Anastomosing Hemangioma of the Genitourinary System · Anatomic Pathology / Anastomosing Hemangioma...
8
450 Am J Clin Pathol 2011;136:450-457 450 DOI: 10.1309/AJCPJPW34QCQYTMT © American Society for Clinical Pathology Anatomic Pathology / Anastomosing Hemangioma of the Kidney and Ovary Anastomosing Hemangioma of the Genitourinary System Eight Cases in the Kidney and Ovary With Immunohistochemical and Ultrastructural Analysis Oleksandr N. Kryvenko, MD, 1 Nilesh S. Gupta, MD, 1 Frederick A. Meier, MD, 1 Min W. Lee, MD, 1 and Jonathan I. Epstein, MD 2 Key Words: Anastomosing hemangioma; Genitourinary; Intravascular; Hyaline globules DOI: 10.1309/AJCPJPW34QCQYTMT Abstract We describe 3 ovarian and 5 renal anastomosing hemangiomas. One manifested with polycythemia, others were incidental; none recurred. The mean patient age was 58 years. Three hemangiomas developed in end-stage renal disease. Tumors were well-demarcated, mahogany brown, spongy lesions measuring 0.1 to 5 cm. Tortuous large vessels fed and drained tightly packed anastomosing sinusoidal capillary channels. Four hemangiomas exhibited lobular architecture, central edema/hyalinization, and intravascular growth. Five cases had thrombosis, hemorrhage, and hemosiderin. One ovarian tumor induced stromal luteinization. Three tumors had foci of extramedullary hematopoiesis (one associated with polycythemia). Six cases demonstrated eosinophilic intracytoplasmic globules. Three cases included hobnail endothelial cells. Atypia was minimal and mitoses were absent in all cases. We find this vascular neoplasm unique for the genitourinary system. Despite selected features mimicking angiosarcoma, our data support its benign nature. The current study expands the gross and radiographic appearance, clinical aspects, and ultrastructure, with the first report of the lesion occurring in the ovary. Primary vascular tumors of the genitourinary system are rare. From multiple institutions, Brown et al 1 found only 25 cases of vascular tumor and tumor-like lesions of the kidney. These included 3 arteriovenous malformations, 8 angiosarcomas, and 14 capillary hemangiomas. 1 Montgomery and Epstein 2 recently described 6 cases of a new variant of a benign vascular tumor involving the kidneys, perinephric adipose tissue, and testes, which they designated anastomosing hemangioma. Ovarian hemangiomas are reported as isolated cases. 3-8 The current study presents an additional 8 anastomosing hemangiomas (ovary and kidney) in 7 patients encountered in our practice during a 12-year period. Materials and Methods The 3 hemangiomas from the ovary and 5 from the kidney in this study were diagnosed at the Henry Ford Hospital, Detroit, MI, from 1999 to 2011. Clinical information and follow-up data were obtained from the institutional electronic medical record system. H&E-stained slides from all cases were reviewed, and the following panel of immunohistochemical stains was performed in various combinations using standard immunohistochemical procedures after microwave pretreatment: CD31, CD34, factor VIII–related protein, κ light chain, λ light chain, hemoglobin A, smooth muscle actin, chromogranin, pancytokeratin (AE1/ AE3), HMB-45, Melan-A, α-fetoprotein, and S-100. In the immunohistochemical stains, 3'3'-diaminobenzidine was used as the chromogen. Periodic acid–Schiff stains with and without diastase digestion (PAS-D and PAS, respectively) were also performed in all cases. To examine further the
Transcript of Anastomosing Hemangioma of the Genitourinary System · Anatomic Pathology / Anastomosing Hemangioma...
