ANATOMY OF THE PELVIS/SACROILIAC JOINT -...
17
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ ANATOMY OF THE PELVIS/SACROILIAC JOINT Joint Anatomy The pelvic girdle consists of the two innominate bones, the sacrum, and the bones of the coccyx. Six joints lie within the pelvic girdle, which include the two sacroiliac joints (SIJ), the sacrococcygeal, in many cases the intercoccygeal, and the pubic symphysis. The sacroiliac joint is a synovial joint with the sacral surface covered with hyaline cartilage and the iliac surface covered with a type of fibrocartilage (1)(Table 11.1). The anterior portion is synovial and the posterior-superior portion is classified as a typical syndesmosis joint (2). These articular surfaces are different from any other joint within the body (3). The surfaces are designed for stability versus mobility; the persistence of selected furrows and ridges create an extremely rough integrated surface of congruency (4). Table 11.1: General Information about the Sacroiliac Joint. Topic Information Joint type Diarthrodial joint (synovial) surrounded anteriorly and posteriorly by a joint capsule with inner synovial membranes and hyaline cartilage on both joint surfaces Surface regions Only a superficial layer of hyaline cartilage covers the iliac surface, and its roughened surface is suggested to increase the friction coefficient of the joint, thus increasing joint stability Shape of the joint The SIJ is roughly L-shaped with a short superiorly orientated joint and a longer A-P orientated arm, which intersects at approximately the S2 level Figure 11.1: The Sacroiliac Joint
-
Upload
nguyenhanh -
Category
Documents
-
view
234 -
download
1
Transcript of ANATOMY OF THE PELVIS/SACROILIAC JOINT -...

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
ANATOMY OF THE PELVIS/SACROILIAC JOINT
Joint Anatomy
The pelvic girdle consists of the two innominate bones, the sacrum, and the bones of the
coccyx. Six joints lie within the pelvic girdle, which include the two sacroiliac joints (SIJ), the
sacrococcygeal, in many cases the intercoccygeal, and the pubic symphysis. The sacroiliac joint is a
synovial joint with the sacral surface covered with hyaline cartilage and the iliac surface covered with
a type of fibrocartilage (1)(Table 11.1). The anterior portion is synovial and the posterior-superior
portion is classified as a typical syndesmosis joint (2). These articular surfaces are different from any
other joint within the body (3). The surfaces are designed for stability versus mobility; the persistence
of selected furrows and ridges create an extremely rough integrated surface of congruency (4).
Table 11.1: General Information about the Sacroiliac Joint.
Topic Information Joint type Diarthrodial joint (synovial) surrounded anteriorly and posteriorly by
a joint capsule with inner synovial membranes and hyaline cartilage on both joint surfaces
Surface regions Only a superficial layer of hyaline cartilage covers the iliac surface, and its roughened surface is suggested to increase the friction coefficient of the joint, thus increasing joint stability
Shape of the joint The SIJ is roughly L-shaped with a short superiorly orientated joint and a longer A-P orientated arm, which intersects at approximately the S2 level
Figure 11.1: The Sacroiliac Joint

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
Wilder et al. (5) reported that the topography of the SIJ encourages the function of shock
incorporation through energy absorption of the ligamentous structures. However, the topography of
the SIJ includes flat joints that encumber very large forces, which is a recipe for shear-related
instability (6). Without some form of external passive or active stabilization, the SIJ would allow
considerable unorganized movement.
It has long been noted that women have a greater prevalence of SIJ pain than men, a
problem that is theoretically associated with joint architecture and functional needs. Ebraheim et al.
(7) reported that average females exhibit 12.8 percent less joint surface contact than males, a finding
that contrasted the report of Sgambati et al. (2). Other investigators have reported similar gross
movements between males and females (8) but notable differences in adolescent anatomy (9). Age-
related changes appear to be similar as well (8).
The pubic symphysis is a nonsynovial amphiarthrodial joint (10). The joint exhibits a thick
intrapubic fibrocartilaginous disc between the two hyaline covered pubis bones. Dysfunction to the
symphysis pubis generally results in groin pain and/or inflammatory involvement with adjacent
structures (11,12). As with the cervical spine, most fibrocartilaginous discs exhibit a cavity within the
structure, which is thought to be evidence of degeneration of the disc (1). Injury to the pubic
symphysis may be the result of direct injurious force or microtrauma related to repetitious activity
(12,13).
Figure 11.2: The Anterior Pelvis and the Symphysis Pubis

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
The sacrococcygeal joint is a synovial symphysis connection (1) and can be an origin site for
coccygeal pain (14). Similar to the pubic symphysis, a fibrocartilaginous disc between the sacrum and
the first coccyx bone develops and assists in allowing movement to the structures. When present, the
intercoccygeal joint also presents with a fibrocartilaginous disc.
Osseous Structures
The sacroiliac joint consists of the articulations of sacrum and the innominate bones. The
innominate bones are composed of the ilium, the pubis, and the ischium. The ilium is the superior-
most structure that forms the articulation with the sacrum and two-fifths of the surface of the
acetabulum (1). The pubis is the inferomedial aspect of the innominate and constitutes one-fifth of the
articulation with the acetabulum of the hip. The ischium is the inferolateral aspect of the innominate
that provides the floor of the acetabulum and the posterior two-fifths of the articular surface of the
acetabulum rim. The sacral-coccyx articulation (sacrococcygeal joint) includes the union of the coccyx
and the sacrum (1). The pubic symphysis includes the articulations of the two left and right pubic
bones.
Figure 11.3: Medial and Lateral View of the Innominates
The sacrum is a triangular-shaped bone that articulates with the ilia of the innominates. The
sacrum is formed by the fusion of five sacral vertebrae (15), a process that results in a very strong
and stable keystone. In addition to the articulation with the innominates, the sacrum articulates with
the fifth lumbar process at the base and at the two superior articular processes. The sacrum serves
as an attachment site for multiple ligaments such as the sacrotuberous ligament, the ventral sacroiliac

