Anterior Abdominal Wall
55
1
-
Upload
thomas-jane -
Category
Documents
-
view
62 -
download
0
description
Concise presentation on Anterior Abdominal Wall for medical students.
Transcript of Anterior Abdominal Wall
1

Define surface landmarks, 4 Quadrants, 9 Regions
Layers of Abdominal Wall, attention to superficial fascia and muscles
Function and neurovasculature of abdominal wall
Rectus sheath, arcuate line, conjoint tendon Clinical stuff– Sites of surgical incisions,
McBurney’s point, appendicitis, Hematoma of Rectus Sheath, Liposuction & Hernias
2

Largest cavity in body
Location- between diaphragm and pelvic inlet (superior pelvic aperture)
Continuous with pelvic cavity
Lined with parietal peritoneum (serous membrane)
3
Pelvic inlet

Superior Diaphragm
• Concave dome • Spleen, liver, part of
stomach & kidneys lies under dome• Protected by lower ribs and
costal cartilages Inferior
Lies in greater pelvis • Between ala or wings of
ilia • Ileum, cecum and sigmoid
colon partly protected Anterior & lateral
wallsMuscles
Posterior wallVertebral column, lower
ribs & associated muscles4

5
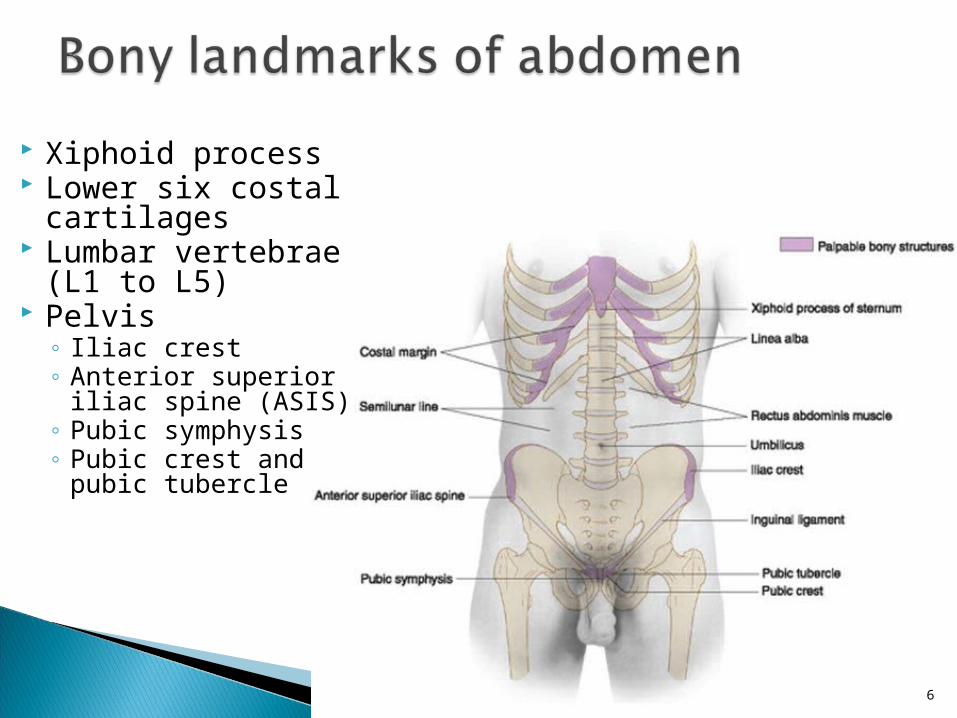
Xiphoid process Lower six costal
cartilages Lumbar vertebrae
(L1 to L5) Pelvis
◦ Iliac crest ◦ Anterior superior
iliac spine (ASIS) ◦ Pubic symphysis ◦ Pubic crest and
pubic tubercle
6

Costal margin
7
Xiphoid process
7
Linea alba
Linea alba •A fibrous raphe where aponeuroses of external oblique, internal oblique and transversus abdominis on either side unite•Slight indentation from xiphoid process to pubic symphysis
Linea alba •A fibrous raphe where aponeuroses of external oblique, internal oblique and transversus abdominis on either side unite•Slight indentation from xiphoid process to pubic symphysis

Inguinal ligament
Pubic tubercle
Ant. Sup. Iliac spine
8

Four quadrants ◦ Right upper ◦ Left upper ◦ Right lower ◦ Left lower
Planes-◦ Median plane
From xiphoid process to pubic symphysis
◦ Transumbilical plane Horizontal line at level of
umbilicus
9