450 Am J Clin Pathol 2011;136:450-457450 DOI: 10.1309/AJCPJPW34QCQYTMT
© American Society for Clinical Pathology
Anatomic Pathology / Anastomosing Hemangioma of the Kidney and Ovary
Anastomosing Hemangioma of the Genitourinary System
Eight Cases in the Kidney and Ovary With Immunohistochemical and Ultrastructural Analysis
Oleksandr N. Kryvenko, MD,1 Nilesh S. Gupta, MD,1 Frederick A. Meier, MD,1 Min W. Lee, MD,1 and Jonathan I. Epstein, MD2
Key Words: Anastomosing hemangioma; Genitourinary; Intravascular; Hyaline globules
DOI: 10.1309/AJCPJPW34QCQYTMT
A b s t r a c t
We describe 3 ovarian and 5 renal anastomosing hemangiomas. One manifested with polycythemia, others were incidental; none recurred. The mean patient age was 58 years. Three hemangiomas developed in end-stage renal disease. Tumors were well-demarcated, mahogany brown, spongy lesions measuring 0.1 to 5 cm. Tortuous large vessels fed and drained tightly packed anastomosing sinusoidal capillary channels. Four hemangiomas exhibited lobular architecture, central edema/hyalinization, and intravascular growth. Five cases had thrombosis, hemorrhage, and hemosiderin. One ovarian tumor induced stromal luteinization. Three tumors had foci of extramedullary hematopoiesis (one associated with polycythemia). Six cases demonstrated eosinophilic intracytoplasmic globules. Three cases included hobnail endothelial cells. Atypia was minimal and mitoses were absent in all cases. We find this vascular neoplasm unique for the genitourinary system. Despite selected features mimicking angiosarcoma, our data support its benign nature. The current study expands the gross and radiographic appearance, clinical aspects, and ultrastructure, with the first report of the lesion occurring in the ovary.
Primary vascular tumors of the genitourinary system are rare. From multiple institutions, Brown et al1 found only 25 cases of vascular tumor and tumor-like lesions of the kidney. These included 3 arteriovenous malformations, 8 angiosarcomas, and 14 capillary hemangiomas.1 Montgomery and Epstein2 recently described 6 cases of a new variant of a benign vascular tumor involving the kidneys, perinephric adipose tissue, and testes, which they designated anastomosing hemangioma. Ovarian hemangiomas are reported as isolated cases.3-8 The current study presents an additional 8 anastomosing hemangiomas (ovary and kidney) in 7 patients encountered in our practice during a 12-year period.
Materials and Methods
The 3 hemangiomas from the ovary and 5 from the kidney in this study were diagnosed at the Henry Ford Hospital, Detroit, MI, from 1999 to 2011. Clinical information and follow-up data were obtained from the institutional electronic medical record system. H&E-stained slides from all cases were reviewed, and the following panel of immunohistochemical stains was performed in various combinations using standard immunohistochemical procedures after microwave pretreatment: CD31, CD34, factor VIII–related protein, κ light chain, λ light chain, hemoglobin A, smooth muscle actin, chromogranin, pancytokeratin (AE1/AE3), HMB-45, Melan-A, α-fetoprotein, and S-100. In the immunohistochemical stains, 3'3'-diaminobenzidine was used as the chromogen. Periodic acid–Schiff stains with and without diastase digestion (PAS-D and PAS, respectively) were also performed in all cases. To examine further the

Am J Clin Pathol 2011;136:450-457 451451 DOI: 10.1309/AJCPJPW34QCQYTMT 451
© American Society for Clinical Pathology
Anatomic Pathology / Original Article
nature of the eosinophilic globules, formalin-fixed, paraffin-embedded tissue samples from 2 cases (1 from the kidney and 1 from the ovary) were reprocessed for electron microscopy using the method described by Wang and Minassian.9 The current series includes none of the previously described cases of anastomosing hemangioma.2
Results
Clinical and Radiographic ManifestationsClinicopathologic features are listed in ❚Table 1❚. Patients'
ages ranged from 39 to 77 years (mean, 58 years). Of the 5 kidney tumors, 4 were in women. The 3 ovarian lesions and 4 kidney tumors in women were incidental findings found during radiographic investigations for other indications or identified in surgical specimens removed for unrelated reasons. Anastomosing hemangioma developed in an end-stage kidney in 3 of the 4 renal tumors occurring in women, bilaterally in 1 patient. The remaining kidney tumor was detected by contrast-enhanced computed tomography (CT) abdominal scan in a 39-year-old man with a 4-year history of polycythemia and hypertension. In this case, the only man in the series, polycythemia and hypertension resolved after nephrectomy.
The ovarian lesions were subtle radiographically. The patient whose ovarian hemangioma measured 1.1 cm (case 3) underwent contrast-enhanced CT and ultrasound imaging that failed to detect the lesion. The same was true for an ultrasound examination in a second patient with an ovarian tumor (case 1). Records of radiologic examination were not available for the third patient with an ovarian hemangioma (case 2).
In all 5 cases of renal tumors, there was no history of hematuria, flank pain, or other clinical syndromes that could be attributed to the kidney lesions. The 3 renal
hemangiomas were seen on contrast-enhanced CT scans as well-demarcated heterogeneous masses enhancing in the arterial phase of contrast infusion ❚Image 1A❚. In the patient with bilateral hemangiomas, the larger lesion was seen as a solid, well-demarcated mass on CT, whereas the smaller lesion was not visible.
