
Armed conflict and mental health Magdalena Cerdá, DrPH Assistant Professor Department of...
40
Armed conflict and mental health Magdalena Cerdá, DrPH Assistant Professor Department of Epidemiology April 16, 2014
-
Upload
corey-short -
Category
Documents
-
view
219 -
download
3
Transcript of Armed conflict and mental health Magdalena Cerdá, DrPH Assistant Professor Department of...
Armed conflict and mental health
Magdalena Cerdá, DrPHAssistant Professor
Department of EpidemiologyApril 16, 2014

Intended Audience & Learning Objectives
This lecture will be most informative for someone with an intermediate knowledge of the topic. With this in mind, by the end of this lecture, users will be able to:
• Describe the epidemiology of armed conflict
• Understand the types of mental health problems that arise in armed conflict
• Describe the risk factors for mental illness in a context of armed conflict
• Identify promising prevention strategies to address mental health in armed conflict settings

What is Collective Violence?
“The instrumental use of violence by people who identify themselves as members of a group against another group or set of individuals, in order to achieve political, economic, or social objectives” (WHO, 2002).
•Examples:– Wars/armed conflict– Terrorism– State-perpetrated violence (torture,
disappearances)– Genocide (intent to destroy a particular group)

Our Focus Today
Wars and other forms of civilian armed conflict:• Interstate wars• Civil wars

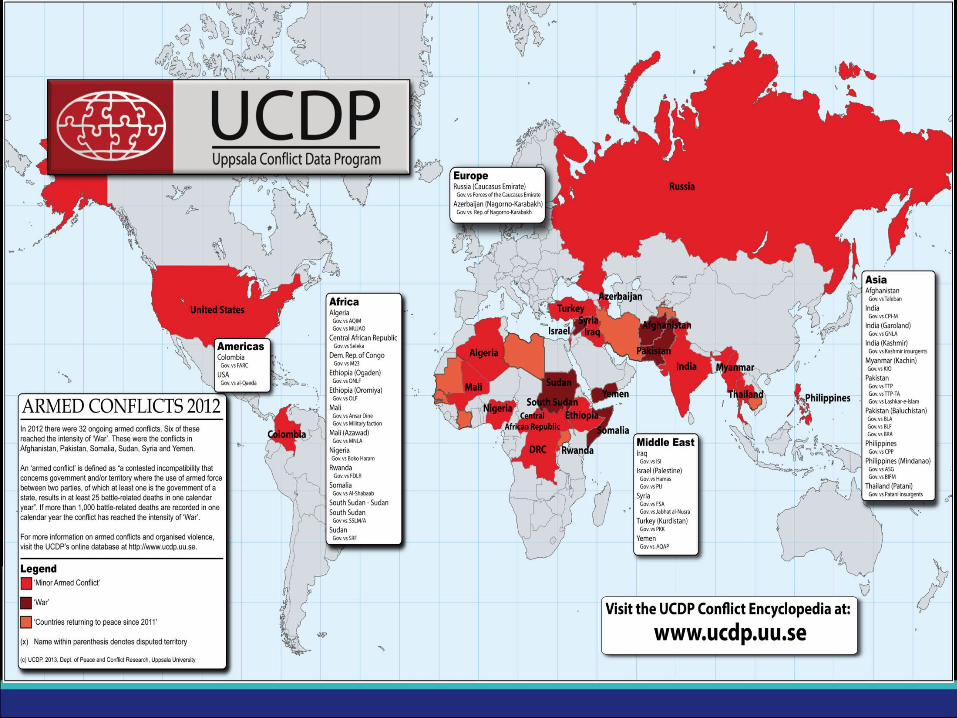
What Types of Armed Conflict Exist Today?
• 32 conflicts were taking place around the world by 2012
• Most conflicts:– Civil conflicts: take place within countries– Concentrated in middle- and low-income
countries– Target local population– Resulting in mass population displacement