Passes through lower border of 10th cc
Transpyloric plane- Sometimes used instead of subcostal
Interspinous plane-Passes through easily palpated ASIS on each side
Transpyloric plane- Sometimes used instead of subcostal
Interspinous plane-Passes through easily palpated ASIS on each side
Transtubercular or Intertubercular plane- passes through tubercles of iliac crests and body of L5
Midpoint of clavicle to midinguinal point
10
Nine regions ◦ For more accurate,
descriptive & diagnostic purposes

11
4 quadrants & 9 regions are essential in clinical practice ◦ Each area represents
certain visceral structures
◦ Allow correlation of pain & referred pain from these areas to specific organs
◦ Palpated, percussed & auscultated during clinical examination

Midway between superior borders of manubrium & pubic symphysis (typically L1 vertebral level)
Transects pylorus when patient is recumbent (supine or prone)
Passes through tip of 9th cc
Structures located at this plane◦ Gall-Bladder (fundus)◦ Origin of SMA◦ Pylorus of Stomach◦ Duodenojejunal junction◦ Pancreas (neck)◦ Kidneys (hilum)
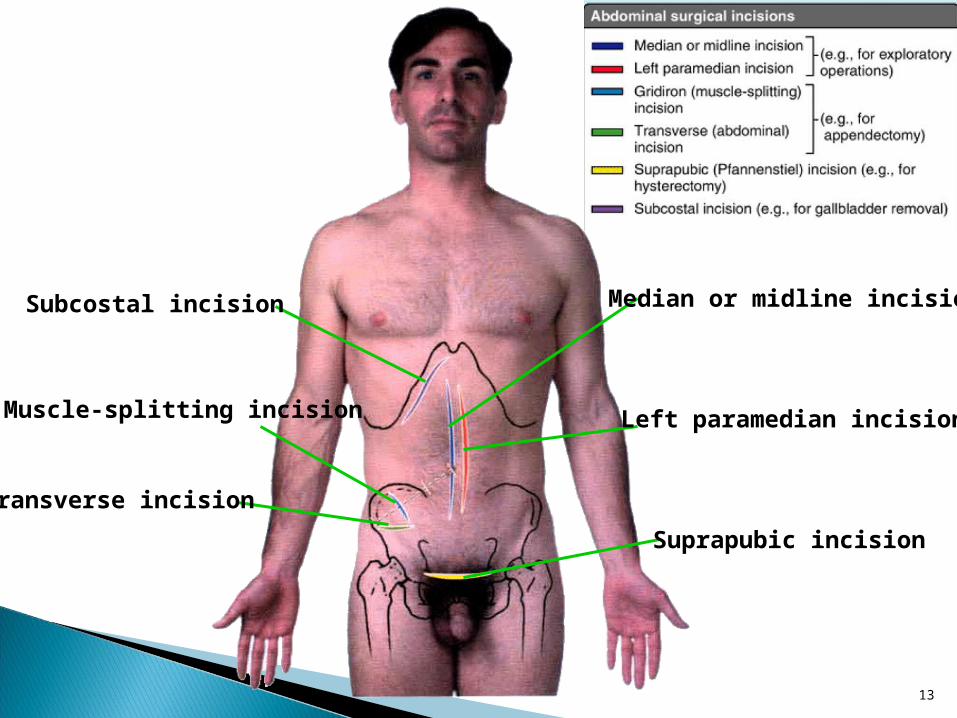
13
Subcostal incision
Muscle-splitting incision
Transverse incision
Median or midline incision
Left paramedian incision
Suprapubic incision

McBurney's point
A surface landmark that roughly indicates location of appendix
Location- ~1/3rd of the way along a line from ASIS to umbilicus
14
AppendicitisInflammation of appendixPain- may presents in umbilical region and then
localizes in right lower quadrantRupture of appendix leads to peritonitis
(inflammation of peritoneum) Presents with severe pain, fever & abdominal rigidity
Muscle-splitting incision (of McBurney)
Used to access appendixEach muscle layer is split in direction of fiber
orientation

Flexible, dynamic container, housing most of the organs of alimentary system & part of urogenital system
Subdivided into ◦ Anterior, right
and left lateral & posterior wall

