Artificial Heart Present Future
7
WWW. M ED S CI M ONIT . COM Review Article Signature: Med Sci Monit, 2002; 8(3): RA72-77 PMID: 11887044 RA72 The artificial heart – past, present, and future Karolina M. Zareba University of Rochester, Rochester, NY, U.S.A. Summary Patients with advanced congestive heart failure have a very high 5-year mortality despite med- ical treatment. In such patients, heart transplantation is the treatment of choice. The number of patients awaiting transplantation is several-fold higher than the number of procedures per- formed. Heart transplantation therapy has numerous limitations and is associated with serious complications. The left ventricular assist device is a step towards this goal. It can be attached to the weakened left ventricle to temporarily increase blood flow to the body. The use of left ventricular assist devices helps the failing heart to recover and extends the duration over which a patient’s heart can wait for a replacement donor heart. This therapy is in use for only up to a few months. The total artificial heart, Jarvik-7, first implanted in 1982, did not succeed due to a poor qual- ity of a patient’s life and numerous complications leading to death. Recently, a successful implantation of the AbioCor (Abiomed), the first fully implantable replacement heart, was accomplished. The AbioCor’s internal battery system eliminates the need for the patient to be permanently immobilized through tubes or wires connected to an external power source. Innovative transcutaneous energy transmission permits the recharging of internal batteries. The total artificial heart will require adapting it to different human body sizes as well as fur- ther improving its technical features. The total artificial heart is a remedy of the future com- ing to fruition right now, giving a chance to numerous heart failure patients by extending and improving their lives. key words: artificial heart • left ventricular assist device • transcutaneous energy transmission Full-text PDF: http://www.MedSciMonit.com/pub/vol_8/no_3/2418.pdf File size: 1520 kB Word count: 3292 Tables: – Figures: 4 References: 18 Received: 2002.01.08 Accepted: 2002.02.27 Published: 2002.03.11 Author’s address: Karolina M. Zareba, Pediatric Cardiology, Strong Memorial Hospital, 601 Elmwood Ave. Box 631, Rochester, NY 14642, U.S.A., email: [email protected]
-
Upload
tina-francis -
Category
Documents
-
view
26 -
download
1
description
heart
Transcript of Artificial Heart Present Future

WWW.MEDSCI MONIT.COM
Review ArticleSignature: Med Sci Monit, 2002; 8(3): RA72-77PMID: 11887044
RA72
The artificial heart – past, present, and future
Karolina M. Zareba
University of Rochester, Rochester, NY, U.S.A.
SummaryPatients with advanced congestive heart failure have a very high 5-year mortality despite med-ical treatment. In such patients, heart transplantation is the treatment of choice. The numberof patients awaiting transplantation is several-fold higher than the number of procedures per-formed. Heart transplantation therapy has numerous limitations and is associated with seriouscomplications. The left ventricular assist device is a step towards this goal. It can be attachedto the weakened left ventricle to temporarily increase blood flow to the body. The use of leftventricular assist devices helps the failing heart to recover and extends the duration overwhich a patient’s heart can wait for a replacement donor heart. This therapy is in use for onlyup to a few months.
The total artificial heart, Jarvik-7, first implanted in 1982, did not succeed due to a poor qual-ity of a patient’s life and numerous complications leading to death. Recently, a successfulimplantation of the AbioCor (Abiomed), the first fully implantable replacement heart, wasaccomplished. The AbioCor’s internal battery system eliminates the need for the patient to bepermanently immobilized through tubes or wires connected to an external power source.Innovative transcutaneous energy transmission permits the recharging of internal batteries.The total artificial heart will require adapting it to different human body sizes as well as fur-ther improving its technical features. The total artificial heart is a remedy of the future com-ing to fruition right now, giving a chance to numerous heart failure patients by extending andimproving their lives.
