Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012

of 12
Transcript of Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
1/12
REGULAR ARTICLE
Distal arthrogryposis: clinical and genetic findingsEva Kimber1,2, Homa Tajsharghi3, Anna-Karin Kroksmark2, Anders Oldfors3, Mr Tulinius ([email protected])2
1.Department of Womens and Childrens Health, Uppsala University Childrens Hospital, Uppsala, Sweden2.Department of Paediatrics, Institute of Clinical Sciences, University of Gothenburg, The Queen Silvia Childrens Hospital, Gothenburg, Sweden
3.Department of Pathology, Institute of Biomedicine, University of Gothenburg, Sahlgrenska University Hospital, Gothenburg, Sweden
Keywords
Arthrogryposis, Distal arthrogryposis 1 and 2,Multiple congenital contractures, Muscle weakness,Muscular disease
Correspondence
Mar Tulinius, Department of Paediatrics, Universityof Gothenburg, The Queen Silvia Childrens Hospital,SE-416 85 Gothenburg, Sweden.Tel: +46-31-3434780 |Fax: +46-31-843010 |Email: [email protected]
Received
13 March 2012; revised 5 April 2012;accepted 12 April 2012.
DOI:10.1111/j.1651-2227.2012.02708.x
ABSTRACT
Aim: Distal arthrogryposis is characterized by congenital contractures predominantlyin hands and feet. Mutations in sarcomeric protein genes are involved in several types of
distal arthrogryposis. Our aim is to describe clinical and molecular genetic findings in indi-
viduals with distal arthrogryposis and evaluate the genotype-phenotype correlation.Method: We investigated 39 patients from 21 families. Clinical history, includingneonatal findings, joint involvement and motor function, was documented. Clinical exami-
nation was performed including evaluation of muscle strength. Molecular genetic investiga-
tions were carried out in 19 index cases. Muscle biopsies from 17 patients were analysed.Results: A pathogenic mutation was found in six families with 19 affected family
members with autosomal dominant inheritance and in one child with sporadic occurrence.In three families and in one child with sporadic form, the identified mutation was de novo.
Muscle weakness was found in 17 patients. Ambulation was affected in four patients and
hand function in 28. Fourteen patients reported pain related to muscle and joint affection.Conclusion: The clinical findings were highly variable between families and alsowithin families. Mutations in the same gene were found in different syndromes suggesting
varying clinical penetrance and expression, and different gene mutations were found in the
same clinical syndrome demonstrating genetic heterogeneity.
INTRODUCTION
Distal arthrogryposis (DA) belongs to a group of syndromes
called arthrogryposis multiplex congenita (AMC), definedas congenital contractures in more than two joints and inmultiple body areas (1). There are more than 200 described
AMC syndromes. The incidence is between 14300 and
15100 (24). DA syndromes are characterized mainly by
distal congenital joint contractures, that is, of the hands andfeet. Twenty-one per cent of patients in a Swedish study of
AMC in children and adolescents were diagnosed with DA
syndromes, which indicates an incidence of about 120 000
(2). In 1982, DA syndromes were delineated as arthrogrypo-
sis with mainly congenital hand and foot involvement (5):
type I with only distal joint involvement and characteristichands at birth with flexed and overlapping fingers, and type
IIA-IIE with distal limb contractures and additional charac-teristic manifestations. A revised and extended classification
was made by Bamshad et al. (6). In this classification, DA isdefined as an inherited primary limb malformation disorder
characterized by congenital contractures of two or more dif-
ferent body areas and without primary neurological andor
muscle disease affecting limb function. Included disorders
are characterized by distal joint involvement, limited proxi-
mal joint involvement, autosomal dominant inheritance,reduced penetrance and variable expressivity. Nine different
clinical forms are originally described, with a 10th
syndrome defined in 2006 (68). The DA syndrome classifi-
cations are shown in Table 1.
The most commonly described forms of DA are DA1 andDA2B. DA1 is characterized by clenched fists at birth, ulnar
deviation, medially overlapping fingers and club feet or
other foot malpositions. The hips may be affected, calves
may be small and the opening of the mouth mildly limited
(9). DA2A, the FreemanSheldon syndrome, is character-ized by small mouth, facial contractures, scoliosis, mainly
distal joint contractures and short stature (10). DA2B, the
SheldonHall syndrome, is similar to DA2A but milder.
Typical findings in DA2B are vertical talus, ulnar deviation,
severe camptodactyly, triangularly shaped face, prominent
Key notes
We investigated 39 patients from 21 families with distalarthrogryposis.
Clinical findings were found to be highly variablebetween families and also within families.
Mutations in the same gene were found in differentsyndromes suggesting varying clinical penetrance andexpression, and different gene mutations were found inthe same clinical syndrome demonstrating genetic het-erogeneity.
Acta Pdiatrica ISSN 08035253
2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012101, pp. 877887 877
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
2/12
nasolabial folds, down-slanting palpebral fissures, smallmouth and prominent chin (11). Foot deformities may be
asymmetric (12).
Mutations in genes encoding sarcomeric muscle proteins
are found in several DA syndromes: Sung et al. (13,14)described mutations in beta-tropomyosin (TPM2) in DA1,
and mutations in fast troponin I (TNNI2) and fast troponinT (TNNT3) in DA2B. Toydemir et al. (15) described muta-
tions in embryonic myosin heavy chain 3 (MYH3) in DA2A,
the FreemanSheldon syndrome, and in DA2B, the Shel-
donHall syndrome. Further, a mutation in the foetal myo-sin heavy chain (MYH8) has been described in DA7, the
trismus-pseudocamptodactyly syndrome (16). Recently,DA1 has been associated with mutations in the slow-twitch
skeletal muscle myosin-binding protein C1 (MYBPC1) (17).Myopathic findings have previously been demonstrated in
DA12B with mutations in TNNI2 (18). Muscle weakness
has been demonstrated in patients with DA2B and muta-
tions in MYH3 and TPM2 (19). A defective function of
contractile muscle proteins during foetal life influencing
the mobility of the foetus seems to be the common causeof congenital joint contractures in these syndromes
(15,16,20).