Macroscopic AppearanceHemangiomas ranged from 1 mm to 5 cm (Table 1). All
but one case presented as a single unilateral lesion. Renal hemangiomas were larger (mean, 1.8 cm) than those in the ovaries (mean, ~0.5 cm). Tumors were mahogany brown, with a spongy consistency, and had well-demarcated borders, but no encapsulation ❚Image 1B❚. In the ovaries, the 2 smaller tumors were located only in the cortex, but the larger tumor involved the cortical and medullary layers. Of the renal tumors, 1 was hilar, 3 spanned the medulla and cortex of the kidney, and 1 abutted the renal capsule and was located in the perinephric adipose tissue.
Histologic FeaturesAt scanning magnification, ovarian anastomosing
hemangiomas were all distinct nodular lesions, well demarcated from the surrounding uninvolved ovarian tissue. The 2 larger renal hemangiomas (cases 5 and 6) were separated from the surrounding renal parenchyma or perinephric adipose tissue by a thin, fibrous capsule. In contrast, the smaller renal lesions (cases 4 and 7) merged with the surrounding renal parenchyma, entrapping renal tubules.
Higher power revealed that the hemangiomas were composed of tightly packed capillary channels with a focal, anastomosing sinusoidal-like pattern. The 4 larger hemangiomas (cases 3-6) demonstrated a vaguely lobular architecture with intermixed large areas of loose stromal edema and/or stromal hyalinization between the cellular
❚Table 1❚Clinicopathologic Features in Eight Cases of Anastomosing Hemangiomas
Case No./Sex/Age (y) Tumor Location Clinical Manifestations Tumor Size Follow-up (mo)
1/F/70 Ovary, right, cortex Endometrial carcinoma 2 mm NED (25)2/F/49 Ovary, right, cortex Benign bilateral serous cysts 1 mm NED (16)3/F/77 Ovary, left, cortex and medulla Serous cystadenoma 1.1 cm NED (32)4/F/51 Kidney, right, hilum Found during evaluation for kidney 1 cm NED (7) transplantation for ESRD 5/M/39 Kidney, right, parenchyma Chronic polycythemia; incidentally 5 cm NED (122) CT-detected renal mass6/F/67 Kidney, left, perinephric Pulmonary embolism after knee 1.2 cm NED (6) replacement; incidentally CT-detected renal mass7/F/54* Kidneys, right and left, parenchyma Found during evaluation for kidney 1.2 and 0.6 cm NED (3) transplantation for ESRD
ESRD, end-stage renal disease; NED, no evidence of disease.* The hemangiomas in both kidneys represent 2 cases.

452 Am J Clin Pathol 2011;136:450-457452 DOI: 10.1309/AJCPJPW34QCQYTMT
© American Society for Clinical Pathology
Kryvenko et al / Anastomosing Hemangioma of the Kidney and Ovary
zones of vascular proliferation ❚Image 2❚. Tortuous “feeding” and draining vessels of large caliber (arteries and veins) were present in the 5 larger hemangiomas. Three cases demonstrated zones of sclerosis and deposition of collagen between the sinusoidal vessels ❚Image 3❚ and ❚Image 4B❚. Scant lymphocytes formed rare lymphoid aggregates, but no plasma cells or acute inflammatory cells were seen in these lesions. The 4 larger tumors also demonstrated tufted vascular
proliferation inside cystically dilated vascular spaces lined by flat endothelium (Image 3). Scattered intravascular thrombi associated with extravasated, intact RBCs and hemosiderin were seen in 4 renal and 1 ovarian hemangioma (5/8 [63%]). The largest ovarian hemangioma (case 3) was associated with stromal luteinization around the tumor and in tongues of ovarian stroma that extended between the tufts of proliferating blood vessels ❚Image 5❚. No stromal luteinization was seen
A B
❚Image 1❚ A, Computed tomography scan demonstrating renal hemangioma enhancing in arterial phase of contrast infusion (arrow). B, Gross image with well-circumscribed mahogany nodule in the renal hilum. A cluster of vessels can be seen within the center of the lesion (same case as in A).
❚Image 2❚ Low magnification demonstrating vaguely lobular architecture of hemangioma with intermixed loose edematous areas. Note the presence of a large “feeding” vessel in vascular area (H&E, ×40).