Protect viscera Help maintain posture Can raise internal pressure
(voluntary or reflexive contraction) to aid◦ Expulsion of fluid (urine or
vomitus), flatus, feces or fetuses from abdominopelvic cavity
◦ Expulsion of air from thoracic cavity Accommodate expansions
caused by ingestion, pregnancy, fat deposition or pathology
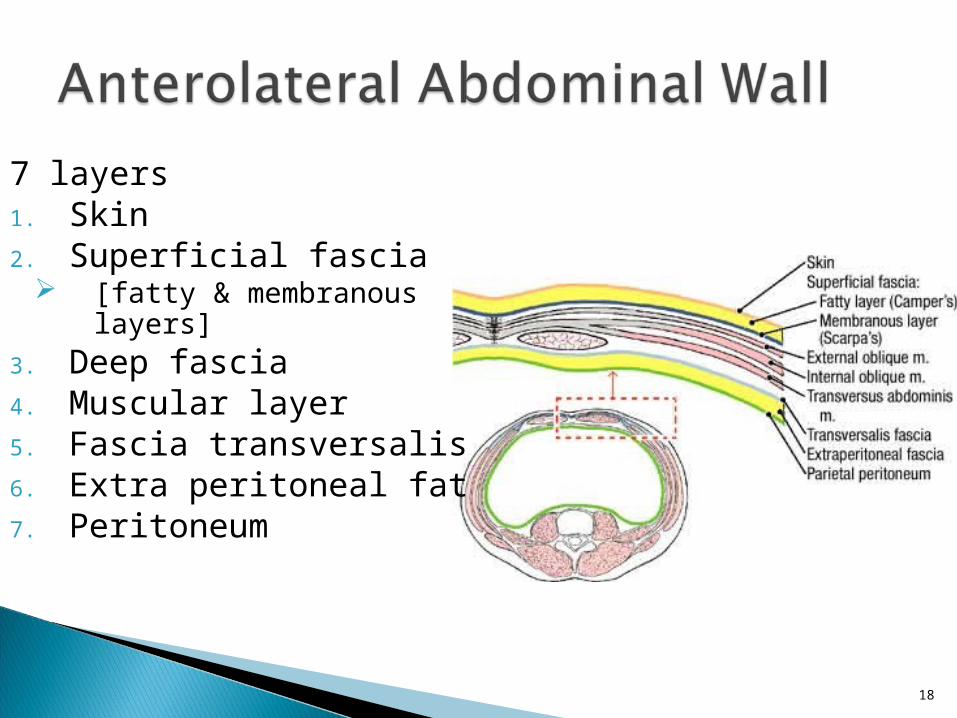
7 layers1. Skin2. Superficial fascia
[fatty & membranous layers]
3. Deep fascia4. Muscular layer5. Fascia transversalis6. Extra peritoneal fat7. Peritoneum
18
19

Superficial fatty layer◦ Camper's fascia◦ Major site of fat
storage◦ Fatty layer continuous
with superficial fascia of thorax & thigh
Deep membranous layer ◦ Scarpa's fascia
20

Scarpa's fascia◦ Membranous layer
continuous with Dartos layer of
scrotum (dartos fascia)
Superficial perineal fascia (Colles' fascia)
Superficial penile fascia
◦ Fuses with Fascia lata of thigh

Note the Arrangement of fatty layer & membranous layer of superficial fascia in lower part of anterior abdominal wall 22
•Note the line of fusion between membranous layer & deep fascia of thigh (fascia lata)•~2.5 cm inferior & parallel to inguinal ligament
Arrows indicate paths taken by urine in cases of ruptured urethra

