As chairman of NMMC’s Cancer Committee, I am … chairman of NMMC’s Cancer Committee, I am...
14
Transcript of As chairman of NMMC’s Cancer Committee, I am … chairman of NMMC’s Cancer Committee, I am...


As chairman of NMMC’s Cancer Committee, I am pleased to present the 2013Cancer Program Annual Report. The Cancer Committee is comprised of a multidisciplinary panel of specialists and ancillary personnel and provides leadership in ensuring the provision of quality patient care throughcancer-related activities that benefit not only patients and their families, but also our community. As an accreditedCancer Program by the American College of Surgeons’ (ACoS) Commission on Cancer (CoC), our goal is to ensureour community has access to a full range of cancer services, including a multidisciplinary approach to patient careand programs that impact survival and quality of life. These programs focus on prevention, early diagnosis, pre-treatment evaluation, staging, optimal treatment, clinical trials, rehabilitation services and surveillance for recurrentdisease, support services, hospice, patient navigation, survivorship and quality of life.
To that end, NMMC opened an inpatient hospice unit in January 2013. This 10-bed unit was renovated to provide a comfortable, homelike environment for patients and families. The inpatient hospice unit is designed to provide compassionate care to patients whorequire intensive management of complex symptoms related to their terminal illness.
For years, breast cancer has been one of the top five most common cancer diagnoses in northeast Mississippi and across the U.S. Toimprove care and services for patients with this disease, the Cancer Committee established a Breast Health Subcommittee in August 2013.In November, this committee began a weekly multidisciplinary Breast Cancer Conference. Conference attendees include physicians fromradiology, pathology, medical oncology, radiation oncology, plastic surgery and general surgery as well as other health care professionals who specialize in care of patients with this disease. Each patient with a new diagnosis of breast cancer is presented for discussion, and comprehensive, individualized treatment plans are formulated to meet each patient’s unique needs.
Benefits of Being an ACoS CoC Accredited Cancer ProgramACoS COC accredited cancer programs are surveyed on a triennial schedule. In 2013, NMMC’s Cancer Program received a three-yearaccreditation. The benefit to the community is not only excellence in patient care but also a cancer program and hospital that meet national standards. By participating in this survey, NMMC’s entire Cancer Program is held to a higher standard of care.
The CoC’s Accreditation Program offers many notable benefits that enhance a cancer program, including:• A model for organizing and managing a cancer program that ensures multidisciplinary,
integrated and comprehensive oncology services.
• Self-assessment of cancer program performance based on recognized standards.
• Recognition by national health care organizations, including The Joint Commission, for the establishment of performance measures for high-quality cancer care.
• The ability to provide robust oncology data for clinicians and other health care professionals, third-party payers, managed care organizations and the public from our required Cancer Registry.
• National marketing and public exposure through collaboration with the American Cancer Society (ACS) in the Facility Information Profile System (FIPS), which is an information-sharing program of resources, services and cancer data made available to the public by the ACS though their National Call Center and website.
• Participation in the National Cancer Data Base (NCDB); a nationwide oncology outcomes database for more than 1,400 hospitals in the United States.
• Access to hospital comparison benchmark reports containing national aggregate data and individual facility data to access patterns of care and outcomes.
• Participation in national studies developed to address important cancer-related problems.
• An Accredited Cancer Program Performance Report that will enable a facility to identify quality improvement initiatives by comparing its CoC compliance standards with other accredited programs statewide and within its accreditation award category.
Report from the Chairman
To promote team involvement and goal attainment, members of the committee
are appointed by the Chairman to coordinate specific areas of program activity.
These areas include:
Cancer Conference Coordinator: Robert McAuley, M.D.
Community Outreach Coordinator: Liz Dawson
Clinical Research Representative/Coordinator: Gayle Elliott, RN
QA Cancer Registry Coordinator: W. Ray Reed, M.D.
Quality Improvement Coordinator: Lee Greer, M.D.
Psychosocial Services Coordinator: Cindy Edwards, LMSW, OSW-C
Stephen Farmer, M.D.
2013 Program ActivityCoordinators

Cancer Program Goals for 2013:Each year, NMMC’s Cancer Committee establishes, implements and monitors atleast one clinical and one programmatic goal for endeavors related to cancer care.Clinical goals involve the diagnosis, treatment and care of patients. Programmaticgoals are directed toward the scope, coordination and processes of patient care.Each goal is evaluated at least twice annually, and the evaluation is documented in Cancer Committee minutes. Annual goals provide direction for the strategicplanning of cancer program activities and serve as the basis for cancer program evaluation.
Clinical goals selected for 2013 include monitoring rates of infection acquiredthrough the use of central intravenous lines and indwelling urinary catheters, aswell as reviewing the efficacy of the PET/CT sodium fluoride bone scan procedure.
Programmatic goals selected were the addition of a dedicated clinical dietitian toexisting cancer program services, the accreditation of the Breast Care Center andmonitoring of time required for obtaining results of flow cytometry testing forleukemia patients.
2013 Annual Oncology ConferenceIn addition to regularly scheduled tumor conferences, the Cancer Committee offers at least one cancer-related educational activity yearly to physicians, nursesand other allied health professionals. This activity is focused on the use of AJCC or other appropriate staging in clinical practice, which includes the use of appropriate prognostic indicators and evidence-based national guidelines used in treatment planning. Providing quality education with the goal of a multidisciplinary team approach to coordinate the best treatment options is anessential component of both ACoS CoC and American College of Radiology (ACR) accreditation.
Rapid Quality Reporting System (RQRS) The CoC developed the RQRS to facilitate quality improvement by encouragingevidence-based care in accredited programs for select quality measures. From initial enrollment through the three-year accreditation period, cancer programsthat participate in RQRS submit all eligible cases for all evaluation of valid performance measures, and adhere to RQRS terms and conditions. Followingrequired enrollment by key members of NMMC’s Cancer Committee, NMMC beganparticipation and enrollment January 1, 2014.
ClosingI am proud and honored to have been Chairman of NMMC’s Cancer Committee. It gives me great pleasure to work alongside other members who have the same commitment to excellence in cancer care. In keeping with NMMC’s stated mission, the Cancer Program at NMMC offers some of the most advanced medical treatments along with support services and educational programs to continuously improve the health and well-being of the patients we serve.