❚Image 3❚ Intravascular growth pattern of hemangioma (H&E, ×40). CD31 stain (inset) highlights hemangioma vasculature and endothelial lining of surrounding vascular space. Note the entrapped renal tubules that are negative for CD31 (×40).
Am J Clin Pathol 2011;136:450-457 453453 DOI: 10.1309/AJCPJPW34QCQYTMT 453
© American Society for Clinical Pathology
Anatomic Pathology / Original Article
in 2 other ovarian hemangiomas. Areas of extramedullary hematopoiesis were seen in the renal tumor from the man with chronic polycythemia ❚Image 6❚ and in both tumors from a patient with bilateral hemangiomas arising in end-stage renal disease (case 7). No other findings were seen in a kidney from the patient with long-lasting polycythemia, which could explain such a clinical presentation.
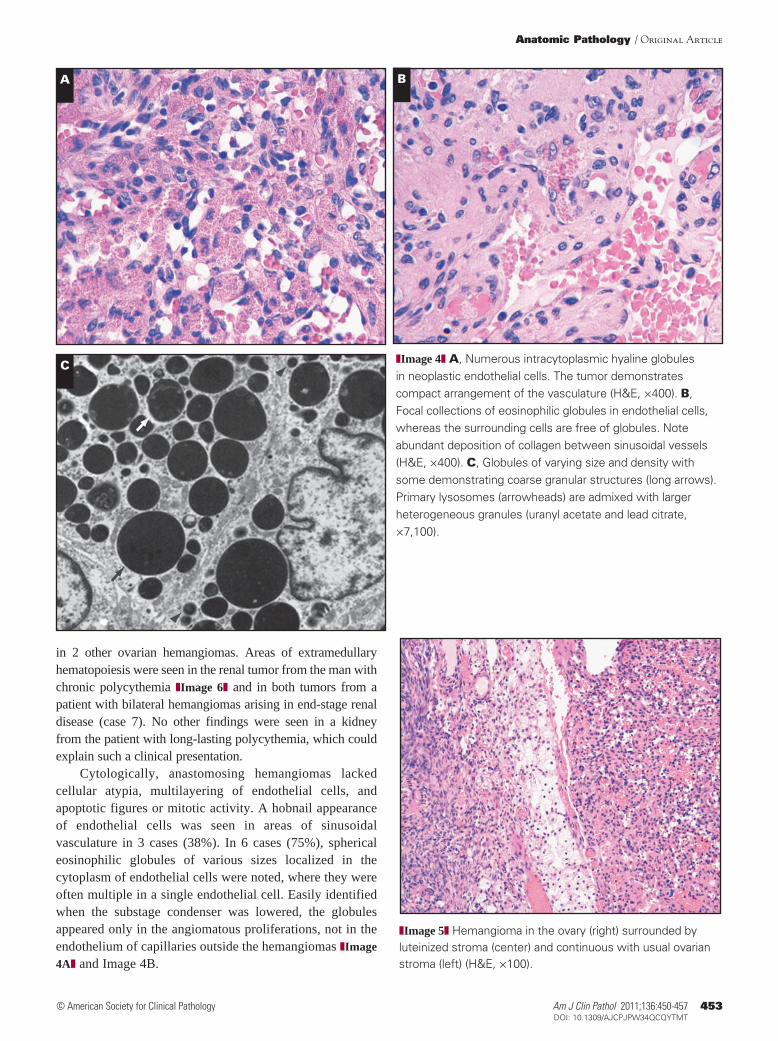
Cytologically, anastomosing hemangiomas lacked cellular atypia, multilayering of endothelial cells, and apoptotic figures or mitotic activity. A hobnail appearance of endothelial cells was seen in areas of sinusoidal vasculature in 3 cases (38%). In 6 cases (75%), spherical eosinophilic globules of various sizes localized in the cytoplasm of endothelial cells were noted, where they were often multiple in a single endothelial cell. Easily identified when the substage condenser was lowered, the globules appeared only in the angiomatous proliferations, not in the endothelium of capillaries outside the hemangiomas ❚Image 4A❚ and Image 4B.
A B
C❚Image 4❚ A, Numerous intracytoplasmic hyaline globules in neoplastic endothelial cells. The tumor demonstrates compact arrangement of the vasculature (H&E, ×400). B, Focal collections of eosinophilic globules in endothelial cells, whereas the surrounding cells are free of globules. Note abundant deposition of collagen between sinusoidal vessels (H&E, ×400). C, Globules of varying size and density with some demonstrating coarse granular structures (long arrows). Primary lysosomes (arrowheads) are admixed with larger heterogeneous granules (uranyl acetate and lead citrate, ×7,100).