key words: artificial heart • left ventricular assist device • transcutaneous energy transmission
Full-text PDF: http://www.MedSciMonit.com/pub/vol_8/no_3/2418.pdf
File size: 1520 kBWord count: 3292
Tables: –Figures: 4
References: 18
Received: 2002.01.08Accepted: 2002.02.27Published: 2002.03.11
Author’s address: Karolina M. Zareba, Pediatric Cardiology, Strong Memorial Hospital, 601 Elmwood Ave. Box 631, Rochester, NY 14642, U.S.A., email: [email protected]

RA
RA73
Med Sci Monit, 2002; 8(3): RA72-77 Zareba KM – The artificial heart – past, present, and future
BACKGROUND
Coronary artery disease, hypertension and cardiomy-opathies frequently lead to a progressive deteriorationof the heart function and congestive heart failure(CHF). The incidence of heart failure approaches 10per 1000 population after the age of 65 years, meaningthat nearly 5 million Americans have this conditiontoday [1]. Despite great advances in medical and surgi-cal management, the five-year mortality rate of patientswith CHF continues to be about 50 percent. Over700,000 Americans die each year from CHF, making itthe number one cause of death in the US [2]. Recentadvances in pharmacological treatment and devicetreatment (defibrillator, pacemaker with left ventricularresynchronization) substantially improved the survivalof CHF patients. However, those measures are not suffi-cient for many CHF patients requiring a bed-riddenregimen and constant intravenous treatment. In thefinal stages of CHF (NYHA Class IV), heart transplanta-tion is the treatment of choice [3].
HEART TRANSPLANTATION IS NOT A UNIVERSAL SOLUTION
Christiaan Barnard first introduced heart transplanta-tion in the late 1960’s. The results of heart transplantsperformed until the early 1980’s were disappointingdue to a very high rate of rejection [4]. After the intro-duction of cyclosporin as an anti-rejection drug (early1980’s), survival of heart transplantation patientsimproved dramatically. Today only 2000 patients in theUS undergo heart transplantation each year, while thenumber of patients awaiting transplantation is several-fold higher (approximately 50,000–70,000). Hearttransplantation therapy has numerous limitations and isassociated with serious complications. Despite improve-ments in anti-rejection therapy, rejection remains aleading problem when managing heart transplantpatients. In addition, the transplanted heart is very vul-nerable to coronary atherosclerosis, which may compli-cate the course of therapy. In such extreme casespatients may require yet another heart transplant. Anti-rejection therapy also increases the risk of infectionsand inflammations – frequent complications of immuno-suppressive treatment. Therefore, there is a need forartificial devices supporting or replacing the function ofthe damaged heart.
THE CONCEPT OF THE ARTIFICIAL HEART
The concept of an artificial heart was already consid-ered even before heart transplantation. The heart-lungmachine, designed by John Gibbon and first used in1953, demonstrated that an artificial device could tem-porarily mimic the functions of the heart [4]. Earlyexperiments by Dr. Willem Kolff and Dr. Tetsuzo Akut-su in 1958 showed that a dog could be sustained for 90minutes with a polyvinyl chloride mechanical device [4].In 1964 the National Heart, Lung and Blood Instituteset a goal of designing a total artificial heart by 1970. In1969 Dr. Denton A. Cooley performed the first humanimplantation of a total artificial heart when he used adevice developed by Dr. Domingo Liotta to sustain the
life of a 47-year-old patient, who was in cardiac failureafter undergoing resection of a left ventricularaneurysm [4]. The Liotta heart supported him for near-ly three days until a suitable donor heart was availableand successfully transplanted. This case demonstratedthe feasibility of bridging to transplantation with amechanical circulatory support system.
Clinical evaluations of a total artificial heart for perma-nent use began in 1982, when the Jarvik-7 artificialheart, powered by an external console, was placed inDr. Barney Clark at the University of Utah [5]. Fiveimplants were performed through 1985 with the longestsurvivor being supported by the Jarvik-7 for 620 days.Patients on the Jarvik-7 were hemodynamically stable,however they suffered from many complications such ashemorrhage, stroke and sepsis. The most difficult prob-lem to solve was that of the power source. The patientswere tethered to a large console that powered theirhearts, and thus were prevented from leaving the hospi-tal [6]. The technology at the time could not be used inany meaningful numbers to address the needs of thelarge amount of patients dying from heart failure. Oneof the biggest problems with the Jarvik-7 was that it ranon pulses of air that jolted the patient with every beat.As a result, the patient had to be tied to an externalwind machine and had large hoses piercing his chest,making those ideal spots for infection.
