Application of Artificial Neural Network (ANN) to Predict Soil

Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1389
Artificial Neural Networks (ANN)in the Assessment of Respiratory
Mechanics
BY
GAETANO PERCHIAZZI
ACTA UNIVERSITATIS UPSALIENSISUPPSALA 2004


Dedication
The personal story of a researcher probably is less important than his achievements. However, research is seldom the simple sum of ideas, techni-cal means and economical resources. May be there is something else worth to be told, that for shyness we tend to hide. I will use a few square centime-ters of paper to remember how I arrived to at Uppsala.
In the place where I was born and in the years during which I went to school, studying was not for everybody. Soon you understood to belong to a differ-ent category of people, the ones that had to wrestle for earning the possibility of staying there. On your shoulder you felt the burden of those who left, strangled by a difficult life. And you had to keep on going, on a path that nobody of your friends and relatives scoured before you.
Alone and deep in thought I measure with slow and lingering steps the deserted fields, ready to flee if my eyes discern a human footprint in the sand.I
My loneliness was warmed by the words of the masters, depicting the joy of knowledge and the desire of a mad flight beyond the pillars of Hercules.
Consider ye the seed from which ye sprang; Ye were not made to live like unto brutes, But for pursuit of virtue and of knowledge. So eager did I render my companions, With this brief exhortation, for the voyage, That then I hardly could have held them back. And having turned our stern unto the morning, We of the oars made wings for our mad flight, Evermore gaining on the larboard side.II
I Francesco Petrarca (1304-1374): Il Canzoniere (Rerum Vulgarium Fragmenta), componi-mento XXXV. Translation by William H. Fredlund II Dante Alighieri (1265-1321): La Divina Commedia, Inferno, Canto XXVI. Translation by Henry Wadsworth Longfellow

Many I met during the travel. Many accompanied me along the road, but then left for their own way. Many helped me: teaching me something or making me feel beloved. Now I am in debt to a lot of persons. If someone asks whether it was worthwhile, I will use the words of others:
Often it happens to explain to a young person why studying is profitable. It is useless to say that it is for love of knowledge, if he has not any love for know-ledge. Neither it is useful to say that the man who knows, faces events of life better than one who does not know, because he may point at someone that, although very learned, leads a miserable life. And then the unique answer is that the exercise of knowledge creates relationships, closenesses, affections, make us know some other Parents, different from our blood ones, make us live more, because we will rememember not only our life, but also others life, establish a fine thread going from our youth (sometimes childhood) until to-day. And all this is marvelous.III
Dedicated to Enza and Michele whose smile warms my life Dedicated to my parents because I still feel their hand on my shoulder
Dedicated to the memory of my Masters
III Umberto Eco (1932 – living): Come si paga un debito a rate (How to pay a debt by instal-ments ). In: L’Espresso 30th October 2003, Personal Translation

Papers making up the Thesis
The present doctoral thesis is based on the following original studies which will be referred to by their roman numerals.
I. Perchiazzi G, Högman M, Rylander C, Giuliani R, Fiore T, Hedenstierna G. Assessment of respiratory system mechanics by artificial neural net-works: an exploratory study. J Appl Physiol 90: 1817-1824, 2001
II. Perchiazzi G, Giuliani R, Ruggiero L, Fiore T, Hedenstierna G.Estimating respiratory system compliance during mechanical ventilation using artificial neural networks. Anaesth Analg 97: 1143-1148, 2003
III. Perchiazzi G, Rylander C, Vena A, Dello Russo ML, Brienza N, Giuliani R, Fiore T, Hedenstierna G. Measurement of total positive end-expiratory pressure during mechanical ventilation by artificial neural networks.Manuscript
IV. Perchiazzi G, Giuliani R, Vena A, Giustolisi O, Vetruccio T, Fiore T, He-denstierna G. Robustness of two different methods for estimating respira-tory system compliance during mechanical ventilation. Submitted


Contents
Introduction...................................................................................................11Background ..............................................................................................11
Connectionism and Artificial Neural Networks ..................................11Lung mechanics and pulmonary inhomogeneities...............................14
Review of Literature.................................................................................15
Rationale and aims of the studies..................................................................17
Materials and Methods..................................................................................18The animal model.....................................................................................18
Anaesthesia ..........................................................................................18Ventilation ...........................................................................................19Acute lung injury .................................................................................19
Respiratory variables recording................................................................20Technical setup ....................................................................................20
Data collection and computation of respiratory mechanics .....................20Study I..................................................................................................21Electrical analogue of the lung (Study I) .............................................22Study II and IV ....................................................................................22Study III...............................................................................................23Perturbation of the signal (Study IV)...................................................24Multilinear regression method (Study IV)...........................................25
Neural networks .......................................................................................26Choice of architecture and training......................................................26Computation of ANN performance .....................................................26
Results...........................................................................................................29Study I ......................................................................................................29Study II.....................................................................................................29Study III ...................................................................................................30Study IV ...................................................................................................31
Discussion.....................................................................................................32The problem of methods ..........................................................................33
Training the ANN................................................................................33From the results: solutions and uncertainties ...........................................34

Robustness ...........................................................................................35
Conclusions...................................................................................................36Study I ......................................................................................................36Study II.....................................................................................................36Study III ...................................................................................................37Study IV ...................................................................................................37
Perspectives ..................................................................................................38
Summary in Swedish ....................................................................................40
Acknowledgements.......................................................................................41
Bibliography .................................................................................................43

Abbreviations
ALI Acute Lung Injury ANN Artificial Neural Network ANNBIO Artificial Neural Network trained on tracings coming from an ani-
mal model of acute lung injury ANNMOD Artificial Neural Network trained on tracings coming from an elec-
trical analogue of the lung CRS Respiratory System Compliance EAO Equivalent of Airways Opening EEHM End-Expiratory Hold Maneuver EIHM End-Inspiratory Hold Maneuvre HL Healthy Lungs IRB Institutional Review Board IT Interrupter Technique MLF Multi-Linear Fitting MSE Mean Squared Error OA Oleic Acid P1 Pressure in the airways immediately after an inspiratory hold ma-
neuvre P2 Pressure in the airways 2 s after inspiratory hold manouvre PAW Pressure at airways opening PAW,EL Pressure at airways opening, elastic component PAW,MAX Peak Airway Pressure PAW,RES Pressure at airways opening, resistive component PAW,TOT Total Pressure at airways opening PEEP Positive End-Expiratory Pressure PEEPAPP Applied Positive End-Expiratory Pressure PEEPI Intrinsic Positive End-Expiratory Pressure PEEPTOT Total Positive End-Expiratory Pressure PR-P Prospective pool of curves, coming from the prospective group of
pigs RADD Additional Resistance RN Random Noise RRS Respiratory System Resistance SL Sick Lungs TD Transient Disconnection TE Expiratory Time

TeBIO-P Pool of curves coming from reference group of pigs, for testingANNBIO
TeMOD-P Pool of curves coming from the electrical analogue, for testingANNMOD
TI Inspiratory Time tINIFLOW time onset of inspiratory flow TrBIO-P Pool of curves coming from reference group of pigs, for training
ANNBIO
TrMOD-P Pool of curves coming from the electrical analogue, for testing ANNMOD
V Volume V’ Flow V’I Instantaneous flow at peak pressure VAW Volume exchanged at airways opening VC-MV Volume Controlled constant flow – Mechanical Ventilation V-P Volume / Pressure VT Tidal Volume
RS Respiratory System Time Constant

11
Introduction
BackgroundModern mechanical ventilation using positive pressures was born in Swe-
den in the middle of the twentieth century. Since then, medical research tried to arrive to new systems to deliver assisted mechanical ventilation. The more sophisticated and (theoretically) natural the pattern of ventilation was, the more difficult was the clinical application of the new techniques.
Modern machines for delivering mechanical ventilation are capable to cut out on patient needs the shapes of flow and pressure curves. Unfortunately the scientific and practical background required from the clinicians to use them, are so large that almost all over the world, the real users of this sophis-ticated technologies are a minority. Experience has shown that it is not a question of cultural diffusion. It is the intrinsic complexity of the problems to be faced that requires an appropriate approach.
The real reason of this situation is the attempt of using rule-based systems that, for their own nature are artificially created and cannot integrate com-pletely the entire spectrum of variables involved in the process of ventila-tion. We propose a change in the method of approaching this type of prob-lems. We realize the necessity of a system able to work with a large number of variables, but at the same time being powerful and flexible. One possible answer is in the Connectionism and in the Artificial Neural Networks (ANNs), that use methods that have these properties.
Connectionism and Artificial Neural Networks If we want to define it synthetically, Connectionism is the attempt to simu-late the biological intelligence on a computer. It consists of theories, ideas and computing techniques that represent a revolution in the study of mind and brain. We can say that it cuts the roots of the Cartesian dualism between mind and brain. It has developed by the observation that behaviours typical of human learning could be reproduced using networks of numerous simple units (the Artificial Neural Networks). A connectionist system has the possibility to learn to perform a particular task without needing an a-priori knowledge. This is the difference with the classical artificial intelligence, based on the so-called expert systems. In an expert system it is necessary first to analytically solve a problem, then trans-

12
late it to a computer, in order to obtain a procedure of calculation. In order to understand what are the limits of expert systems that ANNs can overcome, it is necessary to describe how a connectionist system works.
Figure 1. Feedforward Neural Network
ANNs simulate a network of neurons divided into layers. ANNs are com-posed of three kind of layers: input layer, hidden layers, output layer. Infor-mation enters the net via the input layer and after having propagated through the layers, arrive to the output layer. The net learns by examples. If we want to train an ANN to recognize images, it is necessary to feed it by giving the images at the input and at the same time, the output that we want has to as-sociate to the example. By using particular algorithms (as the error back-propagation algorithm) we modify the connections among the neurons in the intermediate layers, in order to have the right answer when we show an im-age to the ANN. An ANN “works” because each neuron receives inputs from the neurons belonging to the preceding layer. The neuron sums all the inputs arriving on itself and, if the sum reaches a threshold (like biological neurons), it discharges downwards. Each connection between two neurons has a weight. If a connection has a light weight, when the preceding neuron discharges on the next neuron, this last may be not activated, because the stimulus has not reached the threshold. In order to make that neuron acti-vated, it´s necessary that other stimuli, coming from other neurons of the preceding layer, arrive at the same time on it. Various kind of activation functions exist: step, sigmoid, linear, linear with saturation, gaussian, etc. Different architectures of ANNs and various algorithms of learning exist. After the training phase, during which it is possible to monitor the process of learning, ANNs acquire the capacity of generalizing.

