebben tijdens het uitvoeren van de onderzoeken en opstellen van de diverse artikelen. De statistici Martijn Heymans, Maurits van Selms en Tjeerd van der Ploeg waren van ongekend belang, aangezien statistiek niet tot mijn grootste talenten behoort. Ook een woord van dank aan prof.dr. F. Lobbezoo. Beste Frank, je stond direct open voor het onderzoek naar de lange termijn resultaten bij gesloten behandelde bilaterale collumfracturen. Je maakte veel tijd vrij om zelf ook patiënten te beoordelen, wat ik zeer gewaardeerd heb en heeft bijgedragen aan de kwaliteit van de studie. Daarnaast heb ik veel opgestoken van je opmerkingen over hoe een artikel op inhoud en vorm te verbeteren. Hartelijk dank voor je hulp, moeite en tijd.
Bergh, Bart vd.indd 143 23-10-15 16:35

Daarnaast wil ik Freya Duvekot, Circe van Es, Yilian Goey, Annemijn de Groot, Maarten Overgaauw en Gina Peng bedanken. Jullie hebben mij als bachelor-studenten enorm geholpen bij het vergaren van bergen gegevens uit honderden patiëntenstatussen. Zonder jullie zou het geheel niet tot stand zijn gekomen.Mr Attard, dear Alan, with much pleasure I look back on my stay in Birmingham, where I had the opportunity of working alongside you on maxfac-trauma. Thank you so much for this experience and for helping me edit the final version of my thesis. Hope to see you soon, ‘matey’!
Op deze plaats ook een woord van dank aan de stafleden, poli-assistentes en medewerkers van het secretariaat van de afdelingen MKA-chirurgie, van zowel het VUmc als MCA. Speciaal wil ik Hans Blankestijn bedanken, in zijn rol als perifeer opleider. Samen met zijn collega’s Rolf, Ignaz, Roeland, Manon, Roel en later ook Dorien, heb ik altijd vertrouwen gevoeld tijdens mijn opleiding maar ook zeker tijdens het uitvoeren van mijn IMF-schroef onderzoek. Ik heb begrepen dat in het MCA de ouderwetse winterspalken al plaats hebben gemaakt voor IMF-schroeven. Hulde!
Tijdens mijn afwezigheid op het VUmc, tijdens mijn perifere opleidingsjaar in Alkmaar, mijn buitenlandstage in Birmingham en na het afronden van mijn opleiding, is de continuïteit van mijn onderzoek in zowel het VUmc als het MCA altijd gewaarborgd gebleven door mijn dierbare AIOS-collega’s. Hoe enthousiast ook, en hoe goed protocollair ook vastgelegd, het doen van een multicenter-onderzoek vereist het hebben van goede ‘soldaten in het veld’, en daar heb ik veel geluk mee gehad. Veel dank!
Lieve dames van de poliklinieken MKA van de locaties Haarlem en Hoofddorp van het Spaarne Gasthuis, en van het Rode Kruis ziekenhuis Beverwijk, inmiddels ben ik alweer 2 jaar met jullie aan het werk. Bedankt voor de steun de afgelopen periode, ik vind het heel fijn om dagelijks met jullie te werken!
Lieve vrienden en familie, ook jullie veel dank voor de steun en de interesse in mijn onderzoek. Het is nu tijd voor een goed feest!
Lieve Martine, beste Roy, ook jullie wil ik bedanken voor jullie interesse.
Bergh, Bart vd.indd 144 23-10-15 16:35

145
Dankwoord / Acknowledgements
Beste Jaap, lieve Anke, ik prijs me gelukkig met zulke schoonouders. Jullie waren altijd geïnteresseerd in de voortgang van mijn onderzoek, waarvoor mijn dank. Gelukkig is het nu zover.
Lieve papa en mama, na 2 studies en een opleiding, is nu ook het promotieonderzoek afgerond! Veel dank voor jullie steun, ik weet zeker dat jullie erg trots zijn en hier veel van genieten.
Mijn lieve kleine aapjes Casper en Emmelie, vanaf nu een minder wegdromende papa, beloofd!
Lieve Sas, in goede tijden, maar ook in minder goede tijden, altijd de jouwe.
Bergh, Bart vd.indd 145 23-10-15 16:35

Bergh, Bart vd.indd 146 23-10-15 16:35

Curriculum vitae
Bergh, Bart vd.indd 147 23-10-15 16:35

Bergh, Bart vd.indd 148 23-10-15 16:35

149
Curriculum vitae
Bart van den Bergh was born on the 31st of December 1979. He completed high school (gymnasium) at the Hermann Wesselink College in Amstelveen in 1998. In 2007 he graduated from medical school at the VU University medical center Amsterdam. After fi nishing medical school, he started studying dentistry at the Radboud University Nijmegen, and graduated in 2010. In 2009 he started the Oral & Maxillofacial Surgery training, again in the VU University medical center Amsterdam (Prof. dr. I. van der Waal / Prof. dr. E.A.J.M. Schulten). His non-academic rotation was performed at Medical Centre Alkmaar (drs. J. Blankestijn, 2012). A 3-month trauma-oriented fellowship was undertaken at the Maxillofacial Surgery department in the Queen Elizabeth Hospital Birmingham, before he completed his Oral & Maxillofacial Surgery training in the summer of 2013. During his Oral & Maxillofacial Surgery training, he was chairman of the national association of Oral & Maxillofacial registrars (Landelijk Overleg Kaakchirurgen-in-Opleiding; (LOKO)).
The research described in this dissertation was conducted between 2009 and 2015 at the departments of Oral & Maxillofacial Surgery at the VU University Medical Center and Medical Centre Alkmaar. During the annual congress of the Dutch association of Oral & Maxillofacial Surgery (NVMKA) in 2012, he was awarded the Prof. dr. Marten Hut prize for a presentation on the article “Long-term results and complications after bilateral mandibular condyle fractures”, published in this thesis.
He presently works as a consultant Oral & Maxillofacial Surgery at the Spaarne Gasthuis Haarlem/Hoofddorp and Rode Kruis ziekenhuis Beverwijk.
He is married to Saskia, and has two children, Casper and Emmelie.
Bergh, Bart vd.indd 149 23-10-15 16:35

Bergh, Bart vd.indd 150 23-10-15 16:35

Bergh, Bart vd.indd 151 23-10-15 16:35

Bergh, Bart vd.indd 152 23-10-15 16:35