Stephen Farmer, M.D., Chairman, Cancer Committee
Report from the Chairman
2013 Cancer CommitteeMembers
Stephen Farmer, M.D., Chairman, Urology
Montgomery Berry, M.D., Otolaryngology
Carl Bevering, M.D., NeurosurgeryRobert Derveloy, M.D., Cardiothoracic SurgeryAlbert Chang, M.D., Ph.D., Diagnostic Radiology Paul Farabaugh, M.D., CLP, UrologyDavid Gilliland, M.D., CLP, SurgeryLee Greer, M.D., QI CoordinatorRichard Griswold, M.D., PathologyJeff Houin, M.D., DermatologyAndrew Kellum, M.D., Medical OncologyRhodemarie Maron, M.D., Neurology*Robert McAuley, M.D., Surgery, Cancer Conference
CoordinatorRichard McAdory, M.D., Surgery, Vice-ChairmanCharles Montgomery, M.D., Medical Oncology*John Phillips, M.D., GastroenterologyRay Reed, M.D., Radiation Oncology, Cancer Registry
Quality CoordinatorJim Rish, M.D., PulmonologyDaniel Schroyer, M.D., Radiation Oncology*Octavius Ivy, Service Line AdministratorBeth Bryant, MSN, JD, Cancer Services AdministratorShelia Jinkins, CTR, Cancer RegistryCindy Edwards, LMSW, OSW-C, Psychosocial Services
CoordinatorTheresa Jenkins, RN, OncologyJeannine Peters, Pharm.D., Outpatient Infusion*Tina Stevens, RN, Breast Care CenterErin Watson, RN, Oncology*Rachel Wood, MS, RD, CSO, LDRachelle Carter, Pharm.D.Krista Kirksey, ACSLiz Dawson, Community Outreach Coordinator
*Alternates
The Cancer Committee is a multidisciplinary standingcommittee consisting of members of the active medicalstaff representing hematology/oncology, pathology, radiation oncology, diagnostic radiology, dermatology,gastroenterology, pulmonary, neurosurgery, otolaryn-gology, cardiothoracic, urology and surgery. Non-physician members include representatives fromadministration, food and nutrition services, nursing,quality improvement, social work, community health,psychosocial services, pharmacy, American CancerSociety representative and the cancer registry.
The NMMC Cancer Committee meets quarterly andprovides leadership to plan, initiate, stimulate, andassess all cancer-related activities within the NMMCsystem. The committee establishes yearly goals and priorities.

DataAnalysis
The North Mississippi Medical Center Cancer Program is a multidisciplinary program accredited by the American College of Surgeons (ACoS) and the American College of Radiology (ACR). Being nationally accredited ensures that NMMC adheres to the highest quality standards and allows comparison of treatment and outcomes on a local, state and national level.
The tables and graphs included in this report contain data maintained in the NMMC Cancer Registry forcalendar year 2013. During 2013, a total of 1,807 cases were added to our cancer registry database. Ofthose, 1,622 were analytic, which means these patients received all or part of their diagnosis and treatmentat NMMC. Cancer of the lung is the most prevalent site with 308 new cases. Breast cancer is the secondmost common site with 255 cases, and prostate is third with 180 cases. In fourth and fifth place werecolon with 110 and melanoma with 85. Diagnosis and treatment throughout our service area had animpact on 30 counties in Mississippi and multiple counties in Alabama and Tennessee. The county breakdown reflects the widespread service area for our Cancer Program. Counties with the highest number of cases include: Lee, Monroe, Pontotoc, Itawamba, Chickasaw and Union counties.
The top five primary sites have remained relatively consistent over the past five years. This is evidence thatNMMC has a strong program for treating these cancers. Overall, our top five sites represent approximately 58 percent of the total cancer population seen at NMMC.
We continue to meet or exceed national outcomes when comparing five-year survival rates. The NMMC CancerProgram continues to offer cutting edge treatments and ongoing studies, which will add to eventual improvementin long-term survival.
The Cancer Committee will continue to use the Cancer Registry’s data to provide effective screening programsthat will increase early detection and diagnosis among residents of our communities. Early detection in the waragainst cancer is extremely important for long-term survival. It is the goal of the Cancer Committee to support all efforts to increase the early diagnosis of cancer and take the lead in this endeavor.
NMMC’s team of physicians and other health care professionals are committed to providing state-of-the-art cancertreatment in a compassionate and cost-effective manner.
The statistical data graphed in this report includes: Primary Site Table, Sex, Race, Top 5 Sites, Top 5 Sites by Sex,Age at Diagnosis and Geographic Location.
Stephen McAdory, M.D.Vice Chairman, Cancer Committee
Stephen McAdory, M.D.Vice Chairman
Cancer Committee
The NMMC Cancer Center is continuously looking for ways to improve care and serve our community…
that’s good to know.

DeSoto Marshall Benton
Tippah
Alcorn
Tish
omin
go
Prentiss
Yalobusha
Humphreys HolmesAttala
Yazoo
Madison
Issaq
uena
Hinds
Tate
Panola LafayetteUnion
Pontotoc
Warren
Claiborne
Jefferson
Adams
Shar
key
Franklin
Wilkinson
Amite
Lee Itawamba
MonroeChickasawCalhoun
Grenada
Tallahatchie
LeFloreCarroll
Mon
tgom
ery
Tunica
QuitmanCoahoma
Bolivar
Sunf
low
er
Washington
Copiah
Lincoln
Pike
Leake
WebsterClay
Oktibbeha Lowndes
NoxubeeWinston
Neshoba Kemper
LauderdaleNewtonScott
Rankin
ClarkeJasperSmith
WayneJonesCovington
JeffersonDavisLa
wre
nce
Simpson
StoneGeorge
Jackson
Harrison
Hancock
GreenePerryForrest
LamarMarion
Walthall
Pearl River
Choctaw
Top FivePrimary Sites
RaceCaucasian..........................................1,305African-American ................................315Hawaiian ..................................................1Asian Indian ............................................1
SexMale ....................................................869Female ................................................753
Top 5 OverallLung ....................................................308Breast ..................................................255Prostate ................................................180Colon ..................................................110Melanoma/Skin ......................................85
Age At Diagnosis0-29 ......................................................2230-39 ....................................................5140-49 ..................................................15650-59 ..................................................30360-69 ..................................................49470-79 ..................................................39780-89 ..................................................18490+ ........................................................15
Total Mississippi............................1,535Alabama ............................................75Tennessee ............................................9Illinois..................................................1Louisiana..............................................1Utah ....................................................1Total Analytic Cases ..................1,622
More than 400 patients
100-200 patients
50-99 patients
15-49 patients
Less than 15 patients
Geographic Location:
Lung180
Prostate180
Colon71
Bladder63
Melanoma42
Breast254
Lung128
Melanoma43
Colon 39
Hemato-poietic
33
Demographic DataAll Analytic Patients

LiaisonReport
Who is a Cancer Liaison Physician?A Cancer Liaison Physician (CLP) is a leader of the cancer program,someone who will support the facility’s efforts in complying with andmaintaining the Commission on Cancer (CoC) standards, facilitateactivities with the interests of the cancer patients, NMMC and the community in mind, and is dedicated to improving the quality of caredelivered to the cancer patient.
The Cancer Liaison Physician serves as a link between the hospital andthe community, between the national standards organizations and thehospital, and between the Cancer Committee and the various depart-ments at North Mississippi Medical Center. For example, the liaison collaborates with the Cancer Committee to meet and exceed cancer program standards and improve clinical practice. CLPs serve a three-year term with eligibility to serve an unlimited number of terms.
In particular, the liaison works with the multispecialty cancer teams todevelop best practices, evaluate compliance with adopted guidelines,expand participation in clinical trials, and improve quality of care. Theliaison also works with local agencies and the American Cancer Societyon community outreach and education as well as participates in peergroup meetings to provide direction according to criteria established by the American College of Surgeons Commission on Cancer.