13
Figure 2: Artificial Neuron
Like human learning, after the ANN has learnt the paradigmatic examples, it builds an internal representation of the rules it has extracted from the reality.
Figure 3: The process of training consists in adjusting the connection weights.
So if it has been trained to recognize the picture of apples, all kind of apples will be appropriately classified. It´s not a futile property. An expert system trained to perform the same type of task will stop each time that the rules to identify the apple do not correspond to the image (to be at the same time sufficiently red, round with green leaves, etc...).

14
An other property of ANNs is that the learning is ”strong”. If the network loses a neuron, the overall performance is only slighty affected (the knowl-edge is in the net of connections and not belonging to some particular neu-ron). The ANNs have also the capacity of extrapolate way of behaviour in situations that were not presented to them during the learning phase.
Figure 4: Training and testing neural networks (supervised training)
They recognize the intermediate situations among the known examples and react with intermediate answer. For example: if an ANN trained to recognize pictures of apples and oranges, is for the first time facing an assembled photo having the look of a hybrid between orange and apple, the answer will be, correctly, that the picture looks for the 30% an apple and for the 70% an orange. This property is impossible to be obtained with expert systems, that will react with a message of inability to classify.
When we move to complex problems, we can observe other useful fea-tures. The ANN builds an internal representation of input data. This is ex-tremely useful when we deal with signal processing problems or when the prediction of the behaviour of a complex system is required. This is the case of our application of ANN.
Lung mechanics and pulmonary inhomogeneities The mechanical properties of the respiratory system are often measured in mechanically ventilated patients in order to obtain information about lung pathology and to optimize ventilatory strategy. The gold standard is consti-

15
tuted by the interrupter technique (IT), which derives from the notion that after the inspiratory flow is stopped, the ratio between inspired volume and the subsequent pressure change, is related mainly to the static components of respiratory mechanics [5].
However, a prolonged breath-hold maneuver may have harmful conse-quences on unstable patients. Hence, different methods have been proposed for assessing respiratory mechanics during continuous mechanical ventila-tion. The widely used multi-linear fitting (MLF) method [32], can extract respiratory system compliance, assuming that the motion equation of the respiratory gases is composed of linear equations i.e. the mechanical proper-ties of the respiratory system are constant and time-invariant over the ana-lyzed breath.
However, in pathologic conditions, the lung, in most cases, exhibits in-homogeneous mechanical properties. One of the expressions of pulmonary inhomogeneity (i.e. mechanical behaviour defined by different time con-stants), is the change in morphology of the pressure/time curve at airway opening, during constant flow ventilation. In a perfectly homogeneous lung, during inspiration, the pressure trend is linear. In inhomogeneous lung, dur-ing inspiration the pressure rise is not linear and during the pause phase, there is a slow decay. The reason of this change in pressure is the pendelluft flow that redistribute volume between compartments that reached different end-inspiratory pressures, due to different time-constants. An Otis [48] lung model, can be used to simulate different conditions of pulmonary inhomoge-neity by changing the values of the implemented parameters. Although the determinants of this model are all analytically known, the practical use of these variables is difficult. In fact, the presence of inhomogeneous patholo-gies, introduces an error in estimating respiratory parameters that becomes more important during pathologic conditions. In these conditions it is possi-ble to verify that respiratory mechanics parameters may no longer be linear [55] and the accuracy of the method becomes lower, thus requiring correc-tions of the algorithm [34] or limiting the application of MLF to specific segments of the breathing cycle [26].
Review of Literature ANNs can learn different tasks, as confirmed by the increasing amount of literature of the last years. A review on the applications of ANNs to the dif-ferent fields of medicine was published by The Lancet in 1995 [7; 14; 17]. ANNs have been used as clinical decision support tools [15; 18; 22], for predicting the clinical likelihood of a pathological condition [50] , the chronicity in ICU patients [11; 45] or the possible successful weaning from mechanical ventilation [4; 42]. ANNs can also analyze signals of various sorts: electrocardiograms [12; 29-31; 46], electromyograms [2], electroen-

16
cephalograms [33; 53], haemodynamic variables recording [3], cardioto-cograms [40]. Other examples of utilization are: intelligent alarms for oper-ating rooms based on ANNs [47; 65] and use for monitoring the depth of anaesthesia [58]. ANNs have been used as classifiers of heart [21] and lung [20; 63] sounds and to support image analysis [1; 13; 19; 24].
We are proposing the use of ANNs in the respiratory monitoring of the in-tensive care units. In this wide field of possible applications, very little work has been done.
In a recent study [38] Leon and Lorini investigated the capability of ANNs to identify spontaneous and pressure support ventilation modes from gas flow and airway pressure signals. Wilks and English [66] used ANNs, in an exploratory experiment, to classify respiratory patterns in effective or not, in order to predict harmful changes of O2 saturation in infants. Snowden et al. [61], fed an ANN with blood gas parameters and the ventilator settings that determined them, in order to obtain new ventilator settings. However the limit of this study was that they trained an ANN using the rules of an expert system: in this situation ANNs cannot express all their properties. Bright et al. [9] have described the use of an ANN to identify upper airway obstruc-tion (UAO). The ANN was fed with six indices taken from the expiratory limb of a flow-volume loop and the performance obtained was better than human experts at identifying flow loops with UAO. Leon et al. [39] devel-oped a successful ANN-based system to detect esophageal intubation using airways flow and pressure signals. Räsänen and León [57], in a review pub-lished for the Yearbook 1995 of Emergency and Intensive Care Medicine, report some experiments (then published in 1998 [56]) in which they trained an ANN with the expiratory waveform of injured lungs of dogs. They gave to the ANN the tracings of healty and oleic acid injured lungs and the net had to classify the damage as absent or present (and to what extent). In two studies [51; 52] presented at the APICE Congress (held in Trieste, Italy dur-ing November 1998), Perchiazzi et al. have shown the possibility to assess the respiratory mechanics of inhomogeneous lungs (in a controlled ventila-tion setting) using ANN. Those exeperiments were performed using com-puter simulators of lung function.

17
Rationale and aims of the studies
After the review of literature and in consideration of the pending problem of measuring respiratory mechanics during ongoing mechanical ventilation, we wanted to study whether the application of ANNs could solve some of the problems encountered during clinical practice. A gradual approach has been decided, first testing whether ANNs presented a comparable performance to accepted methods under the same conditions; then applying ANNs to situa-tions potentially arising during clinical practice. One of the key-topics that emerged in the different studies preceding ours, is the close connection be-tween the training strategy (choice of examples and their number) and the quality of ANN performance. The issue of researching a suitable pool of data, effective for training the ANN on the single task, is addressed in each paper.In study I the aims of the experiments reported, were to evaluate in an ani-mal model:
1) whether ANNs can assess respiratory system resistance and com-pliance using the tracings of pressure at airways opening, instantane-ous inspiratory flow and tidal volume, during an end-inspiratory hold maneuver and 2) if it is possible to substitute the animal tracings, in the learning process, by simulations obtained by non-biological models.
In study II we evaluated in an animal model 3) whether ANNs can estimate respiratory system compliance using tracings of pressure and flow at airways opening, without any inter-vention of an inspiratory hold maneuver during continuous mechani-cal ventilation.
In study III we tested 4) whether artificial neural networks, fed by inspiratory airway pres-sure and flow, are able to measure intrinsic and total positive end-expiratory pressure (PEEP) during ongoing mechanical ventilation.
In study IV we evaluated and compared: 5) the robustness of ANN and multi-linear fitting methods in extract-ing respiratory system compliance when facing signals corrupted by perturbations likely to be found in the clinical environment.