Note the attachment of membranous layer to posterior margin of perineal membrane
23
Arrows indicate paths taken by urine in cases of ruptured urethra
24
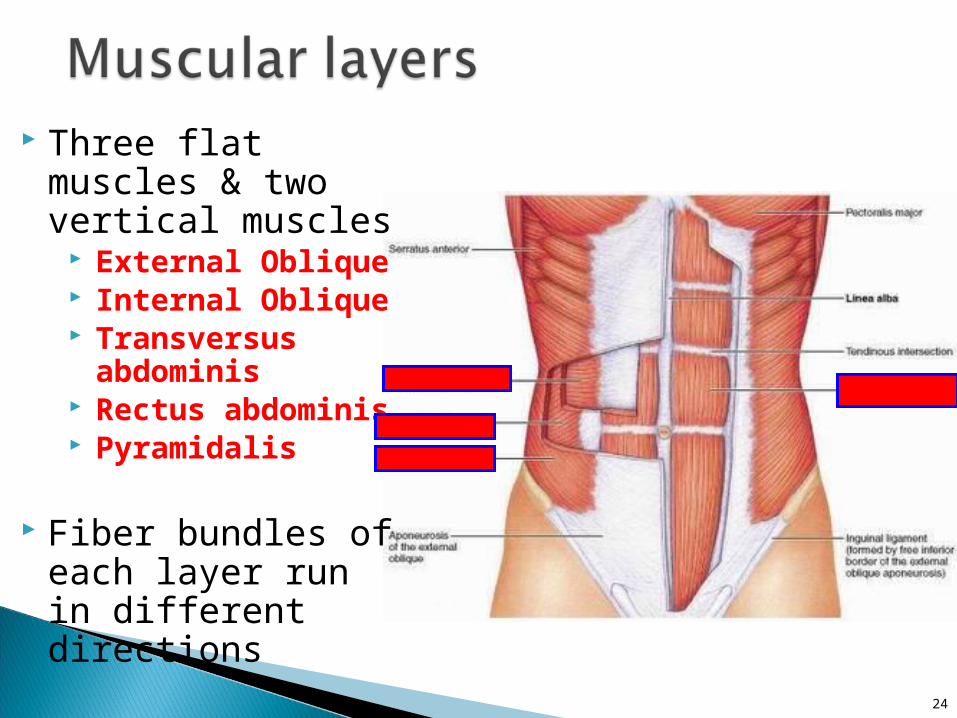
Three flat muscles & two vertical muscles
External Oblique Internal Oblique Transversus
abdominis Rectus abdominis Pyramidalis
Fiber bundles of each layer run in different directions

Largest & superficial Fibers run
downward, forward & medially
Fibers end in aponeurosis that contributes to rectus sheath
Innervation- T7-T11 spinal nerves and subcostal nerve

Derivatives of external oblique aponeurosis◦ Inguinal ligament
Thickens and folds back on itself
◦Lacunar ligament Forms medial boundary of
femoral ring◦Superficial inguinal
ring Triangular-shaped Defect in aponeurosis of
external oblique above pubic tubercle
26


28

Thin muscular layer Fibers run
upwards, forwards and medially
Fibers end in an aponeurosis that contributes to rectus sheath
Innervation- ◦ Ventral rami of T6-T12
spinal nerves◦ First lumbar nerves
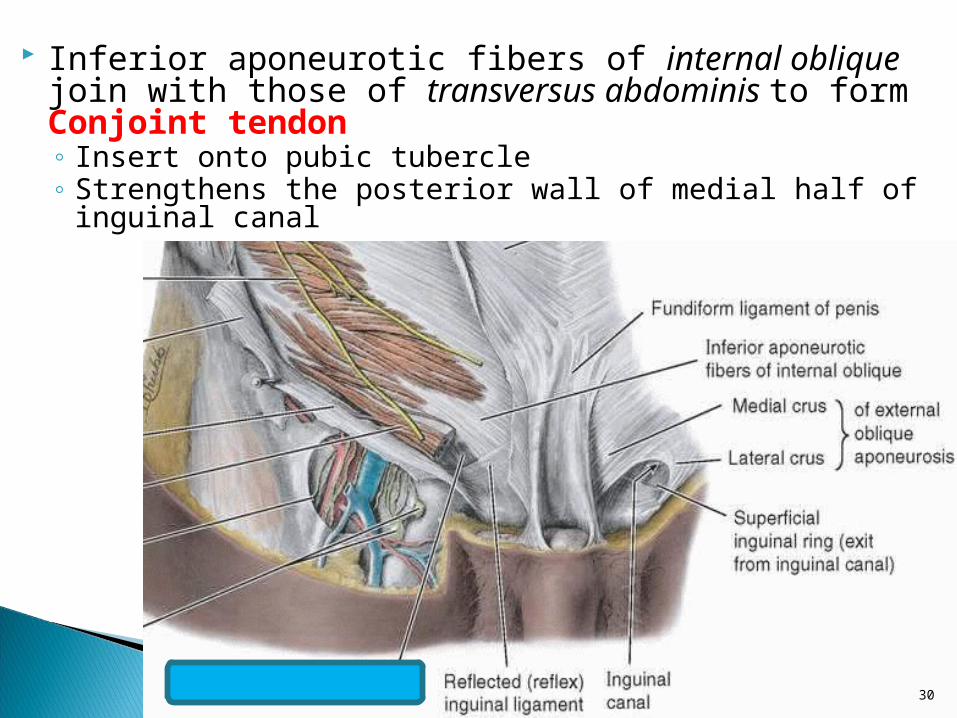
Inferior aponeurotic fibers of internal oblique join with those of transversus abdominis to form Conjoint tendon◦ Insert onto pubic tubercle ◦ Strengthens the posterior wall of medial half of inguinal
canal
30