The concept of the total artificial heart (TAH) was asso-ciated with several challenges that had to be overcome.First, there was a need for a surface material that wouldallow blood to flow without a high thromboembolic inci-dence such as a special very slick surface, made of acoating compound that would reduces the incidence ofplatelet aggregation and the possibility of stroke [6].Another big challenge was the need of a mechanism forhaving the blood be ejected from one chamber, requir-ing compliance within the chest [7]. Yet another chal-lenge was constructing a device capable of runningwithout failure, a pump that could work perfectly bymimicking the beat of the heart – about 100,000 beats aday (35 million beats a year). However, the most impor-tant problem was the need for an external battery sys-tem that could power the artificial heart without the riskof infection and thus provide a better quality of life. Allof these obstacles, as shown by the complications expe-rienced by the Jarvik-7 patients (sepsis, convulsions, kid-ney failure, respiratory problems, stroke, multi-organsystem failure), diminished further interest in TAHresearch [7]. Thus research was redirected from theTAH to another medical miracle, left ventricular assistdevices, which are able to prolong the life of a naturalheart.
THE LEFT VENTRICULAR ASSIST DEVICE
The left ventricular assist device (LVAD) assists thepumping of the weakened left ventricle to temporarilyincrease blood flow to the body. The LVAD (Fig. 1) con-nects the left ventricle to the ascending aorta, unloadingthe left ventricle. This assist device can perform the roleof the heart, without having to remove the heart. In
RA74
Med Sci Monit, 2002; 8(3): RA72-77Review Article
1994, the Food and Drug Administration (FDA) appro-ved pneumatically driven left ventricular assist devicesas a bridge to transplantation, and self-contained, vent-ed electric devices were approved for this purpose in1998 [4]. Short-term use of these devices in patientsawaiting transplantation improves hemodynamics, end-organ dysfunction and exercise tolerance, and providesa reasonable quality of life [8]. Currently, LVADs areroutinely implanted in patients who are eligible forheart transplantation to improve their suitability fortransplantation and their chances for survival. End-stage congestive heart failure, signs of near circulatorycollapse, generalized debilitation, or end-organ deterio-ration are usual indications for LVAD therapy [8].
Currently used LVAD’s include Novacor and HeartMa-te devices applied as a bridge to transplant and a long-term alternative to drug treatment and heart transplan-tation. There are about 900 patients worldwide whohave received the Novacor LVAS, with several of thembeing supported for more than one year [4]. The devicehas allowed patients to resume daily activities whileawaiting heart transplantation. There are two versionsof the HeartMate Implantable Left Ventricular AssistSystem (LVAS): the Vented Electric device, powered bywearable batteries that allow the patient completemobility and independence, and the Implantable Pneu-matic device, which is powered by an external driveconsole. Both devices are fully implanted alongside thenative heart and are designed to assist the pumpingfunction of the heart’s left ventricle.
