bull It is the time between conception and the onset of labor
bull Often used to describe the period during which a woman is pregnant
REPRODUCTIVE SYSTEMDanica Bianca F Agbay
bull Consists of external structures visible from the pubis to the perineum and internal structures located in the pelvic cavity
bull Develop and mature in response to estrogen and progesterone
bull This process starts in fetal life and continues to puberty and the childbearing years
Reproductive System
Female Reproductive System on the outside
Mons veneris Fatty pad that lies over the anterior surface of the
symphysis pubis
Mons pubis
Two rounded folds of fatty tissue covered with skin that extend downward and backward from the mons pubis
Protect the structure lying between them
Labia Majora
Soft folds of the skin within the labia majora that converge near the anus forming the fourchette
Fused to form prepuce and frenulum
Labia minora
Located underneath the prepuce With erectile tissue with numerous nerve endings
Clitoris
Enclosed by the labia minora that containsoopening to the urethrao Skenersquos glandoVagina hymenoBartholinrsquos gland
Vaginal vestibule
Area between the fourchette and the anus
Perineum
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
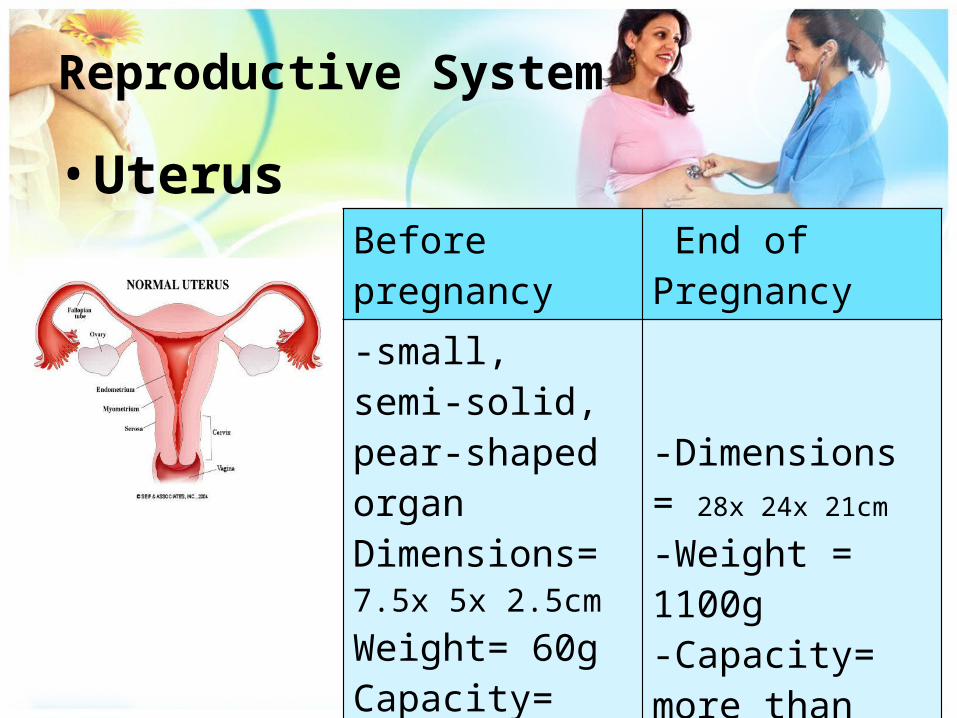
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
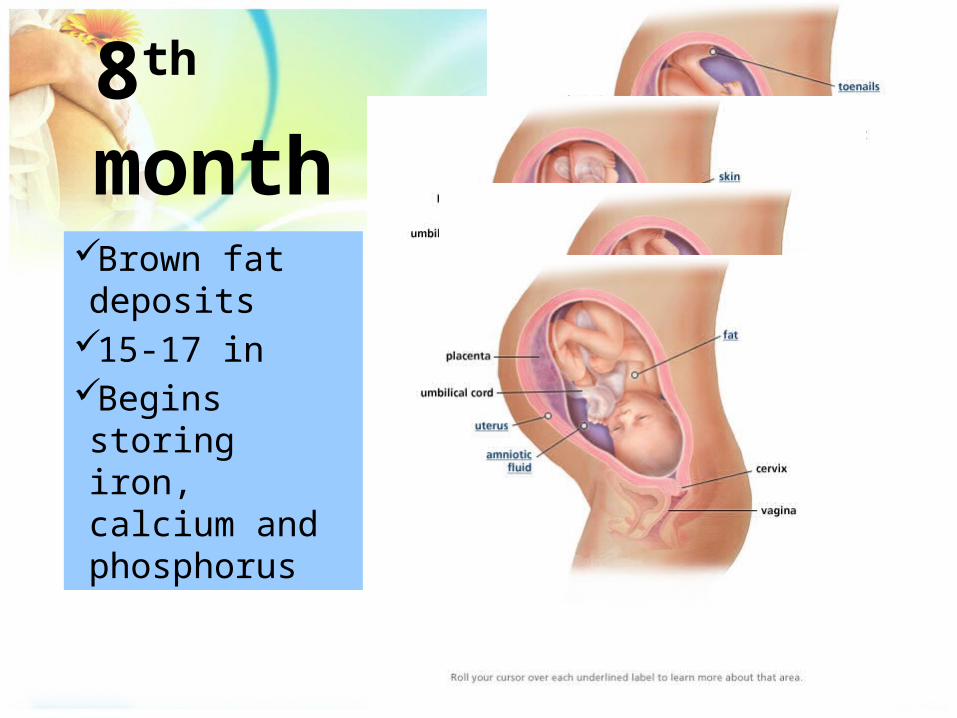
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
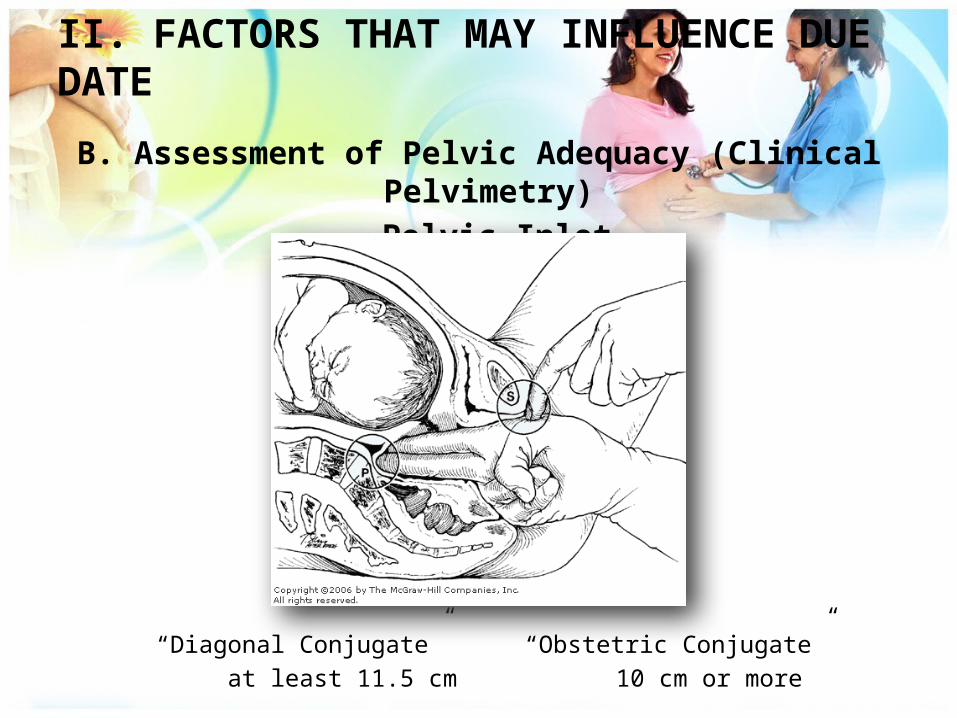
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
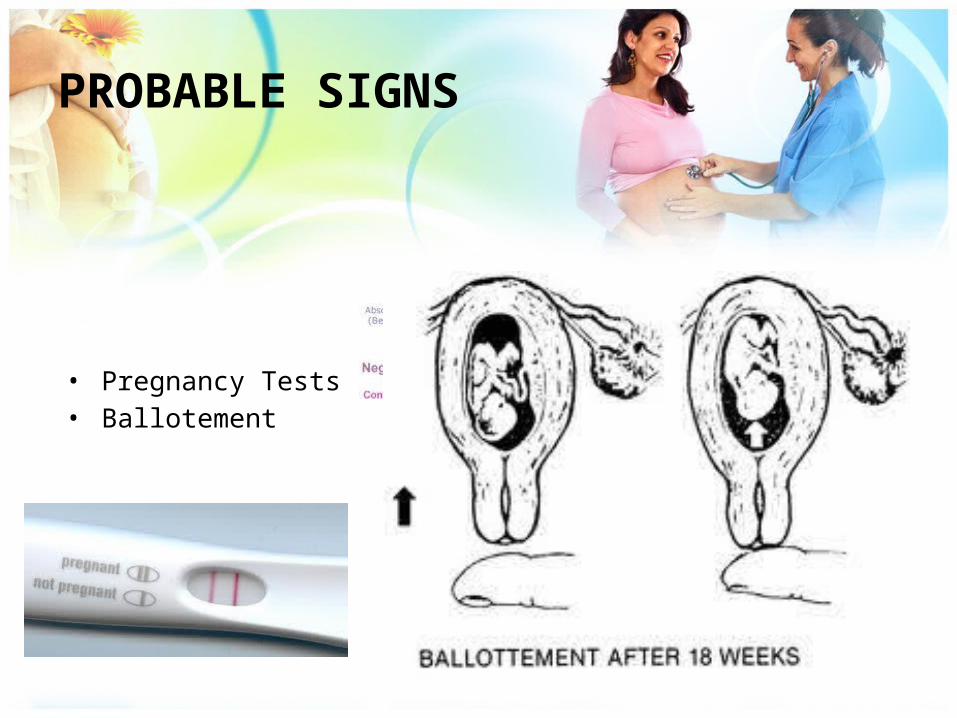
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
ANTEPARTUM
bull It is the time between conception and the onset of labor
bull Often used to describe the period during which a woman is pregnant
REPRODUCTIVE SYSTEMDanica Bianca F Agbay
bull Consists of external structures visible from the pubis to the perineum and internal structures located in the pelvic cavity
bull Develop and mature in response to estrogen and progesterone
bull This process starts in fetal life and continues to puberty and the childbearing years
Reproductive System
Female Reproductive System on the outside
Mons veneris Fatty pad that lies over the anterior surface of the
symphysis pubis
Mons pubis
Two rounded folds of fatty tissue covered with skin that extend downward and backward from the mons pubis
Protect the structure lying between them
Labia Majora
Soft folds of the skin within the labia majora that converge near the anus forming the fourchette
Fused to form prepuce and frenulum
Labia minora
Located underneath the prepuce With erectile tissue with numerous nerve endings
Clitoris
Enclosed by the labia minora that containsoopening to the urethrao Skenersquos glandoVagina hymenoBartholinrsquos gland
Vaginal vestibule
Area between the fourchette and the anus
Perineum
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
REPRODUCTIVE SYSTEMDanica Bianca F Agbay
bull Consists of external structures visible from the pubis to the perineum and internal structures located in the pelvic cavity
bull Develop and mature in response to estrogen and progesterone
bull This process starts in fetal life and continues to puberty and the childbearing years
Reproductive System
Female Reproductive System on the outside
Mons veneris Fatty pad that lies over the anterior surface of the
symphysis pubis
Mons pubis
Two rounded folds of fatty tissue covered with skin that extend downward and backward from the mons pubis
Protect the structure lying between them
Labia Majora
Soft folds of the skin within the labia majora that converge near the anus forming the fourchette
Fused to form prepuce and frenulum
Labia minora
Located underneath the prepuce With erectile tissue with numerous nerve endings
Clitoris
Enclosed by the labia minora that containsoopening to the urethrao Skenersquos glandoVagina hymenoBartholinrsquos gland
Vaginal vestibule
Area between the fourchette and the anus
Perineum
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull Consists of external structures visible from the pubis to the perineum and internal structures located in the pelvic cavity
bull Develop and mature in response to estrogen and progesterone
bull This process starts in fetal life and continues to puberty and the childbearing years
Reproductive System
Female Reproductive System on the outside
Mons veneris Fatty pad that lies over the anterior surface of the
symphysis pubis
Mons pubis
Two rounded folds of fatty tissue covered with skin that extend downward and backward from the mons pubis
Protect the structure lying between them
Labia Majora
Soft folds of the skin within the labia majora that converge near the anus forming the fourchette
Fused to form prepuce and frenulum
Labia minora
Located underneath the prepuce With erectile tissue with numerous nerve endings
Clitoris
Enclosed by the labia minora that containsoopening to the urethrao Skenersquos glandoVagina hymenoBartholinrsquos gland