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
ligament, the sacrospinous ligament, and the iliolumbar ligament and muscles including the piriformis,
the multifidi, the erector spinae, and the gluteus maximus.
The triangular-shaped coccyx includes the complete or partial fusion of four bones (15). Of
the four segments, the first is the largest; and each vertebra progressively is smaller distally. The
coccyx provides an attachment for the sacrosciatic ligaments, the coccygeus muscles, and the tendon
of the external sphincter muscle.
Ligaments and Fascia
Several structures are involved in the control of movements and/or stabilization of the
sacroiliac and pelvic complex (Table 11.2). The primary ligaments associated with the sacroiliac joint
include the ventral sacroiliac ligament, the interosseous sacroiliac ligament, the long dorsal sacroiliac
ligament, the iliolumbar ligament, the sacrotuberous ligament, and the sacrospinous ligament (1). The
ligaments of the sacroiliac joint provide afferent output from the joint capsule and are innervated by
the dorsal rami of the sacral nerves S1-S4 (16).
Table 11.2: The Ligaments of the Sacroiliac Joint Region.
Ligament Information Interosseous ligament and posterior SI ligament
Lie directly posterior to the SIJ and form a strong link between the sacrum and ilium that limits nutation and inferior shear of the sacrum
Long dorsal SI ligament From posterior superior iliac spine to S2 and S3 sacral crests. This ligament limits sacral counternutation and is commonly a source of pain in patients with SIJ symptoms.
Sacrotuberous ligament Attaches from the ischeal tuberosity to the inferior lateral angle (ILA) of sacrum. The sacrotuberous ligament limits sacral nutation and will be tensioned by hamstrings contraction or stretch due to fascial linkage between biceps femoris and the lateral portion of the sacrotuberous ligament. The sacrotuberous ligament has also been shown to have fascial connections to the posterior layer of thoracolumbar fascia, gluteus maximus, and piriformis
Iliolumbar ligaments Runs from the TP of L4 and L5 to the anterior surface of the iliac crest
Sacrospinous ligament Runs from the ILA to the ischial spine
The ventral sacroiliac ligament and the interosseous sacroiliac ligament are less studied and
are poorly understood. Bowen and Cassidy (17) report that the ventral sacroiliac ligament is primarily