CLP Selection Criteria • The CLP position is a required component of CoC-accredited
cancer programs.• The CLP serves a three-year term with eligibility to serve an unlimited
number of terms based on performance as assessed by the CoC and the Cancer Committee.
• The CLP is a required member of the cancer committee. • The CLP is a member of the medical staff. The Cancer Committee
must ensure that the physician is authorized to access facility-specific information that is maintained by the CoC.
• The CLP serves as the liaison among the cancer program, the CoC and the American Cancer Society.
• The CLP can fulfill a leadership position within the cancer committee such as chair, vice chair or quality improvement coordinator.
Primary Responsibility The primary responsibilities of the Cancer Liaison Physician are to monitor, interpret and report the program’s performance using NCDBdata to evaluate and improve the quality of care. The CLP reports anddiscusses the facility’s performance and response related to the account-ability and quality improvement measures or other NCDB facility datawith the Cancer Committee four times each year. A quality-related auditis initiated for any of the accountability and quality improvement measures that fall below required levels of compliance.
Cancer Program Practice Profile Reports (CP3R)To monitor quality initiatives, the Commission on Cancer has createdthe CP3R site. This site allows facilities to monitor compliance withquality initiatives related to breast, colon and rectal cancers and to compare their performance with other accredited facilities in the state,region, with similar classification, or all other accredited facilities.NMMC can monitor performance over time looking for trends inpatient care. Many times these trends may be related to changes in datacapture or difficulty obtaining information on a timely basis. The NMMCCancer Registry audits these cases periodically and takes extra measures
to collect missing data and update these reports. The Cancer LiaisonPhysician reports the data to the Cancer Committee, whose responsibilityis to monitor the data, identify any measure that falls below requiredlevels of compliance and work to resolve these issues appropriately.Discussions are documented in Cancer Committee minutes and subsequently shared with the medial staff and administration.
American Cancer Society/Commission on Cancer working together
The Cancer Liaison Physician helps make the connection between theAmerican Cancer Society and the Commission on Cancer. • The Society and the College have a long-standing partnership that dates
to the founding of both organizations in 1913. • The Society is a member organization of the Commission on Cancer and
supports the National Cancer Data Base and the Cancer Liaison Program with more than $1 million in funding annually.
• The two organizations collaborate at the national, state and local levels in cancer control, research and community outreach initiatives.
• Visitors to cancer.org and the Society’s National Cancer Information Center (1.888.227.2345) are referred to the CoC Hospital Locator and local support groups and services offered at CoC- accredited programs.
• Local Society staff can provide CoC-accredited programs and staff with information on Society resources and patient offerings that support CoC accreditation standards.
The Cancer Program and its team of physicians, nurses and staff havecontinued their progress in quality and service throughout 2013.Inspiration is present all around us as we recognize the accomplishmentsof our staff and courageous patients. As we approach 2014, we remaincommitted to growth and improvements in the exceptional services atNMMC. Our staff, nurses, and physicians are champions of compassion-ate patient care and talented in their expertise of oncology. Our breastcancer patients continue to experience the higher level of care at theBreast Care Center and assistance in the early diagnosis and treatmentthrough the weekly multidisciplinary Breast Conference.
We have been inspired to achieve excellence in care by the courageousfriends, families and patients visiting our campus daily. Our staff, nurses and physicians at NMMC remain committed to our high standards of cancer care and truly rise to the challenges of consistentgrowth, compassionate care and improvement of the experience andquality of our exceptional services.
Paul Farabaugh, M.D., CLPDavid Gilliland, M.D., CLP
Paul Farabaugh, M.D. David Gilliland, M.D.Cancer Liaison Physician Cancer Liaison Physician
The Commission on Cancer works through cancer programs andhealth care professionals to serve the
community, patients and families.
The American Cancer Society works through the community
to serve the community, patients and families
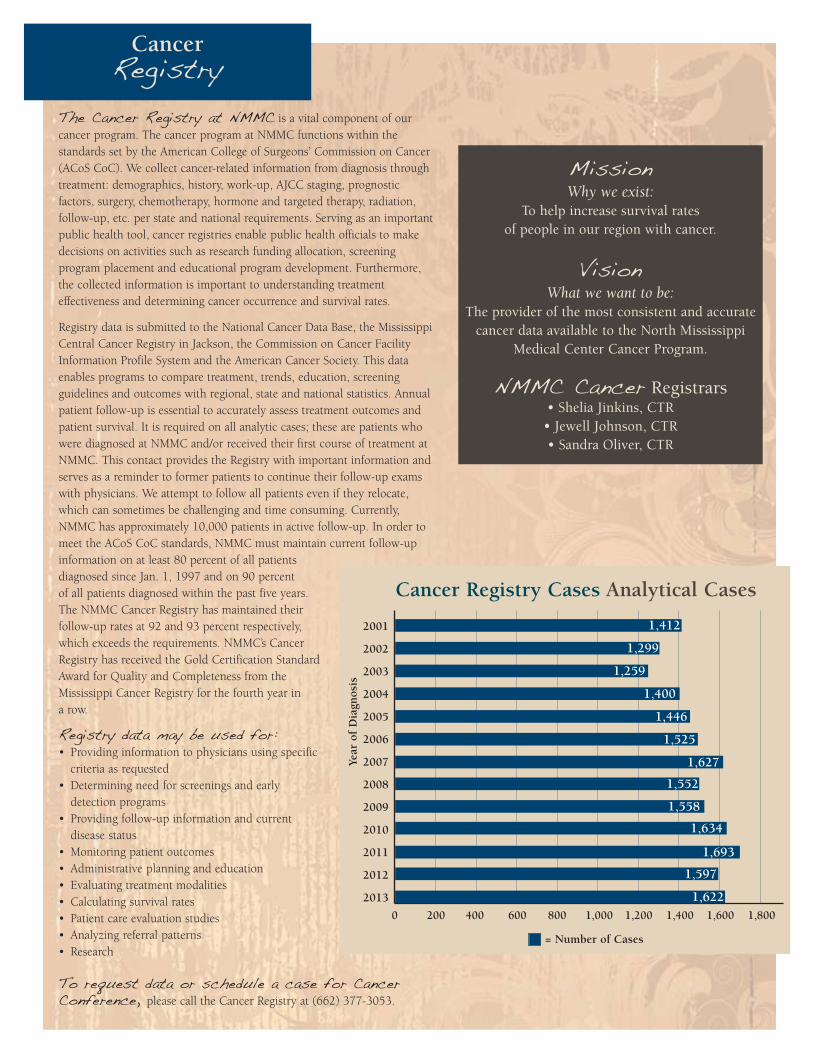
The Cancer Registry at NMMC is a vital component of ourcancer program. The cancer program at NMMC functions within the standards set by the American College of Surgeons’ Commission on Cancer(ACoS CoC). We collect cancer-related information from diagnosis throughtreatment: demographics, history, work-up, AJCC staging, prognostic factors, surgery, chemotherapy, hormone and targeted therapy, radiation,follow-up, etc. per state and national requirements. Serving as an importantpublic health tool, cancer registries enable public health officials to makedecisions on activities such as research funding allocation, screening program placement and educational program development. Furthermore,the collected information is important to understanding treatment effectiveness and determining cancer occurrence and survival rates.