Vaginal vestibule
Area between the fourchette and the anus
Perineum
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Female Reproductive System on the outside
Mons veneris Fatty pad that lies over the anterior surface of the
symphysis pubis
Mons pubis
Two rounded folds of fatty tissue covered with skin that extend downward and backward from the mons pubis
Protect the structure lying between them
Labia Majora
Soft folds of the skin within the labia majora that converge near the anus forming the fourchette
Fused to form prepuce and frenulum
Labia minora
Located underneath the prepuce With erectile tissue with numerous nerve endings
Clitoris
Enclosed by the labia minora that containsoopening to the urethrao Skenersquos glandoVagina hymenoBartholinrsquos gland
Vaginal vestibule
Area between the fourchette and the anus
Perineum
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Mons veneris Fatty pad that lies over the anterior surface of the
symphysis pubis
Mons pubis
Two rounded folds of fatty tissue covered with skin that extend downward and backward from the mons pubis
Protect the structure lying between them
Labia Majora
Soft folds of the skin within the labia majora that converge near the anus forming the fourchette
Fused to form prepuce and frenulum
Labia minora
Located underneath the prepuce With erectile tissue with numerous nerve endings
Clitoris
Enclosed by the labia minora that containsoopening to the urethrao Skenersquos glandoVagina hymenoBartholinrsquos gland
Vaginal vestibule
Area between the fourchette and the anus
Perineum
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Soft folds of the skin within the labia majora that converge near the anus forming the fourchette
Fused to form prepuce and frenulum
Labia minora
Located underneath the prepuce With erectile tissue with numerous nerve endings
Clitoris
Enclosed by the labia minora that containsoopening to the urethrao Skenersquos glandoVagina hymenoBartholinrsquos gland
Vaginal vestibule
Area between the fourchette and the anus
Perineum
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Enclosed by the labia minora that containsoopening to the urethrao Skenersquos glandoVagina hymenoBartholinrsquos gland
Vaginal vestibule
Area between the fourchette and the anus
Perineum
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Female Reproductive System on the inside
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull produce eggsbull receive the spermsbull provide the site for fertilizationbull implantation of the growing embryo and
development of the fetusbull produces hormones that control the various stages
of ovulation and maintenance of pregnancy
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull The secretions are acidic which is not conducive to the sperms as semen is alkaline
ndash Passage for menstrual flowndash Female organ of copulationndash Part of the birth canal for vaginal childbirth
Vagina
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull Upper end- corpusbull Lower end- cervix which provides a protective
entrance for the body of the uterus
bull serves for reception implantation retention and nutrition of the fertilized ovum and for cyclic menstruation
Uterus
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull Function of the cervical mucousndash To lubricate the vaginal canalndash To act as bacteriostatic agentndash To provide an alkaline environment to shelter deposited
sperm from the acidic vagina
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull Uterine wall
Endometrium- several glands (innermost)
Myometrium- smooth muscles (midlayer)
Peritoneum- connective tissue
bull The inner surface of the uterus provides a site for the implantation of the embryo
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull Arises from the ovaries of each side to the uterus supported by the broad ligaments
bull Provide transport for the ovum from the ovary to the uterus
bull Provide site for fertilization of the egg by the sperm
Fallopian tubeoviduct
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull For ovulation and hormone productionbull produce eggs one at a time every month bull The eggs are produced by the germinal epithelial cells
of the ovarybull Primary source of the estrogen and progesterone
Ovaries
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull Protection of the pelvic structuresbull Accommodation of the growing fetus during pregnancybull Anchorage of the pelvic support structures
Bony pelvis
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
False Pelvis-upper portion above the pelvic brim
or inlet-level of ischial spine
True Pelvis-lower curved bony canal-level of the ischial tuberosities and the pubic archinlet cavity and outlet
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull Conical and symmetrically placed on side of the chest