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
a thickening of the anterior aspect of the SIJ capsule. Although it is reported to be very strong, the
interosseous ligament is not suspected as a cause of clinically determined low back pain (17,18).
The sacrotuberous ligament has extensive connections posteriorly with the gluteus maximus,
the long head of the biceps femoris, and the sacrospinous ligament and anteriorly with the
iliococcygeus muscle (19). During loading or tension to the sacrotuberous ligament, the amount of
available movement (posterior rotation of the ilium to the sacrum or anterior rotation of the sacrum
with relation to the ilium) is restricted. Conversely, during counternutation (anterior rotation of the ilium
to the sacrum or posterior rotation of the sacrum with relation to the ilium), a slackening of the
sacrotuberous ligament occurs allowing freer movement and less stability contribution from this
ligament (19).
The long dorsal ligament can be palpated directly caudal to the posterior superior iliac spine.
The long dorsal ligament is closely integrated with the erector spinae, the posterior layer of the
thoracolumbar fascia, and the sacrotuberous ligament. The ligament contributes to the movement
stability of the SIJ, specifically counternutation (19). During counternutation, the tension is increased
in the long dorsal ligament and is slackened during nutation, a finding in opposition to the
sacrotuberous ligament (Table 11.3). Although both ligaments are physiologically connected, each
performs contradictory stabilization tasks for the SIJ.
Table 11.3: Nutation and Counternutation of the Sacroiliac Joint
Movement Plane of Motion Biomechanical Orientation Sacral flexion Sagittal Sacral nutation: sacral promontory tilts anteriorly
and inferiorly Sacral extension Sagittal Sacral counternutation: sacral promontory back
to the neutral position from an anterior-tilted position
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
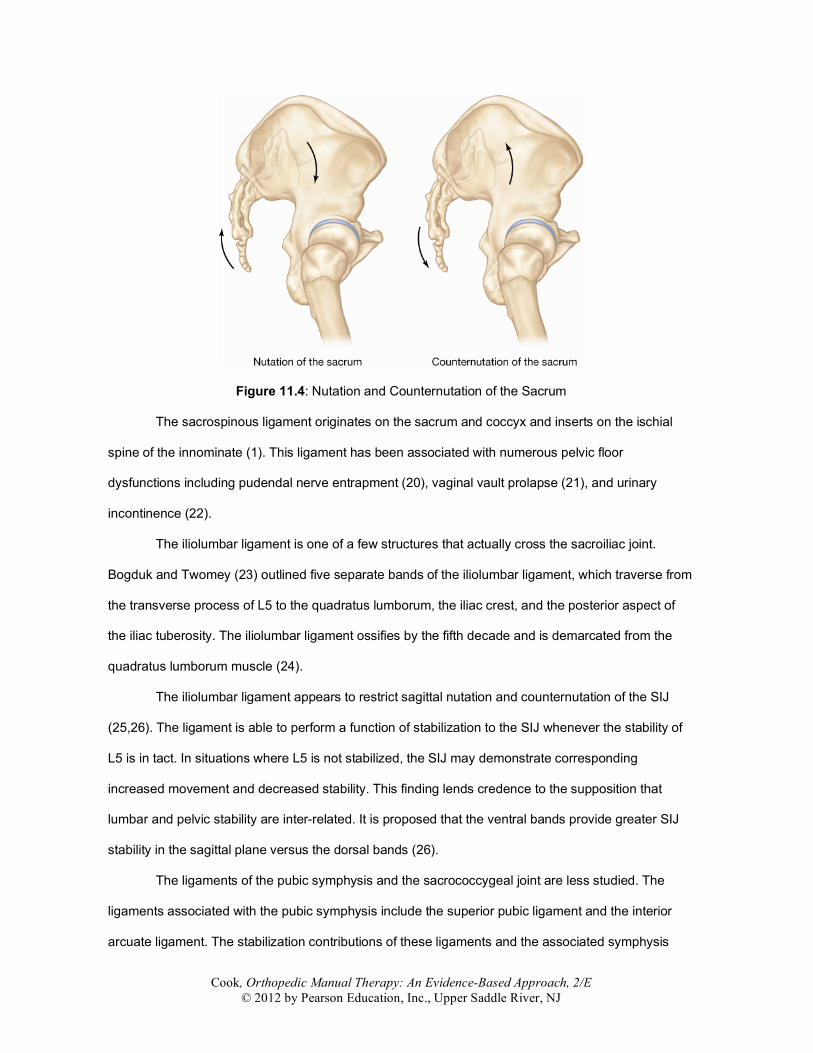
Figure 11.4: Nutation and Counternutation of the Sacrum
The sacrospinous ligament originates on the sacrum and coccyx and inserts on the ischial
spine of the innominate (1). This ligament has been associated with numerous pelvic floor
dysfunctions including pudendal nerve entrapment (20), vaginal vault prolapse (21), and urinary
incontinence (22).
The iliolumbar ligament is one of a few structures that actually cross the sacroiliac joint.
Bogduk and Twomey (23) outlined five separate bands of the iliolumbar ligament, which traverse from
the transverse process of L5 to the quadratus lumborum, the iliac crest, and the posterior aspect of
the iliac tuberosity. The iliolumbar ligament ossifies by the fifth decade and is demarcated from the
quadratus lumborum muscle (24).
The iliolumbar ligament appears to restrict sagittal nutation and counternutation of the SIJ
(25,26). The ligament is able to perform a function of stabilization to the SIJ whenever the stability of
L5 is in tact. In situations where L5 is not stabilized, the SIJ may demonstrate corresponding
increased movement and decreased stability. This finding lends credence to the supposition that
lumbar and pelvic stability are inter-related. It is proposed that the ventral bands provide greater SIJ
stability in the sagittal plane versus the dorsal bands (26).
The ligaments of the pubic symphysis and the sacrococcygeal joint are less studied. The
ligaments associated with the pubic symphysis include the superior pubic ligament and the interior
arcuate ligament. The stabilization contributions of these ligaments and the associated symphysis
Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
joint create a typically stable structure (1). The ligaments associated with the sacrococcygeal joint are
the ventral, dorsal, and lateral sacrococcygeal ligaments. The ventral sacrococcygeal ligament is a
continuation of the anterior longitudinal ligament, whereas the dorsal ligament is a continuation of the
posterior longitudinal ligament of the spine (1).
The thoracolumbar fascia envelopes the dorsal muscles of the trunk and forms an attachment
for several upper limb and trunk muscles, including the latissimus dorsi, the gluteus maximus, the
transversus abdominis, and internal oblique musculature (27). The thoracolumbar fascia transmits
forces between the spine, pelvis, and legs, and may play a role in trunk stabilization during rotation
and flexion-based activities (28). Vleeming et al. (29) purported that increased tension within the
thoracolumbar fascia leads to increased force closure and subsequent increased stability.
Summary
• The pelvic girdle consists of the two innominate bones, the sacrum, and the bones of the
coccyx. • The sacroiliac joint is a synovial joint with the sacral surface covered with hyaline cartilage
and the iliac surface covered with a type of fibrocartilage. • The primary ligaments associated with the sacroiliac joint include the ventral sacroiliac
ligament, the interosseous sacroiliac ligament, the long dorsal sacroiliac ligament, the iliolumbar ligament, the sacrotuberous ligament, and the sacrospinous ligament.
BIOMECHANICS OF THE PELVIS/SACROILIAC JOINT
Movement Analysis
The mobile sacroiliac joints function as shock absorbers (28) even during older ages (30–31).
Mooney (3) suggests that the principle function of the SIJ is to “dissipate or attenuate the loads of the
torso to the lower extremities and vice versa.” The amount of movement has been debated for
decades by clinicians and a number of assumptions have prevailed through clinical proviso.
A 2008 study by Goode et al. (32) analyzed actual three-dimensional (3-D) Cartesian
movements in studies that limited analysis to Roentgen stereophotogrammetric analysis (RSA).
Because SIJ movement is 3-D, the Cartesian system more accurately defines movement by
rotations and translations within the six degrees of freedom. RSA involves a 3-D mapping of
movements and is much more accurate than use of skin markers or other measures that have a