The purpose of this study is to describe the clinical find-
ings in individuals with DA, to classify them into different
DA syndromes, to describe molecular genetic findings in theinvestigated individuals and to evaluate the genotype-phe-
notype correlation.
MATERIALS AND METHODS
SubjectsIn a national Swedish study of 131 children, adolescents
and young adults with AMC, 27 individuals with DA were
identified from 21 families. Including the affected parents
and extended family members, 39 individuals with familial
or sporadic DA were examined. The 27 patients were identi-fied via paediatric rehabilitation centres or, in a few cases,
via the orthopaedic surgeon or the Swedish AMC-associa-
tion. Affected relatives were contacted by the investigators
after an interview with and examination of the patients.From each of the 21 families, one patient was defined as the
index case (Tables 24).Written informed consent was obtained from adult par-
ticipating individuals and from the parents. The study was
approved by the Ethical Review Board at the Universities of
Gothenburg, Uppsala, Stockholm, Umea, Orebro, Malmo,Lund and Linkoping, and by the heads of the Paediatric
departments in the Swedish health-care regions.
Clinical investigationA detailed clinical examination was carried out of the origi-
nally identified 27 individuals, including physical examina-
tion by the same paediatric neurologist (EK) and
physiotherapist (A-KK). The physical examination included
a general examination, evaluation of facial involvement,
other associated signs and symptoms, and a neurologicalexamination.
Medical charts were studied, and results from previous
investigations, including orthopaedic procedures and mus-
cle biopsies, were recorded. A structured interview with the
27 patients was carried out and included their family his-tory, prenatal and perinatal history, neonatal findings,
developmental milestones, associated medical problems,
treatment and outcome.
Affected adult family members were examined by the
same physician and physiotherapist, and information ontheir family history was obtained through personal inter-
views. Family members who were found to be asymptomatic
carriers of the pathogenic gene mutation were seen and
interviewed personally to exclude the presence of previ-
ously undiagnosed distal joint involvement.
Table 1 Classification of distal arthrogryposis syndromes
Key distinguishing features
Classification
Bamshad Classification Hall Other name OMIM number
Overlapping fingers neonatally, ulnar deviation DA1 DA type I Digitotalar dysmorphism 108120
Facial contractures, small pursed mouth DA2A FreemanSheldon syndrome, FSS 193700
Intermediate DA12A DA2B SheldonHall syndrome 601680
Cleft palate, short stature DA3 DA type IIA Gordon syndrome 114300
Scoliosis DA4 DA type IID Arthrogryposis with severe scoliosis 609128Cleft lip DA type IIC
Ptosis, limited ocular mobility DA5 DA type IIB Arthrogryposis with oculomotor limitation
and electroretinal abnormalities
108145
Sensorineural hearing loss DA6 Arthrogryposis-like hand anomaly and
sensorineural hearing loss
108200
Trismus, facultative finger contractures DA7 Trismus-pseudocamptodactyly syndrome,
Hecht syndrome
158300
Multiple pterygium DA8 AD multiple pterygium syndrome 178110
Ear deformity, long fingers DA9 Beals syndrome, congenital contractural
arachnodactyly, CCA
121050
Plantar flexion contractures DA10 Short tendo calcaneus 187370
DA, Distal arthrogryposis.
DA: clinical and genetic findings Kimber et al.
878 2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012 101, pp. 877887
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
3/12
The diagnostic criteria used to distinguish the different
forms of DA are, according to Bamshad et al. from 1996 (6),
described in Table 1.Ambulation was classified according to Hoffer (21), using
the four categories of community ambulator, household
ambulator, nonfunctional ambulator and nonambulator
(22).Passive range of motion was measured with an ordinary
goniometer. Isometric muscle strength was measured with a
hand-held dynamometer using a method standardized by
Eek et al. (23), or, in children too young to participate in
this, by clinical evaluation. Motor function was assessed
according to Scott et al. (24), using a scale designed for chil-dren with muscle disease. In adults and in children younger
than one year, gross and fine motor function was evaluated
by inspection and interview.
Hand function was assessed by classification into one offour categories as follows:
1 Normal function
2 Able to perform all tasks completely but with compen-
satory strategies
3 Able to perform all tasks but incompletely and with
compensatory strategies
4 Able to perform tasks incompletely, very limited hand
function
The tasks evaluated in children included grasping a
paper, holding a pen and writingdrawing, assembling Legoand Duplo bricks, threading beads on a string and screwing
together a nut and bolt (22).
Hand function and gross motor function were videotaped
to facilitate evaluation and comparisons.
Short stature was defined as below 3 SD.
Muscle pathologyMuscle biopsy specimens were obtained from eleven indi-
viduals and analysed by the same pathologist (AO). Staining
techniques included haematoxylin-eosin, Gomori tri-
chrome, myofibrillar ATPase, oxidative enzymes (NADH-tetrazolium reductase, succinate dehydrogenase and cyto-
chrome oxidase), glycogen, lipids and major histocompati-
bility complex class 1 antigen. In another six patients,
results from previously performed muscle biopsies wererecorded from medical charts.