bull Nipplebull Areolabull Provide nourishment and
protective maternal antibodies to infants through the lactation process
bull Source of pleasurable sexual sensation
Breasts
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
EstrogenProgesteroneProstaglandins
Female hormones
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Estrogen
bull Associated with characteristics contributing to the ldquofemalenessrdquo
bull Controls the development of the female secondary sex characteristics
bull Assists in the maturation of the ovarian follicles and cause the endometrial mucosa and proliferative following menstruation
bull Amount is greatest during proliferative phase of the menstrual cycle
bull Causes the uterus to increase in size and weight
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Progesterone
bull Hormone of pregnancybull Secreted by the corpus luteumbull Amount is greatest during secretory phasebull Decreases uterine motility and contractility caused by the
estrogenbull Causes the uterine endometrium to further increase its supply
of glycogen arterial blood secretory glands amino acids and water
Prostaglandin
bull Oxygenated fatty acids produced by the cellls of the endometrium
bull Increases during follicular maturation dependent on gonadotropin
Neurohumoral basis of FRC
Hypothamlamus
GnRHanterior pituitary gland
FSH and LH lutenizing the theca and Dec Est and Inc Prog granulosa cells of the
Ovarian follicle ruptured follicle Ovulation
Inc Estrogen
Enhance the development of the follicle
bull Periodic uterine bleeding that begins approximately 14 days after ovulationEndometrial
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
In modern practice a gestation calculator or wheel permits the caregiver to calculate the EDB
even more quickly
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull It is the time measured from the first day of the womans last menstrual cycle to the current date It is measured in weeks A normal pregnancy can range from 38 to 42 weeks
Age of Gestation (AOG)
LMP September 28 2008Assessment date April 21 2009
LMP September 28 ndash 7 = 21 days left after LMP
September 21October 31November 30December 31 January 31February 28March 31April 21 2009
= 224 divided by 7 = 32 weeks AOG 32 weeks divided by 4 = 8 months
TINAMBAN STYLE
A Uterine Assessment
Physical Examinationbull First 10-12 weeks of pregnancybull Uterine size is compatible to
menstrual historybull May be the single most important clinical method
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Reproductive System
bull UterusBefore pregnancy End of Pregnancy-small semi-solid pear-shaped organDimensions= 75x 5x 25cmWeight= 60gCapacity= 10mL
-Dimensions = 28x 24x 21cm-Weight = 1100g-Capacity= more than 5000mL
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Reproductive System-Uterus
bull Limited increase in cell number during the pregnancy
bull Enlarging of the uterus developing placenta and growing fetus inc blood flow to the uterus
bull 16 of the maternal blood flow is within the vascular system of the uterus
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Reproductive System-Uterus
Inc fibrous tissue between muscle bands inc strength and elasticity of the muscle wall
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Reproductive System
bull Cervixbull Estrogen stimulates glandular
tissue of the cervix which increases in cell number and becomes hyperactive
bull Endocervical glands secrete thick and sticky mucus mucus plug
= protects the endocervical canal from the ascent of microorganisms into the uterus Expelled as the cervical dilatation begins
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Reproductive System-Cervix
bull Increased cervical vascularity causes Goodellrsquos sign (softening of the cervix) and Chadwickrsquos sign (bluish discoloration)
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Reproductive System
bull Ovaries
bull Ovaries stopped producing ova during pregnancybull Corpus luteum continues to produce hormones until week6-8 bull Progesterone is secreted until 7th week placenta assumes the role to
support the endometrium
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Reproductive System
bull Vaginabull Estrogen thickens the vaginal
mucosa loosening its connective tissues and increases vaginal secretions
bull Its secretions are thick white and acidic prevents bacterial infection but favors the growth of yeast organism
bull susceptibility to monilial infections
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Breasts
bull Enlarged and become more nodular as glands increase in size and number in preparation for lactation
bull Nipples become more erectile areolas darken
bull Montgomeryrsquos follicles enlarge striae may develop
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Respiratory System
bull Volume of air breath increases each minute from 30 to 40