Who is Affected?
• Armed combatants fighting in the conflict–Members of state military organizations– Civilian combatants:• Paramilitaries• Guerrillas• Child soldiers
• Civilian populations exposed to the conflict
What Types of Mental Illness Have Been Studied in Relation
to Conflict?• A focus on common psychiatric disorders
• Bulk of studies focus on posttraumatic stress disorder (PTSD)
• Other disorders considered include:– Depression– Substance use disorders, in particular alcohol
abuse and dependence

How Prevalent is Mental Illness among Armed Combatants?
• Prevalence of psychiatric disorders in military populations– PTSD: 12% to 20%: – Depression: 3%-15%
• Prevalence of psychiatric disorders among child soldiers:– PTSD: 16%-34.9% – Depression: 55%-88.2%
• No systematic data on the prevalence of psychiatric disorders among civilian combatants

How Prevalent is Mental Illness among Civilians Following
Conflict?• Wide variability in rates of mental disorders• Meta-analysis of 161 articles published on 40
countries in 1980-2009 (Steel, 2009) found:– Prevalence of posttraumatic stress disorder (PTSD):
0-99%– Prevalence of depression: 3-85.5%– Weighted prevalence:
• PTSD: 30.6% (26.3%-35.2%)• Depression: 30.8% (26.3%-35.6%)
• Substance Use (Kerridge et al., 2013)– 1% + deaths from collective violence 0.14%
more disability-adjusted life years lost due to substance use disorders
Methodological Issues that Affect Studies of Collective
Violence• Larger prevalence estimates are found in
studies characterized by:– Sample size: smaller samples– Sampling design: convenience sampling– Measurement: self-report (rather than clinical
interview) measures of disorders
• Need to draw random samples of a population to obtain valid estimates of prevalence
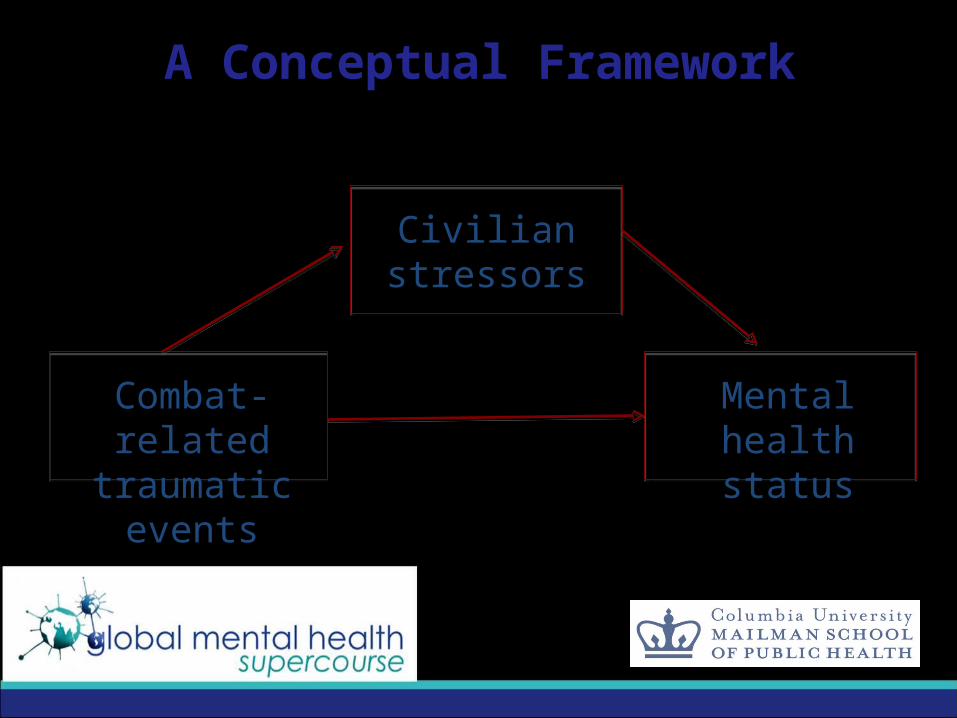
A Conceptual Framework
Combat-related traumatic events
Civilian stressors
Mental healthstatus