Table 2 Eight patients in three families with DA owing to mutations in embryonic myosin heavy chain,MYH3
Case
Familyindividual 1:1 1:2 (IC) 2:1 2:2 (IC) 2:3 2:4 3:1 3:2 (IC)
Age at investigation
(years)
49 21 41 10 10 8 7 4
Male(M)female(F) F F M F F M M M
Facial involvement + + + + ) ) ) )
Impairedmouth opening + + + + + + ) )
Joint involvement
Hands + + + + + + + +
Feet + + + + + + + +
Proximal joints + + + + + + + )
Asymmetric legsfeet + + ) ) + ) + (+)
Smooth palms ) ) + + + + ) )
Scoliosiskyphosis + + ) ) ) ) ) ))
Short stature + + ) ) ) ) ) )
Muscle weakness + + ) ) ) ) ) )
Level of ambulation* 2 2 1 1 1 1 1 1
Hand function** 3 2 2 2 1 2 1 2
No of orthopaedic
hand surgeries
220 30 00 00 20 20 00 00
Pain problems + + ) ) ) ) ) )
Additional signs
symptoms
Lip hem-angioma
hypertonia
Lip hemangioma Inguinal
hernia
keratoconus
Cleft palate Mental
retardation
ADHD
Cleft palate, CHD,
ADHD duodenal
atresia
Muscle pathology + + ) NA NA NA ) NA
DA classification DA2B DA2B DA2B DA2B DA1 DA1 DA1 DA1
Mutation found MYH3
D462G
MYH3
D462G
MYH3
A234T
MYH3
A234T
MYH3
A234T
MYH3
A234T
MYH3
A1752T
MYH3
A1752T
NA, not analyzedlacking information; ADHD, attention deficit hyperactivity disorder; CHD: congenital heart disease; IC, index case in the family; +: present; ): not
present; *1: community ambulator; 2: household ambulator; 3: nonfunctional ambulator; 4: nonambulatory; **1: able to perform tasks completely; 2: able to per-
form tasks completely but with compensatory strategies or aberrant function; 3: able to perform tasks incompletely; 4: not able to perform tasks.
Kimber et al. DA: clinical and genetic findings
2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012101, pp. 877887 879
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
4/12
Table
3
Twopatientsinone
fam
ilyw
ithDAow
ingtomutationsb-tropomyos
in,
TPM2an
dn
inepatientsintwo
fam
iliesw
ithDAduetomutations
intropon
in1
,TNNI2
Case
Fam
ilyindividua
l
4:1
4:2
(IC)
5:1
5:2
5:3
5:4
5:5
(IC)
5:6
6:1
6:2
(IC)
6:3
Ageatinvestigation
(years)
65
28
64
38
34
30
5
0,7
26
6
1
Male(M)female(F)
F
F
M
F
M
M
F
F
F
F
M
Facialinvolvement
+
+
)
+
)
)
)
)
+
+
+
Impairedmouth
opening
+
+
+
+
+
)
)
+
NA
+
)
Jointinvolvement
Hands
+
+
+
+
+
+
+
+
+
+
+
Feet
+
+
+
+
+
+
+
+
+
+
+
Proximaljoints
+
+
+
+
+
+
)
)
NA
+
+
Asymmetriclegsfeet
+
+
)
)
+
)
)
)
NA
)
)
Smoothpalms
+
+
+
+
+
)
)
+
NA
+
NA
Scoliosiskyphosis
+
+
)
+
)
)
)
)
NA
+
)
Shortstature
+
+
)
)
)
)
)
)
)
+
)
Muscleweakness
+
+
)
)
)
)
)
)
NA
+
NA
Levelofambulation*
1
1
1
1
1
1
1
)
1
1
1
Handfunction**
2
2
2
2
2
1
1
2
3
2
NA
Nooforthopaedic
handsurgeries
00
30
60
60
60
00
30
10
>20
12
10
Painproblems
+
)
+
)
)
+
)
)
NA
)
)
Additionalsigns
symptoms
Reduced
hearing
Reduced
hearing
Neckpterygium
)
)
)
Reduced
hearing,
inguinal
hernia
Inguinal
hernia
Neck
pterygium
NA
Cranio-stenosis
Pelvo-uretheral
stenos
is
Inguinalhernia,
retentiotestis
Musclepathology
+
+
+
+
+
+
NA
NA
NA
NA
NA
DAclassification
DA2B
DA2B
DA1
DA2B
DA1
DA2B
DA1
DA2B
DA2B
DA2B
DA2B
Mutationfound
TPM2
R133W
TPM2
R133W
TNNI2
K176del
TNNI2
K176
del
TNNI2
K176del
TNNI2
K176del
TNNI2
K176del
TNNI2
K176del
TNNI2
R174Q
TNNI2
R174Q
TNNI2
R174Q
NA,notanalyzedlackinginformation;IC,
indexcaseinthefamily;+:present;:notp
resent;*1:communityambulator;2:household
ambulator;3:nonfunctionalambulator;4:nonambulatory;**1:abletoper-
form
taskscompletely;2:abletoperfor
m
taskscompletelybutwithcompensatorystrate
giesoraberrantfunction;3:abletoperform
task
sincompletely;4:notabletoperform
tasks.
DA: clinical and genetic findings Kimber et al.
880 2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012 101, pp. 877887
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
5/12
Molecular genetic investigationBlood samples for genetic analysis were obtained from 19 of
the 21 index patients and from their relevant family mem-bers. In two index patients, no blood sample was obtained
(12:1 and 21:1).
Extraction of DNA, polymerase chain reaction (PCR)
and sequence analysis were performed as previouslydescribed (17,19,20). The entire coding region of MYH3,
TPM2and TNNI2was sequenced in 15 index patients using
the previously described primers (15,16,20). The presence
of each mutation was confirmed in each affected individual
by restriction fragment length polymorphism (RFLP) analy-
sis. RFLP analysis was also used to screen for the presenceof each mutation in 200 control chromosomes. In addition,
in five of the 15 index patients in whom mutations in
MYH3,TPM2and TNNI2were excluded, the entire coding
region of other sarcomeric thin filament componentsincluding TNNI1, TNNT3, TNNC1, TNNC2 and TNNT1was also analysed. Furthermore, additional sarcomeric
genes were considered as the plausible cause of the disease
based on similarities in the clinical features with previously
reported cases. This included one patient with multiple
pterygium syndrome where the acetylcholine receptor gene
gamma and the entire coding region ofGHRNGwere anal-
ysed in addition to TPM2. The entire coding region of the
slow-twitch skeletal muscle myosin-binding protein C (MY-BPC1) was also analysed in two index patients, and the
entire coding region of both MYH8 and MYH3was analy-
sed in one index patient.