bull Progesterone decreases airway resistance which permits increase of oxygen consumptions of 15 - 20
bull Abdominal breathing thoracic breathingbull As uterus enlarges it presses upward and elevates
the diaphragm
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Cardiovascularbull Blood volume increases starting in the 1st
trimester increases rapidly in the 2nd and slows in the 3rd and peaks near term at about 40 to 45 above non-pregnant levels
bull inc BV = inc in erythrocytes + plasmabull CO begins to inc early in pregnancy amp
remains elevated throughout gestationbull Pulse = inc of 10-15 bpmbull Leukocyte production = inc slightly to an
average of 5000 to 12000mm3
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Cardiovascularhellip
bull Pressure to the femoral and pelvic vessels=Stasis of blood in the lower extremities = Postural hypotension
bull Stasis of blood in LE dependent edema Varicosities in the veins in the legs vulva and rectum (hemorrhoids)
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Cardiovascularhellipbull When lying on supine position uterus
puts pressure on the vena cava and aorta supine hypotensive syndrome (vena caval syndrome or aortocaval compression)
SSx= dizziness pallor and clamminessPlasma increases up to 50Erythrocytes increases up to 30May lead to physiologic anemia of pregnancy or pseudoanemia
Gastrointestinal System
bull Nausea and vomiting are common = elevated human chorionic gonadotropin levels + changed carbohydrate metabolism
bull Increased secretion of saliva ptyalism (if excessive)
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS
QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS
PROBABLE SIGNS
bull Pregnancy Testsbull Ballotement
POSITIVE SIGNS
POSITIVE SIGNS
Fetal Movement
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS
QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS
PROBABLE SIGNS
bull Pregnancy Testsbull Ballotement
POSITIVE SIGNS
POSITIVE SIGNS
Fetal Movement
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
PRESUMPTIVE SIGNS
QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS
PROBABLE SIGNS
bull Pregnancy Testsbull Ballotement
POSITIVE SIGNS
POSITIVE SIGNS
Fetal Movement
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
PROBABLE SIGNS
PROBABLE SIGNS
PROBABLE SIGNS
bull Pregnancy Testsbull Ballotement
POSITIVE SIGNS
POSITIVE SIGNS
Fetal Movement
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
PROBABLE SIGNS
PROBABLE SIGNS
bull Pregnancy Testsbull Ballotement
POSITIVE SIGNS
POSITIVE SIGNS
Fetal Movement
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
PROBABLE SIGNS
bull Pregnancy Testsbull Ballotement
POSITIVE SIGNS
POSITIVE SIGNS
Fetal Movement
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
POSITIVE SIGNS
POSITIVE SIGNS
Fetal Movement
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
POSITIVE SIGNS
Fetal Movement
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
POSITIVE SIGNS
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Fetal DevelopmentEunice Heincy Aguda
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
3rd Month
2nd Month
5th Month
6th Month
7th Month
8th Month
6th Month
1st Month
Conception
4th Month
Fetal Development
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Conception
sperm fertilizes the ovum
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
1st month
first body segments Heart blood circulation and digestive tract take shape less than a 1 4rdquo
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
2nd month o Rapido Heart -- pump bloodo developed limb budso Facial features and major divisions of the brain are discernibleo Ears -- skin foldso Tiny bones and muscles
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
3rd month
o Embryo becomes fetuso Heartbeat is discernibleo more human shape o lower body developso Week 12 ndash first movements begino Sex determinableo urine production
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
4th month
o Maturation of musculoskeletal system
o Nervous system -- control
o Blood vesselso graspo Legs kick activelyo All organs begin to
mature and growo 7 ozo FHT discernibleo Insulin production
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
5th month
VernixLanugoEyebrows
eyelashes and head hair develop
schedule of sleeping sucking and kicking
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
6th month
Skeleton develops rapidly as bone forming cells increase activity
Respiratory movements begin
Fetus weighs 1 lb 10oz
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
7th month
breathe swallow regulate temperature
Surfactant formsoEyes begin to
open and close23 the size it will
be at birth
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
8th month
Brown fat deposits
15-17 inBegins storing iron calcium and phosphorus
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
9th monthuterus is