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
high degree of error. The review captured data from seven manuscripts, which were also evaluated
for study quality.
SIJ rotation ranged between –1.1 to 2.2 degrees along the X–axis, –0.8 to 4.0 degrees
along the Y-axis, and –0.5 to 8.0 degrees along the Z-axis during a number of functional
movements such as bending over, squatting, or sitting to standing. During the same functional
movements, the measures of SIJ translation ranged between –0.3 to 8.0 millimeters (mm) along the
X-axis, –0.2 to 7.0 mm along the Y-axis, and –0.3 to 6.0 mm along the Z-axis. The studies that
reported the largest degree of motion also presented with the largest degree of instrument
measurement error. The review summary suggested that the motion of the SIJ is limited to minute
amounts of rotation and of translation, suggesting that clinical methods using palpation for
diagnosing SIJ pathology may have limited clinical utility.
Movement of the pubic symphysis has also been investigated. Walheim and Selvik (33)
indicated the pubic symphysis rotates 3 degrees and translates 2 degrees. During single-legged
stance, the symphyseal can move vertically 2.6 mm and sagittally 1.3 mm on the weight-bearing side
(34). During walking, the pubic symphysis can piston (move up and down) up to 2.2 mm in the vertical
direction and 1.3 mm in the sagittal direction. Because hypermobility beyond this normal range could
lead to pubis instability, several investigators have examined the diagnostic utility of a standing x-ray
to determine vertical displacement (12,35,36). Berezin et al. (35) reported movements up to 5.9 mm
(s.d. 3.3 mm) in a population of patients with pelvic pain versus only 2 mm in an asymptomatic
population. Rieger and colleagues (37) reported that fail rates during externally applied loads
generally resulted in disruption in a vertical direction, typically at the pubic symphysis.
Because the movements of the pelvis, even when displaced, are so small, the most
discriminatory radiographic analysis appears to be the Chamberlain x-ray (38,39). The Chamberlain
x-ray involves an x-ray performed while the patient is standing on a box on the involved lower limb,
while the other lower limb is non–weight-bearing. This maneuver allows a vertical migration of the
weight-bearing side (pubic symphysis) and has been associated with pelvic instability (36).

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
Summary
• The mobile sacroiliac joints function as shock absorbers during younger and older ages (with
a principle function to dissipate or attenuate the loads of the torso to the lower extremities and vice versa.
• During single-legged stance, the symphyseal can move vertically 2.6 mm and sagittally 1.3 mm on the weight-bearing side.
Muscular Contribution
Thirty-five muscles attach to the pelvis and/or sacrum and have a direct or indirect role in
stabilizing this region (15). Muscular contribution is necessary for both form and force closure at the
SIJ/pelvis. Form closure includes the passive stabilization contributions of interlocking ridges and
grooves on the joint surfaces (28) and ligamentous stabilization. Force closure is a term that
corresponds to increased SIJ/pelvis stiffness by isolated contraction of selected muscle groups. Key
muscles of force closure are the gluteus maximus, biceps femoris, erector spinae, and latissimus
dorsi (4,38,40–43). Other muscles, commonly identified as local muscles, are responsible for the
preset tension on the pelvis prior to initiation of movement. These muscles include the transversus
abdominis, the multifidi, the piriformis, and the pelvic floor muscles.
The transversus abdominis is a key muscle for stabilization of the sacroiliac joint (44,45).
Others have found the feed-forward temporal contraction of the multifidus and obliquus internus
abdominis a necessity prior to pelvic stabilization during hip flexion in standing (46,47). Pain of the SIJ
was associated with delays of these muscles.
The multifidi originations of the lower lumbar spine insert onto the articular processes of the
sacrum, the posterior thoracodorsal fascia, and the sacrotuberous ligament (15). The deep fibers of
the muscle span from one segment to the adjacent segment, while the superficial fibers span three
segmental levels. The deep fibers of the multifidi are considered the most significant stabilizers of the
pelvis and lumbar spine.
The piriformis originates from the anterior aspect of the sacrum, the anterior aspect of the
posterior inferior iliac spine, the upper aspect of the sacrotuberous ligament, and the capsule of the
sacroiliac joint (15) and inserts on the greater trochanter of the femur. Snijders et al. (6) suggest that
the piriformis plays an important role during force closure of the SIJ. The muscle is implicated as a