RESULTS
SubjectsWe identified 27 patients, children and young adults, and
twelve affected relatives. Of the 39 affected individuals, 22
were male and 17 were female. The age span was from ninemonths to 65 years at the time of investigation. There were
ten families with a total of 28 affected individuals: in one
family three generations were affected, in eight families two
generations and in one family one generation. In four fami-lies there were two affected siblings, and in one family three
affected siblings. Eleven cases were sporadic.
Perinatal dataPerinatal data were available for 26 of the 27 patients. Data
were missing for one child who was adopted at three years
Table 4 Nine patients in four families with familial DA with no identified mutations
Case Familyindividual 7:1 7:2 (IC) 8:1 8:2 (IC) 8:3 9:1 9:2 (IC) 10:1 10:2 (IC)
Age at investigation
(years)
50 18 34 7 3 36 1 38 4
Male(M)female(F) F M M M M M M F M
Facial involvement + + + + + ) ) ) +
Impaired mouth
opening
+ + NA + + ) ) ) )
Joint involvement
Hands + + + + + + + + +
Feet + + + + + + + + +
Proximal joints + + NA + + + + + +
Asymmetric legsfeet + ) + + + ) + ) )
Smooth palms + + + + + + + ) )
Scoliosiskyphosis ) ) + + ) ) ) ) +
Short stature ) ) NA ) ) ) ) ) )
Muscle weakness NA + NA + + ) ) ) )
Level of ambulation* 1 1 1 1 1 1 NA 1 1
Hand function** 2 2 2 2 2 2 2 1 1
No of orthopaedic
hand surgeries
411 55 10 01 20 120 10 10 00
Pain problems + + + + ) + ) ) )
Additional signs
symptoms
High blood
pressure
Reduced hearing
Urether stenosis,
Urolithiasis Ing.
hernia
Ing. hernia Ing. hernia
Retentio
testis
Ing. hernia
Retentio
testis
Myopia Bowed
lower leg
Crumpled
ears
Crumpled
ears
Muscle pathology + NA NA + NA NA NA NA NA
DA classification DA2B DA2B DA2B DA2B DA2B DA1 DA1 DA9 DA9
Mutation found None found None found None
found
None
found
None
found
None
found
None
found
None
found
None
found
NA, not analyzed lacking information; IC, index case in the family; +: present; : not present; *1: community ambulator; 2: household ambulator; 3: nonfunc-
tional ambulator; 4: nonambulatory; * *1: able to perform tasks completely; 2: able to perform tasks completely but with compensatory strategies or aberrant func-
tion; 3: able to perform tasks incompletely; 4: not able to perform tasks.
Kimber et al. DA: clinical and genetic findings
2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012101, pp. 877887 881
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
6/12
of age. Birth was by Caesarean section in 14 patients, eight
of whom were in breech position. One child had intrauter-ine growth retardation, and two were born prematurely 32
gestational weeks. Feeding problems during the neonatal
period were reported for 15 patients.
Joint involvement at birthInformation regarding joint position at birth was available
for 33 of the 39 individuals. In the remaining six individuals,congenital, mainly distal, joint contractures were described,
but no detailed information was available. Hand involve-
ment included ulnar deviation (n = 16), adducted thumbs(n = 15), clenched fists (n = 13), contractures of the fingers
(n = 12), contractures of the wrists (n = 10) and overlap-
ping fingers (n = 6). Foot involvement included pes equi-
novarus (n = 18), pes calcaneovalgus (n = 11) and otherfoot malpositions (n = 8). Involvement of proximal joints
included contractures of the hips (n = 12), knees (n = 10),shoulders (n = 7) and elbows (n = 6), dislocation of the
hips (n = 5), scoliosiskyphosis (n = 3) and torticollis
(n = 3).
Other neonatal findingsReported neonatal findings included facial haemangioma
(n = 4), epicanthic folds (n = 4), asymmetric face (n = 3),
microphthalmia (n = 3), low-set ears (n = 3), hypertelo-rism (n = 2), micrognathia (n = 1) and small mouth
(n = 1). Cleft palate was described in two patients, one of
whom also had multiple malformations including duodenal
atresia and congenital heart vitium with ventricular septum
defect and anomalous outlet of the pulmonary veins. One
patient with DA2A, the FreemanSheldon syndrome, had
severe facial contractures with blepharophimosis and anextremely small and puckered mouth. Inguinal hernia was
present in four patients, and diaphragmatic hernia in onechild who was later identified as having a multiple ptery-
gium syndrome. Congenital pterygias were described intwo patients.
Clinical findings at follow-upThe clinical findings are described in Tables 25 and illus-
trated in Figure 1. The number of patients with facial
involvement and joint involvement of the hands, feet andproximal joints is shown in Table 6.
Facial involvement was found more frequently in familial
than in sporadic cases. The most frequent findings, in
decreasing order, were impaired mouth opening (mild con-
tractures of the temporomandibular joints), low-set ears,high arched palate, micrognathia, high nose bridge, down-
slanting andor narrow palpebral fissures, facial asymmetry,
small mouth and epicanthic folds.
Flexion or, more rarely, extension contractures of the
wrists were the most frequent findings in the hands, fol-lowed by ulnar deviation of the wristsfingers. Smooth
palms with absent flexion creases and contractures in meta-
carpophalangeal (MCP) and finger joints resulting in cam-
ptodactyly were also seen frequently. Adducted thumbs andother thumb malpositions were also found.
The most common types of foot involvement, in order offrequency, were ankle contractures, adductionmetatarsus
varus, prominent heel pads, overlapping toes, short Achilles
tendons, pes planovalgus and equinus feet. Asymmetric
involvement of the feet was a common finding, while asym-
metric foot size was found in only a few patients.
The proximal joints were more often affected in the upperlimbs than in the lower limbs, with elbow and shoulder con-
tractures being the most common finding. Prominent radialheads were found in combination with impaired prona-
tionsupination, while impaired flexionextension of the
elbows was less commonly found. Contractures of the kneeswere less frequently seen than contractures of the hips.