18
Materials and Methods
In study I, the ANN had to extract the resistance and the compliance of the respiratory system when fed by curves having an end-inspiratory hold ma-neuver. An expert manually computed the two variables and these were used for training and testing the ANN. In study I, ANN performance was also tested on tracings produced by an electrical analogue of the lung developed via software on a computer. In study II and IV, the ANN was fed by curves not having an end-inspiratory hold maneuver and the ANN had to extract the compliance of the respiratory system. Its performance could be supervised because compliance was manually computed on a curve belonging to the same train of breaths. In study III, ANN had to extract the total positive end-expiratory pressure, using the tracings of pressure and flow at airways open-ing, during ongoing mechanical ventilation. In study IV, ANN had to esteem CRS using pressure tracings artificially perturbated by adding random noise or presenting interruptions of the signal continuity.
The animal model We needed to obtain pressure/time and flow/time curves of mechanically ventilated lungs, in health and in conditions of lung injury. We used pigs belonging to Yorkshire, Hampshire and Swedish mixed country breed. They were included in the studies, after approval by the local animal ethics com-mittee. A total of fifty animals were involved: fourteen in study I, twenty-six for study II and IV, ten in study III.
AnaesthesiaAfter premedication with azaperone (40 mg im, Stresnil, Janssen, Wien, Austria), given at the farm before the transportation, the pigs underwent general anesthesia. It was induced using atropine (0.04 mg/kg), tiletamin-zolazepam (5 mg/kg Zoletil, Boehringer Ingelheim, Copenhagen, Danmark) and medetomidin (5 g/kg, Dormitor Vet., Orion Pharma AB, Sollentuna, Sweden), injected intramuscularly in the neck. Then they were orally intu-bated using a cuffed endotracheal tube (in study I, II, IV: n. 6, Hi-Contour™, Mallinckrodt Medical, Athlone, Ireland; n. 5.5, Portex, Smiths Medical Inc, St Paul, USA in paper III). Anesthesia was maintained using a continuous

19
intravenous infusion of ketamine (20 mg/kg/h, Ketaminol, Vetpharma AB, Zurich, Switzerland), pancuronium (0.24 mg/kg/h, Pavulon, Organon Tek-nika, Göteborg, Sweden) and fentanyl (5 g/kg/h, Pharmalink, Spånga, Swe-den).
A constant infusion of Rehydrex® (Fresenius Kabi, Uppsala, Sweden) with glucose 25 mg/ml was given at the average rate of 5ml/kg/h. Fluid re-placement was constantly regulated in order to maintain a constant hemo-globin value and a stable systemic arterial pressure. For invasive arterial pressure measurement and arterial blood gas analysis, an 18 gauge catheter was inserted into the left carotid artery. A floating tip pulmonary artery (PA) catheter, together with an 18-gauge catheter, was introduced into the right external jugular vein. The position of the PA catheter was confirmed by the pressure traces on the connected bedside monitor (CS/3™, Datex Ohmeda, Helsinki, Finland). Measurement of oxyhemoglobin saturation (SaO2) was performed by a transcutaneous sensor (EarSat™, Datex Ohmeda, Helsinki, Finland). Cardiac output was measured in triplicates, by injection of a cold bolus (~10 ml, 3-5°C) of physiological saline randomly during the respira-tory cycle. A temperature sensor located in the PA catheter allowed continu-ous monitoring of blood temperature.
A catheter was surgically inserted into the bladder in order to measure uri-nary output. Arterial and mixed venous samples were taken to measure pO2,pCO2 and pH during the various phases of the experiment and to adjust the ventilator settings for normocapnia.
VentilationThe pigs were ventilated using volume controlled - constant flow mechanical ventilation (VC-CFMV) (Servo 900C for Sudies I, II and IV and Servo 300 for Study III; Siemens Elema, Solna, Sweden). At the beginning of the ex-periments, inspiratory-to- expiratory ratio was set to 1:2 [s]; tidal volume (VT) was adjusted to result in normocapnia (35-45 Torr) by using blood gas analysis. Inspiratory fraction of oxygen (FIO2) was 0.5. Extrinsic positive end-expiratory pressure (PEEPAPP) was initially set to 5 cmH2O.
Acute lung injury Oleic acid (OA) 0.1 ml/kg (Apoteksbolaget, Göteborg, Sweden) was frac-tionally injected directly into the central venous catheter in repeated doses of 0.5 ml. Before entering the circulation, it mixed in a three-way stopcock with the turbulent flow of a high-pressure washing line opened during the injec-tion. This procedure allowed as complete as possible dispersion of the OA into the infusate, avoiding large droplets. Administration of OA was sus-pended if SaO2 fell to 80%. Any fall in systemic arterial pressure during OA injection was countered using adrenalin, in boluses of 0.01 mg.

20
Respiratory variables recording Technical setup For studies I, II and IV we have used the same technical setup. A D-Lite connector (Datex Ohmeda, Helsinki, Finland) was mounted to the endotra-cheal tube. The two sampling ports of the D-Lite were connected to a differ-ential pressure transducer (Sensym, SensorTechnics, Pucheim, Germany). The transducer was calibrated at the beginning of each experimental session, using a water column for static pressures. Calibration of flow measurement was performed with a source of constant flow, the transducer to be calibrated and a precision flow meter (Calibration Analyzer TS4121/P, Timeter In-strument Corporation, St. Louis, MO, USA) connected in series. Moreover, by using a pneumatic short-circuit system [41] driven by a magnetic valve, it was possible to check the transducer for the zero point value at the beginning and repeatedly during the experimental sessions. Data from the transducer were collected by the Carina 2.4.0 acquisition program (C-O Sjöberg Engi-neering AB, Upplands-Väsby, Sweden), purposely written for the LabView acquisition system (LabView 4.0.1, National Instruments, Austin, TX, USA). The traces of flow and pressure, collected in real time at 200 Hz, were stored on the hard disk of a personal computer.
In study III, we recorded flow by a Fleisch pneumotacograph (Laminar Flow Element type PT, Special Instruments GmbH, Nördlingen, Germany) positioned between endotracheal tube and ventilator and connected to a dif-ferential pressure transducer (Diff-Cap Pressure Transducer, Special Instru-ments GmbH, Nördlingen, Germany). Calibration of flow measurement de-vice was performed in the same way as described for studies I, II, IV.
PAW was measured by a pressure transducer (Digima Clic Pressure Trans-ducers, Special Instruments GmbH, Nördlingen, Germany). Signals from transducers were forwarded to an analogic/digital converter card (DAQ-card AI-16XE50, National Instruments Corp., Austin, USA) and stored in a Per-sonal Computer (Intel Pentium III, Intel Corp., Santa Clara, USA) at a sam-pling frequency of 200 Hz, using the BioBench Software (ver.1.0, National Instruments Corp., Austin, USA).
Data collection and computation of respiratory mechanicsIn study I, II and IV we needed examples of tracings subtending different conditions of lung mechanics. The progressive worsening of the lung after the induction of damage, yields different "snapshots" of the respiratory me-chanics as reflected by RRS and CRS changing over the time (Paper I, Fig. 1) In the above mentioned three studies, pressure and flow tracings were re-
21
corded after a stabilization period (SP) of 60 minutes following instrumenta-tion and 5, 20, 35, 50, 65, 95, 125 minutes after the first administration of OA. In the period between 65 and 95 minutes after the first administration of OA, the PEEPAPP of 5 [cmH2O] was randomly changed to 0 or 10 [cmH2O]. After that, PEEP was returned to 5 cmH2O. Study III was centered on the estimation of PEEPTOT during mechanical ventilation and the strategy for gathering the required pool of data followed a different procedure, described later in this chapter.
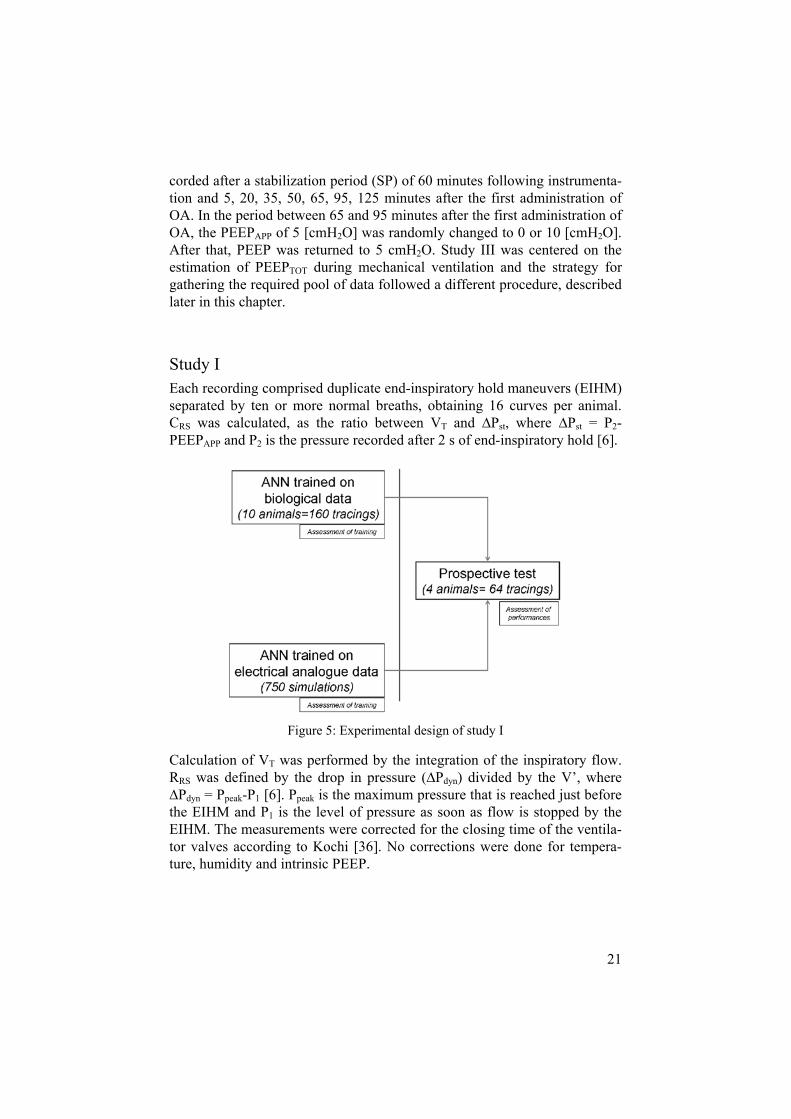
Study I Each recording comprised duplicate end-inspiratory hold maneuvers (EIHM) separated by ten or more normal breaths, obtaining 16 curves per animal. CRS was calculated, as the ratio between VT and Pst, where Pst = P2-PEEPAPP and P2 is the pressure recorded after 2 s of end-inspiratory hold [6].
Figure 5: Experimental design of study I
Calculation of VT was performed by the integration of the inspiratory flow. RRS was defined by the drop in pressure ( Pdyn) divided by the V’, where
Pdyn = Ppeak-P1 [6]. Ppeak is the maximum pressure that is reached just before the EIHM and P1 is the level of pressure as soon as flow is stopped by the EIHM. The measurements were corrected for the closing time of the ventila-tor valves according to Kochi [36]. No corrections were done for tempera-ture, humidity and intrinsic PEEP.