The suitability of LVAD’s for their ultimate intendeduse as a long-term myocardial-replacement therapy forpatients who are ineligible for cardiac transplantationhas recently been evaluated by the REMATCH StudyGroup (Randomized Evaluation of Mechanical Assista-nce for the Treatment of Congestive Heart Failure
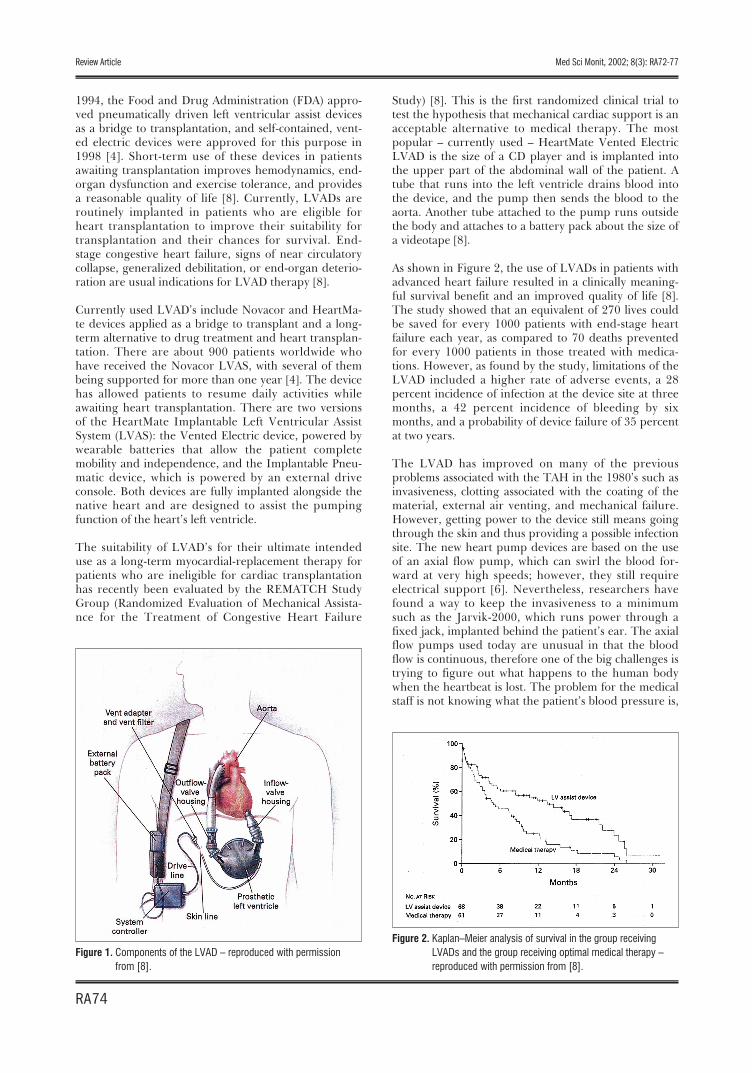
Study) [8]. This is the first randomized clinical trial totest the hypothesis that mechanical cardiac support is anacceptable alternative to medical therapy. The mostpopular – currently used – HeartMate Vented ElectricLVAD is the size of a CD player and is implanted intothe upper part of the abdominal wall of the patient. Atube that runs into the left ventricle drains blood intothe device, and the pump then sends the blood to theaorta. Another tube attached to the pump runs outsidethe body and attaches to a battery pack about the size ofa videotape [8].
As shown in Figure 2, the use of LVADs in patients withadvanced heart failure resulted in a clinically meaning-ful survival benefit and an improved quality of life [8].The study showed that an equivalent of 270 lives couldbe saved for every 1000 patients with end-stage heartfailure each year, as compared to 70 deaths preventedfor every 1000 patients in those treated with medica-tions. However, as found by the study, limitations of theLVAD included a higher rate of adverse events, a 28percent incidence of infection at the device site at threemonths, a 42 percent incidence of bleeding by sixmonths, and a probability of device failure of 35 percentat two years.
The LVAD has improved on many of the previousproblems associated with the TAH in the 1980’s such asinvasiveness, clotting associated with the coating of thematerial, external air venting, and mechanical failure.However, getting power to the device still means goingthrough the skin and thus providing a possible infectionsite. The new heart pump devices are based on the useof an axial flow pump, which can swirl the blood for-ward at very high speeds; however, they still requireelectrical support [6]. Nevertheless, researchers havefound a way to keep the invasiveness to a minimumsuch as the Jarvik-2000, which runs power through afixed jack, implanted behind the patient’s ear. The axialflow pumps used today are unusual in that the bloodflow is continuous, therefore one of the big challenges istrying to figure out what happens to the human bodywhen the heartbeat is lost. The problem for the medicalstaff is not knowing what the patient’s blood pressure is,
Figure 1. Components of the LVAD – reproduced with permissionfrom [8].
Figure 2. Kaplan–Meier analysis of survival in the group receivingLVADs and the group receiving optimal medical therapy –reproduced with permission from [8].
RA75
Med Sci Monit, 2002; 8(3): RA72-77 Zareba KM – The artificial heart – past, present, and future
which is measured by looking at pulsations. Yet anotherimportant problem with non-pulsating devices is theirlack of ability to help clear away cell aggregates.Without this pulsatile action, a clot could eventuallyform, grow, and become dislodged to cause a stroke,heart attack or other medical problem. In addition, thebrain, the kidneys, and the endocardium require pul-satility to remain viable.