Asymmetric leg length andor muscle bulk especially of the
calves was also seen.
Additional signs and symptoms
Inguinal hernia occurred in seven familial cases and onesporadic case, and cryptorchism in three familial and three
sporadic cases. Ureteric stenosis was found in two familial
cases. Attention deficit hyperactivity disorder (ADHD) was
present in two brothers one of whom also had mental retar-dation, while the other brother had multiple malformations
(palate, heart, duodenum). Reduced hearing, unilat-
eralbilateral, was present in four familial cases. Multiple
pterygias were present in the two patients with DA8, andmild neck pterygium was found in a further three familial
cases. Malformation of the outer ear (crumpled ear) was
present in the two familial cases with DA9. Dimples over
affected joints were present in 11 familial and in six spo-
radic cases.
Orthopaedic surgeryThe number of orthopaedic surgical interventions varied
between one and 22 in 31 patients, 21 familial cases and tensporadic cases. When malpositioning of the feet had beenpresent at birth, orthopaedic surgery had generally been
performed during the first year of life.
PainPain, either generalized muscle pain or localized pain, was
present in 14 patients: ten familial and four sporadic cases.Pain was more frequent in the patients with more severe
joint contractures, and in the patients who had undergone
multiple orthopaedic surgeries. Muscle fatigue and pain on
exertion were described in several of the adult patients.
Gross motor function and hand functionAmbulation was affected in four patients: a mother and
daughter with DA2B, one sporadic case with DA2B and
one sporadic case of DA8. Ambulation could not be evalu-
ated in two children less than one year of age.
Hand function was mildly affected (able to perform thetasks completely but with compensatory strategies) in 23
patients, 19 familial and four sporadic cases and severely
affected (able to perform the tasks incompletely and with
compensatory strategies) in five patients, two familial andthree sporadic cases.
DA: clinical and genetic findings Kimber et al.
882 2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012 101, pp. 877887
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
7/12
Table
5
Patientsw
ithspora
dica
llyoccurring
DA
,onew
ithmutation
inem
bryon
icmyos
inheavy
cha
in,
MYH3an
dtenpatientsw
ithno
identifie
dmutations
Case
Fam
ilyindividua
l
11:1
12:1
13:1
14:1
15:1
16:1
17:1
18:1
19:1
20
:1
21:1
Ageatinvestigation
(years)
4
16
17
13
10
5
3
18
11
4
10
Male(m)female(f)
M
M
F
F
F
M
M
M
M
F
M
Facialinvolvement
+
+
)
)
)
+
)
+
+
+
+
Impairedmouth
opening
++
+
)
)
)
+
)
+
+
)
+
Jointinvolvement
Hands
+
+
+
+
+
+
+
+
+
+
+
Feet
+
+
+
+
+
+
+
+
+
+
+
Proximaljoints
+
+
+
+
)
+
+
+
+
+
+
Asymmetriclegsfeet
)
+
+
)
)
)
)
)
)
+
+
Smoothpalms
)
+
+
+
+
+
)
)
+
)
)
Scoliosiskyphosis
+
+
)
)
)
)
)
+
+
)
+
Shortstature
+
+
)
)
)
)
)
)
+
)
+
Muscleweakness
+
+
+
+
+
)
+
+
+
)
+
Levelofambulation*
1
2
1
1
1
1
1
1
1
2
1
Handfunction**
2
3
2
2
2
1
1
3
3
1
1
Nooforthopaedic
handsurgeries
31
14
05
122
06
00
01
52
03
20
01
Painproblems
)
)
+
+
)
)
)
+
+
)
)
Additionalsigns
symptoms
CHDPtosis
Ptosis,pubertas
praecox,
retentiotestis
)
)
)
Facial
hemangioma
)
Inguinal
herniaMild
neckpterygium
Ptosis,
retentiotestis
Multiple
pterygium
Multiple
pterygium
retentiotestis
Musclepathology
+
+
NA
)
NA
NA
)
)
NA
NA
NA
DAclassification
DA2A
DA2B
DA1
DA1
DA1
DA2B
DA1
DA7
DA3
DA
8
DA8
Mutationfound
MYH3T178M
NA
Nonefound
Nonefoun
d
Nonefound
Nonefound
Nonefou
nd
Nonefound
Nonefound
NA
NA
NA,notanalyzedlackinginformation;CHD,congenitalheartdisease;+:present;):n
otpresent;*1:communityambulator;2:house
holdambulator;3:nonfunctionalambulator;4:
nonambulatory;**1:ableto
perform
taskscompletely;2:abletope
rform
taskscompletelybutwithcompensatorystrategiesoraberrantfunction;3:abletoperform
tasksincompletely;4:notabletoperform
tasks.
Kimber et al. DA: clinical and genetic findings
2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012101, pp. 877887 883
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
8/12
Muscle involvementMuscle weakness was found in 17 individuals, eight familial
and nine sporadic cases.
Muscle morphologyMorphological findings in skeletal muscle are illustrated in
Figure 2. Muscle pathology was demonstrated in twelve of17 patients. In two patients with DA2B and TPM2 muta-
tion, there was minor type-1 fibre predominance. In the
patient with DA2A and MYH3 mutation, marked type-1
fibre predominance and scattered small type-1 fibres were
found. In two patients with DA2B and MYH3 mutation,
increased variability in fibre size owing to the presence offrequent small type-1 fibres was found. In four familial cases
with DA1 or DA2B and TNNI2 mutation, muscle biopsy
specimens showed findings of myopathy with changes
mainly restricted to type-2 fibres. In one patient with DA2B
with no known mutation, a previously performed musclebiopsy showed type-1 fibre predominance.