22
Electrical analogue of the lung (Study I) An electrical analogue of the lung was implemented on a computer via soft-ware (Pater program, University of Bari, Italy). It reproduced the model pro-posed by Otis in 1956 [48] and was composed of two parallel limbs con-nected to the equivalent of airways opening by a common resistance. Each limb consisted of a resistor and a capacitor, connected in series. This circuit is a bi-compartmental model of the lung. By changing the values of resis-tance and compliance, different conditions were simulated. "Ventilation" of the model is obtained by simulating the application of forcing currents, whose variation in time is equal to the ventilatory pattern. Resistance and compliance were kept constant and invariable over the time during each ventilatory session. Each session consisted of six respiratory cycles, in order to ensure that the last cycle was performed under steady state condition. The values assigned to each resistance and compliance were chosen in order to reproduce the same range of RRS, CRS and Time Constant ( RS=RRS•CRS) as found in the reference group of pigs .
Figure 6: Otis model of the respiratory system.
Study II and IV Each recording session comprised the simultaneous collection of pressure and flow in the airways coming from ten or more consecutive breaths in volume control – mechanical ventilation, followed by a breath having an End - Inspiratory Hold Maneuver (EIHM). EIHM was held until a stable plateau pressure was reached and never less than 2.5 seconds. In the refer-ence group of pigs, two recording sessions per time interval were performed, with 20 regular breaths in between, allowing the return to a steady state con-

23
dition before the second measurement. At the end, sixteen recording sessions per each of the sixteen animals were performed. In the prospective group of pigs, only one recording session was performed.
Figure 7: Experimental design of study II
Study III Study III was designed to create a condition of dynamic pulmonary hyperin-flation, by shortening expiratory time in proportion to the time constant of the respiratory system. Forty-five minutes after instrumentation a baseline recording of PAW and V’AW was obtained. A tracing of Volume (VRS) versus time was obtained from V’AW by integration. Using the slope of the expira-tory volume/flow curve, the expiratory RS was determined. This was used for calculating the ventilatory patterns of the following part of the experi-ment.
Maintaining constant minute ventilation and respiratory cycle time (TTOT),expiratory time was progressively shortened in proportion to expiratory RS.Experimental protocol comprised different recording sessions of PAW and V’AW, characterized by a TE equal to decreasing multiples of RS. TE was equal to 3.0, 2.5, 2.0, 1.5, 1.0 times RS. After setting TE to a predefined multiple of RS, ventilation with the new pattern was kept up to the reaching of a steady state. Then PAW and V’AW were recorded for 10 or more consecu-tive cycles, with the last breath having an end-inspiratory hold maneuver (EIHM) and an end-expiratory hold maneuver (EEHM). This last breath was used to estimate PEEPtot,dyn and PEEPtot,stat.
After the measurement at 1.0 times RS, TE was returned to three times RS and an additional resistance (RADD) was mounted in series to the endotra-
cheal tube, in order to rise tubing resistance and to artificially increase time constant of the system connected to the ventilator. The same protocol of progressive reduction of TE in proportion to multiples of RS was applied in presence of RADD. After the last recording, RADD was removed and TE was again returned to three times RS. After reaching a steady state of the new ventilatory condition, acute lung injury (ALI) was induced by repeated injec-tions of small boluses of oleic acid (OA).

24
After a period not shorter than 120 minutes, similar recording sessions having a progressive reduction of TE in proportion to RS were obtained. Then, as before, the same measures were repeated with an equal RADD.
Figure 8: Computer simulation showing that, being equal respiratory mechanics, minute volume and res-piratory cycle time, the progressive shortening of ex-piratory time leads to volume trapping (in A and B). Y-axis: volume; X-axis: time
Perturbation of the signal (Study IV) We tested two types of perturbation of the signal: Random Noise (RN) and transient Sensor Disconnection (TD). Random Noise is a noise signal that never repeats and has a flat frequency spectrum [43]. By definition it has a sampling distribution characterized by having zero mean and, in the case of our study, it had a uniform distribution around the mean. We tested the ef-fects of 25 different levels of RN on the pool of breaths. After the applica-tion of a given level of RN on all the pool of Mechanical Breaths (MB), MLF and ANN were used to extract CRS from the modified curves.

25
Figure 9: Experimental design of study IV
During the inspiratory phase of the respiratory cycle, a sensor disconnec-tion of the pressure sensor was simulated. Each level of TD was applied to the entire pool of curves. We tested 25 TD levels on the entire pool of MB.
Multilinear regression method (Study IV) This method is based on an inverse modeling technique that assumes that Pressure (PAW,TOT) in the airways is the sum of elastic (PAW,EL), resistive (PAW,RES), and constant components (Positive End-Expiratory Pressure, PEEP):
PAW,TOT = PAW,EL + PAW,RES + PEEP (1)
MLF stems from the assumption that the elastic and resistive components are linearly related to delivered volume and inspiratory flow, respectively.
PAW,EL = V/CRS (2) PAW,RES = V’·RRS (3)
Where RRS and CRS are the resistance and the compliance of the respiratory system, respectively. Then, the equation (1) takes the form of
PAW,TOT = V/CRS + V’·RRS + PEEP (4)
Having the tracings of PAW,TOT , V and V’ it is possible, by applying the least squares fitting method, to obtain CRS, RRS and PEEP.

26
Neural networks Choice of architecture and training The ANNs used in the four studies were implemented via software on a computer (Neural Networks Toolbox ver. 3.0 for MatLab ver. 5, The Math-Works Inc., Natick, MA, USA). The learning algorithm was resilient back-propagation. The ANNs consisted of three layers, whose activating functions were log-sigmoids for the input and intermediate layer and linear for the output layer. The number of neurons in the input layer was determined by the dimensions of the input pattern to be given. In study I it was composed of 162 neurons and corresponded to 3.2 seconds of recording, comprising an EIHM; in study II and IV it was composed of 100 neurons, corresponding to 50 equally spaced coordinates of PAW and V; in study III, it was of 40 neu-rons and corresponded to PAW and V’ recorded for 0.2 at the beginning of inspiration. The output layer consisted of 2 neurons for study I and 1 neuron in study II, III and IV.
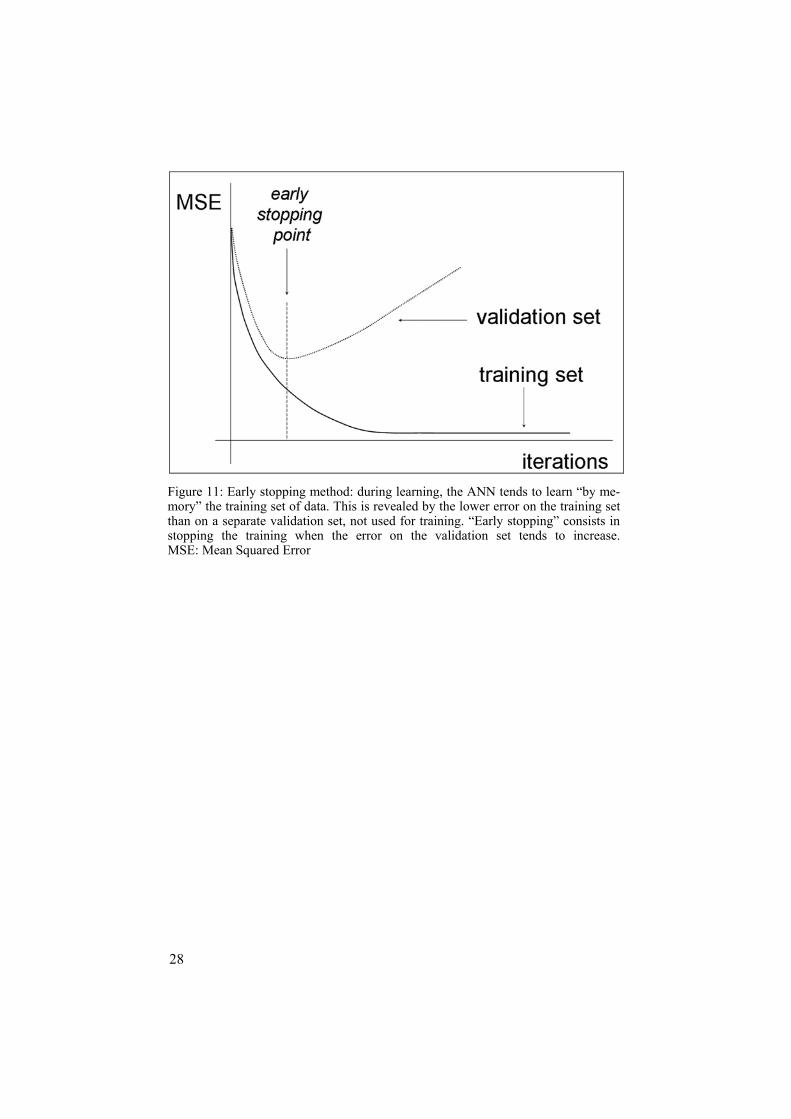
To determine the best architecture, i.e. the number of intermediate neu-rons that provided the best performance for the required task, we used a method known as eightfold cross-validation (fig. 10) with early stopping (fig.11). We tested architectures with a different numbers of intermediate neurons. The pool of data is divided in eight subgroups. The ANN architec-ture was trained on seven of the eight subgroups, using the one left out for assessing the Mean Squared Error (MSE). For each architecture, this proce-dure was performed eight times, leaving a different subgroup out. The mean of the obtained eight MSE is used for calculating the performance of each architecture. After choosing the best architecture, the ANN training starts. First, the available pool of curves is randomly divided into two new subsets, in the ratio of 80:20. The biggest subset is used for training the ANN, the smaller one to validate the learning process.
Computation of ANN performance In study I, two ANNs were trained (one for extracting mechanics from trac-ings produced by an electrical analogue and the other from tracings coming from the animal model). Their performance was assessed by computing the MSE, the linear regression between the results yielded by them versus the “true value” obtained by applying the interrupter technique. Then they had to face a prospective test, again MSE and linear regression were applied.