THE ABIOCOR IMPLANTABLE REPLACEMENT HEART
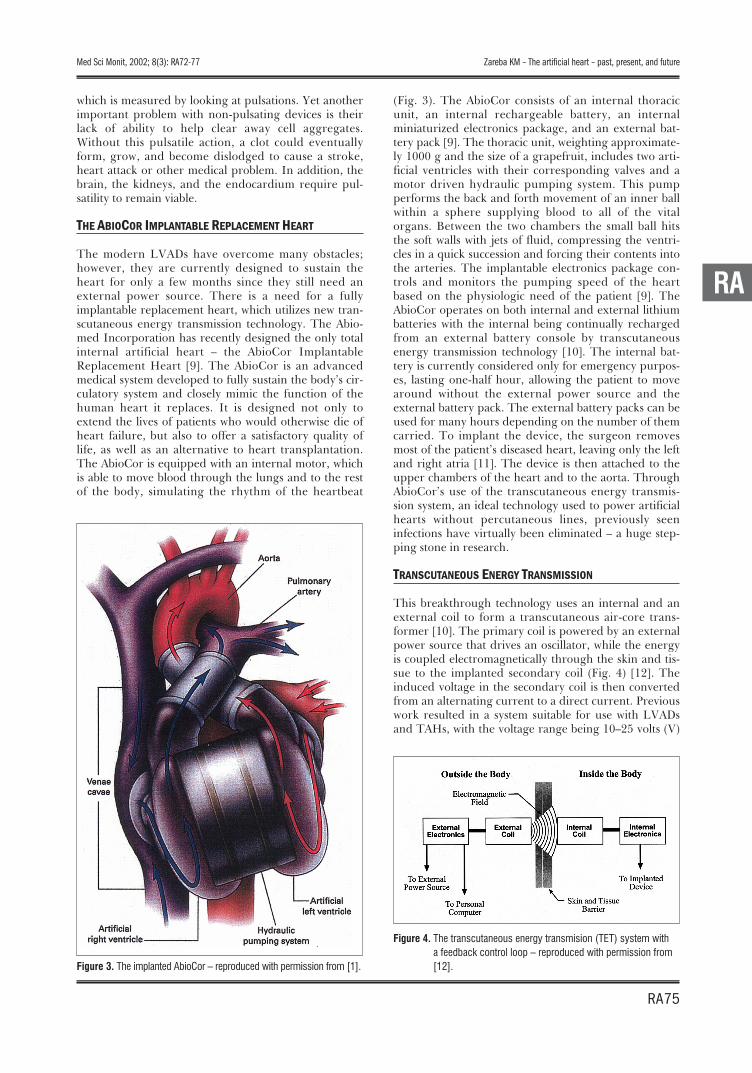
The modern LVADs have overcome many obstacles;however, they are currently designed to sustain theheart for only a few months since they still need anexternal power source. There is a need for a fullyimplantable replacement heart, which utilizes new tran-scutaneous energy transmission technology. The Abio-med Incorporation has recently designed the only totalinternal artificial heart – the AbioCor ImplantableReplacement Heart [9]. The AbioCor is an advancedmedical system developed to fully sustain the body’s cir-culatory system and closely mimic the function of thehuman heart it replaces. It is designed not only toextend the lives of patients who would otherwise die ofheart failure, but also to offer a satisfactory quality oflife, as well as an alternative to heart transplantation.The AbioCor is equipped with an internal motor, whichis able to move blood through the lungs and to the restof the body, simulating the rhythm of the heartbeat
(Fig. 3). The AbioCor consists of an internal thoracicunit, an internal rechargeable battery, an internalminiaturized electronics package, and an external bat-tery pack [9]. The thoracic unit, weighting approximate-ly 1000 g and the size of a grapefruit, includes two arti-ficial ventricles with their corresponding valves and amotor driven hydraulic pumping system. This pumpperforms the back and forth movement of an inner ballwithin a sphere supplying blood to all of the vitalorgans. Between the two chambers the small ball hitsthe soft walls with jets of fluid, compressing the ventri-cles in a quick succession and forcing their contents intothe arteries. The implantable electronics package con-trols and monitors the pumping speed of the heartbased on the physiologic need of the patient [9]. TheAbioCor operates on both internal and external lithiumbatteries with the internal being continually rechargedfrom an external battery console by transcutaneousenergy transmission technology [10]. The internal bat-tery is currently considered only for emergency purpos-es, lasting one-half hour, allowing the patient to movearound without the external power source and theexternal battery pack. The external battery packs can beused for many hours depending on the number of themcarried. To implant the device, the surgeon removesmost of the patient’s diseased heart, leaving only the leftand right atria [11]. The device is then attached to theupper chambers of the heart and to the aorta. ThroughAbioCor’s use of the transcutaneous energy transmis-sion system, an ideal technology used to power artificialhearts without percutaneous lines, previously seeninfections have virtually been eliminated – a huge step-ping stone in research.