Determinants of Postdeployment Mental Illness
among Combatants• Combat-related traumatic events: being
under fire, attacked by civilians/insurgents, engaging in battle, injury in battle, killing others in battle
• Post-battle traumatic events: seeing soldiers wounded/dead, seeing wounded/dead civilians
• Civilian stressors: divorce or break-up, losing job, stressful legal problems, lack of adequate health care, financial problems

Combat-Related and Post-Battle Traumatic Events
• Consistent relationship between exposure to traumatic events during & after combat and common psychiatric disorders: PTSD, depression, alcohol dependence
• Bulk of research focused on PTSD; most studies of U.S. and United Kingdom military forces
• Studies usually measure a count of exposure to different types of traumatic combat-related and post-battle events
• Virtually no studies on effects on paramilitary or guerrilla forces– A few studies conducted on former child soldiers
Example of a Study(click title of article to link to article online--in Slide Show
mode only)

Example of a Study
Objective: To describe the relationship between combat exposures and post-traumatic stress disorder symptoms in a large population-based military cohort
Sample: 50,184 US service members recruited for the Millennium cohort before wars in Iraq and Afghanistan
Results: •US service members who were deployed and reported combat experiences—at greater odds for PTSD than those deployed who did not report combat experiences and those not deployed•7.6-8.7% of deployers reporting combat exposures reported PTSD symptoms, while 1.4-2.1% of deployers without reported combat exposures and 2.3-3.0% of non-deployers reported PTSD symptoms
Civilian Stressors Experienced by Combatants
Civilian stressors following deployment linked to an increase in PTSD, depression & substance use disorders•Particularly affected in the US and UK: members of reserve forces who return home without the support of a military unit and must enter civilian employment
•Factors that increase difficulties upon return from deployment include: problems at home regarding children, financial distress, job loss, and lack of employer support
•Little systematic research on the role that civilian stressors play in mental illness among paramilitary or guerrilla members who return home from combat

Example of a Study(click title of article to link to article online--in Slide Show
mode only)
Example of a StudyObjectives: To determine if financial hardship, job loss, employer support & effect of deployment absence on co-workers are associated with PTSD & depression among reserve soldiers
Methods: Cross-sectional study of a sample of US 4034 National Guard soldiers
Results: Job loss & financial difficulties linked to PTSD & depression•PTSD rates of those who lost jobs or reported financial difficulties at least twice as high compared with rates of those who had not •Depression rates almost three times as high among those who lost jobs or experienced financial difficulties

Example of a Study(click title of article to link to article online--in Slide Show
mode only)

Example of a StudyObjectives: Determine risk and the protective factors related to PTSD among former child soldiers (average age 16.6) in Sierra LeoneMethods: Longitudinal Study of War Affected Youth in Sierra Leone (n= 529) identified by the International Rescue Committee; assessed war experiences, PTSD, stigma, family acceptance, family abuse and neglect Results:
– 36% endorsed having injured or killed someone– 32% met the criteria for PTSD – War experiences and post-conflict family abuse were
significantly associated with increased PTSD– Death of a parent due to the war was significantly
associated with increased PTSD

Determinants of Post-Conflict Mental Health among Civilians
• Exposure to combat-related traumatic events as civilians– Injury, death or disappearance of loved ones,
seeing dead/injured bodies, torture, physical assault, sexual assault
• Experience of civilian stressors associated with conflict– Displacement, loss of housing, loss of job,
financial problems, poverty, divorce, malnutrition, loss of social network
Combat-Related Traumatic Events
Experienced by Civilians• Civilian experiences of torture and cumulative
exposure to traumatic events are consistently associated with civilian rates of depression and PTSD– Steel et al., 2009: strongest determinants of depression and
PTSD across 161 studies
• Consistent dose-response relationship between number of traumatic events and level of psychiatric symptoms
• Civilian responses to combat may differ from soldier responses: – Can shatter civilian assumptions about safety– Civilians experience higher frequency of intrusive recollections
and less emotional numbing
Example of a Study(click title of article to link to article online--in Slide Show
mode only)