27
Figure 10: Cross-validation. Explanation in the text.
Moreover, on prospective test, a Bland-Altman analysis [8] of measurement agreement was performed. In study II, the ANN was trained and tested pro-spectively on animal data, not used for the training. Their performance was computed by calculating MSE, linear regression and Bland-Altman analysis. The available pool of data was also labeled as coming from “healthy” or “sick” animals and the ANN performance was separately assessed.
In study III, ANN performance was studied by linear regression and Bland and Altman analysis. Moreover we checked the dependency of esti-mation error from PEEPAPP and also the relation between ANN performance and PEEPtot,dyn.
In study IV, performance of ANN was calculated per each level of pertur-bation (25 levels of sensor disconnection and 25 levels of random noise), by means of Bland-Altman analysis, under the same conditions of perturbation.
In order to compare the scatters of the two methods (ANN and MLF) at each level of applied perturbation (RN and TD, separately), the F-test for variance comparison was performed.
28
Figure 11: Early stopping method: during learning, the ANN tends to learn “by me-mory” the training set of data. This is revealed by the lower error on the training set than on a separate validation set, not used for training. “Early stopping” consists in stopping the training when the error on the validation set tends to increase. MSE: Mean Squared Error

29
Results
Study I The architecture having the best performance for the required task (lowest average MSE over the eight sessions of cross-validation test) was the one with 27 intermediate neurons.
The performance of the ANN trained on the pool of animal (ANNBIO) data was expressed by a MSE of 0.00081 and a linear regression between neural network output and manually computed values with a regression coefficient of r = 0.97 for RRS and r = 0.99 for CRS. The performance of the ANN trai-ned on the pool of electrical analogue data (ANNMOD), showed an MSE of 0.00056; linear regression between output and manually calculated values had r = 0.99 on RRS and r = 1.00 on CRS. In the prospective test, linear re-gression between measured respiratory mechanics by ANNBIO and manually computed values, was expressed by r = 0.40 on RRS and r = 0.98 on CRS with MSE = 0.0037. For ANNMOD, regression was expressed by r = 0.61 on RRSand r = 0.98 on CRS with MSE = 0.0038. According to Bland and Altman method, the measurement error, expressed as mean±standard deviation, was for ANNBIO: -2.11 ± 4.61 [cmH2O·s·l-1] on RRS and 0.17 ± 1.14 [ml/cmH2O]on CRS. ANNMOD had on RRS: 0.36 ± 4.81 [cmH2O·s·l-1] and on CRS:1.57 ± 1.31 [ml/cmH2O].
Study II The best ANN architecture for the required task was the one with 25 inter-mediate neurons, which showed the lowest mean squared error (MSE) in the eight cross-validation tests. At the end of the training procedure, the chosen ANN presented a performance expressed by the linear regression y = 0.98x + 0.53 with r = 0.99 (r2 = 0.98), where x is CRS calculated accord-ing to interrupter technique (IT) and y is CRS extracted by ANN. Applying the previously trained ANN to the prospective group of data, the ANN per-formance in assessing CRS was expressed by (using the same notation as above) y = 0.94x + 1.69 with r = 0.97 (r2 = 0.94). Bland-Altman analysis of ANN versus IT methods for extracting CRS, showed a bias±standard devia-tion of –0.67 ± 1.52 [ml/cmH2O]. Analysis of the ANN performance in healthy (HL) and sick lungs (SL) separately, showed bias±standard deviation

30
of –0.46 ± 2.14 [ml/cmH2O] in HL and –0.75 ± 1.26 [ml/cmH2O] in SL. Comparing the two populations of errors (error in assessing CRS by ANN in HL and in SL), by the application of the two-tailed Student t-test, showed no significant difference between the two groups (p = 0.53). Linear regression of ANN error in assessing CRS (y) versus the average measure of CRS by ANN and IT (x), showed y = 0.03x - 1.23 with r = 0.12 (r2 = 0.01), not sig-nificant. Thus, the severity in lung pathology, as assessed by CRS, had no influence on the relationship between ANN and IT. Moreover, the error in estimating CRS from recordings made at PEEP = 0 and PEEP = 10 is not different from the error obtained from recordings at PEEP = 5.
Study III Total PEEP, measured in dynamic conditions, presented a tendency to in-crease while shortening expiratory time, passing from 3.48 ± 3.46 cmH2O (at TE = 3 RS) to 5.93 ± 3.93 cmH2O (at TE = 1 RS), at PEEPAPP = 0. When PEEPAPP was 5 cmH2O, PEEPtot,dyn rose from 6.36 ± 1.34 cmH2O (at TE = 3 RS) to 10.51 ± 5.98 cmH2O (at TE = 1 RS). At PEEPAPP of 10 cmH2O, PEEPtot,dyn changed from 10.99 ± 0.98 cmH2O (at TE = 3 RS) to 13.82 ± 2.83 cmH2O (at TE = 1 RS).
When PEEP was measured in static conditions, a similar tendency to-wards higher values at short expiratory times was found. In fact at PEEPAPP= 0 cmH2O, PEEPtot,stat raised from 4.11 ± 4.08 cmH2O (at TE = 3 RS) to 13.92 ± 6.41 cmH2O (at TE = 1 RS); at PEEPAPP = 5 cmH2O, PEEPtot,statvaried from 6.49 ± 2.17 cmH2O (at TE = 3 RS) to 17.82 ± 7.74 cmH2O (at TE = 1 RS); at PEEPAPP = 10 cmH2O, PEEPtot,stat changed from 11.25 ± 2.77 cmH2O (at TE = 3 RS) to 20.40 ± 6.53 cmH2O (at TE = 1 RS). In our ex-perimental setting, the relation between PEEPtot,dyn and PEEPtot,stat, extracted by the same tracings, was expressed by a linear regression of y = 0.25x + 1.11 and a r2 = 0.24
We found that the best ANN architecture for the required task, after the cross-validation with early stopping procedure, was the one with 18 interme-diate neurons. The linear regression between ANN estimation of PEEPtot,statand the reference measurement (based on EEHM), was described by y = 1.0001x + 0.397 with a coefficient r = 0.94. Bland Altman analysis of estimation error by ANN, showed -0.40 ± 2.84 (expressed as bias±standard deviation). Linear regression of estimation error by ANN versus PEEPAPP,had an equation of y = 0.11x - 0.87 and a coefficient r = 0.1.
When analyzing estimation error by ANN in computing PEEPtot,dyn, bias and standard±deviation were -3.30 ± 5.76 cmH2O .

31
Study IV In the absence of perturbations, ANN estimated CRS, presenting a perform-ance (expressed as bias±standard deviation) of 0.02 ± 1.02[ml/cmH2O]; in the same conditions and using the same notation as above, the MLF algo-rithm showed a performance of –1.97 ± 2.57 [ml/cmH2O].
When testing the application of a perturbation constituted by a Random Noise (RN), MLF -based algorithm presented a lower scatter than the ANN based algorithm throughout the entire test, except when RN was 2%.
At each level of applied RN, the population of measurement error was normally distributed. The difference between the two scatters at each level of applied RN was evaluated by the F-test for variance comparison and it was found to be statistically significant. Biases of the MLF algorithm and of ANN were significantly correlated with the level of applied random noise.
When simulating disconnection of the pressure sensor, ANN showed a lower scatter than MLF in estimating CRS at each level of applied TD.
The measurement error was normally distributed at each level of applied TD, for both ANN and MLF. The F-test for variance comparison revealed that at each level of TD, the scatters of MLF and ANN algorithms were sta-tistically different. Linear regression between TD level and bias of the two algorithms had no statistical significance.

32
Discussion
Knowledge in artificial neural networks is gathered by learning of examples. The critical point in creating one ANN for a specific purpose is the choice of the examples. In the four studies on which this comprehensive summary is based on, discussion of results has left an important place to the methods used to gain the required training. Scientists working in the field of applied Life Sciences may have difficulties in obtaining the bulk of examples that, in theory, would warrant a perfect training. Luckily, ANNs exhibit a property known as capacity of generalizing knowledge. This means that they can, suitably trained, interpolate and extrapolate from key examples the correct response. On the other side, our effort was to exploit biological models (por-cine model of a ventilated patient) and mathematical analogues (bi-compartmental Otis model) in order to create arrays of examples covering the range of possible situations that the trained ANN would have faced dur-ing its real use. We will differentiate, in this Discussion, the problem of methods from the implications of the obtained results.
Figure 12: Location of knowledge. ANN can extract informa-tion from complex tracings, provided that the required infor-mation is located in the signal.