occupied by the baby thus restricting its activity
Material antibodies
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Diabetes mellitusAngelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
FOUR CARDINAL SIGNS AND SYMPTOMS
Weight loss
Polyphagia
Polyuria
Polydipsia
Babie
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
WHITErsquoS CLASSIFICATION OF DIABETES MELLITUS
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Class A Diabetes (Type 1) Insulin Dependent
ndash Absolute insulin deficiency
Glucose tolerance test slightly abnormal
Fetal survival is high
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Class C and E (Type 2) NIDDM
>
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Gestational Diabetes
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Predisposing factors
Family history of DM
Other factors
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Maternal Risks
Gestational hypertension
Spontaneous abortion
Retinopathy
Ketoacidosis
Hydramnios
Pre-term labor
Pre-eclampsia-eclampsia
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Fetal-Neonatal Risks
bull Congenital defectsndash Sacral agenesis
bull Large for gestational age Macrosomiabull Intrauterine growth restrictionbull Respiratory distress syndromebull IUFDbull Delayed lung maturitybull Ketoacidosisbull Neonatal hyperbilirubinemiabull Hypoglycemiabull Polycythemiabull Learning disabilitiesbull Childhood obesity and Type 2 DM later in life
DIAGNOSTIC TESTS
Betha Fe Albarida
Non-stress Testbull A nonstress test (NST) measures the fetal heart rate in response to
the fetus movements
Test results of the NST may be
bull Reactive (normal) - two or more accelerations of FHR of 15 beatsmin lasting 15 seconds or more in 20 min period
bull Nonreactive - there is no change in the fetal heart rate when the fetus moves lt15 betasmin or lasting lt15 seconds throughout the testing period
bull Unsatisfactory test - the data cannot be interpreted
Biophysical Profilebull Test that measures the health of your baby during
pregnancy A BPP test may include a nonstress test with electronic fetal heart monitoring and a fetal ultrasound
bull The BPP is most common in the third trimester
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Amniocentesis
bull Amniocentesis is a procedure in which amniotic fluid is removed from the uterus for testing or treatment
bull Possible after 14 week of pregnancy
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
2nd Trimester 3rd Trimester
Down syndrome (trisomy 21)Trisomy 18 and neural tube defects (NTDs)Chromosome analysisFetal hemolytic disease (Rh-
Fetal lung maturity-LS ratio
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull If neural tube defects or Rh incompatibility are a concern an amniocentesis will be performed
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Indications for use
bull Genetic concernsbull Fetal Maturity
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Chorionic Villus Sampling
bull Chorionic villus sampling (CVS) is a prenatal test in which a sample of chorionic villi is removed
from the placenta for testing
bull Done between the 10th and 12th weeks of pregnancy
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
bull The test is a way of detecting genetic disorders The sample is used to study the DNA chromosomes and chemical markers of disease in the developing baby
bull Chorionic villus sampling does not detect neural tube defects
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
You may consider chorionic villus sampling if
bull You had abnormal results from a prenatal screening test
bull You had a chromosomal abnormality in a previous pregnancy
bull Youre age 35 or older
bull You have a family history of a specific genetic disorder or you or your partner is a known carrier of a genetic disorder
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Oral Glucose Tolerance Test
bull An OGTT can be used to diagnose prediabetes and diabetes An OGTT is most commonly done to check for diabetes that occurs with pregnancy (gestational
diabetes)
For the 50-gram oral glucose tolerance test that is used to screen for gestational diabetes
bull 1 hour less than 140 mgdL
For the 100-gram oral glucose tolerance test
Fasting less than 95 mgdL1 hour less than 180 mgdL2 hours less than 155 mgdL3 hours less than 140 mgdL
Oral Glucose Challenge Test
bull A glucose challenge test (GCT) also called a one hour glucose screening test 50 gram glucose
challenge or gestational glucose screening test is a test which measures the blood sugar levels of
pregnant women
Nursing Care PlansBenedict Alcanices
Assessment
bull Objectivebull BP 240110bull RR 28minbull CR 123minbull T 375bull (+) Edema (grade 2)bull Distended neck veinsbull Bibasilar crackles BLF
Nursing Diagnosis
Decreased cardiac output related to decreased venous
return
Rationale
- Inadequate blood is pumped by the heart to meet the metabolic demands of the body