Example of a Study

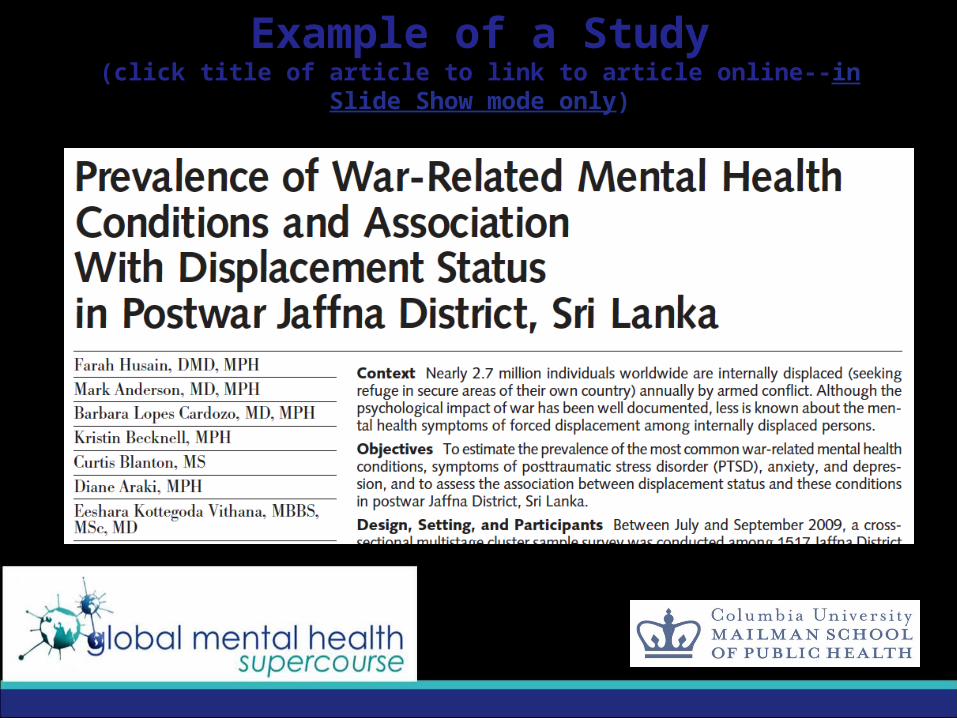
Example of a StudyObjective: Determine association of displacement due to war with symptoms of PTSD, anxiety, and depression in postwar Jaffna District, Sri Lanka
Methods: In 2009, 1409 residents of Jaffna were surveyed on displacement status and PTSD, anxiety and depression
Results: •Participants who were displaced at the time of the survey were more likely to report PTSD symptoms and depression compared to those individuals who had been long term residents of the displacement camps. •Displacement was no longer associated with mental health conditions after controlling for trauma exposure.

Civilian Stressors Associated with Conflict
• Armed conflict leads to the destruction of the physical and material infrastructure & social fabric of communities
• Given high prevalence of civilian conflicts & absence of a State in many civilian conflicts, civilian stressors are a particularly important driver of post-conflict mental health
(over)
Civilian Stressors Associated with Conflict
• Civilian stressors following conflict have shown strong & significant associations with common psychiatric disorders, in particular PTSD
• A number of studies have shown a stronger effect of civilian stressors compared to combat-related traumatic events on mental illness
Example of a Study(click title of article to link to article online--in Slide Show
mode only)
Example of a StudyObjectives: What was the impact of war-related stressful life events on health of families living during war conditions in Lebanon? Methods: 540 families from Beirut were surveyed on indicators of somatization, depression, other psychological symptoms, interpersonal relations, and marital relations, war-related events, economic hardship, reduction in social network, social class, social support, and migration. Results:
• Reduction in social networks associated with increased depression among parents • Reduction in food safety associated with increased other psychological symptoms for the mother and adolescents • Migrating associated with reduced depression and other
psychological symptoms among mothers• Availability of social support was associated with reduced depression
and other psychological symptoms among fathers