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
contributor for chronic buttock pain (48) and can refer pain to the sacroiliac region (15). Often, imaging
of the pelvis and lumbar spine performed on patients with suspected piriformis syndrome is
unremarkable (49).
The pelvic floor muscles such as the levator ani and coccygeus muscles have shown to
contribute considerably to pelvic ring stability. In a study by Pool-Goudzwaard et al. (50), simulated
tension in the pelvic floor muscles increases SIJ stiffness by 8.5 percent. Selected authors have
outlined the contribution of the pelvic floor muscles to increasing intra-abdominal pressure and an
increase in lumbar spinal stiffness (51,52). The muscle functions to stabilize the SIJ through force
closure and the capacity to provide counterforce stiffness on the ligaments of the SIJ (29). O’Sullivan
et al. (53) outlined inappropriate pelvic floor descent (versus ascent) during altered motor control
recruitment of the pelvic muscles in patients with SIJ pain during the active straight leg raise.
Hungerford et al. (46) indirectly lent evidence to the importance of the contribution of these
muscles to stability through their report of delayed onsets of the multifidus, the internal obliques, and
the gluteus maximus in patients with sacroiliac joint pain. Multiple authors (47,51,54,55) have reported
that a feed- forward mechanism of selected pelvic stabilization exists in asymptomatic individuals and
is absent in patients with lumbopelvic pain. O’Sullivan et al. (53) suggested abnormalities in
stabilization of the diaphragm and the pelvic floor muscles during an active straight leg raise in
patients with known pelvic dysfunction. This finding demonstrates the critical role these local muscles
play in concert with ligamentous attachments for preset stability, a role very similar to the one played
in the lumbar spine.
The erector spinae is a complex muscle group that originates on multiple lumbar segments
and inserts into the medial aspect of the posterior superior iliac spine (PSIS) bilaterally and the
intermuscular aponeurosis (15). The muscle can provide lumbar extension–based movements or
unilateral side flexion when contracted on one side only.
The quadratus lumborum is thought to contribute to stability by increasing the tension of the
iliolumbar ligament. The transversus abdominis, psoas, quadratus lumborum and multifidus were
each noted to have segmental attachment patterns in the lumbar spine (56). As a group, these
muscles surround the lumbar motion segments from the anterolateral aspect of a vertebral body to

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
the spinous process. Generally, the quadratus lumborum is considered a strong ipsilateral flexor (57).
McGill et al. (58) suggest that electromyographic evidence, together with architectural features such
as attachment location and activity during selected movements make the quadratus lumborum a
better stabilizer of the spine than the psoas.
Using surface electromyographic (EMG) analysis, van Wingerden et al. (59) analyzed a
battery of muscle groups to determine which muscles most significantly contributed to force closure.
Their findings outlined the significant contribution of the erector spinae, the biceps femoris, and the
gluteus maximus to increased stiffness and decreased shear at the SIJ. To a lesser extent, the
latissimus dorsi also contributed. Notable were the contralateral and simultaneous contractions of the
erector spinae with the gluteus maximus and the contractions of the biceps femoris ispilaterally, with
the gluteus maximus. The aspect of the erector spinae that contributed most was the distal aspect,
specifically the multifidus, hypothetically contributing with the attachments to the sacral ligamentous
structures.
Summary
• Stabilization of the SIJ occurs through form and force closure. Form closure includes the
passive stabilization contributions of interlocking ridges and grooves on the joint surfaces and ligamentous stabilization. Force closure is a term that corresponds to increased SIJ/pelvis stiffness by isolated contraction of selected muscle groups.
• Thirty-five muscles attach to the pelvis and/or sacrum and have a direct or indirect role in stabilizing this region. Muscular contribution is necessary for both form and force closure at the SIJ/pelvis.
• Key muscles of force closure are the gluteus maximus, biceps femoris, erector spinae, and latissimus dorsi; however, contribution of the local muscles, such as the transversus abdominis, the multifidi, the piriformis, and the pelvic floor muscles are responsible for the preset tension on the pelvis prior to initiation of movement.
Dysfunction versus Pain
Clinicians often use a number of identifiers during implication of the SIJ region. The first
identifier used involves the term dysfunction, which proposes that the joint is malfunctioning in
some manner resulting in movement abnormalities and mal-positions. The second identifier
involves the term pain, which assumes the SIJ is the pain generator. Unfortunately, the terms SIJ
dysfunction and SIJ pain are commonly used interchangeably, as though each has the same
meaning, which they do not (60).

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
SIJ Dysfunction
In essence, a dysfunction of the pelvic girdle occurs when stabilization is lost or when
asymmetric stabilization is present between the two sides of the SIJ (61). Normally, a predictable
biomechanical sequence occurs in asymptomatic patients within the lumbopelvic region that stabilizes
the pelvis and prepares the structure for weight bearing. This process occurs through two different
methods—movement initiation and muscular contraction. Muscle contraction of the multifidi, the
gluteus maximus, and the piriformis creates initial tension in the sacrotuberous ligament and
thoracolumbar fascia prior to nutation, pre-engaging the ligaments for stability (28). During movement,
nutation (posterior rotation of the ilium with respect to the sacrum) tensions the majority of the largest
SIJ ligaments such as the sacrospinous and sacrotuberous ligaments (19). The contact area of the
sacroiliac joint is the lowest during posterosuperior displacement of ilium on the sacrum (7), thus
requires the greatest amount of force closure. Because of the muscle connections to the ligaments
and due to the nature of nutation’s increase in force closure during ligamentous tension, the SIJ
demonstrates increased stiffness. Anterior rotation of the innominate on the sacrum (counternutation)
appears to be a primary source of pain and instability in patients with chronic pelvic pain (37). Causal
displacement that occurs during counternutation (anterior rotation of the innominate on the sacrum)
places stress on the long dorsal ligament, which is normally taut during neutral positions (40).
Problems associated with feed-forward failures of ligament laxity discourage the process of
form and force closure and lead to SIJ/pelvic instability. This is the primary dysfunction associated
with SIJ and pubic symphysis pain. Instability is defined as “the inability of the joint and surrounding
structures to bear load without uncontrolled displacements” (25). Many patients report pain during
movements of the lower extremity and describe a feeling of paralysis during painful provocation (36).
Additionally, an instable pelvis has been associated with the inability to move the lower limbs (36).
Instability of the sacroiliac joints has long been suspected as a cause of low back pain and
lumbopelvic dysfunction (47). Stabilization of the SIJ is accomplished through increased friction
throughout the joint during tension of selected muscles and ligaments (62). More specifically, Pool-
Goudzwaard et al. (28) suggest that the SIJ is protected from traumatic shear forces in three ways.