❚Image 5❚ Hemangioma in the ovary (right) surrounded by luteinized stroma (center) and continuous with usual ovarian stroma (left) (H&E, ×100).

454 Am J Clin Pathol 2011;136:450-457454 DOI: 10.1309/AJCPJPW34QCQYTMT
© American Society for Clinical Pathology
Kryvenko et al / Anastomosing Hemangioma of the Kidney and Ovary
Immunohistochemical and Histochemical FindingsCD34 was immunoreactive in all 8 lesions. CD31 and
factor VIII–related protein were positive in all 6 lesions studied. All showed similar positive reactivity in endothelial cells of the proliferating tufts and along the cystically dilated spaces surrounding the vascular proliferations (Image 3). The eosinophilic globules were diffusely and strongly PAS+ before and after diastase digestion in all 6 cases that had these globules.
The following immunostains were negative in all lesions studied: κ and λ light chain (n = 5), pancytokeratin (n = 5), Melan-A (n = 2), HMB-45 (n = 2), chromogranin (n = 3), α-fetoprotein (n = 3), muscle-specific actin (n = 6), and hemoglobin A (n = 5).
Electron Microscopic FindingsUltrastructural examination of 1 ovarian and 1 renal
hemangioma showed good preservation of structures to the level of organelles. Homogeneous electron-dense globules within the endothelial cytoplasm were demonstrated in both cases located to the endothelial cells (Weibel-Palade and basal lamina formation were seen as well). The globules ranged from 170 to 450 nm; some had coarse internal granular structures within the homogeneously electron-dense matrix. Increased primary lysosomes were present in the cytoplasm of involved endothelial cells ❚Image 4C❚.
PrognosisAll patients were without recurrence with an average
follow-up of 27 months (range, 3-122 months).
Discussion
Hemangiomas are much more commonly located in the skin and subcutaneous soft tissues than in viscera. In the viscera, the liver is the most common location, and hepatic hemangiomas tend to be of the cavernous type. Similarly, most previously described renal and ovarian hemangiomas have also been classified as cavernous rather than capillary.4,7,10 However, Gehrig et al3 reported a “capillary hemangioma” of the ovary, and Nation11 reported a case of renal capillary hemangioma more than half a century ago. Unfortunately, these earlier published descriptions do not permit morphologic correlation with the cases in our series.
The reported clinical manifestations of ovarian hemangiomas include “apoplexy” (hemorrhage) within the ovarian mass, ascites, elevation of the CA-125 cancer marker in serum, and associated endometrial hyperplasia or carcinoma.3-8 In our series, all ovarian hemangiomas were incidental findings.
Reported clinical manifestations of renal hemangiomas are hematuria and flank pain, but a significant proportion
of these lesions are found as incidental findings. Of our 5 renal hemangiomas, 1 demonstrated an intriguing, previously unreported association of polycythemia due to extramedullary hematopoiesis. In this case, clinical polycythemia, which had persisted for 4 years, disappeared after the hemangioma was removed by a nephrectomy. This presentation may be misleading because of the reported association of renal cell carcinoma with polycythemia.12 One of the cases in the series reported by Brown et al1 also had a history of polycythemia, but the lesion in the latter report was an arteriovenous malformation and was negative for extramedullary hematopoiesis within the tumor. In the series by Montgomery and Epstein,2 2 of the 4 anastomosing hemangiomas in the kidney also demonstrated extramedullary hematopoiesis, but no association with polycythemia was reported. The 4 renal hemangiomas in our series appeared as well-demarcated, heterogeneous, solid, enhancing lesions on contrast-enhanced CT scans. This radiographic presentation is in keeping with the appearance of renal hemangiomas in other series.13,14
Microscopically, anastomosing hemangioma in the genitourinary system manifested in our series as solitary, mostly well demarcated, capillary-sized vascular proliferations supported by scattered large feeding and draining blood vessels. Larger lesions demonstrated lobulated patterns with scattered areas of stromal edema and/or stromal hyalinization with deposition of collagen and nonendothelial supporting cells between
❚Image 6❚ Extramedullary hematopoiesis composed predominantly of nucleated RBC precursors. Scattered granules of hemosiderin are present around the hematopoietic areas (H&E, ×200).