How do We Address Mental Health after Conflict?
• Prevention
• Treatment

Prevention Four guidelines outlined by Miller and Rasmussen:
• A rapid and contextually grounded assessment of stressors that are salient is needed before developing interventions; Possible methods include: focus groups, free-listing, key informant interviews
• First address the combat-related civilian stressors before providing clinical services that target mental health
• When clinical services are indicated, services should target a broad range of mental health conditions and not only PTSD
• It is also imperative to take into account that the symptomology seen may not be solely due to conflict exposure; there may be other sources of psychological trauma

TreatmentA systematic review of 29 Randomized Control Trials and Clinical Controlled Trials (Tol, 2011) assessed various domains of treatment: •Specialized services
- Narrative exposure therapy showed beneficial effects on PTSD among Romanian, Ugandan, Sri Lankan and Rwandan cohorts
•Focused non-special supports - Studies assessing treatment methods such as: classroom-
based skills, psychoeducation, group-based trauma and grief-focused, testimony therapy found mixed results
•Strengthening community and family support- Studies examining the impact of increased family support
and community strength found improvements on psychological symptoms
Treatment
Specialized service• In a study among torture survivors in Romania,
PTSD and depression improved in those survivors who had narrative exposure therapy. On average, after treatment, PTSD symptoms reduced 50% and depression symptoms by 67% (Bichescu, 2007).

Treatment Specialized service
• Among Sudanese refugees in Uganda, narrative exposure therapy was more effective in reducing PTSD compared to supportive counseling and psychoeducation. One year after treatment, only 29% of the narrative exposure therapy participants compared to 79% of the supportive
counseling group and 80% of the psycho- educational group had PTSD (Nuener, 2004).

Treatment Focused non-special supports • In Bosnia and Herzegovina, war-affected 13–
18-year-olds underwent classroom-based skills and psychoeducation intervention aimed at trauma and loss and the related stress and grief and a group-based trauma-focused and grief-focused treatment.
• Both treatments improved depression and PTSD. The group-based treatment group, showed the greatest improvement. At the 4-month follow-up, there was on average there was a 81% reduction in PTSD symptoms and a 61% reduction in depressive symptoms (Layne, 2008).

Treatment Strengthening community and family support
• A randomized-clinical trial in northern Uganda of a school-based intervention (structured activities including drama, movement, music, and art), resulted in improvements in overall wellbeing among those children aged 7-12 year olds who received the intervention (Ager, 2011)
• A study among 250 children from the West Bank and 150 children from Gaza, found that children among the treatment group (structured events including: cultural and recreational activities traditional dancing, art work, sports, drama and puppetry) had lower total problem scores, externalizing problem scores, and internalizing problem scores (Loughry, 2006)

Conclusions• Traumatic events directly related to conflict,
and civilian stressors that follow conflict, shape post-conflict mental health among combatants and civilians
• To address mental health consequences of combat, need to:– Address the stressors combatants face upon return
from deployment– Rebuild infrastructure that was destroyed by conflict– Provide access to treatment to combatants and
civilians particularly vulnerable to the consequences of armed conflict

Acknowledgements
Spruha Joshi, MPH, for assistance in reviewing and synthesizing the literature for this presentation.














![DORMITORIOS/ - Angel Cerdá · DORMITORIOS by Angel Cerdá 18/ 01 50 04 51 16 52 03 02 54 07 40 15 55 14 53 67 Telas / Fabrics [Duo collection] LA CALIDEZ DEL TEXTIL Los tonos neutros](https://static.fdocuments.in/doc/165x107/5fa0374764032261cc0cb682/dormitorios-angel-cerd-dormitorios-by-angel-cerd-18-01-50-04-51-16-52-03.jpg)