TRANSCUTANEOUS ENERGY TRANSMISSION
This breakthrough technology uses an internal and anexternal coil to form a transcutaneous air-core trans-former [10]. The primary coil is powered by an externalpower source that drives an oscillator, while the energyis coupled electromagnetically through the skin and tis-sue to the implanted secondary coil (Fig. 4) [12]. Theinduced voltage in the secondary coil is then convertedfrom an alternating current to a direct current. Previouswork resulted in a system suitable for use with LVADsand TAHs, with the voltage range being 10–25 volts (V)
RA
Figure 3. The implanted AbioCor – reproduced with permission from [1].
Figure 4. The transcutaneous energy transmision (TET) system witha feedback control loop – reproduced with permission from[12].

RA76
Med Sci Monit, 2002; 8(3): RA72-77Review Article
direct current [12]. By not regulating the delivered volt-age, maximum power transfer efficiency was obtained,and the complexity of the design was reduced. Howev-er, current artificial heart designs require a system thathas voltage regulation capabilities to ensure a constantvoltage level to the device. To control the output voltageavailable to the implanted device actively, a transcuta-neous feedback control loop was incorporated into thetranscutaneous energy transmission design. Powertransfer efficiencies were determined to be in the rangeof 68–72% over the tested range of coil separations (3and 10 mm) and output currents from 1.5 to 3.6amperes. By integrating this type of TET system with aTAH, the quality of life for the device recipient is great-ly improved.
ABIOCOR ADDRESSED PREVIOUS PROBLEMS
The AbioCor Implantable Replacement Heart has alsoaddressed the issue of clotting associated with the typeof material and coating used. In the past, ventriclesmade from segmented polyurethane membranes wereknown to undergo biomaterial-associated calcification,however Abiomed has designed a material with a highresistance to calcification [13]. AbioCor is primarilymade of titanium and AngioFlex, Abiomed’s proprietarypolyether-based polyurethane plastic. AngioFlex is adependable non-toxic material as well as safe for contactwith properly flowing blood [9]. The AbioCor’s movingparts, such as valves and ventricular membranes, aremanufactured from AngioFlex, which has proven flexi-ble and durable enough to withstand beating for manyyears (at least 180 million beats – five years). Thedevice’s smooth and seamless construction is engineeredto reduce the likelihood of damage to blood cells, as wellas to reduce the potential for deposition of cells onsmooth surfaces. The AbioCor is also a device that uti-lizes pulsatile flow, helping clear away cell aggregatesthat could form into clots within time.
The FDA has approved the AbioCor as an Investigatio-nal New Device to be tested on selected patients [9]. Thegoals of the initial AbioCor trial are to determinewhether the device can extend life with acceptable quali-ty for patients with less than 30 days to live and noother therapeutic alternative. The inclusion criteria con-centrated on patients with bi-ventricular heart failurewho were greater than 18 years old. They must have ahigh likelihood of dying within the next 30 days as veri-fied by the Shock Index and be unresponsive to maxi-mum existing therapies. These patients are ineligible forheart transplantation and must undergo successfulAbioFit analysis. The exclusion criteria included alonger life expectancy due to a significant potential forheart failure reversibility. Initial authorization from theFDA permitted Abiomed to implant the artificial heartin five patients and expand to 15 if the experience wassatisfactory to the FDA. According to Abiomed, initialsuccess constitutes as six months or more of life addedwith a satisfactory quality of life for a good number oflarge patients. In the future, Abiomed hopes to extend apatient’s life by 5 years and incorporate AbioCor into abroader patient population.