Registry data is submitted to the National Cancer Data Base, the MississippiCentral Cancer Registry in Jackson, the Commission on Cancer FacilityInformation Profile System and the American Cancer Society. This dataenables programs to compare treatment, trends, education, screening guidelines and outcomes with regional, state and national statistics. Annualpatient follow-up is essential to accurately assess treatment outcomes andpatient survival. It is required on all analytic cases; these are patients whowere diagnosed at NMMC and/or received their first course of treatment atNMMC. This contact provides the Registry with important information andserves as a reminder to former patients to continue their follow-up examswith physicians. We attempt to follow all patients even if they relocate,which can sometimes be challenging and time consuming. Currently,NMMC has approximately 10,000 patients in active follow-up. In order tomeet the ACoS CoC standards, NMMC must maintain current follow-upinformation on at least 80 percent of all patients diagnosed since Jan. 1, 1997 and on 90 percentof all patients diagnosed within the past five years. The NMMC Cancer Registry has maintained their follow-up rates at 92 and 93 percent respectively,which exceeds the requirements. NMMC’s CancerRegistry has received the Gold Certification StandardAward for Quality and Completeness from theMississippi Cancer Registry for the fourth year in a row.
Registry data may be used for:• Providing information to physicians using specific
criteria as requested• Determining need for screenings and early
detection programs• Providing follow-up information and current
disease status• Monitoring patient outcomes• Administrative planning and education• Evaluating treatment modalities• Calculating survival rates• Patient care evaluation studies• Analyzing referral patterns• Research
To request data or schedule a case for CancerConference, please call the Cancer Registry at (662) 377-3053.
MissionWhy we exist:
To help increase survival ratesof people in our region with cancer.
VisionWhat we want to be:
The provider of the most consistent and accuratecancer data available to the North Mississippi
Medical Center Cancer Program.
NMMC Cancer Registrars• Shelia Jinkins, CTR
• Jewell Johnson, CTR• Sandra Oliver, CTR
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Cancer Registry Cases Analytical Cases
0 200 400 600 800 1,000 1,200 1,400 1,600 1,800
Year
of
Dia
gnos
is
= Number of Cases
1,634
1,693
1,400
1,446
1,525
1,627
1,552
1,558
1,597
1,622
1,259
1,299
1,412
CancerRegistry
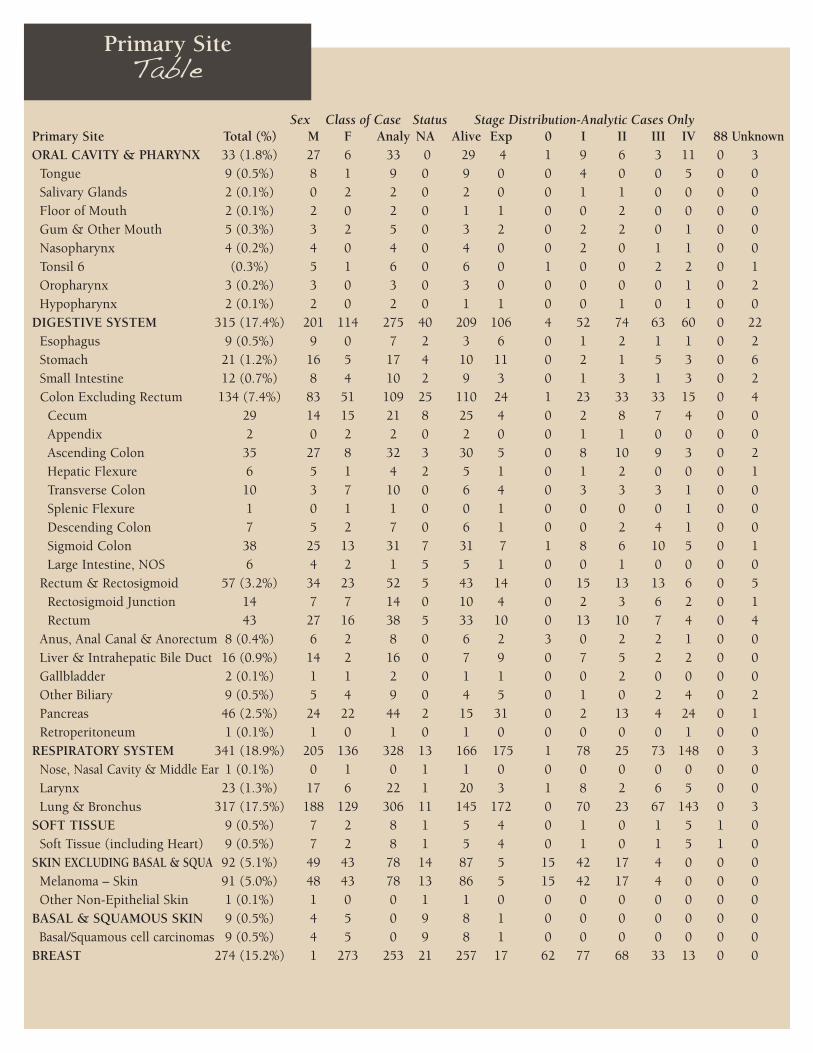
Sex Class of Case Status Stage Distribution-Analytic Cases Only Primary Site Total (%) M F Analy NA Alive Exp 0 I II III IV 88 UnknownORAL CAVITY & PHARYNX 33 (1.8%) 27 6 33 0 29 4 1 9 6 3 11 0 3
Tongue 9 (0.5%) 8 1 9 0 9 0 0 4 0 0 5 0 0 Salivary Glands 2 (0.1%) 0 2 2 0 2 0 0 1 1 0 0 0 0Floor of Mouth 2 (0.1%) 2 0 2 0 1 1 0 0 2 0 0 0 0Gum & Other Mouth 5 (0.3%) 3 2 5 0 3 2 0 2 2 0 1 0 0Nasopharynx 4 (0.2%) 4 0 4 0 4 0 0 2 0 1 1 0 0Tonsil 6 (0.3%) 5 1 6 0 6 0 1 0 0 2 2 0 1Oropharynx 3 (0.2%) 3 0 3 0 3 0 0 0 0 0 1 0 2Hypopharynx 2 (0.1%) 2 0 2 0 1 1 0 0 1 0 1 0 0
DIGESTIVE SYSTEM 315 (17.4%) 201 114 275 40 209 106 4 52 74 63 60 0 22Esophagus 9 (0.5%) 9 0 7 2 3 6 0 1 2 1 1 0 2Stomach 21 (1.2%) 16 5 17 4 10 11 0 2 1 5 3 0 6Small Intestine 12 (0.7%) 8 4 10 2 9 3 0 1 3 1 3 0 2Colon Excluding Rectum 134 (7.4%) 83 51 109 25 110 24 1 23 33 33 15 0 4
Cecum 29 14 15 21 8 25 4 0 2 8 7 4 0 0Appendix 2 0 2 2 0 2 0 0 1 1 0 0 0 0Ascending Colon 35 27 8 32 3 30 5 0 8 10 9 3 0 2Hepatic Flexure 6 5 1 4 2 5 1 0 1 2 0 0 0 1Transverse Colon 10 3 7 10 0 6 4 0 3 3 3 1 0 0Splenic Flexure 1 0 1 1 0 0 1 0 0 0 0 1 0 0Descending Colon 7 5 2 7 0 6 1 0 0 2 4 1 0 0Sigmoid Colon 38 25 13 31 7 31 7 1 8 6 10 5 0 1Large Intestine, NOS 6 4 2 1 5 5 1 0 0 1 0 0 0 0
Rectum & Rectosigmoid 57 (3.2%) 34 23 52 5 43 14 0 15 13 13 6 0 5Rectosigmoid Junction 14 7 7 14 0 10 4 0 2 3 6 2 0 1Rectum 43 27 16 38 5 33 10 0 13 10 7 4 0 4
Anus, Anal Canal & Anorectum 8 (0.4%) 6 2 8 0 6 2 3 0 2 2 1 0 0Liver & Intrahepatic Bile Duct 16 (0.9%) 14 2 16 0 7 9 0 7 5 2 2 0 0Gallbladder 2 (0.1%) 1 1 2 0 1 1 0 0 2 0 0 0 0Other Biliary 9 (0.5%) 5 4 9 0 4 5 0 1 0 2 4 0 2Pancreas 46 (2.5%) 24 22 44 2 15 31 0 2 13 4 24 0 1Retroperitoneum 1 (0.1%) 1 0 1 0 1 0 0 0 0 0 1 0 0