Molecular geneticsMolecular genetic investigations revealed pathogenic muta-tions in one sporadic and 19 familial cases. Three de novomutations were identified, including a D462G mutation in
MYH3in family 1, a R133W mutation in TPM2in family 4
and a K176del mutation in TNNI2in family 5. In addition,
A234T and A1752T mutations in MYH3 were identified in
family 2 and 3, respectively. Two asymptomatic carrierswere identified in these families, the paternal grandfather in
family 2 with A234T mutation in MYH3 and the father in
Figure 1 Clinical features in patients with Distal arthrogryposis2B (SheldonHall syndrome) with mutations of different sarcomeric protein genes: from right to left
patient with mutation of fast troponin I (TNNI2), embryonic myosin heavy chain (MYH3),b-tropomyosin (TPM2) and a patient with no identified mutation. Note asym-
metric lower legs and feet.
Table 6 Facial involvement, involvement of hands, feet and proximal joints according to inheritance in 28 familial and 11 sporadic patients with distal arthrogryposis syndromes
Facial involvement F S Hand involvement F S Foot involvement F S Involvement of proximal joints F S
Impaired mouth opening 14 5 Ulnar deviation 15 5 Metatarsus varus 13 11 Shoulder contractures 14 7
Low-set ears 12 4 Wrist contractures 16 4 Ankle contractures 13 8 Elbows impaired prosup 15 6
High arched palate 14 0 Smooth palms 13 1 Prominent heel pads 7 1 Elbow flexext
contractures
7 3
Micrognathia 8 3 Contractures in MCP joints 12 2 Overlapping toes 6 1 Elbow hyperextension 2 2
High nasal bridge 7 2 Contractures in finger joints 9 4 Short Achilles tendons 2 3 Prominent radial heads 5 0
Down-slanting eyes 6 1 Thumbs in hands 7 2 Curlyadducted toes 3 2 Contractures in hips 7 4
Narrow palpebral fissures 6 1 Proximal syndactyly 3 0 Pes planovalgus 3 1 Hip dislocation 1 0
Asymmetric facejaw 5 1 Hyperextended PIP-joints 2 1 Equinus feet 1 3 Hip hypermobility 0 1
Small mouth 5 1 Laterallow-set thumbs 3 1 Proximal syndactyly 1 0 Contractures in
knee joints
7 4
Epicanthal folds 4 0 Short dorsal extensor
tendons
1 1 Cavus feet 0 1 Patellar luxation 2 0
Lip hemangioma 3 0 Sublux thumbs 1 0Down-pressed tip of nose 2 0
Ptosis 0 2
Cleft palate 2 0
Hypertelorism 2 0
Prominent chin 1 0
F, familial; S, sporadic; MCP, metacarpophalangeal; PIP, proximal interphalangeal; pro, pronation; sup, supination.
DA: clinical and genetic findings Kimber et al.
884 2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012 101, pp. 877887
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
9/12
family 3 with A1752T mutation inMYH3. The latter patient
had a history of contractures of the feet as a child, but was
asymptomatic at the time of investigation. Notably, two
nonsynonymous single-nucleotide polymorphisms at posi-
tion 1752 (A1752S and A1752T) have been identified(rs34393601). No mutations were found in TNNC1,
TNNC2,TNNT1,GHRNG, MYBPC1andMYH8.
Distal arthrogryposis classificationThirteen patients, nine familial and four sporadic cases,
were classified as having DA1. Seventeen patients, 15 famil-
ial and two sporadic cases, were classified as having DA2B.
In two familial patients, the clinical findings were interme-
diate between DA1 and DA2B. Clinically, the dividing line
between these two syndromes was not clear-cut.One child was classified as having DA2A, FreemanShel-
don syndrome, one child as DA3, Gordon syndrome, and
one young man as DA7, trismus-pseudocamptodactyly syn-drome. All three were sporadic cases. DA8, multiple ptery-gium syndrome, was found in two sporadic cases, and DA9,
Beal syndrome, in one family with an affected mother and
son.
In seven patients with DA2B, five familial cases from two
families and two sporadic cases, and in six patients with
DA1, two familial and four sporadic cases, no mutation wasidentified. The clinical findings in these cases did not differ
from the findings in patients with DA1 or DA2B in whom
pathogenic mutations were identified.
DISCUSSION
Distal arthrogryposis syndromes, at least DA1, DA2A and
DA2B, may be regarded as diseases caused by sarcomeric
protein dysfunction causing foetal myopathy and secondary
congenital joint contractures. The involvement is predomi-nantly distal in milder cases, but with more severe affection
all joints are involved, proximal and distal, and facial devel-
opment is also affected. Our findings indicate that familialcases are often more severe.
The phenotypic variability was found to be wide, varying
from unaffected carriers to severely affected individuals.
The correlation between genotype and phenotype was low.
Facial involvement and involvement of proximal joints were
seen as expressions of increasing severity rather than of clin-ically separate syndromes. DA1 and DA2B appear as differ-
ent clinical expressions of the same genetic mutation in two
of our investigated families: family 2 with mutation in
MYH3and family 5 with mutation in TNNI2.In this study, there was not a strict genotype-phenotype
correlation. Dysfunction of several different sarcomeric pro-
teins during foetal life results in similar clinical features, and
the presence of so far nonidentified gene mutations can
cause the same clinical symptoms as the mutations identi-
fied inMYH3,TPM2andTNNI2.
The likelihood of identifying a genetic cause of DA wasfound to be far greater in familial than in sporadic cases. A
pathogenic mutation causing sarcomeric protein dysfunc-
tion was found in 19 familial cases but only in one sporadic
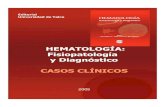
Figure 2 Muscle pathology in three patients with Distal arthrogryposis2B (SheldonHall syndrome) owing to mutations in different sarcomeric protein genes: In the
biopsy specimen from the patient with fast troponin I (TNNI2) mutation, there are myopathic changes affecting mainly type 2 fibres and minor increase in interstitial con-
nective tissue. In the biopsy specimen from the patient with embryonic myosin heavy chain (MYH3) mutation, there is variability in fibre size with many small type 1
fibres. In the biopsy specimen from the patient with -tropomyosin (TPM2)mutation, there is type 1 fibre predominance as the only pathologic change.
