Are Combined CT Scans of the Thorax Being Overused?
3
Are Combined CT Scans of the Thorax Being Overused? David C. Levin, MD a,b , Laurence Parker, PhD a , Ethan J. Halpern, MD a , Vijay M. Rao, MD a Purpose: A news article in June 2011 reported that Medicare claims showed considerable overuse of “double” CT scans of the thorax (ie, combined scans without contrast followed by with contrast) at a number of hospitals. Most radiologists agree that they should be done only on rare occasions. The aim of this study was to determine what proportion of all thoracic CT scans are combined scans in the Medicare population. Methods: The data sources were the Medicare Part B Physician/Supplier Procedure Summary Master Files for 2001 to 2011. The 3 Current Procedural Terminology codes for thoracic CT (with contrast, without contrast, and without plus with contrast) were selected. Utilization rates per 1,000 beneficiaries and the percentage that were combined scans were calculated. Results: The utilization rate of combined scans increased from 2001 through 2006, remained steady in 2007, but then decreased sharply thereafter. The compound annual rate of change from 2007 to 2011 was 10.4%. From 2001 through 2006, combined thoracic CT scans constituted 6.0% to 6.1% of all thoracic CT scans. However, from 2006 to 2011, this percentage progressively declined, reaching a low of 4.2% in 2011. Conclusions: Despite the 2011 news report, only a very small percentage of thoracic CT scans nationwide are done both without and with contrast. Moreover, that percentage dropped by almost one-third from 2006 to 2011, suggesting that the practice is declining. The figure of 4.2% can be used as a benchmark against which to judge radiology facilities in the future. Key Words: Medical economics, thoracic CT, CT with contrast, utilization of imaging, radiology and radiologists, socioeconomic issues J Am Coll Radiol 2014;-:---. Copyright © 2014 American College of Radiology INTRODUCTION Thoracic CT is a widely performed imaging examina- tion. It can be performed in 3 ways: without contrast, with contrast, and without contrast followed by with contrast (hereafter referred to as a combined scan). Most radiologists would agree that combined CT scans of the thorax should be performed only infrequently [1,2]. Those infrequent indications might include suspected aortic dissection and some cases of indeterminate pul- monary nodules [3]. However, most cases can be properly evaluated using single-phase scans (ie, either with contrast or without contrast). As will be discussed later, concern has at times been raised that combined thoracic CT scans are overused. If this happens, costs are increased because combined scans are reimbursed at a higher rate than either of the two single-phase scans. Moreover, it leads to increased radi- ation exposure to patients. Our purpose in this study was to use a large national database to determine how widespread the use of these scans is and to also ascertain whether it has increased or decreased in recent years. METHODS The data source was the CMS Part B Physician/Supplier Procedure Summary Master Files for 2001 through 2011. These files cover all beneficiaries in traditional fee-for-service Medicare (36.3 million in 2011) but not those in Medicare Advantage plans (12.6 million in 2011). For each Current Procedural Terminology, version 4, code, the files provide data on examination volume and other administrative information. We selected the 3 codes for CT of the thorax: (1) 71250 (CT thorax without contrast), (2) 71260 (CT thorax with contrast), and (3) 71270 (CT thorax without, followed by with contrast). Total thoracic CT volume in the Medicare fee-for-service population was tabulated each year, as was the volume of the combined examination a Center for Research on Utilization of Imaging Services, Department of Radiology, Thomas Jefferson University Hospital and Jefferson Medical College, Philadelphia, Pennsylvania. b HealthHelp, Inc, Houston, Texas. Corresponding author and reprints: David C. Levin, MD, Thomas Jefferson University Hospital, Department of Radiology, Main 1090, Philadelphia, PA 19107; e-mail: [email protected]. ª 2014 American College of Radiology 1 1546-1440/14/$36.00 http://dx.doi.org/10.1016/j.jacr.2013.12.010
Transcript of Are Combined CT Scans of the Thorax Being Overused?