33
The problem of methods Training the ANN The first step in the studies we have performed, was to dimension the ANN for the required tasks. While the number of neurons forming the input and output layer are directly imposed by the dimension of the input pattern (i.e. dimension of the tracing) and the dimension of the required output, respec-tively, the determination of the number of intermediate neurons is not straightforward.
In the four studies, we have used an empirical approach to the selection of ANN architecture to be used on the single tasks. We have used a pool of data to train in batch mode different ANN architectures, varying for the number of intermediate neurons. This method has the advantage of selecting the ar-chitecture on the basis of effective performance on the required task. After having decided architecture, ANNs were trained. Each ANN started with random weights assigned to its connections and the process of learning con-sisted in adjusting them. Although two networks having the same architec-ture can show similar performance on the same task, in reality they start the process of learning from different "backgrounds". This background is the random assignment of weights to the ANN when it is initialized. This means that, in order to observe similar performance by two physically similar ANNs, it is necessary to push the number of iterations to a high number. In order to optimize our computational resources, we preferred stopping the training after a discrete number of iterations and evaluate the performance [27]. The ANNs with the lower MSE were the ones in which the conver-gence to a minimum error was also driven by a favorable random matrix of weights assigned at the beginning.
In study I, we have used an electrical analogue of the lung, mathemati-cally implemented on a computer, in order to evaluate its usefulness in train-ing an ANN. It is a noise-free source of data that can simulate infinite com-binations of RRS and CRS. By this way it is possible to obtain tracings created by combinations of RRS and CRS that, although possible, are unlikely to be found in the spectrum of natural variability. The results of study I show that the model of lung may play an important role. It is necessary to be aware that an ANN trained on a model, will reproduce that model. Then, models should be (carefully) used to create system behaviors generated by extreme parameters. Changes in system intrinsic properties (as passing from linearity to non-linearity) may require the use of other types of model.
In the present thesis, we did not deal with the so-called computational burden necessary for training and testing one ANN. Our opinion is that de-velopment of technology will solve this issue, by providing more and more powerful computers. Another aspect, worth to be cited, concerns the rela-tionship between optimal training and ANN performance in the medical

34
field. We hypothesize that, in future time, an approach to the safety of ANN-based monitoring technology will be necessary. In fact, ANNs trained by different researchers to perform similar tasks will appear. The task of provid-ing objective tests of ANN performance should be provided by Health Care Authorities, may be using reference pool of data.
Moreover, nowadays it is already possible to implement in a computer a self-training ANN [16], capable of modifying its knowledge during its use. The practical effect of this unsupervised knowledge (particularly in medical field) is far from being completely conceived.
From the results: solutions and uncertainties Our explorative studies on the application of ANN technology to respiratory mechanics, has yielded at the same time, solutions and uncertainties. We believe they represent a starting point: may be more valuable for the effort in finding a method than for the results by themselves.
In Study I, results have shown the feasibility of extracting respiratory me-chanics by ANNs. A first caveat has come out from the discrepancy between the performances on assessing CRS and RRS. The results suggested that better control on ANN training might have been obtained by using two different ANNs, one for extracting CRS the other for RRS. The issue of which ANN yields an optimal performance on RRS extraction has not been addressed in the framework of this thesis, although a future study seems worth.
Study II demonstrated the possibility of assessing CRS without needing to stop inspiratory flow, presenting a good performance in “healthy” and “sick” conditions of the lung. This finding may result in a clinical advantage: it profits from the ANN property of extracting information from signals. The ANN of study II, can be used when a close monitoring of CRS is necessary and repeated breath hold maneuvers rise concerns about gas exchange in hemodynamically unstable patients. We are aware that CRS is not a single point: it is a function, sometimes also complicate, of different variables. We would place this method of extracting CRS by ANN, in the context of moni-toring technology than in the group of research tools. The same applies to the ANN of paper III. Here we demonstrated the possibility of assessing PEEPi, without needing to apply an end-expiratory hold maneuver. The per-formance by this ANN was good, suggesting a possible role in continuous PEEPi monitoring.
The difference between a monitoring tool and a research tool, may appear as a trivial matter. It depends on the idea that measuring a physiological variable is simply an act of research, an attempt to know the true numberexpressing that particular variable. The consequence is that the property of the measurement the scientist tries to obtain is mainly precision.

35
When facing the problem of monitoring a variable or controlling a ma-chine, precision is no longer the main property of the measures to aim at. More important become robustness because of the possibility of noise and malfunction of the sensors. Whatever kind of interfacing system between sensors and machines, if developed for working in real life (and not in aca-demic laboratories) has to be based on a platform that presents this property.
RobustnessPaper IV was devoted to evaluate robustness of ANN performance. The idea of investigating this topic stemmed from the studies of Kerlirzin on robust-ness of multi-layer perceptrons [35]. Robustness of a method is the property for which degradation of performance, in case of corrupted inputs, is slow and smooth. So a method is robust if it “works well not only under ideal conditions, but also under conditions representing a departure from an as-sumed distribution or model” [59]. The main finding of the paper is that ANNs show a stable performance also in presence of transient sensor dis-connection. This is important when the output of a neural network has to be used to guide another machine. While noise (like random noise) can be eas-ily filtered out, sudden changes in signal characteristics (like the discontinui-ties represented by sensor disconnection) render it unsuitable for feeding a control system.

36
Conclusions
Study I Both ANNs, the one trained on animal data and the one trained on the elec-trical analogue of the lung, were able to learn the relation between the input pattern and the corresponding RRS and CRS. This fact is demonstrated by the performance shown on their respective test groups, expressed by a regression coefficient r no lower than 0.97. In the prospective tests, the performance on CRS remained very good, in both ANNs. However this was not true for RRS.In fact the regression coefficient of ANN performance versus manually com-puted results, was 0.98 for CRS (in both networks) but only 0.40 (in ANNBIO)and 0.61 (in ANNMOD) for RRS. It is possible to conclude that:
1) The estimation of CRS and RRS by ANNs, using the tracings of PAW, V’I and VT, during an end-inspiratory hold maneuver, is feasible.
2) The use of tracings obtained by non-biological models in the learning process, has the potential of substituting biologi-cal recordings.
Study II In this study, ANN assessed the CRS with a low error and a low scatter in both healthy and diseased lungs. The amount of error was not statistically different in healthy and sick lung conditions; the ANN error had no depend-ency from the absolute level of CRS. Study II showed that
3) respiratory system compliance can be estimated by artifi-cial neural networks during volume control mechanical venti-lation, without having to stop inspiratory flow.

37
Study III In terms of linear regression, ANN estimated PEEPtot,stat with a very good correlation and a close proximity of the regression line to the identity line. Bland and Altman analysis, shown low bias and scatter of ANN estimation of PEEPtot,stat. No dependency was found between estimation error by ANN and PEEPapp. Considering that PEEPapp can be easily read on the ventilator display and that PEEPi=PEEPtot-PEEPapp we can conclude that:
4) ANN can estimate PEEPtot,stat and thus PEEPi reliably, dur-ing ongoing mechanical ventilation, without needing to exe-cute an end-expiratory hold maneuver
Study IV Our results show that in case of RN application test, the MLF-based method had a lower bias and scatter than the ANN-based algorithm, except for situa-tions in which the application of random noise was lower than 2% of PAW,MAX. However, the ANN-based algorithm presented a lower bias and scatter than the MLF-based method in the whole TD test. We can conclude that:
5) after the application of RN, ANN and MLF maintain a sta-ble performance, although in these conditions MLF may show better results. ANN have a more stable performance and yield a more robust estimation of CRS than MLF in conditions of transient sensor disconnection.

38
Perspectives
In recent times, research in mechanical ventilation is aiming at building in-telligent machines able to interface patient's respiratory variables with venti-lators. Different modalities of ventilation exist, but not all simple to be ap-plied at bedside. The consequence of these two needs ("interface" and "sim-plify") together with the availability of new engineering solutions, is bring-ing towards closed loop approaches to mechanical ventilation. The idea is to use signals coming from the patient to control mechanical ventilation [54].
Among the reasons that urged us to investigate the application of ANN to the estimation of respiratory mechanics is the possibility of using them as tool for feeding control systems to be included in a mechanical ventilator [28]. The studies on which this thesis is based on, represent a first step in this area of research. It was necessary to start with strict experimental conditions (like controlled ventilation and an animal model) to explore this issue. A second phase will be devoted to study the integration of the physiological variables involved in artificial ventilation and to control the system able to deliver it.
We believe that the future of mechanical ventilation is not in the research for new and more complex pattern of ventilation. The future will be in build-ing a system able to simulate the control centers of respiration (using ANNs or other technologies) in order to build a prosthesis of the respiratory centers in the brain stem.
The challenge for controlling a mechanical ventilator in closed-loop be-gan during 1950’s [23; 60]. Since then various approaches have been tried [10], however the passage from laboratories to clinical practice has been difficult. Development of computer technology has made available several interfacing methods: apart from ANN, fuzzy logic and neuro-fuzzy systems can also play a role [37; 44; 64]. On the other side monitoring technology has produced commercially available devices for on-line blood gas analysis [25; 49; 62]. It is not difficult to imagine their application to closed-loop mechanical ventilation.
History of Science of XX century has demonstrated that often the drivingforce for solving research problems has been the Industry. However in this field, despite the availability of the previously described technologies, Uni-versities have to take back a leading role. In fact, although all the compo-nents are easily available (monitoring technology and powerful computers), it is necessary to re-consider the basic philosophy of artificial ventilation.

39
Taken for granted the purpose of keeping alive an insufficiently-ventilatingsubject (which was the aim of the newborn mechanical ventilation), how to take a step forward? Our opinion is that Imitation of Nature, reproducing closely the activity of the brain stem may be a good philosophy of investiga-tion. This will require time, studies and integration of information from dif-ferent fields. On the horizon looms the possibility of miniaturize sensors and circuits, in order to assist ventilation from the inside: this is the promise of the new developing biomedical nano-technologies.