Kimber et al. DA: clinical and genetic findings
2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012101, pp. 877887 885
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
10/12
case. The only sporadic case of DA with an identified patho-
genic mutation in our study was a child with DA2A, theFreemanSheldon syndrome. However, in three families
with familial DA ade novomutation could be demonstrated
in the oldest affected individual, which indicates that patho-
genic sarcomeric gene mutations may also be present in
other sporadic cases. One of the de novo mutations was in
MYH3 (family 1), one was in TPM2 (family 4) and one in
TNNI2(family 5).Asymptomatic carriers were found in two extended fami-
lies, demonstrating varying penetrance. In family 2, the
unaffected paternal grandfather carried the same mutationin MYH3 as his affected son and three affected grandchil-
dren. In family 3, also with a mutation in MYH3, the father
was an asymptomatic carrier with the same mutation as that
found in the two affected children. The father had a historyof contractures of his feet as a child.
Muscle involvement in childhood and in adult life wasvariable, with muscle weakness present in some families but
not in others. In some instances, the muscle weakness
affected only the hands and feet, and in others all the mea-
sured muscle groups. Muscle weakness was found in bothfamilial and sporadic DA. Interviews did not indicate any
clear progression of muscle weakness over time, but
affected adults described increasing muscle fatigue with age.
Generalized muscle pain was more common in older thanin young individuals. Where pain was reported in children,
it seemed, in most of the cases, to be a consequence of
repeated surgical interventions, especially in the feet. Pain
of the hands was rarely reported.
Limitations to daily life seemed to be correlated mainly to
pain and muscle fatigue, but in some cases also to quitesevere limitations of joint mobility. Joint contractures of the
hands were sometimes a problem in daily life. Finger con-
tractures were more easily compensated for by using thehands in a different manner one man was a skilled manual
worker in spite of quite severe finger contractures whileimpaired function of the thumbs, especially thumb-finger
opposition, was more difficult to compensate for. Difficulty
of pronation and supination was also found to cause practi-
cal problems in daily life, such as difficulty of receiving small
objects (for example loose change) in the palm of the hand,
and difficulty of pushing or applying pressure using thepalms of the hands. Feet malpositions were more often trea-
ted surgically, as plantigrade position of the feet is necessary
for ambulation.
We found pathological changes in muscle biopsy speci-
mens from patients with DA2A and DA2B. Whether thesefindings are specific for the respective gene mutations is not
known, and requires further muscle morphologic studies in
DA patients.
Several of the DA syndromes, DA1, DA2A, DA2B and
DA7, have recently been shown to be caused by sarcomericprotein dysfunction (1316,1820). DA3, DA4, DA6 and
DA10 also include clinical findings that can be present in
DA syndromes where the cause is known to be sarcomeric
protein dysfunction. Mitochondrial dysfunction has beenfound in DA5 with ophthalmoplegia and retinal
pigmentation (5,25). Pulmonary disease has also beendescribed in this syndrome (26,27). Autosomal dominant
multiple pterygium syndrome is classified as DA8 (6). In
multiple pterygium syndrome, the Escobar syndrome, muta-
tions of embryonic acetylcholine receptor genes (28,29) or
absence ofb-tropomyosin (30) are described. Overlapping
clinical findings have been described in DA8 and DA2B(31). In DA9 (contractural arachnodactyly, Beal syndrome),
a pathogenic mutation of a fibrillin gene, FBN2, has beendescribed (32), indicating collagen dysfunction.
In conclusion, we suggest that DA syndromes be defined
according to the pathogenic background, that is, sarcomericprotein dysfunction, connective tissue dysfunction or other
pathology. DA1, DA2B and DA2A may be regarded as a
continuum of increasingly severe forms of myopathy,
caused by foetal sarcomeric protein dysfunction. Moleculargenetic and muscle morphological investigations, in addi-
tion to careful clinical evaluation, including evaluation ofmuscle strength and joint involvement, are of importance in
patients with DA syndromes, to further define and under-
stand these disorders.
References
1. Hall JG. Arthrogryposis multiplex congenita: etiology, genetics,classification, diagnostic approach and general aspects.J Pedi-atr Ortop B1997; 6: 15966.
2. Darin N, Kimber E, Kroksmark AK, Tulinius M. Multiple con-genital contractures: birth prevalence, etiology, and outcome.JPediatr2002; 140: 617.
3. Pakkasjarvi N, Ritvanen A, Herva R, Peltonen L, Kestila M,Ignatius J. Lethal congenital contracture syndrome (LCCS) andother lethal arthrogryposes in Finland an epidemiologicalstudy.Am J Med Genet2006; 140A: 18349.
4. Lowry BR, Sibbald B, Bedard T, Hall JG. Prevalence of multiple
congenital contractures including arthrogryposis multiplex con-genital in Alberta, Canada, and a strategy for classification andcoding.Birth Defects Res A Clin Mol Teratol 2010; 88: 105761.
5. Hall JG, Reed SD, Greene G. The distal arthrogryposes: delin-eation of new entitiesreview and nosologic discussion.Am JMed Genet1982; 11: 185239.
6. Bamshad M, Jorde LB, Carey JC. A revised and extended classi-fication of the distal arthrogryposes.Am J Med Genet1996; 65:27781.
7. Bamshad M, Bohnsack JF, Jorde LB, Carey JC. Distal arthrogry-posis type 1: clinical analysis of a large kindred.Am J MedGenet1996; 65: 2825.
8. Stevenson DA, Swoboda KJ, Sanders RK, Bamshad M. A newdistal arthrogryposis syndrome characterized by plantar flexion
contractures.Am J Med Genet A 2006; 140: 2797801.9. Beals RK. The distal arthrogryposes: a new classification ofperipheral contractures.Clin Orthop Relat Res2005; 435: 20310.