Intramuscular & intermuscular fiber exchanges within the bilaminar aponeuroses of external and internal oblique muscles

Fibers run transversely & medially
Fibers end in an aponeurosis that contributes to rectus sheath
Innervation- ◦ Ventral rami of
T6–T12 spinal nerves
◦ First lumbar nerves

Separated by linea alba in midline
Wider superiorly than inferiorly
Composed of four segments connected by tendinous intersections that attach anteriorly to the sheath of this muscle

Innervation- ◦ Ventral rami of T6–T12 spinal nerves ◦ First lumbar nerves
Superior epigastric & inferior epigastric arteries running on their deep surfaces
Semilunar line (linea semilunaris) ◦ Vertical indentation seen as a curved line from tip
of 9th rib cartilage to pubic tubercle on each side ◦ Represents lateral edge of rectus abdominus
muscle
34

When you see a six pack, this is the muscle you're seeing
Semilunar line
35

Small, insignificant, triangular muscles
Lies anterior to rectus abdominis
Located in rectus sheath
Function◦ Tenses the linea alba◦ Surgeons use
attachment of pyramidalis to linea alba as a landmark for median abdominal incision
36
Pubic crest linea alba
Absent in ~20% people

37

Tough, incomplete fibrous sheath
Semilunar line marks lateral border
Composed of aponeuroses of three flat muscles
Contents- ◦ Rectus abdominis
& pyramidalis◦ Superior &
inferior epigastric vessels, lymphatics, & ventral primary rami of T7–T12
38

Arcuate line (linea semicircularis)◦ Crescent-
shaped line◦ Demarcates
lower limit of posterior layer of rectus sheath
39
39

40
Above arcuate lineAnt layer
Formed by fusion of aponeurosis of external oblique and anterior leaf of aponeurosis of internal oblique
Post layer Formed by fusion of
posterior leaf of aponeurosis of internal oblique and aponeurosis of transverses abdominis
Below arcuate lineAnt layer
Formed by aponeuroses of all three muscles
Post layer Absent below arcuate line
(~4-5cm below umbilicus) Rectus abdominis is in
contact with transversalis fascia


Linea alba ◦ Tendinous raphe ◦ Running vertically in
midline ◦ Formed by union of
aponeuroses of flat muscles on either side
◦ Largely avascular
42
Umbilicus◦ Found in midline◦ All layers of
anterolateral abdominal wall fuse at this point

Neurovascular plane ◦ Found between
internal oblique & transversus abdominis
◦ Contains vessels & nerves supplying skin and muscles of anterior and lateral abdominal wall
◦ Nerves and vessels are transversely oriented and segmental
43


Arteries ◦ Branches of Internal
thoracic Superior epigastric Musculophrenic
◦ Branches of External iliac Inferior epigastric Deep circumflex iliac
◦ Branches of Femoral Superficial epigastric Superficial circumflex iliac
◦ Branches of Posterior intercostal (10th & 11th) & Subcostal
Veins ◦ Veins corresponding to
arteries◦ Drains away from umbilicus
to caval system 45