Since July 2, 2001 the AbioCor has successively beenimplanted in five patients. The first patient has had aremarkable recovery, living 151 days. He died of stroke-related complications [14]. Another patient died ofmulti-organ failure, surviving for 56 days. The thirdpatient, surviving 143 days, has recently died from com-plications lingering from a stroke. Thus far, two otherpatients are doing well. With the presence of such posi-tive results, the usage of the artificial heart mightinclude other candidates such as people with diseasesthat destroy the heart (amyloidosis), cancer survivorswho have taken anti-cancer drugs that have injuredtheir hearts and still have a high risk of cancer recur-rence, people with rare tumors of the heart, an thosefor whom heart transplants have failed [15].
At the outset, the AbioCor will cost approximately$75,000, excluding the cost of surgery and follow-up[14]. Skeptics question whether a brief respite from afatal condition justifies the cost; however, the last year oftreatment for patients with heart failure is alwaysexpensive, with hospitalizations costing about $90,000 amonth. It is predicted that the price of the AbioCor willeventually fall to about $25,000. If the device gives peo-ple five years of health and mobility, no one is likely tocomplain since a heart transplant costs at least 10 timesthat amount. Surgical and hospital costs for regularheart transplants are even as high as $500,000.
STILL NOT THE PERFECT HEART
The AbioCor Implantable Replacement Heart has shownremarkable results in the last few months; however forthe future successful implementation of the device on aregular basis a number of things need to be improved.The major problem with AbioCor remains its limitationby patient size; hence, many women and adolescentpatients will likely be precluded from support becauseof their smaller stature. The approximately 1000 gAbioCor heart is currently only able to fit in the chest ofan average male weighing above 90 kg. A smaller ver-sion of the AbioCor would greatly benefit many patientssuch as a child with dilated cardiomyopathy, in whomthe disease may progress so rapidly that they die duringthe waiting period before a suitable donor heart isfound [16]. A system similar in design but with a smallerstroke volume (50cc vs. 70cc) has been tested on a calf[17]. Development of a scaled down TAH expands thistype of circulatory support to those critically ill patientspreviously deemed poor candidates because of theirsmaller body habitus. Another long-term drawback ofthe AbioCor is the thermal impact of the transcutaneousenergy transmission system on the biological tissue, cur-rently resulting in limitations on usable coil geometries.This aspect requires further study. The constant prob-lem with TAHs, which has not yet been fully solved, isthe incidence of clotting leading to stroke. Most of thedeaths associated with patients who have had TAHshave resulted from a thromboembolic event, whicheventually caused stroke [18]. Even though AbioCor hasaddressed this problem tremendously well, furtherinquiry is necessary to fully prevent this from happen-ing.

RA77
Med Sci Monit, 2002; 8(3): RA72-77 Zareba KM – The artificial heart – past, present, and future
In summary, the recent years have brought tremendousprogress in the field of total artificial heart research.Perfecting the design of specific materials and coatingsin order to reduce the incidence of clotting and strokehas lead to many improvements over previous total arti-ficial heart models. The breakthrough transcutaneousenergy transmission technology, which effectively elimi-nates the worry of infection, could spread to many othercardiac assist devices (including implantable pacemakersand defibrillators), increasing their use and simplifyingtheir management. Despite the fact that the fullyimplantable total artificial heart has many aspects toimprove on, it has opened new perspectives for severelyill cardiac patients and the physicians taking care ofthem.