RESPIRATORY SYSTEM 341 (18.9%) 205 136 328 13 166 175 1 78 25 73 148 0 3Nose, Nasal Cavity & Middle Ear 1 (0.1%) 0 1 0 1 1 0 0 0 0 0 0 0 0Larynx 23 (1.3%) 17 6 22 1 20 3 1 8 2 6 5 0 0Lung & Bronchus 317 (17.5%) 188 129 306 11 145 172 0 70 23 67 143 0 3
SOFT TISSUE 9 (0.5%) 7 2 8 1 5 4 0 1 0 1 5 1 0Soft Tissue (including Heart) 9 (0.5%) 7 2 8 1 5 4 0 1 0 1 5 1 0
SKIN EXCLUDING BASAL & SQUA 92 (5.1%) 49 43 78 14 87 5 15 42 17 4 0 0 0Melanoma – Skin 91 (5.0%) 48 43 78 13 86 5 15 42 17 4 0 0 0Other Non-Epithelial Skin 1 (0.1%) 1 0 0 1 1 0 0 0 0 0 0 0 0
BASAL & SQUAMOUS SKIN 9 (0.5%) 4 5 0 9 8 1 0 0 0 0 0 0 0 Basal/Squamous cell carcinomas 9 (0.5%) 4 5 0 9 8 1 0 0 0 0 0 0 0
BREAST 274 (15.2%) 1 273 253 21 257 17 62 77 68 33 13 0 0
Primary SiteTable

Sex Class of Case Status Stage Distribution-Analytic Cases Only Primary Site Total (%) M F Analy NA Alive Exp 0 I II III IV 88 UnknownFEMALE GENITAL SYSTEM 73 (4.0%) 0 73 58 15 65 8 5 26 5 7 12 0 3
Cervix Uteri 15 (0.8%) 0 15 9 6 13 2 0 3 3 2 1 0 0 Corpus & Uterus, NOS 36 (2.0%) 0 36 28 8 34 2 0 21 1 2 2 0 2
Corpus Uteri 35 0 35 27 8 33 2 0 21 0 2 2 0 2 Uterus, NOS 1 0 1 1 0 1 0 0 0 1 0 0 0 0
Ovary 15 (0.8%) 0 15 15 0 11 4 0 1 1 3 9 0 1 Vulva 7 (0.4%) 0 7 6 1 7 0 5 1 0 0 0 0 0
MALE GENITAL SYSTEM 226 (12.5%) 226 0 187 39 212 14 0 54 108 10 15 0 0 Prostate 218 (12.1%) 218 0 180 38 205 13 0 49 106 10 15 0 0 Testis 6 (0.3%) 6 0 6 0 5 1 0 4 2 0 0 0 0 Penis 2 (0.1%) 2 0 1 1 2 0 0 1 0 0 0 0 0
URINARY SYSTEM 165 (9.1%) 111 54 152 13 143 22 52 57 13 11 17 0 2 Urinary Bladder 89 (4.9%) 65 24 81 8 78 11 48 17 11 2 2 0 1 Kidney & Renal Pelvis 68 (3.8%) 41 27 65 3 59 9 0 40 1 8 15 0 1 Ureter 6 (0.3%) 4 2 5 1 5 1 3 0 1 1 0 0 0 Other Urinary Organs 2 (0.1%) 1 1 1 1 1 1 1 0 0 0 0 0 0
EYE & ORBIT 1 (0.1%) 1 0 1 0 1 0 0 0 0 0 0 1 0 BRAIN & OTHER NERVOUS SYSTEM 40(2.2%) 20 20 37 3 31 9 0 0 0 0 0 37 0
Brain 24 (1.3%) 13 11 22 2 15 9 0 0 0 0 0 22 0 Cranial Nerves Other Nervous System 16 (0.9%) 7 9 15 1 16 0 0 0 0 0 0 15 0
ENDOCRINE SYSTEM 56 (3.1%) 22 34 54 2 54 2 0 25 3 9 4 13 0 Thyroid 42 (2.3%) 15 27 41 1 40 2 0 25 3 9 4 0 0 Other Endocrine including Thymus 14 (0.8%) 7 7 13 1 14 0 0 0 0 0 0 13 0
LYMPHOMA 69 (3.8%) 36 33 65 4 55 14 0 17 19 13 15 0 1 Hodgkin Lymphoma 11 (0.6%) 7 4 10 1 8 3 0 1 2 5 2 0 0 Non-Hodgkin Lymphoma 58 (3.2%) 29 29 55 3 47 11 0 16 17 8 13 0 1
NHL - Nodal 34 24 10 32 2 29 5 0 6 11 8 6 0 1 NHL - Extranodal 24 5 19 23 1 18 6 0 10 6 0 7 0 0
MYELOMA 16 (0.9%) 12 4 15 1 9 7 0 0 0 0 0 15 0 LEUKEMIA 51 (2.8%) 27 24 45 6 40 11 0 0 0 0 0 45 0
Lymphocytic Leukemia 34 (1.9%) 18 16 28 6 29 5 0 0 0 0 0 28 0 Acute Lymphocytic Leukemia 2 2 0 2 0 0 2 0 0 0 0 0 2 0 Chronic Lymphocytic Leukemia 31 16 15 25 6 28 3 0 0 0 0 0 25 0 Other Lymphocytic Leukemia 1 0 1 1 0 1 0 0 0 0 0 0 1 0
Myeloid & Monocytic Leukemia15 (0.8%) 9 6 15 0 9 6 0 0 0 0 0 15 0 Acute Myeloid Leukemia 11 7 4 11 0 5 6 0 0 0 0 0 11 0 Chronic Myeloid Leukemia 3 1 2 3 0 3 0 0 0 0 0 0 3 0 Other Myeloid/Monocytic Leukemia 1 1 0 1 0 1 0 0 0 0 0 0 1 0
Other Leukemia 2 (0.1%) 0 2 2 0 2 0 0 0 0 0 0 2 0 Other Acute Leukemia 1 0 1 1 0 1 0 0 0 0 0 0 1 0 Aleukemic, Subleukemic & NOS 1 0 1 1 0 1 0 0 0 0 0 0 1 0
MESOTHELIOMA 3 (0.2%) 3 0 3 0 1 2 0 1 0 1 1 0 0 KAPOSI SARCOMA 1 (0.1%) 1 0 1 0 1 0 0 0 0 0 0 1 0 MISCELLANEOUS 33 (1.8%) 20 13 29 4 16 17 0 0 0 0 0 29 0
Total 1,807 973 834 1,622 185 1,389 418 140 439 338 228 301 142 34
Primary SiteTable

NMMC’s Cancer Committee continually works to bring our patients the highest quality cancer care. In 2013, the Committee completed a review of prostate cancer patientswho underwent robotic-assisted laparoscopic prostatectomy(RALP) as part of their treatment plan. RALP was first performedin 2000, and since then, introduction of devices such as the Da Vinci “robot” has caused this method to take the place of the more traditional open surgical approach. Currently, it is estimated that more than 70 percent of all prostatectomies performed in the United States are done using the RALP method.Studies show that RALP reduces hospital length of stay and therate of surgical and immediate post-surgical complications, aswell as re-admission for postoperative complication. However,since it is a relatively new technique, it is important to routinely measure its success when it comes to prostate cancer.