Goals and Objectives
bull Short term
bull After 3 hours of nursing interventions the patient will display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient will demonstrate activities that reduce the workload of the heart stress
Nursing Interventions Rationale
Keep client on bed or chair rest in position of comfort In congestive state semi-fowlerrsquos position is preferred
Decreases oxygen consumption and risk of decompensation
Administer high flow oxygen via nasal canula
To increase oxygen available for cardiac function tissue perfusion
Administer blood fluid replacement antibiotics diuretics inotropic drugs as indicated
To determine therapeutic adverse or toxic effects to therapy
Nursing Interventions Rationale
Assess urine output hourly weigh daily noting total fluid balance
To allow for timely alterations in therapeutic regimen
Decrease stimuli provide quiet environment
To promote adequate rest
Elevate legs when in sitting position To enhance venous return
- Encourage changing positions slowly dangling legs before standing
To reduce risk for orthostatic hypotension
Evaluation
bull Short term
bull After 3 hours of nursing interventions the patient display hemodynamic stability in blood pressure within her normal range
bull Long term
bull After 3 days of nursing interventions the patient demonstrates activities that reduce the workload of the heart stress
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
NURSING DIAGNOSIS
Ineffective tissue perfusion cardiopulmonary related to vasoconstriction of blood vessels secondary to pre-
eclampsia
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
RATIONALE
bull It is resulted from a systemic vasoconstriction in the body caused by pre eclampsia Vasoconstriction is the decrease in the diameter of the blood vessels which occur in diseases like pregnancy-induced hypertension Decrease in oxygen resulting in the failure to nourish the tissues at the capillary level
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
OBJECTIVES
Short termbull Client will demonstrate adequate perfusion as evidenced by stable vital
signs palpable pulses and alert and oriented absence of seizure episodes balanced intake and output decrease in presence of edema and good fetal status evaluation within a week
Long termbull Client will demonstrate readiness during the postpartal period in
monitoring onersquos health and involving oneself to dietary restrictions and medical follow up checkups and intervention
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
NURSING INTERVENTIONS RATIONALE
Monitor vital signs palpate peripheral pulses and note capillary refill assess urinary output weigh client daily and evaluate changes in mentation
Indicators of adequacy of systemic perfusion fluid blood needs and developing complications
Place client on left recumbent position Monitor maternal well- being periodically
This is to avoid uterine pressure on the vena cava and prevent supine hypotension syndrome
Ensure safety by putting the side rails always up and monitor client for tonic- clonic convulsions
Convulsions are evident in Eclampsia so it should be watched out and monitored
Provide quiet and restful environmentMaintain activity restrictions
Helps reduce stimulation and promotes relaxationReduces physical stress and tension
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
NURSING INTERVENTIONS RATIONALE
Administer oxygen as prescribed To ensure supply of oxygen to both the mother and the fetus
Administer Hydralazine as ordered Hydralazine is used to treat high blood pressure It works by relaxing the blood vessels so that blood can flow more easily through the body
Administer Magnesium sulfate as ordered
Magnesium sulfate prevents or controls seizures in pre-eclampsia brought about by vasospasm secondary to vasoconstriction of blood vessels
Promote diet with low protein low cholesterol and fat
These restrictions can help manage fluid retention and with associated hypertensive response which decrease cardiac workload
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
EVALUATION
Short termbull Clientrsquos blood pressure is below 14090mmHg urine output of above
30mlhour fetal heart rate is between 120-160 beats per min absence of seizure episodes decrease in presence of edema
Long termbull Client verbalizes plans upon discharge participates during lecture-
discussion sessions and demonstrates willingness to perform monitoring measures
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
MEDICATIONS
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
FeSO4
bull Elevates the serum iron concentration which then helps to form Hgb or trapped in the reticuloendothelial cells for storage and eventual conversion to a usable form of iron
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Nursing consideration
bull 1 Confirm that patient does have iron deficiency anemia before treatment