Am J Clin Pathol 2011;136:450-457 455455 DOI: 10.1309/AJCPJPW34QCQYTMT 455
© American Society for Clinical Pathology
Anatomic Pathology / Original Article
proliferating capillaries. The latter finding was reported in kidney hemangiomas and papillary and glomeruloid hemangiomas.2,15 The sinusoidal pattern observed in our series was similar to the sinusoidal patterns described by Brown et al1 and Montgomery and Epstein.2 Montgomery and Epstein2 also reported an intravascular growth pattern in 50% of their cases (3/6). This frequency is identical to the rate of occurrence of this feature in our series (4/8 [50%]). The propensity of renal hemangiomas to exhibit intravascular growth patterns has also been noted by Hull et al14 and Bhayani et al13 in their case reports. In all of our cases, the overall cytology was bland with only a focal endothelial hobnail appearance. No increased mitotic activity, spindle cells, or endothelial multilayering was seen.
One of the ovarian cases reported herein demonstrated prominent stromal luteinization in the hemangioma and in the ovarian parenchyma adjacent to the hemangioma. This stromal luteinization may have been induced by the proliferation, but it could represent an incidental finding. Stromal luteinization in ovarian hemangiomas has been reported in other series as well.3,6-8 The presence of stromal luteinization in the 77-year-old woman in our series (case 3) and the postmenopausal age in some patients from other reviewed reports leaves the defensible hypothesis that there may be a relationship between ovarian vascular proliferation and stromal luteinization.6,8
Of interest, in the context of the current report, Montgomery and Epstein2 found hyaline globules of endothelial cells in 2 of their 6 cases. Such globules have been described in cutaneous and soft tissue vascular lesions such as glomeruloid or papillary hemangioma16-19 and in Kaposi sarcoma,20,21 angiosarcoma,22 granulation tissue,20 pyogenic granuloma,20 and littoral cell angioma of the spleen,23 but no globules of this sort were described in the more recent report of renal capillary hemangiomas by Brown et al.1 These globules are a common finding in anastomosing hemangioma, which may facilitate the diagnosis but cannot be used in the differential diagnosis of Kaposi sarcoma. We interpret these granules as thanatosomes (Greek “death bodies”), secondary lysosomes whose degradation has been arrested so that the lysosomes expand, overfilled by phagocytized proteinaceous material. This observation is in keeping with other studies addressing the nature of intracytoplasmic globules in endothelial cells.20-22,24 The proteinaceous nature of this material is further supported by the positive PAS-D stain in all cases. Our immunohistochemical panel did not identify the nature of the protein in the thanatosomes and failed to support the previously stated theories that globules may represent phagocytized immunoglobulins or RBCs.18,21,24,25
In terms of differential diagnosis, Kaposi sarcoma and well-differentiated angiosarcoma also contain hyaline
globules.20-22 No predisposing factors associated with Kaposi sarcoma or angiosarcoma were seen in our cases. The dense cellularity, intravascular growth pattern, lack of circumscription with a rather infiltrative growth pattern and entrapment of renal tubules at the periphery in a minority of lesions, along with thrombosis and blood extravasation may be misinterpreted as features of malignancy. However, most cases in our series showed relative circumscription, a mixture of vessels of varying caliber, and variation in types of vessels within the proliferation. All cases revealed a lack of endothelial atypia, lack of spindling, absence of multilayering and papillary endothelial tufting, and virtually absent mitotic activity to distinguish anastomosing hemangioma from malignant vascular neoplasms.
One further needs to consider in the differential diagnosis a clear cell renal cell carcinoma that has sinusoid-like rich vascularity. Authors have encountered unusual cases of clear cell renal cell carcinoma that have undergone degenerative changes leaving large areas of loose myxohyalinized stoma with complex anastomosing capillary networks and rare indistinct clear cells ❚Image 7❚. These changes may lead to a false impression of primary vascular neoplasm in the kidney, especially in a needle core biopsy specimen of the renal mass. Pancytokeratin and/or epithelial membrane antigen immunostaining may distinguish this pattern of renal cell carcinoma from hemangioma of the kidney. Although some vascular neoplasms may express keratin, we demonstrated a lack of immunoreactivity with pancytokeratin in anastomosing hemangiomas. Angiomyolipoma could be considered in the differential diagnosis, given the presence of isolated smooth muscle cells picked up by muscle actin immunostain in the renal hemangiomas. However, even cases of angiomyolipoma with prominent vessels have totally different morphologic features characterized by large vessels with unique PEComa (perivascular epithelioid cell tumor) stromal cells radiating off the outer edge of the vessel walls. None of the cases of anastomosing hemangioma were positive for HMB-45 or Melan-A.