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
First, because the joint is wedge shaped, the sacrum is stabilized during weight bearing by locking
into the innominates like a keystone. Second, the cartilage surfaces of the SIJ are not smooth as in
other synovial joints, thus this encourages stability, specifically in men. Men demonstrate more
cartilage abnormalities than women, thus providing greater passive stability based on structural
interface (17); however, in situations that do not involve pregnancy, ranges are similar between sexes
(8). Third, multiple furrows and ridges within the joint itself encourage a locking function during weight
bearing. This complementary system creates ‘form closure’ secondary to a closely congruent passive
locking system that is further enhanced during weight bearing (4).
Force closure involves the active element of controlled stability (28). Vleeming et al. (4)
identified this process as a ‘self-locking’ or ‘self-bracing’ mechanism that allows enough functional
movement but controlled stability to appropriately transfer large forces from the legs to the trunk. To
accomplish this challenging task, several ligaments, muscles, and fascial elements are critical. As
discussed previously, the force closure muscular contributions of the multifidi, transversus abdominis,
and other surrounding musculature are critical.
In 2002, Damen et al. (61) reported that instability is not necessarily a requisite for SIJ
dysfunction, rather that asymmetric stability is more likely the cause. Normal subjects demonstrate
large variations in laxity that is commonly stabilized by appropriate muscle contribution. Their study
used a doppler imaging (DIV) method of measuring stiffness, which analyzes pelvic girdle mobility in
vivo.
One notable consideration of the sacroiliac joint is the purported ability of the joint to assume
a ‘subluxed’ position. Because of the surface irregularities, Vleeming et al. (41) have proposed that it
is theoretically possible for the joint to move and assume a new position that is ‘locked’ into a position
of displacement. Furthermore, the amount of displacement may be so minute that radiographic
verification is unlikely (4,63). Consequently, a dysfunction may be present, which is typically
associated with stability loss, but will not likely have palpable or identifiable mal-positions (or such
subtle mal-positions that these cannot be identified) when involved. At present, the ability to palpate
variations in SIJ stability has not been confirmed.

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
SIJ Pain
SIJ pain reflects a situation in which the SIJ is the pain-generating component. Studies have
shown that the SIJ has more pain receptors than movement receptors embedded within the joint (64).
A number of systematic problems may cause pain and inflammation and pain from a dysfunction may
be present as well. What is worth noting is that pain can be present with a stability dysfunction;
however, the dysfunction may be below a clinical threshold in its presentation.
Summary
• Dysfunction of the pelvic girdle occurs when stabilization is lost or when asymmetric
stabilization is present between the two sides of the SIJ. • Anterior rotation of the innominate on the sacrum (counternutation) appears to be a primary
source of pain and instability in patients with chronic pelvic pain. • A posterior rotated innominate tends to be a more stable position as compared to anterior
rotation. • The SIJ is protected from traumatic shear forces in three ways: 1) through the wedge-shaped
anatomy, 2) through the interlocking furrows and ridges, and 3) through the shape of the surface cartilage.
• Because of the surface irregularities, it is theoretically possible for the joint to move and assume a new position that is ‘locked’ into a position of displacement, a position that is too small for radiographic verification.
ONLINE REFERENCES
1. Lee D. The pelvic girdle. An approach to the examination and treatment of the lumbo-pelvic-hip region. Edinburgh; Churchill Livingstone: 1989.
2. Sgambati E, Stecco A, Capaccioloi L, Brizzi E (Abstract). Morphometric análisis of the sacroiliac joint. Ital J Anat Embryol. 1997;102:33–38.
3. Mooney V. Sacroiliac joint dysfunction. In: Vleeming A, Mooney V, Dorman T, Snijders C, Stoeckart R. Movement stability and low back pain: the essential role of the pelvis. New York; Churchill Livingstone: 1997.
4. Vleeming A, Stoeckart R, Volkers C, Snijders C. Relation between form and function in the sacroiliac joint. Part 1: Clinical anatomic aspects. Spine. 1990;15:130–132.
5. Wilder DG, Pope MH, Frymoyer JW. The functional topography of the sacroiliac joint. Spine. 1980;5:575–579.
6. Snijders C, Vleeming A, Stoeckart R. Transfer of lumbosacral load to iliac bones and legs 1. Biomechanics of self-bracing of the sacro-iliac joints and its significance for treatment and exercise. Clin Biomech. 1993;8:285–294.
7. Ebraheim NA, Madsen TD, Xu R, Mehalik J, Yeasting RA. Dynamic changes in the contact area of the sacroiliac joint. Orthopedics. 2003;26(7):711–714.
8. Jacobs H, Kissling R. The mobility of the sacroiliac joints in healthy volunteers between 20 and 50 years of age. Clin Biomech. 1995;10:352–361.
9. Bollow M, Braun J, Kannenberg J, et al. Normal morphology of sacroiliac joints in children: magnetic resonance studies related to age and sex. Skeletal Radiol. 1997;26:697–704.
10. Gamble J, Simmons S, Freedman M. The symphysis pubis. Anatomic and pathologic considerations. Clin Orthop. 1986;203:261–272.