One of the obvious measures of success in cancer surgeries is clear surgical margins, meaning that all of the tumor has been successfully removed. In 2013, surgeons at NMMC performed atotal of 48 RALP procedures. Positive surgical margins (PSM), meaning there was residual tumor present, were found in only four of these cases. NMMC’s resulting 8.3 percent PSM rate is well below the 10.7 percent to 17.6 percent PSM rate reported in medical journals by researchers studying this procedure.NMMC’s low PSM rate means that the vast majority of ourpatients did not require more extensive or repeat surgery toachieve tumor removal. As always, NMMC will continue to monitor this and other prostate cancer treatments to ensure thatour patients receive the best care possible.
With the exception of skin cancer, prostate cancer is the mostcommon cancer in American men. For 2014, the AmericanCancer Society (ACS) estimates that 233,000 new cases ofprostate cancer will be diagnosed. Prostate cancer is the secondleading cause of cancer death in the U.S., and the ACS estimatesthat 29,480 men will die of the disease in 2014.
While prostate cancer can be a serious disease, most men diag-nosed with prostate cancer do not die from it. According to theACS, more than 2.5 million men in the U.S. who have been diag-nosed with prostate cancer at some point are still alive today.When caught early before it spreads to distant lymph nodes, thebones or other organs, the 10-year survival rates for prostate can-cer are almost 100 percent.
Although the cause of most prostate cancers remains unclear,there are some known risk factors for this disease:
• Risk increases rapidly after age 50; 60 percent of cases are diagnosed in men 65 or older.
• Prostate cancer occurs more often in African-American men, who are also more likely to be diagnosed at later stages, and are twice as likely to die from the disease as Caucasian males.
• Men with a father or brother who have had prostate cancer are at increased risk, especially if their relatives were diagnosed before age 50.
• Studies show that men who eat a lot of red meat and high-fat dairy products are at increased risk. As with many cancers, eating a diet rich in vegetables and fruits, being physically active and achieving and maintaining a healthy weight can lower the risk for prostate cancer.
Early prostate cancer usually causes no symptoms. Advanced cases can cause symptoms such as problems passing urine; blood in the urine; impotence; pain in the hips, spine, chest orother areas from spread of the cancer to the bones; weakness or numbness in the legs and feet, or loss of bowel or bladdercontrol from the cancer pressing on the spinal cord. Other diseases can cause many of these same symptoms, so it is important to report such symptoms to your doctor promptly so the cause can be found and treated appropriately.
The diagnosis of prostate cancer is usually made after a thorough medical history and physical exam, PSA blood testing,ultrasound and/or biopsy. Depending on the stage at diagnosis,treatment options can include active surveillance, surgery, radiation therapy, hormone therapy, vaccine therapy or bone-directed treatment. Treatment decisions are typically based on age and expected life span, the presence of other serious healthconditions, the stage and grade of the cancer, the treatment’s likelihood of success, the physician’s expert opinion and thepatient’s wishes and needs.
As with any cancer, the likelihood of successful treatment is best with early diagnosis. With respect to screening to increasethe chance for early diagnosis of prostate cancer, both the ACSand the American Urological Association recommend that beginning at age 50, men should talk to their health careprovider about their personal risk profile and what screenings are appropriate for them.
Prostate CancerAnalysis
Prostate CancerInformation

CancerConference
The Cancer Conference is held every Thursday at noon and offers multidisciplinary consultative services for patients,discussion among cancer program team members, and educational conferences for physicians and allied health professionals.
In 2012, a total of 44 conferences were held with 231 cases discussed. Ninety-eight percent of the cases were prospective presentations, discussing diagnosis, stage, treatment options and follow-up care. Among the leading sites presented were breast,lung, colon, prostate, bladder, pancreas, head and neck, melanoma and lymphoma. In addition to Cancer Conference, the cancer program offered two guest speakers for cancer-related educational activities to physicians, nurses and other allied healthcare professionals.
All of these activities related to the use of AJCC stage, other site-specific prognostic indicators and evidence-based nationaltreatment guidelines in planning treatment for cancer patients. NMMC is accredited by the Mississippi State MedicalAssociation to provide continuing medical education (CME) for physicians. Participation in Cancer Conference, an educationalactivity, earns one CME credit toward the AMA Physicians Recognition Award. Physicians may contact the Cancer Registry at(662) 377-3053 for more information, to schedule a patient to be presented at Cancer Conference, or to receive a currentmeeting schedule.
Stephen Amann, M.D.
John Averette, M.D.
Richard Arriola, M.D.
Robert Becker, M.D.
Montgomery Berry, M.D.
Carl Bevering, M.D.
Richard Hunt Bobo, M.D.
John Burk, M.D.
Albert Chang, M.D.
Doug Clark, M.D.
Curt Collins, M.D.
Mark Craig, M.D.
Chris Croot, M.D.
Robert Derveloy, M.D.
Jayant Dey, M.D.
Elbert Duncan, M.D.
Eric Emig, M.D.
Gideon Ewing, M.D.
Paul Farabaugh, M.D.
Stephen Farmer, M.D.
Leonil Gan Lim, M.D.
Edward Giaroli, M.D.
David Gilliland, M.D.
Richard Griswold, M.D.
Jimmy Hamilton, M.D.
Newt Harrison, M.D.
Kevin Harbour, M.D.
Ricky Hicks, M.D.
Julian Hill, M.D.
Jeff Howard, M.D.
Roger Huey, M.D.
Jeffrey Houin, M.D.