10. Stevenson DA, Carey JC, Palumbos J, Rutherford A, Dol-court J, Bamshad MJ. Clinical characteristics and natural his-tory of Freeman-Sheldon syndrome. Pediatrics 2006; 117:75462.
11. Toydemir RM, Bamshad MJ. Sheldon-Hall syndrome.OrphanetJ Rare Dis2009; 4: 11.
12. Krakowiak PA, Bohnsack JF, Carey JC, Bamshad M. Clinicalanalysis of a variant of Freeman-Sheldon syndrome (DA2B).Am J Med Genet1998; 76: 938.
DA: clinical and genetic findings Kimber et al.
886 2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012 101, pp. 877887
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
11/12
13. Sung SS, Brassington AM, Grannatt K, Rutherford A, WhitbyFG, Krakowiak PA, et al. Mutations in genes encoding fast-twitch contractile proteins cause distal arthrogryposis syn-dromes.Am J Hum Genet2003; 72: 68190.
14. Sung SS, Brassington AM, Krakowiak PA, Carey JC, Jorde LB,Bamshad M. Mutations in TNNT3 cause multiple congenitalcontractures: a second locus for distal arthrogryposis type 2B.Am J Hum Genet2003; 73: 2124.
15. Toydemir RM, Rutherford A, Whitby FG, Jorde LB, Carey JC,
Bamshad MJ. Mutations in embryonic myosin heavy chain(MYH3) cause Freeman-Sheldon syndrome and Sheldon-Hallsyndrome. Nat Genet2006; 38: 5615.
16. Toydemir RM, Chen H, Proud VK, Martin R, van Bokhoven H,Hamel BC, et al. Trismus-pseudocamptodactyly syndrome iscaused by recurrent mutation of MYH8.Am J Med Genet A2006; 140: 238793.
17. Gurnett CA, Desruisseau DM, McCall K, Choi R, Meyer ZI,Talerico M, et al. Myosin binding protein C1: a novel gene forautosomal dominant distal arthrogryposis type 1.Hum MolGenet2010; 19: 116573.
18. Kimber E, Tajsharghi H, Kroksmark AK, Oldfors A, Tulinius M.A mutation in the fast skeletal muscle troponin I gene causesmyopathy and distal arthrogryposis.Neurology2006; 67: 597601.
19. Tajsharghi H, Kimber E, Holmgren D, Tulinius M, OldforsA. Distal arthrogryposis and muscle weakness associatedwith a beta-tropomyosin mutation. Neurology 2007; 68: 7725.
20. Tajsharghi H, Kimber E, Kroksmark AK, Jerre R, Tulinius M,Oldfors A. Embryonic myosin heavy-chain mutations cause dis-tal arthrogryposis and developmental myosin myopathy thatpersists postnatally.Arch Neurol2008; 65: 108390.
21. Hoffer MM, Swank S, Eastman F, Clark D, Teitge R. Ambula-tion in severe arthrogryposis.J Pediatr Orthop1983; 3: 2936.
22. Kroksmark AK, Kimber E, Jerre R, Beckung E, Tulinius M.Muscle involvement and motor function in amyoplasia.Am JMed Genet A2006; 140: 175767.
23. Eek MN, Kroksmark AK, Beckung E. Isometric muscle torquein children 5 to 15 years of age: normative data. Arch Phys MedRehabil2006; 87: 10919.
24. Scott OM, Hyde SA, Goddard C, Dubowitz V. Quantitation ofmuscle function in children: a prospective study in Duchennemuscular dystrophy.Muscle Nerve1982; 5: 291301.
25. Schrander-Stumpel CT, Howeler CJ, Reekers AD, De SmetNM, Hall JG, Fryns JP. Arthrogryposis, ophthalmoplegia, andretinopathy: confirmation of a new type of arthrogryposis.J
Med Genet1993; 30: 7880.26. Beals RK, Weleber RG. Distal arthrogryposis 5: a dominant
syndrome of peripheral contractures and ophthalmoplegia.AmJ Med Genet A2004; 131: 6770.
27. Williams MS, Elliott CG, Bamshad MJ. Pulmonary disease is acomponent of distal arthrogryposis type 5.Am J Med Genet A2007; 143: 7526.
28. Michalk A, Stricker S, Becker J, Rupps R, Pantzar T, Miertus J,et al. Acetylcholine receptor pathway mutations explain vari-ous fetal akinesia deformation sequence disorders.Am J HumGenet2008; 82: 46476.
29. Vogt J, Harrison BJ, Spearman H, Cossins J, Vermeer S, tenCate LN, et al. Mutation analysis of CHRNA1, CHRNB1,CHRND, and RAPSN genes in multiple pterygium syn-dromefetal akinesia patients.Am J Hum Genet2008; 82: 222
7.30. Monnier N, Lunardi J, Marty I, Mezin P, Labarre-Vila A, Diete-
rich K, et al. Absence of beta-tropomyosin is a new cause ofEscobar syndrome associated with nemaline myopathy.Neu-romuscul Disord2009; 19: 11823.
31. Rajab A, Hoffmann K, Ganesh A, Sethu AU, Mundlos S. Esco-bar variant with pursed mouth, creased tongue, ophthalmologicfeatures, and scoliosis in 6 children from Oman.Am J MedGenet A2005; 134: 1517.
32. Gupta PA, Putnam EA, Carmical SG, Kaitila I, Steinmann B,Child A, et al. Ten novel FBN2 mutations in congenital con-tractural arachnodactyly: delineation of the molecular patho-genesis and clinical phenotype.Hum Mutat2002; 19: 3948.
Kimber et al. DA: clinical and genetic findings
2012 The Author(s)/Acta Pdiatrica 2012 Foundation Acta Pdiatrica 2012101, pp. 877887 887
-
7/21/2019 Artrogriposis Distal Descubrimientos Clinicos y Geneticos 2012
12/12
Copyright of Acta Paediatrica is the property of Wiley-Blackwell and its content may not be copied or emailed
to multiple sites or posted to a listserv without the copyright holder's express written permission. However,
users may print, download, or email articles for individual use.