aCenter for ReRadiology, ThoCollege, PhiladebHealthHelp, In
CorrespondinJefferson UnivePhiladelphia, PA
ª 2014 America
1546-1440/14/$
Are Combined CT Scans of the ThoraxBeing Overused?
David C. Levin, MDa,b, Laurence Parker, PhDa, Ethan J. Halpern, MDa,
Vijay M. Rao, MDa
Purpose: A news article in June 2011 reported that Medicare claims showed considerable overuse of“double” CT scans of the thorax (ie, combined scans without contrast followed by with contrast) at a numberof hospitals. Most radiologists agree that they should be done only on rare occasions. The aim of this studywas to determine what proportion of all thoracic CT scans are combined scans in the Medicare population.
Methods: The data sources were the Medicare Part B Physician/Supplier Procedure Summary Master Filesfor 2001 to 2011. The 3 Current Procedural Terminology codes for thoracic CT (with contrast, withoutcontrast, and without plus with contrast) were selected. Utilization rates per 1,000 beneficiaries and thepercentage that were combined scans were calculated.
Results: The utilization rate of combined scans increased from 2001 through 2006, remained steady in2007, but then decreased sharply thereafter. The compound annual rate of change from 2007 to 2011 was�10.4%. From 2001 through 2006, combined thoracic CT scans constituted 6.0% to 6.1% of all thoracicCT scans. However, from 2006 to 2011, this percentage progressively declined, reaching a low of 4.2%in 2011.
Conclusions: Despite the 2011 news report, only a very small percentage of thoracic CT scans nationwideare done both without and with contrast. Moreover, that percentage dropped by almost one-third from 2006to 2011, suggesting that the practice is declining. The figure of 4.2% can be used as a benchmark againstwhich to judge radiology facilities in the future.
Key Words: Medical economics, thoracic CT, CT with contrast, utilization of imaging, radiology andradiologists, socioeconomic issues
J Am Coll Radiol 2014;-:---. Copyright © 2014 American College of Radiology
INTRODUCTIONThoracic CT is a widely performed imaging examina-tion. It can be performed in 3 ways: without contrast,with contrast, and without contrast followed by withcontrast (hereafter referred to as a combined scan). Mostradiologists would agree that combined CT scans of thethorax should be performed only infrequently [1,2].Those infrequent indications might include suspectedaortic dissection and some cases of indeterminate pul-monary nodules [3]. However, most cases can beproperly evaluated using single-phase scans (ie, eitherwith contrast or without contrast).As will be discussed later, concern has at times been
raised that combined thoracic CT scans are overused. Ifthis happens, costs are increased because combined scans
search on Utilization of Imaging Services, Department ofmas Jefferson University Hospital and Jefferson Medicallphia, Pennsylvania.
c, Houston, Texas.
g author and reprints: David C. Levin, MD, Thomasrsity Hospital, Department of Radiology, Main 1090,19107; e-mail: [email protected].
n College of Radiology
36.00 � http://dx.doi.org/10.1016/j.jacr.2013.12.010
are reimbursed at a higher rate than either of the twosingle-phase scans. Moreover, it leads to increased radi-ation exposure to patients. Our purpose in this studywas to use a large national database to determine howwidespread the use of these scans is and to also ascertainwhether it has increased or decreased in recent years.
METHODSThe data source was the CMS Part B Physician/SupplierProcedure Summary Master Files for 2001 through2011. These files cover all beneficiaries in traditionalfee-for-service Medicare (36.3 million in 2011) but notthose in Medicare Advantage plans (12.6 million in2011). For each Current Procedural Terminology,version 4, code, the files provide data on examinationvolume and other administrative information. Weselected the 3 codes for CT of the thorax: (1) 71250(CT thorax without contrast), (2) 71260 (CT thorax withcontrast), and (3) 71270 (CT thorax without, followedby with contrast). Total thoracic CT volume in theMedicare fee-for-service population was tabulated eachyear, as was the volume of the combined examination
1

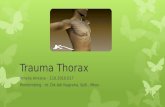
Fig 2. Utilization rate per 1,000 Medicare fee-for-servicebeneficiaries of combined CT scans of the thorax (ie, per-formed without contrast followed by with contrast). Thevertical axis shows studies per 1,000 and includes scansdone in all places of service.