Mark Huffman, M.D.
Robert Jarrett, M.D.
C. Allen Justice, M.D.
Andrew Kellum, M.D.
Robert McAuley, M.D.
Cohra Mankey, M.D.
Rhodemarie Maron, D.O.
Stephen McAdory, M.D.
Hughes Milam, M.D.
David Morris, M.D.
Micah Monaghan, M.D.
Charles Montgomery, M.D.
Paul Perry, M.D.
Lyndon Perkins, M.D.
John Phillips, M.D.
Charles Pigott, M.D.
Terry Pinson, M.D.
David Reed, D.O.
W. Ray Reed, M.D.
James Rish, M.D.
Danny Sanders, M.D.
Daniel Schroyer, M.D.
Susan Shamburger, M.D.
Mark Shepherd, M.D.
Ryan Simmons, M.D.
Clint Smith, M.D.
Robert Stewart, M.D.
Jaime Ungo, M.D.
C.K. White, M.D.
Kris Whitehead, M.D.
Robert Yarber, M.D.
Physicians Presenting at Cancer Conference in 2013:
CommunityReport
Advancements in Cancer Care at NMMC
New PartnershipNorth Mississippi Medical Center in Tupelo partnered with NorthMississippi Hematology and Oncology Associates to benefit area cancerpatients. This arrangement will allow NMMC to restructure, expand andadd services to the state’s largest hematology and oncology program.
Shane Spees, North Mississippi Health Services president and chiefexecutive officer, said, “This exciting and innovative partnership willenable us to coordinate all of our cancer services to best meet ouroncology patients’ needs. This change will lead to an expansion of ouroncology services and enhancements that will provide patients withgreater convenience and easier access to treatment and support services.”
The hematology and oncology offices in Tupelo and Starkville are nowan outpatient department of NMMC. All oncology infusion services arenow provided at the NMMC Hematology and Oncology office onSouth Gloster in Tupelo.
“As a community of health care providers, we have looked for a way tobecome the primary referral center for cancer care in north Mississippi,”said Ronald Young, M.D., NMMC medical staff chairman. “We have agreat group of hematologists and oncologists and they have a greatfacility that is not being fully utilized. Our hope is that within a shortperiod of time NMMC will prove to be the center of excellence for cancer care in north Mississippi.”
NMMC is one of only two cancer treatment centers in north Mississippiaccredited by the Commission on Cancer of the American College ofSurgeons. “This partnership will enable NMMC to pursue additionalnationally recognized designations, research opportunities and academicaffiliations,” said Beth Bryant, NMMC cancer services administrator.
Cancer Patient NavigatorsIn 2014, NMMC added a cancer patient navigator program. ShelleyHamblin, RN, serves as the breast cancer patient navigator.
“Breast cancer patients now have someone who is there for themthroughout their care,” Bryant said. “This is someone who can answertheir questions and make sure their needs are met. Our plans includeadding navigators for other diagnoses soon.”
A cancer patient navigator acts as a patient advocate for newly diagnosedbreast cancer patients. The primary function of the navigator is to serveas a clinical liaison. She will assist the patient in accessing referrals andresources that meet her individual needs, and follow a patient througha continuum of care and treatment. She works with all members of thebreast cancer team – including radiology, surgery, medical oncology,radiation oncology and others – to help coordinate care.
ACR AccreditationNMMC has been awarded a three-year term of accreditation in radiation oncology as a result of a recent review by the AmericanCollege of Radiology (ACR).
Radiation oncology (radiation therapy) is the careful use of high-energy radiation to treat cancer. A radiation oncologist may use radiation to cure cancer or to relieve a cancer patient’s pain.
“At NMMC, quality care and patient safety are of utmost importance,”Bryant said. “The ACR accreditation survey verifies that the facility’spersonnel, equipment, patient care policies and quality control procedures adhere to national standards.”
Tumor ConferencesFighting cancer takes a team of health care providers – surgeons,pathologists, radiologists, medical and radiation oncologists, nurses,technicians and more. NMMC holds weekly breast cancer conferenceswhere each new breast cancer diagnosis is reviewed by a multi-disciplinary group of physicians and other health care professionals.
“Everyone comes to the table with their own perspective and ideas,and works together to make sure the patient is getting the best carepossible,” said Bryant. “The team communicates about every patientso that the treatment plan is individualized and takes into account allthe clinical viewpoints.”
Stereotactic Body Radiation Therapy (SBRT)Stereotactic Body Radiation Therapy (SBRT) is a radiation treatmenttechnique in which high dose radiation can be delivered to a precisetarget area in a few treatments, usually up to five.
The SBRT technique requires minimal motion to the target area andprecise radiation beam placement. This is accomplished through careful immobilization techniques, complex planning and a well-communicated team approach. The physician recommends this technique based on tumor size and location; and patient’s ability totolerate treatment.
At NMMC, a Varian Medical Systems Truebeam® linear accelerator isused to deliver SBRT. The Truebeam® allows for faster treatment timeswhile still providing the accuracy of image-guided radiotherapy.www.nmhs.net/cancer_services.php
Community ServiceNMMC staff is dedicated to helping patients battle cancer – and thatgoes beyond administering treatments and medications. The staff isactive in the Komen North Mississippi Race for the Cure and hostsfundraisers each year for the NMMC Cancer Patient Fund, whichassists qualified cancer patients with medications, transportation andother necessities while they are undergoing treatment.
Camp BluebirdA special camp for adults who have been diagnosed with cancer
Camp Bluebird is held each April and is moving in 2015 toFellowship Christian Retreat at Crow’s Neck in Tishomingo.
“Camp Bluebird, which is co-sponsored by North Mississippi MedicalCenter and the AT&T Pioneers, provides campers with a few days ofrest, recreation and the opportunity to share experiences,” said CampBluebird director Cheri Nipp, an NMMC occupational therapist.Campers are encouraged to participate in a variety of activities rangingfrom arts and crafts to educational programs.
Each camper in the medically supervised camp will be assigned acounselor, who is an NMMC staff member or AT&T Volunteer. Couns-elors complete a special training session prior to their participation.
CommunityReport
“Camp Bluebird has quite a loyal following. Many of our campers andcounselors come back year after year because the experience helpedthem at a time in their lives when they needed it, and they also enjoyspending time with the many special friends that they have made,”Nipp said.
The cost of the camp is $40 per person. Scholarships are available tothose who need financial assistance. All campers sleep on bunk bedsin dormitory facilities and bring their own toiletry items, linens, comfortable clothing and walking shoes. The registration fee includesmeals, a Camp Bluebird T-shirt and any materials needed for specialprograms or activities.
For more information, call (662) 377-4049 or visitwww.nmhs.net/camp_bluebird.php.
Midnite Pottery ButterfliesMidnite Pottery and NMMC have partnered to raise money for localcancer patients through the sale of a series of original butterfly art.The seventh in the series is currently on sale, and the eighth willdebut in January 2015.
Local artist Jennifer Hankins-Shelton created the pottery butterfly tobe sold exclusively by the NMMC Cancer Center. Each butterfly sellsfor $20 and benefits the NMMC Cancer Patient Fund, which isadministered by the Health Care Foundation of North Mississippi.