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
11. Aslan E, Fynes M. Symphysial pelvic dysfunction. Curr Opin Obstet Gynecol. 2007;19(2):133–9.
12. Williams P, Thomas D, Downes E. Osteitis pubis and instability of the pubic symphysis. When nonoperative measures fail. Am J Sports Med. 2000;28:350–355.
13. Phieffer L, Lundberg W, Templeman D. Instability of the posterior pelvic ring associated with disruption of the pubic symphysis. Orthop Clin North Am. 2004;35:445–449.
14. Traycoff RB, Crayton H, Dodson R. Sacrococcygeal pain syndromes: diagnosis and treatment. Orthopedics. 1989;12(10):1373–1377.
15. Lee D. The pelvic girdle. An approach to the examination and treatment of the lumbo-pelvic-hip region. 2nd ed. Edinburgh; Churchill Livingstone: 1999.
16. Grob KR, Neuhuber WL, Kissling RO. (Abstract). Innervation of the sacroiliac joint of the human. Z Rheumatol. 1995;54(2):117–122.
17. Bowen V, Cassidy J. Macroscopic and microscopic anatomy of the sacroiliac joint from embryonic life until the eighth decade. Spine. 1985;6:620–628.
18. MacAvoy MC, McClellan RT, Goodman SB, Chien CR, Allen WA, van der Meulen MC. Stability of open-book pelvic fractures using a new biomechanical model of single-limb stance. J Orthop Trauma. 1997;11(8):590–593.
19. Vleeming A, de Vries H, Mens J, van Wingerden JP. Possible role of the long dorsal sacroiliac ligament in women with peripartum pelvic pain. Acta Ostet Gynecol Scand. 2002;81:430–436.
20. Ramsden CE, McDaniel MC, Harmon RL, Renney KM, Faure A. Pudendal nerve entrapment as source of intractable perineal pain. Am J Phys Med Rehabil. 2003;82(6):479–484.
21. Silva-Filho AL, Santos-Filho AS, Figueiredo-Netto O, Triginelli SA. Uncommon complications of sacrospinous fixation for treatment of vaginal vault prolapse. Arch Gynecol Obstet. 2005;271(4):358–362.
22. Boukerrou M, Lambaudie E, Collinet P, et al. (Abstract). Mechanical resistance of pelvic ligaments used for incontinence or prolapse surgery. Gynecol Obstet Fertil. 2004;32(7-8):601–606.
23. Bogduk N, Twomey L. Clinical anatomy of the lumbar spine. Melbourne; Churchill Livingstone: 1987.
24. Luk K, Ho H, Leong J. The iliolumbar ligament: a study of its anatomy, development and clinical significance. J Bone Jnt Surg. 1986;68:197–200.
25. Pool-Goudzwaard A, van Dijke G, Mulder P, Spoor C, Snijders C, Stoeckart R. The iliolumbar ligament: its influence on stability of the sacroiliac joint. Clin Biomech. 2003;18:99–105.
26. Pool-Goudzwaard AL, Kleinrensink GJ, Snijders CJ, Entius C, Stoeckart R. The sacroiliac part of the iliolumbar ligament. J Anat. 2001;199(Part 4):457–463.
27. Sturesson B, Selvik G, Uden A. Movements of the sacroiliac joints. A roentgen stereophotogrammetric analysis. Spine. 1989;14(2):162–165.
28. Pool-Goudzwaard AL, Vleeming A, Stoeckart R, Snijders CJ, Mens JM. Insufficient lumbopelvic stability: a clinical, anatomical and biomechanical approach to 'a-specific' low back pain. Man Ther. 1998;3(1):12–20.
29. Vleeming A, Pool-Goudzwaard AL, Stoeckart R, van Wingerden J, Snijders C. The posterior layer of the thoracolumbar fascia. Its function in load transfer from spine to legs. Spine. 1995;20:753–758.
30. Miller JA, Schultz AB, Andersson GB. Load-displacement behavior of sacroiliac joints. J Orthop Res. 1987;5(1):92–101.
31. Vleeming A, Buyruk HM, Stoeckart R, Karamursel S, Snijders CJ. An integrated therapy for peripartum pelvic instability: a study of the biomechanical effects of pelvic belts. Am J Obstet Gynecol. 1992;166(4):1243–1247.
32. Goode A, Hegedus E, Sizer PS, Brismee JM, Linberg A, Cook C. Three dimensional movements of the sacroiliac joint: A systematic review of the literature and assessment of clinical utility. J Man Manipulative Ther. 2007;16(2):25–38