REFERENCES:
1. Jessup M: Mechanical cardiac-support devices – dreams and devil-ish details. New Engl J Med, 2001; 345: 1490-1493
2. SoRelle R: Cardiovascular news. Totally contained AbioCor artifi-cial heart implanted July 3, 2001. Circulation, 2001; 104: E9005-9006
3. SoRelle R: Cardiovascular news. Circulation, 2001; 103: E9015-9016
4. Cooley DA, Frazier OH: The past 50 years of cardiovascularsurgery. Circulation, 2000; 102: IV87-93
5. Debakey ME: The odyssey of the artificial heart. Artif Organs,2000; 24: 405-411
6. Oz M: State-of-the-Art in Artificial Hearts. Interview by Sean Hena-han. Access Excellence, 27 Feb. 2001:http://www.accessexcellence.org/
7. Messmer BJ: From the heart-lung machine to the total artificialheart. International Journal of Artif Organs, 2001; 24: 63-69
8. Rose EA, Gelijns AC, Moskowitz AJ et al: Long-term use of a leftventricular assist device for end-stage heart failure. New Engl JMed, 2001; 345: 1435-1443
9. ABIOMED, Inc: ABIOMED, Inc, 5 Nov. 2001: http://www.abio-med.com/
10. Puers R, Vandevoorde G: Recent progress on transcutaneous ener-gy transfer for total artificial heart systems. Artif Organs, 2001; 25:400-405
11. Dowling RD, Etoch SW, Stevens K et al: Initial experience with theAbioCor implantable replacement heart at the University ofLouisville. ASAIO Journal, 2000; 46: 579-581
12. Mussivand T, Holmes KS, Hum A et al: Transcutaneous energytransfer with voltage regulation for rotary blood pumps. ArtifOrgans, 1996; 20: 621-624
13. Yang M, Zhang Z, Hahn C: Assessing the resistance to calcificationof polyurethane membranes used in the manufacture of ventriclesfor a totally implantable artificial heart. J Biomed Mater Res, 1999;48: 648-659
14. CNN.com: CNN, 24 Nov. 2001: http://www.cnn.com/15. Barth L: Now there are three patients with self-contained artificial
hearts. Health Leader, 2001:http://www.healthleader.uthouston.edu/
16. Stiller B, Dahnert I, Berger F et al: Artificial heart in terminal stageof dilated cardiomyopathy in childhood. Zeitschrift fur Kardiologie,2000; 89: 1039-1045
17. Mehta SM, Weiss WJ, Snyder AJ et al: Testing of a 50 cc stroke vol-ume completely implantable artificial heart: expanding chronicmechanical circulatory support to women, adolescents, and smallstature men. ASAIO Journal, 2000; 46: 779-782
18. Conger JL, Inman RW, Tamez D et al: Infection and thrombosis intotal artificial heart technology: past and future challenges – a his-torical review. ASAIO Journal, 2000; 46: S22-27
RA

Index Copernicus integrates
www.IndexCopernicus.com
Index CopernicusGlobal Scientific Information Systems for Scientists by Scientists
Index Copernicus integrates
IC Virtual Research Groups [VRG]
Web-based complete research environment which enables researchers to work on one project from distant locations. VRG provides:
customizable and individually self-tailored electronic research protocols and data capture tools,
statistical analysis and report creation tools,
profiled information on literature, publications, grants and patents related to the research project,
administration tools.
IC Scientists
Effective search tool for collaborators worldwide. Provides easy global networking for scientists. C.V.'s and dossiers on selected scientists available. Increase your professional visibility.
IC Patents
Provides information on patent registration process, patent offices and other legal issues. Provides links to companies that may want to license or purchase a patent.
IC Lab & Clinical Trial Register
Provides list of on-going laboratory or clinical trials, including research summaries and calls for co-investigators.
IC Grant Awareness
Need grant assistance? Step-by-step information on how to apply for a grant. Provides a list of grant institutions and their requirements.
IC Journal Master List
Scientific literature database, including abstracts, full text, and journal ranking. Instructions for authors available from selected journals.
IC Conferences
Effective search tool for worldwide medical conferences and local meetings.
Index Copernicus integrates
EVALUATION & BENCHMARKING
PROFILED INFORMATION
NETWORKING & COOPERATION
VIRTUAL RESEARCH GROUPS
GRANTS
PATENTS
CLINICAL TRIALS
JOBS
STRATEGIC & FINANCIAL DECISIONS
EVALUATION & BENCHMARKING
PROFILED INFORMATION
NETWORKING & COOPERATION
VIRTUAL RESEARCH GROUPS
GRANTS
PATENTS
CLINICAL TRIALS
JOBS
STRATEGIC & FINANCIAL DECISIONS