40
Summary in Swedish
Syftet med avhandlingen är att undersöka möjligheten att använda artificiell intelligens (Artificial Neural Networks, ANN) för att beräkna andningsme-kaniska variabler under mekanisk ventilation (MV).
Vi undersökte i en djurmodell med akut lungskada om ANN kan beräkna respiratorisk resistans (RRS) och compliance (CRS) utifrån registreringar av luftvägstryck (PAW) inandningsflöde (V´) och andningsvolym under en än-dinspiratorisk paus för att säkerställa kvasistatiska förhållanden. Vi fann att ANN kan beräkna CRS och RRS under dessa betingelser. Vi fann också att icke biologiska signaler (matematisk modell) kan användas för upplärning av ANN, vilket minskar behovet av biologiska träningsförsök.
Vi undersökte om ANN kan beräkna CRS utifrån registreringar av PAW och V´ utan användning av en ändinspiratorisk paus under MV, dvs under dyna-miska förhållanden. Vi fann att CRS kan bestämmas med hjälp av ANN under dessa betingelser. Konventionell teknik för bestämning av CRS är i dessa fall ej möjlig att använda.
Vi undersökte om ANN med registrering av PAW och V kan beräkna statiskt totalt positivt ändinspiratoriskt tryck (PEEPtotstat) under pågående MV. Vi skapade en dynamisk hyperinflation av lungan i en djurmodell genom att stegvis korta ner utandningstiden. Olika nivåer av externt PEEP (PEEPAPP)användes i försöken. Resultaten visade att ANN kan tillförlitligt bestämma PEEPtotstat vid alla testade grader av hyperinflation av lungan.
Slutligen jämfördes stabiliteten (“robustness”) vid beräkningar av CRS med hjälp av ANN och jämförelser gjordes med multilinjära regressionsanalyser (MLF). Jämförelser gjordes vid olika grader av störningssignaler pålagrade den ursprungliga mätsignalen och vid varierande avbrott i mätsignalen. När en brussignal pålagrades mätsignalen visade både ANN och MLF god för-måga att beräkna CRS under det att ANN gav mer stabila resultat vid avbrott i mätsignalen.
Sammanfattningsvis anser vi att ANN är en mycket intressant teknik för beräkning av andningsmekaniska variabler.

41
Acknowledgements
Five years have past; five summers, with the length Of five long winters! and again I hear These waters, rolling from their mountain-springs With a soft inland murmur.- Once again Do I behold these steep and lofty cliffs, That on a wild secluded scene impress Thoughts of more deep seclusion; and connect The landscape with the quiet of the sky IV
Some old persons coming from south-italian countryside, affirm that saying “thank you” is a nice way to close the accounts with other people. They usu-ally become upset if a friend thanks them, because they perceive a message of settling the relationship without anything more to claim. This is not the case. I want to affirm the opposite: I am in debt for life.
In Sweden I learned more than a PhD program could have given to me. Coming from a chaotic society, typical of a Mediterranean city, I was ama-zed at seeing the Nordic style of life. So, when people started betting on my survival time at the freezing temperatures of January in Uppland, my Swed-ish friends allowed me to enter their houses. It was for me a real revelation. May be it was for the quarter of blood coming from my Norman ancestors (Bari, my city, during the Middle Age was Norman) that I start feeling like I lived there since ever.
Now it is difficult for me to depict in a few lines what each single person has given to me, also because, if I try to remember those years of my life,
[…]things beheld which to repeat Nor knows, nor can, who from above descends; Because in drawing near to its desire Our intellect ingulphs itself so far, That after it the memory cannot go V
IV William Wordsworth (1770-1850): Lines Composed a Few Miles above Tintern Abbey, On Revisiting the Banks of the Wye during a Tour. July 13, 1798. V Dante Alighieri (1265-1321): La Divina Commedia, Paradiso, Canto I. Translation by Henry Wadsworth Longfellow.

42
Göran Hedenstierna, for my life has represented an exceptional and lucky encounter. Supervisor with endless patience towards young researchers, he is a Master of Life and Science. He conveyed to me the Flame of Curiosity in the steady hands of the Method. His name will live in my deep thoughts and in my more impassioned discourses for ever.
Karin Fagerbrink, Eva-Maria Hédin and Agneta Ronéus, are the differ-ence between the Idea and the Achievement. They transform into reality the Pyndaric flights of researchers.
Marieann Högman introduced me into the world of laboratory research. Although our professional ways separated, I remember affectionately all the time we spent together.
My colleague Christian Rylander has given to me the pleasure of long and profitable scientific discussions giving birth to a strong co-authorship and a greater friendship.
Luise Andrée and Birgit Andersson are the fine thread linking the deep South of Europe to the fresh plains of the Upplands. They represent the warm continuity of a long-lasting harmony in our research group.
Staffan Dahl satisfied all my informatics desires for the neural networks, also the most unspeakable (and I must confess that my requests were some-times really complicated).
Brian Högman: saying that he provided me a strong engineering and logis-tic support when I lived in Uppsala is only part of the truth. He was the first to show me the warmth of Sweden, opening his house to me. I will not forget our walks in the winter snowy woods together with Peter and Flaks, discuss-ing about the future of mechanical ventilation.
Carl-Olof Sjöberg, Åke Larsson and Sergio Santostasi have projected and built the data acquisition systems I have used during the different phases of these studies, promptly helping me with technical support.
Orazio Giustolisi in a cold December of 1994, told me for the first time about the wonders of artificial neural networks and taught me their use.

43
Bibliography
[1] Abe H, Ashizawa K, Li F, Matsuyama N, Fukushima A, Shirai-shi J, Macmahon H and Doi K. Artificial neural networks (ANNs) for differential diagnosis of interstitial lung disease: results of a si-mulation test with actual clinical cases. Acad Radiol 11: 29-37, 2004.
[2] Abel EW, Zacharia PC, Forster A and Farrow TL. Neural net-work analysis of the EMG interference pattern. Med Eng Phys 18: 12-17, 1996.
[3] Allen J and Murray A. Comparison of three arterial pulse wave-form classification techniques. J Med Eng Technol 20: 109-114, 1996.
[4] Ashutosh K, Lee H, Mohan CK, Ranka B, Mehrotra K and Alexander C. Prediction criteria for successful weaning from respi-ratory support: statistical and connectionist analyses. Crit Care Med20: 1295-1301, 1992.
[5] Bates JHT, Baconnier P and Milic-Emili J. A theoretical analysis of interrupter technique for measuring respiratory mechanics. J Appl Physiol 64: 2204-2214, 1988.
[6] Bates JHT, Rossi A and Milic-Emili J. Analysis of the behavior of the respiratory system with constant inspiratory flow. J Appl Physiol58: 1840-1848, 1985.
[7] Baxt WG. Application of artificial neural networks to clinical medi-cine. Lancet 346: 1135-1138, 1995.
[8] Bland JM and Altman DG. Statistical methods for assessing agre-ement between two methods of clinical measurement. Lancet 1: 307-310, 1986.

44
[9] Bright P, Miller MR, Franklyn JA and Sheppard MC. The use of a neural network to detect upper airway obstruction caused by goi-ter. Am J Respir Crit Care Med 157: 1885-1891, 1998.
[10] Brunner JX. History and principles of closed-loop control applied to mechanical ventilation. Nederlandse Vereniging voor Intensive Care 6: 6-9, 2002.
[11] Buchman TG, Kubos KL, Seidler AJ and Siegfort MJ. A com-parison of statistical and connectionist models for the prediction of chronicity in a surgical intensive care unit. Crit Care Med 22: 750-762, 1994.
[12] Camps-Valls G, Martinez-Sober M, Soria-Olivas E, Magdalena-Benedito R, Calpe-Maravilla J and Guerrero-Martinez J. Foetal ECG recovery using dynamic neural networks. Artif Intell Med 31: 197-209, 2004.
[13] Coppini G, Diciotti S, Falchini M, Villari N and Valli G. Neural networks for computer-aided diagnosis: detection of lung nodules in chest radiograms. IEEE Trans Inf Technol Biomed 7: 344-357, 2003.
[14] Cross SS, Harrison RF and Kennedy RL. Introduction to neural networks. Lancet 346: 1075-1079, 1995.
[15] Cross SS, Harrison RF and Sanders DS. Supporting decisions in clinical medicine: neural networks in lower gastrointestinal haemor-rhage. Lancet 362: 1250-1251, 2003.
[16] Demuth H and Beale M. Adaptive filters and adaptive training. In: Neural Networks Toolbox user's guide, Natick: The Mathworks, 2002, p. 10.2-10.26.
[17] Dybowski R and Gant V. Artificial neural networks in pathology and medical laboratories. Lancet 346: 1203-1207, 1995.
[18] Ennett CM, Frize M and Charette E. Improvement and automa-tion of artificial neural networks to estimate medical outcomes. Med Eng Phys 26: 321-328, 2004.
[19] Evander E, Holst H, Jarund A, Ohlsson M, Wollmer P, Astrom K and Edenbrandt L. Role of ventilation scintigraphy in diagnosis of acute pulmonary embolism: an evaluation using artificial neural networks. Eur J Nucl Med Mol Imaging 30: 961-965, 2003.
[20] Folland R, Hines E, Dutta R, Boilot P and Morgan D. Compari-son of neural network predictors in the classification of tracheal-