bull 2 Give drugs with meals ( avoiding milk eggs coffee and tea) if GI discomfort is severe slowly increase to build up tolerance
bull 3 Administer liquid preparations in water or juice to mask the taste and prevent staining of teeth have the patient drink solution with a straw
bull 4 Warn patient that stool may be dark or greenbull 5 Arrange for periodic monitoring of Hct and Hgb levels
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Contraindications Side-effectsSulfite allergy hemochromatosis hemosiderosis hemolytic anemias Use cautiously with normal iron balance peptic ulcer regional enteritis ulcerative colitis
- CNS toxicity acidosis coma and death with overdose
- GI upset anorexia nausea vomiting constipation diarrhea dark stools temporary staining of the teeth
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
MgSO4
bull Magnesium sulfate inhibits convulsion by acting at the myoneural junction to prevent release of acetylcholine and to decrease the motor and plate potential It inhibits the contraction of the uterus by directly acting on the myometrial cells and enhancing uterine blood flow
Nursing intervention
bull 1 Observe constantly when given IV Check BP and pulse q15 min or more often if indicated
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
tiredness or weakness- low body temperature- severe headache- fainting- rash or flushing
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Dexamethasone
bull Dexamethasone is a synthetic glucocorticoid which decreases inflammation by inhibiting the migration of leukocytes and reversal of increased capillary permeability It suppresses normal immune response
NURSING INTERVENTION
bull 1 Establish baseline of VS IO weight bull 2 Monitor BP during stabilization phasebull 3 Assess patient to take anti-inflammatory on schedule and
donrsquot stop abruptly expect a slight weight gain and avoid alcohol and caffeine
bull 4 May be beneficial for HELPSS
CONTRAINDICATION SIDE EFFECTS
Hypersensitivity active untreated infections ophthalmic use in viral fungal disease of the eye
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Hydralazine
bull Hydralazine is a vasodilator that works by relaxing the muscles in the blood vessels to help them dilate (widen) This lowers blood pressure and allows blood to flow more easily through the veins and arteries
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Nursing intervention
bull 1 Monitor the clientrsquos blood pressure and pulse frequently during initial dosage adjustment and periodically throughout therapy Report significant changes to the physician
bull 2 Monitor frequency of prescription refills to determine adherencebull 3 Prior to and periodically during prolonged therapy the following lab values
should be monitored CBC electrolytes LE Cell Prep and ANA titerbull 4 The nurse must be aware that Hydralazine may cause a positive direct
Coombrsquos test resultbull 5 IM or IV route should be used only when the drug cannot be given orallybull 6 Hydralazine may be administered concurrently with diuretics or beta
blockers to permit lower doses and minimize side effectsbull 7 It is important to remind the patient to keep using Hydralazine as
directed even if he or she feels well High blood blood pressure often has no symptoms so you may not know when your blood pressure is high
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
CONTRAINDICATION SIDE EFFECTSHypersensitivitySevere tachycardiaDissecting aortic aneurysmHeart failure with high cardiac outputCor pulmonaleMyocardial insufficiency due to
mechanical obstructionCoronary artery diseasIdiopathic SLEPatients with recent MI
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Nicardipine
bull Inhibits the transport of calcium into myocardial and vascular smooth muscle cells resulting in inhibition of excitation-contraction coupling and subsequent contraction
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
NURSING INTERVENTION
bull 1 Advise patient to avoid grapefruit and grapefruit juice during therapybull 2 Caution patient to change positions slowly to minimize orthostatic
hypotensionbull 3 May cause drowsiness or dizziness Advise patient to avoid driving or other
activities requiring alertness until response to the medication is knownbull 4 Instruct patient to avoid concurrent use of alcohol or OTC medications
especially cold preparations without consulting health care professionalbull 5 Advise patient to notify health care professional if irregular heartbeat
dyspnea swelling of hands and feet pronounced dizziness nausea constipation or hypotension occurs or if headache is severe or persistent
bull 6 Caution patient to wear protective clothing and to use sunscreen to prevent photosensitivity reactions
bull 7 Angina Instruct patient on concurrent nitrate or beta-blocker therapy to continue taking both medications as directed and to use SL nitroglycerin as needed for anginal attacks