2 Journal of the American College of Radiology/Vol. - No. - Month 2014
(code 71270). To ascertain examination volume, wecounted only global and professional component claims.Technical component claims were not included becausethat would have led to double counting. The numberof fee-for-service Medicare beneficiaries each yearwas determined from the CMS Medicare AdvantageState/County Penetration Reports. We then calculatedutilization rates per 1,000 fee-for-service beneficiaries.Data analysis was carried out using SAS version 9.3 forWindows (SAS Institute Inc, Cary, North Carolina).
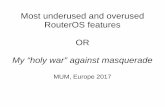
RESULTSThe trend in total thoracic CT use in the Medicare fee-for-service population (all 3 codes together) is shown inFigure 1. From 2001 to 2007, there was a rapid pro-gressive increase in utilization rate per 1,000 benefi-ciaries. The rate per 1,000 that year peaked at 99.6.There were small declines each year thereafter through2011, by which time the rate had decreased to 91.3.These changes were not influenced by the introductionof any new codes; the code for CT angiography of thethorax (71275) had been introduced in 2001 and wastherefore in existence for the entire period of the study(that code was not included in this analysis).Figure 2 shows the utilization rate of combined CT
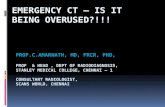
scans only (code 71270). Use of combined scans roserapidly from 3.6 per 1,000 in 2001 to a peak of 5.9 in2006 and 2007. This represented a compound annualgrowth rate for 2001 to 2006 of 10.4%. However, from2007 through 2011, a steady and substantial declineoccurred, dropping to a utilization rate in the latter yearof 3.8 per 1,000. This amounted to a compound annualrate of change for 2007 to 2011 of �10.4%.Figure 3 shows combined CT scans of the thorax as a
percentage of all thoracic CT scans (all 3 codes together)
Fig 1. Total utilization rate per 1,000 Medicare fee-for-service beneficiaries of all diagnostic CT scans of thethorax (without contrast, with contrast, and without followedby with contrast). The vertical axis shows studies per 1,000and includes scans done in all places of service.
each year. From 2001 through 2006, it held fairlyconstant at either 6.0% or 6.1%. But it then declinedsteadily thereafter to 4.2% in 2011.
DISCUSSIONConcern about the overuse of combined thoracic CTscans has been expressed by the federal Hospital Comparewebsite. This site is run by CMS in conjunction with itsHospital Outpatient Quality Reporting program, whichhas identified numerous measures it considers indicatorsof quality in the care of outpatients with a variety ofclinical conditions. It tracks these measures for all acutecare hospitals in the country, using claims data submittedby the hospitals. Among the measures are 6 that are
Fig 3. Percentage of all thoracic CT scans that were com-bined scans (ie, performed without followed by withcontrast) in the Medicare fee-for-service population.