45
bronchial breath sounds by respiratory auscultation. Artif Intell Med31: 211-220, 2004.
[21] Folland R, Hines EL, Boilot P and Morgan D. Classifying coro-nary dysfunction using neural networks through cardiovascular aus-cultation. Med Biol Eng Comput 40: 339-343, 2002.
[22] Frize M, Ennett CM, Stevenson M and Trigg HC. Clinical deci-sion support systems for intensive care units: using artificial neural networks. Med Eng Phys 23: 217-225, 2001.
[23] Frumin MJ, Bergman MA and Holaday DA. Carbon dixide and oxygen blood level with a carbon dioxide controlled artificial respi-rator. Anaesthesiology 20: 313-321, 1959.
[24] Fukushima A, Ashizawa K, Yamaguchi T, Matsuyama N, Haya-shi H, Kida I, Imafuku Y, Egawa A, Kimura S, Nagaoki K, Honda S, Katsuragawa S, Doi K and Hayashi K. Application of an artificial neural network to high-resolution CT: usefulness in dif-ferential diagnosis of diffuse lung disease. AJR Am J Roentgenol183: 297-305, 2004.
[25] Gehrich JL, Lubbers DW, Opitz N, Hasmann DR, Miller WW, Tusa JK and Yafuso M. Optical fluorescence and its application to an intravascular blood gas monitoring system. IEEE Trans Biomed Eng BME-33: 117-132, 1986.
[26] Guttmann J, Eberhard L, Wolff G, Bertschmann W, Zeravik J and Adolph M. Maneuver-free determination of compliance and re-sistance in ventilated ARDS patients. Chest 102: 1235-1242, 1992.
[27] Haykin S. Cross-Validation. In: Neural Networks: a comprehensive foundation, edited by Haykin S. London: Prentice-Hall Interna-tional, 1999, p. 213-218.
[28] Haykin S. Dynamically driven recurrent networks. In: Neural Net-works: a comprehensive foundation, edited by Haykin S. London: Prentice-Hall International, 1999, p. 732-789.
[29] Hedén B, Ohlsson M, Edenbrandt L, Rittner R, Pahlm O and Peterson C. Artificial Neural Networks for Recognition of Electro-cardiographic Lead Reversal. Am J Cardiol 75: 929-933, 1995.
[30] Hedén B, Ohlsson M, Rittner R, Pahlm O, Haisty WK, Jr., Pe-terson C and Edenbrandt L. Agreement between artificial neural networks and experienced electrocardiographer on electrocardio-

46
graphic diagnosis of healed myocardial infarction. J Am Coll Car-diol 28: 1012-1016, 1996.
[31] Hedén B, Ölin H, Rittner R and Edenbrandt L. Acute myocardial infarction detected in the 12-lead ECG by artificial neural networks. Circulation 96: 1798-1802, 1997.
[32] Iotti G, Braschi A, Brunner J, Smits T, Olivei M, Palo A and Veronesi R. Respiratory mechanics by least squares fitting in me-chanically ventilated patients: applications during pressure support ventilation. Intensive Care Med 21: 406-413, 1995.
[33] Jandó G, Siegel RM, Horváth Z and Buzsáki G. Pattern recogni-tion of the electroencephalogram by artificial neural networks. Elec-troencephalogr Clin Neurophysiol 86: 100-109, 1993.
[34] Kano S, Lanteri CJ, Duncan AW and Sly PD. Influence of nonlinearities on estimates of respiratory mechanics using multilin-ear regression analysis. J Appl Physiol 77: 1185-1197, 1994.
[35] Kerlirzin P and Vallet F. Robstness in Multilayer Perceptrons. Neural Computation 5: 473-483, 1993.
[36] Kochi T, Okubo S, Zin WA and Milic-Emili J. Flow and volume dependence of pulmonary mechanics in anesthetized cats. J Appl Phisiol 64: 441-450, 1988.
[37] Kwok HF, Linkens DA, Mahfouf M and Mills GH. Rule-base derivation for intensive care ventilator control using ANFIS. Artifi-cial Intelligence in medicine 29: 185-201, 2003.
[38] Leon MA and Lorini FL. Ventilation mode recognition using arti-ficial neural networks. Comp Biomed Res 30: 373-378, 1997.
[39] Leon MA, Räsänen J and Mangar D. Neural network-based detec-tion of esophageal intubation. Anesth Analg 78: 548-553, 1994.
[40] Liszka-Hackzell JJ. Categorization of fetal heart rate patterns using neural networks. J Med Syst 25: 269-276, 2001.
[41] Meriläinen P, Hänninen H and Tuomaala L. A novel sensor for routine continuous spirometry of intubated patients. J Clin Monit 9: 374-380, 1993.
[42] Mueller M, Wagner CL, Annibale DJ, Hulsey TC, Knapp RG and Almeida JS. Predicting extubation outcome in preterm new-

47
borns: a comparison of neural networks with clinical expertise and statistical modeling. Pediatr Res 56: 11-18, 2004.
[43] National Instrument measurement encyclopedia. Definition of random noise. Available at: zone.ni.com. Accessed 6-9-2004
[44] Nemoto T, Hatzakis GE, Thorpe CW, Olivestein R, Dial S and Bates JHT. Automatic control of pressure support mechanical venti-lation using fuzzy logic. Am J Respir Crit Care Med 160: 550-556, 1999.
[45] Nimgaonkar A, Karnad DR, Sudarshan S, Ohno-Machado L and Kohane I. Prediction of mortality in an Indian intensive care unit. Comparison between APACHE II and artificial neural net-works. Intensive Care Med 30: 248-253, 2004.
[46] Olsson SE, Ohlsson M, Ohlin H and Edenbrandt L. Neural net-works--a diagnostic tool in acute myocardial infarction with con-comitant left bundle branch block. Clin Physiol Funct Imaging 22: 295-299, 2002.
[47] Orr, J. A. and Westenskow, D. R. Evaluation of a breathing circuit alarm system based on neural networks. Anestesiology 73, A445. 1990.
[48] Otis AB, Mckerrow CB, Bartlett RA, Mead J, Mcilroy MB, Sel-verstone NJ and Radford EP. Mechanical factors in distribution of pulmonary ventilation. J Appl Physiol 427-443, 1956.
[49] Palmer TEA, Cumpston PHV, Foster WJ and Jones RDM. Con-tinuous intravascular blood gas analysis during aortic aneurysm re-pair: the Paratrend 7. Anaesthesia And Intensive Care 23: 200-202, 1995.
[50] Patil S, Henry JW, Rubenfire M and Stein PD. Neural network in the clinical diagnosis of acute pulmonary embolism. Chest 104: 1685-1689, 1993.
[51] Perchiazzi G, Indelicato L, D'Onghia N, Coniglio C, Fanelli AM and Giuliani R. Assessing respiratory mechanics of inhomogeneous lungs using artificial neural network: network design. Proceedings of APICE Congress 209-212, 1998.
[52] Perchiazzi G, Indelicato L, D'Onghia N, De Feo E, Fanelli AM and Giuliani R. Assessing respiratory mechanics of inhomogeneous lungs using artificial neural network: preliminary results. Proceed-ings of APICE Congress 213-216, 1998.

48
[53] Poulos M, Rangoussi M, Alexandris N and Evangelou A. On the use of EEG features towards person identification via neural net-works. Med Inform Internet Med 26: 35-48, 2001.
[54] Ranieri VM. Optimization of patient-ventilator interactions: closed-loop technology to turn the century. Intensive Care Med 23: 936-939, 1997.
[55] Ranieri VM, Giuliani R, Fiore T, Dambrosio M and Milic-Emili J. Volume-pressure curve of the respiratory system predicts effects of PEEP in ARDS: "Occlusion" versus "Constant Flow" technique". Am J Respir Crit Care Med 149: 19-27, 1994.
[56] Räsänen J and León M. Detection of lung injury with conventional and neural network-based analysis of continuous data. J Clin Monit14: 433-439, 1998.
[57] Räsänen J and León MA. Neural networks in critical care. In: Ye-arbook of emergency and intensive care medicine, 1995, p. 1010-1019.
[58] Robert C, Karasinski P, Arreto CD and Gaudy JF. Monitoring anesthesia using neural networks: a survey. J Clin Monit Comput 17: 259-267, 2002.
[59] Santa Fe Institute. Working definitions of robustness. Available at: http://discuss.santafe.edu/robustness/stories/storyReader$9. Ac-cessed 22-9-2004
[60] Saxton GA and Myers GH. A servomechanism for automatic regu-lation of pulmonary ventilation. J Appl Physiol 11: 326-328, 1957.
[61] Snowden S, Brownlee KG, Smye SW and Dear PRF. An advisory system for artificial ventilation of the newborn utilizing a neural network. Med Inform 18: 367-376, 1993.
[62] Venkatesh B, Clutton Brock TH and Hendry SP. A multiparame-ter sensor for continuous intra-arterial blood gas monitoring: A pro-spective evaluation. Critical Care Med 22: 588-594, 2002.
[63] Waitman LR, Clarkson KP, Barwise JA and King PH. Represen-tation and classification of breath sounds recorded in an intensive care setting using neural networks. J Clin Monit Comput 16: 95-105, 2000.

49
[64] Westenskow DR. Fundamentals of feedback control: PID, fuzzy logic, and neural networks. Journal of clinical Anesthesia 9: 33S-35S, 1997.
[65] Westenskow DR, Orr AJ, Simon FH, Bender HJ and Franken-berger H. Intelligent alarms reduce anesthesiologist's response time to critical faults. Anesthesiology 77: 1074-1079, 1992.
[66] Wilks PAD and English MJ. A system for rapid identification of respiratory abnormalities using a neural network. Med Eng Phys 17: 551-555, 1995.

Acta Universitatis UpsaliensisComprehensive Summaries of Uppsala Dissertations
from the Faculty of MedicineEditor: The Dean of the Faculty of Medicine
Distribution:Uppsala University Library
Box 510, SE-751 20 Uppsala, Swedenwww.uu.se, [email protected]
ISSN 0282-7476ISBN 91-554-6090-9
A doctoral dissertation from the Faculty of Medicine, Uppsala University,is usually a summary of a number of papers. A few copies of the completedissertation are kept at major Swedish research libraries, while the sum-mary alone is distributed internationally through the series Comprehen-sive Summaries of Uppsala Dissertations from the Faculty of Medicine.(Prior to October, 1985, the series was published under the title “Abstracts ofUppsala Dissertations from the Faculty of Medicine”.)