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
CONTRAINDICATION SIDE EFFECTSHypersensitivity Sick sinus syndrome 2nd- or 3rd-degree AV block (unless an artificial pacemaker is in place) BP lt90mmHg Advanced aortic stenosis Use Cautiously in Severe hepatic impairment (dose reduction recommended) Geri Geriatric patients (dose reductionslower IV infusion rates recommended foremost agents increased risk of hypotension) Severe renal impairment (dose reduction may be necessary) History of serious ventricular arrhythmias or CHF OB Lactation Pedi Pregnancy lactation or children (safety not established)
- increased heart rate due to the drop in blood pressure
- Other side effects include swelling of the feet(edema)
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Furosemide
bull Inhibits the reabsorption of sodium and chloride from the proximal and distal renal tubules and the loop of Henle leading to a sodium-rich diuresis
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
Nursing intervention
bull 1 Administer with food or milk to prevent GI upsetbull 2 Reduce dosage if given with other antihypertensives readjust dosage gradually as BP
respondsbull 3 Give early in the day so that increased urination will not disturb sleepbull 4 Avoid IV use if oral use is at all possiblebull 5 Do not mix parenteral solution with highly acidic solutions with pH below 35bull 6 Do not expose to light may discolor tablets or solution do not use discolored drug
or solutionsbull 7 Discard diluted solution after 24 hrbull 8 Refrigerate oral solutionbull 9 Measure and record weight to monitor fluid changesbull 10 Arrange to monitor serum electrolytes hydration liver function
bull 11 Arrange for potassium-rich diet or supplemental potassium as needed
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation
NAEGELErsquoS RULE (Expected date of birth) EDB = (1st day of LMP)
PARIKHrsquoS FORMULA EDB = LMP + 9 months + (Duration of previous
In modern practice a gestation calculator or wheel permits the
Age of Gestation (AOG)
TINAMBAN STYLE
II FACTORS THAT MAY INFLUENCE DUE DATE
II FACTORS THAT MAY INFLUENCE DUE DATE (2)
II FACTORS THAT MAY INFLUENCE DUE DATE (3)
II FACTORS THAT MAY INFLUENCE DUE DATE (4)
II FACTORS THAT MAY INFLUENCE DUE DATE (5)
II FACTORS THAT MAY INFLUENCE DUE DATE (6)
Leopolds Maneuver
III SUBSEQUENT PRENATAL ASSESSMENT
III SUBSEQUENT PRENATAL ASSESSMENT (2)
IV PREGNANCY NUTRITION
Maternal Weight Gain
Maternal Weight Gain (2)
Nutritional Concerns
Maternal Physiologic Changes
Maternal Physiologic Changes (2)
Reproductive System (2)
Reproductive System-Uterus
Reproductive System-Uterus (2)
Reproductive System (3)
Reproductive System-Cervix
Reproductive System (4)
Reproductive System (5)
Breasts (2)
Respiratory System
Cardiovascular
Cardiovascularhellip
Cardiovascularhellip (2)
Gastrointestinal System
Urinary Tract
Urinary Tract (2)
PHYSIOLOGICAL CHANGES IN PREGNANCY
DERMATOLOGIC CHANGES
MUSCULOSKELETAL CHANGES
EYES
METABOLIC CHANGES
ENDOCRINE CHANGES
Slide 74
SIGNS OF PREGNANCY
SIGNS OF PREGNANCY (2)
PRESUMPTIVE SIGNS
PRESUMPTIVE SIGNS (2)
PRESUMPTIVE SIGNS QUICKENING
PROBABLE SIGNS
PROBABLE SIGNS (2)
PROBABLE SIGNS (3)
POSITIVE SIGNS
POSITIVE SIGNS Fetal Movement
POSITIVE SIGNS (2)
Fetal Development Eunice Heincy Aguda
Slide 87
Conception
1st month
2nd month
3rd month
4th month
5th month
6th month
7th month
8th month
9th month
Diabetes mellitus Angelini Agreda
FOUR CARDINAL SIGNS AND SYMPTOMS
Whitersquos Classification of Diabetes Mellitus
DR PRISCILLA WHITE
Class A Diabetes (Type 1) Insulin Dependent
Class C and E (Type 2) NIDDM
Gestational Diabetes
Predisposing factors
Maternal Risks
Fetal-Neonatal Risks
DIAGNOSTIC TESTS
Non-stress Test
Slide 110
Test results of the NST may be
Biophysical Profile
Slide 113
Indications
Fetal Variables
Slide 116
Ultrasound
First Trimester
Second Trimester
Third Trimester
Slide 121
Amniocentesis
Slide 123
Slide 124
Indications for use
Slide 126
Chorionic Villus Sampling
Slide 128
You may consider chorionic villus sampling if
Slide 130
Oral Glucose Tolerance Test
For the 50-gram oral glucose tolerance test that is used to scr
Oral Glucose Challenge Test
Nursing Care Plans
Assessment
Nursing Diagnosis
Rationale
Goals and Objectives
Slide 139
Slide 140
Evaluation
Assessment (2)
NURSING DIAGNOSIS
RATIONALE
OBJECTIVES
Slide 146
Slide 147
EVALUATION
MEDICATIONS
FeSO4
Nursing consideration
Slide 152
MgSO4
Nursing intervention
Slide 155
Dexamethasone
NURSING INTERVENTION
Slide 158
Hydralazine
Nursing intervention (2)
Slide 161
Nicardipine
NURSING INTERVENTION (2)
Slide 164
Furosemide
Nursing intervention (3)
Slide 167
CONTRAINDICATION SIDE EFFECTSContraindicated with allergy to furosemide sulfonamides allergy to tartrazine (in oral solution) electrolyte depletion anuria severe renal failure hepatic coma pregnancy lactation