Superficial lymphatics ◦ Above
umbilicus→ drains to axillary nodes
◦ Below umbilicus→ drain to superficial inguinal nodes
Deep lymphatics ◦ Accompany deep
veins ◦ Drain to external
iliac, common iliac and lumbar nodes
46
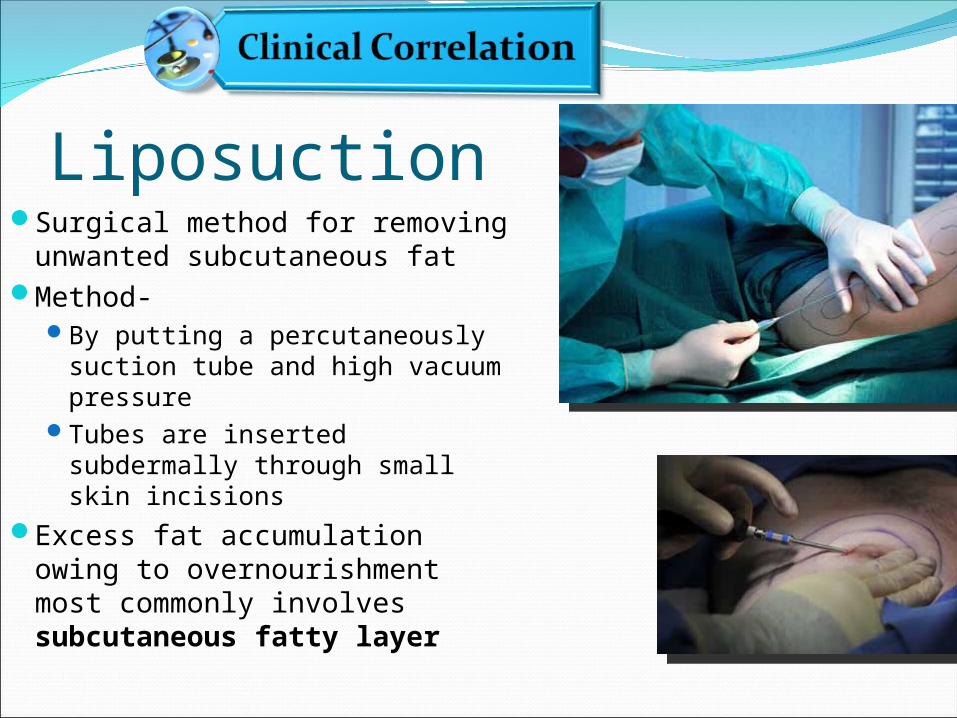
LiposuctionSurgical method for removing
unwanted subcutaneous fat Method-
By putting a percutaneously suction tube and high vacuum pressure
Tubes are inserted subdermally through small skin incisions
Excess fat accumulation owing to overnourishment most commonly involves subcutaneous fatty layer

Lined by parietal peritoneum Has five peritoneal folds (below the umbilicus)
◦ Median umbilical fold Represents remnant of urachus
◦ Medial umbilical folds (two) Represent remnants of umbilical arteries
◦ Lateral umbilical folds (two) Over the inferior epigastric vessels
Falciform ligament ◦ Extends between abdominal wall & liver (above the
umbilicus) ◦ Contains round ligament of liver


Abdominal HerniasHernia
When part of an internal organ bulges through a weak area of muscle
Most hernias occur in abdomen
Types- InguinalUmbilicalEpigastric Spigelian

Umbilical herniasCongenital
Common in newborns especially LBW infants
Anterior abdominal wall is relatively weak in umbilical ring
Usually result from increased intra-abdominal pressure in presence of incomplete closure of anterior abdominal wall after ligation of umbilical cord at birth

Acquired umbilical hernias Occur most
commonly in women and obese people
Extraperitoneal fat and/or peritoneum protrude into the hernial sac

Epigastric herniaIn epigastric region
through linea alba (in upper abdomen)
Spigelian hernias Along the semilunar
lines
Tend to occur in obese and >40 years old

Ascites‐related hernia

Thank You!Thank You!
References Keith L. Moore, Anne M. R. Agur; Essential Clinical
Anatomy- 3rd Edition, Lippincott Williams & Wilkins, 2007.
Keith L. Moore, Arthur F Dalley, Anne M. R. Agur; Clinically Oriented Anatomy- 6th Edition, Lippincott Williams & Wilkins, 2010.
Susan Standring; Gray's Anatomy: The Anatomical Basis of Clinical Practice 39th edition, Churchill Livingstone 2004.
Richard S. Snell; Clinical Anatomy By Regions- 8th Edition, Lippincott Williams & Wilkins, 2008.
55











![Anterior Abdominal Wall and Inguinal Canal …2+Unit... · Web viewAnterior Abdominal Wall and Inguinal Canal Learning Objectives – 1/5/09 [LANE] Define the boundaries of the abdominal](https://static.fdocuments.in/doc/165x107/5ae73f0a7f8b9aee078ded34/anterior-abdominal-wall-and-inguinal-canal-2unitweb-viewanterior-abdominal.jpg)