Some variants of glomus tumor may have an abundant vasculature network and be considered in the differential diagnosis of anastomosing hemangioma. Glomangioma and glomangiomyoma have been described in the kidney and ovary as rare mimickers of primary vascular neoplasm.26-28 In these locations, the glomus tumors may have lobular architecture and a prominent capsule, and larger tumors may have areas of stromal myxoid changes and hyalinization similar to those seen in anastomosing hemangioma.26,27 Moreover, the vascular pattern of the glomangioma described in the ovary may have a mixture of larger gaping vessels and small anastomosing sinusoidal-type vessels, further complicating the differential diagnosis with

456 Am J Clin Pathol 2011;136:450-457456 DOI: 10.1309/AJCPJPW34QCQYTMT
© American Society for Clinical Pathology
Kryvenko et al / Anastomosing Hemangioma of the Kidney and Ovary
References
1. Brown JG, Folpe AL, Rao P, et al. Primary vascular tumors and tumor-like lesions of the kidney: a clinicopathologic analysis of 25 cases. Am J Surg Pathol. 2010;34:942-949.
2. Montgomery E, Epstein JI. Anastomosing hemangioma of the genitourinary tract: a lesion mimicking angiosarcoma. Am J Surg Pathol. 2009;33:1364-1369.
3. Gehrig PA, Fowler WC Jr, Lininger RA. Ovarian capillary hemangioma presenting as an adnexal mass with massive ascites and elevated CA-125. Gynecol Oncol. 2000;76:130-132.
4. Gupta R, Singh S, Nigam S, et al. Benign vascular tumors of female genital tract. Int J Gynecol Cancer. 2006;16:1195-1200.
5. Koh LW, Sun YL, Koh PH, et al. Ovarian capillary hemangioma presenting as pseudo-Meigs’ syndrome: a case report. J Minim Invasive Gynecol. 2007;14:367-369.
6. Miliaras D, Papaemmanouil S, Blatzas G. Ovarian capillary hemangioma and stromal luteinization: a case study with hormonal receptor evaluation. Eur J Gynaecol Oncol. 2001;22:369-371.
7. Uppal S, Heller DS, Majmudar B. Ovarian hemangioma: report of three cases and review of the literature. Arch Gynecol Obstet. 2004;270:1-5.
8. Yamawaki T, Hirai Y, Takeshima N, et al. Ovarian hemangioma associated with concomitant stromal luteinization and ascites. Gynecol Oncol. 1996;61:438-441.
9. Wang NS, Minassian H. The formaldehyde-fixed and paraffin-embedded tissues for diagnostic transmission electron microscopy: a retrospective and prospective study. Hum Pathol. 1987;18:715-727.
10. Jahn H, Rasmussen L, Nissen HM. Hemangioma of the kidney. Urol Int. 1991;46:200-202.
11. Nation EF. Renal hemangioma. Calif Med. 1951;75:219-221.
anastomosing hemangioma.28 Regardless of vascularity, the areas composed predominantly of glomocytes can be found in vasculature-rich variants of glomus tumors, which have a pivotal role in the differential diagnosis. Immunohistochemical studies may be used to identify glomus cells positive for muscle markers (smooth muscle actin, muscle-specific actin) and negative for endothelial markers (CD31, CD34, factor VIII–related protein).
We expand the clinical and morphologic understanding of an unusual variant of hemangioma recently described in the kidney and testis.2 An identical vascular neoplasm may be seen in the ovary sharing distinct circumscription of the tumor from the surrounding tissue as seen in testis. In the kidney, anastomosing hemangioma may have infiltrative and intravascular growth patterns, hemorrhage, and high cellularity, which should not be interpreted as signs of malignancy.
From the 1Department of Pathology and Laboratory Medicine, Henry Ford Hospital, Detroit, MI; and 2Department of Pathology, The Johns Hopkins Medical Institutions, Baltimore, MD.
Address reprint requests to Dr Kryvenko: Pathology and Laboratory Medicine, Henry Ford Hospital, 2799 W Grand Blvd, Detroit, MI 48202.
Acknowledgments: We thank Arthur Gaba, MD, for contributing the ovarian hemangiomas to our series and Kathleen Roszka and Thomas Christopherson for expert immunohistochemical and electron microscopy technical services, respectively. We also thank Natalia Draga for expert histologic technical services.