Levin et al/Combined CT Scans of the Thorax 3
termed “outpatient imaging efficiency”measures and thatare felt to be misused or overused. One of the 6 iscombined CT of the thorax. The descriptor of thismeasure states that if the percentage is high, it may meanthat too many patients are receiving combination or“double” scans when single-phase scans would suffice andthat lower percentages are better.Concern about overuse of these scans was also high-
lighted in a front-page article in the New York Times onJune 17, 2011 [4]. The article reported that in 2008,many thousands of Medicare patients received com-bined thoracic CT scans, that >200 hospitals in thecountry administered combined scans in >30% of thecases, and that the cost to Medicare of these scans was>$25 million in that 1 year. The article did not casthospital imaging facilities in a very favorable light. Theobvious implication was, why did the responsible peopleallow this to happen?Our data indicate that, contrary to the aforemen-
tioned concerns, the use of combined CT scans of thethorax in the Medicare population is actually quite low.Moreover, it seems to have decreased even further inrecent years. Radiology groups practicing in hospitalscan check on their own percentages of use of combinedthoracic CT by accessing the Hospital Compare website.We have found this site somewhat difficult to use, andgetting to this specific information for an individualhospital is a convoluted process. One way to do it is asfollows: (1) Google “Hospital Compare website.” (2)Select the first item that appears, “Medicare HospitalCompare Quality of Care-Medicare.gov.” (3) On thenext page, type in the name and ZIP code of yourhospital and click “Search.” (4) On the next page, thename of your hospital should appear. Click on it. (5) Onthe next page, select the tab for “Use of medical imag-ing.” This will bring you to the list of the 6 outpatientimaging efficiency measures, and you can see how yourhospital performs on each of them. It also shows, foreach measure, the state and national averages. Accordingto the website at the time of this writing (December2013), the national average use of combined thoracicCT was 3.7%, and use at our institution was 1.9%. Thedifference between the Hospital Compare nationalaverage of 3.7% and our finding of 4.2% could beexplained by two possible factors. First, the 4.2% figureis from 2011, and the current 3.7% figure could indicatea further decline in use since then. Second, the HospitalCompare figure pertains only to hospital outpatients,whereas the Times article [4] and our study included allpatients.The substantial decrease in the use of combined
thoracic CT scans is obviously a favorable development,for which there are several likely explanations. Radiol-ogists seemed to have learned through experience and/or
education that only single-phase scans are needed inthe large majority of cases. Referring physicians mayhave become more cognizant of appropriateness criteria.Payers and radiology benefits managers have probablyexercised more stringent oversight. Finally, the existenceof the Hospital Compare website may have created peerpressure to reduce the use of combined scans.
CONCLUSIONSAlthough the New York Times article [4] identified aproblem that existed in certain hospitals, it is not thenorm. Throughout the country as a whole, the use ofcombined CT of the thorax is quite low, and it appearsto be trending even lower. The vast majority of thoracicCT examinations are performed by radiologists [5], andthey have clearly become aware of appropriateness issuesand acted responsibly. The 2011 figure of 4.2% can beused as a benchmark to which practices can comparethemselves.
TAKE-HOME POINTS
� An article in the New York Times in 2011 indicatedthat “double” or combined CT scans of the thoraxwere being performed too often at many hospitals,thereby increasing radiation burden and costs.
� Nationwide Medicare data from 2001 to 2011 showthat from 2001 through 2006, combined thoracic CTaccounted for only 6.0% to 6.1% of all thoracic CTand that the percentage thereafter declined steadily to4.2% in 2011.
� Thus, it does not seem that combined CT of thethorax is being overused in the population at large.
� Radiologists can access the CMS Hospital Comparewebsite to determine the frequency of use of theseexaminations on outpatients at their own hospitals.
REFERENCES
1. Agency for Healthcare Research and Quality. NQF-endorsed measure.Imaging efficiency: ratio of thorax CT studies that are performed with andwithout contrast out of all thorax CT studies performed. Available at:http://www.qualitymeasures.ahrq.gov/content.aspx?id¼34199. AccessedNovember 12, 2013.
2. Appleby J, Rau J. “Double” chest scans increase costs and exposure toradiation. Kaiser Health News. June 18, 2011. Available at: http://www.kaiserhealthnews.org/Stories/2011/June/19/double-ct-chest-scans.aspx?p¼1.Accessed November 12, 2013.
3. Swensen SJ, Viggiano RW, Midthun DE, et al. Lung nodule enhancementat CT: multicenter study. Radiology 2000;214:73-80.
4. Bogdanich W, McGinty JC. Medicare claims show overuse for CTscanning. The New York Times. July 17, 2011. Available at: http://www.nytimes.com/2011/06/18/health/18radiation.html?pagewanted¼all&_r¼0.Accessed June 19, 2011.
5. Levin DC, Rao VM, Parker L, Frangos AJ, Sunshine JH. Recent trendsin utilization rates of noncardiac thoracic imaging: an example of howimaging growth might be controlled. J Am Coll Radiol 2007;4:886-9.