Hankins-Shelton has also created a large pottery platter featuring thebutterfly motif. The limited-edition platter sells for $35 and also benefits the NMMC Cancer Patient Fund.
“Each of us knows someone touched by cancer,” Hankins-Sheltonsaid. “This is a great project to help people in need. You never knowwhen that person could be you.”
The fund assists an average of 32 patients each month. Assistance provided to each patient ranges from $10-$2,000, depending on individual needs. Funds are raised through an annual fundraiser aswell as donations given by family members in memory or honor of acancer patient. NMMC employees also donate approximately $7,000each month through payroll deduction. Additional funds are receivedfrom grants through United Way and Project Hope.
For more information about the butterfly pottery pieces, call CindyEdwards, NMMC Cancer Center social worker, at (662) 377-4049.
Take a Swing at Cancer Benefit Golf TournamentEach year, The Health Care Foundation of North Mississippi sponsorsthe annual Take a Swing at Cancer Benefit Golf Tournament. The 19thannual tournament will be held Monday, May 18, 2015, at OldWaverly in West Point.
Proceeds benefit the NMMC Cancer Center Patient Assistance Fund,which provides about $90,000 annually for needy patients and theirfamilies who qualify for assistance.
The golf tournament is organized by community volunteers fromacross the region, as well as representatives from the Health CareFoundation and the NMMC Cancer Center.
The cost is $250 per player for the four-person scramble. There will betwo flights offered – one morning and one afternoon. Golfers who arecancer survivors will receive special recognition. More informationregarding registration and start time will be available closer to the date.
The entry fee will include 18 holes of golf, cart fee, lunch, registrationgift, door prize entry and the evening social. Prizes will be awardedfor first and second place finishers as well as for longest drive andclosest to the pin.
Sponsorship opportunities are available for companies interested inhelping this cause.
For more information on the Take a Swing at Cancer Benefit GolfTournament, call (662) 377-3613 or 1-800-THE DESK (1-800-843-3375), or log on to www.nmhs.net/hcf.php.
Cancer Support GroupsNMMC’s Cancer Center offers the following support groups for cancerpatients and their families. These groups allow cancer patients theopportunity to share common experiences, problems and solutions.They also provide an avenue for patients to talk confidentially withothers who are coping with and surviving cancer.www.nmhs.net/cancer_support_groups.php
NMMC Cancer Support Groups
I Can Cope, a group for those undergoing cancer treatment, meets atnoon on the second Friday of each month at NMMC HematologyOncology, 961 S. Gloster St., Tupelo. For more information, call (662)213-8478.
Man to Man is designed to help men diagnosed with prostate cancerand their families find answers to common questions and concerns.
Stepping Stones is a support group for cancer patients and theircaregivers. The group meets at 4 p.m. on the last Monday of eachmonth at NMMC Radiation Oncology, 990 S. Madison St., Tupelo.
For more information on support groups offered through NMMC, call1-800-THE DESK (1-800-843-3375).
Support Services and Community Outreach Programs
Barbershop Talk. A collaborative community program between NMMCand area barbers that targets the African-American male populationand provides educational information on early screenings for prostateand colon cancers. For more information, call (662) 377-4077.
Guided Imagery. A relaxation session that can help combat someside effects associated with a cancer diagnosis and treatment by focusing on healthful changes in the body and mind. For more information, call (662) 377-4049.
Home Health. NMMC Home Health offers patients a range of services, including skilled and specialty nursing and rehabilitation.Technology has developed to the point that almost any service available in the hospital can be delivered in the home setting withsome modification. For more information, call (662) 377-2499.

Cancer Has aColor
At NMMC, we know how difficult it is to hear a diagnosis of cancer, no matter what type. There’s a lot ofinformation out there, and we want to provide our patients with the best information available. Our “CancerHas a Color” page on our website provides links to find more information on many different types of cancer.The topics are organized by month and cancer ribbon for easy use. Visit www.nmhs.net/cancer_ribbons.phpfor more information.
CommunityReport
Hospice. Hospice care is a specialized program to help manage painand other symptoms associated with terminal illness. Chaplains, dietitians, social workers, nurses, therapists and volunteers are available to meet with patients and speak frankly about cancer andother life-limiting illness, share ideas and offer support. Services are available regardless of ability to pay. For more information, call 1-800-852-4910. www.nmhs.net/hospice.php
Lymphedema. A number of breast cancer patients suffer from painfulswelling in their arms, a condition called lymphedema. NMMC’sOutpatient Rehabilitation Center offers manual lymphatic treatment topeople with chronic lymphedema. Lymphedema is a chronic swellingthat can affect any part of the body. It is caused when the lymph nodesare unable to remove and process protein-rich fluids in the normalway. Breast cancer patients who have undergone a lumpectomy or amastectomy lose a number of their lymph nodes and are more proneto develop lymphedema in their arms. The manual lymphatic treat-ment combines light massage, sequential compression pumps andcompression bandaging to remove the fluid and help return the armto normal. For more information about lymphedema and manual lymphatic treatment, call 1-800-843-3375.www.nmhs.net/lymphedema_management_program.php
Mobile Mammography. The mobile mammography unit travels toarea communities and offers easy access to screening mammograms athospitals, physicians’ offices, businesses and industries throughoutnorth Mississippi and northwest Alabama. This special communityservice encourages preventive breast health and early detection ofbreast cancer. When breast cancer is caught early, survival rate increases to 90 percent. Call (662) 377-7984 or (662) 377-4910 foran appointment or more information.www.nmhs.net/mobile_mammo.php
Palliative Care Program. Palliative care uses an interdisciplinaryapproach to provide the comprehensive care and management of thephysical, psychological, emotional and spiritual needs of patients of all ages, and their families with chronic debilitating or life-limiting illnesses. For more information, call (662) 377-3810.
Pastoral Care. An NMMC Pastoral Care chaplain visits the CancerCenter to assist patients with spiritual needs. For more information,call (662) 377-3439.www.nmhs.net/pastoral_care.php
Resource Center. NMMC offers access to a cancer resource center,where patients and their family members can learn about cancer prevention, detection and treatment. The center houses a collection of information, including magazines, medical journals and referencebooks, self-help publications and periodicals on health and medicineas well as video and audio tapes. New information is added regularly.A computer and Internet access is available for patients and familymembers to do research on cancer, and the Cancer Center is a Wi-Fi hotspot.
Transportation Assistance. For those who qualify, transportation is available to help patients get to their treatments. For more information, call (662) 377-4077.
Social Services. An oncology certified social worker helps patients and families handle the changes associated with a cancerdiagnosis. Issues can include work-related stress, marriage and family disruptions, depression, anxiety, phobias, child and adolescent problems, well being and spiritual concerns. For more information, call (662) 377-4077.
Wellness Program. Available at NMMC Wellness Centers inBaldwyn, Iuka, Pontotoc, Tupelo and West Point, the Cancer Wellness Program is for people receiving treatment for all types and stages of cancer. The program combines specifically prescribedexercise with education and support to guide a person through recovery. For more information, call (662) 377-4141.www.nmhs.net/wellness_centers.php