❚Image 7❚ A, Rich anastomosing vascular network in renal cell clear cell carcinoma with degenerative changes. Carcinoma cells are difficult to recognize, and the tumor may be misinterpreted as a vascular neoplasm (H&E, ×100). B, CD31 stain highlights rich vasculature (×100), and only occasional clusters of carcinoma cells are demonstrated by pancytokeratin stain (inset, ×200). Note surrounding vessels negative for cytokeratin (inset).
A B

Am J Clin Pathol 2011;136:450-457 457457 DOI: 10.1309/AJCPJPW34QCQYTMT 457
© American Society for Clinical Pathology
Anatomic Pathology / Original Article
21. Kao GF, Johnson FB, Sulica VI. The nature of hyaline (eosinophilic) globules and vascular slits of Kaposi’s sarcoma. Am J Dermatopathol. 1990;12:256-267.
22. Vuletin JC, Wajsbort RR, Ghali V. Primary retroperitoneal angiosarcoma with eosinophilic globules: a combined light-microscopic, immunohistochemical, and ultrastructural study. Arch Pathol Lab Med. 1990;114:618-622.
23. Michal M, Skalova A, Fakan F, et al. Littoral cell angioma of the spleen: a case report with ultrastructural and immunohistochemical observations. Zentralbl Pathol. 1993;139:361-365.
24. Papadimitriou JC, Drachenberg CB, Brenner DS, et al. “Thanatosomes”: a unifying morphogenetic concept for tumor hyaline globules related to apoptosis. Hum Pathol. 2000;31:1455-1465.
25. Zak FG, Solomon A, Fellner MJ. Viscero-cutaneous angiomatosis with dysproteinaemic phagocytosis: its relation to Kaposi’s sarcoma and lymphoproliferative disorders. J Pathol Bacteriol. 1966;92:594-549.
26. Al-Ahmadie HA, Yilmaz A, Olgac S, et al. Glomus tumor of the kidney: a report of 3 cases involving renal parenchyma and review of the literature. Am J Surg Pathol. 2007;31:585-591.
27. Siddiqui NH, Rogalska A, Basil IS. Glomangiomyoma (glomus tumor) of the kidney. Arch Pathol Lab Med. 2005;129:1172-1174.
28. Slone SP, Moore GD, Parker LP, et al. Glomus tumor of the ovary masquerading as granulosa cell tumor: case report. Int J Gynecol Pathol. 2010;29:24-26.
12. Palapattu GS, Kristo B, Rajfer J. Paraneoplastic syndromes in urologic malignancy: the many faces of renal cell carcinoma. Rev Urol. 2002;4:163-170.
13. Bhayani SB, Humphrey PA, Kibel AS. Renal sinus haemangioma with inferior vena cava involvement. BJU Int. 2003;92(suppl 3):e53. doi: 10.1111/j.1464-410X.2003.04195.x
14. Hull GW III, Genega EM, Sogani PC. Intravascular capillary hemangioma presenting as a solid renal mass. J Urol. 1999;162(3 pt 1):784-785.
15. Suurmeijer AJ. Papillary hemangiomas and glomeruloid hemangiomas are distinct clinicopathological entities. Int J Surg Pathol. 2010;18:48-54.
16. Chan JK, Fletcher CD, Hicklin GA, et al. Glomeruloid hemangioma: a distinctive cutaneous lesion of multicentric Castleman’s disease associated with POEMS syndrome. Am J Surg Pathol. 1990;14:1036-1046.
17. Forman SB, Tyler WB, Ferringer TC, et al. Glomeruloid hemangiomas without POEMS syndrome: series of three cases [letter]. J Cutan Pathol. 2007;34:956-957.
18. Lee H, Meier FA, Ma CK, et al. Eosinophilic globules in 3 cases of glomeruloid hemangioma of the head and neck: a characteristic offering more evidence for thanatosomes with or without POEMS. Am J Dermatopathol. 2008;30:539-544.
19. Suurmeijer AJ, Fletcher CD. Papillary haemangioma: a distinctive cutaneous haemangioma of the head and neck area containing eosinophilic hyaline globules. Histopathology. 2007;51:638-648.
20. Fukunaga M, Silverberg SG. Hyaline globules in Kaposi’s sarcoma: a light microscopic and immunohistochemical study. Mod Pathol. 1991;4:187-90.