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
33. Walheim GG, Selvik G. Mobility of the pubic symphysis. In vivo measurements with an electromechanic method and a roentgen stereophotogrammetric method. Clin Orthop. 1984;(191):129–135.
34. Meissner A, Fell M, Wilk R, Boenick U, Rahmanzadeh R. (Abstract). Biomechanics of the pubic symphysis. Which forces lead to mobility of the symphysis in physiological conditions? Unfallchirurg. 1996;99:415–421.
35. Berezin D. Pelvic insufficiency during pregnancy and after parturition. Acta Obst Gynecol Scand.1954;23:1–130.
36. Mens J, Vleeming A, Snijders C, Stam H, Ginai A. The active straight leg raising test and mobility of the pelvic joints. Eur Spine J. 1999;8:468–473.
37. Rieger H, Winckler S, Wetterkamp D, Overbeck J. Clinical and biomechanical aspects of external fixation of the pelvis. Clin Biomech. 1996;11:322–327.
38. Abramson D, Sumner MR, Wilson PD. Relaxation of the pelvic joints in pregnancy. Surg Gynecol Obst. 1934;58:595–613.
39. Death A, Kirby R, MacMillan C. Pelvic ring mobility: assessment by stress radiography. Arch Phys Med Rehabil. 1982;63:204–206.
40. Vleeming A, Pool-Goudzwaard AL, Hammudoghlu D, Stoeckart R, Snijders CJ, Mens JM. The function of the long dorsal sacroiliac ligament: its implication for understanding low back pain. Spine. 1996;21(5):556–562.
41. Vleeming A, Mooney V, Dorman T, Snijders C, Stoeckart R. Movement stability and low back pain: the essential role of the pelvis. New York; Churchill Livingstone: 1997.
42. Sturesson B, Uden A, Vleeming A. A radiostereometric analysis of movements of the sacroiliac joints during the standing hip flexion test. Spine. 2000;25(3):364–368.
43. Sturesson B, Uden A, Vleeming A. A radiostereometric analysis of the movements of the sacroiliac joints in the reciprocal straddle position. Spine. 2000;25(2):214–217.
44. Richardson C, Snijders C, Hides J, Damen L, Pas M, Storm J. The relation between the transverse abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine. 2002;27:399–405.
45. Kidd AW, Magee S, Richardson CA. Reliability of real-time ultrasound for the assessment of transversus abdominis function. J Gravit Physiol. 2002;9(1):P131–132.
46. Hungerford B, Gilleard W, Hodges P. Evidence of altered lumbopelvic muscle recruitment in the presence of sacroiliac joint pain. Spine. 2003;28(14):1593–1600.
47. Hodges P. Is there a role for the transversus abdominus in lumbo-pelvic stability? Man Ther. 1999;4:74–86.
48. Broadhurst NA, Bond MJ. Pain provocation tests for the assessment of sacroiliac joint dysfunction. J Spinal Disord. 1998;11(4):341–345.
49. Lee EY, Margherita AJ, Gierada DS, Narra VR. MRI of piriformis syndrome. AJR Am J Roentgenol. 2004;183(1):63–64.
50. Pool-Goudzwaard A, van Dijke G, van Gurp M, Mulder P, Snijders C, Stoeckart R. Contribution of pelvic floor muscles to stiffness of the pelvic ring. Clin Biomech. 2004;19:564–571.
51. Hodges P, Richardson R. Contraction of the abdominal muscles associated with movement of the lower limb. Phys Ther. 1997;77:1132–1144.
52. Shirley D, Hodges P, Eriksson A, Gandevia S. Spinal stiffness changes throughout the respiratory cycle. J Appl Physiol. 2003;95:1467–1475.
53. O’Sullivan P, Beales D, Beetham J, et al. Altered motor control strategies in subjects with sacroiliac joint pain during the active straight leg raise test. Spine. 2002;27:E1–E8.
54. Hodges P, Richardson C. Feedforward contraction of transverses abdominus is not influenced by the direction of arm movement. Exp Brain Res. 1997;114:362–370.
55. Moseley G, Hodges P, Gandevia S. Deep and superficial fibers of the lumbar multifidus muscle are differentially active during voluntary arm movements. Spine. 2002;27:29–36.
56. Jemmett RS, Macdonald DA, Agur AM. Anatomical relationships between selected segmental muscles of the lumbar spine in the context of multi-planar segmental motion: a preliminary investigation. Man Ther. 2004;9(4):203–210.

Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ
57. Andersson EA, Oddsson LI, Grundstrom H, Nilsson J, Thorstensson A. EMG activities of the quadratus lumborum and erector spinae muscles during flexion-relaxation and other motor tasks. Clin Biomech. 1996;11(7):392–400.
58. McGill S, Juker D, Kropf P. Quantitative intramuscular myoelectric activity of quadratus lumborum during a wide variety of tasks. Clin Biomech. 1996;11(3):170–172.
59. van Wingerden JP, Vleeming A, Buyruk HM, Raissadat K. Stabilization of the sacroiliac joint in vivo: verification of muscular contribution to force closure of the pelvis. Eur Spine J. 2004;13(3):199–205.
60. Vleeming A, Albert H, Ostgaard H, Stuge B, Sturesson B. European Guideline on the Diagnosis and Treatment of Pelvic Girdle Pain. February 2, 2005.
61. Damen L, Buyruk HM, Guler-Uysal F, Lotgering FK, Snijders CJ, Stam HJ. The prognostic value of asymmetric laxity of the sacroiliac joints in pregnancy-related pelvic pain. Spine. 2002;27(24):2820–2824.
62. Wang M, Dumas GA. Mechanical behavior of the female sacroiliac joint and influence of the anterior and posterior sacroiliac ligaments under sagittal loads. Clin Biomech. 1998;13(4-5):293–299.
63. Mooney V, Puzos R, Vleeming A, Gulick J, Swenski D. Exercise treatment for sacroiliac pain. Orthopedics. 2001;24:29–32.